Embed Size (px)
Citation preview
Reino Stoffelsen, child and adolescent psychiatrist (VUmcde Bascule, Amsterdam)
Anna van Spanje, senior policy officer (Dutch Knowledge Centre for Child and Adolescent Psychiatry, Utrecht)
ESCAP, Madrid, June 20th 2015
Not getting out of bed…A lazy adolescent, or…a sleep disorder?!
None
Conflicts of interest

• Ed de Bruin, clinical neuropsychologist and researcher, University of Amsterdam (UvA)
• Jeannette Hop, child and adolescent psychiatrist, Altrecht
Thanks to
Introduction
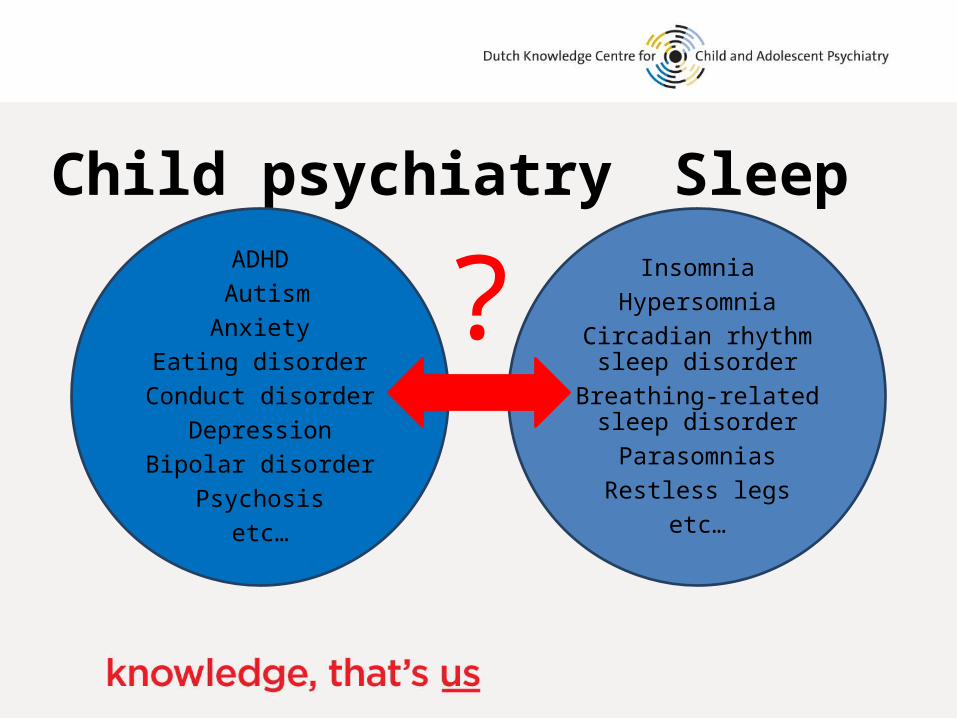
Child psychiatry SleepADHD
AutismAnxiety
Eating disorderConduct disorder
DepressionBipolar disorder
Psychosisetc…
InsomniaHypersomnia
Circadian rhythm sleep disorder
Breathing-related sleep disorderParasomniasRestless legs
etc…
?
PrevalenceIn adolescents with…
…ADHD: 50-80% (Van der Heijden et al., 2005; Owens, 2008; Cortese et al., 2009)
…Autism: 50-80% (Richdale & Schreck, 2009)
…Mood disorders: one of the diagnostic criteria…Anxiety disorders: 90% approx. (Cortese et al., 2014)
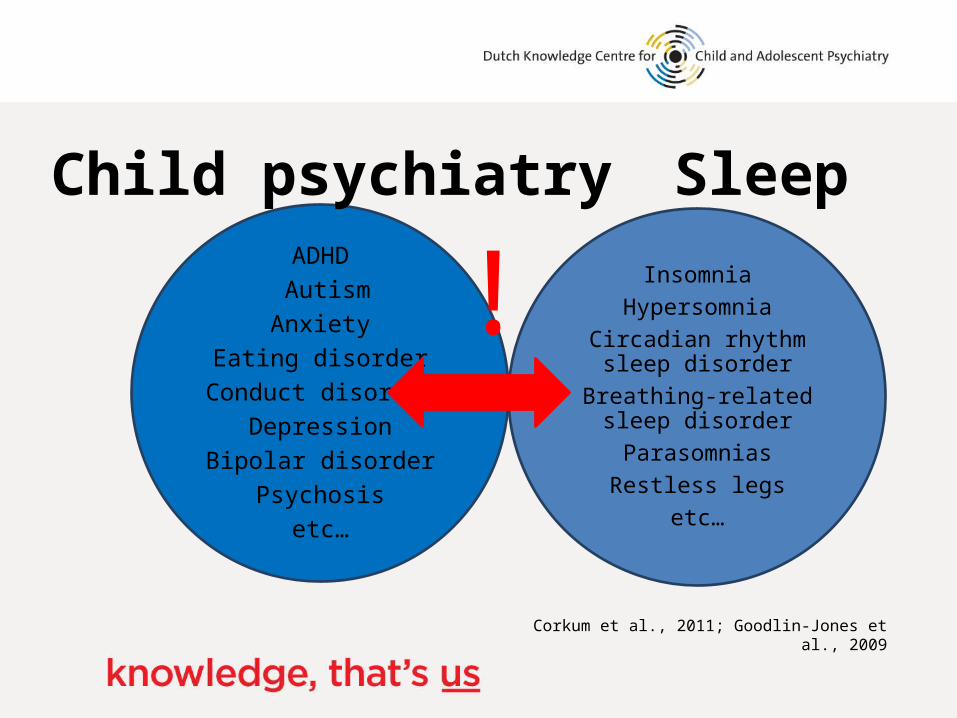
ADHD AutismAnxiety
Eating disorderConduct disorder
DepressionBipolar disorder
Psychosisetc…
InsomniaHypersomnia
Circadian rhythm sleep disorder
Breathing-related sleep disorder
ParasomniasRestless legs
etc…
Child psychiatry Sleep
!
