Embed Size (px)
Citation preview

VENTILATION
Dr. Amith Sreedharan

DEFINITIONANATOMY OF THE AIRWAYSDISTRIBUTION OF VENTILATIONPULMONARY PRESSURESMECHANICS OF BREATHINGFACTORS AFFECTING VENTILATIONSPIROMETRY VOLUMESCONTROL OF BREATHINGABNORMAL VENTILATIONREFERENCES

DEFINITION
• Mass movement of gas in and out of the lungs

ANATOMY
Nostrils (Nares)• Transfer air back and forth between the
outside environment and the Nasal Cavity.• These structures serve as the primary air
intake site.


Nasal Cavity
• A chamber that transfers air and gases back and forth between the nostrils and the pharynx.
• Air is warmed and humidified – temp rises to within 1⁰ F of body temperature and to within 2-3 % of full saturation with water vapour before it reaches trachea.
• Partially filtered- turbulent filtration(>6 micron)• Clinical significance

Pharynx
• The throat passage way that allows air and gases to pass back and forth between the nasal cavity and the glottis.
• During inspiration,pressure in pharynx fall below atm.pressure
• Opposed by pharyngeal dilator muscles(genioglossus and tensor palati)
• Patency in supine position maintained by tensor palati,palatoglossus and palatopharyngeus

Epiglottis
• A flap-like structure in the lower pharynx that is located above the glottis.
• The epiglottis operates like a valve that allows air to pass through the glottis and into the trachea during breathing, but, closes over the glottis during the swallowing of food and drink to prevent choking.

Glottis
• An opening that allows air to pass back and forth between the pharynx and the larynx during breathing
• A set of cartilaginous structures and membranes that allow air to pass back and forth between the glottis and the trachea.
• The larynx (voicebox) also contains cord-like membranes that produce sounds.
Larynx

WIEBEL MODEL

Trachea
• Generation 0• Length 11 cm• Mean diameter 1.8 cm• A tube reinforced by a series of u-shaped
cartilaginous rings that passes air back and forth between the larynx and the primary bronchi.
• Lined by ciliated columnar epithelium

Main Bronchus
• Generation 1• A tubular structure that passes air back and
forth between the trachea and lobar bronchi• 2 in nos• Mean diameter – 12 mm• Irregular shaped cartilage present in the walls• The epithelial lining- ciliated columnar

LOBAR BRONCHI
• Generation 2 – 3• 5-8 in nos• Mean diameter 5 mm – 8mm• Supply lobes• Irregular shaped cartilages

Segmental Bronchi
• Generation 4• 16-20 in nos• Supplies segments• A tubular passageway that passes air back and
forth between a lobar bronchus and the remainder of a bronchial tree ( third, fourth, fifth degree branches, etc. ).
• Mean diameter 4 mm

Terminal Bronchiole
• Generations 5 - 16• One of the smallest tubular passageways in
the lung that passes air back and forth between the smallest bronchial tube and the respiratory bronchiole.
• Mean diameter 0.7mm• Cuboidal epithelium• Strong helical muscle bands in the wall

Respiratory Bronchiole
• Generations 17- 19• Transitional and respiratory zone• The smallest air tubes in the lungs that passes
air back and forth between a terminal bronchiole and an alveolar sac.
• Mean diameter 0.4mm• Cuboidal to flat epithelium

ALVEOLAR DUCTS
• Generation 20,21,22• Along with alveoli forms the lung parenchyma• Mean diameter 0.3 mm• Lined by alveolar epithelium• Thin bands of muscle in alveolar septa

Alveolar Sac
• Generation 23• Last generation of air passage• A sac-like (blind) extension of a respiratory bronchiole
that is divided into many small alveolar compartments.
• The alveolar sac will contain many small septa that act as partitions between the alveoli.
• The septa and alveolar surfaces provide surface area for gas exchange.
• 17 alveoli arise from each alveolar sac

Alveolus
• The smallest site in the lung for gas exchange.• Made up of a thin membrane that is ideal for
diffusion of gases back and forth between the air of the alveolar sac and the blood of pulmonary capillaries.
• 270 – 790 million • Mean diameter at FRC = 0.2 mm

Pulmonary acinus
• Aka primary lobule/terminal respiratory unit• Zone supplied by first order respiratory
bronchioles,alveolar ducts and alveolar sacs distal to a single terminal bronchiole.
• 30000 acinus present in human lung• Diameter = 3.5mm• Contain > 10000 alveolus


DISTRIBUTION OF VENTILATION
• Influenced by POSTURE and MANNER OF VENTILATION.
• Right lung > Left lung (larger size)• Lateral position : lower lung more ventilated• Horizontal slices: uppermost portion one third
ventilated as base.• Preferential ventilation only present at inspiratory
flow rates below 1.5 L/S.(N=0.5 L/S)• At high rate,uniform distribution.

