Embed Size (px)
Citation preview
1
The Chronic Care
2
Paradox:
We are still practicing acute care medicine in a world of chronic disease
19th century models at the dawn of the 21st century
3
Some Ideas are Just Wrong
4
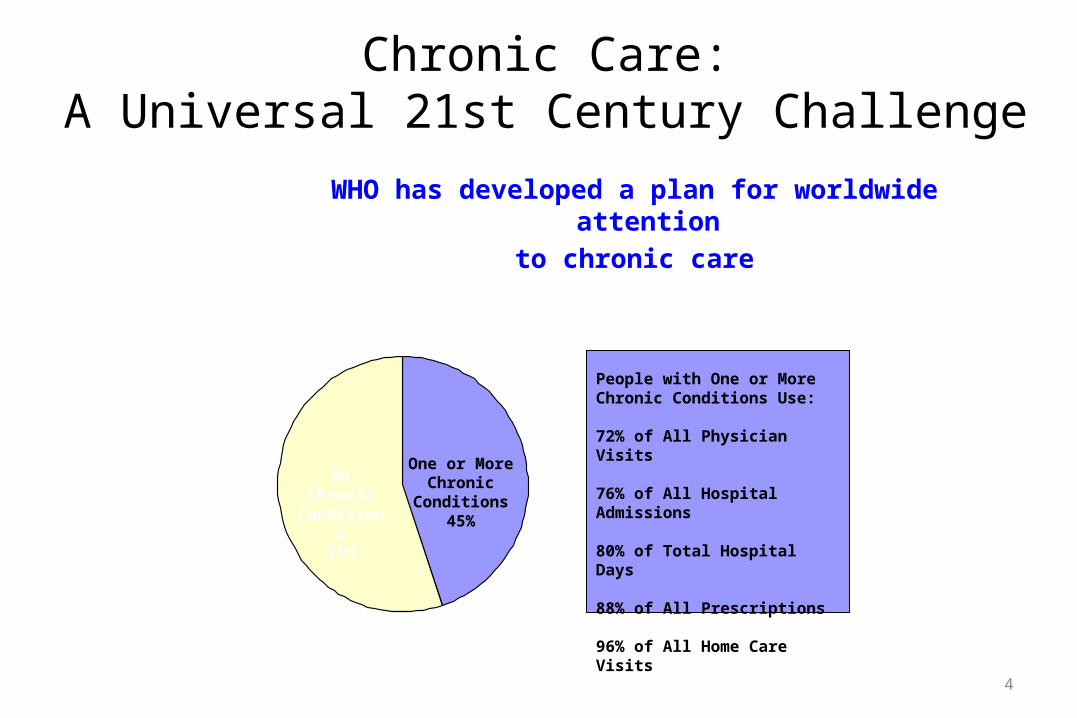
No Chronic Conditions
55%
One or MoreChronic
Conditions45%
People with One or More Chronic Conditions Use:
72% of All Physician Visits
76% of All Hospital Admissions
80% of Total Hospital Days
88% of All Prescriptions
96% of All Home Care Visits
Chronic Care:A Universal 21st Century Challenge
WHO has developed a plan for worldwide attention to chronic care
5
II. The Chronic Care Model
6
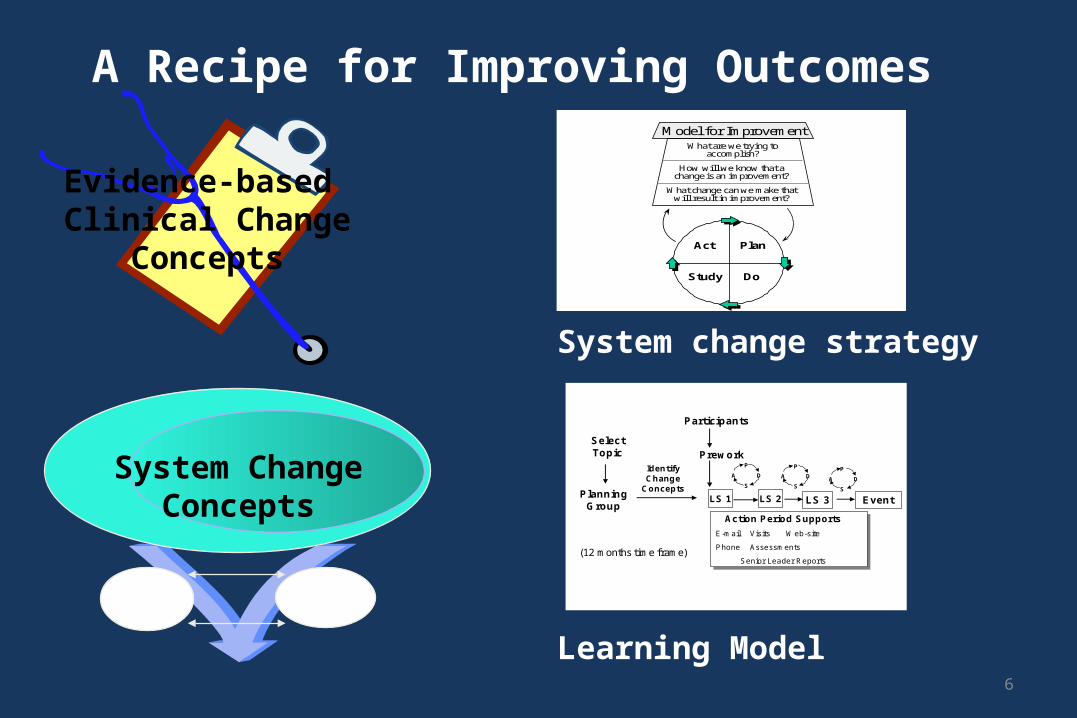
Evidence-basedClinical Change
Concepts
A Recipe for Improving Outcomes
Learning Model
System ChangeConcepts
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
System change strategy
Select Topic
Planning Group
Identify Change
Concepts
Participants
Prework
LS 1
P
S
A D
P
S
A D
LS 3LS 2
Action Period Supports
E-mail Visits Web-site
Phone Assessments
Senior Leader Reports
Event
A D
P
S
(12 months time frame)
7
System Change ConceptsWhy a Chronic Care Model?
• Emphasis on physician, not system, behavior.
• Characteristics of successful interventions weren’t being categorized usefully.
• Commonalities across chronic conditions unappreciated.
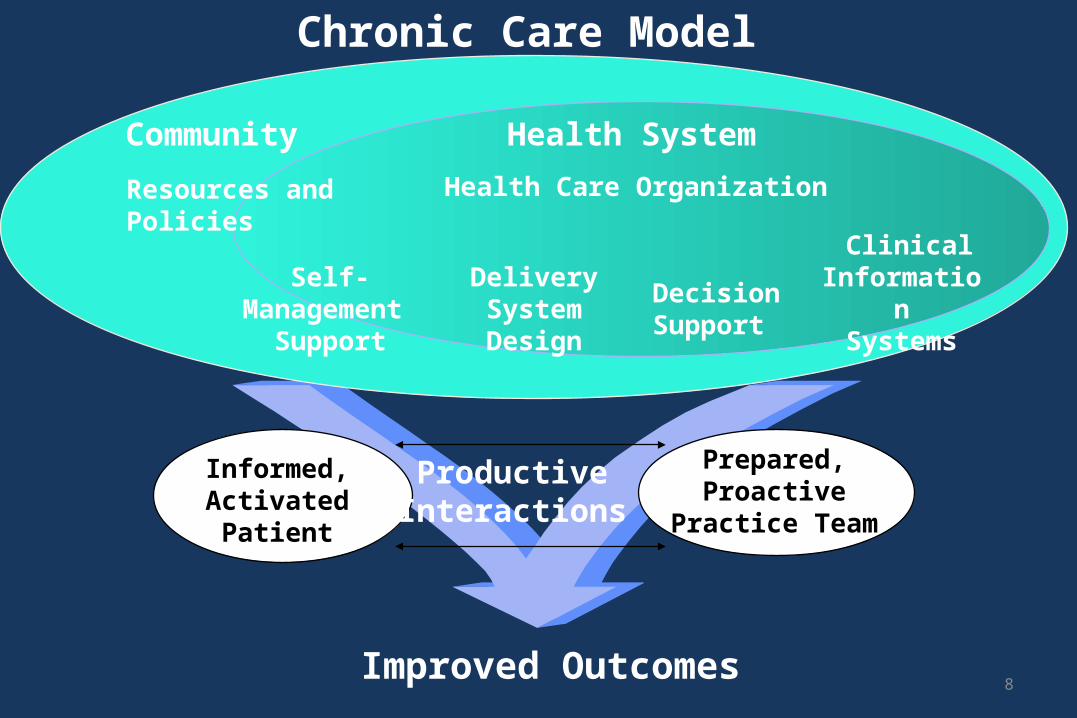
8
Informed,Activated
Patient
ProductiveInteractions
