Embed Size (px)
Citation preview
BRONCHOPNEUMONIA
LINTU THOMASMSC NURSING II YR

• INTRODUCTION
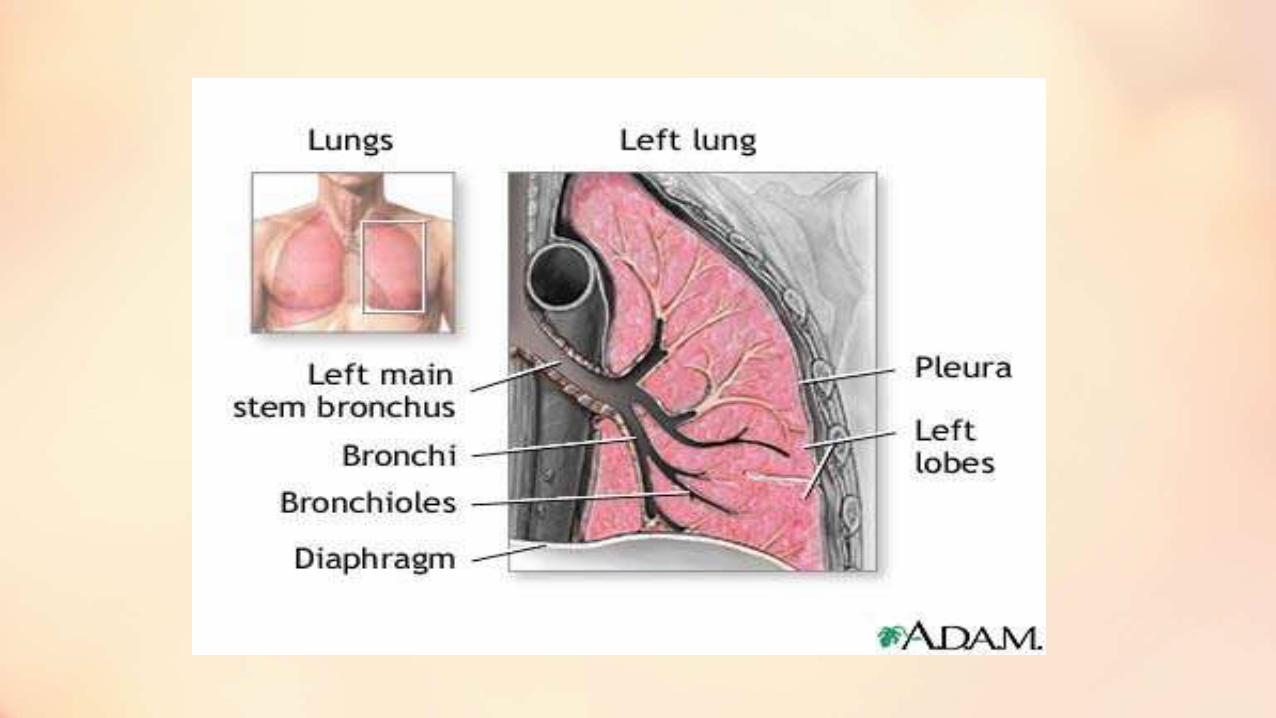
• DEVELOPMENTAL ANATOMY
at the of 4 weeks ,the respiratory system begins as an out growth of the foregut ,it is anterior to the pharynx ,the out growth is called Lung bud or Respiratory diverticulum
• The endoderm lining the respiratory diverticulumgive rise to the epithelium and glands of the trachea ,bronchi and alveoli
•Mesoderm surroundings the respiratory diverticulum give rise to connective tissue ,cartilage and smooth muscles of these structures
•Respiratory diverticulum elongates and form tracheal buds divides into bronchial buds ,which branches repeatedly and develop with bronchi .by 24 weeks respiratory bronchioles have developed
•At 6 -16 weeks all major elements of lungs have formed .
