Embed Size (px)
Citation preview

Examining quality of end-‐of-‐life care from the perspec8ve of bereaved rela8ves: Development and valida8on of a postal ques8onnaire framed by na8onal standards.
Kathleen McLoughlin1, Mary Lovegrove2, Kieran McKeown2 and Andy Cochrane1 1. Department of Psychology, Maynooth University, Maynooth, Co. Kildare
2. The Irish Hospice FoundaFon, Nassau Street, Dublin 2.
Background: High quality end-‐of-‐life care can make a significant difference to the physical, psychological and spiritual outcomes for the bereaved, conversely, when care is poor, it can have a detrimental impact. The Office of the Ombudsman in Ireland recently published a themaCc collecCon of complaints received regarding end of life care focusing on the need for improvement with regard to communicaCon, paCent autonomy, access to specialist palliaCve care, support for families and friends, post-‐mortem examinaCons, returning the deceased person’s belongings and management of complaints. These elements are all central features of the Quality Standards for End of Life Care in Hospitals and NaConal Standards mandated by the Health InformaCon and Quality Authority within their focus on improving the quality of care for people generally and at end of life. In Ireland, there is no agreed, validated tool to examine the quality of end-‐of-‐life care against published standards. The complexiCes associated with evaluaCng the quality of care from a dying paCent’s perspecCve have been well documented internaConally and hearing the voice of bereaved relaCves is considered a reasonable proxy and an important component of a quality and risk approach. In 2011/2 The Hospice Friendly Hospitals (HFH) programme and the HSE PalliaCve Care Clinical Programme developed a pilot NaConal End of Life Care Audit and Review System, that included a survey of bereaved relaCves intended for use as a normal part of the quality improvement process in all care seVngs where people die in Ireland. Aim: To describe the process used to develop and validate a survey of bereaved relaCves to assess the quality of end of life care in all seVngs where people die.
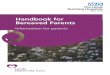
Design: The tool was developed in four disCnct phases (Figure 1). SeBng: The pilot was conducted in acute hospitals (n=4) and residenCal care services for older people (n=10).
Results: CogniCve tesCng revealed that the quesConnaire was considered to be an appropriate length, taking on average 20 minutes to complete. All parCcipants were able to complete the quesConnaire and did not find it burdensome or too distressing. ParCcipants welcomed the survey and two recommended that it should become a rouCne part of service delivery following the death of a person in a healthcare seVng. Audit mangers reported that the process of extracCng the bereaved relaCves contact details, checking whether they could be contacted with both the clinical team and local complaints management personnel, making the call and sending out documentaCon was a very Cme consuming process, taking approximately 45-‐60 minutes per parCcipant. Phone calls were someCmes difficult, with people taking the opportunity to “tell their story” over the telephone and in a small number of cases, people refused to engage in the study but gave their feedback over the telephone. It was suggested that clear, robust procedures are required to process and manage the feedback given over the phone by bereaved relaCves who do not choose to engage with the survey. Of the 120 bereaved relaCves who were invited to parCcipate in the pilot run, 59 (49.2%) responded. 36 (61.0%) were recruited via an acute hospital and 23 (39.0%) from a residenCal care service for older people. There was generally weak levels of agreement between staff and relaCves on most items of the survey with weak – no agreement on most items except the single room.
Conclusions: The tool is the first instrument to specifically assess the quality of end of life care against naConal standards in Ireland and has demonstrated both acceptability and feasibility, with good face and content validity, clarified by the logical, pragmaCc approach to tesCng adopted in this study. QualitaCve findings were of greatest interest to staff and had most potenCal to drive quality improvement locally. The significant disagreement in findings between staff and bereaved relaCves is interesCng and highlights the different perspecCves of relaCves and staff which themselves reflect different subjecCve understandings and experiences of the person who is also a paCent and the quality of care delivered. Whilst evidence suggests that proxies can reliably report on the quality of services, and on observable symptoms. Agreement is usually poorest for subjecCve aspects of the paCent's experience, such as pain, anxiety and depression, as was the case in this study. These differences are natural and inevitable which is why they are reflected in our objecCve measurements of quality. For that reason, these differences are useful in the assessment of quality but not necessarily useful in assessing validity and reliability of the tools in quesCon. Further studies are
Phase 3: Wider Audience Review
Aim: To provide support for face and content validity
!
Phase 4: Pilot with bereaved relatives, Cognitive interviews, comparison survey results with staff review tool and audit manager feedback Aim: To provide support for face and content validity and to examine reliability and feasibility
Questionnaire circulated to the Specialist Palliative Care Clinical Programme (n=19). Feedback was invited and collated. Amendments made as necessary
Questionnaire distributed using an agreed procedure (n= 120). Response rate of 49.2% (59/120). Cognitive testing (n=2) and cognitive interviews (n=3) conducted. Findings from bereaved relatives survey compared with findings from staff review tool (n=53). Findings from audit managers (n=10) regarding the process of recruitment obtained from focus groups (n=2).
Phase 1: Question Formulation
Aim: To generate potential questions representing quality of end of life care for the person and family
Phase 2: Expert Advisory Committee Review
Aim: To achieve consensus regarding which questions and domains to include for the draft survey
Final Advisory Committee Meeting
Aim: Final review before wider use and approval of alterations based on pilot findings
Survey of Bereaved Relatives
Questions based on quality of care domains in literature, outcome of the National End of Life Audit 2008/9 and key areas in published standards
An expert advisory group of 23 members reviewed potential questions via email and a meeting was called to achieve consensus regarding content, and wording of questions.
Draft Questionnaire Developed
Expert advisory committee meeting to agree final version of questionnaire for inclusion in the National End of Life Audit and Review System after incorporation of changes from the pilot with opportunity for review and comment.