Embed Size (px)
Citation preview
VITAMIN D &
HYPERPARATHYROIDISM
-Dr.Apoorva.E
PG,DCMS
VITAMIN-D AND ITS METABOLISM
- Vitamin D is a fat soluble vitamin.
- It is the precursor of 1,25-dihydroxycholecalciferol which is the active form of vitamin D secreted by the kidney, under the control of parathyroid hormone.
- Its deficiency causes rickets in children and osteomalacia in adults.
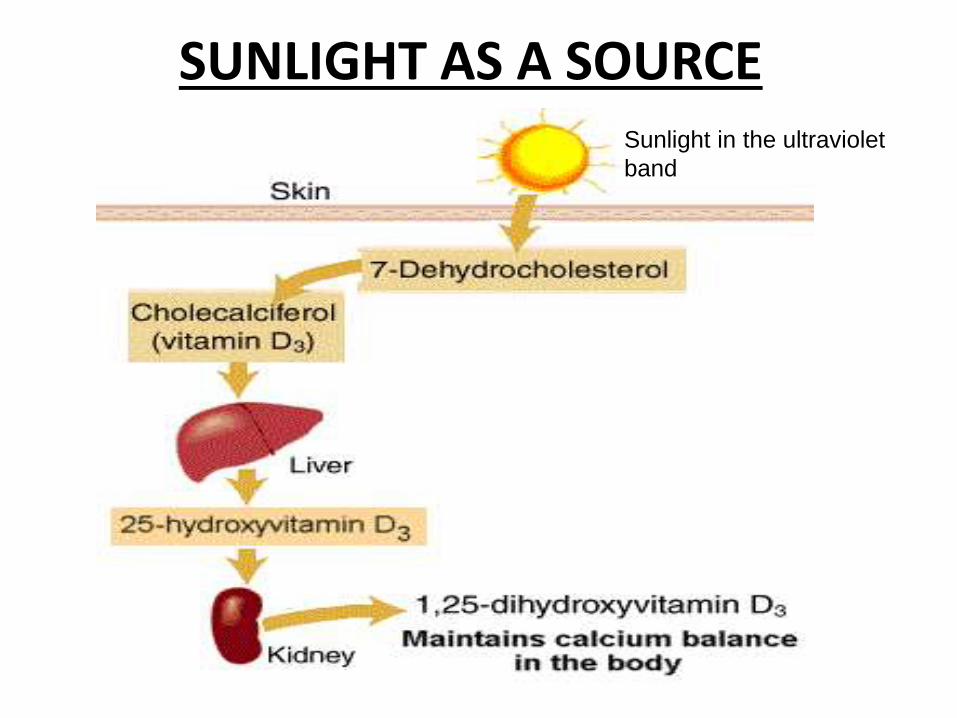
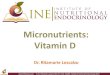