•Gas exchange started
•During 6 to 26 weeks lung tissue become vascular ,repiratory bronchioles ,alveolar ducts ,some
• 20 weeks surfactant production started very small amount .
• Sufficient amount produced at 26 to 28 weeks of gestation
•At 30 weeks mature alveoli will develop
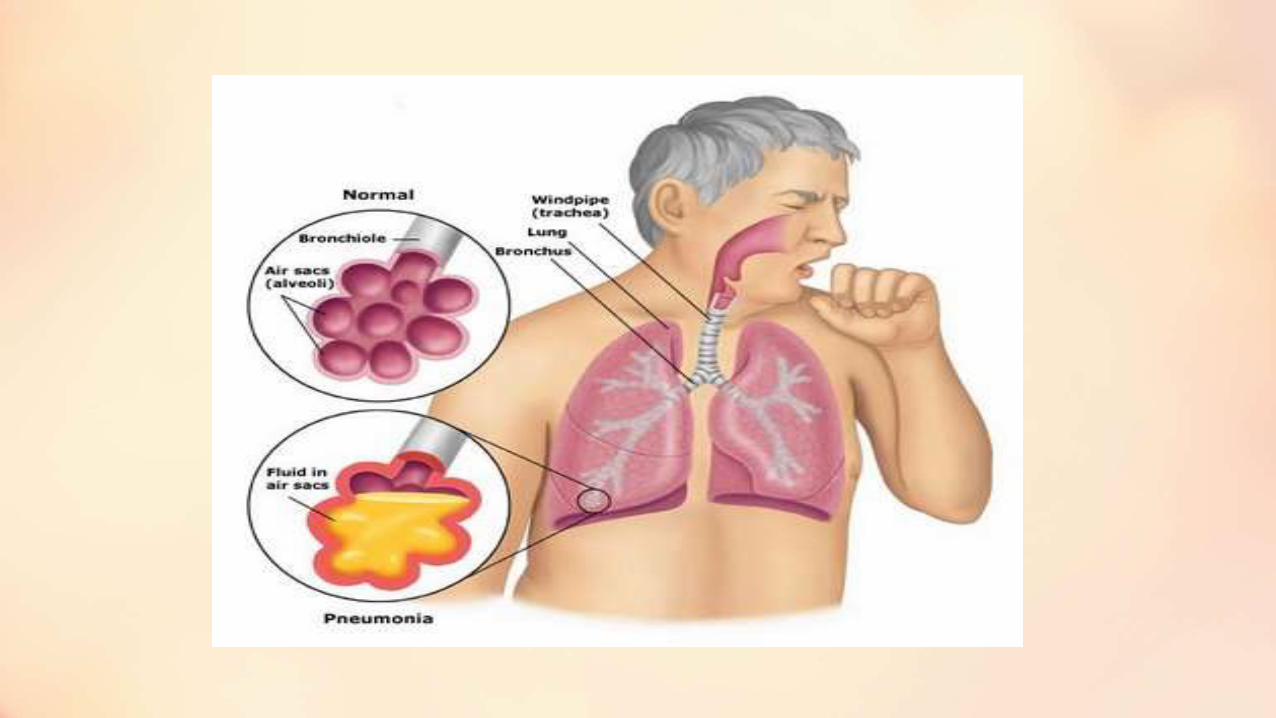
DEFINITION
• PNEUMONIA
IT IS AN INFLAMMATORY PROCESS INVOLVING LUNG PARENCHYMA
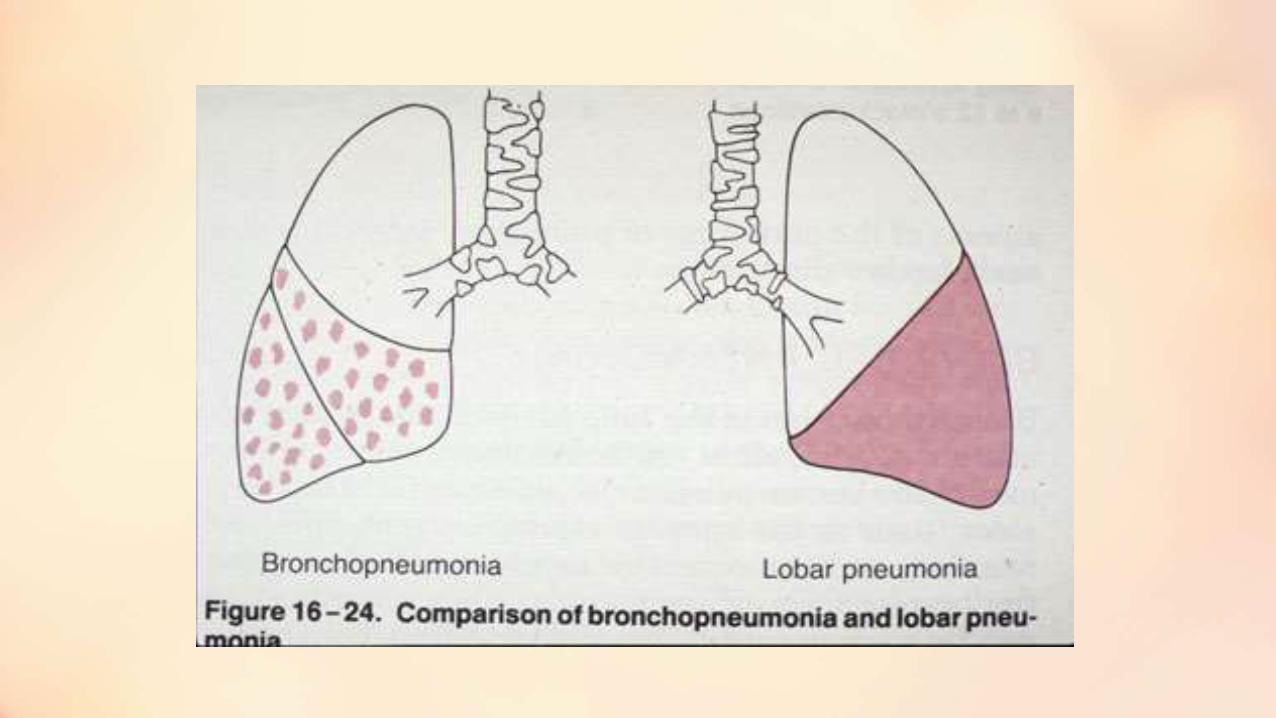
BRONCHOPNEUMONIA
IT IS PRIMARILY SPREADING INFLAMMATION OF A TERMINAL BRONCHIOLES AND THEIR RELATED ALVEOLI

•CLASSIFICATION OF PNEUMONIA
INCIDENCE
• IT IS SEEN IN AROUND 156 MILLION PEOPLE
,MORE SEEN IN CHILDRENS THAN ADULT
,28-34 % DEATH UNDER 5 YEARS ,
ETIOLOGY
• BACTERIAL INFECTION
Pneumococcus ,streptococcus ,staphylococcus ,
