Embed Size (px)
Citation preview

BUILDing Multi-Sector
Collaborations to Advance
Community Health
• Peter Eckart, Co-Director, Data Across Sectors for Health (DASH); Director for Health Information and Technology, Illinois Public Health Institute
• Alison Rein, Director, Community Health Peer Learning Program (CHP); Senior Director, Evidence Generation and Translation, AcademyHealth
• Gretchen Benson, Manager, Healthcare Systems Integration, Minneapolis Heart Institute Foundation
• Rebecca Lindberg, Director, Population Health, Minneapolis Heart Institute Foundation
• Stephanie Fenniri, Senior Community Partnerships Manager, Parkland Center for Clinical Innovation

All In: Data for Community Health
1. Support a data movement that empowers communities to address social determinants of health
2. Build an evidence base for the field of multi-sector data use to improve health
3. Stimulate and support peer learning and collaboration
DASH and CHP are All In!
Community Health Peer Learning Program (CHP)
NPO: AcademyHealth, Washington DC; with National Partnership for Women & Families and NORC as partners
Funded by the Office of the National Coordinator for Health IT
15 communities: 10 Participant and 5 Subject Matter Expert
Data Across Sectors for Health (DASH)
NPO: Illinois Public Health Institute in partnership with the Michigan Public Health Institute
Funded by the Robert Wood Johnson Foundation
10 communities

DASH and CHP Theory of Change
Shared data and
information
Multi-sector
Collaboration
Outcome:
Capacity Building to Drive
Community Health
Improvement
The Metcalfe Network Effect

All In is a Learning Collaboration

Total Network of 25 Projects 10 projects – DASH Cohort
15 projects – CHP Cohort

Geographic Scale
0 1 2 3 4 5 6 7 8
Metropolitan Area
Neighborhood
Tribal Area
State
Multiple Neighborhoods
Multi-County Region
City or Town
County
CHP DASH

Sectors Represented
0 5 10 15 20 25
Tribal
Community Development
Transportation
Economic Development
Private
Environment
Criminal Justice
Government
Academia
Education
Housing
Nonprofit/Community-based Organizations
Public Health
Behavioral Health & Social Services
Health Care
CHP DASH

Data Types / Sources
0 2 4 6 8 10 12 14 16
Community Health Needs Assessment
Service Utilization
Other
Social Service
Survey Data
Public Health
Geographic, Temporal Data
Health Information Exchange
Insurance Claims
Private Records
Public Records
Electronic Health Records
CHP DASH

Collaboration: A National Perspective
Organizational missions both drive and inhibit collaboration
Collaboration slows down the work, at least initially
In-person encounters are critical to relationship building
Meaningful peer-to-peer collaboration must be staffed
Opportunities for learning exist at ALL levels:
• NPO-to-NPO
• Grantee-to-grantee
Distributed leadership requires clear delineation and documentation of roles, responsibilities and accountability
Honesty, respect, and compassion are key ingredients
It helps (a lot) to like your collaborators

Indicators of Progress
Enabling Factors
• Community collaboration
• Resources
• Data & technology infrastructure
System Features
• Structure and process• Governance
• Workflow
• Training
• Technical factors• User-
orientation
• Timeliness
• Interoperability
Successful Use Cases
• Number and variety of use cases
• Participating sectors
• Usefulness
• Acceptability
• Sustainability

@MHIF_Heart
@HeartofNewUlm

HONU is a 10-year demonstration project designed to apply and widely disseminate established, evidence-informed health improvement practices, based on the community’s own level of risk and customized to their preferences.

