Embed Size (px)
Citation preview

Basics of IPC
Ministry of InteriorSECURITY FORCES HOSPITAL
MAKKAH
Prepared by:Dr. Ahmed Farouk
MD,EBFM,MRCGP,CICIPC Team Manager- SFHPM

Objectives:• How chain of infection work ?
• How to break the chain of infection ?
• Dangerous message about hand hygiene
• What is meant by the standard precautions?
BASICS OF IPC

• What is meant by transmission based precautions & how to implement?
• How can we deal with biological spills?
• How can we deal with any occupational exposure to patient blood or body fluids
• What is meant by medical waste cycle
BASICS OF IPC

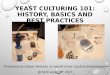
CHAIN OF INFECTION

Agent
Reservoir
Place of Exit
Mode of Transmissio
n
Place of Entry
Susceptible Host


ISOLATION PRECAUTION

8
TYPES OF PRECAUTIONS
1. Standard precaution
2. Transmission Baseda) Contact precautionb) Droplet precautionc) Airborne precaution
3. Protective environment
SFHM-IPC

9
STANDARD PRECAUTION
Definition: IC practices that should be applied to all
patients regardless of suspected or confirmed diagnosis

SFHM-IPC 10
STANDARD PRECAUTION
Hand Hygiene PPE Cough Etiquette Pt. Placement
Pt. Care Equipment Safe Injection HK Linen Management
Lumbar puncture Infectious Waste Worker’s Safety

HAND HYGIENE

If you could see the germs
you’d wash your hands

HAND WASHING

INDICATIONS OF HAND WASHING
• Visibly dirty or contaminated hands with proteinaceous material, blood or other body fluids
• After caring for patients with diarrhea, including Clostridium Difficile associated diarrhea
• Before handling/preparing/ eating food
• After use of the toilet

Hand Washing Technique (40-60 Seconds)
1- Wet hands with warm water & apply enough liquid soap & rub palm to palm
بلل اليدين بالماء الدافئ -1والصابون السائل ثم دلك
باطن اليدين ببعضهما
2- Right palm over left dorsum with interlaced fingers and vice versa
دلك باطن اليد اليمنى على -2ظاهر اليد اليسرى ثم بالعكس
مع جعل االصابع متداخلة
3- Palm to palm with interlaced fingers
دلك باطن اليدين ببعضهما -3 واالصابع متداخلة
4 - backs of fingers to opposing palms with fingers interlocked & vice versa
دلك ظاهر االصابع بباطن اليد -4االخرى مع االمساك باالصابع ثم
العكس
5- Rotational rubbing of left thumb clasped in right palm and vice versa
قم بالدعك الدائرى لkالبهام االيسر -5ممسوكا بباطن اليد اليمنى ثم
العكس
6- Finally finger tips to clean center of palms by rotational rubbing & vice versa then rinse under running water ,dry hands by clean tissue & close the faucet with the drying tissue
أخيرا قم بالدعكk الدائرى لباkطن -6اليد اليمنى باطراف اصابع اليد
اليسرى ثم بالعكس ثم شطف اليدين بالماء الجارى ثم التنشيف باستخدام
مناشف ورقية ثم غلق الصنبور بها
Whenever hands visibly soiled

HAND RUB

INDICATIONS OF ALCOHOL HAND RUB
• All the times for hand hygiene except when hands are soiled (alcohol does not act on microbes in presence of dirt)

Alcoholic Hand Rub Technique (20-30 Seconds)
1- Apply Enough Amount of alcohol & rub palm to palm
ضخ كمية كافية من الكحول -1 ودلكk باطن اليدين ببعضهما
2- Right palm over left dorsum with interlaced fingers & vice versa
دلك باطن اليد اليمنى على -2ظاهر اليد اليسرى ثم بالعكس
مع جعل الصابع متداخلة
3- Palm to palm with interlaced fingers
دلكk باطن اليدين ببعضهما -3 واالصابع متداخلة
4 - backs of fingers to opposing palms with fingers interlocked & vice versa
دلك ظاهر االصابع بباطن اليد -4االخرى مع االمساك باالصابع ثم
العكس
5- Rotational rubbing of left thumb clasped in right palm and vice versa
قم بالدعك الدائرى لkالبهام االيسر -5ممسوكا بباطن اليد اليمنى ثم
العكس
6- Finally finger tips to clean center of palms by rotational rubbing & vice versa until dryness
أخيرا قم بالدعكk الدائرى لباkطن -6اليد اليمنى باطراف اصابع اليد
اليسرى ثم بالعكس حتى تجف بدون استخدام اى مناkشف

ADVANTAGES OF ALCOHOLIC HAND RUB OVER HAND WASH
• Reducing the microorganisms count on hands better than antimicrobial soap
• Easier to use
• Quicker to use
• Side effects negligible: AHR leave skin in better condition


NOTICE ON PRACTICES OF HAND HYGIENE
• Alcohol gel should not be used with antimicrobial soap concomitantly.
• Soiled hands should not be cleaned by Alcohol, it must be cleaned with hand washing.
• Hands must be washed after caring for diarrhea patients.
• Hot water must be avoided when washing hands, as repeated exposure to hot water may increase the risk of dermatitis.

