Embed Size (px)
Citation preview

PRESENTED BY:
DR.MEENAKSHI
SINGH
M.D.S 1st YEARGUIDED BYDR.S.K SINGHDR.AJAY SINGHDR.B.K TONDON

Dentistry has evolved from a curative to a creative science in a very short span of time.
The newest advancement in this esthetic dentistry is the introduction of all ceramic materials.

INTRODUCTIONCeramics was originally referred to the art of
fabrication of pottery. The term derives from the greek word of "keramos" which means "a potter or pottery". It is believed that this word is related to the Sanskrit term meaning "Burned Earth".
The earliest ceramic articles date back to 23,000 BC & consisted of earthenware, stoneware & porcelain. Porcelain was first obtained by fluxing white china clay with china stone to produce a translucent material.

Ceramics Compounds of one or more metals with a non
metallic element (usually silicon, boron, oxygen) that may be used as a single structural component or as one of the several layers that are used in the fabrication of a ceramic based prosthesis G.P.T 7, Anusavice. ORThey are non-metallic, inorganic structures, primarily containing compounds of oxygen with one or more metallic or semi- metallic elements (Aluminium, Calcium, Lithium, Magnesium, Titanium, Potassium, Silicon, Sodium, Zirconium). Dental ceramics may consist primarily of glasses, porcelains, glass-ceramics or highly crystalline structures.

Ceramics may be classified into four categories according to their composition
Silicate ceramics( dental porcelain fall in this category)
Oxide ceramics Non oxide ceramics Glass ceramicsMany dental ceramics have a crystal phase and a glass phase based on the silica structure. This structure is characterized by a Si-O tetrahedron in which a Si4+ cation is positioned at the center of a tetrahedron with O- anions at each of the four corners. The resulting structure is not close-packed, and it has both covalent and ionic characteristics. The SiO4 tetrahedra are linked together by sharing their corners.

Porcelain is a special type of ceramic based on a specific dominant composition that includes silica, alumina, and potassium oxide. These three oxides are alloyed and produce a potassium aluminosilicate. Dental porcelain is a very narrow range of these compositions.
Most dental porcelains are partially crystalline. Their bonding is mixed and dominated more by covalent than ionic character. The composition includes non-crystalline and crystalline phases. Dental porcelain is created, not by directly mixing the three main oxides, but by mixing clay, feldspar, and quartz that contain the oxides.
Dental porcelains are dominated by feldspar and tend to have more silicate matrix in the final microstructure than dispersed crystalline phases. These are called feldspathic porcelains.
Feldspathic porcelains are esthetic but not very strong. As the alumina content is increased the amount of crystalline dispersed phase, particularly alumina rich ones, is increased and the material becomes stronger. However, aluminous porcelains are whiter and lack the translucency of feldspathic ones. Aluminous porcelains are good for underlying cores while feldspathic ones are good for esthetic veneers.

PROPERTIES OF CERAMICSDental porcelain is chemically very stable, and
provides excellent aesthetics that do not deteriorate with time. The thermal conduction and the coefficient of thermal expansion are similar to those of enamel and dentine, so in the presence of a good marginal seal, marginal percolation is less likely to be a problem.• The material, being primarily a glass, lacks any fracture
toughness. The maximum strain that a glass can withstand is less than 0.1%. Glasses are extremely sensitive to the presence of surface microcracks and this represents one of the major drawbacks in the use of dental porcelain.

REVIEW OF CERAMIC PROPERTIES
1. Physical Properties:a. Intermediate density (1.0-3.8 gms/cc)b. High melting point (= refractory)c. Low coefficient of thermal expansion (12-15 ppm/C)
2. Chemical Properties:a. Low chemical reactivityb. Low absorption and solubility
3. Mechanical Properties:a.High modulusb.Much stronger in compression(350-550Mpa) than
tension( (~10X)c.Brittle (low plastic deformation (<0.1%); low fracture toughness
d.Surface hardness (460 KHN),tooth 4. Biological Properties:
a. Relatively inert

Properties of Ceramic which make it desirable for Dental Use : Chemically inert Compatible with soft tissue- no hyperplastic or inflammatory change with
gingiva seen Resistant to sudden thermal change Provides good insulation Colour stability
Drawbacks of ceramics1. Brittleness2. Shrinkage during firing3. Ability to abrade opposing tooth4. They need to have accurate margins as they are
fabricated outside the mouth

Uses of ceramics in dentistry Make denture teethFixed partial denturesSingle unit crownsInlays and onlaysLabial veneersCeramic brackets used in orthodontics

History of dental ceramics
Fauchard in 1728,described the use of backed enamel in colour and shade corresponding to natural teeth.
1774,Alexis Duchateau,constructed first set of mineral teeth.
Guisepangello Fonzi of Italy in 1808,introduced terrometallic teeth.
Plantou in 1817,introduced porcelain denture teeth.In 1825,Stockton began the production of porcelain
teeth. Porcelain inlays and crowns were developed by Wain
in 1923 as reported by Jones.

In 1889,Dr Charles H Land filed the first patent for porcelain jacket crown
Glass ceramics was developed by Corning glass works.
Weinstein and weinstein in 1962 described the formulation of feldspathic porcelains .
Vita Zahnfabrik in 1963 developed the first commercial porcelain.
A significant improvement in the fracture resistance of porcelain crowns was reported by Mclean & Hughes in 1965.
MacCulloch in 1968 proposed the use of glass ceramics in dentistry.
O’Brien in 1985 developed magnesia core ceramic.

CAD CAM systems were developed in the early 1980’s .
Magnesia core ceramic was developed as an experimental material in 1985 (O'Brein, 1985).
Dr. Horn developed the platinum foil technique .
Calamia reported the refractory die technique.
Early 1990’s IPS Empress was developed and IPS Empress 2 was developed in the late 1990’s.
In 1992 Duceram LFC was marketed .
Andersson and Oden developed Procera all ceram .
Johnson and Johnson developed the cerestore ceramics

Classification of ceramics According to their firing temperature1. high fusing -1290 to 1370 degree C2. medium fusing-1095 to 1260 degree C3. low fusing -870 to 1065 degree C According to type1. feldspathic or conventional porcelain2. leucite reinforced porcelain3. aluminous porcelain 4. glass infiltrated alumina5. glass infiltrated spinel6. glass ceramic According to use1. porcelain for artificial teeth2. jacket crown, veneer, and inlay porcelain3. metal ceramics4. anterior and posterior bridge porcelain

According to processing method sintered porcelain cast porcelain machined porcelain
According to method of firing air fired i.e at atmospheric pressure vacuum fired i.e at reduced pressure
According to substructure material
cast metal,swaged metal, glass ceramic, CAD-CAM porcelain, sintered ceramic core
According to esthetic role of porcelain: Opaque porcelain Body porcelain (incisal or enamel;
gingival or dentin; modifier) Stains or glazes

Processing of ceramic materials Ceramics are obtained by sintering fine ground particles. In the
traditional laboratory technique, these particles are applied onto the framework as a water slurry dried and fired a process referred to as "HYDROPLASTIC FORMING".
CERAMMING-By subjecting the material to specific temperature cycles,
a stronger crystalline phase is grown out of an initially glassy mass
SLIP CASTING- randomly packed alumina crystals are lightly sintered so that only the contact points of the alumina crystal fuse. The porous structure is then infiltrated with molten glass drawn into the mesh by capillary action
HEAT PRESSING- achieved by sintering under pressure thus decreasing the porosity of the material and increasing strength. IPS EMPRESS and PROCERA ALLCERAM are manufactured using this principle.