SUNLIGHT AS A SOURCESunlight in the ultraviolet
band
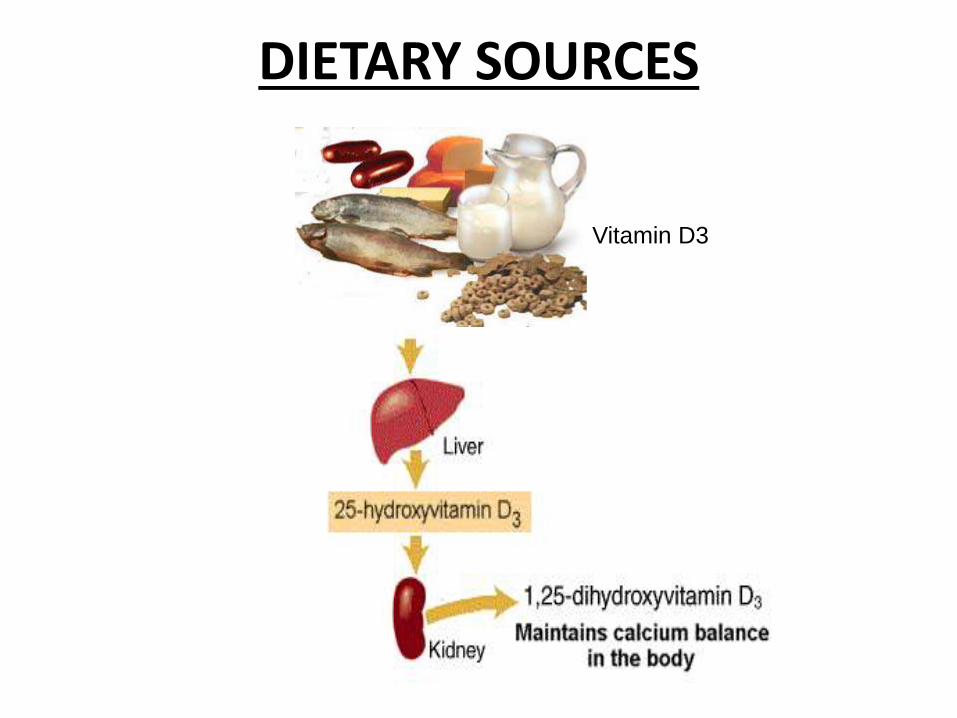
DIETARY SOURCES
Vitamin D3
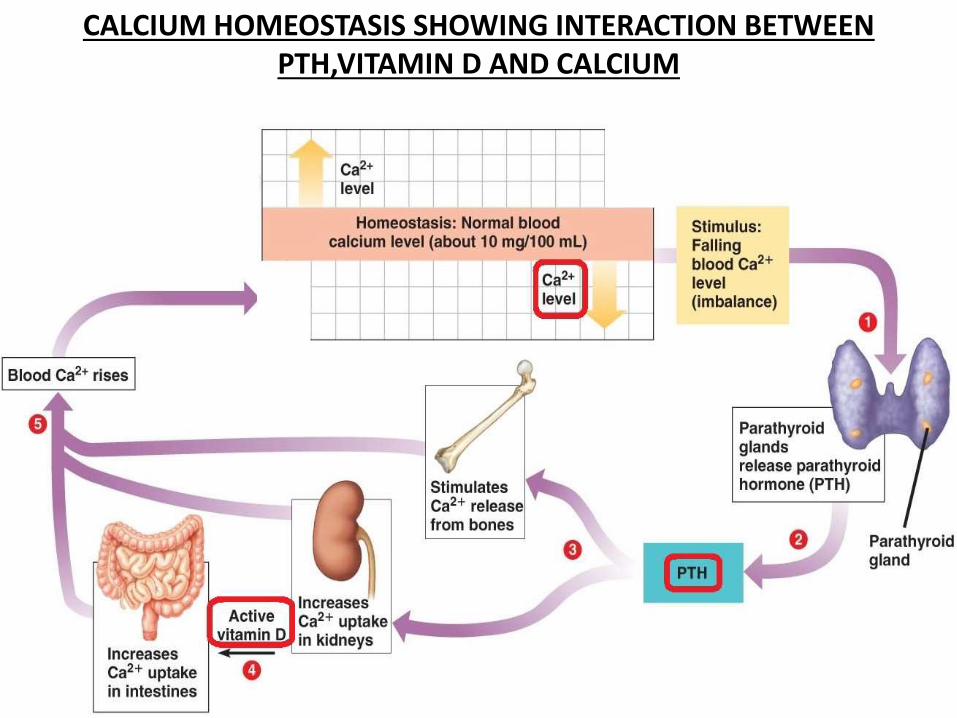
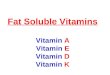
CALCIUM HOMEOSTASIS SHOWING INTERACTION BETWEEN PTH,VITAMIN D AND CALCIUM
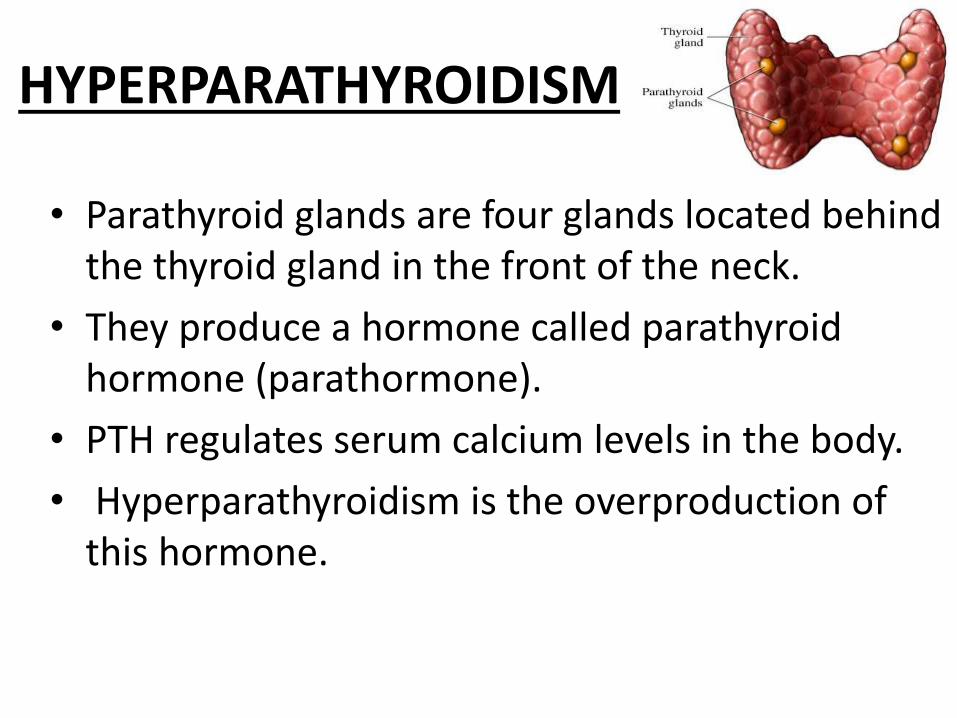
HYPERPARATHYROIDISM
• Parathyroid glands are four glands located behind the thyroid gland in the front of the neck.
