Embed Size (px)
DESCRIPTION
Citation preview
Erik Adler, MDFebruary 4, 2014

A 6 year old boy presents with a scalp laceration that requires suturing . His mother tells you that he is scared of needles and is liable to become
upset. Are there other options?
A patient presents to the Emergency Department with a laceration to the right forearm. He
sustained the injury while intoxicated last night. Upon waking, he noticed the wound and came to the ED. The injury was 14 hours ago. He requests
it be stitched closed.
A 28 year old man attends the emergency department with a simple laceration requiring suturing. You wonder whether application of a
topical antibiotic ointment may promote healing and reduce incidence of infection. You also
wonder if washing the wound with tap water is appropriate.
Create optimal conditions for healing. Preserve function. Minimize complications. Improve the chances of a cosmetically
pleasing result.
Secondary survey Mechanism of injury Elicit host factors that adversely affect wound
outcome ◦ Increased age◦ Diabetes◦ Peripheral Vascular Disease◦ Smokers◦ Wound width◦ Contamination or foreign body.
Tetanus immunization
Adequate setting/lighting Hemostasis Neurovascular exam Foreign body Radiography
5th cause of malpractice claims against emergency physicians
50% was glass Anver and baker 1992: 7% missing. 21% in
deeper wounds. In a medical/legal review, Kaiser et al:
unsuccessful defense in 60% of cases. When in doubt, do the X-ray!
Reactive materials, such as wood and vegetative material
Contaminated material Clothing (should always be considered
contaminated) Most foreign bodies in the foot Impingement on neurovascular structure
X-Ray
CT Scan/ MRI
US :sensitivity of 95-98% and a specificity of 89-98%
Anesthesia : Local anesthetic injections
Topical anesthetics
Regional anesthetics
Essential skill for all ED physicians Save time Decrease possibility of systemic toxicity Less painful than local infiltration Does not cause volume-related tissue
distortion
While data is convincing that local anesthetics with epinephrine do not cause long term damage to tissue with single blood supply (fingers, toes, nose, penis), it is still recommended that local anesthetic with epinephrine be avoided in these areas.
Epinephrine will cause vasoconstriction, which can be beneficial when requiring bloodless field
Small-bore needles Buffered solutions Warmed solutions Slow rates of injection Injection through wound edges Subcutaneous rather than intradermal
injection Pretreatment with topical anesthetics
LET (lidocaine, 4%; epinephrine, 0.1%; tetracaine, 0.5%)
Face and scalp
Liquid or gel forms
Lidocaine Marcaine (Bupivicaine)
◦ Drug concentration is expressed as a percentage (eg, bupivacaine 0.25%, lidocaine 1%).
◦ Percentage is measured in grams per 100 mL (ie, 1% is 1 g/100 mL [1000 mg/100 mL], or 10 mg per mL).
Toxic Doses-◦ Lidocaine without epinephrine- 4.5 mg/kg; not to
exceed 300 mg total dose◦ Lidocaine with epinephrine- 7 mg/kg◦ Bupivicaine without epinephrine- 2.5 mg/kg; not
to exceed 175 mg total dose◦ Bupivicaine with epinephrine- Not to exceed 225
mg total dose
While generally safe, local anesthetic agents can be toxic if administered inappropriately.
Central Nervous System, Cardiovascular System, Methemoglobinemia, Allergic Response.
Etiology-◦ Inadvertent intravascular administration◦ Excessive dose or rate of injection◦ Delayed drug clearance◦ Administration into vascular tissue
Ruthman et al : closure of lacerations without caps and masks did not lead to an increased incidence of wound infection
Worral and later Perelman: sterile versus nonsterile gloves found no difference in wound infection rates.
Non-sterile gloves, which provide “universal precaution “ is appropriate.
Latex gloves should also be avoided
Reduce quantity of bacteria on the surface of the skin
Shaving the hair does make closure easier Increased risk of wound infection by inducing
trauma Seropian and Reynolds : infection risk increased
from 0.6% to 5.6% when hair was shaved from a wound
The use of clippers .