Ceramic processing methods
Feldspathic porcelain of traditional PFM restorations, aluminous porcelain and pure alumina ceramic (Procera all ceram )are condensed by vibration and dry pressed and sintered at high temperatures.
Pressable ceramics (IPS Empress ,IPS Empress2, Finesse all ceramic ,OPC,OPC-3G) when heated and subjected to hydrostatic pressure flow in a mold and after removal and divesting are then veneered.
Cast and cerammed crowns such as Dicor are made using the lost wax technique. The molten glass is cast into a mold, heat-treated to form a glass-ceramic, and colored with shading porcelain and surface stains.

Slip cast ceramics (In-ceram spinel,In-ceram-zirconia,In-ceram alumina),a slurry of liquid and particles of alumina ,spinel,zirconia is placed on a refractory die that draws out the water from the slurry and the slip cast deposit is then sintered on this die and then it is coated with a slurry of a glass phase layer. During firing, the glass melts and infiltrates the porous ceramic core.
For CAD CAM processes ,the ceramic block materials are shaped into inlays or crowns using a CAD-CAM system(CEREC)

Heat
particulate mass cohesive object
PORO SITY(INCOM PLETE SINTERING )
SCHEMATIC DIAGRAM OF SINTERING PROCESS

METHODS OF STRENGTHENING CERAMICS
1.Minimize the effect of stress raisers: Numerous minute scratches & other defects are present on
the surfaces of the materials. These surface flaws behave as sharp notches whose tips may be as narrow as the spacing between several atoms in the material.
When the induced mechanical stress exceeds the actual strength of the material bonds, at the notch tip break, forming a crack.
Stress raisers are discontinuities in ceramic & metal-ceramic structures and in other brittle materials that cause a stress concentration in these areas.

Abrupt changes in shape or thickness in the ceramic contour can act as stress raisers & make the restoration more prone to failure. Thus the incisal line angles on an anterior tooth should be well rounded for a ceramic crown.
Several conditions can cause stress concentrations. • Creases or folds of the platinum foil or gold foil substrate that become embedded in the porcelain leave notches that act as stress raisers.
• Sharp line angles in the preparation also create areas of stress concentration in the restoration.
• Large changes in porcelain thickness, a factor also determined by the tooth preparation, can create areas of stress concentration

Increase the fracture resistance by one of the following options:
1. Select stronger and tougher ceramics.2. Develop residual compressive stress within the
surface of the material by thermal tempering.3. Develop residual compressive stresses by
matching thermal expansion coefficients.4. Reduce tensile stress by using stiffer supporting
materials.5. Minimize the number of firing cycles.6. Design the ceramic FPD with greater bulk and
broader radii of curvature7. Adhesively bond ceramic crowns to tooth
structure.

2.Develop residual compressive stresses:
One method of strengthening glasses and ceramics is the introduction of residual compressive stresses within the ceramic.
The metal and ceramic should be selected with a slight mismatch in their thermal contraction, so that the metal contracts slightly more than the porcelain on cooling from the firing to the room temperature.
For the ceramic prosthesis the thermal contraction coefficient of the core ceramic is slightly greater than that of the veneering ceramic.
This mismatch leaves the porcelain in residual compression & provides additional strength for the prosthesis.

A fundamentally different method of strengthening glasses & ceramics is to reinforce them with a dispersed phase of a different material that is capable of hindering a crack from propagating through the material.
There are two different types of dispersions used to interrupt crack propagation. One type relies on the toughness of the particle to absorb energy from the crack & deplete its driving force for propagation. The other relies on a crystal structural change under stress to absorb energy from the crack.

3.Minimize the number of firing cycles
The purpose of porcelain firing procedures is to densely sinter the particles of powder together & to produce a relatively smooth, glassy layer (glaze) on the surface.
In some cases, a stain layer is applied for shade adjustment
or for characterization such as stain lines or fine cracks.
Leucite, is a high expansion crystal phase, which can greatly
affect the thermal contraction coefficient of the porcelain.

Some porcelains undergo an increase in leucite crystals after multiple firings that will change their thermal expansion coefficients.
If the expansion coefficient increases above the value for the metal, the expansion mismatch between the porcelain & the metal can produce stresses during cooling that are sufficient to cause immediate or delayed crack formation in the porcelain.

4.MINIMIZE TENSILE STRESS THROUGH OPTIMAL DESIGN OF CERAMIC PROSTHESES:
Sharp line angles in the preparation will create areas of stress concentration in the restoration. Because the forces on anterior teeth are relatively small, the low to moderate tensile stresses produced can be supported by ceramic crowns more safely.
• If there is a great amount of vertical overlap (overbite) with only a moderate amount of horizontal overlap (overjet), high tensile stresses can be produced.


•.The tensile stresses in a ceramic FPD can be reduced by
usinga greater connector height and by broadening the radius of curvature of the gingival embrasure portion of the inter proximal connector.
However, a connector height greater than 4mm makes the anatomic form in the buccal area of a posterior FPD too bulky & unaesthetic.
One way to reduce tensile stresses on the cemented surface in the occlusal region of ceramic inlays or crowns is to use the
maximum occlusal thickness as possible. This thickness is typically 2.0 mm.

5.Ion exchange:K.J Anusavice ,C.Shen ,and R.B.Lee: Strengthening of
feldspathic porcelain by ion exchange and tempering : J Dent Res 71(5):1134-1138,May,1992
“The study was carried out on seven feldspathic porcelains to see the effectiveness of thermal tempering and ion exchange on crack growth and bi-axial flexural strength. The results showed that tempering treatment was more effective in strengthening porcelain than was the ion exchange process as measured by the bi-axial flexural strength and that ion exchange process yielded a surface that was more resistant to crack initiation than was yielded by thermal tempering.”

The ion - exchange process is sometimes called CHEMICAL TEMPERING and can involve the sodium ion since sodium is a common constituent of a variety of glasses and has a relatively small ionic diameter.
If a sodium - containing glass article is placed in a bath of molten potassium nitrate, potassium ions in the bath exchange places with some of the sodium ions in the surface of the glass article and remain in place after cooling.

Since the potassium ion is about 35%larger that the sodium ion, the squeezing of the potassium ion into the place formerly occupied by the sodium ion creates very large residual compressive stresses.
The product 6C Tuf-Coat was potassium rich slurry that
could be easily applied to a ceramic surface and when heated
to 450 O C for 30 min (in a standard porcelain furnace) caused a sufficient exchange between the potassium ions in the slurry and the sodium ions in the ceramic.