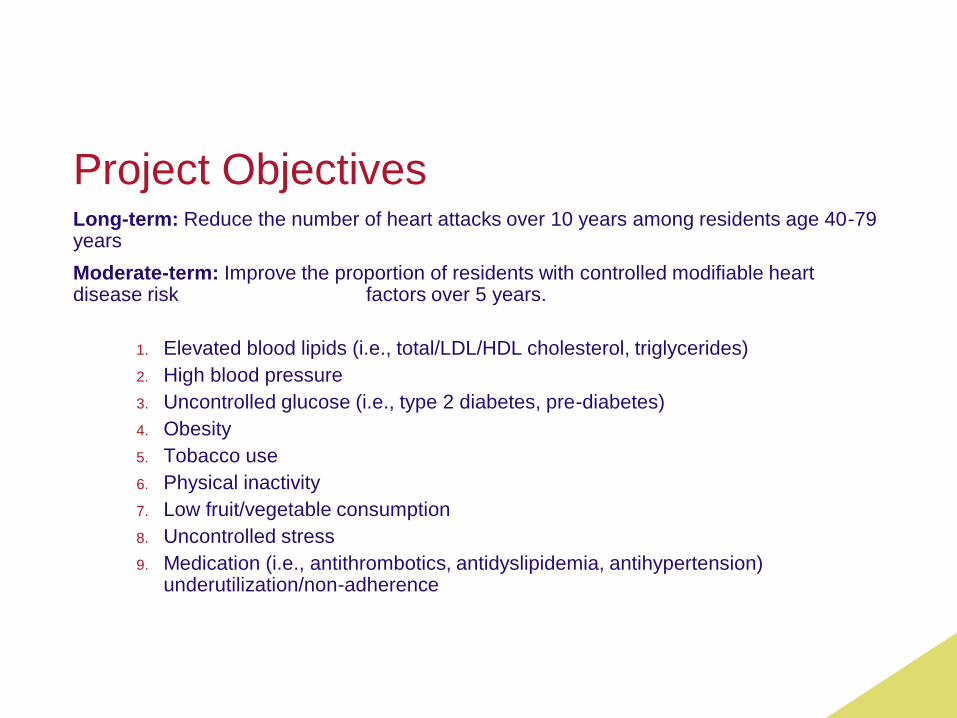
Project ObjectivesLong-term: Reduce the number of heart attacks over 10 years among residents age 40-79 years
Moderate-term: Improve the proportion of residents with controlled modifiable heart disease risk factors over 5 years.
1. Elevated blood lipids (i.e., total/LDL/HDL cholesterol, triglycerides)
2. High blood pressure
3. Uncontrolled glucose (i.e., type 2 diabetes, pre-diabetes)
4. Obesity
5. Tobacco use
6. Physical inactivity
7. Low fruit/vegetable consumption
8. Uncontrolled stress
9. Medication (i.e., antithrombotics, antidyslipidemia, antihypertension) underutilization/non-adherence

Challenge #1
Most health related behaviors
are not systematically tracked
in the electronic health record

Collecting & Utilizing Data
Data Integration Plan
Synthesize & share with target
audiences
Community Needs
Resident surveys
Focus groups
Parent surveys
Classroom tallies
Environmental assessments
Built environment
Nutrition environment
Policy assessment
Electronic health records
90% of residents have data in the record
(80% of target population)
Screening data
Behavioral
Health-related data
Desired Impact
Create interventions to improve population health

New Ulm, MN - 2009 Community Diagnosis
41% Obese
35% Overweight
38% Metabolic
syndrome
17% Consumed 5 fruits
and vegetables a day

Heart of New Ulm Project Approach
Healthcare
CommunityWorksite
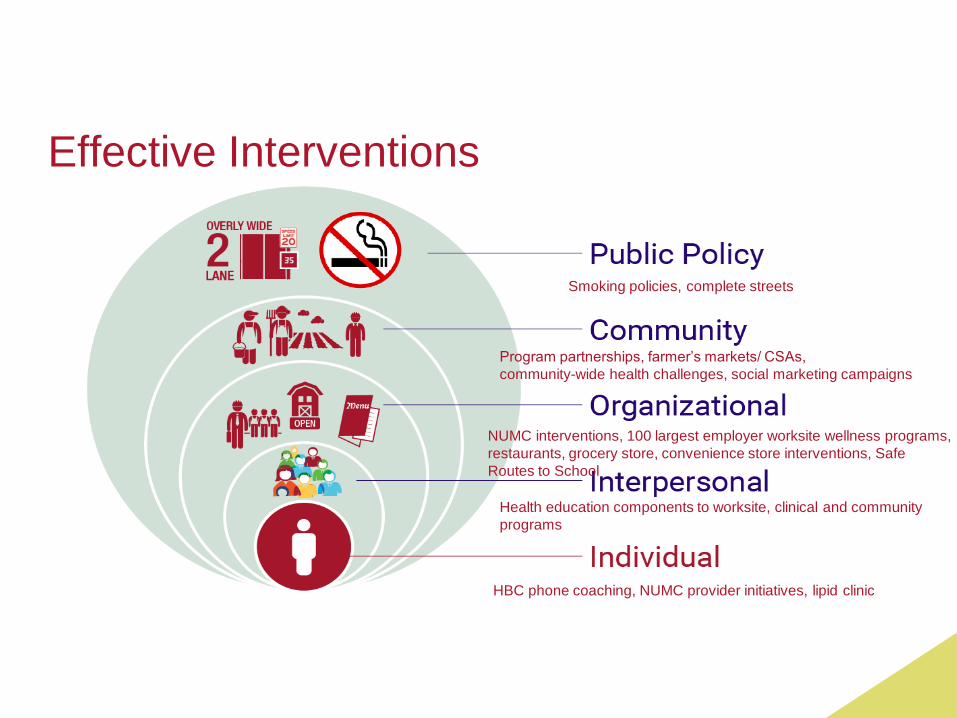
Effective Interventions
Smoking policies, complete streets
Program partnerships, farmer’s markets/ CSAs,
community-wide health challenges, social marketing campaigns
NUMC interventions, 100 largest employer worksite wellness programs,
restaurants, grocery store, convenience store interventions, Safe
Routes to School
Health education components to worksite, clinical and community
programs
HBC phone coaching, NUMC provider initiatives, lipid clinic

NUMC’s RoleLeveraging data to engage key
stakeholders & create community
ownership
Challenge #2

Communications Strategy
Spread Educational Lifestyle Messages Everywhere

Insert visual data
example?

