Embed Size (px)
DESCRIPTION
Gout for pharmacists; class version
Citation preview

GoutGout
Alexa Carlson, PharmD, BCPSNortheastern University

1. Define and explain commonly used medical terminology and abbreviations within the context of a patient case.
2. Describe and correlate signs and symptoms, epidemiology, risk factors, pathogenesis, natural history of disease, clinical course, etiology, and prevention and treatment of commonly encountered diseases.
3. Apply scientific knowledge and principles of medicinal chemistry, pharmacology, pharmaceutics, pharmacogenomics and pharmacokinetics to the design of rational therapeutic strategies
4. Identify evidence based, patient specific therapeutic goals and outcome measures for a patient started on a drug therapy regimen.
5. Apply evidenced based medicine to compare and contrast therapeutic options for a given medical problem and/or disease state in terms of safety, efficacy (including clinical evidence), ease of administration, cost, and other patient specific factors.
6. Design and defend a patient-specific therapeutic regimen, which is safe, efficacious and practical. For each drug selected, include drug name (generic and brand) dose, route, frequency and time of administration, and duration of therapy when applicable.
7. Predict the influence of selected drugs on a patient’s other diseases or problems and outline which agents should be avoided or monitored more carefully.

Neogi T. Gout. N Engl J Med. 2011:364(5):443-452.Khanna D, Fitzgerald JD, Khanna PP, et al. 2012 American College of Rheumatology Guidelines for Management of Gout. Part 1: Systematic Nonpharmacologic and Pharmacologic Therapeutic Approaches to Hyperuricemia. Arthritis Care & Research. 2012:64(10);1431-1446.Khanna D, Khanna PP, Fitzgerald JD, et al. 2012 American College of Rheumatology Guidelines for Management of Gout. Part 2: Therapy and Antiinflammatory Prophylaxis of Acute Gouty Arthritis. Arthritis Care & Research. 2012:64(10);1447-1461.Jordan DM, Cameron JS, Snaith M, et al. British Society for Rheumatology Guideline for the Management of Gout. Rheumatology. 2007;46:1372-1374.Zhang W, Doherty M, Pascual E, et al. EULAR evidence based recommendations for gout. Part I: Report of a task force of the standing committee for international clinical studies including therapeutics (ESCISIT). Ann Rheum Dis. 2006l65:1301-1311.Zhang W, Doherty M, Bardin T, et al. EULAR evidence based recommendations for gout. Part II: Management. Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2006;65:1312-1324.Roddy E, Zhang W, Doherty M. Concordance of the management of chronic gout in a UK primary-care population with the EULAR gout recommendations. Ann Rheum Dis. 2007;66:1311-1315.

Gout is the most common cause of inflammatory arthritis in the US
Substantial gaps in the management of gout
Significant lack of patient education and adherence to management

Hyperuricemia: elevated serum uric acidTophus: a calculus containing sodium urate that develops around fibrous tissue around joints, typically in patients with goutPodagra: a painful condition of the big toe caused by goutUricase: An enzyme that oxidatively degrade uric acid, thereby catalyzing conversion to soluble allantoin, which is much more soluble than uric acid. This enzyme is found in most animals, but not in humans.Uricosuric medications: Medications administered to increase the elimination of uric acid.

Elevated serum uric acid (SUA)>7mg/dL (416μmol/L) at 37°C for men>6mg/dL (357μmol/L) at 37°C for women
Considered to be the principle cause of gouty arthritis
Not all patients with hyperuricemia develop acute gout flares or chronic gouty complications

Clinical spectrum of disease:HyperuricemiaRecurrent acute arthritis attacks due to monosodium urate (MSU) crystals in synovial fluidDeposition of MSU into articular and extra-articular space (tophi)Interstitial renal diseaseUric acid nephrolithiasis
Primarily caused by elevated SUA levels, but can occur in patients with normal SUA levels.
http://www.healthinplainenglish.com/health/musculoskeletal/gout/
http://www.assh.org/Public/HandConditions/Pages/GoutandPseudogout.aspx

“Disease of Kings”Alexander the GreatKing Henry VIIIBenjamin FranklinAlexander HamiltonVoltaire
Health.com List of 8 people with gout: http://www.health.com/health/gallery/0,,20451892,00.html
Image from: antabusediaries.blogspot.com

Increasing prevalence of gout
Developed Countries > Developing Countries
3.9% of adults in the US (~8.3 million people)
$3.9 million in annual physician visits
Richette P, Bardin T. Gout. Lancet. 2010;375:318-28.

