Embed Size (px)
DESCRIPTION
Citation preview

RG
H
F
*D
PfdqsttFinmmagmthfathfartwtratattt
Triad
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
GASTROENTEROLOGY 2009;137:1593–1608
EVIEWS IN BASIC AND CLINICALASTROENTEROLOGY
John P. Lynch and David C. Metz, Section Editors
epatitis B Virus Resistance to Nucleos(t)ide Analogues
ABIEN ZOULIM*,‡,§ and STEPHEN LOCARNINI�
‡ § �
INSERM, U871, Lyon; Université Lyon 1, Lyon; Hospices Civils de Lyon, Service d’hépatologie et de gastroentérologie, Lyon, France; and Victorian Infectiousiseases Reference Laboratory, North Melbourne, Victoria, Australiarcamrcaooeaorr
mctawumodtpcocHg
cv
atients with chronic hepatitis B (CHB) can be success-ully treated using nucleos(t)ide analogs (NA), butrug-resistant hepatitis B virus (HBV) mutants fre-uently arise, leading to treatment failure and progres-ion to liver disease. There has been much research intohe mechanisms of resistance to NA and selection ofhese mutants. Five NA have been approved by the USood and Drug Administration for treatment of CHB; it
s unlikely that any more NA will be developed in theear future, so it is important to better understandechanisms of cross-resistance (when a mutation thatediates resistance to one NA also confers resistance to
nother) and design more effective therapeutic strate-ies for these 5 agents. The genes that encode the poly-erase and envelope proteins of HBV overlap, so resis-
ance mutations in polymerase usually affect theepatitis B surface antigen; these alterations affect in-
ectivity, vaccine efficacy, pathogenesis of liver disease,nd transmission throughout the population. Associa-ions between HBV genotype and resistance phenotypeave allowed cross-resistance profiles to be determined
or many commonly detected mutants, so genotypingssays can be used to adapt therapy. Patients that expe-ience virologic breakthrough or partial response toheir primary therapy can often be successfully treatedith a second NA, if this drug is given at early stages of
hese events. However, best strategies for preventing NAesistance include first-line use of the most potentntivirals with a high barrier to resistance. It is impor-ant to continue basic research into HBV replicationnd pathogenic mechanisms to identify new therapeuticargets, develop novel antiviral agents, design combina-ion therapies that prevent drug resistance, and decreasehe incidence of complications of CHB.
he hepatitis B virus (HBV) is a DNA virus thatreplicates its genome via an RNA intermediate using
everse transcription1 (Supplementary Figure 1); chronicnfection with this virus can result in cirrhosis and hep-tocellular carcinoma.2 Effective treatments have been
eveloped for chronic hepatitis B (CHB), significantlyeducing morbidity and mortality. Therapeutic efficacyan be affected by factors such as the development ofdverse effects, poor patient compliance, previous treat-ent with suboptimal regimens, infection with drug-
esistant viral strains, and inadequate drug exposure be-ause of pharmacologic properties of particular drug(s)nd individual genetic variation. Interferon (conventionalr pegylated) and 5 other drugs that belong to the classf nucleos(t)ide analogues (NA) (lamivudine [LMV], ad-fovir dipivoxil [ADV], entecavir [ETV], telbivudine [LdT],nd tenofovir [TDF]) have been approved for treatmentf CHB in many parts of the world.2 The NA inhibiteverse transcription of the HBV polymerase, and this articleeviews the emergence of resistance to this class of agents.
Clinical Importance of ResistanceImpact on Disease SeverityThe development of drug resistance begins with
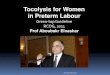
utations in the polymerase gene, followed by an in-rease in viral load, an increase in serum alanine amino-ransferase (ALT) levels several weeks to months later,nd progression of liver disease3–5 (Figure 1). In patientsith LMV resistance, the risk of increased serum ALT issually correlated with the duration of infection with theutant virus.6 These patients are also at significant risk
f ALT flare, which may be accompanied by hepaticecompensation.6 The emergence of LMV-resistant mu-ations is reflected in histologic assessment of liver sam-les.7 The detrimental effect of HBV drug resistance onlinical outcome was shown by a placebo-controlled trialf LMV in patients with advanced fibrosis.8 Patients suc-essfully treated with LMV who maintained wild-typeBV had a significantly lower risk of liver disease pro-
ression compared with those who received placebo, but
Abbreviations used in this paper: ADV, adefovir dipivoxil; CHB,hronic hepatitis B; ETV, entecavir; HBV, hepatitis B virus; LdT, telbi-udine; LMV, lamivudine; NA, nucleos(t)ide analogs; TDF, tenofovir.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2009.08.063

tr
tsrn
sAt
oruifpctct
ctatrsLhai
rHHtAphatt
FvicslmgAiosobbmavtcmrt
T
LTTAA
TEE
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1594 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
his effect was lost in patients who developed LMV-esistant mutant forms of the virus.8
The kinetics of emergence of resistance to ADV areypically slower than those of LMV but follow the sameequence of events: polymerase variants with the specificesistance mutations can be detected initially, which is
igure 1. Kinetics of drug resistance emergence. Panel A: Evolution ofiral load and ALT levels. After an initial drop in viral load following thenitiation of antiviral therapy, virologic breakthrough may occur as aonsequence of antiviral drug resistance. It corresponds to the rise inerum HBV DNA levels of at least 1-log10 IU/mL compared with the
owest value during therapy (nadir value), in 2 consecutive samples 1onth apart, in patients who have previously responded and have aood treatment compliance. It may be followed by an elevation in serumLT levels in patients who previously showed transaminases normal-
zation under treatment. It may result in hepatitis flares and in worseningf liver histology. Panel B: Evolution of the viral quasispecies with re-pect to primary and secondary resistance mutations. At the beginningf therapy, wild-type virus is the major strain circulating in the patient’slood, whereas viral genomes harboring polymorphic mutations maye detected. Because of the spontaneous error rate of the viral poly-erase, primary resistance mutations are usually present at levels that
re undetectable by conventional diagnostic techniques. At the time ofirologic breakthrough, viral genomes harboring primary resistance mu-ations start to emerge and become the dominant viral strains. Theontinuation of viral replication under the selective pressure of the drugay lead to the accumulation of additional mutations that increase the
esistant mutant replication capacity (ie, secondary resistance muta-ions).
ext followed by virologic breakthrough and then rising
erum levels of ALT.9 In some cases, the emergence ofDV resistance was also associated with acute exacerba-
ion of disease and liver failure.10
Only limited data are available on the clinical outcomef patients who are infected with LdT-, ETV-, or TDF-esistant HBV, mainly because treatment adaptation,sually based on in vitro cross-resistance data, has been
nitiated during early stages of resistance, or treatmentailure. Thus, the availability of antiviral drugs with com-lementary cross-resistance profiles (see below) hashanged the management of patients with drug resis-ance, allowing physicians to prevent the worsening oflinical outcome resulting from the emergence of resis-ance.
Incidence and Prevalence of ResistanceLMV resistance increases progressively over the
ourse of treatment; 14%–32% of patients become resis-ant to the drug each year after treatment was initiated,nd more than 80% are resistant after 48 months ofreatment5 (Table 1). The rate of emergence of LdT-esistant HBV is lower than that of LMV but is stillubstantial. In a phase III trial that compared LdT withMV, genotypic resistance occurred in 4.4% and 21% ofepatitis B e antigen (HBeAg)-positive patients after 1nd 2 years of treatment, respectively, and 2.7% and 8.6%n HBeAg-negative patients, respectively11,12 (Table 1).