• They produce a hormone called parathyroid hormone (parathormone).
• PTH regulates serum calcium levels in the body.
• Hyperparathyroidism is the overproduction of this hormone.
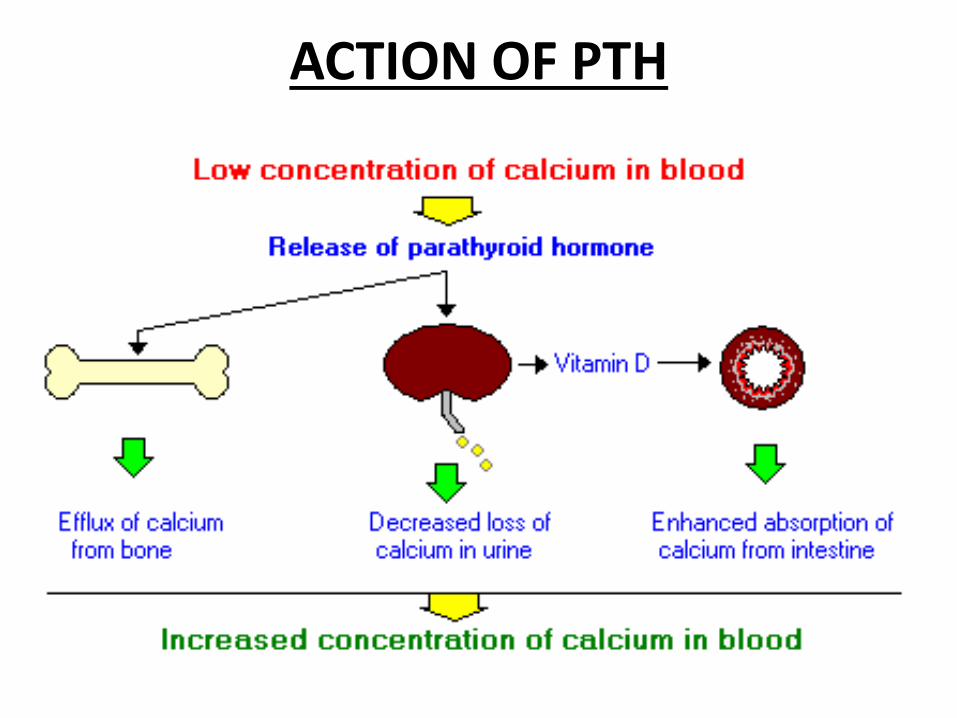
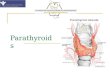
ACTION OF PTH
CLASSIFICATION OF HYPERPARATHYROIDISM
1. Primary
2. Secondary
3. Tertiary
PRIMARY HYPERPARATHYROIDISM
• Excess secretion of PTH from one or more parathyroid glands.