Date of download: 5/20/2014 Copyright © 2012 McGraw-Hill Medical. All rights reserved.
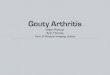
Purine metabolism. (HGPRT, hypoxanthine-guanine phosphoribosyltransferase; PRPP, phosphoribosyl pyrophosphate.)
Legend:
From: Chapter 74. Gout and Hyperuricemia
Pharmacotherapy: A Pathophysiologic Approach, 9e, 2014

Uric acid is the end product of purine metabolism

Elevated uric acid can occur from over-production or under-excretion of uric acid
Over-production:Less commonGenetic abnormalities in enzymes related purine metabolism
Increased phosphoribosyl pyrophosphate synthetase (PRPP)Decreased hypoxanthine-guanine phosphoribosylthransferase (HGPRT)
Increased cell turnover (cytotoxic chemotherapy, malignancies)
Under-excretion:More common (~90%)Decline in urinary excretion of uric acid
Can determine by measuring urine uric acid>600mg/24h over-production<600mg/24h under-excretion

Image from: www.goutrx.com

A. All patients with gout with progress to chronic tophaceous gout
B. All patients with gout have hyperuricemia
C. Patients with gout will have recurrent acute attacks separated by intercritical periods
D. Gout is primarily due to the overproduction of uric acid

Increasing age
Sex (Male > Female)
Hyperuricemia
Obesity
High Blood Pressure
Injury
Fasting
Recent surgery
Foods/Drinks
Medications
Medical Conditions
Genetics

Foods high in purines
Foods and drinks with high fructose corn syrup
Alcohol
Picture taken from: aldrodriguezliverfoundation.com

Diuretics (thiazide and loop diuretics)
Cyclosporine and tacrolimus
Low dose salicylates (<2g/day)
Levodopa
Pyrazinamide
Cytotoxic chemotherapy
Cyclosporine
Nicotinic Acid (Niacin)
Ethambutol

Chronic renal insufficiencyHypothyroidismRenal TransplantHypertensionCoronary heart diseaseMyeloproliferative disordersLymphoproliferative disordersLead toxicityStarvationAcromegalyDown’s syndromeHypoxanthine-guanine phosphoribosyltransferase deficiency
Diabetes mellitusVolume depletionKetoacidosisLactic AcidosisHyper/Hypo-parathyroidismSarcoidosisPreeclampsiaStarvationHeart FailureAcute alcoholismPhosphoribosylpyrophosphate synthetase overactivityPernicious anemiaPsoriasis

RT is a 48 year old male
PMH: HTN, Type II DM, CHF
SH: 5 pack-year history, drinks 2 beers per night
Current Medications: metoprolol XL 50mg po daily, aspirin 81mg po daily, lisinopril 20mg po daily, metformin 1000mg po BID, furosemide 40mg po daily

A. One
B. Two
C. Three
D. Four

Symptoms:Symptoms:•Rapid onsetRapid onset•Over night or after a trigger Over night or after a trigger (alcohol, meats, diuretics)(alcohol, meats, diuretics)•Excruciating painExcruciating pain
Signs:Signs:•Monoarticular arthritis early on Monoarticular arthritis early on (may become polyarticular in late (may become polyarticular in late gout)gout)•Often occurs in a joint in the lower Often occurs in a joint in the lower extremityextremity•Redness/Swelling/Inflammation/Redness/Swelling/Inflammation/Warmth of the jointWarmth of the joint•FeverFever•Elevated serum uric acid Elevated serum uric acid leukocytosisleukocytosis•Monosodium urate cyrstals in Monosodium urate cyrstals in synovial fluidsynovial fluid

http://knol.google.com/k/gout

• Differential Diagnosis:– Pseudogout (calcium pyrophosphate crystals)– Septic arthritis– Rheumatoid arthritis– Trauma
• Diagnosis:– Evidence of monosodium urate (MSU) crystals by
joint aspiration is gold standard for definitive diagnosis
– Often made on as a clinical diagnosis

Zhang W, Doherty M, Pascual E, et al. EULAR Evidence Based Recommendations for Gout. Part I: Diagnosis. Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis. 2006;65:1301-11.