Corkum et al., 2011; Goodlin-Jones et al., 2009
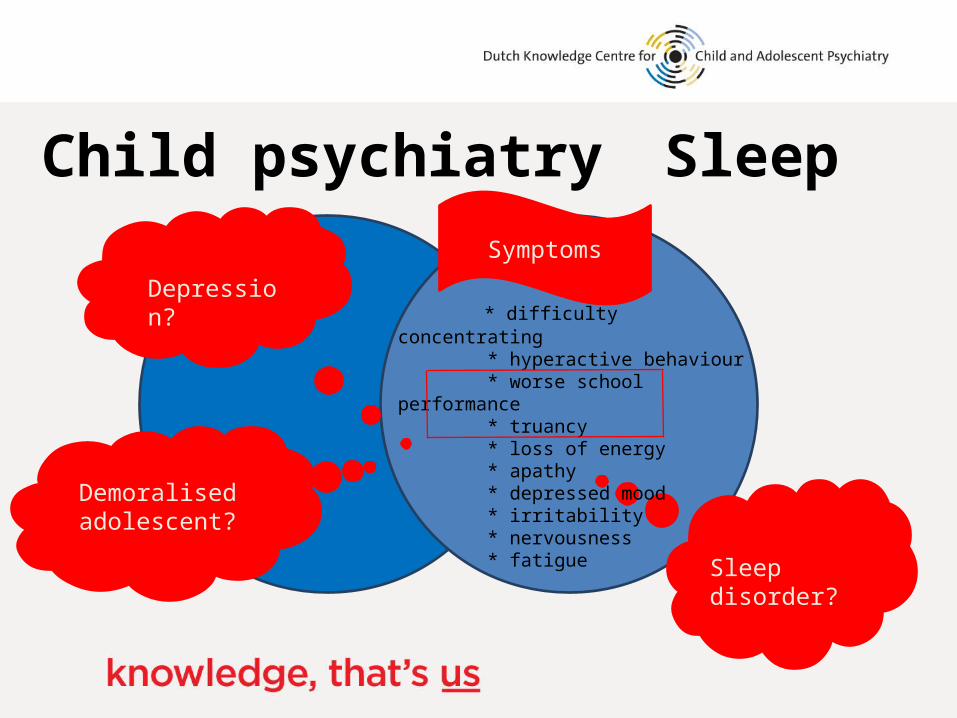
Child psychiatry SleepSymptoms
Sleep disorder?
Depression?
Demoralised adolescent?
* difficulty concentrating * hyperactive behaviour * worse school performance * truancy * loss of energy * apathy * depressed mood * irritability * nervousness * fatigue
Today’s workshop• Introduction• Clinical case• Theory: the two most common sleep disorders
in adolescence• Diagnostics: tips & tricks• Treatment• Discussion
Clinical case: Maria Discuss:
• Have you seen these symptoms in your own clinical practice?
• What is your differential diagnosis?• What would your next step be?
Summary clinical case• Maria, age 16 years, increasing truancy,
indifferent attitude• Since some months trouble falling asleep, hard
to awaken, doesn’t sleep in at weekends• Tired, attention-concentration problems,
