Embed Size (px)
Citation preview

Worksite Obesity Research and
Recommendations
Charlotte A. Pratt, PhD
Program Director
National Heart, Lung, and Blood Institute,
National Institutes of Health
January 21, 2015
George Washington University
#GWICF2015

Financial or material support: None
The views expressed are my own and do not
necessarily represent the views of the National
Institutes of Health or the United States
Government.
Disclosures#GWICF2015

Overview of NIH funding for Worksite Obesity Research: 2007-2014
Important Research Questions in Worksite Obesity Control
Examples of Promising Active NIH-funded grants: Investigator-Initiated
Recommendations for Future Research
NIH Workshop Recommendations
Pathways to Prevention Workshop-NIOSH-CDC/NIH: upcoming late fall/early winter
Outline#GWICF2015

16%
15%
14%
12%
11%
11%
11%
10%
Number of grants
NHLBI NINR NIDA NIDDK NIAAA NCI NICHD NIEHS
Worksite obesity-related grants: 2007-2014
Total= 119, 2007-14
8 Institutes-- 61% of NIH worksite obesity -related grants;
16 Other Institutes: N= 46 or 39%
Search term: Worksite or workplace and obesity
#GWICF2015

#GWICF2015

Altering the worksite physical activity and nutrition environments, social, economic or organizational systems
Addresses obesity control from multiple fronts
Larger reach; may be more generalizable
Opportunity to enhance weight loss maintenance
Social support
Reduction of health care cost for the employer and employee--cost benefit; cost effective
Socially responsible employer
Worksite Overweight and Obesity Control #GWICF2015

Do interventions that modify the worksite food and physical activity environments (or combined with individual approaches) control body weight in adults?
Will participation in a worksite obesity intervention sustain and maintain weight loss, and reduce cardiovascular disease risk factors in adults?
Key Research Questions for Worksite
Obesity Research
#GWICF2015

Coordinating
Functions
Vic Stevens
Kaiser
Permanente
20 School
personnel
(ACTION!)
N=600 school
staff
6 Hospitals
(Step Ahead)
N= 806
30 Hotels
(3W: Work,
Weight and
Wellness
N=~12,000
30 Small-
mediums size
Businesses
(PACE)
N=3,000
4 Bus
Garages-transit
workers
Route H)
N=1,200
12 Dow
Chemical Co.
(Lighten Up)
N=6,000
12 Kodak Co
(Images of a
Healthy
Workplace)
N=4,000
To test environmental or combinations of environmental and individual interventions
Emory
Univ.
Univ. Mass
Tulane
Univ.
Univ. of
Rochester
Univ. of
MN
Univ. of
Washington
Univ. of Hawaii
Total N= 23,000 selected for measures
Worksite Obesity Trials– R01s (Research Projects Grants)
#GWICF2015

Citation Lemon et al. Am J Prev Med. 38(1):27-38; 2010
Research
question
Would a worksite environmental intervention prevent weight
gain among hospital employees?
Conceptual
Framework
Socio-ecological model of health behavior, social marketing
campaign, leadership support
Design 6 hospitals; 3 matched pairs; random assignment
Intervention Cafeteria menu and vending machine changes, portion
control, web-based counseling, walking groups, stairwell
changes, group-level behavioral programs
Outcomes PO: change in BMI at 12 and 24 months; SO: change in
organizational commitment
Overall take
home
message
Intervention had a dose-response relationship with
participation but overall, no BMI effect.
Overweight & Obesity Control at Worksites-
Hospitals#GWICF2015

Lemon et al. Am J Prev Med. 38(1):27-38; 2010
BMI effect related positively to participation.
Improved perceptions of organizational commitment to worker health
#GWICF2015

ROUTE H! Mean change in selected foods, physical activity
& perceptions of metro employees
Intervention Effect 95% CI
BMI effect -0.14 -0.84, 0.57
Fast foods (times/wk) -0.31** (-0.66, 0.04)
Kcal/day -407** (-778, -36)
Fruits and Vegetables
svg/day)
0.25* (0.01, 0.49)
MVPA (min/day) 2.7 (-5.2, 10.6)
TV viewing (h/day) -0.09 (-0.35, 0.18)
Information on health eating 18.6* (3, 34.2)
Easy to eat healthfully at
work
12.2* (0.2, 24.2)
French et al., Preventive Medicine, 50, 180-185, 2010
Adjusted for age, education, income, marital status, race, gender, smoking
Status; * p<.05, ** p<.10, 2 df
#GWICF2015

