Embed Size (px)
Citation preview

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
c
Holly Rimmasch2016
Clinical Integration

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Objectives● Understand the importance of having a clinically
integrated organizational structure to support systematic improvement and sustainability
● Describe key roles and processes critical to sustained improvement methodology
2

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 3
"Every system is perfectly designed to get the results it gets.” - Dr. Paul Batalden
Organize around process. - William Edwards Deming
... so re-design your system to get better results

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Three Systems for Improvement
4
What should we be doing? How are we doing?
How do we transform?Clinical Integration

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Clinical Integration● What is it?
‒ The organization around clinical processes to facilitate clear accountabilities for care across the continuum
● Why is it important?‒ Our core business is providing value
through better clinical care.
8

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 6
Another emerging definition-
For many who work on the front lines of delivery system reform, clinical integration is not a generic phrase to describe health care professionals working more closely together. It’s a specific type of legal arrangement that allows hospitals and physicians to collaborate on improving quality and efficiency, while remaining independent entities.
Advisory Board
We are not going to spend time today diving into the legal arrangement

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 7
Typical Healthcare System?Just some examples…
Departments
Executive Leadership
Executive CEO
CFO
HR Finance
COO
Departments Departments
Executive Leadership
Executive CEO
CFO
HR Finance
COO
Departments
Hospital or Healthcare system
Clinics

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 8
Budgeted Departments- examples• Nursing
• Medical Surgical Units• Intensive Care Units
• Pharmacy
• Respiratory Therapy
• Physical Therapy
• Emergency Department
• IT
• Sourcing (purchasing)
• Care Management
• Medical Group/Physician Division
• Clinics
• Home Care
• Rehabilitation
• Cardiovascular (Cath labs, echo, EKG, etc)
• Radiology
• Quality
• Finance
• Environmental Services
• Medical Group
• Laboratory
• Food & Nutrition
• Health Information Management
Is this enough ?

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 9
Heart Failure Readmissions14% reduction in 90-day readmits
21% reduction in 30-day readmits
2X increase in phone calls 48 hours
63% increase in med reconciliation

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 10
Reducing Sepsis Mortality
22% reduction in sepsis mortality
$1.3 million in savings

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Improved ACO Care CoordinationAdvanced Care Planning
64% increase in high-risk patients with ACPs
1,243 high-risk patients with ACPs
980 physicians and community facilitators engaged
Integrated EDW solution in a heterogeneous EHR environment
5

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Key Functions of a Clinically Integrated System
● Create a shared vision● Create integrated information systems● Integrate clinical and operations management structure● Integrate incentives and cost structures
11

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 13
Poll QuestionPlease rate your organization. How integrated are your clinical and operational management structures? – 201 respondents
1. 100%-- we are there! – 2%
2. 75%-- we are getting there! – 11%
3. 50%-- we are well on our way – 33%
4. 25%-- we are not too far on this journey – 34%
5. Don’t know – 20%

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Outcomes Improvement Organizational Structure
14
Provides domain oversight and recommended prioritiesGUIDANCE
TEAM (S)
Leads specific outcomes improvement discovery intervention design and implementation. Lead unit based change
OUTCOMES IMPROVEMENT
TEAM (S)
Assigned specific discovery and intervention design work by OIT e.g. order set, new workflow
WORKGROUP (S)
Supports developmentof clinical content and
supporting analytics
CONTENT ANDANALYTICS
TEAM (S)
Provides overall governance, prioritization, and cultural change leadership for all outcomes improvement
CLINICAL OUTCOMES IMPROVEMENT
LEADERSHIP TEAM
ENSURETHAT…
• Governance and Teams are appropriately empowered to make decisions• Outcomes Improvement Teams are created based on organizational improvement priorities• Teams are cross discipline, permanent and include the right stakeholders
DATA GOVERNANCE TEAM
Provides overall governance over
the 6 phases of Data Governance

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Accountabilities:
• Provides overall governance, prioritization, and cultural change leadership for all outcomes improvement
• Establishes clinical integration (clinical programs, clinical services, patient quality, and safety) and clinical improvement work
• Represents the continuum of clinical services
• Recommends clinical board-levelgoals
• Reviews progress and remove roadblocks
Clinical Outcomes Improvement Leadership Team
14

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Clinical Outcomes Improvement Leadership TeamMembership should represent key stakeholders in system (e.g., acute, ambulatory, MD division):
• Chief Medical Officer (CMO) or VP of Medical Affairs
• Chief Nursing Officer/Executive or VP for Nursing
• Chief administrators or operational officers
• Other key stakeholders− IT, Finance, Patient Quality, and Safety, ACO, Population Health,
etc.
− Leadership representing Clinical Programs (CV, Pediatrics) and Clinical Support Services (pharmacy, lab)
16

