Embed Size (px)
Citation preview
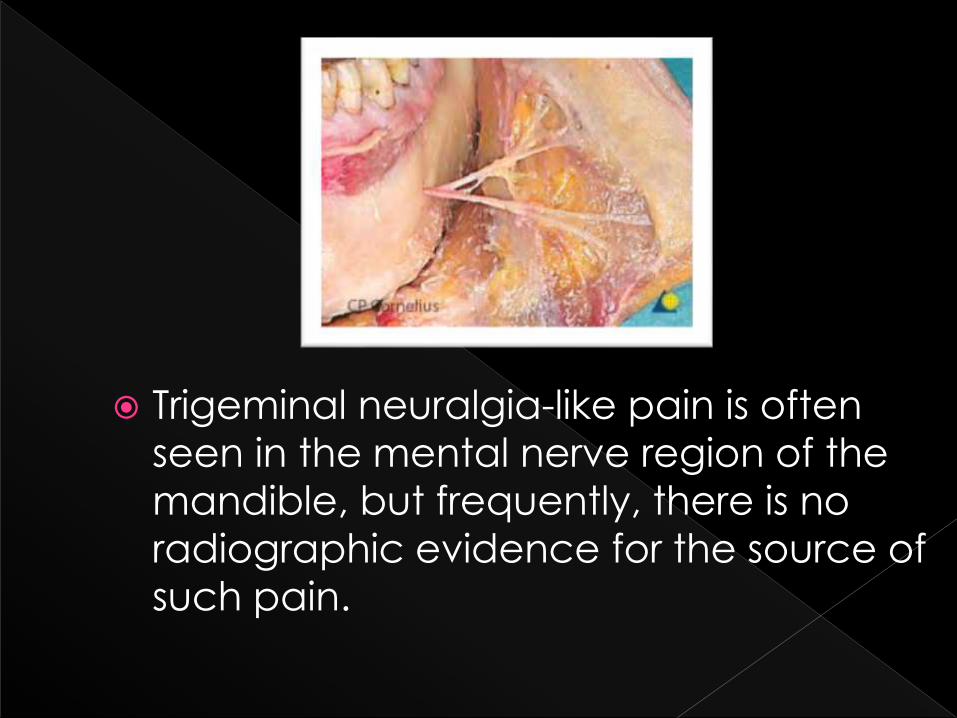
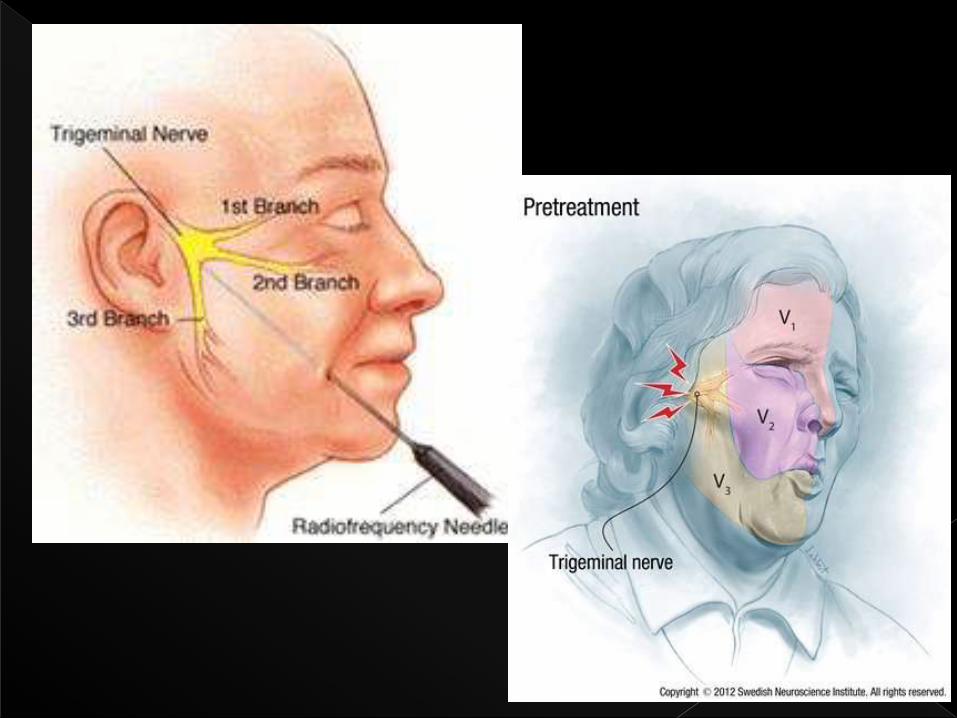
Trigeminal neuralgia-like pain is often
seen in the mental nerve region of the
mandible, but frequently, there is no
radiographic evidence for the source of
such pain.