5.Thermal tempering :
The most common method for strengthening glass is by thermal tempering. Thermal tempering creates residual surface compressive stresses by rapidly cooling (quenching) the surface of the object while it is hot and in the softened (molten) state. This rapid cooling produces a skin of rigid glass surrounding a soft (molten) core.
As the molten core solidifies it tends to shrink, but the outer skin remains rigid.
For dental applications, it is more effective to quench hot glass-phase ceramics in silicone oil or other special liquids rather than using air jets that may not uniformly cool the surface.
This thermal tempering treatment induces a protective region of compressive stress within the surface.


6.Dispersion strengthening:
A method of strengthening glasses & ceramics is to reinforce them with a dispersed phase of a different material i.e. capable of hindering a crack from propagating through the material. This process is referred to as dispersion strengthening.
Toughening depends upon the crystals type, its size, its volume fraction, the interparticle spacing, and its relative thermal expansion coefficient relative to the glass matrix.
When a tough, crystalline material such as alumina (Al2O3) is added to a glass, the glass is toughened and strengthened because the crack cannot pass through the alumina particles as easily as it can pass through the glass matrix.

8.TRANSFORMATION TOUGHENING :-
Dental ceramics are strengthened & toughened by a variety of dispersed crystalline phases including alumina (Vitadur Alpha, Procera Allceram, In-Ceram alumina), leucite (Optec HSP, IPS Empress, OPC), tetrasilicic fluormica (Dicor, Dicor MGC), lithia disilicate (OPC3G, IRS Empress 2), magnesia-alumina spinell (In-ceram spinell).
Dental ceramics based primarily on zirconia crystals (Cercon & Lava)undergo transformation toughening that involves a transformation of ZrO2 from a tetragonal crystal phase to a monoclinic phase at the tips of crack that are in regions of tensile stress.

SHADE SELECTION AND MANAGEMENTLight sources: Shade selection should not be made using
daylight, because daylight subjected to constant changes
The color of the operatory can also affect shade selection. Walls and cabinets should be glossy enough to maintain brightness without causing a glare. It is recommended that the color of the walls and ceiling be white or off-white.
The dentist should be concerned with "blue fatigue:' this occurs when the eye is unable to differentiate between the various shades of blue. However, blue fatigue increases sensitivity to yellow therefore, to improve shade selection in the yellow range, the operator should stare at a blue card or patient napkin between shade comparisons.

Problems with shade guides:
1. Porcelains do not match the shade guide that they are being compared to .
2. Shade variations occur between different die lots of porcelain from the same manufacturer.
3. Shade guide tabs are 4-5 mm thick compared to the thin 1.5 mm piece of porcelain used for the restoration.
4. Shade guides are not always made with fluorescent porcelain ,which causes inconsistencies in color matching.
5. It is difficult to predict the final shade after the layering of opaque, dentin and enamel.
6. Guide tab lack a metal backing when using porcelain-fused to metal restorations.
7. Shade tabs are condensed differently than porcelain used for final restorations.

Shade selection guidelines:
There are a number of methods that can be employed to intensify the shade selection. They are as follows:
If patient is wearing bright clothing ,drape him or with a neutral colored cover.
Having patient remove lipstick or other makeup.Clean the teeth and remove all stains and debris.Have patient’s mouth are dentist’s eye level.Determine the shade at the beginning of the appointment
to avoid ocular fatigue.Shade comparisons should be performed at five second
interval so as not to fatigue the cone cells of the retina.

7. Obtain value levels by squinting.8. Compare shade under varying conditions (wet
vs dry lips: retracted vs pulled down lips).9. Use the canine as reference for shade because
of the highest chroma of the dominant hue of the teeth.
10. Select a shade of lower chroma and higher value,if unable to match shade precisely.
11. Grind off the necks of the shade tabs because they tend to be darker than the rest of the shade tab.

R.Duane Douglas ,DMD,MS,and Jane D.Brewer,DMD,MS
(Faculty of Dentistry , University of Manitoba,Winnipeg,Manitoba,Canada) :
Acceptability of shade differences in metal ceramic crowns:J Prosthet Dent 1998;79:254-60
Purpose: The CIELAB colorimetric system was used to study the relationship between measured colour differences and human observer assessment of colour differences in metal ceramic crowns.
Results :Correlations between instrumental and vital assessment of colour differences in the crown pairs did not disagree in all dimensions of colour space.
Conclusion: acceptability thresholds were found to be dependant on chromaticity. Observers were more sensitive and critical of crowns whose color differed in redness as opposed to crowns whose color differs to the same extent in yellowness.

3-D SHADE GUIDE SELECTION
How to select the shade with the VITAPAN 3D-Master Shade Guide
There are three distinct steps: - determine lightness-darkness
=Value determine intensity of colour
=Chroma determine colour =
hue

3-D VITA SHADE GUIDE

Step 1 . Select one group from the five lightness groups-Three things are clearly visible.A scale from lightest to darkest across the full width
of the shade guide. This light dark scale is divided into 5 separate ,
uniformly spaced groups of lightness-1,2,3,4,5All shade tabs within one group have the same
lightness. Human dentition progressively darkens with
increasing age. This can be an indicator and assist in choosing the lightness group
i.e teen = group1 adult =group 2 middle age = group 3
older = group4 elderly =group 5

In each of the groups there is one shade tab which is positioned more prominent and higher than the others in its group.
These 5 tabs can be used to select the appropriate lightness group. Each is numbered MI with its group number preceding [i.e 1MI ,2 MI, 3 MI, 4MI,5MI], rather than trying to pick up the appropriate MI tab from the five , decide by eliminating those which are obviously too light or too dark.
The lightness group selection is best accomplished with the patient standing in subdued lighting.In this first step ,colour is not being selected but rather , the appropriate level of lightness is selected.(group 1,2,3,4,5)
Finally record the number of selected group[1,2,3,4,5] . Intermediate selections are recorded as 1.5/2.5etc

Step 2 (good quality colour balanced lighting is necessary for steps 2 and 3)Select the chroma = colour saturation or
intensity From the group selected in step 1,
remove the middle stick ‘M’ and fan out three blades . Choose which of the three tabs most closely correspond to the body of the standing teeth in terms of colour intensity [i.e weak – medium- strong]
We are selecting “ intensity or strength colour” –NOT COLOUR
Record choice 1-2 or 3.Intermediates can also be selected and recorded as 1.5,2.5

Step 3 Select the hue-Natural unmodified dentition ranges in hue
from a strong yellow to a faint yellow to reddish / brownish. The letter below each stick on the shade guide base indicate the hue as follows.
L =left side of the group = yellowish hueM= middle of the group =middle hue
[discernable yellow or red]R= right side of the group = reddish hue Look at the body of the patient’s teeth and
decide if a yellowish or reddish /brownish influence is visible . If neither can be seen, select stick ‘M’.
Record your choice L,M,RRemove the selected hue stick from the group
and compare with the patients teeth to verify your choice.

Numbering of shade tabs
The first number of a shade is always and only the group number.
The letter is the hue The remaining number is the chroma
Example: 3M2 = VALUE 3/HUE M/ CHROMA 2After selecting the group in step 1, the
remaining selection of chroma and hue are made solely from within the same group .