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 17
Clinical Programs: Ordering of Care
Community Care
Care Process Families
e.g., Diabetes
Cardio-vascular
Care Process Families
e.g., Coronary
Artery Disease
General Medicine
Care Process Families
e.g., Sepsis
Respiratory
Care Process Families
e.g., Obstructive
Lung Disorders
Neuro-sciences
Care Process Families
e.g., Back and Neck Pain
Surgery
Care Process Families
e.g., Head Injury
Hematology /Oncology
Care Process Families
e.g., GI Neoplasm
Behavioral Health
Care Process Families
e.g., Depressive Disorders
Women and Newborns
Care Process Families
e.g., High-Risk
Pregnancy
Gastro-intestinal
Care Process Families
e.g., Pancreatic Disorders
Musculo-skeletal
Care Process Families
e.g., Osteoarthritis

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 18
Community Care
Care Process Families
e.g., Diabetes
Cardio-vascular
Care Process Families
e.g., Coronary
Artery Disease
General Medicine
Care Process Families
e.g., Sepsis
Respiratory
Care Process Families
e.g., Obstructive
Lung Disorders
Neuro-sciences
Care Process Families
e.g., Back and Neck Pain
Surgery
Care Process Families
e.g., Head Injury
Hematology /Oncology
Care Process Families
e.g., GI Neoplasm
Behavioral Health
Care Process Families
e.g., Depressive Disorders
Women and Newborns
Care Process Families
e.g., High-Risk
Pregnancy
Gastro-intestinal
Care Process Families
e.g., Pancreatic Disorders
Musculo-skeletal
Care Process Families
e.g,Osteoarthritis
Clinical Support Services: Delivery of Care Ordered
Diagnostic Clinical Support Service (workflow models)(e.g., Pathology and Laboratory Medicine, Diagnostic Radiology)
Therapeutic Clinical Support Service (workflow models)(e.g., Pharmacy, Transfusion Medicine, Respiratory Therapy, Physical, Occupational, Speech Therapy)
Ambulatory Operations (workflow models)(e.g., Primary Care Clinics, Chronic Disease Specialty Clinics, Sub-specialty Clinics)
Capacity Management (workflow models)(e.g., Emergency Care, ICU/CCU/NICU/PICU, General Med-Surg)
Invasive Clinical Support Service (workflow models)(Interventional Medical [e.g., cath lab, interventional radiology, GI lab, L&D, rad onc] and Surgical [e.g., amb, IP])

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
19
Heart Rhythm Disorde
rs
Vascular
Disorders
Ischemic Heart Disease
HeartFailure
CARDIOVASCULAR
Level B:Care Process
Families
Level A: Clinical
Program
CardiacValve
DisordersCHF
Cardio-myopath
y
Pulmonary Heart Disease
Level C: Care
Processes
SystolicDysfuncti
onDiastolic
DysfunctionLevel D: Care
Sub-Processes
ICD-9 and ICD-10Diagnosis Codes
ICD-9 and ICD-10
Procedure Codes
CardiacValve
Procedures
Car
e-Le
vel H
iera
rchy

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
20
Heart Rhythm Disorde
rs
Vascular
Disorders
Ischemic Heart Disease
HeartFailure
CARDIOVASCULAR
Level B:Care Process
Families
Level A: Clinical
Program
CardiacValve
DisordersCHF
Cardio-myopath
y
Pulmonary Heart Disease
Level C: Care
Processes
SystolicDysfuncti
onDiastolic
DysfunctionLevel D: Care
Sub-Processes
ICD-9 and ICD-10Diagnosis Codes
ICD-9 and ICD-10
Procedure Codes
CardiacValve
Procedures
Clin
ical
Impl
emen
tatio
n Te
ams Guidance Team
Clinical Implementation Team
Work Groups
CV
CareProcessFamilies
e.g.,coronary artery
disease
=

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Care Process Pareto AnalysisCardiovascular Clinical Program
Top 13 Care ProcessesMiddle 27 Care ProcessesBottom 45 Care Processes
Adult_CareProcess Adult_CareProcessFamily Adult_ClinicalProgramNormalized Revenue % of All CPs
Running % of All CPs
Coronary artery disease Ischemic heart disease Cardiovascular $28,516,437 4.47% 4.47%Congestive heart failure Heart failure Cardiovascular $10,935,531 1.71% 6.18%Arterial aneurysm, dissection Vascular disorders Cardiovascular $8,838,347 1.39% 7.57%Cardiac valve disorders Heart failure Cardiovascular $8,095,210 1.27% 8.84%Vascular insufficiency Vascular disorders Cardiovascular $5,918,680 0.93% 9.76%Atrial fibrillation, flutter and other supraventricular tachyarrhythmiasHeart rhythm disorders Cardiovascular $4,972,392 0.78% 10.54%Venous phlebitis, thrombosis, embolismVascular disorders Cardiovascular $2,808,147 0.44% 10.98%Ventricular tachyarrhythmias Heart rhythm disorders Cardiovascular $2,702,363 0.42% 11.41%Pulmonary embolism Heart failure Cardiovascular $2,599,832 0.41% 11.81%Complication of vascular device, implant or graftVascular disorders Cardiovascular $2,304,288 0.36% 12.18%Sick sinus and conduction disordersHeart rhythm disorders Cardiovascular $1,892,212 0.30% 12.47%Peripheral vascular disease Vascular disorders Cardiovascular $1,860,751 0.29% 12.76%
24