A common cause of pain in the middle and anterior portion of the mandible is an injury or abnormality of the inferior alveolar nerve or its largest terminal branch, the mental nerve. Procedures such as implant placement, simple and complex oral surgical procedures, or improper retraction of a tissue flap containing the mental nerve are all known causes for injury to the mental nerve.
In addition, crushing injuries, producing permanent nerve injury, is another recognized cause of mental nerve pain.
Publication:01/01/2009
Name: CRANIO: The Journal of Craniom
andibular Practice Publisher: Chroma
Subject: Science and
technology
This irritation may be severe enough to
produce a chronic, atypical type of
trigeminal neuralgia, which is not
amenable to treatment with
medications. Such was the situation in
the current case report Published in 2009
as well as
EXCRUCIATING
ELECTRIC SHOCK LIKE
PAIN !!...
An 88-year-old Caucasian married female was
seen in a craniofacial pain practice with the chief
complaint of left jaw pain. The pain had been
present for about a year with no known etiology
nor a prior history of any type of trigeminal pain.
Teeth numbers 17 through 22 had been removed
years earlier without any post-operative
complications.
Ten years earlier, she had been successfully
surgically treated for a bony lesion in the posterior
portion of the left side of her mandible, but until
the onset of this current problem, she had
experienced no additional mandibular pain.
The pathological diagnosis was ischemic
osteonecrosis and for nine years, she had been
pain-free.
With the onset of her current pain, she consulted her primary care physician who referred her to a neurologist.
Neurological evaluation, which included MRI evaluation, was negative. Cranial nerve examination was normal. with the exception of elicitation of pain in the mental nerve origin only. The patient was placed on a trial dose of gabapentin with no success.
She described her pain as sharp, shooting, and at times, electrical, which affected the normal distribution of the mental nerve.
Panoramic radiographic evaluation demonstrated
what appeared to be a normally formed mental
foramen.
A diagnostic anesthetic injection of the mental
nerve with one cubic centimeter of Citanest
(Prilocaine HCl 4% without vasoconstrictor. Dentsply
International, York, PA) alleviated all pain
complaints with any movement of her face or lip.
When the anesthetic effects were gone, her pain
returned just as before the injection.
A diagnosis of atypical trigeminal neuralgia of the
mental nerve of unknown etiology was
determined.
NAME = M.ABBAS
AGE=50
DOA=13/8/2014
SHARP SHOOTING,LANCINATING PAIN IN
THE RT SIDED MENTAL REGION SINCE 1
YEAR 2 DAYS AFTER EXTRACTION OF
MAXILLARY TOOTH…
PT UNDER different Rx since 1 year at
various settings
(Hyderabad,Dadu,Karachi)
NO RELIEF IN PAIN WHATSOEVER!...