The rate of selection for ADV-resistant virus is lower;esistance occurs in approximately 2% of patients withBeAg-negative CHB after 2 years of therapy (Table 1).owever, following 4 –5 years of ADV monotherapy, up
o 30% of patients are found to be resistant.9,13 WhenDV has been used in patients who are resistant to LMV,rimary ADV resistance as detected by genotype analysisas been found in up to 20% of patients by 12 monthsfter ADV therapy began.14 Recent trials of TDF reportedhat no resistance had developed by weeks 4815 and 96 ofreatment, although at week 72, the majority of viremic
able 1. Cumulative Annual Incidence of Resistance forLamivudine, Telbivudine, Adefovir, Tenofovir, andEntecavir
Drug and patientpopulation
Resistance at year of therapy expressed aspercentage of patients
1st
(y)2nd
(y)3rd
(y)4th
(y)5th
(y)6th
(y)
amivudine 23 46 55 71 80 —elbivudine HBeAg-Pos 4.4 21 — — — —elbivudine HBeAg-Neg 2.7 8.6 — — — —defovirHBeAg-Neg 0 3 6 18 29 —defovir (LAM-resistant)
Up to 20% — — — — —
enfovir 0 0 — — — —ntecavir (naïve) 0.2 0.5 1.2 1.2 1.2 1.2ntecavir (LAM 6 15 36 46 51 57
resistant)
pa
ryapga6
ctDchFwiiraamct
teii
phthpndChpqcsh
ddvtatfitt
FldmltagcmcspsaEstipwoldsf
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1595
atients was given a combination of TDF and emtricit-bine (Truvada; Gilead Sciences, Inc, Foster City, CA).16
Very low rates of genotypic resistance to ETV have beeneported in treatment-naïve patients after 1 year (0.1%), 2ears (0.4%), 3 years (1.2%), 4 years (1.2%), 5 years (1.2%),nd 6 years (1.2%) of therapy17,18 (Table 1). In contrast, inatients previously treated with LMV, the cumulativeenotypic resistance rates are 6% (year 1), 14% (year 2),nd 32% (year 3) (Table 1), steadily increasing to almost0% by year 6.17,18
Principles of Resistance andCross-resistanceA major determinant in the slow kinetics of HBV
learance from infected cells is the presence of a replica-ive form of the viral DNA termed covalently closed circularNA (cccDNA)19,20 (Supplementary Figure 1). During
hronic HBV infection, cccDNA is maintained in theepatocyte nuclei with a long half-life in infected cells.21
urthermore, it has been shown that antiviral therapyith NA cannot prevent the initial formation of cccDNA,
ndicating that persistent viremia during therapy leads tonfection of new cells.22,23 The HBV cccDNA acts as aeservoir for the reactivation of viral genome replicationnd is responsible for viral relapse after withdrawal ofntiviral therapy or those patients with CHB with im-une suppression. It has also been shown in the wood-
huck model of hepadnavirus infection that drug resis-ance mutations are archived in cccDNA and may
igure 2. Mechanisms of se-ection and emergence of HBVrug-resistant mutants. Theain factors involved in the se-
ection of escape mutants are: (i)he long half-life of hepatocytesnd viral cccDNA; (ii) the HBVenome variability leading to aomplex viral quasispecies andutant archiving in cccDNA. The
omposition of the viral quasi-pecies evolves over time de-ending on the selective pres-ure including antiviral therapynd the host immune response.scape mutants may thenpread in the liver and becomehe dominant species depend-ng on their fitness (ie, their ca-acity to replicate and dominateild-type strain in the presencef antiviral pressure) and the rep-
ication space available for theirissemination in the liver. Theirelection results in treatment
ailure.herefore be selected rapidly out when using drugs thatxhibit cross-resistance.24 Thus, the stability and replen-shment of cccDNA is the stumbling block for eradicat-ng CHB infection with current antiviral agents.25–28
A combination of host and viral factors determine viralersistence and also NA resistance. Infected hepatocytesave a long half-life, contributing to HBV persistence inhe liver.29 –32 Mathematical modeling showed that thealf-life of hepatocytes varies from 30 to 100 days, de-ending on individuals’ immune response.33,34 HBV ge-ome variability during the chronic phase of the diseaseetermines the selection for viral resistant strains.20,35,36
lonal and pyrosequencing analysis of HBV genomesave shown that single mutants exist in the overall viralopulation of HBVs even before therapy begins. Viraluasispecies within the same patient evolve during theourse of infection: different variants or mutants areelected at different stages of infection in response to theost immune response or antiviral therapy (Figure 2).Different mechanisms are involved in the selection of
rug-resistant mutants during antiviral therapy.20,35 Asescribed above, a complex mixture of genetically distinctariants have a replicative advantage in the presence ofhe selective pressure of NA therapy. A newly acquired or
preexisting mutation conferring a selective advantageo a variant will generate progeny virus, which is moret and can spread more rapidly in the liver, allowinghe corresponding mutant to accumulate and becomehe dominant species in the liver in the presence of the

alidsncratisenlbcrtfi
tipmhbobt
mmwdnpltsaogcmtata
wrpLaa
t(dt
FtaiLo
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1596 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
ntiviral drug.37– 40 The replacement of wild-type virus iniver cells by a dominant mutant is a slow process; studiesn animal models indicate that resistant mutants pre-ominately infect uninfected cells (ie, replication space),o the spread of the dominant mutant depends on theumber of uninfected cells in which HBV can repli-ate.24,41 It might take months for the immune system toemove hepatocytes that are infected with wild-type HBVnd for new hepatocytes to develop that are susceptibleo infection by viral drug-resistant mutant HBV. Thenfectivity of the drug-resistant mutants can impact thepeed of their selection; mutations in the genes thatncode overlapping surface antigens can affect viral fit-ess and infectivity,42 virion release (because of intracel-
ular retention of newly synthesized virus),43 virologicreakthrough (with slower kinetics of viral load in-rease),43 and vaccine prophylaxis.44 Finally, the level ofesistance to a drug, usually conferred by specific muta-ion in the viral polymerase, not surprisingly affects thetness of the mutant.Antiviral drug resistance results from adaptive muta-
ions in the viral genome.45 HBV infection is character-zed by very high levels of virus production and turnover,roducing more than 1011 virions per day.46 Further-ore, the viral population in an infected person is highly
eterogeneous.47 The high rate of HBV replication, com-ined with the high mutation rate (1 in every 105 nucle-tide substitutions during each cycle of replication,ecause of the error-prone nature of reverse transcrip-ion48), results in patients with CHB having a diverse
igure 3. Primary antiviral drug resistance mutations. Polymerase gene mo lamivudine (LMV) and telbivudine (LdT) is conferred by mutations in the Yssociated with compensatory mutations in the B domain restoring a highe
s conferred by a rtA181V or rtA181T substitution or a rtN236T substitution.dT. Resistance to entecavir (ETV) is conferred by a combination of mutatio
f substitutions at position rt204. Resistance to tenofovir (TDF) may be conferredixture of viral quasispecies, each differing in 1 or moreutations.49 The probability that a mutation associatedith drug resistance is selected for during therapy alsoepends on the potency of that drug.50 Replication fit-ess (defined as the ability to replicate under selectionressure45) and the replication capacity of resistant iso-
ates can shape the pattern of primary vs secondary mu-ations that emerge.51 The availability of replicationpace for HBV also determines resistance; the liver canccommodate new transcriptional templates of cccDNAnly if uninfected cells are generated by normal liverrowth or hepatocyte proliferation or by direct loss ofccDNA.52 The genetic barrier to resistance of the treat-ent regimen increases as the number of specific muta-
ions required for drug resistance increases.53 Finally,ntiviral drug resistance is also affected by host charac-eristics of virus-infected hepatocytes, immune response,nd genetic background.
Cross-resistance is defined as resistance to drug(s) tohich a virus has never been exposed. From a cross-
esistance perspective, the 5 approved NA have beenlaced, based on structural characteristics, into 3 groups:-nucleosides (LMV and LdT), alkyl phosphonates (ADVnd TDF), and D-cyclopentane group (ETV). Resistancend cross-resistance tend to be structure specific.
Two types of mutations have been associated withreatment failure to NA: primary resistance mutationsFigure 3 and Table 2), which are directly responsible forrug resistance, and secondary (compensatory) muta-ions, which promote or enhance replication compe-
ns conferring resistance to nucleos(t)ide analogs are depicted. Resistancemotif within the C domain of the polymerase, ie, rtM204V or rtM204I, oftenication capacity, ie, rtL180M and/or rtV173L. Resistance to adefovir (ADV)tA181V/T substitution can also confer decreased susceptibility to LMV andthe B, C, or D domain of the viral polymerase, in addition to a background
utatioMDDr replThe rns in
by amino acid substitution at position rt194, which needs to be confirmed.

tspctbttmtfsmTEptdrrrCudctcimua
mcawamtoi
fass
tmCClsr
tdrsraFtt1rosdrrrq
mmtcv
T
LLASDD
I
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1597
ence.53 Compensatory mutations emerge because theelection of resistance-associated changes in the viralolymerase is usually associated with some cost in repli-ation fitness for the virus; these compensatory muta-ions are important in the context of antiviral resistanceecause they “fix” the discriminatory primary drug-resis-ant mutations into the genetic archive of viral cccDNA,he HBV minichromosome, thus providing “quasispecies
emory.”49 The common mutations that confer resis-ance to LMV and LdT (eg, rtM204V/I � rtL180M) con-er cross-resistance to other L-nucleosides and reduceensitivity to ETV but not to ADV or TDF. Conversely,
utants that are resistant to ADV (eg, rtN236T) andDF generally remain sensitive to L-nucleosides andTV. Both the L-nucleosides (LMV and LdT) and alkylhosphonates (ADV and TDF) also select for the muta-ion rtA181T/V, thereby making it a marker for multi-rug resistance. Multiple mutations (eg, rtA184A/A/I/L,tS202G/L, rtM250I/V) in addition to those that conferesistance to LMV and LdT (rtM204V/I � rtL180M) areequired for high-level resistance to ETV (see Table 2).ross-resistance across NA groups (eg, rtA181T) (see Fig-re 3 and Table 2) might eventually be overcome byevelopment of drugs that block stages of the viral lifeycle distinct from those inhibited by NA (Supplemen-ary Figure 1). However, such drugs are unlikely to be-ome available for clinical use in the near future. Thus, its important to understand more fully the molecular
echanisms of NA resistance because, to optimize theirse, we must develop methods for defining, detecting,nd quantifying drug resistance and cross-resistance.
Factors That Predispose to ResistanceThere are several major risk factors for develop-
ent of resistance to NA, especially to LMV. These in-lude a high level of HBV DNA, high serum levels of ALT,nd high body mass index.3,5,54 Prior therapy with NA, asell as inadequate viral suppression during therapy, haslso been shown to predict drug resistance.3,4,9,11 Trans-ission of drug-resistant mutants in newly infected pa-
ients is also likely to predispose to more rapid resistancence treatment is initiated, as it was shown for HIV
able 2. Cross-resistance Data for the Main Drug-Resistant M
Pathway Amino acid substitutions in the rt domain
Wild-type-nucleoside M204I-nucleoside L180M�M204Vlkyl phosphonate N236Thared A181T/V-Cyclopentane (ETV) L180M�M204V/I�I169T�V173L�M250V-Cyclopentane (ETV) L180M�M204V/I�T184G�S202I/G
, intermediate; R, resistant; S, sensitive.
nfection. a
Pathways of ResistanceThe molecular mechanisms of resistance to drugs
or CHB have been recently reviewed in this Journal,55
nd resistance tends to be NA structure (sugar residue)pecific, providing a structural framework for resistanceelection.
