Embed Size (px)
Citation preview
Factors affecting Factors affecting surgical outcome surgical outcome
in Resurgery – How in Resurgery – How to proceedto proceedDr. Madhu KarnaDr. Madhu Karna
Consultant Pediatric OphthalmologistConsultant Pediatric Ophthalmologist
Cooper’s dictum – as though new cases Cooper’s dictum – as though new cases with appropriate orthoptic, medical with appropriate orthoptic, medical and surgical remediesand surgical remedies
Careful measurements and ocular Careful measurements and ocular rotations rotations
Force and velocity studiesForce and velocity studies Findings at surgeryFindings at surgery
Risk factors for overcorrection- A Risk factors for overcorrection- A pattern, amblyopia, high hyperopiapattern, amblyopia, high hyperopia
Non seeing eyeNon seeing eye Seeing pts-Seeing pts-
first surgery resultfirst surgery result Progressive problemProgressive problem Unmasking of other components - Unmasking of other components -
Reoperations inevitableReoperations inevitableCongenital esotropia without nystagmus- Congenital esotropia without nystagmus-
80-85% success rate80-85% success rate
Operated infantile Operated infantile esotropia presenting with esotropia presenting with
DVDDVD
PostopPostop
When to reoperateWhen to reoperate
At least 2 months after the initial At least 2 months after the initial surgery except:surgery except:
Lost or slipped muscleLost or slipped muscle Large overcorrection after an SO Large overcorrection after an SO
tucktuck Large vertical deviations induced by Large vertical deviations induced by
muscle transposition proceduresmuscle transposition procedures
ExpectationsExpectations
Stable alignmentStable alignment Full ocular rotationFull ocular rotation Good cosmesis – white /noninflamed Good cosmesis – white /noninflamed
eye , symmetric lid fissureseye , symmetric lid fissures
PlanningPlanning
Lookup the records – helps to decide Lookup the records – helps to decide virgin muscle or redo operated virgin muscle or redo operated musclesmuscles
Look for the scar at the insertion. Look for the scar at the insertion. Plica drawn up into medial bulbar Plica drawn up into medial bulbar
scar scar 12-15 LRrec,11-12 MRrec causes -12-15 LRrec,11-12 MRrec causes -
1.5 limitation of abd and add1.5 limitation of abd and add
HurdlesHurdles
Conjunctiva – String or indentation signConjunctiva – String or indentation sign Muscle – Excessive resectionsMuscle – Excessive resections Scar – Following intraconal fat violationScar – Following intraconal fat violation
Leash – restrict rotation the opposite fieldLeash – restrict rotation the opposite field
Reverse leash – limit rotations in the same Reverse leash – limit rotations in the same field Uncooperative patient – do under field Uncooperative patient – do under GAGA
PlanningPlanning
Residual Eso-Residual Eso- Distance deviation more Distance deviation more than near MR not be recessedthan near MR not be recessed
Secondary Eso-Secondary Eso- Distance deviation Distance deviation more than near and near less than more than near and near less than 10pd needs LR advancing in operated 10pd needs LR advancing in operated eye, LR res in unoperated eyeeye, LR res in unoperated eye
Secondary ExoSecondary Exo – Due to slipped MR – Due to slipped MR will need excision of psuedotendon & will need excision of psuedotendon & advancing MRadvancing MR
Planning Planning
IO ResurgIO Resurg – iatrogenic mydriasis – iatrogenic mydriasis /bleeding/bleeding
Vertical residual deviationVertical residual deviation larger in larger in upgaze-SR/IO Surgupgaze-SR/IO Surg
Res incyclodviation-Res incyclodviation- tenect ant SO or tenect ant SO or SR nasal/IR tempSR nasal/IR temp
Res excyclotorsion-Res excyclotorsion- Harado Ito or SR Harado Ito or SR temp/IR nasaltemp/IR nasal
Horizontal and vertical squint too- Horizontal and vertical squint too- maybe due to verticals not being maybe due to verticals not being handled- handled-
15 -25 prism of V pattern in the 15 -25 prism of V pattern in the presence of Io overaction can be presence of Io overaction can be dealt with IO surgery alone. dealt with IO surgery alone.