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% of Total Cumulative %
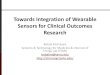
Pareto Analysis >> Prioritization
22
X-Axis = Care Processes by resources consumed (High to Low)
Y-A
xis
= Pe
rcen
t of t
otal
reso
urce
s co
nsum
ed
Top 85 Care Processes account for 80% of the opportunity (+45)
Top 40 Care Processes account for 62% of the opportunity (+27)
Top 13 Care Processes account for 34% of the opportunity

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Internal Variation versus Resource Consumption(Excel Example shown)
Y- A
xis
= In
tern
al V
aria
tion
in R
esou
rces
Con
sum
ed
Bubble Size = Resources Consumed
Bubble Color = Clinical DomainX Axis = Resources Consumed
1
2
3
4

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Accountabilities:
• Provides domain oversight and recommended priorities
• Develop and implement best practices across the continuum within domain (i.e. heart failure from prevention through treatment and maintenance)− Each clinical program is assigned accountability for care process families
and related care processes
• Recommend board and clinical program goals
• Prioritize resources
• Determine order and timing for creation of teams to support goals
• Ensure best practices are diffused and sustained systemwide
• Review and report progress; remove barriers
Guidance Team
30

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 25
Guidance Team
Chaired by physician and nurse director with domain expertise. Team membership should include:
• Physician, nurse director, and administrator from each cluster representing domain
• Knowledge manager, data architect/analyst
• Other key stakeholders:− IT, Finance, Patient Quality, and Safety

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Permanent Teams Characteristics
= Subject Matter Expert= Data Capture= Data Provisioning & Visualization= Data Analysis
Women & Children’s Clinical Program Guidance Team
Pregnancy
MD LeadRN SME
Knowledge Manager
DataArchitect
Application Administrator
RN, Clin Ops Director
Guidance Team MD lead
Normal Newborn
MD LeadRN SME
Gynecology
MD LeadRN SME
• Organized permanently for long term improvement• Integrated clinical and technical members• Supports multiple care process families• Choose innovators and early adopters to lead
Innovators
Early Adopters

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
DATA CAPTURE
• Acquire key data elements• Assure data quality• Integrate data capture into operational
workflow
DATA ANALYSIS
• Interpret data• Discover new information in the data
(data mining)• Evaluate data quality
DATA PROVISIONING
• Move data from transactional systems into the data warehouse
• Build visualizations for use by clinicians• Generate external reports (e.g., CMS)
Knowledge Managers (data quality, data stewardship, and
data interpretation)
Application Administrators (optimization of source systems)
Data Architects(infrastructure, visualization, analysis, reporting)
= Subject Matter Expert= Data Capture= Data Provisioning= Data Analysis
Critical Key Functions to Consider…
41

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 28
Outcomes Improvement TeamAccountabilities:
• Leads specific outcomes improvement discovery intervention design and implementation. Lead unit based change• Provide broad feedback to smaller workgroup teams on aims,
metrics, and best practices
Membership:
• Broad representation across your system (facilities, clinics, regions) and should include members with deep knowledge and experience:− Physician leader
− Nurse subject matter expert
− Other disciplines (respiratory therapy, finance, lab, etc.)

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 29
Workgroup TeamAccountabilities:
• Assigned specific discovery and intervention design work by OIT e.g. order set, new workflow
• Responsible for the “heavy lifting” related to improvement− Targeted on care process or care sub-process
− Integrate best practices; build key metrics
− Report and request input from Outcomes Improvement Team
Membership:
• Small integrated team of domain experts (physicians, nurses, finance) and analytical/technical experts− Data architects/analysts
− Application administrators

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Improvement Cycle
30
Prerequisites
Recruit team Train team
• Solicit front line plan input
• Finalize analytics dev, testing, and rollout support
• Finalize intervention rollout plan
• Guidance team validation
Rollout
• Review initial results• Identify, approve any
modifications to intervention rollout
• Review lessons learned
• Create next AIM statement
• Repeat process
Results
• Finalize cohort• Identify intervention(s)• Direct observation• Solicit front line input
on AIM and intervention
• Define intervention rollout plan
• Guidance team validation
Intervention
• Review visualized drafts of AIM cohort findings
• Identify data quality issues
• Direct observation• Prioritize and select
AIM #1• Review cohort criteria
and visualizations • Guidance team
validation
AIM
• Confirm team mission, charter, roles
• Review AIM options• Gather best practices• Profile and visualize
preliminary data• Select 2-3 potential
AIMs• Guidance team
validation
Kickoff
Select Build and Refine Build and Refine Build and Refine
Rollout Date
MajorMilestones
Work Streams
7. Measure Progress
1. Best Practices
2. Define Cohort
3. AIM Statement
4. Design Metrics
5. Rollout Plan
6. Rollout
Rollout Date