A good working definition for a ceramic is any material that is composed primarily of a metal and non-metal composition. Porcelain is a special type of ceramic based on a specific dominant composition that includes silica, alumina, and potassium oxide. These three oxides are alloyed and produce a potassium aluminosilicate. Dental porcelain is a very narrow range of these compositions.
Most dental porcelains are partially crystalline. Their bonding is mixed and dominated more by covalent than ionic character. The composition includes non-crystalline and crystalline phases. Dental porcelain is created, not by directly mixing the three main oxides, but by mixing clay, feldspar, and quartz that contain the oxides. Dental porcelains are dominated by feldspar and tend to have more silicate matrix in the final microstructure than dispersed crystalline phases. These are called feldspathic porcelains. Feldspathic porcelains are esthetic but not very strong. As the alumina content is increased the amount of crystalline dispersed phase, particularly alumina rich ones, is increased and the material becomes stronger. However, aluminous porcelains are whiter and lack the translucency of feldspathic ones. Aluminous porcelains are good for underlying cores while feldspathic ones are good for esthetic veneers. Dental porcelains are limited severely by their defects, particularly pores which originate cracks.

DENTAL PORCELAINIT IS A VITREOUS CERAMIC BASED ON SILICA NETWORK
AND POTASH FELDSPAR OR SODA FELDSPAR.PIGMENTING OXIDES – Iron or nickel
oxide(brown),copper oxide(green),titanium oxide(yellowish brown),manganese oxide(lavender),and cobalt oxide(blue).
OPACIFIERS – Cerium oxide, zirconium oxide, titanium oxide, or tin oxide.
GLASSESFLUXES GLASS MODIFIERS-Na,K,Ca,water,boric oxide BINDERS –starch and sugarPorcelain is a ceramic material formed of infusible
elements joined by lower fusing materials. Most dental porcelains are glasses and are used in fabrication of teeth for dentures, pontics and facings, crowns, inlays, onlays and other restorations

FELDSPATHIC PORCELAINFeldspars are used in the preparation of many dental
porcelains designed for metal ceramic crowns and many dental glasses and ceramics.
Feldspathic porcelains contain a variety of oxide components,including silica(52-62%),alumina(11-16%),sodium and potassium oxide, and certain additives,including lithium and boric oxide.
These ceramics are called porcelain because they contain a glass matrix and one or more crystal phases.They cannot be classified as glass ceramics because ,crystal formation does not occur, through controlled nucleation and crystal formation and growth.

• When potassium feldspar is mixed with various metal oxides and fired to high temperatures,it can form leucite and a glass phase that will soften and flow slightly.
• The softening of this glass phase during porcelain firing allows the porcelain particles to colaesce together(liquid phase sinering) to form a dense solid.
• When feldspar is heated to a temperature between 1150-1530 C,it undegoes incongruent melting(forming liquid and a crystalline material) to form crystals of leucite in a liquid glass.
• This tendency of feldspar to form leucite during melting is used to advantage in the manufacture of porcelains for metal bonding.

There are four types of veneering ceramicsLow fusing ceramics(feldspar and nepheline
syenite based porcelain)Ultra low fusing ceramics(porcelains and
glasses)StainsGlazes(self and add on glazes)

Boric oxide acts as a glass modifier , it decreases the viscosity ,lowers the softening temperature and forms its own glass network.
Alumina can take part in glass network to alter the softening point and viscosity
Pigmenting oxides are added to obtain the various shades needed to stimulate natural teeth, examples: iron or nickel oxide (brown) , copper oxide (green) , titanium oxide (yellowish brown), of cerium manganese oxide (lavender), cobalt oxide (blue)
Opacity may be achieved by the addition oxide,zirconium oxide, titanium oxide or tin oxide.

CAPTEK TM A NEW CAPILLARY CASTING TECHNOLOGY FOR CERAMOMETAL RESTORATIONS

CAPTEK tm A NEW CAPILLARY CASTING TECHNOLOGY FOR CERAMOMETAL RESTORATIONS Captektm restorations include inlays , onlays, crowns,
anterior and posterior prostheses that are based on Captek TMprecious –metal understructure veneered with bake on porcelain.
Captektm alloys are made of two major components – 1. When heated, forms a microscopic dimensional network
of capillaries 2. When melted, flows to these capillaries. Captektm system includes three pairs of materials that form
composite metals:1. Captektm P and Captektm G are used for crown copings and
fixed partial denture abutments.2. CapconTM and CapfilTM are used to connect copings and
pontics to a prosthetic structure3. Captek repair pastetm and CapfilTM are used to form
extensions and additions on the various CaptekTM structures.


CAPTEK PTM
Captek PTM platinum colored strips contain metal particles of less than 30 mm and binders. The strips come in two thickness: one for incisors, canines and premolars & one for molars.
CAPTEK GTM
Captek GTM is applied over the processed Captek PTM and it comes in two thickness , for anterior teeth and for molars. It contains fine particles with 97 % pure gold content and binders and 2.5 mt% silver sections of Captek GTM are cut and fixed with the same firing cycle in the porcelain furnace

CAPBONDTM
CapbondTM is a gold based, gold –colored ceramometal bonder.CapbondTM is used as a very thin point- on layer that forms a fine and open gold colored sponge. Porcelain flows into the sponge like surface to form a strong bond.
CAPTEK REPAIR PASTETM
This material allows additions and corrections on CaptekTM coping after they are recovered from the refractory die.

Fabrication ProcedureDuplicate the working die in the special refractory
material.Cut a piece of the gold-platinum-palladium impregnated
wax sheet.Adapt the foil to the die. Then it is fired to 1075 C (1965 F),
forming a porous metal coping.Adapt the second gold-impregnated wax and refire.
Capillary action draws the gold into the porous gold-platinum structure to form the finished coping.
Build up the opaque body and incisal porcelains in a manner similar to that for a conventional metal-ceramic crown.
Glaze the completed restoration and polish the metal foil at the margin. The procedure has been adapted for FPDs.

Reduced thickness Captektm metal and thin opaque layers make it possible to achieve acceptable margins with a total metal and ceramic thickness of 0.3 - 0.5mm. A thickness of 0.5 - 0.7 mm yields pleasing esthetics on the labial aspect of anterior crowns and a thickness of 0.7 - 1.00 mm provides optimal porcelain thickness.
For best results, premolars & molars should not be thinner than 0.7 mm near the margins. As recommended for conventional cast metals & porcelain, the occlusal surfaces of premolars & molars should be at least 1.2 mm thick.
The minimal thickness possible with esthetic Captek crowns helps present over contouring of the porcelain and enables normal emergence profile with conservative tooth reduction.


Electroformed The Helioform HF 600 system uses an electroforming
technique to produce a thin pure gold coping. The gold is
deposited on polyurethane dies that are coated with a
silver spacer using computer-controlled plating equipment
to control thickness. The coping is coated with a noble
metal paste primer before porcelain application.
Electroforming enables very good marginal adaptation
(better than conventional casting). The system has been
adapted for FPDs.

