Embed Size (px)
Citation preview
DURGESH NANDINEUNIVERSITY OF HYDERABAD
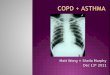
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Burden Of COPD
• Most epidemiological studies have found that COPD prevalence, morbidity and mortality increase over time and are greater in men than in women.
• COPD prevalence is directly related to prevalence of smoking.
• Very few studies have quantified the economic
and social burden of COPD and its quality of life.
• Directed costs of COPD are substantial in developed countries while indirect cost are important in developing countries.
Definition of COPD
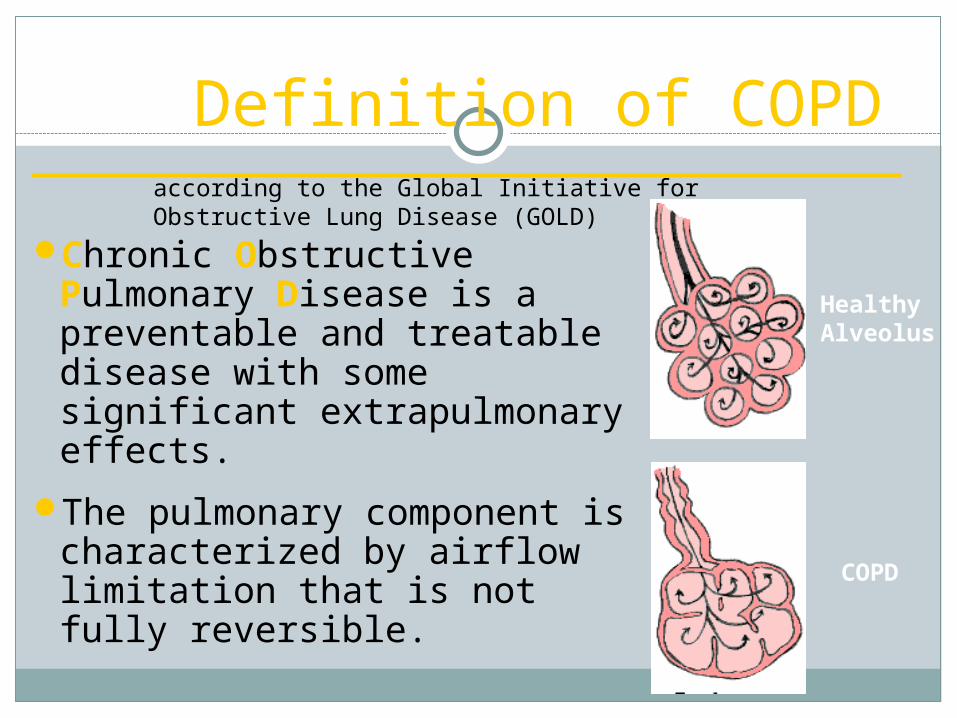
Chronic Obstructive Pulmonary Disease is a preventable and treatable disease with some significant extrapulmonary effects.
The pulmonary component is characterized by airflow limitation that is not fully reversible.
Healthy Alveolus
COPD
according to the Global Initiative for Obstructive Lung Disease (GOLD)
Chronic Obstructive Pulmonary Disease (COPD)
The airflow limitation in COPD is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles and gases
Severe COPD leads to respiratory failure, hospitalization and eventually death from suffocation
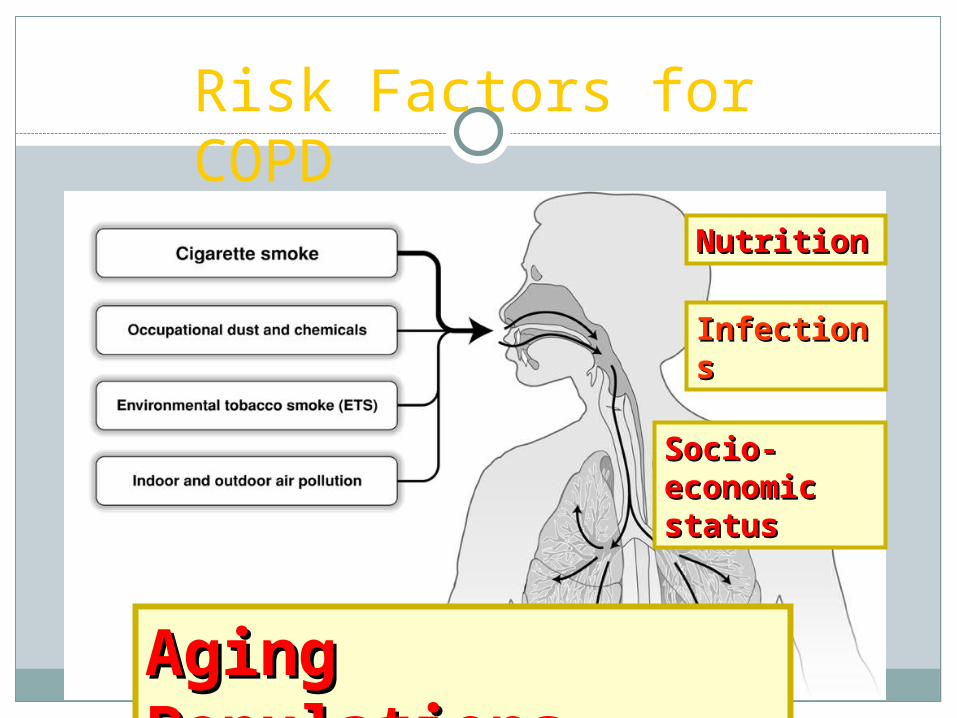
Risk Factors for COPD
NutritionNutrition
InfectionInfectionss
Socio-Socio-economic economic statusstatus
Aging Aging PopulationsPopulations
Goals of Biopsychosocial treatment approach
• Prevent disease progression .
