Embed Size (px)
DESCRIPTION
Presentation to participants of the 'Resuscitation Workshop' in the Emergency Department - Canberra Hospital, 2006
Citation preview

Ventilation: Basic Principles
Jamie Ranse
Registered Nurse
Emergency Department
The Canberra Hospital

• Introduction to Ventilation Principles
• Respiratory Anatomy and Physiology
• Indications for Ventilation
• Modes of Ventilation
• Patient Management
• Complications
• Questions
Overview

• Ventilation is the movement of air into and out of the alveoli.
Introduction
Hudak, et al, 1997, Critical Care Nursing: A Holistic Approach (7th Edn), Lippincott, Philadelphia, USA

Mechanics of Ventilation:
• Elasticity
• Compliance
• Resistance
• Pressure
• Gravity
Introduction
Hudak, et al, 1997, Critical Care Nursing: A Holistic Approach (7th Edn), Lippincott, Philadelphia, USA

• Respiratory Structures
• Respiratory Zones
• Partitioning of Respiratory Pressures
• Boyles Law
• Respiratory Volumes and Capacity
• Ventilation and Perfusion
Anatomy and Physiology

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Respiratory Structures

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Respiratory Zones

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Partitioning of Respiratory Pressures

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Boyles LawIncrease V = Decreased P
Decreased V = Increased P

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Boyles Law
• Air flows from a region of higher pressure to a region of lower pressure.
• To initiate a breath, airflow into the lungs must be precipitated by a drop in alveolar pressures.

Anatomy and Physiology
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Respiratory Volumes and Capacity

Anatomy and Physiology
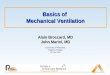
perfusion without ventilation = shunt
normal ventilation and perfusion
ventilation without perfusion = dead space
airway
venous blood arterial blood
Porth CM, 1998, Pathophysiology (5th Edn), Lippincott, Philadelphia, USA
Ventilation
and
Perfusion

• Airway Compromise (potential)
• Respiratory Failure– pH: <7.25
– PaCO2: >50 mmHg
– PaO2: <50 mmHg
• Increased Work of Breathing
• Head Injury Management
Indications for Ventilation
Hudak, et al, 1997, Critical Care Nursing: A Holistic Approach (7th Edn), Lippincott, Philadelphia, USA

• Support though illness• Reversal of hypoxemia• Reversal of acute respiratory acidosis• Relief of respiratory distress• Resting of the ventilatory muscles• Decrease in oxygen consumption• Reduction in intracranial pressures• Stabilisation of the chest wall
Objective of Ventilation
Hudak, et al, 1997, Critical Care Nursing: A Holistic Approach (7th Edn), Lippincott, Philadelphia, USA

• freq
• Vt
• MV
• I:E ratio
• Trigger
• Ramp
Modes of Ventilation
Diepenbrock NH, 1999, Quick Reference to Critical Care, Lippincott, Philadelphia, USA: P166.
• Pmax
• Paw
• fspn
• MVspn
• PEEP

• Controlled – Pressure Control (PC)– Volume Control (VC)
• Supported– Continuous Positive Airway Pressure (CPAP) – Pressure Support (PS)
• Combined– SIMV (PC) + PS– SIMV (VC) + PS
Modes of Ventilation
Diepenbrock NH, 1999, Quick Reference to Critical Care, Lippincott, Philadelphia, USA: P166.

Modes of Ventilation: Control
Controlled Mechanical Ventilation:
• The Minute Volume is determined by the ventilator
• The patient has no option to override the ventilator


Modes of Ventilation: Control
Pressure Control:
• A preset peak inspiratory pressure is delivered to the patient at a preset respiratory rate
• Volume is not preset and is determined by the mechanics of ventilation.
(elasticity, compliance, resistance, pressure, gravity)

Modes of Ventilation: Control
Volume Control:
• A preset tidal volume is delivered at a present respiratory rate
• 7 – 10 mls/kg 50kg = 350 – 500mls
70kg = 490 – 700mls
90kg = 630 – 900mls

Modes of Ventilation: Support
Continuous Positive Airway Pressure:
• A spontaneous breathing mode, where the patient generates their own breath
• The ventilator maintains a constant positive pressure on expiration (PEEP)
• Aims to increase Functional Residual Capacity

Modes of Ventilation: Support
Pressure Support:
• A spontaneous breathing mode
• Need for additional support to achieve optimal tidal volumes
• Ventilator delivers a constant preset pressure on inspiration
CPAP + PS = BiPAP

Modes of Ventilation: Combined
Synchronised Intermitted Mandatory Ventilation:
• Similar to IMV
• If the patient initiates a breath and the ventilator synchronises so the ventilator doesn’t deliver a breath at the same time

Modes of Ventilation: Combined
SIMV (PC) + PS:
• Pressure controlled ventilation with pressure support on spontaneous breaths
SIMV (VC) + PS:
• Volume controlled ventilation with pressure support on spontaneous breaths

SIMV (VC) + PS
Freq: 10
Vt: 500
(MV = 5.0)
PEEP: 5
PS: 10

• Monitoring
• Suctioning
• Other– Sedation– Positioning– Oral and Eye Care
Patient Management

• ECG
• SpO2
• ETCO2
• Alarm limits• Air Entry / Work of Breathing• Ventilator observations and alarm limits• Full assessment
Patient Management:Monitoring

• PRN– Increasing airway pressures
– Decreasing SpO2
– Increased work of breathing
• Pre-oxygenate (100% oxygen)
• Less than 15 Seconds
Patient Management:Suctioning

Patient Management:Other
• Sedation– Propofol, Morphine and Midazolam
• Positioning– 2/24
• Oral and eye care– 2/24

• Airway– Aspiration, decreased clearance of secretions,
predisposition to infection
• Endotracheal Tube– Tube kinking, sputum plug, right main bronchus
intubation, tube migration, cuff failure, laryngeal oedema
• Mechanical– Ventilator malfunction, hypoventilation,
hyperventilation, barotrauma, pneumothorax
Complications

Questions

Ventilation: Basic Principles
Jamie Ranse
Registered Nurse
Emergency Department
The Canberra Hospital