weaker performance• Little interest in doing anything, irritable
Theory
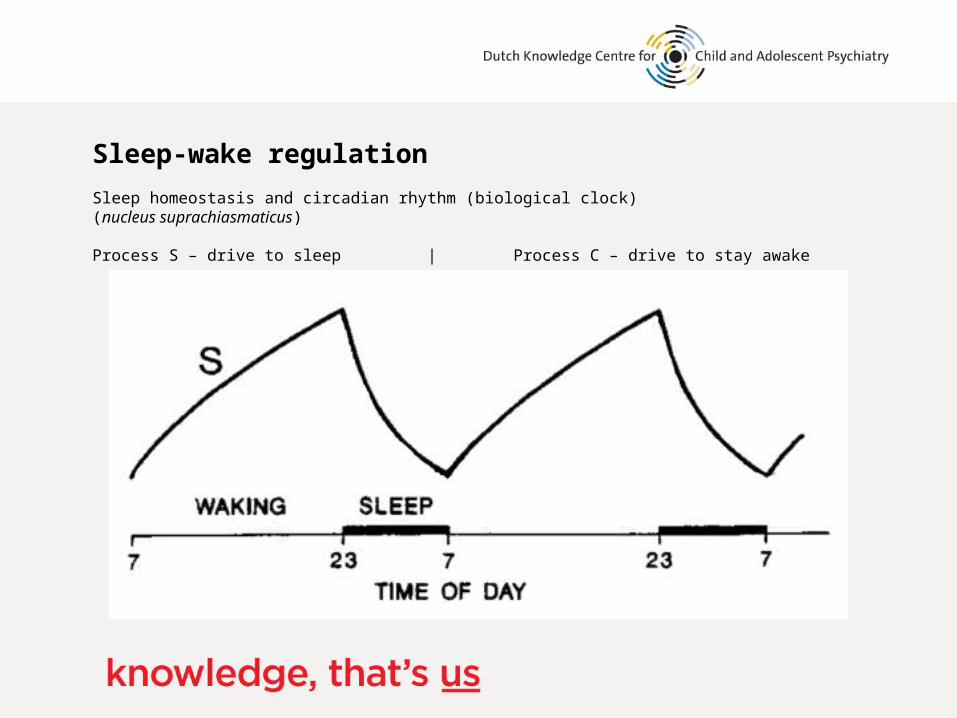
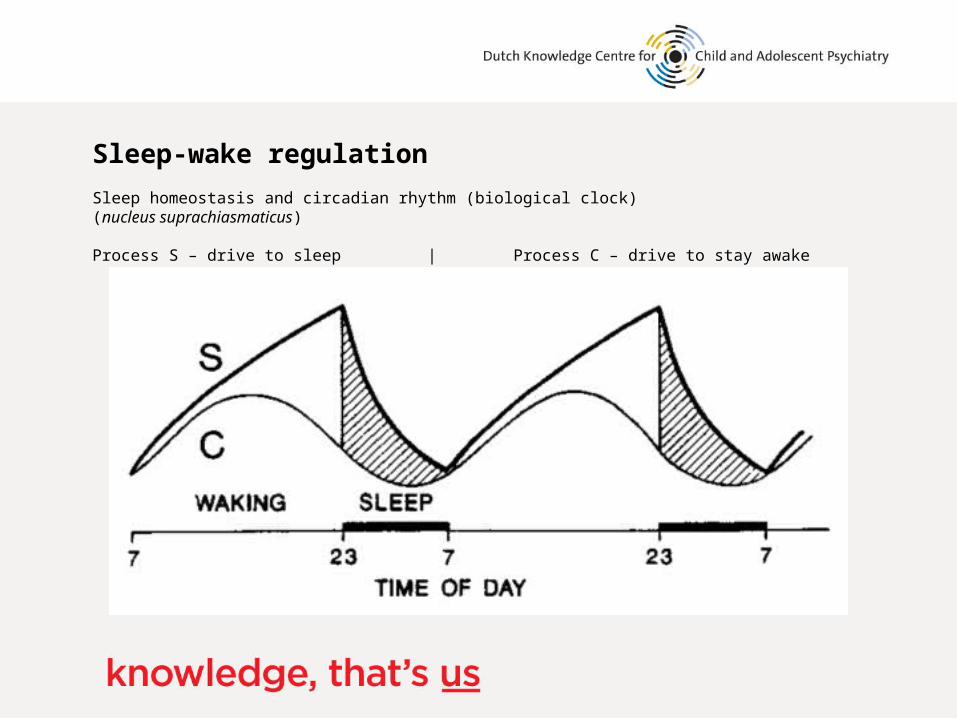
Sleep-wake regulation
Sleep homeostasis and circadian rhythm (biological clock)(nucleus suprachiasmaticus)
Process S – drive to sleep | Process C – drive to stay awake
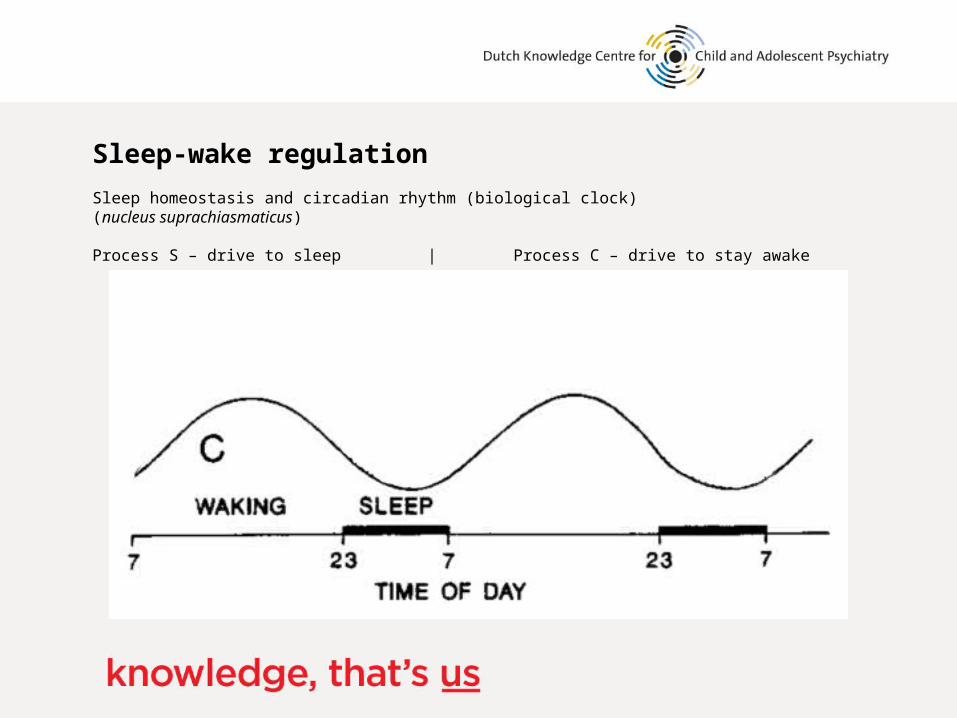
Sleep-wake regulation
Sleep homeostasis and circadian rhythm (biological clock)(nucleus suprachiasmaticus)
Process S – drive to sleep | Process C – drive to stay awake
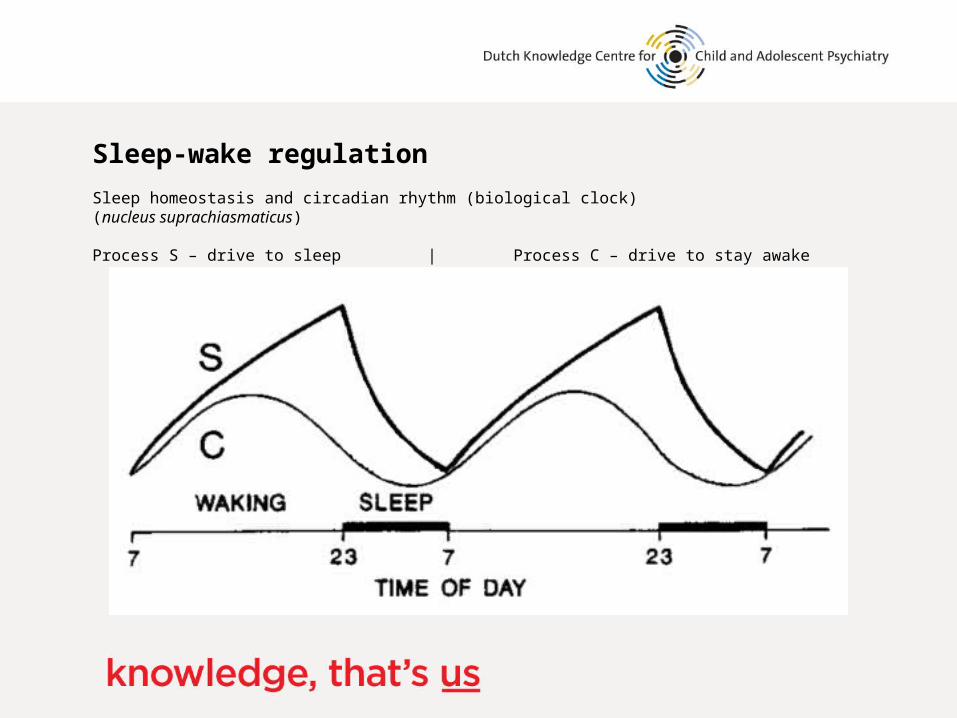
Sleep-wake regulation
Sleep homeostasis and circadian rhythm (biological clock)(nucleus suprachiasmaticus)
Process S – drive to sleep | Process C – drive to stay awake
Sleep-wake regulation
Sleep homeostasis and circadian rhythm (biological clock)(nucleus suprachiasmaticus)
