Embed Size (px)
Citation preview

Evidence of the MonthEvidence of the Month
Comment on: International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes
Petra-Maria Schumm-DraegerPetra-Maria Schumm-Draeger
Investigators: The International Expert Committee
Published: Diabetes Care. 2009;32:1327-1334

Goals and key findingsGoals and key findings
• International Expert Committee appointed by ADA, EASD, and IDF to consider current and future means of diagnosis of diabetes
• Committee convened in 2008 and reported in 2009
• Committee recommended use of HbA1c for diagnosis, based on
– Close correlation between HbA1c and diabetic retinopathy
– Improved instrumentation and standardization of HbA1c assay
– Less biologic variability, greater preanalytic stability of HbA1c versus glucose tests (FPG, OGTT)
– No requirement for pretest fasting
– Broad familiarity with HbA1c in diabetes management
• Committee recommended HbA1c diagnostic threshold of ≥6.5 % and preventive intervention when HbA1c is <6.5 % but ≥6.0 %
ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes;FPG=fasting plasma glucose; IDF=International Diabetes Federation; OGTT=oral glucosetolerance test

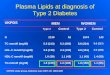
Prevalence of retinopathy by Prevalence of retinopathy by distribution of glucose and HbAdistribution of glucose and HbA1c1c
Prevalence of retinopathy by deciles of the distribution of fasting plasmaglucose (FPG), 2-hour plasma glucose (2hPG), and HbA1c in Pima Indians

Prevalence of diabetic retinopathyPrevalence of diabetic retinopathy by HbA by HbA1c1c intervals intervals
Prevalence of retinopathy by 0.5 % intervals of HbA1c in individualsaged 20-79 years. NPDR=nonproliferative diabetic retinopathy

Recommendations of the International Recommendations of the International Expert CommitteeExpert Committee
For the diagnosis of diabetes:
• The HbA1c assay is an accurate, precise measure of chronic glycaemic levels and correlates well with the risk of diabetes complications
• The HbA1c assay has several advantages over laboratory measures of glucose
• Diabetes should be diagnosed when HbA1c is ≥6.5 %. Diagnosis should be confirmed with a repeat HbA1c test. Confirmation is not required in symptomatic subjects with plasma glucose levels >200 mg/dl (>11.1 mmol/l)
• If HbA1c testing is not possible, previously recommended diagnostic methods (e.g., FPG or 2hPG, with confirmation) are acceptable
• HbA1c testing is indicated in children in whom diabetes is suspected but the classic symptoms and a casual plasma glucose >200 mg/dl (>11.1 mmol/l) are not found

Recommendations of the International Recommendations of the International Expert CommitteeExpert Committee
For the identification of those at high risk for diabetes:
• The risk for diabetes based on levels of glycaemia is a continuum; therefore, there is no lower glycaemic threshold at which risk clearly begins
• The categorical clinical states prediabetes, impaired fasting glucose, and impaired glucose tolerance fail to capture the continuum of risk and will be phased out of use as HbA1c measurements replace glucose measurements
• As for the diagnosis of diabetes, the HbA1c assay has several advantages over laboratory measures of glucose in identifying individuals at high risk for developing diabetes
• Those with HbA1c levels below the threshold for diabetes but ≥6.0 % should receive demonstrably effective preventive interventions. Those with HbA1c below this range may still be at risk and, depending on the presence of other risk factors, may also benefit from prevention efforts
• The HbA1c level at which population-based prevention services begin should be based on the nature of the intervention, the resources available, and the size of the affected population

Clinical implicationsClinical implications
• HbA1c for diabetes diagnosis offers greater convenience and accuracy than glucose measurements and correlates well withlong-term complications
• HbA1c may be too expensive for routine use in some parts of world
• HbA1c may be influenced by haemoglobin traits and precluded for people with conditions that affect red cell turnover (haemolytic anaemia, chronic malaria)
• HbA1c not ‘gold standard’ for diabetes diagnosis, as no single assay can define the relationship between glucose and vascular complications
• ADA endorses committee recommendations on HbA1c ‘in principle’ while evaluating implications





![Laboratory Diagnosis and Monitoring of Diabetes Mellitus 2002 · Laboratory diagnosis and monitoring of diabetes mellitus / Hans Reinauer ... [et al.] 1.Diabetes mellitus - diagnosis](https://img.pdfslide.net/doc/110x75/5ec89e79cc5c715c612bb0f3/laboratory-diagnosis-and-monitoring-of-diabetes-mellitus-2002-laboratory-diagnosis.jpg)