Rest has to be dealt with additional Rest has to be dealt with additional horizontal displacementshorizontal displacements
Weakening IO’s or tuck of SO’s each Weakening IO’s or tuck of SO’s each correct 15 prism to 25 prism of a V correct 15 prism to 25 prism of a V patternpattern
Bilateral superior oblique Bilateral superior oblique tenotomies correct 35-45pd of A tenotomies correct 35-45pd of A patternpattern
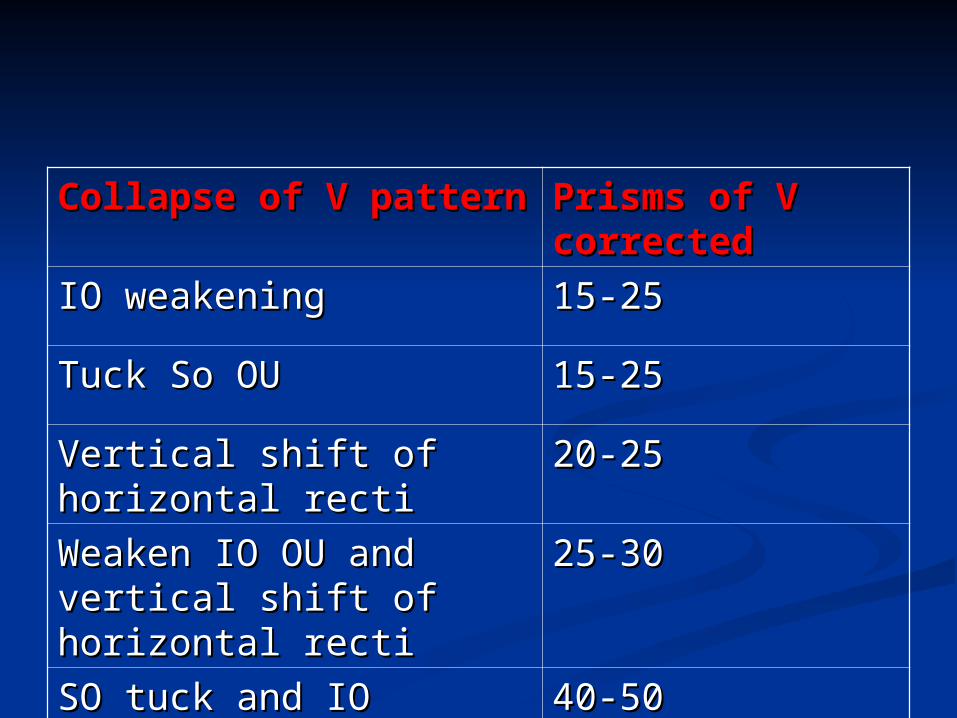
Collapse of V patternCollapse of V pattern Prisms of V Prisms of V correctedcorrected
IO weakeningIO weakening 15-2515-25
Tuck So OUTuck So OU 15-2515-25
Vertical shift of Vertical shift of horizontal rectihorizontal recti
20-2520-25
Weaken IO OU and Weaken IO OU and vertical shift of vertical shift of horizontal rectihorizontal recti
