Embed Size (px)
Citation preview

Case Discussion
Muhammad Asim RanaBSc, MBBS, MRCP, MRCPS, FCCP, EDIC, SF-CCM
Department of Critical Care MedicineKing Saud Medical City
Comatose Patient

Clinical Summary
• You are the on call ICU Registrar and are covering the night shift.
• You have almost finished your energy reserves at around 4 am, after finishing wards round and just came back to the ICU doctors room and thrown your self in chair when the bleep rings
Why does Asim like such worst scenarios always?

History• 34 years old male Indian patient• Car mechanic by profession• Brought to A & E by Red Crescent• No past medical history• No attendant available.• Patient was found unconscious in the workshop and they
found empty bottle of radiator fluid near him.• ER called MSP and he has called you as patient is
unconscious

Dilemma continues
• ER and MSP are looking at you to take him to ICU because of low conscious level.
• What you are supposed to do?1. Fight with ER & MSP that why they have not
assessed the case before calling you2. Read the file……3. Call your senior4. Start examining the patient
Very Bad Senior Again!!!

Causes of COMA
StructuralOR
Surgical
•DIFFUSE DAMAGE TO BOTH HEMISPHERES•VASCULAR DAMAGE• INCREASED ICP
MetabolicOR
Medical
Diffuse insult to both cerebral hemispheres by toxins, either from within or from outside

Alco
hol
Epile
psy/
Expo
sure
Insu
lin (D
iabe
tic)
Ove
rdos
e/O
xyge
n lo
w
Ure
mia
(kid
ney
failu
re)
Trau
ma/
Head
Inju
ry
Infe
ction
or I
atro
geni
c
Psyc
hosis
or p
oiso
ning
Stro
kesA E I O U T I P S
Causes of COMA

Clinical Summary• You see him wearing a single T-Shirt and Trousers with very cold
weather out side, otherwise GPE is unremarkable. You are told pt has been having diarrhea
• Vitals: – Temp 32⁰C, BP 130/85, HR 129/min regular, SpO2 87% on 10 liters per
min NRM• CNS:
– GCS: E1M5V2
– No lateralization– No signs of meningeal irritation– Pupils bilaterally constricted equal and reactive– Bilateral up going planters

Clinical Summary
• Cardiovasular Exam:– Unremarkable except for tachycardia, auscultation
normal• Abdomen: – Unremarkable, the patient vomited while you were
examining the abdomen-coffee ground• Respiration:– Decreased Rt sided movements with decreased air
entry on Rt lower zone especially in Rt axillary area with coarse crepts and broncheal breathing

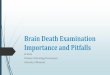
Chest X-Ray

Laboratory Investigations
• CBC.. Hb% 14, WBCs 12, Platelets 230• Na 140. K 6.6, Cl 109, Blood Glucose 200mg%• BUN 28, Creatinine 344• CK 8700, ALT 77, AST 92, ALP 150, Billir 17• Amylase 23, Lipase 12• Hepatitis viral markers negative• HIV negative

Wha
t you
will
do
now
? • Think of the steps you have to take as an Intensivists:
• Need to know Diagnosis or ???• Intubation and securing the airway?• Reviewed the labs… What next?• Looked at CXR.. What is this?• What next?• What antibiotics?• What we are missing?• Hypothermia needs attention or NO?

What else do you need?
Ct Brain Normal
CSF analysisProteins 34, LDH 12, Sugar 67mg% (RBS 200mg%), Cell count 3, all lymphocytes.Latex negative

Any thing else you would ask for?
ABGs:pH 7.77, PaCO2 35.5, PaO2 57, HCO3 50.6
Check Internal data for consistency[H+]= 24 x PaCO2/HCO324 x 35.5/50.6= 16.8[H+]=7.8-pH x 1007.8-7.77x 100= 3

Venous Blood Gas Repeated
• pH 6.878, PaCO2 20, PaO2 27.2, HCO3 4• What is the impression now?• How do we analyze the Blood Gas results?• The six steps approach• Although there is much to discuss about
reading blood gases…

Step-wise Approach
1. Acedemia or Alkalemia2. Metabolic or Respiratory3. For metabolic is it anion gap or non anion gap.4. For anion gap acidosis,is it associated with
other disturbances.5. What is the respiratory compensation for the
metabolic disturbances.6. For respiratory disturbances is it acute or
chronic.