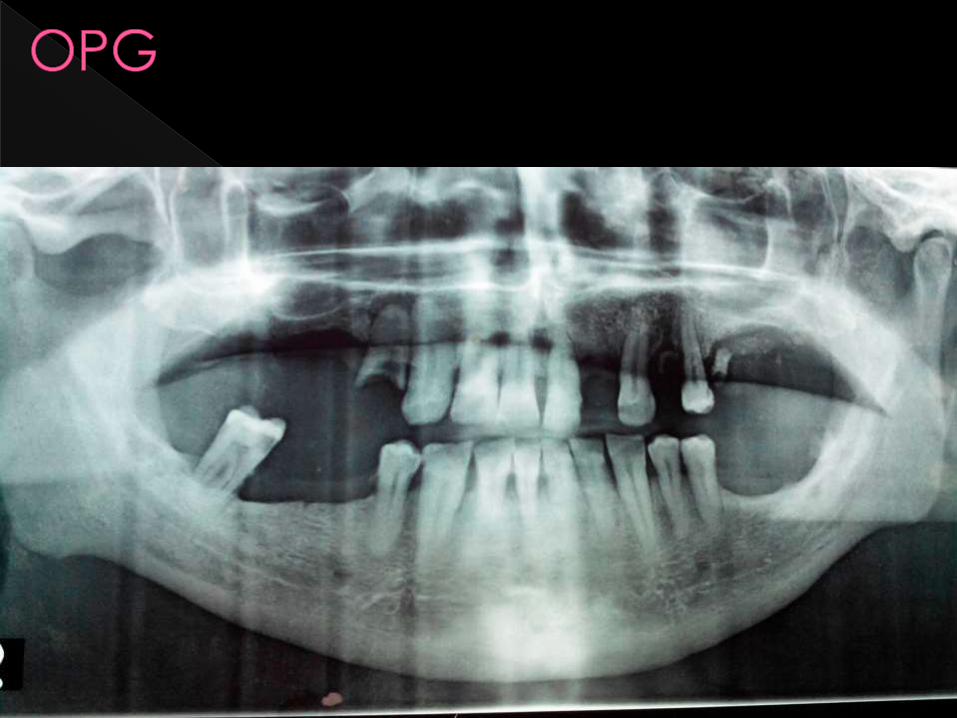
The mental foramen is the structure which
conveys the mental nerve, artery and vein.
Research locates the foramen as most
commonly being situated directly below
the apex of the second premolar. (3-11)
When reviewing the literature, it is clear that
the position of the mental foramen varies,
but the most common location is below the
second mandibular premolar tooth.
Article presents a case of trigeminal neuralgia-like pain of the mental nerve
. An 88-year-old female presented with trigeminal neuralgia-like pain in the distribution of the mental nerve due to no known etiology. Conservative therapy using the appropriate medication by her neurologist was not beneficial and she could not tolerate the side effects of the medication.
Her pain was immediately and totally eliminated with a diagnostic anesthetic block of the painful mental nerve.
Successful treatment was provided by carefully
smoothing of the osseous edge or rim of the mental foramen.

NOTE THE DIFFERENCE IN SIZE

The first line of treatment for patients with
trigeminal neuralgia is always
medication. Even minimally invasive
surgery carries risks and should be
considered a last resort.
ANTICONVULSANTS
ANTIDEPRESSANTS
CARBAMEZAPINE,GABAPENTIN,PHENYTOIN etcCommonly experienced side effects of drug therapy for TN include dizziness, drowsiness, forgetfulness, unsteadiness, and nausea.
In addition, carbamazepine and other drugs prescribed for TN do not always remain effective over time, requiring high doses each time.
Surgical evaluation for trigeminal neuralgia includes confirming the diagnosis of trigeminal neuralgia, reviewing a brain magnetic resonance imaging (MRI) scan to exclude other treatable causes of face pain, and evaluating the severity of the pain, the general medical condition of the patient, and the patient's preference for treatment goals versus risk aversion.