25-3025-30
SO tuck and IO SO tuck and IO weakeningweakening
40-5040-50
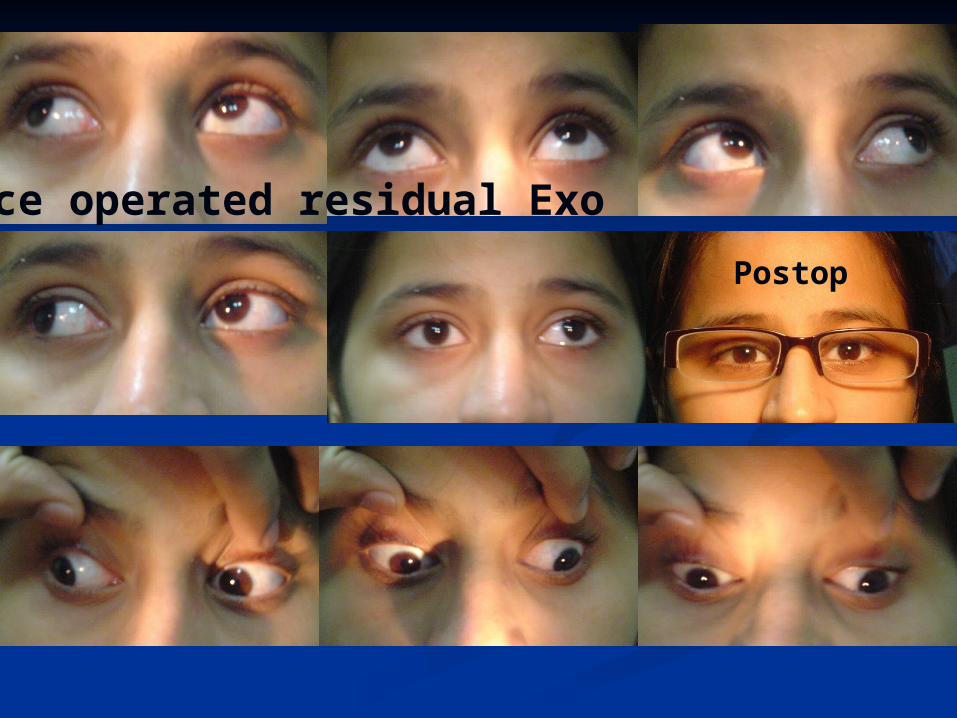
Postop
Twice operated residual Exo
Sensory strabismus mainly sensory Sensory strabismus mainly sensory exotropia exotropia
Do FDT Do FDT Release the restrictions and do maximum Release the restrictions and do maximum
recess- resect recess- resect Inferior Oblique and SO can be weakened Inferior Oblique and SO can be weakened
which are additional abductors.which are additional abductors. Raab, unilateral 4 muscle study for large Raab, unilateral 4 muscle study for large
angle exotropia, Ophthal, 1979: 86, 1441angle exotropia, Ophthal, 1979: 86, 1441
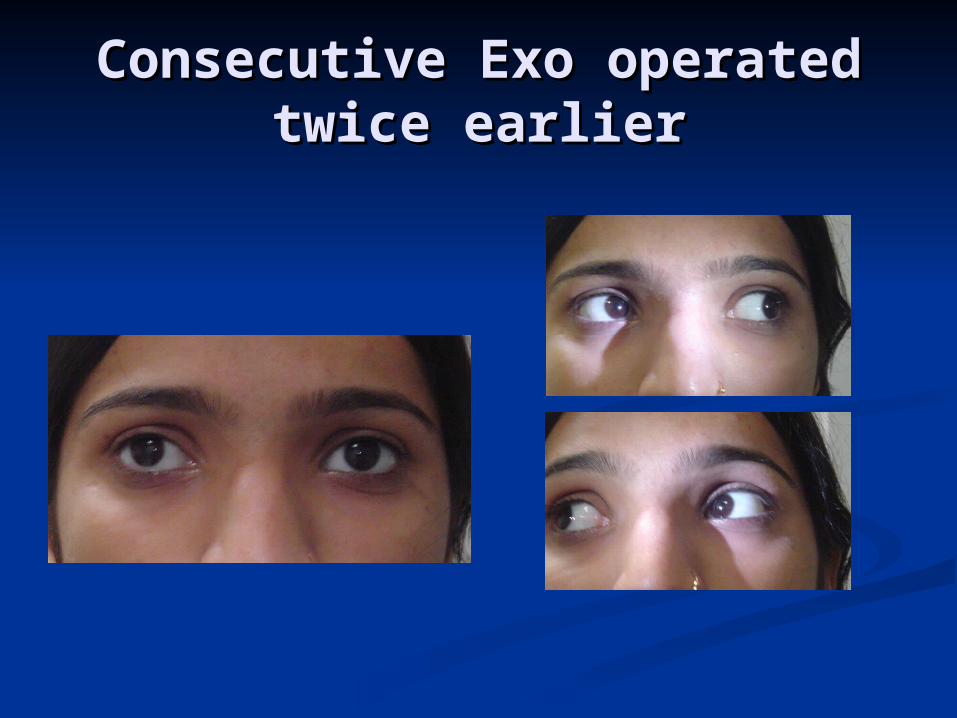