• Prevalence is 1 in 800,2-3times more common in women,average age being 55years.
• Is associated with familial MEN syndromes
-MEN I: Primary hyperparathyroidism+pituitarytumors+pancreatic tumors
-MEN IIa: Primary hyperparathyroidism+medullarycarcinoma of thyroid+pheochromocytoma
ETIOLOGY
-Single adenoma in 90%
-Nodular hyperplasia in 5%
-Multiple adenomas in 4%
-Carcinoma in 1% .
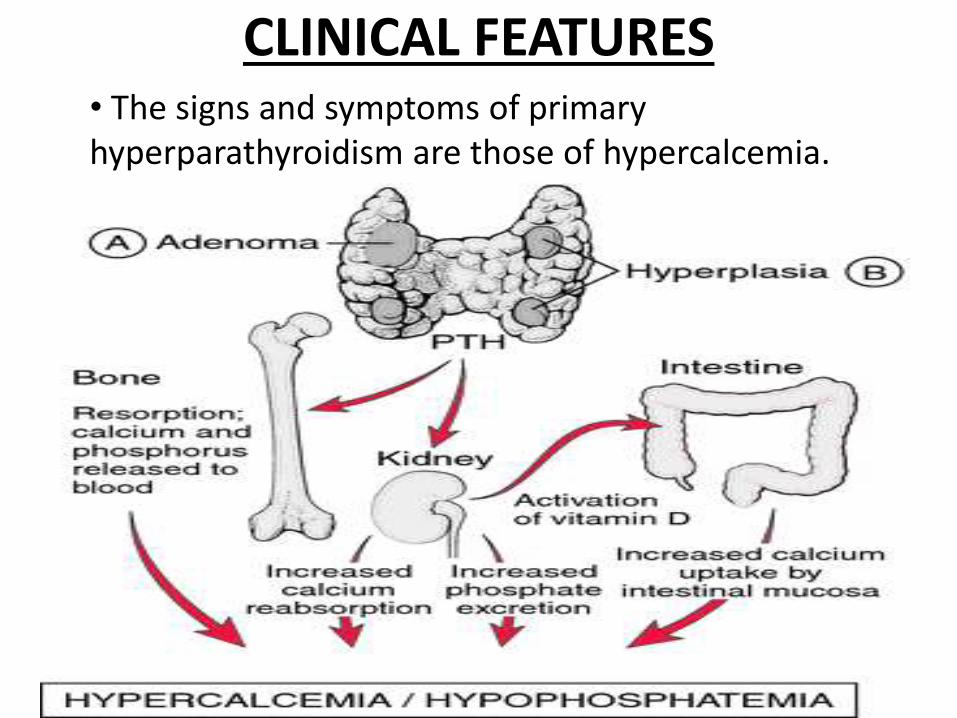
• The signs and symptoms of primary hyperparathyroidism are those of hypercalcemia.
CLINICAL FEATURES
- Patients present with kidney stones,nephrocalcinosis,diabetes insipidus(polyuria and polydipsia).These ultimately lead to renal failure.
- bone-related complications like osteitis fibrosa(bone pain and pathological fractures),osteoporosis,osteomalaciaand arthritis.