L-Nucleoside-Associated ResistanceResistance to LMV and LdT has been mapped to
he YMDD locus in the catalytic (C domain) of HBV Pol,56
ediated primarily by the mutations rtM204I/V (domain) � rtL180M (domain B) and rtA181T/V57 (Figure 3).ompensatory mutations that increase viral replication
evels can be found in other domains of the HBV Pol,uch as rtL80V/I,58 rtI169T,59 rtV173L,60 rtT184S/G,tS202I, and rtQ215S.61
The mutations rtM204V/I do not confer cross-resis-ance to ADV or TDF (Table 2), whereas rtA181T/Voes.61,62 The mutations rtI169T, rtT184S/G, andtS202I/G contribute to ETV resistance but do not conferignificant resistance on their own59,63; rtM204V/I andtA181T are cross resistant with all other L-nucleosidenalogues tested including LdT (USA product insert;DA, Washington, DC) (Table 2 and Figure 3). Muta-ions that confer LMV resistance decrease in vitro sensi-ivity of hepatocytes to the drug by 100- to more than000-fold. rtM204I has been detected in isolation, buttM204V and rtM204S are found only in association withther changes in the A or B domains.64 The pattern of polequence in which resistance mutations are usuallyetected include the following: (1) rtM204I, (2)
tL180M�rtM204V, (3) rtL180M�rtM204I, (4) rtV173L�tL180M�rtM204V, and (5) rtL80V/I � rtL180M�tM204I; the dominance of a particular mutation se-uence is associated with HBV genotype.3,65
Alkyl Phosphonate-Associated ResistanceResistance to ADV was initially associated with
utations in the B (rtA181T/V) and D (rtN236T) do-ains of the enzyme62,66,67 (Figure 3). These substitu-
ions result in only a modest (3- to 8-fold) increase in theoncentration of the drug required for 50% inhibition foriral replication in vitro (effective concentration [EC50])
nts and the Approved Antivirals
Lamivudine Telbivudine Entecavir Adefovir Tenofovir
S S S S SR R I S SR R I S SS S S R II/R R S R IR R R S SR R R S S
uta
nd are partially cross resistant with TDF (Table 2) al-

mtatccmptpmct
hntsHrttrrsice
ed(PmrwmtrE
a1tppasn(I
tmaict
fwsEhanfMdetheaMmgwac
ssoAtmtttsra
mtaoHr
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1598 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
ost certainly because of their similar chemical struc-ures.61 The mutation rtN236T does not significantlyffect sensitivity to LMV, LdT, or ETV66,67 but decreaseshe efficacy of TDF in vitro.68 rtA181T/V confer de-reased susceptibility to ADV and TDF and are partiallyross resistant to LMV62 and LdT (Table 2). Anotherutation (rtI233V) has been recently identified that ap-
eared to confer resistance to ADV.69 In clinical studies,he rtI233V mutation occurred in approximately 2% of allatients with CHB,69 but the final significance of thisutation does require independent confirmation be-
ause other groups have not found an association be-ween rtI233V and ADV resistance.70 –72
Tenofovir was originally approved for the treatment ofuman immunodeficiency virus (HIV)-acquired immu-odeficiency syndrome (AIDS) and has also been used toreat patients with HIV-HBV coinfection. Genotypic re-istance to TDF has been detected in several patients withIV-HBV coinfection; the substitution rtA194T (plus
tL180M�rtM204V) has been associated with TDF resis-ance73; however, a recent report failed to confirm this74;herefore, further studies are needed. The detection oftA181T/V and rtN236T in patients failing ADV therapyesulted in reduced antiviral efficacy when patients werewitched to TDF. Van Bommel et al75 demonstrated anntensification and consolidation of these ADV-resistantlones following this switch and also reduced antiviralfficacy of TDF.
D-Cyclopentane-Associated ResistanceMutations in HBV polymerase associated with the
mergence of ETV resistance have been mapped to the Bomain (rtI169T, rtL180M, and/or rtS184G), C domain
rtS202I and rtM204V), and E domain (rtM250V) of HBVol (Figure 3). In the absence of the LMV-resistanceutations rtL180M and rtM204V/I, the mutation
tM250V increases the median EC50 of ETV by 10-fold,hereas the rtI169T, rtT184G, or rtS202I have only aodest effect on IC50 values.59,61,76 –79 Three other mu-
ations in HBV Pol (rtL180M�rtM204V and eithertT184G/S or rtS202I/G or rtM250V) are required forTV resistance to develop (Figure 3).
Mutational Pathways and Cross-resistanceEight codons in HBV polymerase are thus associ-
ted with primary drug resistance to NA: 169, 180, 181,84, 202, 204, 236, 250. These 8 codons have been showno be involved in HBV antiviral drug resistance via 4athways of viral evolution80 (Table 2). (1) the rtM204V/Iathway for L-nucleosides; (2) the rtN236T pathway forlkyl phosphonates; (3) the rtA181T/V pathway, which ishared between the L-nucleosides and alkyl phospho-ates; and (4) the D-cyclopentante/entecavir pathway
rtL180M�rtM204V�I169T�T184S/G/C�S202C/G/
�M250I/V). wThe first 3 pathways are associated with only 1 muta-ion, whereas the fourth pathway requires at least 3
utations for resistance. This “pathways of evolutionpproach” facilitates understanding HBV evolution dur-ng NA therapy and can be used to predict patient out-omes and improve our understanding of cross-resis-ance patterns and profiles.80
Multidrug ResistanceSequential monotherapy can promote selection
or multidrug-resistant (MDR) strains of HBV, especiallyhen patients are sequentially treated with drugs with
imilar characteristics, such as with LMV followed byTV63,81 or LMV followed by ADV.37,68 Clonal analysesave shown that MDR usually occurs via the sequentialddition of resistance mutations to the same viral ge-ome; mutants that arise from this selection process have
ull resistance to both drugs. Studies have shown thatDR strains arise if an “add-on” therapeutic strategy
oes not result in rapid and complete viral suppression,specially if there is a large replication space available forhe mutants to spread (ie, necroinflammatory activity origh levels of serum ALT, resulting in hepatocyte prolif-ration or need for a liver graft). A longitudinal clonalnd phenotypic analysis of variants in a patient with aDR strain of HBV after liver transplantation revealedutations in the overlapping polymerase and surface
enes that conferred resistance to both LMV and ADV asell as a decreased recognition of the virus by anti-HBsntibodies.37 These findings emphasize the need to achieveomplete viral suppression during antiviral therapy.
Some specific single mutations confer MDR. This washown with the rtA181V/T substitution, which is respon-ible not only for decreased susceptibility to the L-nucle-sides LMV and LdT but also to the alkyl phosphonatesDV and TDF.43,62 This emphasizes the need for geno-
ypic testing in patients with treatment failure to deter-ine the resistance mutation profile and tailor therapy to
he major viral strain circulating in the patient. Studies ofhe antiretroviral agents used to treat HIV have shownhat drug resistance testing can be used to monitor re-ponse to therapy and aide in the selection of new drugegimens for patients who have failed to respond tontiviral therapy.82
Detection and Monitoring of ResistanceViral Load AssaysMeasurement of viral load is indispensable for
onitoring and confirming the presence of drug-resis-ant virus because nearly all instances of resistance to NAre initially identified by a sustained rise in viral load thatccurs despite continuing antiviral therapy. The sensitiveBV DNA assays that are currently in use will detect
ising viral loads because of drug-resistant virus even
hen the emergence of the drug-resistant HBV popula-
t(cadc
cpbHpats
bpipi�ocatrsTpsbtHc
rmtdstCtstrmrci
mi
(
(
(
mripsa1divntst
ftidtveet
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1599
ion is slow. Because factors other than drug resistancefor example, poor patient compliance and/or pharma-ogenomic factors) can affect viral load, it cannot beutomatically assumed that rising loads are indicative ofrug resistance because drug-resistant HBV can only beonfirmed by genotyping and/or phenotyping.
GenotypingTo identify potential genotypic resistance, the nu-
leotide and deduced amino acid sequence of the HBVolymerase isolated from the patient during virologicreakthrough should be compared with the sequence ofBV isolated from a pretherapy sample from the sameatient.83 When pretherapy samples are not available fornalysis, sequence data at the time of virologic break-hrough should be compared with consensus publishedequences(s) of the same HBV genotype.72
Genotyping relies on either DNA sequencing or hy-ridization. Sequencing-based methods include standardopulation-based polymerase chain reaction (PCR), clon-
ng of PCR products, and restriction fragment-lengtholymorphism analyses. Direct PCR-based DNA sequenc-
ng can detect a particular mutant only if it is present20% of the total quasi species pool.61 Cloning can
vercome this problem, but analysis of large numbers oflones is required. Viral mutants that constitute as littles 5% of the total population can be detected by restric-ion fragment-length polymorphism analyses, but sepa-ate sets of endonuclease reactions must be designedpecifically for each (and known) mutant of interest.hese methods are labor intensive, require highly skilledersonnel, and are not suitable for high-throughputcreening. They are used only for “in house” or “home-rew” assays; with the exception of the TRUGENE geno-yping test developed by Visible Genetics (Siemensealthcare Diagnostics, Tarrytown, NY), few have been
ommercialized or approved by regulatory bodies.
PyrosequencingPyrosequencing is a new sequencing method that
elies on the detection of DNA polymerase activity byeasuring the pyrophosphate (PPi) released by the addi-
ion of a dNMP to the 3= end of a primer. It allowsetermination of the sequence of a single DNA strand byynthesizing a complementary strand, 1 base pair at aime, and detecting which base was added at each step.urrently, the main limitation of pyrosequencing is that
he maximum length of individual sequencing runs arehorter than those obtainable with conventional chainermination sequencing methods. Pyrosequencing is cur-ently the fastest and probably most sensitive (0.1%)
ethod available for detecting small subpopulations ofesistant virus84,85 and is likely to become the method ofhoice in the near future, particularly if the associated
nstrumentation becomes more affordable. sHybridizationExamples of hybridization-based genotyping
ethods, which can detect single nucleotide mismatchesnclude the following:
1) Mass spectrometric (matrix-assisted laser-desorptionionization time of flight mass spectrometry [MALDI-TOF MS]) analysis of small DNA fragments that canidentify mutants that constitute as little as 1% of thetotal viral population.86
2) The commercially available line probe assay, (INNO-LiPA, Innogenetics, Ghent, Belgium) which relies onthe differential hybridization of particular targets toa series of short membrane-bound oligonucleotideprobes to discriminate between wild-type sequencesand those of known drug-resistant mutants.87 LiPAassays can detect developing viral resistance when themutants responsible constitute only a minor fractionof the total viral population (5%–10%), an advantagein cases in which there is a high risk of diseaseprogression.88
3) DNA chip technologies. Sequencing with microchip-based technology using oligonucleotide microarrayshas the clear advantage of improved sensitivity as wellas ability to detect “new” mutants.89 These assays arerelatively easy to perform for the simultaneous detec-tion of a multitude of unique mutations as well asrecognized polymorphisms.90
One of the main limitations of all hybridization-basedethods is their specificity: new sets of specific probes are
equired for every mutant, and natural sequence variabil-ty in regions of interest reduces their discriminatoryower and specificity. Furthermore, sequence context andecondary structures in the target can affect sensitivity,nd minor subpopulations (those constituting less than0% of the total population) may escape detection. Foretection of known and “new” mutants, genotyping us-
ng oligonucleotide microarrays appears to be the onlyiable alternative to direct sequencing, but, because theumber of clinically relevant HBV mutants is still rela-ively small and the technology is specialized and expen-ive, it will be some time before they become cost-effec-ive.