Most important step Remove bacteria and contamination 15 psi removed 85% of bacterial contamination
from a wound, whereas (1 psi) removed only 49%
5 – 8 psi 30-60-cc syringe to push fluid through a 18-
gauge catheter with maximal hand pressure.
Minimum of 250 cc
60 cc/ cm wound length
Large volume with low pressure may be good.
Sterile saline solution Povidone-Iodine
Solution (Betadine®) 10%
- tissue toxic -did not reduce infection incidence. Diluted betadine : use
indeterminate.
Hydrogen peroxide no role, tissue toxic. Tap water : low cost, available. Sandy : Medline 1966-10/03, 397 papers found Tap water is a safe and effective solution for
cleaning recent wounds requiring closure and is the treatment of choice
Cochrane review database : -Although evidence is limited, there is no
difference in wound infection rates with the use of tap water as an irrigation fluid.

“Safe” time interval from wounding that allows primary wound closure
The ACEP clinical policy for penetrating
injury of the extremity supports an 8-12-hour cutoff for primary wound closure.
6-10 hours - wounds of the extremities —
and up to 10-12 hours or more for the face and scalp
Bites◦ Appropriate to close bites if on the face, but loose
approximation preferred to tight closure. ◦ All other bites should be left for delayed primary
closure or closure by secondary intent.◦ All bites deserve ABX (Augmentin is preferred)
Stab Wounds◦ Wound packing with wet to dry for 5 days
followed by delayed primary closure Infected tissue or significantly contaminated
tissue
The standard for wound closure
Percutaneous sutures are used for low- to medium-tension wounds
Absorbable suture material for dermal stitches Interrupted versus other types of sutures has no
effect on infection rate
Faster repair time Less painful Eliminate the risk for needle sticks Antibacterial effect Does not require removal of sutures
FDA approval in 1998 =Dermabond®
50% of the strength of 5-0 suture material.
Cochrane review : comparable cosmetic outcomes compared to standard suturing
Short (< 6-8 cm) Low tension (< 0.5 cm
gap) Clean edged Straight to curvilinear
wounds that do not cross joints or creases
Stellate lacerations Bites, punctures or crush
wounds Contaminated wounds Mucosal surfaces Axillae and perineum
(high-moisture areas) Hands, feet and joints
(unless kept dry and immobilized)
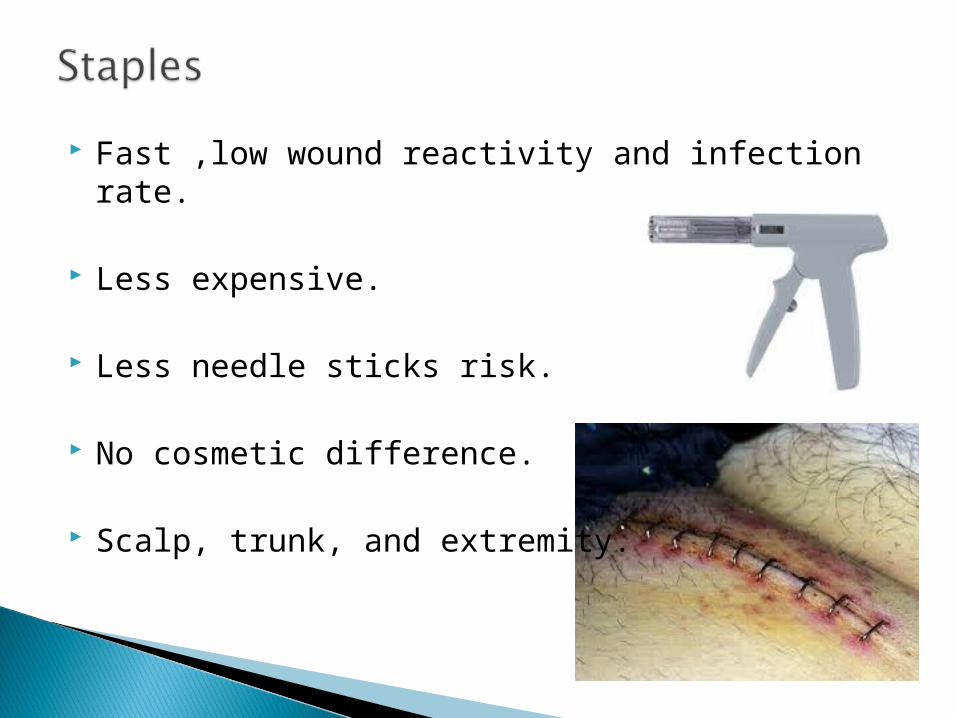
Fast ,low wound reactivity and infection rate.