Process S – drive to sleep | Process C – drive to stay awake
Sleep-wake regulation
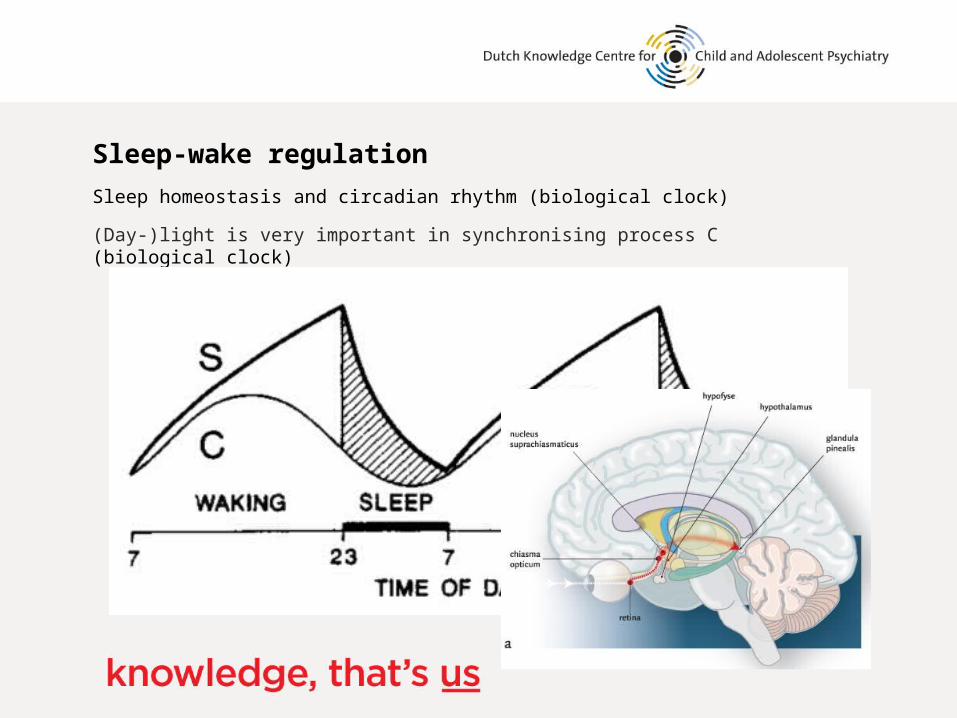
Sleep homeostasis and circadian rhythm (biological clock)
(Day-)light is very important in synchronising process C (biological clock)
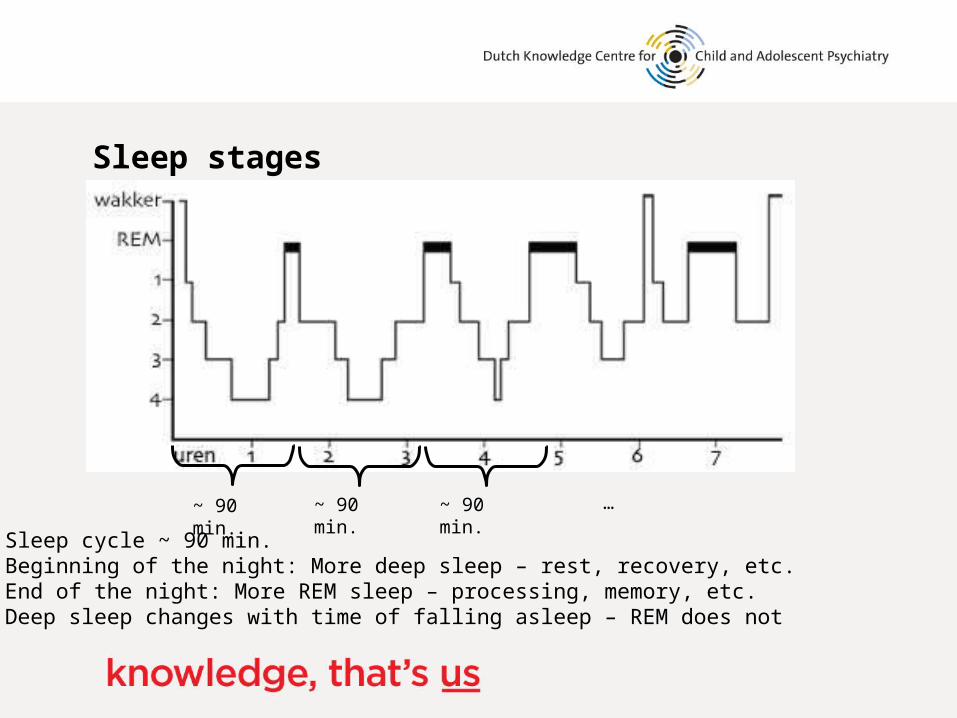
Sleep stages
• Sleep cycle ~ 90 min. • Beginning of the night: More deep sleep – rest, recovery, etc.• End of the night: More REM sleep – processing, memory, etc.• Deep sleep changes with time of falling asleep – REM does not
~ 90 min. ~ 90 min. ~ 90 min. …
The functions of sleep• Rest (energy saving)• Recovery (e.g., immune system): Necessary
for daily functioning and survival• Growth (brain cells, body) • Memory processes (brain reorganisation)
Hour of falling asleep• Shifts in youth – starting at puberty – to a later
hour.