In Vitro Phenotypic AssaysSeveral approaches have been developed to per-
orm in vitro phenotypic analysis of the resistant mu-ants identified in vivo in patients. These assays are crit-cal to determine the role of a given mutation profile inrug resistance as well as to determine the cross-resis-ance profile of those mutants. These approaches includeiral polymerase enzymatic assays, cell lines permanentlyxpressing HBV resistant mutants, and cell culture mod-ls in which the viral genome of resistant mutants isransferred for the analysis of viral replication and drug
usceptibility; these assays have been reviewed recently.91
Aottmmmttpp
btaHmdambar
1lnpaspvaesioTtm
tttrpHdd
fw
wili
slttpw(o
DaHrappaDtio
bdapcplittmlAp
o(tiAAodps
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1600 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
ll these assays have been useful to demonstrate the rolef a given polymerase gene mutation, observed in pa-ients with treatment failure, in the development of an-iviral drug resistance. They are also important to deter-
ine the cross-resistance profile of the main resistanceutations (see Table 2)51,92 and help develop clinicalanagement algorithms.53,93,94 Further useful informa-
ion is also generated on viral fitness, which is an impor-ant determinant in the process of understanding theatterns and profiles of resistant mutant selection in theatient.
Clinical Aspects of ResistanceDefinitionsAll patients receiving NA therapy for CHB should
e closely monitored for virologic response and break-hrough during treatment and for durability of responsend viral relapse after treatment has stopped.53 SerumBV DNA should be tested every 3 months during treat-ent.93 Failure of antiviral therapy of CHB may follow
ifferent directions, which rely on specific mechanismsnd therefore have clinical implications in terms of treat-ent adaptation. Thus, it is important to distinguish
etween primary nonresponse, partial virologic response,nd virologic breakthrough because of antiviral drugesistance (Figure 1).
Primary nonresponse. The failure to achieve a-log10 copies/mL (or 1.0 log10 IU/mL) decline in viral
oad after 12 weeks of therapy is considered as a primaryonresponse.53,93,94 It may be due to a problem of com-liance or the medication may not exhibit its antiviralctivity in a given patient. Suboptimal response has beenhown to be due to host pharmacologic effect and/or toatient compliance but not to a reduced susceptibility ofiral strains to ADV as measured in vitro by phenotypicssay.70 With more potent antiviral drugs, this phenom-non seems to be less frequent. When a primary nonre-ponse is identified, antiviral treatment should be mod-fied to prevent disease progression and subsequent riskf emergence of populations of drug-resistant mutants.he week 12 time point of therapy is therefore important
o determine the antiviral activity of the treatment regi-en and assess treatment adherence.
Partial response. A partial response correspondso the failure to achieve a viral load decline to a thresholdhat translates to an improvement in liver histology ando a minimum risk of resistance.95 The most recent Eu-opean Association for the Study of the Liver clinicalractice guidelines recommended to achieve undetectableBV DNA during therapy; therefore, partial response wasefined by detectable HBV DNA on real-time PCR assayuring continuous therapy.96
The antiviral response at week 24 of therapy has beenound to be a predictor of resistance in patients treated
ith LdT or LMV.11,12 Higher rates of resistance at 2 years nere observed when week 24 viral load was �1000 cop-es/mL (�200 IU/mL) compared with patients with aower viral load at the same time point, whatever theirnitial HBeAg status.
ADV was shown to suppress viremia levels with alower effect by comparison with other nucleoside ana-ogs, ie, LMV, ETV, LdT, or TDF. Therefore, the week 48ime point may be used for predicting resistance to ADVherapy.9 It has been demonstrated, in HBeAg-negativeatients treated with ADV for 192 weeks, that patientsith HBV DNA levels greater than 1000 copies/mL
�200 IU/mL) after 48 weeks of therapy had a higher riskf developing ADV resistance at week 192.
With ETV and TDF, the rate of undetectable HBVNA after 1 year of therapy is much higher, reaching 67%
nd 74% in HBeAg-positive patients and 90% and 91% inBeAg-negative patients, respectively.15,97,98 Because the
ate of viral suppression increases over time with these 2ntiviral drugs, the timing of treatment adaptation de-ends on the kinetics of viral load decay, especially inatients starting from very high viral load who may needdditional weeks of therapy to reach undetectable HBVNA by PCR testing. Thus, persisting low viremia/pla-
eau levels should lead to treatment adaptation to max-mize viral suppression and minimize the subsequent riskf resistance.99
Virologic breakthrough: viral rebound. Virologicreakthrough typically results from the emergence ofrug-resistant viral strains. It is defined by an increase oft least 1-log10 copies/mL (or �1.0-log10 IU/mL) com-ared with the lowest value (or nadir) during treatment,onfirmed by a second test, in a treatment compliantatient.53,93,94 Depending on the mutation profile se-
ected by the drug, viral load increase may be slow, mak-ng the diagnosis of rebound difficult. It usually followshe detection of genotypic resistance (Figure 1), ie, detec-ion of resistance mutations.3,53,93 In the absence of treat-
ent adaptation, the rise in viremia levels may be fol-owed in subsequent weeks or months by an increase inLT levels (biochemical breakthrough) and subsequentlyrogression of liver disease (clinical breakthrough).
Treatment of HBV Drug ResistancePrimary nonresponse. A primary nonresponse is
bserved more frequently in patients treated with ADVapproximately 10%–20% of patients) than in thosereated with other NA, probably because patients arenadequately dosed.70 Patients who do not respond toDV should be rapidly switched to TDF or ETV therapy.primary nonresponse to LMV, LdT, ETV, or TDF is
bserved only rarely2; in these patients, it is important toetermine the level of compliance. If a patient with arimary nonresponse to these drugs is compliant, analy-is of HBV NA-resistance mutations can identify alter-
ate treatment strategies96 (see Table 2).
sA2ltpfi(tn
ittHvibibv(mtassm
fta
lai
rdmr
HetpaatEAtddacvtaow
etlrLeabp
qcdtemustt
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1601
Partial virologic response. Partial virologic re-ponses have been observed with all NA used in CHB.gain, it is important to check for compliance. There arestrategies for treating patients who have a partial viro-
ogic response to LMV, ADV, or LdT at week 24: changeo a more potent drug (ETV or TDF) or add a moreotent drug that does not share cross-resistance. Teno-ovir should not be added to ADV therapy if the patients infected with an HBV mutant that is resistant to ADVie, rtA181T/V � rtN236T) because these drugs belong tohe same chemical group of NA, the alkyl phospho-ates.15,96,99,100
Virologic breakthrough. Virologic breakthroughn compliant patients is related to viral resistance. Resis-ance is associated with prior treatment with NA or, inreatment-naïve patients, with high baseline levels ofBV DNA, a slow decline in HBV DNA levels, and partial
irologic response to treatment. Resistance should bedentified as early as possible, before ALT levels increase,y monitoring HBV DNA levels and if possible identify-
ng the NA resistance profile; the therapeutic strategy cane determined based on this information. Clinical andirology studies have demonstrated the benefit of an earlyas soon as viral load increases) adaptation of treat-
ent.95,96,101 In cases of resistance, an appropriate rescueherapy should be initiated that has the most effectiventiviral effect and minimal risk for selection of MDRtrains. Therefore, adding a second drug that is not in theame cross-resistance group as the first is the recom-
ended strategy.Table 2 shows the cross-resistance data for the most
requent resistant HBV variants.92,96 Treatment adapta-ion should be performed accordingly and is summarizeds follows:
● LMV resistance: add TDF (add ADV if TDF notavailable);
● ADV resistance: it is recommended to switch to TDFif available AND add a second drug without cross-resistance. If an rtN236T substitution is present, addLMV, ETV, or LdT or switch to TDF plus emtricit-abine. If an rtA181V/T substitution is present, it isrecommended to add-on ETV or to switch to TDFplus ETV or TDF plus emtricitabine (as a singletablet: Truvada);
● LdT resistance: it is recommended to add TDF (orADV if TDF is not available);
● ETV resistance: it is recommended to add TDF;
● TDF resistance: primary resistance to TDF has notbeen confirmed so far. It is recommended that geno-typing and phenotyping be done by a reference-typelaboratory to determine the cross-resistance profile.
Entecavir, LdT, LMV or emtricitabine could be dadded but would depend on the profile (refer toTable 2).
Note that the safety of some combinations in theonger term is presently unknown and that add-on ther-py is not always successful in achieving adequate viralnhibition (PCR undetectability).
Preventing ResistanceThe spread of drug-resistant HBV mutants can be
educed by avoiding unnecessary drug use, choosingrugs and combinations more carefully, and continuallyonitoring or carrying out targeted surveillance for drug
esistance.45
Because of the unusual replication strategy used byBV, viral populations are genetically heterogeneous, so
ven treatment-naïve patients have drug-resistant mu-ants that constitute only a minor component of theopulation in the absence of selection pressure fromntiviral drugs. A majority of patients may not requirentiviral therapy. Several professional bodies (includinghe American Association for the Study of the Liver, theuropean Association for the Study of the Liver, thesian Pacific Association for the Study of the Liver, and
he National Institutes of Health) publish regularly up-ated guidelines to assist clinicians with recognition,iagnosis, prevention, and management of CHB: thesere unanimous in recommending that therapy should beonsidered for patients with only more active or ad-anced liver disease and others most likely to respond inhe context of defined treatment end points. Treatmentlgorithms have been developed to assist in identificationf suitable candidates for treatment and to determinehen to initiate treatment.Because drug-resistant mutant HBV populations are
stablished and expand through replication, antiviralherapy, once initiated, should aim to suppress viral rep-ication as completely and rapidly as possible. The lowerisk of resistance to TDF and ETV (compared with LMV,dT, and ADV) supports their use as first-line therapy,specially in patients who have received liver transplantsnd those with cirrhosis or decompensated liver diseaseecause development of drug resistance is more likely torecipitate clinical deterioration in these groups.Combination chemotherapy is being used more fre-
uently to treat CHB. It is effective when the appropriateombinations are employed and can reduce the risk ofrug resistance. Although HBV mutants that are resis-ant to single drugs exist before therapy starts and canvolve rapidly in patients, HBV mutants with MDR areuch less likely to exist before treatment. Ideally, drugs
sed in combination should have different mechanismso that they have additive/synergistic effects. Combina-ion therapy using NA with a complementary cross-resis-ance profile prevents the development of resistance but
oes not have increased antiviral effects, compared with
swipHb
ehlooctufia
teApecaymvtdsesmmmb
lmbacihlirnTrmtw
damacsf(pmrmmgct
Ft
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1602 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
ingle-drug therapy.102 Use of interferon in combinationith NA is probably the next logical step. Although
nitial clinical trials of such combinations were disap-ointing, results from later trials are more encouraging.owever, the added benefit of the combination tends to
e lost after treatment cessation.103,104
Combinations of L-nucleosides are unlikely to be moreffective than therapy with single L-nucleosides and canave antagonistic effects (because they compete for cel-
ular activation mechanisms and viral targets). The lackf cross-resistance of HBV mutants to LMV and ADVbserved in vitro (except for rtA181T/V) and in somelinical studies indicates that these drugs could be effec-ive in combination. Preliminary data also support these of ETV in combination with ADV or TDF, but de-nitive recommendations will require further clinical tri-ls and cost-benefit studies.