Step-by-step Procedure
1.Duplicate the working die with the poly-urethane material.
2.Drill the polyurethane and glue the electrode into the die.
3.Apply an even coat of the silver spacer to the preparation and
allow it to dry.
4.Insert the dies into the plating equipment. A magnetic stirrer
ensures circulation of the cyanide-free gold sulfite solution.

5. Turn on the electric current, and gold will be deposited on
the die at an approximate rate of 0.02 mm per hour.
6. Remove the plated copings by heating the dies and remove
the silver spacer with nitric acid or air abrasion.
7. Trim flash from the margin with an abrasive silicone wheel
and seat the coping on the die.
8. Air-abrade the surface and apply the special bonding paste
before porcelain application.

Aluminous porcelain A method of bonding porcelain to metal makes use of tin oxide on platinum
foil.The objective of this technique is to improve the esthetics, by a replacement of the thick metal coping with a thin platinum foil,thus allowing more room for porcelain.
The method consists of bonding aluminous porcelain to platinum foil copings.
Attachment of the porcelain, is secured by electroplating the
platinum foil ,with a thin layer of tin and then oxidising it in a furnace to provide a continuous film of tin oxide for porcelain bonding.
The rationale is that the bonded foil will act as an inner skin on the fit surface to reduce subsurface porosity and formation of microcracks in the porcelain ,thereby increasing the fracture resistance of the crowns and bridges.
They provide a slightly better aesthetics for anterior teeth than are the metal ceramic crowns that employ a metal coping
However ,the strength of the core porcelain used for alumina –reinforced crown is inadequate to warrant its use for posterior teeth.

These are based on the principle of dispersion strengthening i.e.dispersing alumina crystals of high strength in glass matrix.
The concentration of alumina crystals ranges from 40-50%
Flexural strength is raised to 120-150 Mpa as compared to 60Mpa of feldspathic porcelain.

ALUMINOUS PORCELAIN CROWNS (PORCELAIN JACKET CROWN)
McLean AND Hughes in 1965 developed an alumina reinforced porcelain core material for the fabrication of ceramic crowns.

Compaction The production of a porcelain jacket crown involves
three technical stages:
In the construction of a porcelain jacket crown, the porcelain powder is mixed with water and made into a paste. This paste is applied to the die, which has been coated before hand with a very thin platinum foil to allow the porcelain crown to be separated from the die and transported to the furnace.
The powder is mixed with water and a binder to form slurry, which can be applied to the die in a number of ways, such as spatulation, brush application, whipping or vibrating, all of which are aimed at compacting the powder. The objective of these condensation techniques is to remove as much water as possible, result is a more compact arrangement with a high density of particles that minimizes the firing shrinkage.

The particle size and shape are extremely important as they affect the handling characteristics of the powder and have an effect on the amount of shrinkage on firing.
The binder helps to hold the particles together, as the material is extremely fragile in this so-called GREEN STATE
Three basic types of porcelain powder are used :
opaque shade , dentine shade ,enamel shade

FIRING LOW BISQUE STAGE(650-1200OC)-when the
porcelain begins to fuse, continuity is achieved at points of contact between the powder particles. The material is still porous and this state is the low bisque stage.
3. GLAZING There are two ways in which it can be achieved: OVERGLAZE Glasses that fuse at low temperatures are applied
to the crown after construction, and a short period at a relatively low temperature is sufficient to fuse the glaze.
SELFGLAZE Final firing of the crown under carefully controlled
conditions fuses the superficial layer to an impervious surface glaze. In this method, porcelain is heated to its fusion temperature and maintained for 5 min.

The technique presented is a practical, predictable, and accurate method of constructing an aluminous porcelain jacket crown without a platinum matrix.
Advantages :Elimination of the platinum foil
matrix.Ease of fabrication and accuracy of fit.
Edwin J.Riley,D.M.D,Ralph B.Sozio,D.M.D: Precision porcelain jacket crown technique: J Prosthet Dent ,volume 34, number 3,September 1975,(346-50)
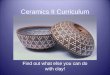
CROSS SECTION OF A METAL CERAMIC CROWN

Technique:• Using any satisfactory technique, obtain , an
impression of the prepared tooth and fabricate a master die.
• Trim the dies and make an elastomeric impression of the prepared dies.
• Pour a non-contaminating ceramic material into the impression, providing the refractory die with an adequate base.The powder-liquid ratio employed is 3 gm of powder to 1cc of liquid. This ratio provides adequate strength and optimum handling characteristics.
• After seating for one hour, separate the die. Separation is easily accomplished by directing an air stream between the die and the impression.
• Paint a ceramic metal agent on the refractory die(to avois shrinkage of die?) ,to the margin , providing a thin uniform layer.

• Fire the refractory die (firing cycle :dry in front of the muffle for two minutes and then vacuum fire at 1600 or 2048O C
• If bare areas are observed ,apply a second application of the ceramic metal agent, and fire using the same firing cycle.
• Apply aluminous porcelain core material ,condense it and fire it on the the treated refractory i.e as recommended by the manufacturer .
• As expected cracks are encountered in the aluminous porcelain with the first firing due to its inherent shrinkage. The ceramic metal agent , however remains intact and fuses to the aluminous porcelain, preventing loss of adaptation. Fill the cracks , and fire the die as in step no. 8

• Recover the core from the die with a blunt instrument under running water and ultrasonic cleaner. Thus , the refractory die is destroyed , leaving an aluminous core lined with the ceramic metal agent. This core can now serve as a coping.
• Return the coping to the working cast. Apply a suitable match of veneering porcelain , condense it , and fire it as recommended by the manufacturer.
Coat the master cast die with a thin layer of petroleum jelly to prevent subsequent intrusion of porcelain and condense it. Normally, the crown can be fired on ordinary stagger tray. However , to prevent any possible distortion on extremely thin aluminous cores, it is suggested that a second refractory die be utilized as a custom tray during subsequent firings.
Shaping and adjusting can be performed at this time , and the restoration can be stained and glazed

Master model with dies Platinum foil adapted to die
Dentin Ceramic additions
Finished Cores
Unsintered Crowns

Finished Crowns on dies Post-Cementation

THE CASTABLE AND MACHINABLE GLASS
DICOR was the first available castable ceramic marketed by Dentsply International. Dicor is a castable glass that is formed into an inlay, facial veneer, or a full crown restoration by a casting process similar to that employed for metals.

Dicor glass ceramic contains about 55 volume % of tetrasilicic fluormica crystals. The ceramming process results in increased strength and toughness, increased resistance to abrasion, thermal shock resistance, chemical durablity and decreased translucency.
Dicor MGC is a higher quality product that is crystallized by the manufacturer and provided as CAD - CAM blanks or ingots.
Advantages of Dicor: Ease of fabricationImproved aestheticsMinimal processing shrinkage
Good marginal fit

Moderately high flexural strengthGood marginal fitLow thermal expansion equal to that of tooth
structureMinimal abrasiveness to tooth enamel
Disadvantages of Dicor:Inability to be colored internallyIts limited use in low stress areas
DICOR PLUS AND WILLI’S GLASS –are two veneering materials to improve the colour of Dicor crowns.