Consecutive Exo operated Consecutive Exo operated twice earliertwice earlier
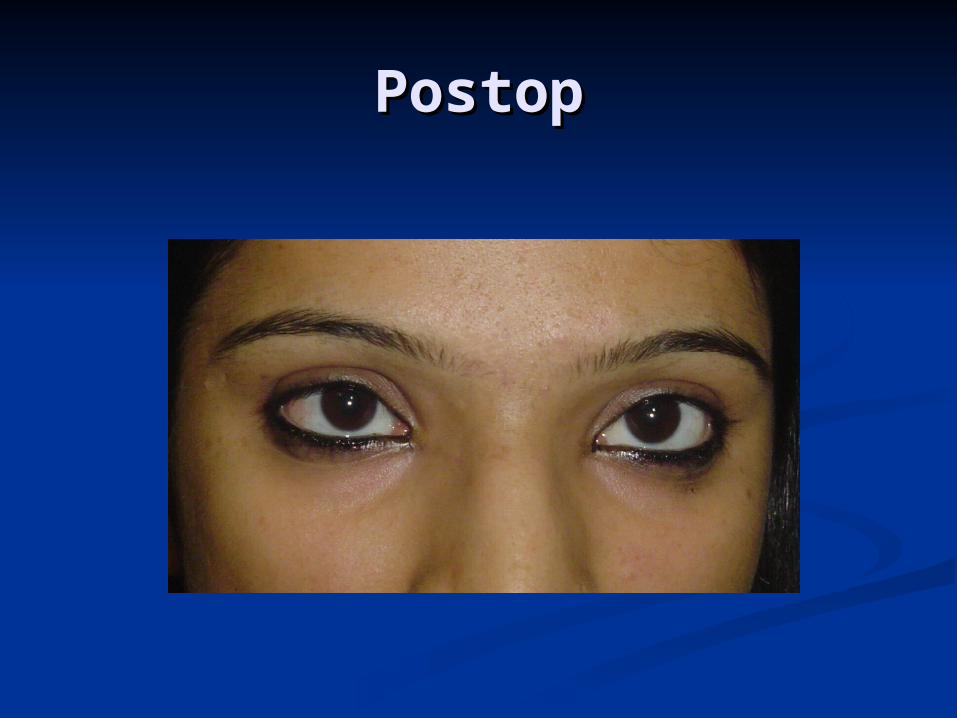
PostopPostop
Careful Careful
Scar tissueScar tissue Pulled plica Pulled plica Suture granulomaSuture granuloma Fat adherenceFat adherence Muscle ruptureMuscle rupture Anterior segment ischaemiaAnterior segment ischaemia Congenital absence of SO and IRCongenital absence of SO and IR
Suture GranulomaSuture Granuloma
Inferior oblique adherence Inferior oblique adherence syndromesyndrome
Hypotropia in the primary position and Hypotropia in the primary position and limitation of elevation in adduction in a limitation of elevation in adduction in a eye that has undergone inferior oblique eye that has undergone inferior oblique weakening. weakening.