Each patient’s response to treatment should be moni-ored carefully so that drug resistance can be detectedarly, before viral breakthrough and disease progression.ssays for serum levels of HBV DNA and ALT should beerformed 3– 6 months after therapy begins, to check forfficacy and compliance; lack of compliance is the mostommon cause of primary treatment failure. Additionalssays, performed at 6-month intervals during the first 2ears of treatment, are recommended for patients withild liver disease. Patients should then be assessed for
iral load and ALT level every 3 months after 2 years ofherapy: this is the time during which the probability ofeveloping resistance increases. The consequences of re-istance appear more rapidly and can become life-threat-ning in patients with advanced disease; these patientshould be tested for viral load and ALT level every 3
onths. Once the viral load increases to �1.0-log10 IU/L, HBV Pol should be sequenced to identify resistanceutations and determine the next therapeutic approach,
ased on cross-resistance information (Figure 4).
Infectivity and Public Health AspectsThe gene that encodes the HBV polymerase over-
aps with the gene that encodes the viral envelope, and soutations in the overlapping reading frame can change
oth proteins (Figure 5A). The nucleotide change thatlters codon rt204 (rtM204I/V) in the polymerase geneonfers resistance to LMV, LdT, and ETV and also resultsn a nonsynonymous change in the gene encoding theepatitis B surface antigen (HBsAg), directly in the over-
apping region. The rtM204V mutation typically resultsn the substitution sI195M in HBsAg, whereas thetM204I change can cause sW196S, sW196L, or a termi-ation codon (Figure 5B), depending on codon useage.he mutation rtL180M is synonymous in HBsAg, but
tV173L results in sE164D, and this combination ofutations is found in up to 20% of cases of LMV resis-
ance.3,65 The ADV resistance mutation rtN236T overlaps
ith the stop codon at the end of the envelope gene and ioes not affect HBsAg. The mutation selected by ADVnd/or LMV/LdT at rtA181T typically results in a stoputation in the envelope gene (sW172stop) (Figure 5B),
nd the ADV resistance mutation at rtA181V results in aoncomitant change sL173F. Mutations that result in atop codon mutation in the envelope gene, such as thoseor LMV, LdT (rtM204I and rtA181T), and ADVrtA181T), are usually found in the presence of a lowercentage of wild-type HBV to ensure rescue of theutant by the wild-type to allow viral packaging and
elease of the defective variant.43 The ETV resistanceutation rtI169T results in a change at sF161L. Thisutation, along with sE164D, is located within the re-
ion that is defined as the “a” determinant, which in-ludes amino acids 95 to 165—the major antibody neu-ralization domain of HBV.
Thibault et al published the first case report of primary
igure 4. Management flow chart for first virologic breakthrough/par-ial virologic response.
nfection with LMV-resistant HBV105 (rtL180M�

raTdcp
ardd
FtmsmrplmlvibaTttis
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1603
tM204V), which was associated with a typical bout ofcute hepatitis and an incubation period of 2–3 months.he level of viremia was lower than that usually observeduring the acute phase of hepatitis B, and the virus wasleared. The acutely infected individual had not been
igure 5. Impact of drug resis-ance mutations in the viral poly-erase gene on the overlapping
urface gene. Panel A: Physicalap showing the impact of drug
esistance mutations in the viralolymerase gene on the enve-
ope gene. Resistance mutationsay therefore result in viral enve-
ope changes leading to alteredirion secretion, altered infectiv-ty, and escape to anti-HBs anti-odies. Panel B: Antiviral drug-ssociated HBsAg changes.he main amino acid substitu-ions in the viral polymerase andheir corresponding changesn the envelope proteins arehown.
reviously vaccinated against HBV. t
Several studies have reported mutations in HBsAg thatlter its antigenicity. Torresi et al observed that the LMVesistance mutations rtV173L�rtL180M�rtM204V (pro-ucing sE164D and sI195M in HBsAg) resulted in re-uced binding of antibody to this antigen,106 although
he reduction was not as great as that caused by the
mrc
tnrlspafrtTabiahoTmciribtdma
namsenowdlotcrpTcaudo
Hmttipcmmevsoncpis
ifgbgsalinPtcppdi
Iapsmaittl
titoM
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1604 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
utant sG145R, compared with wild-type HBV. Theseesults were confirmed and extended by Sloan et al usingell-derived HBVs.107
Very few in vitro studies have been performed to studyhe infectivity of the NA-resistant mutants. The combi-ation of polymerase and surface gene mutations mightesult in viruses that exhibit a reduced fitness that trans-ates to differences of selection kinetics. However, thesetudies are hampered by the challenges of working withrimary human hepatocytes, the only cellular systemvailable for these investigations. Bartholomew et al in-ected primary human hepatocytes with HBV using se-um samples collected from patients before the start ofreatment with LMV and after viral breakthrough.108
heir results demonstrated that the viral strains isolatedt the time of viral breakthrough were resistant to LMVut could still infect hepatocytes. The hepatocyte progen-
tor cell line HepaRG has specific hepatocyte functionsnd can be infected by HBV; primary cultures of normaluman hepatocytes were also used in infectivity studiesf clinical isolates, especially of drug-resistant strains.109
hese studies showed that mutations in the HBV poly-erase and overlapping surface genes can impair repli-
ation capacity, virion secretion efficiency, and infectiv-ty;42 some of these mutant HBVs escaped antibodyecognition and could therefore mediate breakthroughnfection in vaccinated individuals and escape detectiony commercial diagnostic kits. The effect of these substi-utions on HBV infectivity was shown to be a criticaleterminant of which resistant mutants would spreadore rapidly in the liver and dominate other HBV vari-
nts.42
In chimpanzees, Kamili et al44 challenged the immu-ity induced by a commercial hepatitis B vaccine againsttissue culture-derived HBV clone that contained 3 poly-erase mutations (rtV173L, rtL180M, rtM204V) and
ubstitution mutations in the overlapping region thatncodes the envelope/HBsAg (sE164D, sI195M). Immu-ologic evidence of HBV infection and replication wasbserved in the vaccinated chimpanzees after challengeith the mutant as well as after rechallenge with serum-erived wild-type HBV, despite robust humoral and cel-
ular anti-HBV immune responses to the vaccine. Thebserved infection by the mutant form of HBV, despitehe presence of high levels of HBV antibody (which wereonsidered to be protective), are consistent with clinicaleports of breakthrough infections in anti-HBs-positiveatients who are infected with escape HBV mutants.44
herefore, “antiviral drug-associated potential vaccine es-ape mutants” have the potential to jeopardize the hep-titis B immunization program110 (Supplementary Fig-re 2). As more HBV mutants arise that have resistance toifferent antiviral agents, the effects on the antigenicity
f the HBsAg protein will need to be established. mFuture Directions and ConclusionVery few new drugs are being developed to treat
BV; therefore, it is important to continue research intoechanisms of pathogenesis and resistance and to iden-
ify new therapeutic targets. Small molecule inhibitorshat are directed against multiple HBV targets shouldmprove viral clearance and prevent resistance (see Sup-lementary Figure 1). For example, virus entry into theell can be inhibited111,112 using pre-S1 peptides, whichimic the envelope protein domain involved in virus-cellembrane interaction. These peptides prevented HBV
ntry into cultured hepatocytes and inhibited subsequentiral infection and spread in the HBV animal model ofevere combined immunodeficient mice.112 Combinationf these peptides with NA could prevent the infection ofew cells when viral load is suppressed by NA and in-rease the rate of clearance of infected cells as well asreventing further de novo infections. Ongoing preclin-
cal and clinical studies will determine their efficacy andafety.
Reagents have been tested that target cccDNA or stepsn its formation and processing, but these have beenound to have cytotoxic effects. Agents that modify epi-enetic regulation of cccDNA transcriptional activity areeing investigated in experimental models.113 Viral pre-enome encapsidation and capsid formation also repre-ent potential targets. Phenylpropenamide derivativesnd heteroaryl-pyrimidines are known to inhibit the rep-ication of wild-type and LMV-resistant mutant genomesn hepatoma cell lines,114 –117 although clinical trials wereot conducted because of formulation problems. AiCurisharmaceuticals (Wuppertal, Germany) has developedhe heteroaryl-pyrimidines molecules further as non-nu-leoside inhibitors of HBV core protein dimerization thatrevent nucleocapsid formation.116,117 The heteroaryl-yrimidines prevented HBV infection in an animal mo-el116 and represent a potentially important new advance
n chemotherapy.Viral morphogenesis and egress are also useful targets.
minosugars, which modulate the glycosylation statusnd conformation of envelope proteins, can decrease theroduction of infectious particles in vitro.118 They werehown to have an antiviral effect in the woodchuck
odel of hepadnavirus infection.119 Therapeutics mightlso be developed to modulate the innate response ofnfected hepatocytes,120,121 dendritic cell activation,122 orhe adaptive immune response.123–125 Induction of sus-ained immunologic control of HBV infection could al-ow for timed cessation of NA administration.