Wax pattern Investing Burnout
450 0C for 1\2 hr
17500C for 1\2hr
Centrifugal casting machine
25000 F
Cast glass coping
Crystallised glass coping (after ceramming) 19000F for 1 ½ hr
Finished crown

PRESSABLE GLASS CERAMICS IPS EMPRESS is a glass - ceramic provided as
core ingots that are heated and pressed until the ingot flows into a mold. It contains a higher concentration of Leucite crystals that increase the resistance to crack propagation (fracture).
IPS EMPRESS AND IPS EMPRESS 2 are typical products of several other leucite reinforced and lithia disilicate reinforced glass ceramics respectively.
The use of glass ceramics in dentistry was first proposed by MacCulloch in 1968.


OPC is a leucite containing ceramic and OPC is a leucite containing ceramic and OPC 3G contains lithia disilicate crystalsOPC 3G contains lithia disilicate crystals

Advantages :1. Lack of metal2. Translucent ceramic core 3. Moderately high flexural strength 4. Excellent fit and aestheticsDisadvantages:1. Potential to fracture in posterior areas2. The need to use a resin cement to bond the
crown micromechanically to tooth structure
IPS EMPRESS


Wax pattern Investing
Burnout 8500C Ceramic ingots
Pressing under vaccum 11500CSprue removal

Full contour wax pattern Cut-back
Investing In-got pressing

IN-CERAM ALUMINA, IN-CERAM SPINELL AND IN-CERAM ZIRCONIA(SLIP CAST CERAMMING) The flexural strength values of the glass-infiltrated core materials are
approx. 350 MPa for In-Ceram spinell (ICS), 500 MPa for In-Ceram Alumina (ICA), and 700 MPa for In-Ceram Zirconia (ICZ) compared with strengths of 100-400 MPa for Dicor, Optec Pressable Ceramic, IPS Empress and
IPS Empress 2. A slurry of one of these materials is slip-cast on a porous refractory die
and heated in a furnace to produce partially sintered coping or framework.The partially sintered core is infiltrated with glass at 1100c for 4 hours to eliminate porosity and to strengthen the slip cast core.
The initial sintering process for the alumina core produces a minimal shrinkage because the temperature and time are sufficient to cause bonding between particles and to produce a desired level of sintering.Thus the marginal fit and adaptation of this core material should be adequate because little shrinkage occurs.

In-ceram spinell is indicated for use as anterior single unit inlays, onlays,crowns and veneers
In-ceram alumina is indicated for anterior and posterior crowns and anterior three unit FPD’s
In-ceram zirconia is indicated for posterior crowns and FPD’s.Because of its high level of opacity it is not recommended for anterior prosthesis.

Collective Advantages of the three glass infiltrated core materials are:
Lack of metalRelative high flexural strength and toughnessAbility to be used successfully cemented with any
cementIn-ceram spinell is the most translucent and
consists of glass infiltrated magnesium spinellIn-ceram zirconia contains 30 wt% zirconia and 70
wt% aluminaIn- ceram alumina contains 70 wt% alumina and 30
wt% sodium lanthanum glass

INCERAM ALUMINA ,INCERAM SPINELL AND INCERAM ZIRCONIA

Advantages of ICA include:
1. A moderately high flexural strength and fracture toughness
2.A metal free structure 3.Ability to be used successfully with conventional
luting agents
Disadvantages of ICA include :
1. marginal adaptation may not be too good2. relative high degree of opacity 3. inability to be etched4. technique sensitivity 5. relative great amount of skilled labour

STEPS FOR FABRICATING IN-CERAM PROSTHESIS
1. Prepare teeth with an occlusal reduction of 1.5 to 2 mm and a heavy circumferential chamfer(1.2mm)
2. MAKE AN IMPRESSION AND POUR two dies3. Apply alumina on a porous duplicate die4. Heat at 120C for two hours to dry alumina5. Sinter the coping for 10 hrs at 1120C6. Apply a sodium lanthanum glass slurry mixture on
the coping7. Fire for 4 hrs at 1120C to allow infiltration of glass8. Trim excess glass from the coping with diamond burs9.Build up the core with dentin and enamel porcelain10.Fire in oven,grind in the anatomy and occlusion,finish, and
glaze

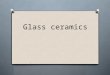
Al2O3 slip
Glass infiltration
Vita Inceramat3 Vaccumat 4000 Premium

Working model Duplication In-Ceram refractory dies
In-Ceram application Al2O3 slip Vita inceramat
10 hrs 1120 0C- 2hrs
Shrinkage of dies Glass infiltration 4hrs
11000CApplication of body and incisal porcelain

PROCERA ALL CERAM•The Procera Allceram crown is composed of densely sintered, high-purity aluminium oxide core combined with a compatible Allceram veneering porcelain. oThis ceramic material contains 99.9% alumina, and its hardness is one of the highest among the ceramics used in dentistry.

Step-by step ProcedureTooth preparation follows all-ceramic guidelines.The cast is made in the conventional way, but the
die is ditched to make the margin easier to identify during scanning.
The die is mapped using a contact scanner.The shape of the prepared tooth is transferred to
the computer screen .The design of the restoration is transferred to the
manufacturer via computer line.The production process starts with milling an
enlarged die to compensate for the sintering shrinkage.

An enlarged high-alumina coping is milled that shrinks to the desired shape after sintering.
The coping is returned to the laboratory, and body and incisal porcelains are applied in the conventional manner.


PROCERA ALLCERAMProcera Allceram can be used for Procera Allceram can be used for
anterior and posterioranterior and posterior
crowns, veneers, onlays & inlays.crowns, veneers, onlays & inlays.

A unique feature of the Procera systems is the ability of the Procera scanner to scan the surface of the prepared tooth and transmit the data to the milling unit to produce an enlarged die through a CAD-CAM process. The core ceramic form is dry pressed onto the die,and the core ceramic is then sintered and veneered.Thus the usual 15-20% shrinkge of the core ceramic during sintering will be compensated by constructing an oversized ceramic pattern,which will shrink during sintering to the desired size to accurately fit the prepared tooth.

MAGNESIA - BASED CORE PORCELAIN Magnesia core ceramic was developed as an experimental
material in 1985 (O' Brien - 1985). Its high thermal expansion coefficient (14.5 x 10-6/0C) closely matches the of body & incisal porcelains designed for bonding to metal (13.55 x 10-6/0C).
ADVANTAGES:•Adequate strength for most anterior crowns.•Esthetics superior to PFM for a given shade & technician(no metal margins, discoloration)•No risk in choosing alloy.
DISADVANTAGES :-• Not used for fixed partial dentures.• Requires learning to do good shoulder preparation

INJECTION-MOLDED HIGH-LEUCITE PORCELAINIn this process high-leucite porcelain ingot
cylinders are heated to 115O 0C to produce a plastic state. Then, the ingots are pressure-injected into the investment molds formed by the lost wax process for crowns, inlays-onlays and veneers.
• Due to the relatively high leucite content and pressure forming process, the flexural strength of porcelain formed by this process is around 200 MPa.
•The advantages of the process are good fit and higher strength for the resulting restorations.