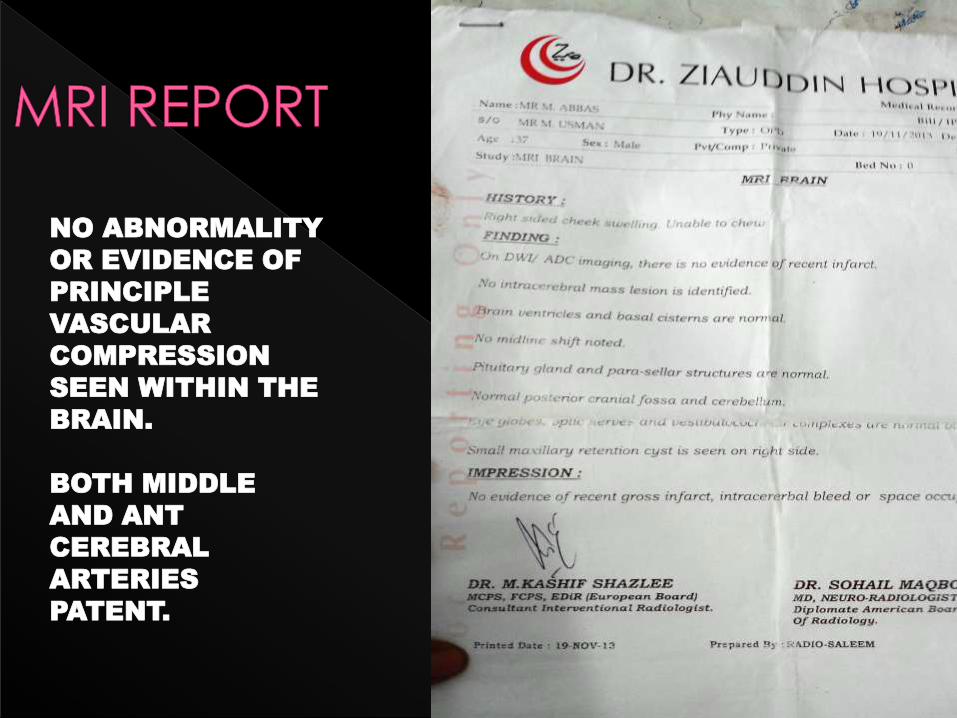
NO ABNORMALITY
OR EVIDENCE OF
PRINCIPLE
VASCULAR
COMPRESSION
SEEN WITHIN THE
BRAIN.
BOTH MIDDLE
AND ANT
CEREBRAL
ARTERIES
PATENT.
CENTRAL CAUSE NOT FOUND

Trigeminal neuralgia surgery is reserved
for people who still experience
debilitating pain despite best medical
management
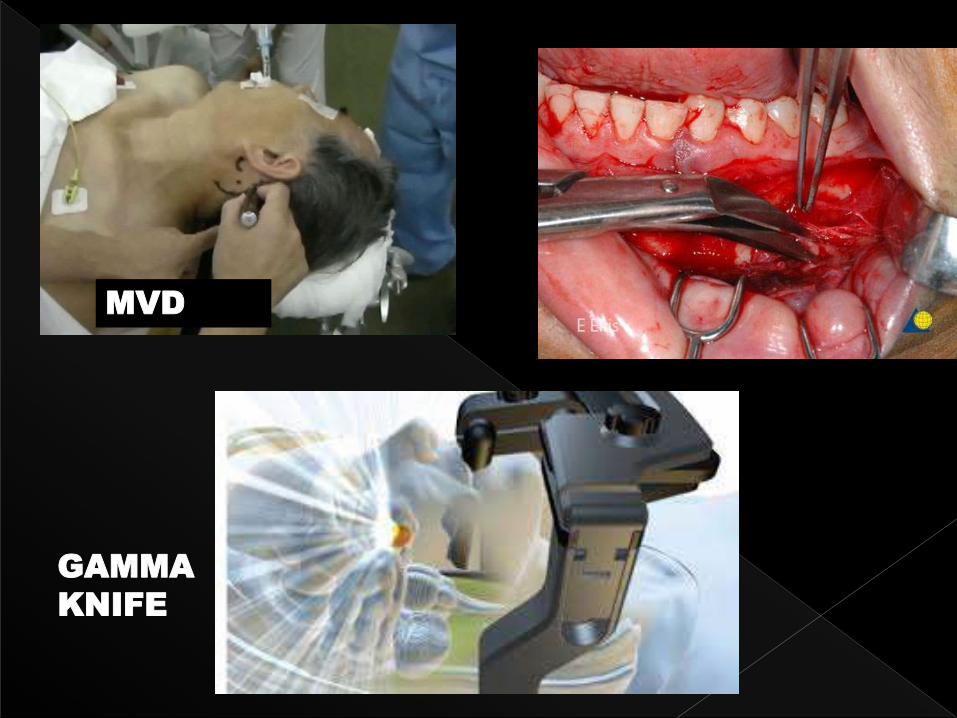
MVD
GAMMA
KNIFE

1-
MENTAL FORAMEN
CONTOURING/RESHAPING???....