- gastrointestinal symptoms of constipation,anorexia,nausea,vomiting,pepticulcers,acute pancreatitis.
- cardiovascular system involvement leading to hypertension,bradycardia,shortened QT interval and left ventricular hypertrophy.
- central nervous system symptoms include lethargy,fatigue,depression,memory loss, psychosis,ataxia,delirium and coma.
- other signs include proximal muscle weakness,itching,band keratopathy of the eyes.
DIAGNOSIS
• Serum calcium levels are elevated.
• Parathyroid hormone level is abnormally high.
• There is hypophosphatemia and increase in 24-hour urinary calcium excretion.
• DEXA scan shows skeletal involvement.
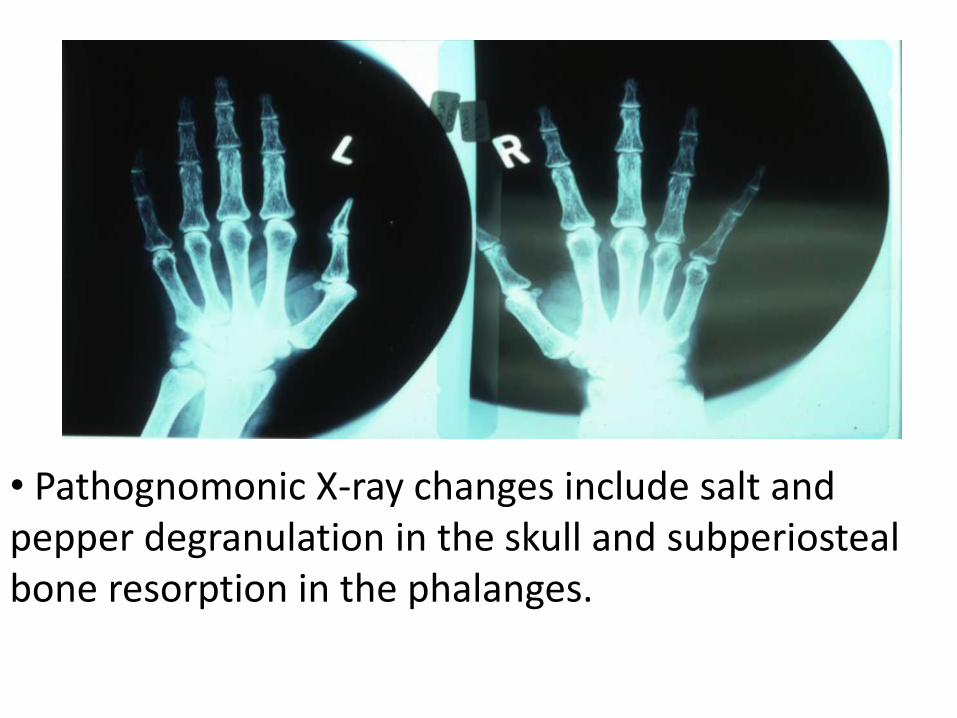
• Pathognomonic X-ray changes include salt and pepper degranulation in the skull and subperiostealbone resorption in the phalanges.
• Imaging of renal tract (X-ray, ultrasound) can demonstrate renal calculi.
• Localisation of parathyroid tumors by technetium scan,ultrasound,CT of the neck followed by FNAC.
TREATMENT 1. Management of acute hypercalcemia by
rehydration with normal saline,bisphosphonates,haemodialysis.
2. Medical line : -Monitor serum creatinine levels and calcium levels every 6 months.DEXA scan on an annual basis.
-Avoid thiazide diuretics.
-Maintain high oral fluid intake.
-Improving bone mineral density and achieving calcium homeostasis by calcimimetics and HRT.
3. Surgery : -Is indicated in patients with complications and in younger age group.
-Minimally invasive surgery to excise solitary adenoma,
Subtotal parathyroidectomy in case of diffuse hyperplasia are being done.