• Relieve symptoms.
• Improve exercise tolerance.
• Improve health status.
• Prevent and treat complications.
• Prevent and treat exacerbations.
• Reduce mortality.
• Prevent or minimize side effects from treatment
Approaches
• Patient education. • Pharmacologic Treatment. - Bronchodilators, - Glucocorticosteroids, - Vaccines, - Antibiotics, - Mucolytic - Antitussives, - Respiratory Stimulants• Non-Pharmacologic Treatment - Rehabilitation, - Oxygen Therapy, - Surgical Treatments
COPD – The DiseaseCOPD – The Disease Patient with COPDPatient with COPD
Airflow obstructionFunction declineContinuous treatmentLifestyleRegular follow-up‘Management plan’ComplianceEffects, safety
treatment
Social isolation Unhealthy
environment Poverty Poor self-efficacy Multiple health
problems Disruptive life
conditions Trust & support Safety line
Biopsychosocial Areas of focus
Guidelines on Tobacco Cessation. Follow the 5A Strategy
ASK (about tobacco use) ASSESS (the status and severity of use) ADVISE (to stop) ASSIST (in smoking cessation) ARRANGE (follow-up programme)
Details of ADVICE for the patientReview your tobacco use. Accept that smoking is a problem and harmful for your health.
Make a decision and determination to quit. Don’t be over confident that you can quit any time you like.
Share your decision with family, friends, doctor. Accept their help. Fix a quit date. Don’t postpone. Remove ashtrays and other objects that are reminders to the habit. Keep away from trigger situations. Adopt healthy lifestyle such as relaxation, exercise, plenty of water, fruits,
vegetables and avoid tea/coffee/alcohol. Take help from family, friends and doctor.
First few steps of quitting tobacco smoking.
To reduce quantity
Change to non-preferred brand. Keep a record of the amount and frequency of tobacco use. Decrease the number of puffs when smoking. Leave large stubs. Don’t inhale deeply.
To deal with triggers when you have an urge to smoke (Trigger coping) For extra-ordinary urge to take tobacco, try alternatives (chewing
gum, toffee, peppermint, cardamom) Increase your water intake Breathe deeply and quietly Do some other work to engage your mind and to keep your mind off
tobacco Delay the act of smoking – count till 100 and think of pleasant
situations.
Smoking cessation
Once you quit Learn to say “no” to tobacco offers from others. Don’t take even a single puff. Try to remain in smoke free areas. Avoid company of smokers and even tobacco chewers. Make a group of people who have quit tobacco – share their
experiences. Collect the money saved from each pack of cigarette or “paan
masala”. Buy a gift for your loved ones with that money. Try alternate ways to deal with mental stress and tension, such as
Relaxation, Deep breathing, Listening to music. Remember there can be some withdrawal symptoms after quitting,
such as headache, irritability, lack of concentration, etc. But bear with them. These are temporary and disappear in a few days.
Even if you fail in quitting smoking. Don’t get disheartened – TRY AGAIN
Seek help of those who have quit smoking Seek professional help and medical advice
Importance of Quality Of Life In Patients With COPD
One study in UK examined whether COPD patients were relatively
disadvantaged in terms of medical and social care compared with
a group with inoperable lung cancer.
Conclusion: This study suggests that :
• patients with end stage COPD have significantly impaired quality of life and emotional well being which may not be as well met as those of patients with lung cancer,.
• COPD patients palliative care needs remain unaddressed Seemungal TA, Donaldson GC, Paul EA, et al
Pulmonary rehabilitation
Pulmonary rehabilitation is a multidimensional continuum of services directed to persons with pulmonary disease and their families, usually by an interdisciplinary team of specialists, with the goal of achieving and maintaining the individual’s maximum level of independence and functioning in the community.
Palliative care:
provides relief from pain and other distressing symptoms;
affirms life and regards dying as a normal process; intends neither to hasten or postpone death;
integrates the psychological and spiritual aspects of patient care;
offers a support system to help patients live as actively as possible until death;
offers a support system to help the family cope during the patients illness and in their own bereavement;
uses a team approach to address the needs of patients and their families, including bereavement counselling, if indicated; will enhance quality of life, and may also positively influence the course of illness;
References
The Tobacco Use and Dependence Clinical Practice Guideline Panel Staff and Consortium Representatives. A clinical practice guideline for treating tobacco use and dependence. JAMA 2000;28:3244-3254.
Seemungal TA, Donaldson GC, Paul EA, et al. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med.1998; 157:1418–1422
References
Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2006. Available from: http://www.goldcopd.org.
Gorski, Lisa MS, RN, CS, CRNI; “COPD Exacerbation: Prevention and Home Management Protocol”. Oasis Answers Inc. http://www.qualidigm.org/uploadedFiles/Professionals/Setting/HomeHealth/Best%20Practice%20Tools%20-%20Emergent%20Care%20-%20Qualidigm%2005.24.07.pdf