Step-wise Approach • Step1:• Acidemia or Alkalemia?• Acidemia• Step2:• Metabolic or Respiratory?• Metabolic• Step3:• Is there anion gap or no?• 140-109+4=27• Yes high anion gap metabolic acidemia

High Anion Gap Metabolic Acidemia
• M• U• D• P• I• L• E• S

High Anion Gap Metabolic Acidemia
• Methanol• Uremia• DKA• Paraldehyde• Ischemia, Iron, INH, Isopropyl alcohol• Lactic acidosis• Ethylene glycol• Salicylates

Back to Brain Exercise
• What could be the cause in our patient? • Yes, He might be a case alcohol ingestion!!• Which Alcohol?• Methanol, Ethanol, Ethylene glycol, Isopropyl
Alcohol• How will you proceed further?• Check Serum Osmolality, Urine for?• Why & which one,.. Calculated or measured?

Continue The Thinking Process
• Osmolal Gap = Measured osmolarity - Calculated osmolarityNormal 0 - 10. Abnormal > 10.
• Calculated osmolarity =2 x (Na+) + BUN/2.8 + Glucose/18

Move your Brain Cells
Na+ = 140, Glucose = 200, BUN = 28Measured serum osmolality = 310
• Osmolal gap = Measured OSM - Calculated OSM:= 310 - (2x140 + 200/18 + 28/2.8)= 310 - (280 + 11 + 10)= 310 - 301= 9
Now What There is NO Osmolal Gap?

Remember!!!• All alcohols are osmotically active • Methanol and Ethanol are characterized by– High Anion Gap Acidosis– Osmolal gap
• Only methanol and ethanol are metabolized to acids• Isopropyl Alcohol is metabolized to acetone.• Ethylene glycol may be metabolized completely to
toxic metabolized not active osmotically…. Normal Osmolal gap..
• Late presentation!!!!

Remaining steps of ABGs analysis
• Is the respiratory compensation adequate?• Winter formula• Exp pCO2 = [1.5(measured HCO3
-)]+8± 2• Exp pCO2 = [1.5(3.7)]+8±2= 13.5 ±2• So what is this?• Respiratory element !!! • Why?• Low GCS and Chest problem infective process

Remaining steps of ABGs analysis
• Are there any other metabolic disturbances?• Corrected HCO3
- = Measured HCO3- + Delta gap
• Delta Gap?• Calculated Anion Gap – Normal Anion Gap• Corrected HCO3= ( AG-12) +Measured HCO3
• 24=(AG-12)+Measured HCO3
• 24=(27-12)+Measured HCO3• 24=(15)+4= 19• This stays less than 24… So what does it mean?
There is additional non anion gap metabolic
acidosisWhat could be the reason?

Normal Anion Gap Acidosis(Hypokalemia)
• Diarrhea• Ureteral diversion• Renal tubular
acidosis– Proximal– Distal
• Mineralcorticoid deficiency
• Carbonic anydrase inhibitor– Acetazolamide– Mefenamic acid
• Post hypocapneic state

Normal Anion Gap Acidosis(Hyperkalemia)
• Early renal failure• Renal disease– SLE interstitial
nephritis–Amyloidosis–Hydronephrosis– Sickle cell
nephropathy
• Acidifying agents–Ammonium
chloride–Calcium chloride–Arginine
• Sulfur toxicity

Summary of Assessment
• Case of alcohol ingestion(Ethylene Glycol) with complications masking the clinical picture
• Late presentation• Aspiration pneumonia• Early Renal Failure– Rhabdomyolysis– Ethylene Glycol
• Hypothermia

Management
• Which of the following interventions is most likely to benefit this patient?
1. IV fluids (Crystalloids)2. Ethanol infusion3. Fomipizole 4. Thiamine5. Haemodialysis

Hope we conveyed the message
Thank you for your patience