PORCELAIN REPAIR
The general method for repair is as follows :-Establish a dry field.Remove the surface of adjacent remaining
porcelain with an abrasive bur.Treat the area to be repaired with etching gel,
& clean off.Silanize the ceramic surface with a silane
component.Apply metal bonding component over exposed
metal surfaces.Apply bonding resin to the entire area Repair the restoration with composite component
& cure.

SHRINK-FREE CERAMIC
Ralph B.Sozio ,and Edwin j.Riley: THE SHRINK-FREE CERAMIC CROWN:J Prosthet Dent ,February 1983,volume 49, number 2(182-187)
The alumina ceramic used in this technique (Cerestore Non-shrink Alumina Ceramic,Coors Biomedical Co., Lakewood, Colo.) is a shrink-free composition unlike conventional ceramic bodies, which undergo considerable shrinkage when fired .
INDICATIONS AND CONTRAINDICATIONS
•Indicated in situations where the ceramometal restoration with porcelain occlusal or the traditional porcelain crown are the treatment selection.
•effectively used as both anterior and posterior restorations
•contraindicated when there is inadequate thickness, i.e. less than 1.3 mm.

ADVANTAGES: Excellent fit generated by direct molding. Excellent esthetics aided by light transmission and lack of metal. Absence of distortion with the veneer application. Ease of formation.
• Ease of adjustment in green state• Low thermal conductivity.
•Radio density similar to that of natural enamel.

CAD – CAM CERAMICS In this system ,the internal surface of inlays,onlays,or
crowns is ground with diamond disks to the dimensions obtained from a scanned image of the preparation.The translational movements of the disk is guided by
computer-controlled input.DISADVANTAGES• need for costly equipment,• lack of computer-controlled processing support for
occlusal adjustment• technique sensitive nature of surface imaging required for
preparing teeth.

CEREC SYSTEMThe Cerec system has been marketed for several years with
the improved Cerec 2 system introduced in the mid-1990s.The equipment consists of a computer integrated imaging and milling system, with the restorations designed on the computer screen. At least three materials can be used with this system: Vita Mark II, Dicor MGC, ++ and ProCod. Vita Mark II contains sanidine (KAISiO) as a major crystalline phase within a glassy matrix. Dicor MGC us a mica -based machinable glass-ceramic that contains 70 volume percent of crystalline phase. The unique “house of cards” microstructure found in Dicor MGC is due to the interlocking of the small platelet-shaped mica crystals with an average size of 1 to 2 um.

This particular microstructure leads to multiple crack deflections and ensures a greater FRACTURE RESISTANCE than leucite-containing ceramics. ProCod is a leucite-containing ceramic designed for making machined restorations. Weaknesses of the earlier Cerec system include the poor marginal fit of the restorations. And the lack of sophistication in the machining of the occlusal surface. The marginal adaptation of Cerce 2 is improved, and the occlusal anatomy can be shaped.

ADVANTAGES negligible porosity levels freedom of making an impression reduced assistant time assosiatd with
impression procedures the need for only a single patient appointment Good patient acceptance.one can select a core
ceramic either for strength and fracture resistance,for low abrasiveness,or for transucency.


CERCON AND LAVA ZIRCONIA CORE CERAMICSThe material that has the greatest potential fracture
toughness and flexural strength is pure tetragonal stabilized zirconia.
The zirconia coping or framework is placed in a Cercon furnace and fired at 1350C for 6 hrs to fully sinter the yttria-sabilized zirconia core coping or framework.
The ssintering shrinkage is achieved uniformly and linearly in the three dimensional space by the integrated process of scanning,enlarging the pattern design,controlled milling ,and sintering. After subsequent trimming with a water cooled ,high speed diamond bur , the finished ceramic core framework is then veneered with a veneering ceramic and stain ceramic.

ABRASIVENESS OF DENTAL CERAMICSCeramics are generally considered the most
biocompatible durable and aesthetic materials available for rehabilitation of teeth occlusal function and facial appearance. In spite of their overall excellence in meeting the ideal requirements of a prosthetic material, dental ceramics have one major drawback. These materials can cause catastrophic wear of opposing tooth structure under certain conditions. The most extreme damage occurs when a roughened surface contacts tooth enamel or dentin under high occlusal forces, which may occur because of bruxing premature occlusal contacts, and/or inadequate occlusal adjustments.

Abrasive wear mechanisms for dental restorative materials and tooth enamel include
(1) adhesion (metals and composites), in which localized bonding of two surfaces occurs, resulting in pullout and transfer of matter from one surface to the other, and
(2) microfracture (ceramics and enamel), which results from gouging asperities, impact, and contact stresses that cause cracks or localized fracture.
The microfracture mechanism is the dominant mechanism responsible for surface breakdown of ceramic and the subsequent damage that a roughened ceramic surface can cause to tooth enamel surfaces.

Enamel is also susceptible to this kind of microfracture through four specific mechanisms :
(1) asperities extending from the ceramic surface that produce high localized stress and mircofracture;
(2) gouging that results from high stresses and large hardness differences between two surfaces or particles extending from these surfaces;
(3) impact or erosion that occurs through the action of abrasive particles carried in a flowing liquid such as saliva; and
(4) contact stress microfracture that increases localized tensile stress and also enhances the damage caused by asperities, gouging, and impact or erosion.

Reducing abrasiveness of ceramics by polishing and glazing
Jagger and Harrison (1994) reported that the amount of enamel wear produced by both glazed (28.8 micro m) and unglazed Vitadur N aluminous porcelain (29 micro m) was similar; however, the wear produced by polished porcelain (12 micro m) was substantially less. Polished or glazed porcelain caused significantly less wear than unglazed porcelain. Polishing was accomplished with 3 M Soflex disks and Shofu rubber points.
Hulterstrom and Bergman (1993) found that two of the best polishing systems are Sof-Lex (3M Dental) and Shofu Porcelain Laminate Polishing kit followed by diamond paste.

Guidelines for minimizing excessive wear of enamel by dental ceramics
To minimize the wear of enamel by dental ceramics,the following steps should be taken:
Ensure cuspid-guided disocclusionEliminate occlusal prematurities Use metal in functional bruxing areasIf occlusion in ceramic ,use ultralow fusing
ceramicsPolish functional ceramic surfacesRepolish ceramic surfaces periodicallyReadjust occlusion periodically if needed

CRITERIA FOR SELECTION OF DENTAL CERAMICSCRITERIA FOR SELECTION OF DENTAL CERAMICS
1. The dentist should not use all-ceramic crowns for patients with evidence of extreme bruxism, clenching, or malocclusion. In this case, metal-ceramic or all metal prostheses should be used.
2. The experience of the laboratory technician should be extensive to ensure a success rate of at least 98% over a 3-year period. 3. The dentist should judge whether previous aesthetic success with metal-ceramic prostheses combined with the aesthetic demands of the specific patients would yield more predictable outcomes and longevity than an all ceramic crown.4. Use all-ceramic crowns when adjacent anterior teeth exhibit a high degree of translucency. Ceramic systems are useful for matching adjacent tooth shades for young patients

5. Patients must accept the described benefits, risks, and alternatives to the proposed treatment, and they must give their consent for the treatment to be performed .The initial cost and the expenses associated with remakes for the ceramic crowns will be higher than those associated with metal-ceramic crowns.
6. Some ceramic crowns will not be aesthetic if the tooth preparations are inadequate, particularly when insufficient tooth structure has been removed .
Patients with shorter crown height should not be treated with ceramic FPDs because inadequate connector for height will increase the risk for connector fracture.
7. The skill of the dentist is of paramount importance in producing perfect impressions derived from smooth preparations free of undercuts with continuous, well-defined margins and with adequate tooth reduction.