Ideally, treatment for CHB should begin at diagnosis;his is not feasible because of limitations of drugs. Clin-cal trials and concurrent improvements in diagnosticechnology ensure that treatment options and expertpinion on patient management will continue to evolve.any laboratories are genotyping and phenotyping HBV
utants to delineate patterns of resistance and cross-
rtvavgtfapgctsofa“wn
outcgitp
tpmcmpt
aG1
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1605
esistance. These data will improve the design of newherapeutic strategies and maximize the benefits of anti-iral agents. Resistance-testing methodologies vary, and,lthough few direct comparisons have been made, initro phenotype testing (if possible, in combination withenotype testing) seems superior to conventional geno-ype or virtual phenotyping testing. This is especially trueor analysis of HBV isolated from patients who havelready been treated with several drugs, in whom multi-le mutations are more likely to have become fixed in theenetic archive. Drug resistance testing of HBV isolates isurrently performed only in a few specialized “reference-ype” laboratories, but it should become routine as moreensitive, reliable, high-throughput, and accurate meth-ds are developed, along with clinically useful algorithmsor interpretation. In particular, standardization of testsnd definition of resistance/susceptibility thresholds orcut-offs” that can be used to correlate laboratory resultsith clinical observations and outcomes are urgentlyeeded.Methods for assessing the relative replication capacity
f HBV mutants are being developed and will proveseful in selecting therapy and tailoring individual pa-ient management. In cases in which treatment failureannot be attributed to patient noncompliance or emer-ence of resistant virus, host factors might be involved. Its important to monitor viral load throughout therapy sohat the treatment strategy can be modified in cases ofartial response or virologic breakthrough.The choice of the first-line agent(s) is very important;
he goal is to delay the development of resistance and toreserve treatment options over the long-term of treat-ent for CHB. The development of therapeutics that
omplement the effects of NA is warranted; new treat-ent strategies must be aimed at increasing viral sup-
ression and promoting virologic clearance and ensuringhe prevention of drug resistance and its complications.
Supplementary Data
Note: To access the supplementary materialccompanying this article, visit the online version ofastroenterology at www.gastrojournal.org, and at doi:0.1053/j.gastro.2009.08.063.
References
1. Summers J, Mason WS. Replication of the genome of a hepatitisB-like virus by reverse transcription of an RNA intermediate. Cell1982;29:403–415.
2. Dienstag JL. Hepatitis B virus infection. N Engl J Med 2008;359:1486–1500.
3. Nafa S, Ahmed S, Tavan D, et al. Early detection of viral resis-tance by determination of hepatitis B virus polymerase muta-tions in patients treated by lamivudine for chronic hepatitis B.Hepatology 2000;32:1078–1088.
4. Yuen MF, Sablon E, Hui CK, et al. Factors associated withhepatitis B virus DNA breakthrough in patients receiving pro-
longed lamivudine therapy. Hepatology 2001;34:785–791.5. Lai CL, Dienstag J, Schiff E, et al. Prevalence and clinical corre-lates of YMDD variants during lamivudine therapy for patientswith chronic hepatitis B. Clin Infect Dis 2003;36:687–696.
6. Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudinetreatment in patients with chronic hepatitis B. Gastroenterology2003;125:1714–1722.
7. Dienstag JL, Goldin RD, Heathcote EJ, et al. Histological out-come during long-term lamivudine therapy. Gastroenterology2003;124:105–117.
8. Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients withchronic hepatitis B and advanced liver disease. N Engl J Med2004;351:1521–1531.
9. Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-termtherapy with adefovir dipivoxil for HBeAg-negative chronic hepa-titis B for up to 5 years. Gastroenterology 2006;131:1743–1751.
10. Fung SK, Andreone P, Han SH, et al. Adefovir-resistant hepatitisB can be associated with viral rebound and hepatic decompen-sation. J Hepatol 2005;43:937–943.
11. Lai CL, Gane E, Liaw YF, et al. Telbivudine versus lamivudine inpatients with chronic hepatitis B. N Engl J Med 2007;357:2576–2588.
12. Liaw YF, Gane E, Leung N, et al. 2-Year GLOBE trial results:telbivudine is superior to lamivudine in patients with chronichepatitis B. Gastroenterology 2009;136:486–495.
13. Marcellin P, Chang TT, Lim SG, et al. Long-term efficacy andsafety of adefovir dipivoxil for the treatment of hepatitis B eantigen-positive chronic hepatitis B. Hepatology 2008;48:750–758.
14. Lee YS, Suh DJ, Lim YS, et al. Increased risk of adefovir resis-tance in patients with lamivudine-resistant chronic hepatitis Bafter 48 weeks of adefovir dipivoxil monotherapy. Hepatology2006;43:1385–1391.
15. Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxilfumarate versus adefovir dipivoxil for chronic hepatitis B. N EnglJ Med 2008;359:2442–2455.
16. Snow-Lampart A, Chappell BJ, Curtis M, et al. Week 96 resis-tance surveillance for HBeAg-positive and negative subjects withchronic HBV infection randomized to receive Tenofovir DF 300mg QD. In 59th Annual Meeting of the American Association forthe Study of Liver Diseases, San Francisco, CA, October 31–November 04, 2008. Hepatology, 2008.
17. Tenney DJ, Rose RE, Baldick CJ, et al. Long-term monitoringshows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology2009;49:1503–1514.
18. Tenney DJ, Pokornowski KA, Rose RE, et al. Entecavir maintainsa high genetic barrier to HBV resistance through 6 years in naivepatients. J Hepatol 2009;50:S10. Abstract 20
19. Zoulim F. New insight on hepatitis B virus persistence from thestudy of intrahepatic viral cccDNA. J Hepatol 2005;42:302–308.
20. Zoulim F. Mechanism of viral persistence and resistance tonucleoside and nucleotide analogs in chronic hepatitis B virusinfection. Antiviral Res 2004;64:1–15.
21. Seeger C, Mason WS. Hepatitis B virus biology. Microbiol MolBiol Rev 2000;64:51–68.
22. Kock J, Baumert TF, Delaney WEt, et al. Inhibitory effect ofadefovir and lamivudine on the initiation of hepatitis B virusinfection in primary tupaia hepatocytes. Hepatology 2003;38:1410–1418.
23. Delmas J, Schorr O, Jamard C, et al. Inhibitory effect of adefoviron viral DNA synthesis and covalently closed circular DNA for-mation in duck hepatitis B virus-infected hepatocytes in vivo andin vitro. Antimicrob Agents Chemother 2002;46:425–433.
24. Zhou T, Saputelli J, Aldrich CE, et al. Emergence of drug-resis-
tant populations of woodchuck hepatitis virus in woodchucks
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1606 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
treated with the antiviral nucleoside lamivudine. AntimicrobAgents Chemother 1999;43:1947–1954.
25. Werle-Lapostolle B, Bowden S, Locarnini S, et al. Persistence ofcccDNA during the natural history of chronic hepatitis B anddecline during adefovir dipivoxil therapy. Gastroenterology2004;126:1750–1758.
26. Sung JJ, Wong ML, Bowden S, et al. Intrahepatic hepatitis Bvirus covalently closed circular DNA can be a predictor of sus-tained response to therapy. Gastroenterology 2005;128:1890–1897.
27. Wursthorn K, Lutgehetmann M, Dandri M, et al. Peginterferon�-2b plus adefovir induce strong cccDNA decline and HBsAgreduction in patients with chronic hepatitis B. Hepatology 2006;44:675–684.
28. Lutgehetmann M, Volzt T, Quaas A, et al. Sequential combina-tion therapy leads to biochemical and histological improvementdespite low ongoing intrahepatic hepatitis B virus replication.Antivir Ther 2008;13:57–66.
29. Moraleda G, Saputelli J, Aldrich CE, et al. Lack of effect ofantiviral therapy in nondividing hepatocyte cultures on theclosed circular DNA of woodchuck hepatitis virus. J Virol 1997;71:9392–9399.
30. Mason WS, Cullen J, Moraleda G, et al. Lamivudine therapy ofWHV-infected woodchucks. Virology 1998;245:18–32.
31. Le Guerhier F, Pichoud C, Jamard C, et al. Antiviral activity of�-L-2=,3=-dideoxy-2=,3=-didehydro-5-fluorocytidine in woodchuckschronically infected with woodchuck hepatitis virus. AntimicrobAgents Chemother 2001;45:1065–1077.
32. Le Guerhier F, Pichoud C, Guerret S, et al. Characterization ofthe antiviral effect of 2=,3=-dideoxy-2=,3=- didehydro-�-L-5-fluoro-cytidine in the duck hepatitis B virus infection model. AntimicrobAgents Chemother 2000;44:111–22.
33. Nowak MA, Bonhoeffer S, Hill AM, et al. Viral dynamics inhepatitis B virus infection. Proc Natl Acad Sci U S A 1996;93:4398–4402.
34. Lewin SR, Ribeiro RM, Walters T, et al. Analysis of hepatitis Bviral load decline under potent therapy: complex decay profilesobserved. Hepatology 2001;34:1012–1020.
35. Pawlotsky JM. The concept of hepatitis B virus mutant escape.J Clin Virol 2005;34(Suppl 1):S125–S129.
36. Gunther S, Fischer L, Pult I, et al. Naturally occurring variants ofhepatitis B virus. Adv Virus Res 1999;52:25–137.
37. Villet S, Pichoud C, Villeneuve JP, et al. Selection of a multipledrug-resistant hepatitis B virus strain in a liver-transplantedpatient. Gastroenterology 2006;131:1253–1261.
38. Seigneres B, Pichoud C, Ahmed SS, et al. Evolution of hepatitisB virus polymerase gene sequence during famciclovir therapyfor chronic hepatitis B. J Infect Dis 2000;181:1221–1233.
39. Pallier C, Castera L, Soulier A, et al. Dynamics of hepatitis Bvirus resistance to lamivudine. J Virol 2006;80:643–653.
40. Pallier C, Rodriguez C, Brillet R, et al. Complex dynamics ofhepatitis B virus resistance to adefovir. Hepatology 2009;49:50–59.
41. Litwin S, Toll E, Jilbert AR, et al. The competing roles of virusreplication and hepatocyte death rates in the emergence ofdrug-resistant mutants: theoretical considerations. J Clin Virol2005;34(Suppl 1):S96–S107.
42. Villet S, Billioud G, Pichoud C, et al. In vitro characterization ofviral fitness of therapy-resistant hepatitis B variants. Gastroen-terology 2009;136:168–176.