• Preference for later bedtime• Get tired at a later hour• Wake up at a later hour (!)
• Very prone to sleeplessness (insomnia)
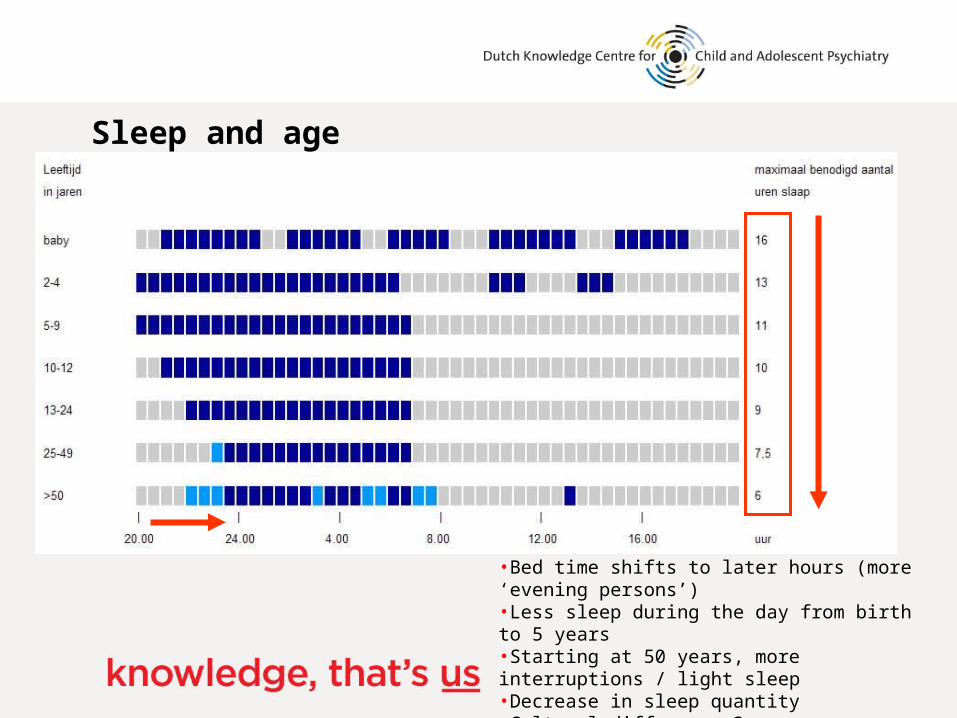
Sleep and age
•Bed time shifts to later hours (more ‘evening persons’)•Less sleep during the day from birth to 5 years•Starting at 50 years, more interruptions / light sleep •Decrease in sleep quantity•Cultural differences?
Prevalence of sleep problems (adolescents)
• 45% sleeps less than 8 hours per night,9% less than 6 hours; even though sleeping a minimum of 9 hours seems required for functioning well during the day.
• 20% to 50% experiences sleepiness during the day.
• 11% to 47% has trouble falling asleep and staying asleep.
Consequences• Behavioural problems (e.g. hyperactivity and ADHD,
impulsiveness, aggressive behaviour)• Learning problems (e.g. attention, concentration, motivation)• Emotional problems (e.g. irritability, anxiety, depression, mood
swings)• Worse school performance• Somatic complaints (e.g. fatigue, headache, stress)• Other long term problems? (Still unclear – possible relations
with obesity and diabetes)
Sleep problems have consequences for the entire family
Astill et al., 2012; Dewald et al., 2010; Meijer et al., 2010; Bell & Belsky, 2008
Sleep disorders (DSM-5)
• Insomnia disorder• Hypersomnolence disorder• Breathing-related sleep disorders• Circadian rhythm sleep-wake disorders
(Delayed sleep phase syndrome; DSPS)• Parasomnias / PLMD (ICSD-2)
Insomnia disorder (DSM-5)
• Trouble falling asleep• Trouble staying asleep (awake often and long
periods at night, wake up early and not fall asleep again)
• Or: not feeling rested in the morning (sleep quality)
• > 3 days /week and > 3 months
Circadian Rhythm Sleep-Wake Disorders (DSM-5)Delayed sleep phase typeDSPS: delayed sleep phase syndrome
The sleep-wake rhythm and the environmental rhythm are not in sync.
• Delayed sleep phase type (DSPS): internal circadian pacemaker is delayed (> 2 hours later than average)
• Frequent in puberty (7% of adolescents)• Changes in circadian rhythms (e.g. body temperature, melatonin
release) x social factors• Week-weekend differences (jetlag-like symptoms)• Similar to insomnia – much trouble falling asleep.