Minute Ventilation
Total volume of air entering and leaving respiratory system each minute
Minute ventilation = VT x RRNormal respiration rate = 12 breaths/minNormal VT = 500 mLNormal minute ventilation =
500 mL x 12 breaths/min = 6000 mL/min

Alveolar Ventilation
• Volume of air reaching gas exchange areas per minute
Alveolar Ventilation = (VT x RR) – (DSV x RR)
Normal Alveolar Ventilation =(500 mL/br x 12 br/min) – (150 mL/br X 12 br/min) =4200 mL/min

DEAD SPACE• An appreciable part of each inspiration do not penetrate
to those regions of gas exchange and therefore exhaled unchanged.
• This fraction of Tidal volume(Tᵥ) = DEAD SPACE• Alveolar ventilation(VA) : Effective part of minute volume
of respiration.• Alveolar ventilation= respiratory rate × (Tᵥ - dead space)• RATIOS• VD/VT = Wasted portion of breath• VA/MV = utilised portion of MV

COMPONENTS OF DEAD SPACE
• APPARATUS DEAD SPACE: First part to be exhaled if subject is employing any form of external breathing apparatus.
• ANATOMICAL DEAD SPACE: Volume of the conducting air passages
• ALVEOLAR DEAD SPACE: Part of inspired gas that passes through anatomical dead space to mix with gas at alveolar level , but does not take part in gas exchange.

ANATOMICAL DEAD SPACEFACTORS INFLUENCING:• Size of subject – increases with size• Age – from adulthood increases 1 ml/year.• Posture- 150 ml sitting,100 ml supine• Position of neck and jaw Neck extended,jaw protruded-143 ml Normal position – 119 ml Neck flexed,chin depressed – 73 ml• Lung volume at end of inspiration- 20 ml additional An.DS/each
litre increase in LV• Tracheal intubation,tracheostomy,LMA- decreased An.DS• Drugs• With Decreased Tidal volume, An.DS decreases

ALVEOLAR DEAD SPACE
FACTORS INFLUENCING:• CARDIAC OUTPUT• PULMONARY EMBOLISM• POSTURE

PHYSIOLOGICAL DEAD SPACE
• Sum of all parts of Tidal volume that do not participate in gaseous exchange
• Sum of anatomical dead space and alveolar deadspace.• 30 % of tidal volume• Factors influencing:• Age and sex• Body size (17ml / every 10 cm ↑)• Posture (↓es in supine)• Pathology (PE,SMOKING)

PULMONARY PRESSURESAtmospheric pressure = Patm
Intra-alveolar pressure = Palv
Pressure of air in alveoliIntrapleural pressure = Pip
Pressure inside pleural sacTranspulmonary pressure = Palv – Pip
Distending pressure across the lung wall

Atmospheric Pressure
760 mm Hg at sea levelDecreases as altitude increasesIncreases under waterOther lung pressures given relative
to atmospheric (set Patm = 0 mm Hg)

Intra-alveolar Pressure
Pressure of air in alveoliGiven relative to atmospheric pressureVaries with phase of respiration
During inspiration = negative (less than atmospheric)
During expiration = positive (more than atmospheric)
Difference between Palv and Patm /(Pₐₒ) drives ventilation

Factors determining intra-alveolar pressureQuantity of air in alveoliVolume of alveoli
Lungs expand – alveolar volume increasesPalv decreasesPressure gradient drives air into lungs
Lungs recoil – alveolar volume decreasesPalv increasesPressure gradient drives air out of lungs

Intrapleural Pressure
Pressure inside pleural sacAlways negative under normal
conditionsAlways less than Palv
Varies with phase of respirationAt rest, -5 mm Hg(MEAN)

Negative pressure due to elasticity in lungs and chest wallLungs recoil inwardChest wall recoils outwardOpposing pulls on intrapleural spaceSurface tension of intrapleural fluid
hold wall and lungs together

Transpulmonary PressureTranspulmonary pressure = Palv – Pip
Distending pressure across the lung wall
Increase in transpulmonary pressure:Increase distending pressure across lungs
Lungs (alveoli) expand, increasing volume




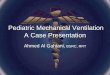
Pressure-volume curves of the lung during inspiration and expiration.HYSTERESIS


PARABOLIC (LAMINAR) FLOW PROFILE

PATTERNS OF AIRFLOW
Laminar flow.
Turbulent flow.
Transition flow

Inspiration of air into trachea via mouth and nose.Accomplished by inspiratory chest wall muscle contraction.