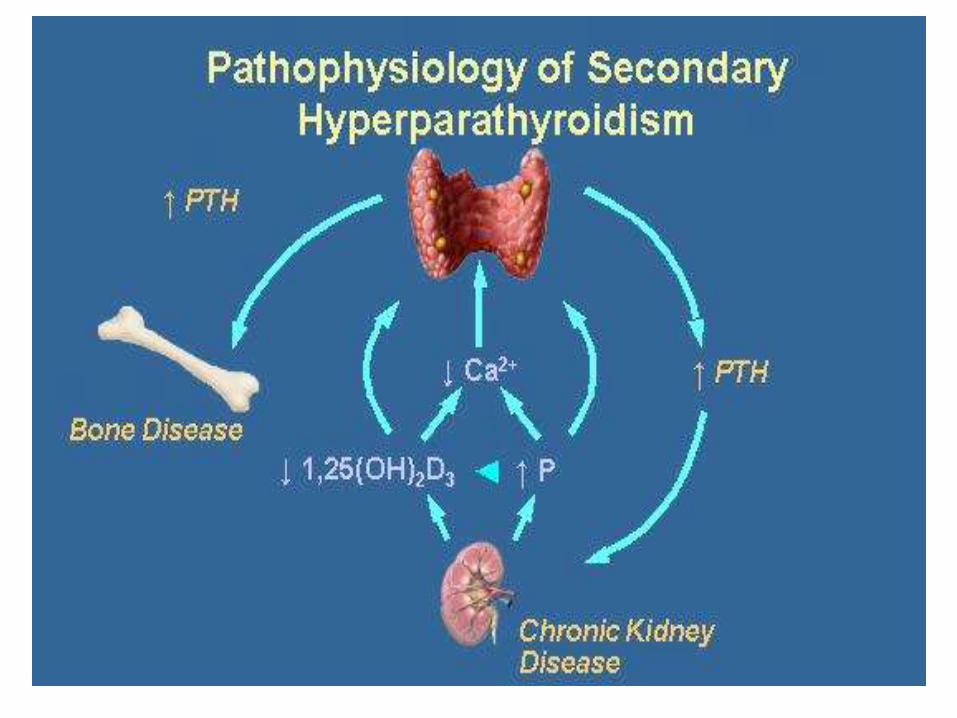
SECONDARY HYPERPARATHYROIDISM
• It occurs when PTH secretion is increased to compensate for prolonged hypocalcemia.
• It is seen in patients with chronic renal failure where the failing kidneys do not convert vitamin D to its active form and they do not excrete phosphate.
Excess phosphate combines with calcium to form calcium phosphate.
• Both processes lead to hypocalcemia,causehyperplasia of all parathyroid tissue and hence secondary hyperparathyroidism.
• Secondary hyperparathyroidism can also result from malabsorption of vitamin D due to chronic pancreatitis,small bowel disease,bariatric surgery.
• CLINICAL FEATURES : are mostly of renal failure.If it is due to vitamin D deficiency,limb deformities,pathologicalfractures occur.
• INVESTIGATIONS : Serum calcium levels are low.PTH levels are raised. Phosphate levels depend on etiology (e.g. high in renal disease, low in vitamin D deficiency).Radiology shows evidence of bone disease.
• TREATMENT : Medical line is the mainstay.The underlying condition needs to be treated-correcting vitamin D deficiency.-treatment of chronic kidney disease
(Calcium supplementation.Treatment with vitamin D and its analogues.Calcimimetics)
TERTIARY HYPERPARATHYROIDISM
• In a small proportion of cases of secondary hyperparathyroidism,continuous stimulation of the parathyroids results in adenoma formation and unregulated PTH secretion.
• Even correction of the underlying cause will not stop excess PTH secretion i.e parathyroid gland hypertrophy becomes irreversible.
• CLINICAL FEATURES : Symptoms and signs are due to hypercalcemia so presentation is similar to primary hyperparathyroidism.
• INVESTIGATIONS : Serum calcium and PTH levels are raised.
Phosphate levels are often high.
• TREATMENT : Total or subtotal parathyroidectomy is the recommended treatment.
Autotransplantation of parathyroid tissue in the forearm is also commonly carried out.
THANK YOU !!