Less expensive.
Less needle sticks risk.
No cosmetic difference.
Scalp, trunk, and extremity.
Least reactive of all closure techniques
Lowest tensile strength
May require tincture of benzoin
Avoid in hairy and wet area.
Simple, low-tension pediatric facial wounds, Steri-Strips™ resulted in a cosmetically equivalent wound closure compared to cyanoacrylate closure
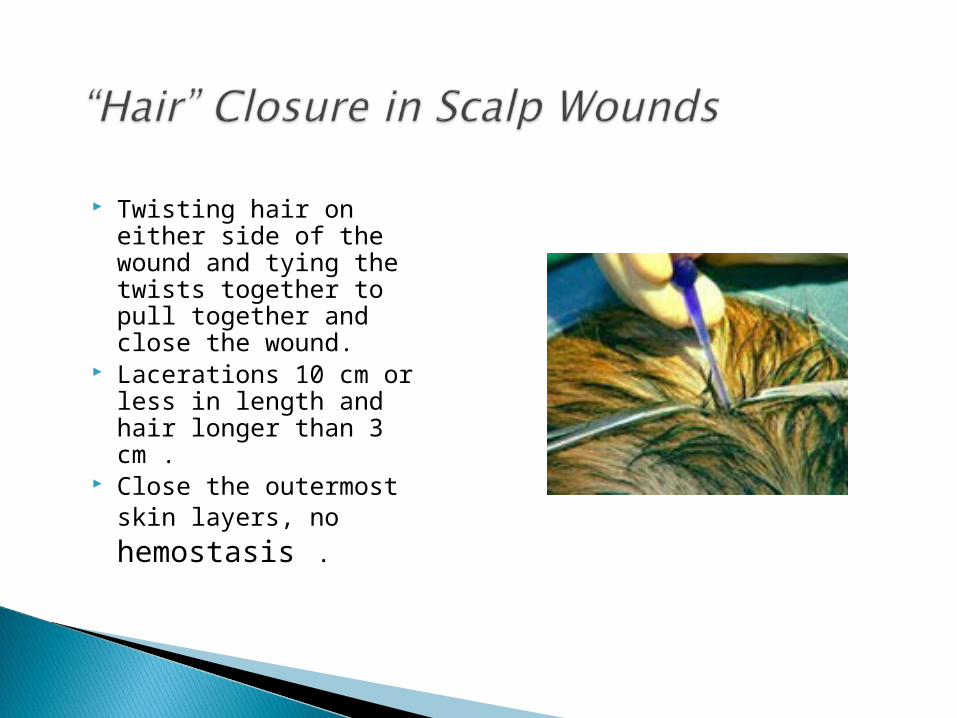
Twisting hair on either side of the wound and tying the twists together to pull together and close the wound.
Lacerations 10 cm or less in length and hair longer than 3 cm .
Close the outermost skin layers, no hemostasis .
Much underused method of wound care .
Reduced the infection rate by 50% in 104 extremity wounds
Recommended technique for contaminated wounds that present to the ED
Technique : clean and debride then separate
wound edges with gauze, and apply bulky dressing.
Allowing a wound to heal without formal closure .
Simple but more wound scaring.
Quinn et al in 2002 : conservative management resulted in no cosmetic or functional difference compared to primary closure in selected hand lacerations.
Prophylaxis studies : no benefits.