• TRUNK / CHEST WALLRIBCAGEABDOMENSeparated by DIAPHRAGM

DIAPHRAGM
• Membranous muscle separating abdominal cavity and chest
• SA = 900 cm²• Most important inspiratory muscle• Motor innervation: Phrenic N(C3,4,5)• Contraction Increase in lung volume

MECHANICS OF DIAPHRAGM MOVEMENT
• ‘Piston in cylinder’ Analogy• ‘Non piston’ behaviour• Combination (piston + non piston)• Combination of all the above mechanisms and
change in shape involving ‘tilting and flattening’ of diaphragm in AP direction.

RIBCAGE MUSCLES
• RIBCAGE = CYLINDER/BUCKET• Length• governed by DIAPHRAGM• And secondarily by flexion and extension of
Spine• CROSS SECTION• By movement of RIBS

MECHANICS OF RIBCAGE MUSCLES
• ‘BUCKET HANDLE’ ACTION• ‘PUMP HANDLE’ MOVEMENT

Intercostal muscles• External intercostals Deficient anteriorly Primarily inspiratory
• Internal intercostals Deficient posteriorly(less powerful) Primarily expiratory Parasternal portion is inspiratory.
• Intercostalis intima
Posture plays important role in ICM action.Extreme postural changes reverts activity of intercostal muscles

ACCESSORY MUSCLES Silent in normal breathing Increased ventilation(about 50 L/min) leads to recruitment of ACCESSORY
muscles.• MUSCLES Generally inspiratory Sternocleidomastoid M Pectoralis minor M Serrati M Extensors of vertebral column ABDOMINAL M Generally expiratory Rectus abdominis Obliques – external and internal Transversalis Muscles of pelvic floor(supportive)

INSPIRATION
• Ribcage inspiratory muscles (ext ¶sternal int ICM) and Diaphragm act in parallel to inflate the lungs.
• Scalene muscles (supportive role)• POSTURE decides the dominant role• Diaphragm contraction alone results in
widening of lower ribcage and indrawing of upper ribcage countered by IC and neck muscle

EXPIRATION
• No musculature required in quiet breathing in supine position
• Elastic recoil of lungs provide energy required for expiration and is also aided by weight of abdominal contents
• In upright position and stimulated ventilation the INTERNAL ICM and Abdominal wall M are active in returning the ribcage and Diaphragm to resting position


EFFECT OF POSTURE ON MUSCLESUPRIGHT: In Standing/Sitting position , Ribcage muscles
more used(67 % contribution)• Scalene and parasternal internal ICM supportSUPINE:Diaphragm upward(4 cm up)• Decreased FRC• Fibre length decreased in supine position• More effective contractionLATERAL: Only lower dome of Diaphragm pushed higher
into chest,upper dome is flat.• Lower dome contract effectively• Increased ventilation of lower lung.

CHEMORECEPTOR ACTIVATION
• Respiratory muscle response to hypoxia / hypercarbia for an equivalent minute volume.
• Hypoxia stimulates mostly inspiratory muscles• Hypercapnea stimulates both inspiratory and
expiratory muscles.
NEXT

Factors Affecting Pulmonary Ventilation
Lung Compliance Airway Resistance

Lung Compliance• Ease with which lungs can be stretched
VLung Compliance =
(Palv – Pip)Larger lung compliance
• Easier for inspiration• Smaller change in transpulmonary pressure
needed to bring in a given volume of airFACTORS AFFECTING COMPLIANCEElasticity• More elastic less compliant
Surface tension of lungs• Greater tension less compliant

Surface Tension in LungsThin layer fluid lines alveoliSurface tension due to attractions between water
moleculesSurface tension = force for alveoli to collapse
or resist expansion
• To Overcome Surface TensionSurfactant secreted from type II cells• Surfactant = detergent that decreases surface tension
Surfactant increases lung compliance • Makes inspiration easier

Resistance to airflow• < 1 cm H₂O pressure gradient (alveolar to atmospheric
pressure) sufficient to cause enough airflow for quiet breathing
• Greatest amount of resistance to airflow is not in minute air passages of terminal bronchioles but in some larger bronchioles and bronchi near trachea.
• In disease,smaller bronchioles play a greater role in determining airflow resistance because of small size and they are easily occluded by
Muscle contraction in their wallsEdema occuring in wallsMucus collecting in lumen

Nervous and local control of bronchial musculature
• Sympathetic dilation of bronchioles• Direct control relatively weak because few fibers
penetrate central portions of lung• Cause dilation of bronchioles• Parasympathetic constriction• Few parasympathetic fibers penetrate lung
parenchyma• Also activated by local irritation(noxious
gases,infection)• Local factors – histamine,SRS-A

FACTORS AFFECTING LUNG VOLUME

LUNG VOLUMES

• Tidal volume (TV):• The tidal volume (TV) is the volume of air that is
drawn into the lungs during inspiration from the end-expiratory position (and also leaves the lungs passively during expiration in the course of quiet breathing).