Comparison of HONU Changes to NHANESNHANES
2009-10
NHANES
2011-12
NHANES
Change
HONU
2008-09
HONU
2012-13
HONU
Change
BP at goal
(<140/90 mmHg)83.1% 82.5% -0.6 79.3% 86.0% +6.7
BP medication 35.2% 36.8% +1.6 38.3% 47.6% +9.3
LDL at goal
(< 130 mg/dL)64.3% 63.7% -0.6 68.0% 72.0% +4.0
Cholesterol at goal
(<200 mg/dL)47.5% 46.9% -0.6 58.3% 65.1% +6.8
Not Obese
(BMI <30)62.5% 62.3% -0.2 55.9% 55.2% -0.7
NHANES data selected for participants age 40-79, white non-Hispanic to provide a comparison group similar
to New Ulm resident demographics, sample weights applied for analysis


Behavior Changes Among Screening Participants age 40-79
Measure 2009
(n = 3123)
2011
(n = 1976)
2014/15
(n = 1008)
Smoking 7.9 7.4 5.5
Physical Activity
(at least 150
minutes / week)
63.9 96.0 96.2
Fruit and
Vegetables (5 or
more servings per
day)
16.3 26.6 30.2
Screening analysis is age and gender adjusted to account for
differential age and gender distributions in each screening time
period.



Current challenge
‣How do we continue to track behaviors over time to continue to inform progress and decisions going forward?
How do we continue to
track behaviors over
time?
Current Challenge

Contact information
Rebecca Lindberg, MPH, RD
Director, Population Health
Minneapolis Heart Institute FoundationP: 612.863.4087
[email protected] Twitter: @relindberg
Gretchen Benson, RD, CDE
Manager, Healthcare Systems Integration
Minneapolis Heart Institute Foundation P: 612.863.4222
[email protected] Twitter: @gbenson300


Food for Health: Coordinating Care Across Sectors
to Improve Health Among Vulnerable Populations

PCCIPIECES.ORG




DIABETES HYPERTENSION
COMMUNITY HEALTH ISSUES

Pieces
Plexus™

Buildinghealthiercommunities.

CHALLENGESFor DASH, Workflows Inform Technology


A framework for challenges
Technical & Operational
Relationship Management
Communication & Governance
Trust & Control
Making the Value Case
Interoperability
Data Quality & Usefulness
Familiarity with Data
Resources

Our Role: To listen, identify, characterize, and then (try) to help resolve
As two coordinating nodes on the All In network, DASH and CHP are continuously:
Monitoring and reflecting back what we hear as being major challenges and areas of mutual concern
Cultivating opportunities for peer-learning and collaboration
This is often an organic process, but sometimes we explicitly ask
With a collective cohort of 25/43, we have started to solicit feedback regarding key challenges and (early) lessons learned

Learning from 43 projects: technical challenges
Partners are ready, but vendors are not; vendor solutions are often clunky with poor user interface
Patient/client matching is hard and under resourced
Building technical interfaces for multiple EHR systems is time and resource intensive, and not scalable
Few standards exist for capture, sharing and integration of social determinants data elements

Learning from 43 projects: governance challenges
Policies on data sharing differ by sector, and within government
Establishing trust relationships within healthcare is (very) hard; tougher still with increased number and nature of partners
HIPAA provides useful frame for data use within healthcare absent consent, but this does not (necessarily) extend to other sectors / other use cases.

Learning from 43 projects: communicating value
Story telling; use case based narrative
Tailor scenarios to specific audiences
Each service offering and use case has a different value proposition; consider what value the data sharer receives
Vertical alignment of missions can demonstrate potential to accomplish everyone's goals together
Show people the PRODUCT. Show them a beautifully designed data display that enables them to answer critical questions, and they will understand the value

Learning from 43 projects: advice
Build on existing trusting relationships
Technology is the least of your concerns - you'll acquire that through a great relationship
This is new to a lot of people; you're not preaching to the converted, so don't underestimate the number of times you have to say the same thing - five different ways!
Include an influential non-government neutral visionary
Get community buy-in and agreement on key evaluation measures
Relationships are the key to being able to move (integration) forward

Discussion Questions
Moderators’ prerogative to begin …

Four tiers to build the All In network

Go All In!
Sign up for news at dashconnect.org
Follow us at @DASH_connect and @AcademyHealth#CHPhealthIT
![THE EASTERN REGIONAL NETWORK (ERN): SIMPLIFYING MULTI … · 2019-03-05 · [ 3] Eastern Regional Network (ERN) •Vision:To simplify multi-campus collaborations and partnerships](https://img.pdfslide.net/doc/110x75/5f873e0e5a501977131087ca/the-eastern-regional-network-ern-simplifying-multi-2019-03-05-3-eastern.jpg)




