Indications For Prophylactic Antibiotics: -Presence of prosthetic device(s) Class III -Patients in need of endocarditis prophylaxis Class III -Open joint or fractures associated with wound Class I -Human, dog, and cat bites Class II -Intraoral lacerations Class II -Immunocompromised patients Class III -Heavily contaminated wounds (eg, feces, etc) Class III
Dire et al (1995), triple antibiotic ointment reduced the incidence of postclosure infection compared to a petroleum jelly control (4.5-5.5% for bacitracin and Neosporin® vs 17.6% for petroleum control).
Important to address patient allergies and avoid if allergic to Neomycin, Bacitracin, Polymyxin.
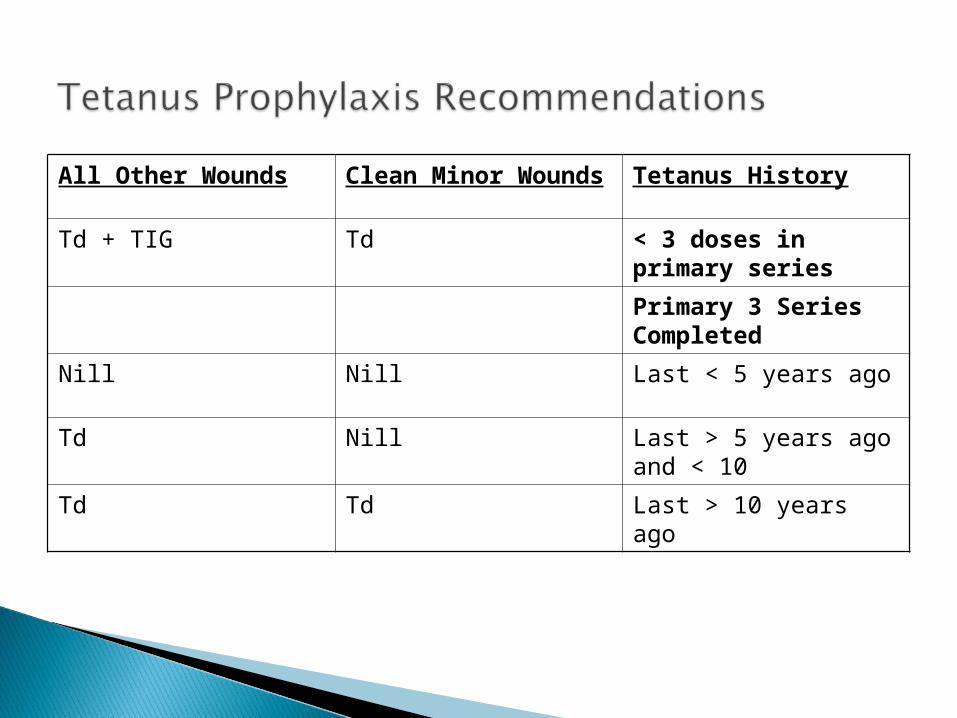
Tetanus HistoryClean Minor Wounds
All Other Wounds
< 3 doses in primary series
TdTd + TIG
Primary 3 Series CompletedLast < 5 years ago NillNill
Last > 5 years ago and < 10
NillTd
Last > 10 years ago TdTd
1. Staples and glue are the quickest closure methods.
2. Small, simple hand lacerations (< 2 cm) do not require primary closure.
3. Sterile gloves have no advantage over nonsterile gloves in reducing wound infection.
4. Clean tap water is as effective as (and cheaper than!) sterile saline for wound irrigation.
5. Cyanoacrylates or absorbable sutures are cost-effective for patients, as they do not require return visits.
6. Application of LET in triage allows a wound to be anesthetized by the time you see the patient.
High-pressure irrigation with normal saline or tap water.
Clean wounds presenting within 8 hours of occurrence can typically be closed primarily. This does not apply to wounds on the face or scalp
PE alone is inadequate for ruling out a foreign body in a wound.
Determine if it is appropriate to close a wound primarily
Prevention of a wound infection
Multitude of wound closure methods including “needleless” methods.