• Inspiratory reserve volume (IRV): Maximum volume of air inspired from the end-tidal inspiratory level.
• Expiratory reserve volume (ERV): The expiratory reserve volume (ERV) is the maximum volume of air that can be forcibly exhaled after a quiet expiration has been completed (i.e., from the end-expiratory position).
• Residual volume: The residual volume (RV) is the volume of air that remains in the lungs after a maximal expiratory effort. always left in lungs, even with forced expiration.Not measured with spirometer

• The functional residual capacity (FRC) is the volume of air that remains in the lungs at the end of a normal expiration.
• The inspiratory capacity (IC) is the maximum volume of air that can be inhaled from the end-expiratory position. It consists of two subdivisions:
• tidal volume and the inspiratory reserve volume (IRV).

• The total lung capacity (TLC) is the total volume of air contained in the lungs at the end of a maximum inspiration.
• The vital capacity (VC) is the volume of air that is exhaled by a maximum expiration after a maximum inspiration.
• So in total there are 4 volumes and 4 capacities.

Centres 1. Voluntary Control --- Motor Cortex
2. Involuntary (autonomic) Control --Brain Stem Pons Medulla Oblongata
• Medulla contains two centres of breathing Inspiratory Centre containing inspiratory neurones Expiratory Centre containing expiratory neurones
• For quiet breathing (eupnoea); I neurones responsible for inspiration; expiration when I neurones cease firing.
• I neurones cease (probably) by a “slow loop negative feedback” mechanism
• During exercise (hyperpnoea) I neurones inhibited by Pneumotaxic centre in the Pons region

Medullary Respiratory Centre
• Two regions: • 1) Dorsal respiratory group(DRG) – Inspiratory Centre • 2) Ventral respiratory group(VRG) – Expiratory Centre • • Probable that cells of the inspiratory centre have the
property of “intrinsic periodic firing” - responsible for the basic rhythm of ventilation
• • With all stimuli abolished inspiratory cells generate repetitive bursts of action potentials - nervous impulses along efferent nerves to respiratory muscles

• Expiratory Centre • Quiescent during normal quiet breathing • In exercise hyperpnoea when breathing is more forceful,
expiration becomes active due to the expiatory neurones. • Pneumotaxic Centre(PRG) - Upper Pons • Appears to switch off inspiration and so regulate
inspiratory volume and respiration rate.• Apneustic Centre • Neurones are suggested to have an excitatory effect on
the inspiratory neurones prolonging the ramp action potentials

Respiratory Reflexes
pH of body fluids/plasma is the most potent stimulus to the respiratory centre
↓ pH > ↑ pCO2 > ↓ pO2
Detected by 1. Peripheral Chemoreceptors aortic bodies carotid bodies 1) Small highly perfused shunts of the main arteries 2) Sensory (afferent) signals to medulla by, vagus (ao) and
glossopharyngeal (ca) 3) pH is the predominant trigger. pO2 less important except at
altitude or in disease

CHEMORECEPTORS

Central Chemoreceptors Surface of the Medulla Oblongata • Measure pH of cerebrospinal fluid (CSF) and brain tissue
fluid • Main aim of respiratory control is brain pH homeostasis
Hydrogen ions [H+] do not freely pass blood/CSF barrier • But CO2 does easily (no lactic acid effect on central
chemoreceptors) • In CSF CO2 + H2O = H+ + [HCO3 ] - H+ liberated then influences
the central chemoreceptors

BRAIN STEM
PHRENIC AND INTERCOSTAL NERVES
MOTOR NEURONS
RESPIRATORY MUSCLES
LUNGS
NEUROMUSCULAR JUNCTION
VENTILATION

ABNORMALITIES
APNEUSTIC BREATHING• occurs with lesions of the pons and is characterized
by prolonged inspiratory duration.KUSSMAUL BREATHING• Seen in ketoacidosis• Virtually no pause between breaths(air hunger)GASPING RESPIRATION(CEREBRAL HYPOXIA)• Irregular,quick inspirations associated with extensions
of the neck and followed by a long expiratory pause.

Cheyne-Stokes breathing is one form of periodic breathing characterized by a cyclic rise and fall in ventilation with recurrent periods of apnea or near apnea.
• Hyperapneic phase more than apneic phase• Supramedullary lesions(tegmentum of pons)
Biot’s breathing• tidal volumes of fixed amplitude are separated by periods
of apnea.• Apneas may be separated by periods of gradually
increasing and decreasing breathing



REFERENCES
1. FISHMAN’S PULMONARY DISEASES AND DSISORDERS
2. CROFTON AND DOUGLAS’S RESPIRATORY DISEASES
3. NUNN’S APPLIED RESPIRATORY PHYSIOLOGY4. GUYTON’S TEXTBOOK OF PHYSIOLOGY5. GANONG REVIEW OF PHYSIOLOGY6. PLEURAL DISEASES - LIGHT

THANK YOU