JOURNAL OF ORAL REHABILITATION 2003
Fracture reasons in ceramic-fused-to-metal restorations
M. O¨ ZCAN
SUMMARY
Fracture of the ceramic veneers as a result of oral function or trauma is not an uncommon problem in clinical practice . Fractures in the anterior region pose an aesthetic problem, but when they are in the posterior, chewing function could also be affected. The published literature reveals that reasons for failures cover a wide spectrum from iatrogenic factors to laboratory mistakes or because of factors related to the inherent structure of the ceramics or simply to trauma.

JADA, VOL. 137 APRIL 2006
Fracture resistance of different partial-coverage ceramic molar restorations
Christian F.J. Stappert,
Within the limits of this investigation, we can conclude the following:All-ceramic PCRs for molars made of IPS e.max Press are fracture-resistant, showing results comparable with those of natural unprepared teeth.A defect-oriented tooth preparation in the posterior region for the restoration of a compromised tooth with a partial-coverage ceramic restoration is justifiable.

JADA, VOL. 136 NOVEMBER 2005
A simplified rubber-dam technique for preparing teeth for indirect restorationsGRANT A. PERRINE
The slit–rubber-dam technique involves the use of a common dental armamentarium to simplify the preparatory phase of indirect restorative procedures. The slit dam enhances visibility enables the practitioner to retract and protect the soft tissues, helps prevent the patient from swallowing or aspirating the tooth or restorative materials, controls oral fluids and promotes operating efficiency. This simple technique considerably reduces the stress for the dentist, dental assistant and patient.

JOURNAL OF PROSTHODONTICS,VOL16,NO3(MAY-JUNE),2007
Effect of Water Storage and Surface Treatments on the Tensile Bond Strength of IPS Empress 2 CeramicLucianaA.Salvio,
Conclusions:Storage time significantly decreased the tensile bond strength for both ceramic surface treatments. The application of 10% hydrofluoric acid resulted in stronger tensile bond strength values than those achieved with aluminum oxide.

JOURNALOFPROSTHODONTICS,VOL14,NO4(DECEMBER),2005
Comparison of Bond Strength of a Pressed Ceramic Fused to Metal versus Feldspathic Porcelain Fused to Metal
DanielM.Schweitzer,DDS;
Conclusion:
The debonding/crack initiation strength of a low-fusing pressable leucite-based glass ceramic fused to metal was equivalent to that of a feldspathic porcelain fused to metal.

J PROSTHOD 1994
In Vitro Fracture Behavior of Ceramic and Metal-Ceramic Restorations
Thomas B. Smith, Ohn A
Conclusions:
Failure for both restorative systems involved interfacial stresses with crack propagation occurring at or near the core-veneer interface. The weaker interface in the Metal- ceramic system probably resulted from an increase in surface oxide volume. For the ceramic crowns, delamination crack fronts appeared to propagate through chemically unaltered veneering porcelain.

International Association for Dental Research (June 25-28, 2003)
In vitro Fracture Strength of Teeth Restored with Different Procera All-ceramic Crowns
Conclusions:
Alumina, zirconia, and metal copings offer the same fracture resistance for teeth restored with resin-bonded all-ceramic or porcelain-fused-to-metal crowns.

International Association for Dental Research (June 25-28, 2003)
Marginal Fit of a Low-fusing Pressable Leucite Glass Ceramic in Full Crowns and Ceramic-pressed-to-Metal Crowns
N.W. BOYD, G.R. GOLDSTEIN
Conclusion:
The marginal fit of the PCCs and the PTMs were similar to conventional PFMs.

International Association for Dental Research (June 25-28, 2003)
Comparison of Tensile Bond Strength of a Pressed Ceramic to Metal vs. Feldspathic Porcelain Fused to Metal
G.R. GOLDSTEIN, N.R.F.A. DA SILVA,
Conclusion:
The TBS of a low fusing pressable leucite glass ceramic was equivalent to that of a feldspathic porcelain fused to metal.

International Association for Dental Research (June 25-28, 2003)
Effect of Sodium Content on the Mechanical Properties of Glass-ceramics
I.DENRY,
Conclusion:
The crystalline phase combination was optimum with 1.9 wt% sodium, leading to the highest apparent fracture toughness.

International Association for Dental Research (June 25-28, 2003)
Effect of Ion Exchange on Flexural Strength of Feldspathic PorcelainsN. JUNTAVEE
Conclusions:
The study indicated that flexural strength of porcelain was treatment is enhanced by ion treatments, except for Li+ ion process. The Li+-Rb+ ion the most effective technique.

International Association for Dental Research (June 25-28, 2003)
Fracture Strength of Composite and All-ceramic CAD-CAM Crowns
Conclusions:
Cyclic loading fatigue reduced the fracture strengths of composite and all-ceramic crowns, while adhesive cementation increased the fracture strengths.

J Prosthod 1995;4: 101- 110
A Comaprison of Infrared and Torch soldering of Au-Pd and Co-Cr Metal-Ceramic Alloys Using a High-Fusing Solderohn T. Dominici, DDS, MS
Conclusions: Although the two heating methods produced solder joints that had strengths that were not significantly different, infrared-heated joints showed less scatter in bond strengths. It was suggested that, in the hands of most technicians, fewer infrared-heated joints would contain defects visible at a magnification of 40x. The presence of such defects may increase the probability of in vivo failure caused by cyclic stresses.

BIBLIOGRAPHY
•Contemporary fixed prosthodontics – Rosenstiel•Phillips science of dental materials – Anusavice•Fundamentals of fixed prosthodontics – Schillingburg•Contemporary esthetic dentistry - Bruce J. Crispin•Esthetic dentistry: an artists science - Ratnadeep Patil•JPD 1996;75:18-32•JPD 2004;91:136-43•Quint Int 1991; 22: 257-262. •Quint Int 2005; 36: 141-147•Operative dentistry 1990;15:61-70 •Int J Periodont Rest Dent 1998;18:587-593•JOR 2005;32:180-187
•JPD 2002;87:133-135•Dent Mater 2000;16:226-233•JPD 2000;83:530-534•Quint Int 1985;3:135-141•JPD 1991;66:754-758•Dent Mater 2002;18:380-388•JPD 1991;66:747-753•J Dent 1990;18:227-235•Quint Int 1998;29:285•Int J Prosthod 1997;10:478•J Prosthet Dent 1999;81:277•Quint Int 1991;22:257-262•Int J Prosthod 1992;5:9-16