THE 5 MOMENTS

23
SURGICAL HAND PREPARATION

PERSONNEL PROTECTIVE EQUIPMENT
PPE

25
Indications
Sterile gloves Non-sterile gloves Utility gloves• Before surgery• Before any invasive procedure that require aseptic technique.• Before wound dressing.• Mixing I.V. fluids and using multidose vials.
• When starting I.V lines or performing phlebotomy.• When changing or handling dressings.• When cleaning or handling soiled equipment or instruments.• When handling specimens and their containers.
• When handling medical waste.• When cleaning up spills of blood or body fluids.• When using chemicals
GLOVE USE

26
Over head Aprons & Gowns Face, and Eye Protection
Disposable caps should be worn to confine
and contain hair during surgical procedures.
Use plastic aprons or gowns should be used during procedures that are likely to generate splashes of blood or
body fluids.
When there is risk of splashes or sprays of blood or body fluids into the face
and eyes of HCP.
SFHM-IPC
P.P.E

• Use a surgical mask alone when there is risk of exposure to droplets that might contain infectious agents. e.g. Neisseria meningitidis, Bordetella pertussis, and influenza virus.
• For airborne infectious agents such as M. tuberculosis a high filtration respiratory protective device is ideal (e.g. N95).
RESPIRATORY PROTECTION

COUGH ETIQUETTE

او • الس777777عال عن777777دبتغطي77ة ق77م العط77سبمندي77ل وفم77ك انف77ك
ورقىس7لة • ف7ى منديل7ك ض7ع
المهمالت
• Cover your mouth and nose with tissue when you cough or sneeze
• Discard your used tissue in the waste basket
الجزء • اس7777تخدم اوك7مك من الع7لوى
يدي7777ك • التس7777تخدمعن77د االن77ف لتغطي77ة
الكحة او العطس
• Or use your upper sleeve
• Don’t use your hands to cover during coughing or sneezing
ORأو

MEDICAL WASTE MANAGEMENT

MEDICAL WASTE MANAGEMENT
Health-care medical waste is a by-product of health care that includes(e.g.):
Sharps(in the safety box)
Infective and pathological waste
Any domestic waste contaminated by blood or the patient secretions.

MOH DISEASE NOTIFICATION

SFHM-IPC 33

SFHM-IPC 34
Suspect Case (patients who should be tested for MERS-CoV)• A person with fever and community-acquired pneumonia or acute respiratory
distress syndrome based on clinical or radiological evidence.2
OR• A hospitalized patient with healthcare associated pneumonia based on clinical and
radiological evidence.2
OR• A person with 1) acute febrile (≥38°C) illness, AND 2) body aches, headache, diarrhea,
or nausea/vomiting, with or without respiratory symptoms, AND 3) unexplained leucopenia (WBC<3.5x109/L) and thrombocytopenia (platelets<150x109/L)3.
OR• A person (including health care workers) who had protected or unprotected
exposure4 to a confirmed or probable case of MERS-CoV infection and who presents with upper5 or lower6 respiratory illness within 2 weeks after exposure.7
MERS-COV CASE DEFINITION

SFHM-IPC 35
Probable Case• A probable case is a patient in category I or II above
with absent or inconclusive laboratory results for MERS-CoV and other possible pathogens who is a close contact8 of a laboratory- confirmed MERS-CoV case or who works in a hospital where MERS-CoV cases are cared for.
Confirmed Case• A confirmed case is a suspect case with laboratory
confirmation9 of MERS-CoV infection
MERS-COV CASE DEFINITION

SFHM-IPC 36

SFHM-IPC 37
EBOLA CASE DEFINITION Suspected Case• Illness in a person who has both consistent
symptoms and risk factors as follows:– Clinical criteria, which includes fever of greater than 38.6
C, and additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, or unexplained hemorrhage (gingival, nasal, cutaneous [petechiae, bruises, ecchymosis], gastrointestinal, rectal [gross or occult blood], urinary [gross or microscopic hematuria], vaginal, or puncture sites bleeding); AND

SFHM-IPC 38
– Epidemiologic risk factors within the past 3 weeks before the onset of symptoms, such as contact with blood or other body fluids of a patient known to have or suspected to have EVD; residence in—or travel to—an area where EVD transmission is active; or direct handling of dead or alive fruit bats, monkeys, chimpanzees, gorillas, forest antelope and porcupines from disease-endemic areas.
– Malaria diagnostics should also be a part of initial testing because it is a common cause of febrile illness in persons with a travel history to the affected countries.
EBOLA CASE DEFINITION

SFHM-IPC 39

SFHM-IPC 40

SFHM-IPC 41

SFHM-IPC 42

SFHM-IPC 43

SFHM-IPC 44

SFHM-IPC 45

PROTECT YOUR KIDS
DON’T TAKE BUGS WITH YOU TO HOME

SFHM-IPC 47
Any questions ?

SFHM-IPC 48