H .influenza
• Viral infection :influenza virus, adenovirus
• Fungus: Candida, Histoplasma
• Hypostatic pneumonia
• Aspiration of amniotic fluid ,food ,foreign bodies
PNEUMONIA PATOGENS IN VARIOUS AGE GROUP
• 1-3 Months :Parainfluenza ,Influenza ,Streptococcus Pneumoniae ,Chlamydia Trachomatis
• 4 Months To 5 Years :Streptococcus Pneumoniae,Chlamydia Pneumoniae ,Mycoplasma Pneumoniae
• 5 To 18 Years : Mycoplasma Pneumoniae ,ChlamediaPneumoniae ,Steptococcus Pneumoniae
CLINICAL FEATURES OF BRONCHOPNEUMONIA• High fever with respiratory distress ,restlessness , air hunger
and cyanosis
• Grunting
• Nasal flaring
• Retraction of the supra clavicular ,intercostals ,subcostal areas
• Tachypnea
• Tachycardia
• Abdominal distention ,liver enlargement
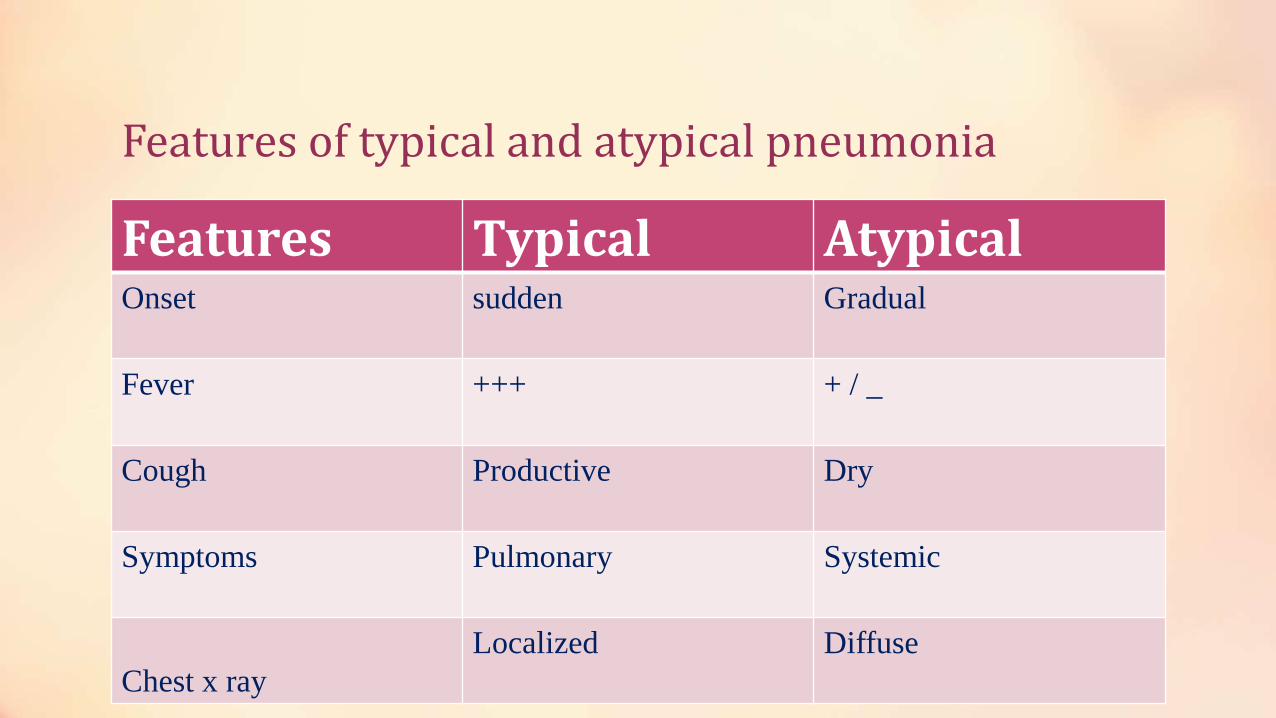
Features of typical and atypical pneumonia
Features Typical Atypical Onset sudden Gradual
Fever +++ + / _
Cough Productive Dry
Symptoms Pulmonary Systemic
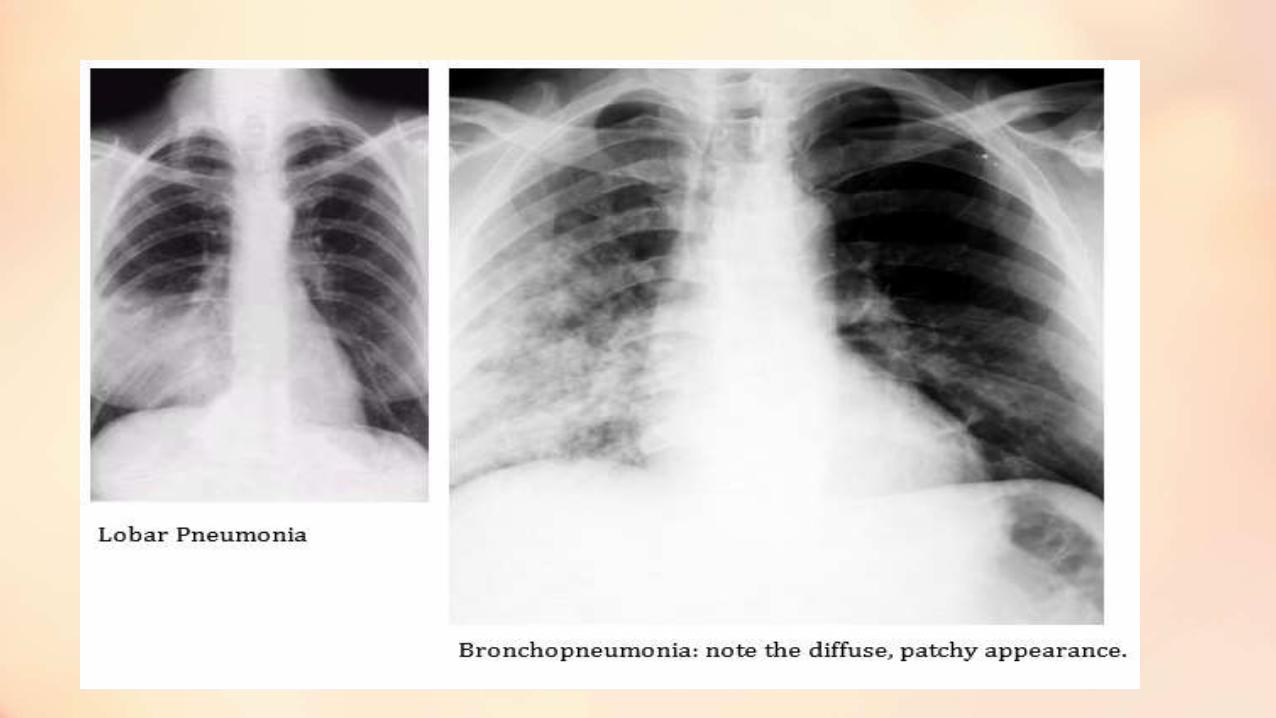
Chest x ray
Localized Diffuse
Diagnostic evaluation of bronchopneumonia
• PHYSICAL EXAMINATION
INSPECTION
Cyanosis ,sub costal ,substernal ,intercostal retraction ,tachypnea ,nasal flaring
AUSCULTATION
Wheezes Sound
PERCUSSION
Dullness over a consolidated area
PALPATION
LABORATORY AND DIAGNOSTIC TESTS
• Pulse Oxymetry
•Chest X Ray
• Sputum Culture
•Blood Examination
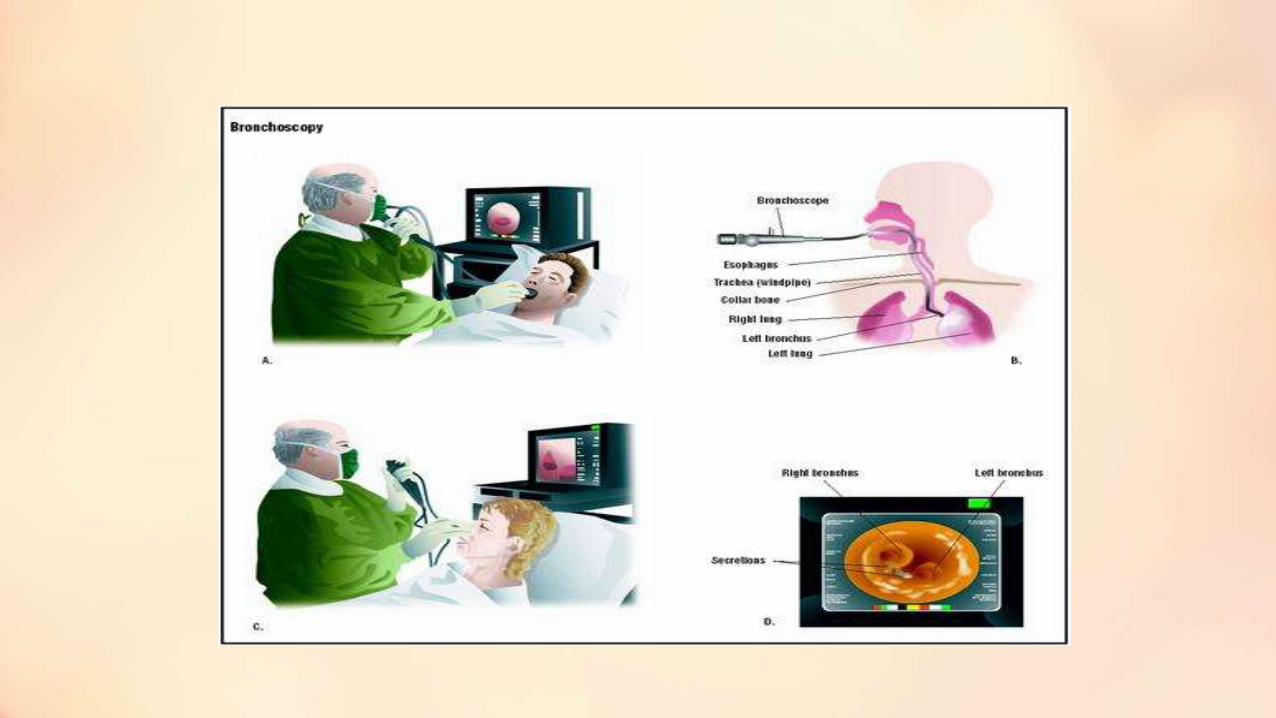
•Bronchoscopy
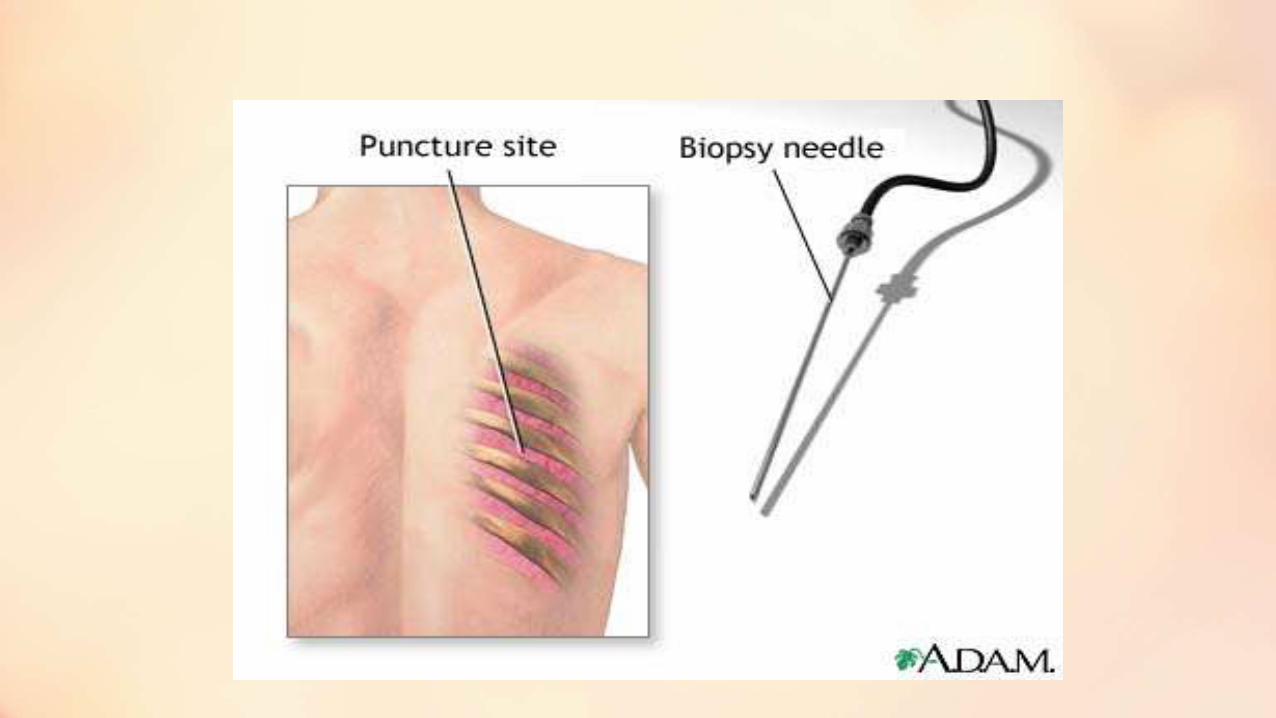
• Lung Biopsy
• Lung Aspiration

MANAGEMENT