Difference: (being able to) sleep in until late
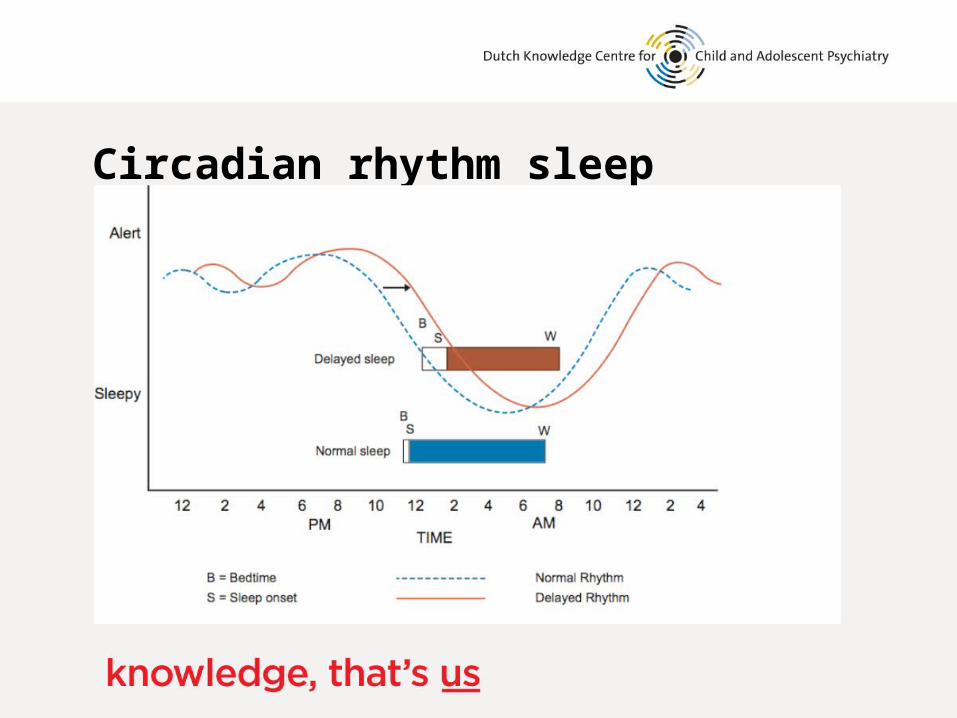
Circadian rhythm sleep disorder
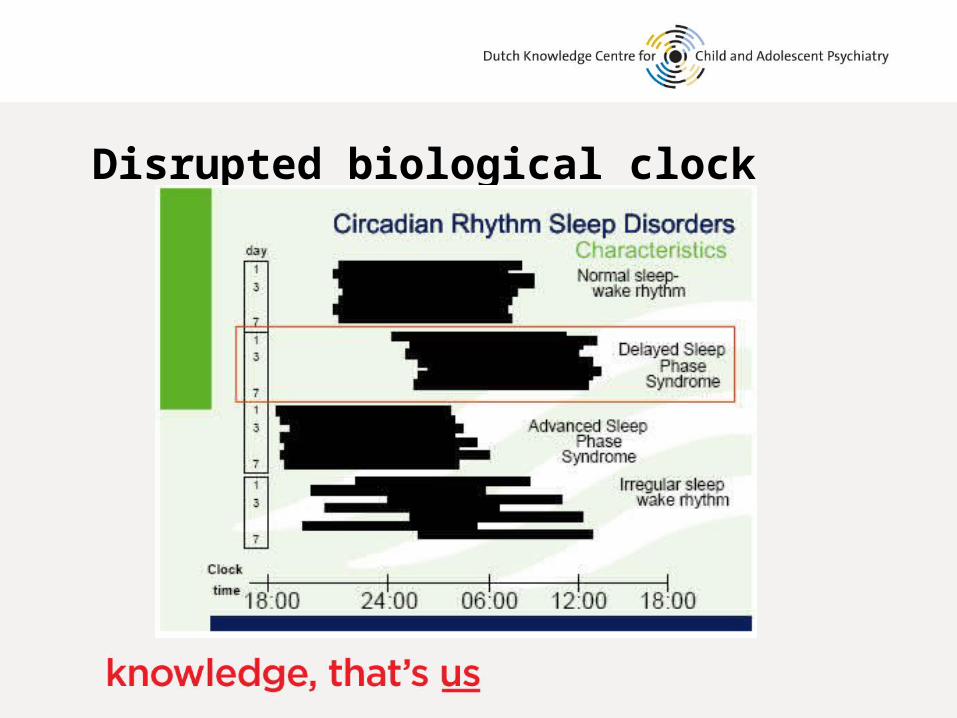
Disrupted biological clock
Diagnostics
Diagnostics• Anamnesis parents/child – age specific factors• Sleep diary +/- actiwatch• Questionnaires
• DLMO• PSG / Video registration

History taking (screening)History - screening: (answers: yes/no, and how often and how long?)• Are there problems falling asleep?• Are there problems staying asleep? (waking up often and/or having trouble
falling asleep after waking up) • Waking up early and not being able to fall asleep again? • Not feeling rested after sleeping?• Unusual behaviour at night?
Impairments (fatigue, little energy, trouble with concentration / memory, mood problems, behavioural problems, achieve less, social problems, parent/child interaction problems)
If “yes” proceed to profound consult
Assumption insomnia (DSM-5): if more than 3 nights per week, during 3 months
History taking (in-depth)
1. Quantitative:• Sleep hours, rhythm, on weekdays / weekends / days off / holidays• Moments awake at night? • Naps during the day? Falling asleep suddenly during the day?• Duration sleep problems? Developmental aspects? (e.g. separations /
magical thinking)
2. Subjective experience sleep (quality) + functioning during the day (e.g. tired / irritable); Subjective experience required sleep
History taking (in-depth)
3. Sleep hygiene, incl. aspects bedroom; specifically gaming, internet, telephone, TV
4. Parasomnia (unusual behaviour at night)
• Nightmares, snoring, anxiety / anger, sleepwalking, talking, moving, teeth grinding, wetting the bed
• Moment at night, memory, responsive yes/no• Nightly epilepsy? (responsiveness / memory)
History taking (in-depth)
5. Activity pattern during the day? Hobbies
6. Family anamnesis (chronotype, other sleep problems)
7. What has been tried, and did it work? (parentsand/or child)
What is the (further) parent/child interaction like?
History taking (in-depth)
8. Anxiety / stress / worry (sleep-related or not) / mood / trauma
9. Somatic problems (current / previous)
10. Medication and substance use
Additional diagnostics• Actigraphy• Polysomnography• Determine melatonin levels
Take home message
Child and Adolescent Psychiatry
Sleep

Diagnostics on both levels!
Child and Adolescent Psychiatry
Sleep

Treatment (1)

Cognitive Behavioural Therapy for Insomnia (CBT-I)
• Behaviour: tackle habits and other behaviours that disrupt sleep.• Sleep hygiene, explain purpose and functioning of sleep• Limit time spend in bed• Stimulus control
• Cognition: tackle thoughts and sentiments that disrupt sleep.• Cognitive restructuring• Stress reduction and relaxation
First choice for treatment insomnia, effective in both short and long term (Morin, 1999; Morgenthaler et al., 2006; De Bruin et al., 2013)
Treatment of insomnia in adolescentsSleep education
Explain functions of sleep (recovery, growth, energy, memory)Explain structure of sleep, personal need, specifically for youth (melatonin)
Sleep hygieneContext: temperature, sound, light.Behaviour: bed time, naps during the day, exercise, caffeine, tobacco use, alcohol, food.