Prepared,Proactive
Practice Team
DeliverySystemDesign
DecisionSupport
ClinicalInformation
SystemsSelf-
Management Support
Health System
Resources and Policies
Community
Health Care Organization
Chronic Care Model
Improved Outcomes
9
Essential Element of Good Chronic Illness Care
Informed,Activated
Patient
ProductiveInteractions
PreparedPractice
Team
Productive means that the work of evidence-based chronic disease care gets done in a systematic way, and patient needs are met.
10
What characterizes an “informed, activated patient”?
Informed,Activated
Patient
They have the motivation, information, skills, and confidence necessary to
effectively make decisions about their health and manage it.
sufficient information to become a wise decision-maker related to their
illness
understanding the importance of their role in managing the
illness.
11
What characterizes a “prepared” practice team?
PreparedPractice
Team
At the time of the interaction they have the patient information, decision support, and
resources necessary to deliver high-quality care.
organized, trained, and equipped to
conduct productive interactions
12
• Assessment of self-management skills and confidence as well as clinical status.
• Tailoring of clinical management by stepped protocol.• Collaborative goal-setting and problem-solving resulting
in a shared care plan.• Active, sustained follow-up.
Informed,Activated
Patient
ProductiveInteractions
PreparedPractice
Team
How would I recognize aproductive interaction?
productive interaction is one that assures that patient needs for evidence-based clinical and behavioral care information and support to become better self-managers, and monitoring over time are met.
13
Productive Interactions
Informed, Activated
Patient and Caregiver
Prepared, Proactive
Practice Team
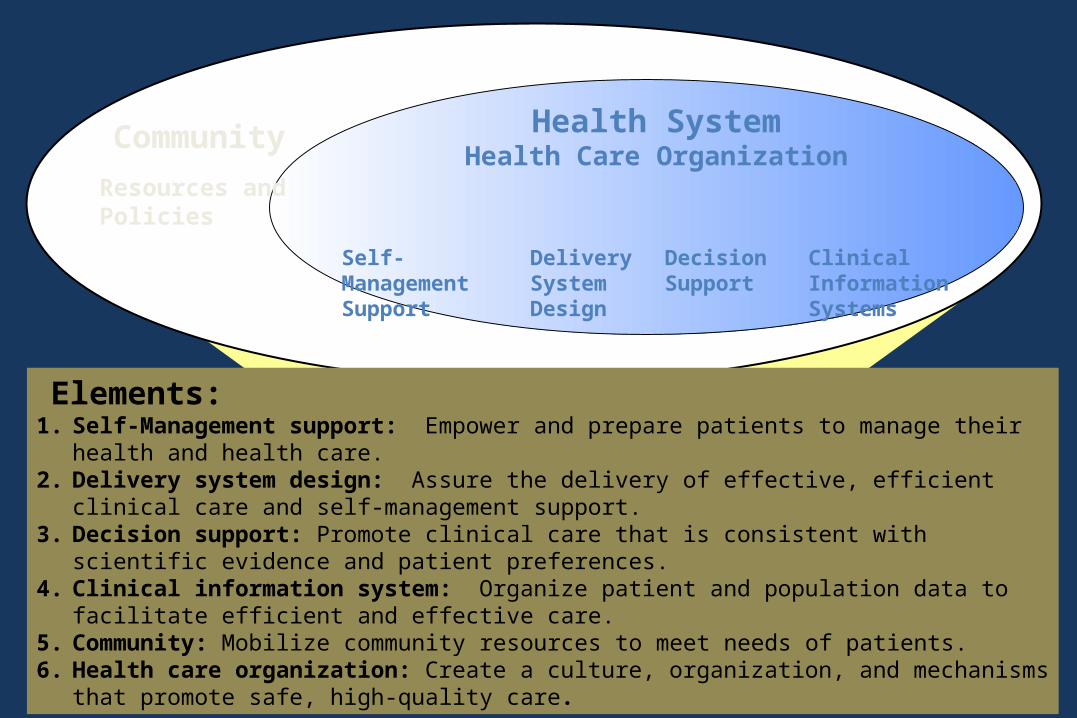
Health SystemHealth Care Organization
Self-Management Support
Delivery System Design
Decision Support
Clinical Information Systems
Community
Resources and Policies
Improved OutcomesWagner, 1996
Elements:1. Self-Management support: Empower and prepare patients to manage their health
and health care.2. Delivery system design: Assure the delivery of effective, efficient clinical care and
self-management support.3. Decision support: Promote clinical care that is consistent with scientific evidence
and patient preferences.4. Clinical information system: Organize patient and population data to facilitate
efficient and effective care.5. Community: Mobilize community resources to meet needs of patients.6. Health care organization: Create a culture, organization, and mechanisms that
promote safe, high-quality care.
What Are Chronic Diseases?>A chronic disease persistent or recurring disease,
usually affecting a person for three months or longer.
• are non communicable illnesses that are prolonged in duration, do not resolve spontaneously, and are rarely cured completely.
Chronic disease vs Chronic illness
• often used interchangeably in the clinical literature and in health services policy and organization, they convey different meanings;
• Chronic disease is defined on the basis of the biomedical disease classification, and includes diabetes, asthma, and depression.
• Chronic illness is the personal experience of living with the affliction that often accompanies chronic disease. It is often not recognized in health systems, because it does not fit into a biomedical or administrative classification.
15
16
Components of Chronic Disease Care
• Patient experience of care• Care delivery teams• Organizations within which
delivery teams and patients interact
• Regulatory and payment environment
17
Some Ideas Need More Thought
18
Characteristics of Chronic Disease:
• Last a lifetime• Accumulate with age• Generally progressive• Life-shaping • Different meaning in different cultures
19
Goals of Chronic Disease Care
1. Manage the disease to reduce exacerbations.2. Prevent the transition from impairment to disability, and
from disability to handicap.3. Encourage patient to play an active role in managing
his/her disease but avoid allowing the disease to dominate the person’s life.
4. Provide care in a culturally sensitive manner.5. Integrate medical care with other aspects of life without
medicalizing those aspects.