43. Warner N, Locarnini S. The antiviral drug selected hepatitis Bvirus rtA181T/sW172* mutant has a dominant negative secre-tion defect and alters the typical profile of viral rebound. Hepa-tology 2008;48:88–98.
44. Kamili S, Sozzi V, Thompson G, et al. Efficacy of hepatitis Bvaccine against antiviral drug-resistant hepatitis B virus mutants
in the chimpanzee model. Hepatology 2009;49:1483–1491.45. Richman DD. The impact of drug resistance on the effectivenessof chemotherapy for chronic hepatitis B. Hepatology 2000;32:866–867.
46. Nowak M, Bonhoeffer S, Hill A, et al. Viral dynamics in hepatitisB virus infection. Proc Natl Acad Sci U S A 1996;93:4398–4402.
47. Okamoto H, Imai M, Kametani M, et al. Genomic heterogeneityof hepatitis B virus in a 54-year-old woman who contracted theinfection through materno-fetal transmission. Jpn J Exp Med1987;57:231–236.
48. Girones R, Miller RH. Mutation rate of the hepadnavirus ge-nome. Virology 1989;170:595–597.
49. Domingo E. Quasispecies and the development of new antiviralstrategies. Prog Drug Res 2003;60:133–158.
50. Richman DD. The implications of drug resistance for strategiesof combination antiviral chemotherapy. Antiviral Res 1996;29:31–33.
51. Durantel D, Carrouee-Durantel S, Werle-Lapostolle B, et al. Anew strategy for studying in vitro the drug susceptibility ofclinical isolates of human hepatitis B virus. Hepatology 2004;40:855–864.
52. Zhang YY, Summers J. Low dynamic state of viral competition ina chronic avian hepadnavirus infection. J Virol 2000;74:5257–5265.
53. Lok AS, Zoulim F, Locarnini S, et al. Antiviral drug-resistant HBV:standardization of nomenclature and assays and recommenda-tions for management. Hepatology 2007;46:254–265.
54. Zoulim F, Poynard T, Degos F, et al. A prospective study of theevolution of lamivudine resistance mutations in patients withchronic hepatitis B treated with lamivudine. J Viral Hepat 2006;13:278–288.
55. Ghany M, Liang TJ. Drug targets and molecular mechanisms ofdrug resistance in chronic hepatitis B. Gastroenterology 2007;132:1574–1585.
56. Stuyver LJ, Locarnini SA, Lok A, et al. Nomenclature for antiviral-resistant human hepatitis B virus mutations in the polymeraseregion. Hepatology 2001;33:751–757.
57. Yeh CT, Chien RN, Chu CM, et al. Clearance of the originalhepatitis B virus YMDD-motif mutants with emergence of dis-tinct lamivudine-resistant mutants during prolonged lamivudinetherapy. Hepatology 2000;31:1318–1326.
58. Ogata N, Fujii K, Takigawa S, et al. Novel patterns of amino acidmutations in the hepatitis B virus polymerase in associationwith resistance to lamivudine therapy in japanese patients withchronic hepatitis B. J Med Virol 1999;59:270–276.
59. Tenney DJ, Levine SM, Rose RE, et al. Clinical emergence ofentecavir-resistant hepatitis B virus requires additional substi-tutions in virus already resistant to Lamivudine. AntimicrobAgents Chemother 2004;48:3498–3507.
60. Delaney WEt, Yang H, Westland CE, et al. The hepatitis B viruspolymerase mutation rtV173L is selected during lamivudinetherapy and enhances viral replication in vitro. J Virol 2003;77:11833–11841.
61. Shaw T, Bartholomeusz A, Locarnini S. HBV drug resistance:mechanisms, detection and interpretation. J Hepatol 2006;44:593–606.
62. Villet S, Pichoud C, Billioud G, et al. Impact of hepatitis B virusrtA181V/T mutants on hepatitis B treatment failure. J Hepatol2008;48:747–755.
63. Villet S, Ollivet A, Pichoud C, et al. Stepwise process for thedevelopment of entecavir resistance in a chronic hepatitis Bvirus infected patient. J Hepatol 2007;46:531–538.
64. Delaney WEt, Locarnini S, Shaw T. Resistance of hepatitis Bvirus to antiviral drugs: current aspects and directions for future
investigation. Antivir Chem Chemother 2001;12:1–35.
1
1
1
REV
IEW
SIN
BA
SIC
AN
DCLI
NIC
AL
GA
STRO
ENTE
RO
LOG
Y
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1607
65. Zollner B, Petersen J, Puchhammer-Stockl E, et al. Viral featuresof lamivudine resistant hepatitis B genotypes A and D. Hepatol-ogy 2004;39:42–50.
66. Angus P, Vaughan R, Xiong S, et al. Resistance to adefovirdipivoxil therapy associated with the selection of a novel muta-tion in the HBV polymerase. Gastroenterology 2003;125:292–297.
67. Villeneuve JP, Durantel D, Durantel S, et al. Selection of ahepatitis B virus strain resistant to adefovir in a liver transplan-tation patient. J Hepatol 2003;39:1085–1089.
68. Brunelle MN, Jacquard AC, Pichoud C, et al. Susceptibility toantivirals of a human HBV strain with mutations conferringresistance to both lamivudine and adefovir. Hepatology 2005;41:1391–1398.
69. Schildgen O, Sirma H, Funk A, et al. Variant of hepatitis B viruswith primary resistance to adefovir. N Engl J Med 2006;354:1807–1812.
70. Carrouee-Durantel S, Durantel D, Werle-Lapostolle B, et al. Sub-optimal response to adefovir dipivoxil therapy for chronic hepa-titis B in nucleoside-naive patients is not due to pre-existingdrug-resistant mutants. Antivir Ther 2008;13:381–388.
71. Curtis M, Zhu Y, Borroto-Esoda K. Hepatitis B virus containingthe I233V mutation in the polymerase reverse-transcriptasedomain remains sensitive to inhibition by Adefovir. J Infect Dis2007;196:1483–1486.
72. Yuen LK, Ayres A, Littlejohn M, et al. SeqHepB: a sequenceanalysis program and relational database system for chronichepatitis B. Antiviral Res 2007;75:64–74.
73. Sheldon J, Camino N, Rodes B, et al. Selection of hepatitis Bvirus polymerase mutations in HIV-coinfected patients treatedwith tenofovir. Antivir Ther 2005;10:727–734.
74. Delaney WEt, Ray AS, Yang H, et al. Intracellular metabolismand in vitro activity of tenofovir against hepatitis B virus. Anti-microb Agents Chemother 2006;50:2471–2477.
75. Van Bommel F, deMann RA, Wedemeyer H, et al. Efficacy ofTenofovir DF for the treatment of adefovir resistance. Hepatol-ogy 2009. In press.
76. Angus P, Locarnini S. Lamivudine-resistant hepatitis B virus andongoing lamivudine therapy: stop the merry-go-round, it’s timeto get off! Antivir Ther 2004;9:145–148.
77. Ono-Nita SK, Kato N, Shiratori Y, et al. Novel nucleoside ana-logue MCC-478 (LY582563) is effective against wild-type orlamivudine-resistant hepatitis B virus. Antimicrob Agents Che-mother 2002;46:2602–2605.
78. Levine S, Hernandez D, Yamanaka G, et al. Efficacies of ente-cavir against lamivudine-resistant hepatitis B virus replicationand recombinant polymerases in vitro. Antimicrob Agents Che-mother 2002;46:2525–2532.
79. Chin R, Shaw T, Torresi J, et al. In vitro susceptibilities ofwild-type or drug-resistant hepatitis B virus to (�)-�-D-2,6-dia-minopurine dioxolane and 2=-fluoro-5-methyl-�-L-arabinofurano-syluracil. Antimicrob Agents Chemother 2001;45:2495–2501.
80. Yuen L, Bartholomeusz A, Ayres A, et al. Multidrug resistanceand cross-resistance pathways in HBV as a consequence oftreatment failure. In 58th Annual Meeting of the American As-sociation for the Study of Liver Diseases, Boston, MA, Novem-ber 02–06, Hepatology 2007.
81. Yim HJ, Hussain M, Liu Y, et al. Evolution of multi-drug resistanthepatitis B virus during sequential therapy. Hepatology 2006;44:703–712.
82. Clavel F, Hance AJ. HIV drug resistance. N Engl J Med 2004;350:1023–1035.
83. Lok AS, Zoulim F, Locarnini S, et al. Monitoring drug resistancein chronic hepatitis B virus (HBV)-infected patients during lami-vudine therapy: evaluation of performance of INNO-LiPA HBV DR
assay. J Clin Microbiol 2002;40:3729–3734.84. Margeridon-Thermet S, Shulman NS, Ahmed A, et al. Ultra-deeppyrosequencing of hepatitis B virus quasispecies from nucleo-side and nucleotide reverse-transcriptase inhibitor (NRTI)-treated patients and NRTI-naive patients. J Infect Dis 2009;199:1275–1285.
85. Solmone M, Vincenti D, Prosperi MC, et al. Use of massivelyparallel ultradeep pyrosequencing to characterize the geneticdiversity of hepatitis B virus in drug-resistant and drug-naivepatients and to detect minor variants in reverse transcriptaseand hepatitis B S antigen. J Virol 2009;83:1718–1726.
86. Kim HS, Han KH, Ahn SH, et al. Evaluation of methods formonitoring drug resistance in chronic hepatitis B patients duringlamivudine therapy based on mass spectrometry and reversehybridization. Antivir Ther 2005;10:441–449.
87. Stuyver L, Van Geyt C, De Gendt S, et al. Line probe assay formonitoring drug resistance in hepatitis B virus-infected patientsduring antiviral therapy. J Clin Microbiol 2000;38:702–707.
88. Hussain M, Fung S, Libbrecht E, et al. Sensitive line probe assaythat simultaneously detects mutations conveying resistance tolamivudine and adefovir. J Clin Microbiol 2006;44:1094–1097.
89. Tran N, Berne R, Chann R, et al. European multicenter evalua-tion of high-density DNA probe arrays for detection of hepatitisB virus resistance mutations and identification of genotypes.J Clin Microbiol 2006;44:2792–2800.
90. Jang H, Cho M, Heo J, et al. Oligonucleotide chip for detectionof Lamivudine-resistant hepatitis B virus. J Clin Microbiol 2004;42:4181–4188.