Post Tenon’s capsule should be left intact, Post Tenon’s capsule should be left intact, if orbital fat is encountered should be if orbital fat is encountered should be reposited behind it and defect closed with reposited behind it and defect closed with 8-0 vicryl 8-0 vicryl
Bleeding controlled with careful cautery, Bleeding controlled with careful cautery, not excessive as it can cause adhesions, not excessive as it can cause adhesions, scarring and scleral meltscarring and scleral melt
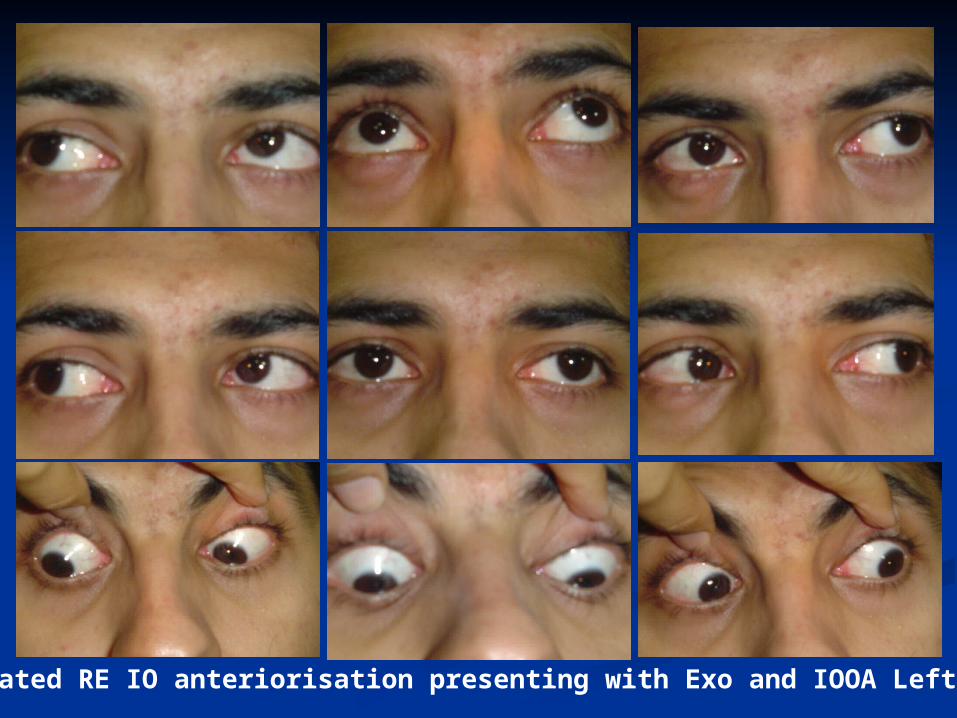
Operated RE IO anteriorisation presenting with Exo and IOOA Left eye
For very tight musclesFor very tight muscles Place sutures 0.5 to 1mm behind the muscle Place sutures 0.5 to 1mm behind the muscle
during recession and a like amount behind the during recession and a like amount behind the muscle clamp.muscle clamp.
Scleral track at least 1.5mm long including Scleral track at least 1.5mm long including superficial scleral fibres and at least 2 mm deep. superficial scleral fibres and at least 2 mm deep.
Limit the dissection of intermuscular membrane Limit the dissection of intermuscular membrane anterior to its emergence through Tenon’s anterior to its emergence through Tenon’s capsulecapsule
Use phenylephrine to blanch Tenon’s and Use phenylephrine to blanch Tenon’s and episclera and make red muscle more evidentepisclera and make red muscle more evident
Simple perforation without prolapse of vitreous Simple perforation without prolapse of vitreous or uvea should be left untreated.or uvea should be left untreated.
Accurate workupAccurate workup Correct choice of surgeryCorrect choice of surgery Proper executionProper execution Surgeon’s ability to learn from Surgeon’s ability to learn from
experienceexperience
It is better to do a wrong It is better to do a wrong procedure well than to do procedure well than to do the correct procedure the correct procedure poorly!!poorly!!
Best to do the correct Best to do the correct procedure and do it wellprocedure and do it well
Reop expected in 5-10% of patients Reop expected in 5-10% of patients who undergo squint surgerywho undergo squint surgery
Any reop introduces a 33% Any reop introduces a 33% probability of yet another procedureprobability of yet another procedure
Talk to the patient immediately before Talk to the patient immediately before surgery and inform the outcomesurgery and inform the outcome
We will make 100% effort to make this We will make 100% effort to make this the last squint surgery neededthe last squint surgery needed