Citation Thorndike et al. Am J. Prev Med 2012; 43 (1) 27-33
Research
question
Will participation in a worksite obesity intervention sustain
and maintain weight loss, and reduce cardiovascular
disease risk factors in adults?
Design Be fit weight loss program; RCT; Teams Rdz into
maintenance intervention (Internet and personal contact);
and control arm
Intervention Goal setting, self monitoring via internet logging and
weekly counseling; personal contact and counseling with
nutritionist every 3 months
Outcomes Weight loss at 10 weeks ~4.2 lb in both groups;
maintenance- 3.4 lb vs. 2.5 lb (I vs.C). Improvement in BP,
TC, LDL-C, TG, Fasting blood glucose
Take home
message
Weight loss maintained in both groups; prevention of
usual increase in weight post intervention.
Overweight & Obesity Control at Worksites- Hospital
#GWICF2015

Weight maintenance after weight loss
Thorndike et al. Am J. Prev Med 2012; 43 (1) 27-33
Absolute weight loss % weight loss
Improvements in all CV risk factors at 10 weeks; TC & LDL-C effects maintained at 1 yr
-4.2 lb
#GWICF2015
Examples of Promising Active NIH-
Funded Grants
#GWICF2015
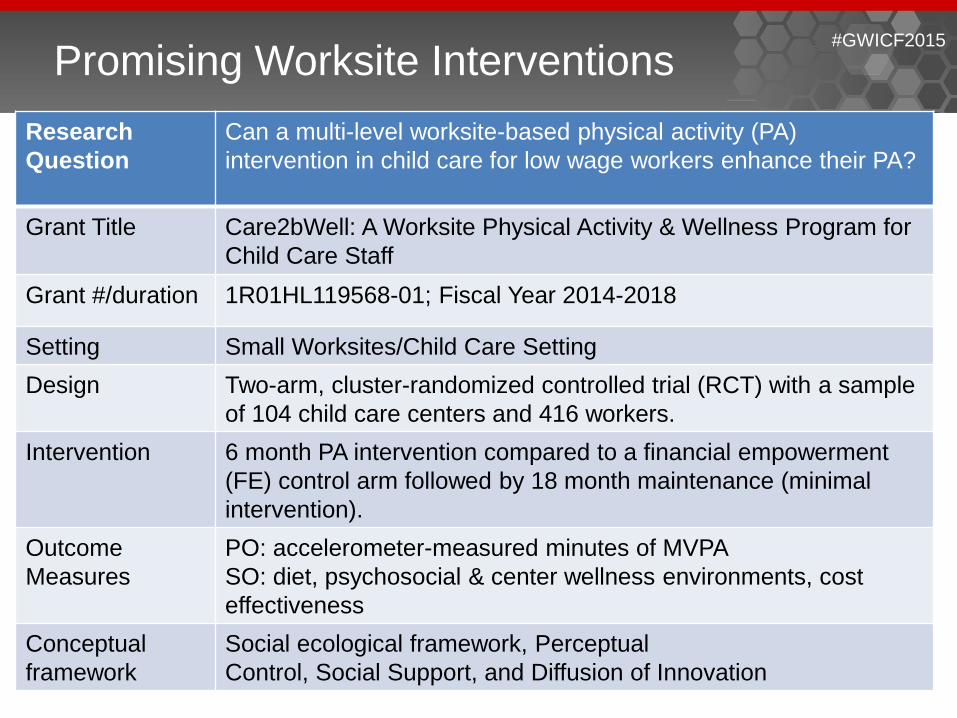
Research
Question
Can a multi-level worksite-based physical activity (PA)
intervention in child care for low wage workers enhance their PA?
Grant Title Care2bWell: A Worksite Physical Activity & Wellness Program for
Child Care Staff
Grant #/duration 1R01HL119568-01; Fiscal Year 2014-2018
Setting Small Worksites/Child Care Setting
Design Two-arm, cluster-randomized controlled trial (RCT) with a sample
of 104 child care centers and 416 workers.
Intervention 6 month PA intervention compared to a financial empowerment
(FE) control arm followed by 18 month maintenance (minimal
intervention).
Outcome
Measures
PO: accelerometer-measured minutes of MVPA
SO: diet, psychosocial & center wellness environments, cost
effectiveness
Conceptual
framework
Social ecological framework, Perceptual
Control, Social Support, and Diffusion of Innovation
Promising Worksite Interventions#GWICF2015