Sleep restriction / Sleep window – restrict time in bedSleep efficiency = (hours of sleep / time in bed)*100. For example, 8 hours in bed, 6 hours sleep: (6/8)*100
= 75% - ideal is >90%.Sleep window as aforementioned, e.g. go to bed at 23:00, get up at 5:30. Add 15-30 minutes with good
sleep efficiency.Rationale: less time in bed, increasing sleep pressure, higher percentage of sleeping in bed, faith in sleep
recovers.
Stimulus controlIf more than 30 minutes awake in bed, get up, sit quietly in another room until sleepy, then go back to bed.Rationale: disconnect association bed/bedroom and not sleeping.
Cognitive restructuringChange dysfunctional cognitions (if I don’t sleep now, I have to cancel everything tomorrow) into functional
ones (if I don’t sleep now, I can still attend my appointments tomorrow), via thought schedule and challenging dysfunctional thought (is it always true, does it happen to others, do others also think this applies to me, how bad is it if it is true some time?)
Rationale: disrupting thoughts keep you awake, helping thoughts break tension and vicious worry-cycle.
Stress reduction/Relaxation For example body scan, progressive muscle relaxation, etc.

Treatment (2)
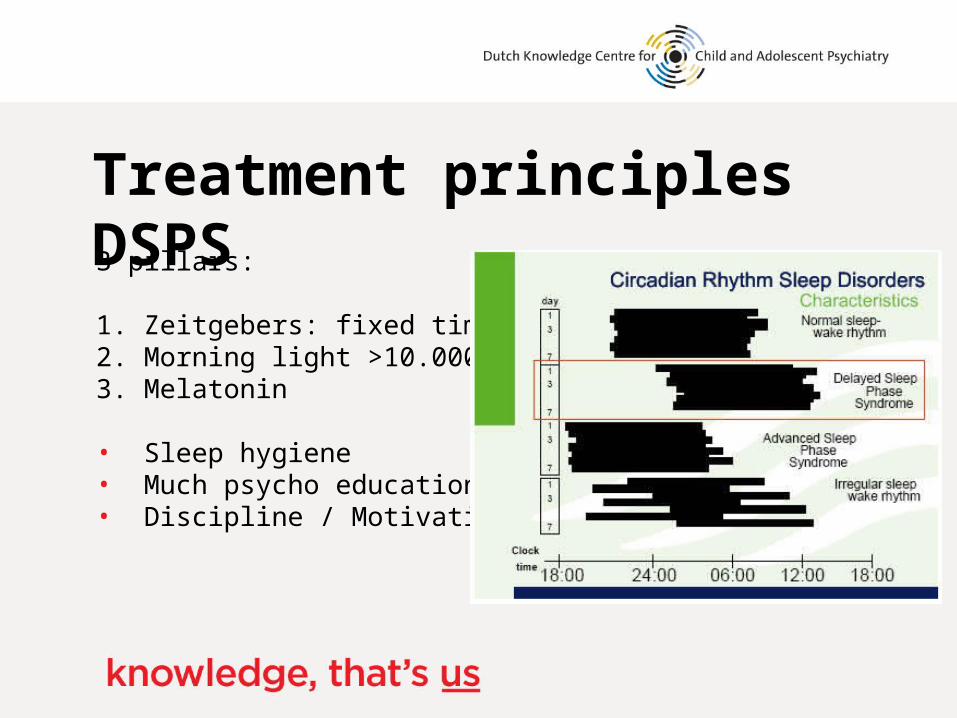
Treatment principles DSPS3 pillars:
1. Zeitgebers: fixed times2. Morning light >10.000 lux3. Melatonin
• Sleep hygiene• Much psycho education• Discipline / Motivation
Melatonin• Drug store: 0,1 mg• Pharmacy: 1-5 mg
• Is being taken and prescribed (too) much