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Identify Potential ImprovementsProcess AIMs and Outcome Goals
Transformation Process
Starter Set Content
Implement Intervention
Measure & Sustain
Review & Select AIM Define Cohort
Iterate on Metrics
Heart Failure: AIM #1
Starter Set Content
Implement Intervention
Measure & Sustain
Review & Select AIM Define Cohort
Iterate on Metrics
Heart Failure: AIM #2
Process Improvement AIM:Improve Follow-up Visit SchedulingFrom 43% to 90% by October 31, 2015
Process Improvement AIM: Improve Medication ReconciliationFrom 58% to 80% by June 30, 2015
Heart Failure Outcome Improvement Goal:Reduce Readmissions = Reduce the readmission rate for the HF population from 30% to 20% by December 31, 2015
2-4 Process Improvement AIMS should produce a significant outcome improvement

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Actionable Visualizations
47

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Permanent Improvement Team Temporary Project Team
Team Structure Options
Pros● Proactive
(strategic investment)● Predictable Cost● Team member establish long
term relationship● Implementation improved● Sustainability improved● Partnership established on
technical priorities
Cons● “Feels” more expensive, actually
saves money long term● True cultural shift
Cons● Difficult to maintain
sustainability● Variable Cost● Speed to trust slower in
temporary teams● Need to reorient team members
don’t always understand context within domain
Pros● “Feels less expensive” one time
cost to fix (not typically true)● Less time to start initially

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 34
Priority Management• Intake process to manage strategic and tactical information
requests of EDW team
Data Stewardship• Legislation of standard definitions
• Quality management processes
• Security/authorization
• Master data management
Data Governance Categories
Executive Oversight
IT Leadership

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 35
Content & Analytics TeamAccountabilities:
• Supports development of clinical content and supporting analytics• Develop the analytic and knowledge management infrastructure needed to support
process and outcomes improvements in clinical, operational, financial and patient experience across all domains of clinical integration.
• Create consistency across clinical programs and clinical support services• Patient & Provider education related to development of best practices, guidelines, etc.
• Align priorities and resources to system goals
Membership:• Chair examples: CMIO, CQO, chief patient safety officer, chief
knowledge officer• Lead data architects and knowledge mangers• Provider and patient education specialists• Lead administrative and clinical application stewards

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Care Improvement MapSepsis and Septic Shock

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential 37
Are your data governance and content & analytics resources aligned with your improvement outcome goals? – 179 respondents
1. Yes – 6%
2. Mostly – 14%
3. Sometimes – 44%
4. No – 18%
5. Don’t know – 18%
Poll Question

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
= Subject Matter Expert
= Data Capture
= Data Provisioning & Visualization
= Data Analysis
Small Teams (Designs)• Meet weekly in iteration planning meeting• Build DRAFT processes, metrics, interventions• Present DRAFT work to Broader TeamsOB
Guidance Team
• Meet quarterly to prioritize allocation of resources• Approves improvement AIMs • Reviews progress and removes road blocks• Monitors and tracks progress and sustainability
OB Newborn GYN
W&N
W&N
Broad Teams (Implements)
• Broad RN and MD representation across system• Meet monthly to review, adjust and approve DRAFTs• Lead rollout of new process and measurementOB
W&N
W&N
W&N
Executive Leadership Team
• Prioritizes sequence of formation of Guidance Teams• Approves Board Level Outcomes Goals• Reviews progress and removes road blocks
GUIDANCE TEAM (S)
OUTCOMES IMPROVEMENT
TEAM (S)
WORKGROUP (S)
CLINICAL OUTCOMES IMPROVEMENT
LEADERSHIP TEAM
(Prioritizes Innovations)

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
Key Success Factors/Lessons Learned• Leadership
• Integration of technical, clinical, and operations
• Dedicated resources− Clinical leadership, domain expertise, operational expertise, Data
Managers, analytic resources
• Permanent structures and processes/systematic approach− Change from “project” to “the way we live”
• Deep culture of quality and improvement; consistent methodologies
• Transparency
• Integrated key concepts into current work/teams/structures
• There are many ways to put this puzzle together
• This is a journey!
59

© 2015 Health Catalystwww.healthcatalyst.comProprietary and Confidential
© 2013 Health Catalyst | www.healthcatalyst.com
Thank you