• PNEUMOCOCCAL PNEUMONIA
• Penicillin G 50,000 units /kg/day ,IV OR IM ,for 5-7 days
• Procaine penicillin 600,000 units IM/DAY
• Allergic to penicillin alternative amoxicillin or ampicillin,the alternatives are ceftrioxone /cefotaxime
•Oxygen administration
• STAPHYLOCOCCAL PNEUMONIA
• Isolation of patient
•Antipyretics for fever
•Maintain hydration with 5% dextrose
•Antibiotics therapy (penicillin ,erythromycin ,cephalosporin)
•Patient not respond soon vancomycin can use
•Hemophilus pneumonia
•Ampicillin 100 to 150 mg /kg /day and chloramphenicol 50 mg /kg /day in a four divided dose
•Cefotaxime 100 mg/kg /day or ceftrioxone 70 mg/kg /day are alternatively in seriously ill patient
• Streptococcal pneumonia
• Penicillin G 50,000 to 10000 units /kg/day for 7 to 10 days
Supportive care
Antipyretics for fever
Oxygen administration
Maintain hydration with iv fluid
Maintain position

• NURSING CARE MANAGEMENT
HOME CARE MANAGEMENT
• Increase oral intake
• Provide adequate bed rest
• Frequently check temperature
• Maintain position
• Give antipyretics to reduce fever
• High humid atmosphere
• Regular follow up

DIET
Complication
•Bactermia
• Sepsis
•Breathing problem
• Lung abscess
•Respiratory distress syndrome
• Pleural thickening
Nursing diagnosis
• Ineffective airway clearances related to inflammation, increased secretions ,mechanical obstruction as evidenced by presences of secretion ,productive cough ,tachypnea
• Ineffective breathing pattern related to inflammation as evidenced by tachypnea ,increased work of breathing
• Impaired gas exchange related to hyperinflation airway plugging as evidenced by cyanosis ,decreased oxygen level and alteration in blood gases
•Risk for infection related to presences of infectious organism as evidenced by fever or presences of viruses or bacteria on laboratory screening
•Activity intolerances related to high respiratory demand as evidenced by increased work of breathing
• Fluid volume deficit related to decreased oral intake
•Altered nutritional status less than body requirement related to feeding difficulty as evidenced by poor oral intake
• Fear related to difficulty in breathing ,unfamiliar situation ,procedures as evidenced by crying ,clinging and lack of co operation

Prognosis

THANK YOU