• Know what you prescribe and for which indication!
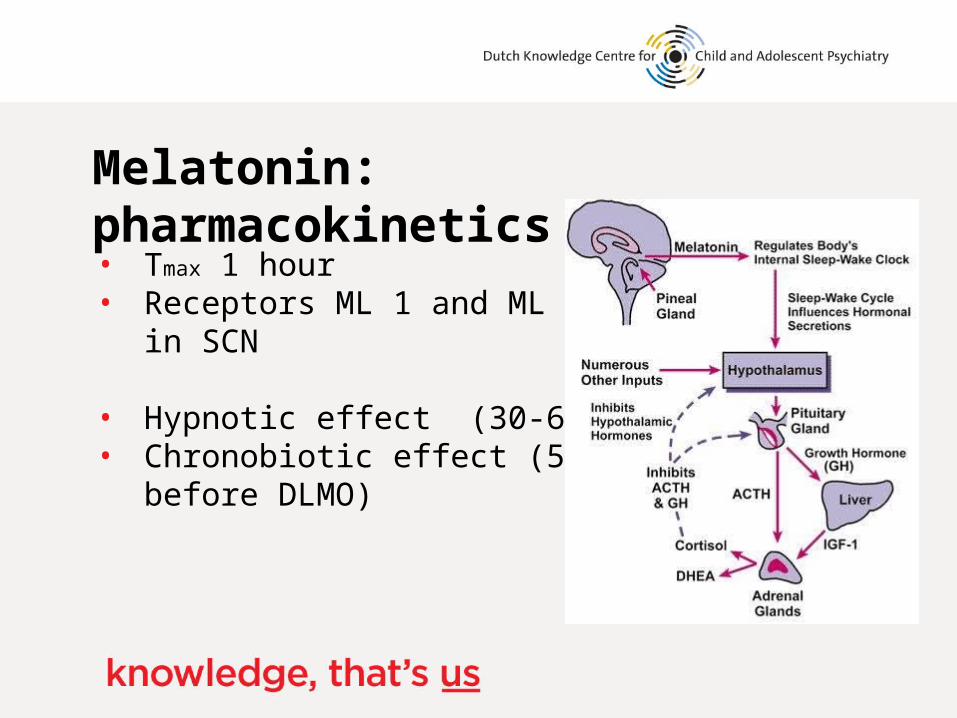
Melatonin: pharmacokinetics
• Tmax 1 hour• Receptors ML 1 and ML 2
in SCN
• Hypnotic effect (30-60 min)• Chronobiotic effect (5 hours
before DLMO)
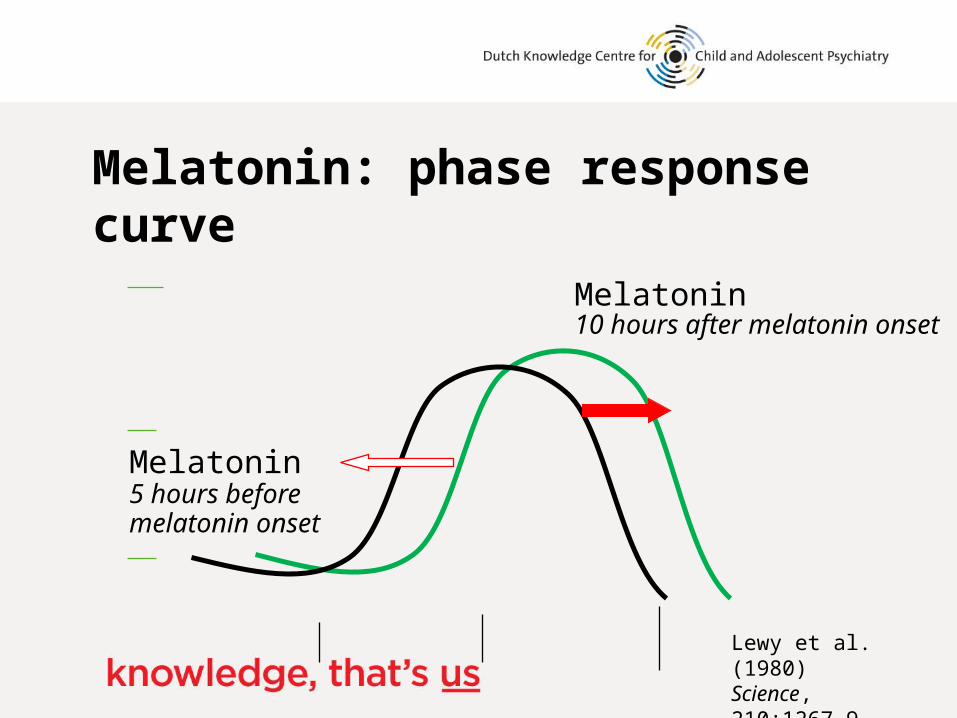
Melatonin: phase response curve
Melatonin10 hours after melatonin onset
Melatonin5 hours beforemelatonin onset
Lewy et al. (1980) Science, 210:1267-9
Time of intake with DSPS• 5 hours before DLMO: determine preferably• In practice 18:00-20.00 hours• Not: ½ hours AN
• Hypnotic effect• Level too high in the morning• Physiological dose 0,1 and 1 mg
Remember:• Melatonin: timing is essential!
• <10 yrs: +/- 18.00 hours• 10-16 yrs: +/- 19.00 hours• >16 yrs: +/- 20.00 hours
• Start with low dosage• <10 yrs: 0.5-1.0 mg• 10-16 yrs: 1.0-2.0 mg to max. 3 mg• >16 yrs: 1.0-3.0 mg to max. 5 mg
• Don’t go too high when the effect is insufficient!
Prescribe melatonin with / without DLMO?
• Decide for yourself: no guideline• Pragmatic
• Costs• Logistics
• Be aware of your own actions:• Off label• No reimbursement• Little research into long term side effects
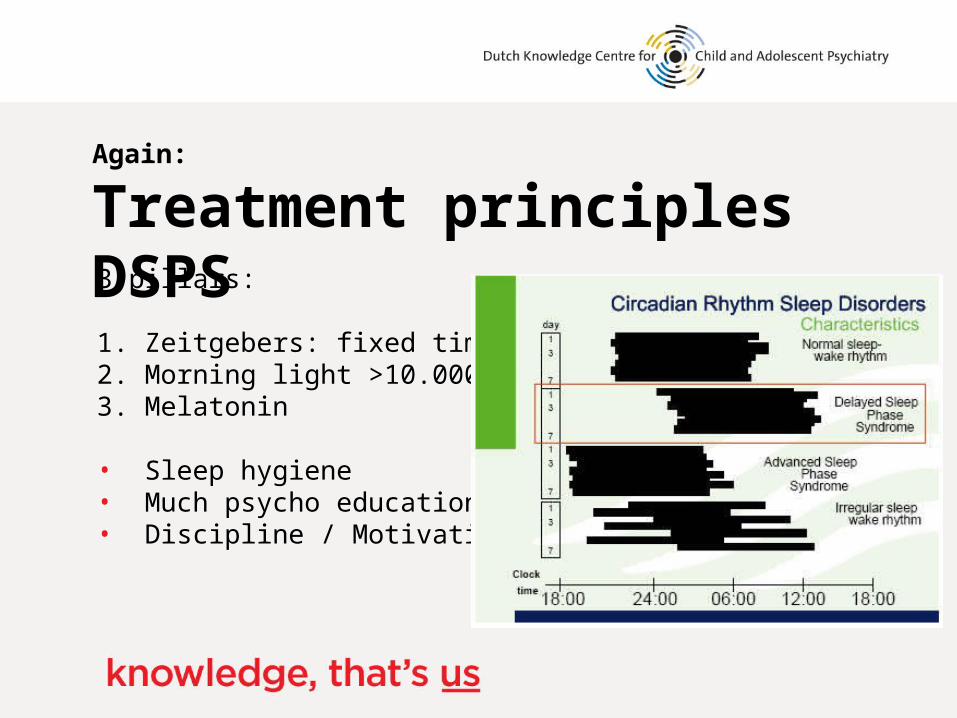
Again:
Treatment principles DSPS3 pillars:
1. Zeitgebers: fixed times2. Morning light >10.000 lux3. Melatonin
• Sleep hygiene• Much psycho education• Discipline / Motivation
Discussion• Do you recognise the symptoms in your own
patients? • Are there cultural differences in what people
consider ‘sleep problems’?