Case Study
• Terri Schiavo CaseReflection:a. If you were Terri Schiavo’s husband what will be your decision on the case of
your wife?b. Is the family of Terri Schiavo selfish ?c. Did the US supreme court made the right decision?d. Discuss the case of Terri Schiavo using the CCM (Chronic Care Model)
20
21
A Lot Depends on Interpretation

22
23
What is involved
• New definitions– Prevention– Patients’ roles– Time– Place
• New approaches– Professional roles– Expectations– Information technology– Management
24
Definitions: Prevention
• Prevent exacerbations
• Reduce expensive utilization
• Prevent dysfunction
• Avoid iatrogenic effects
25
Definitions: Patients’ Roles
• 365/24/7– Shared responsibility– Shared risk
• Ongoing communication
• Shared decision making– Need better information– Need time
26
Definitions: Time
• Episode vs. Encounter• Pay-off horizon
– Up-front investment recovered over time• Manage by change, not routine
– Scheduling appointments– Length of appointments
27
Definitions: Place
• Chronic care occurs across locations• The same care can be provided in different settings
28
What is involved
• New definitions– Prevention– Patients’ roles– Time– Place
• New approaches– Professional roles– Expectations– Information technology– Management
29
New Approaches: Professional Roles
• Downward delegation– non-physicians– non-professionals
• Primary care– simple cases– complex cases
• New teams– Specialists, nutritionist & therapist
30
New Approaches: Expectations
• Cure vs. Management
• Measuring success– actual vs. expected
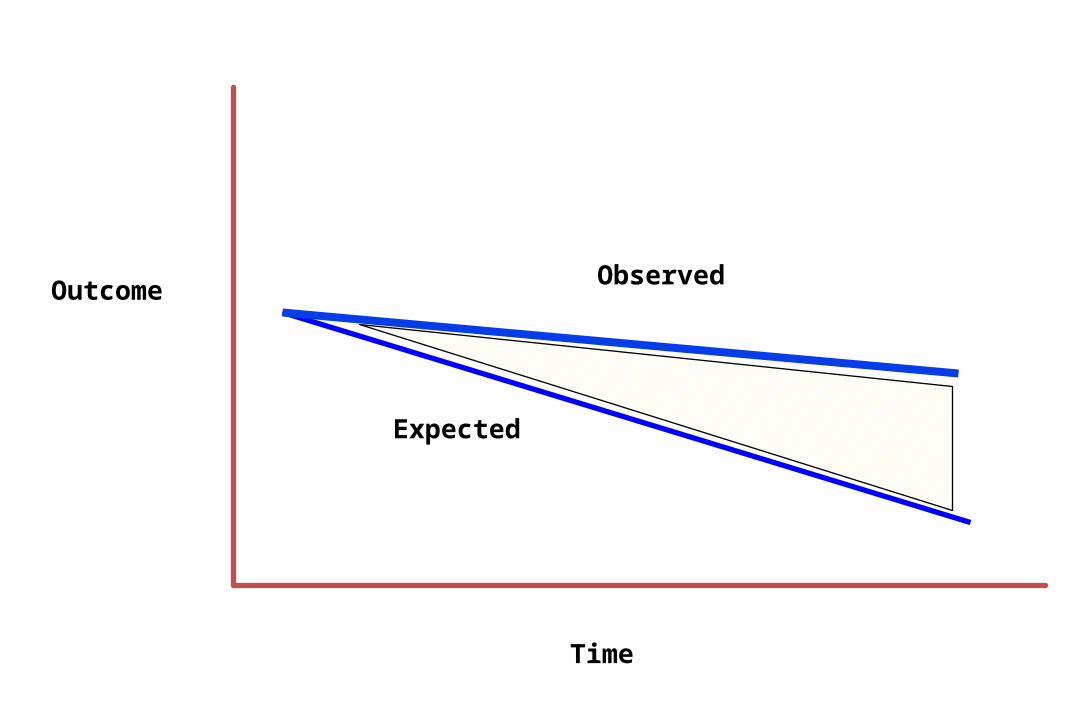
Observed
Expected
Outcome
Time
32
New Approaches: Management
Case Management Variations• Eligibility management – not all health practitioner
not all patient• Care coordination – all areas are involved• Utilization management – proper resources
proper patient• Disease management
– Often independent– Targeted
• Chronic care management -
33
34
New Approaches: Management
• Patient self-care – Education– Motivation– Attitudinal change
• Nurse-patient partnerships– Information based– Patient empowering
35
New Approaches: Information Technology
Problems with too much as well as too little information.Need to focus provider & patient attention on salient data
• Just in time information
• Structured information– Clinical glidepaths

36
Need Relevant Information
37
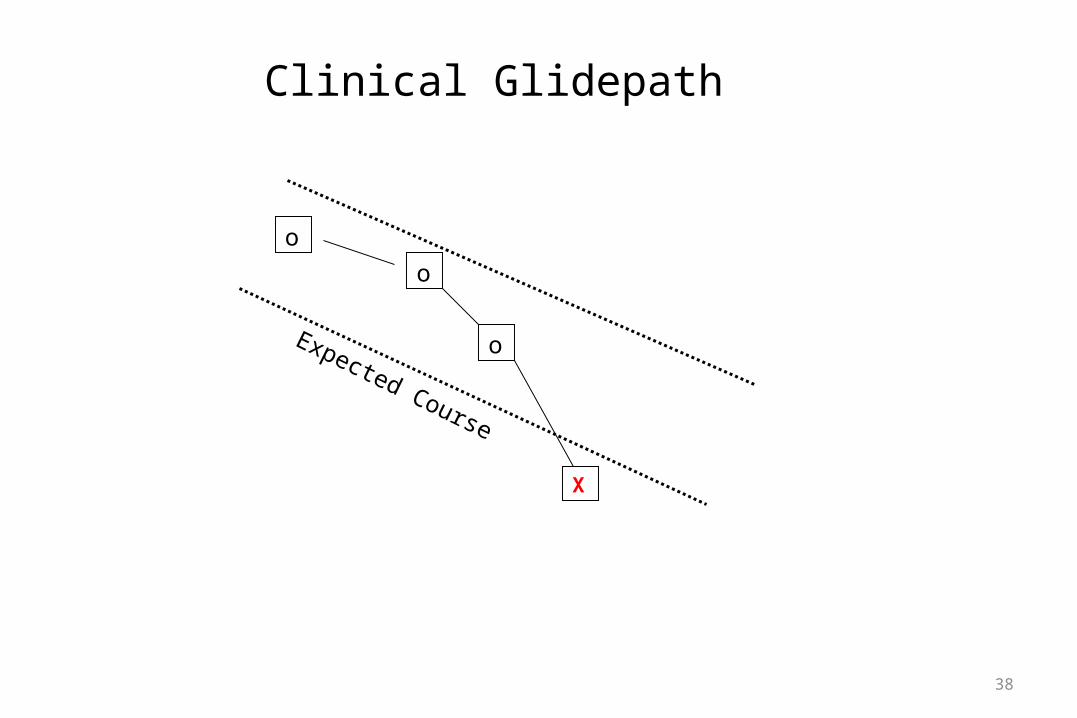