Research
Question
Will adaptations of a Chronic Disease Self-Management (CDSM)
Intervention Program improve chronic disease risk in adults?
Grant Title Putting CDSM Program to Work: Implementation of the Live Healthy,
Work Healthy Program
Grant # 5 R01 HL122330; Fiscal Year 2014-2018
Setting 7 organizations from a rural county in partnership with YMCA trained
staff
Design Two arm: adapted CDSM versus usual CDSM programs
Intervention 6 month followed by 12 month follow up.
Outcome
Measures
PO: Composite of BMI, diastolic and systolic blood pressure, blood
glucose, HDL, LDL, and Total cholesterol
SO: Diet, physical activity, patient-provider communication, quality of
life, medication adherence, work performance and productivity and
cost-effectiveness.
Conceptual
framework
Social Learning Theory
Promising Worksite Interventions#GWICF2015

Desk-Compatible Elliptical Device
R21 HL118453
Fits under desk for simultaneous physical activity and desk work; low cost $100,
space efficient. Participants expended 179.1 kcal/hr (range = 108.2–269.0)
Rovniak et al. J Sci Med Sport. 2014,17(4):376-80
#GWICF2015

Modest-to-minimal or no BMI effects:
demonstrated feasibility, low-cost interventions
could complement individual approaches for
weight management and potentially translate to
long-term gains if sustained.
Lessons: better job of addressing participation in
environmental interventions, consider lifestyle
beyond the worksite, influence of family, peer,
and upper-level administrative/leadership
support.
Summary#GWICF2015

Recommendations for Future
Research
#GWICF2015

NIH, CDC-NIOSH Workshop Report and Recommendations on Preventing Chronic
Disease At the Workplace. Sorensen et al. AJPH. 2011;101(S1):196-207
• Study the adoption of integrated
interventions: individual, work-
family- community factors ,and
work environment.
• Attend to population, job, and
worksite characteristics.
• Use appropriate study designs
and methods.
• Apply appropriate and expanded
measures and metrics.
• Study sustainability and
knowledge transfer from research
to practice.
• Address global concerns. Workshop conceptual model
http://www.nhlbi.nih.gov/resources/docs/index.htm. Workshop: May 21-22, 2009
#GWICF2015

Research that emphasizes combinations of
environmental and individual interventions,
(e.g., adaptation of the DASH diet) plus
outside of the work environment diet and
physical activity are needed.
Research targeting small businesses, minority
owned businesses and businesses in rural
communities by adapting proven modalities
from large businesses are needed.
Future Research Recommendations#GWICF2015

P2P Workshop focusing on worker health planned for late fall/winter 2015
Co-Sponsors NIH (NHLBI) and CDC (NIOSH) serve as content-area leads ODP serves as the programmatic and logistical lead
Goal Understand scientific evidence Develop recommendations for future research
Outcomes Panel report Systematic evidence report Post-workshop dissemination
#GWICF2015

Beresford SAA et al. Worksite study to promote activity and changes in
eating for obesity prevention: The PACE Project. Obesity, Supplement 1, 15,
4S-15S, 2007.
French SA, Harnack LJ, Hannan PJ, Mitchell NR, Gerlach AF, Toomey TL.
Worksite environment intervention to prevent obesity among metropolitan
transit workers. Preventive Medicine. 50: 180-185, 2010.
Pratt, CA, Lemon, SC, Fernandez, ID, Goetzel, RZ, Beresford, SA, French,
SA, Stevens, VJ, Vogt, TM & Webber, LS. Design Characteristics of
Worksite Environmental Interventions for Obesity Prevention, Obesity, 15
(9), 1-10, 2007.
Additional References#GWICF2015


To watch Dr. Charlotte Pratt’s presentation online, visit:
www.icfi.com/ObesityPreventionCharlottePratt
#GWICF2015