91. Zoulim F. In vitro models for studying hepatitis B virus drugresistance. Semin Liver Dis 2006;26:171–180.
92. Fournier C, Zoulim F. Antiviral therapy of chronic hepatitis B:prevention of drug resistance. Clin Liver Dis 2007;11:869–892.
93. Locarnini S, Hatzakis A, Heathcote J, et al. Management ofantiviral resistance in patients with chronic hepatitis B. AntivirTher 2004;9:679–693.
94. Pawlotsky JM, Dusheiko G, Hatzakis A, et al. Virologic monitor-ing of hepatitis B virus therapy in clinical trials and practice:recommendations for a standardized approach. Gastroenterol-ogy 2008;134:405–415.
95. Zoulim F, Perrillo R. Hepatitis B: reflections on the currentapproach to antiviral therapy. J Hepatol 2008;48(Suppl 1):S2–S19.
96. European Association for the Study of the Liver. EASL clinicalpractice guidelines: management of chronic hepatitis B. J Hepa-tol 2009;50:227–242.
97. Chang TT, Gish RG, de Man R, et al. A comparison of entecavirand lamivudine for HBeAg-positive chronic hepatitis B. N EnglJ Med 2006;354:1001–1010.
98. Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine forpatients with HBeAg-negative chronic hepatitis B. N Engl J Med2006;354:1011–1020.
99. Keeffe EB, Zeuzem S, Koff RS, et al. Report of an internationalworkshop: roadmap for management of patients receiving oraltherapy for chronic hepatitis B. Clin Gastroenterol Hepatol2007;5:890–897.
00. Chan HL, Heathcote EJ, Marcellin P, et al. Treatment of hepa-titis B e antigen positive chronic hepatitis with telbivudine oradefovir: a randomized trial. Ann Intern Med 2007;147:745–754.
01. Lampertico P, Vigano M, Manenti E, et al. Low resistance toadefovir combined with lamivudine: a 3-year study of 145 Lami-vudine-resistant hepatitis B patients. Gastroenterology 2007;133:1445–1451.
02. Sung JJ, Lai JY, Zeuzem S, et al. Lamivudine compared withlamivudine and adefovir dipivoxil for the treatment of HBeAg-
positive chronic hepatitis B. J Hepatol 2008;48:728–735.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
R
8f
A
m
C
aNSfA
F
et(
REV
IEWS
INBA
SICA
ND
CLIN
ICA
LG
ASTR
OEN
TERO
LOG
Y
1608 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
03. Marcellin P, Lau GK, Bonino F, et al. Peginterferon alfa-2a alone,lamivudine alone, and the two in combination in patients withHBeAg-negative chronic hepatitis B. N Engl J Med 2004;351:1206–1217.
04. Lau GK, Piratvisuth T, Luo KX, et al. Peginterferon alfa-2a,lamivudine, and the combination for HBeAg-positive chronichepatitis B. N Engl J Med 2005;352:2682–2695.
05. Thibault V, Aubron-Olivier C, Agut H, et al. Primary infection witha lamivudine-resistant hepatitis B virus. Aids 2002;16:131–133.
06. Torresi J, Earnest-Silveira L, Deliyannis G, et al. Reduced anti-genicity of the hepatitis B virus HBsAg protein arising as aconsequence of sequence changes in the overlapping polymer-ase gene that are selected by lamivudine therapy. Virology2002;293:305–313.
07. Sloan RD, Ijaz S, Moore PL, et al. Antiviral resistance mutationspotentiate hepatitis B virus immune evasion through disruptionof its surface antigen a determinant. Antivir Ther 2008;13:439–447.
08. Bartholomew MM, Jansen RW, Jeffers LJ, et al. Hepatitis B virusresistance to lamivudine given for recurrent infection after or-thotopic liver transplantation. Lancet 1997;349:20–22.
09. Gripon P, Rumin S, Urban S, et al. Infection of a human hepa-toma cell line by hepatitis B virus. Proc Natl Acad Sci U S A2002;99:15655–15660.
10. Clements J, Coghlan B, Creati M, et al. Global control of hepa-titis B infection: does the potential for antigenic change of thevirus in the face of antiviral treatment affect the global hepatitisB immunization programme? Bull WHO 2009. In press.
11. Gripon P, Cannie I, Urban S. Efficient inhibition of hepatitis Bvirus infection by acylated peptides derived from the large viralsurface protein. J Virol 2005;79:1613–1622.
12. Petersen J, Dandri M, Mier W, et al. Prevention of hepatitis Bvirus infection in vivo by entry inhibitors derived from the largeenvelope protein. Nat Biotechnol 2008;26:335–341.
13. Pollicino T, Belloni L, Raffa G, et al. Hepatitis B virus replicationis regulated by the acetylation status of hepatitis B viruscccDNA-bound H3 and H4 histones. Gastroenterology 2006;130:823–837.
14. King RW, Ladner SK, Miller TJ, et al. Inhibition of human hepa-titis B virus replication by AT-61, a phenylpropenamide deriva-tive, alone and in combination with (�)b-L-2=,3=-dideoxy-3=-thia-cytidine. Antimicrob Agents Chemother 1998;42:3179–3186.
15. Delaney WEt, Edwards R, Colledge D, et al. Phenylpropenamidederivatives AT-61 and AT-130 inhibit replication of wild-type andlamivudine-resistant strains of hepatitis B virus in vitro. Antimi-crob Agents Chemother 2002;46:3057–3060.
16. Weber O, Schlemmer KH, Hartmann E, et al. Inhibition of humanhepatitis B virus (HBV) by a novel non-nucleosidic compound ina transgenic mouse model. Antiviral Res 2002;54:69–78.
17. Deres K, Schroder CH, Paessens A, et al. Inhibition of hepatitisB virus replication by drug-induced depletion of nucleocapsids.
Science 2003;299:893–896. H18. Lazar C, Durantel D, Macovei A, et al. Treatment of hepatitis Bvirus-infected cells with �-glucosidase inhibitors results in pro-duction of virions with altered molecular composition and infec-tivity. Antiviral Res 2007;76:30–37.
19. Block TM, Lu X, Mehta AS, et al. Treatment of chronic hepad-navirus infection in a woodchuck animal model with an inhibitorof protein folding and trafficking. Nat Med 1998;4:610–614.
20. Thompson AJ, Colledge D, Rodgers S, et al. Stimulation of theinterleukin-1 receptor and Toll-like receptor 2 inhibits hepatitisB virus replication in hepatoma cell lines in vitro. AntiviralTherapy 2009;14:In press.
21. Lucifora J, Durantel D, Testoni B, et al. Control of hepatitis Bvirus replication by innate response of HepaRG cells. Hepatol-ogy 2009; In press.
22. Vincent IE, Lucifora J, Durantel D, et al. Inhibitory effect of thecombination of CpG-induced cytokines with lamivudine againsthepatitis B virus replication in vitro. Antivir Ther 2009;14:131–135.
23. Das A, Hoare M, Davies N, et al. Functional skewing of theglobal CD8 T-cell population in chronic hepatitis B virus infec-tion. J Exp Med 2008;205:2111–2124.
24. Lopes AR, Kellam P, Das A, et al. Bim-mediated deletion ofantigen-specific CD8 T cells in patients unable to control HBVinfection. J Clin Invest 2008;118:1835–1845.
25. Dunn C, Brunetto M, Reynolds G, et al. Cytokines inducedduring chronic hepatitis B virus infection promote a pathway forNK cell-mediated liver damage. J Exp Med 2007;204:667–680.
Received June 19, 2009. Accepted August 28, 2009.
eprint requestsAddress requests for reprints to: Fabien Zoulim, MD, INSERM UNIT
71, 151 Cours Albert Thomas, 69003 Lyon, France. email:[email protected]; fax: �33 472 681971.
cknowledgmentsThe authors thank Tania Candy for editorial help in theanuscript preparation.
onflicts of interestThe authors disclose the following: F.Z. has received consulting
nd speaker honoraria from Gilead Sc, Bristol Myers Squibb,ovartis, and Roche and has received research support from Gileadc and Roche. S.L. has received consulting and speaking honorariarom Gilead Sciences, Bristol-Myers Squibb, Roche Pharmaceuticals,bbott Diagnostic, and Evivar Medical Pty Ltd.
undingSupported by the European Community (ViRgil network of
xcellence; ViRgil LSHM-CT-2004-503359; to F.Z.) and grants fromhe National Agency for Research against AIDS and HepatitisANRS; to F.Z.) and funding from the US National Institutes of
ealth (RO1 AIO60449 and RO1 AI071820; to S.L.).
SiLfIpesia
November 2009 HBV AND RESISTANCE TO NUCLEOS(T)IDE ANALOGUES 1608.e1
upplementary Figure 1. The heptatitis B virus replication cycle andn the viral replication cycle. HBV is able to infect hepatocytes, successinear genomes have a high propensity to integrate into host DNA; vira
ormation of cccDNA), viral messenger RNA are transcribed, including pn the cytoplasm, pgRNA can be bound by the viral reverse transcriptaslace. Following completion of the minus strand DNA and partial condoplasmic reticulum. Nucleoside(tide) analogs mainly inhibit the viraynthesis (DNA dependent DNA polymerase activity) within viral nucleoc
n the nucleus of infected cells, therefore requiring long-term treatment
the potential antiviral targets. The Figure shows all the major steps requiredful infection defined by the formation of covalently closed circular (cccDNA).l genome integration is not required for viral genome replication. Following
regenomic RNA (pgRNA), the template for reverse transcription of viral DNA.e and packaged into viral nucleocapsids, where reverse transcription takes
mpletion of the plus strand DNA, virions are formed via budding into thel minus strand DNA synthesis (reverse transcription) and plus strand DNAapsids. These drugs do not affect directly viral cccDNA, which is maintainedfor a sustained control of viral replication. All other steps of the viral life cycle
re potential targets for antiviral therapy.

Saetpc
1608.e2 ZOULIM AND LOCARNINI GASTROENTEROLOGY Vol. 137, No. 5
upplementary Figure 2. Public health significance of antiviral drugssociated potential vaccine escape mutants (modified from Clementst al, 2009110). Antiviral drug-associated potential vaccine escape mu-ants (ADAPVEMs) have the potential to infect naïve but also immunizedeople and may therefore jeopardize both the antiviral treatment effi-
acy and the hepatitis B immunization program.