Clinical Glidepath• A CLINICAL GLIDEPATH is a way to observe one or more
parameters of a patient’s condition on a regular basis to be able to compare the observed state with the expected state.
• It is a tool to improve communication between patients and primary care providers.
• If the patients stays within the expected course, nothing need be done.
• But if the patient’s clinical course deviates, this change should trigger immediate closer attention to ward off a problem while it is early.
38
o
o
o
X
Clinical Glidepath
Expected Course
39
Strategies for Improving Chronic Disease Care
• Interdisciplinary team care• Group care – nurses or doctors• Information systems
– Electronic medical record– Computerized physician order entry– Clinical tracking systems
• Mobile computing
40
Evidence of Success
• Some encouraging signs but no clear trend• Increased clinic visits and reorganization associated with
fewer hospitalizations and urgent care visits in;
COPD DiabetesPneumonia Chronic renal failureCHF DepressionAngina
Ashton, NEJM, 2003
41
Quality care related to better survival among vulnerable older patients
Higashi, Ann Int Med, 2005
Self-management programs for diabetes and hypertension improve outcomes
Chodosh, Ann Int Med, 2005
Medication adherence reduces hospitalizations for diabetes, hypertension, hypercholesterolemia and CHF
Sokol, Med. Care, 2005
42
“The prevailing evidence appears to be that while disease management programs improve adherence to practice guidelines and lead to better control of the disease, their net effects on health care costs are not clear.”
CBO, 2004
43
Payment Issues• Providers expect to be paid for what they do• Who will invest in primary care• Medicare (PHILHEALTH)
– Expand coverage to include new services• Monitoring• Counseling
– Share savings from decreased inpatient/ER utilization– Pay more per visit for fewer visits– Pay for episodes instead of incidents– Pay for outcomes
44
Conclusions
• Chronic disease is here to stay• More must be done to bring the health care system into
alignment• There is good scientific evidence to show better care is
possible• Managed care does not seem to be the magic carpet
– If managed care is to have any success, need better case mix payment system
• Changing the payment system is necessary but not sufficient
45
How You Implement Is Important





