• Level A: Supported by multiple (ie, more than one) randomized clinical trials or meta-analyses
• Level B: Derived from a single randomized trial, or nonrandomized studies
• Level C: Consensus opinion of experts, case studies, or standard-of-care

Colchicine, Colchicine, NSAIDs, NSAIDs,
CorticosteroidsCorticosteroids

http://rwglobal.com/~slpm/tipe/pictures/gout.jpg

• Acute flares are self-limiting
• Treatment objective is rapid relief of symptoms
• All therapy should be initiated within 24h of gout symptom onset and continued for 1-2 weeks
• Do NOT discontinue urate lowering therapy in an acute attack
Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

Ann Rheum Dis. 2006;65:1312-24.

• Mechanism of Action: Peripheral inhibition of COX leading to inhibition of prostaglandin synthesis
• Dosing:NSAID Typical Regimen
Etodolac 300mg Q12h
Fenoprofen 300-600mg Q6-8h
Ibuprofen 800mg Q6h
Indomethacin 25-50mg Q6h x 3d, then taper to Q12h x 4-7d
Ketoprofen 75mg Q6h
Naproxen 500mg Q12h x 3d, then 250-500mg daily x 4-7d
Piroxicam 20mg daily or divided Q12h
Sulindac 200mg Q12h x 7-10d

• Adverse Effects: increased BP, sodium and water retention, gastritis, GI bleeding
• Contraindications/Precautions:
Ann Rheum Dis. 2006:65:;312-24. NEJM. 2011:364(5);443-452.

• FDA-Approved: indomethacin, naproxen, sulindac
• NO NSAID has been shown to be superior to another
• Role in Therapy: – FIRST LINE for acute gouty attacks w/o
contraindication at high doses FIRST LINE alternative option to colchicine for prophylaxis

• Mechanism of Action: anti-inflammatory
• Dosing:Corticosteroid Typical Regimen
Prednisone 0.5 mg/kg/day x5-10d, then stop (Evidence A)<OR>0.5mg/kg/day x2-5d, then taper for 7-10d, then stop (Evidence C)
Methylprednisolone Methylprednisolone oral dose pack (Evidence C)
Methylprednisolone IM 100-150mg daily x1-2d
Triamcinolone IM 60mg once, then oral prednisone (Evidence C)
Triamcinolone intra-articular 10-40mg (large joints) or 5-20mg (small joints) once (Evidence B)

• Adverse Effects: hyperglycemia, leukocytosis, fluid retention, impaired wound healing, GI upset, insomnia
• Precautions: Infection, DM, peptic ulcer disease
• Role in Therapy: – FIRST LINE therapy in acute gout – Consider intra-articular corticosteroids in patients
with gout affecting 1-2 large joints– SECOND LINE therapy in prophylaxis to NSAIDs and
colchicineJanssens HJEM, Janssen M, van de Lisdonk EH, et al. Use of Oral Prednisolone or Naproxen for the Treatment of Gout Arthritis: a Double-Blind, Randomized Equivalence Trial. Lancet. 2008;371:1854-60.

Use of Oral Prednisolone or Naproxen for the Treatment of Gout Arthritis: a Double-Blind, Randomized Equivalence Trial
Methods Randomized, double-blind, double-dummy, active-comparator, controlled trial in monoarticular gout to assess equivalency
Intervention • Naproxen 500mg po BID x 5 days (n=59)• Prednisolone 35mg po daily x 5 days (n=59)
Primary Outcomes
Pain in the affected joint measured by the 100mm visual analogue scale
Results Reduction in mean pain score on visual analogue scale on day 4:•44.7mm prednisolone•46mm naproxen•Difference 1.3mm (95% CI -9.8-7.1)Relief of symptoms on day 4:•Clinically significant improvements: 80% prednisolone and 87% naproxen patients•Complete relief of symptoms: 22% prednisolone and 17% naproxen patients
Janssens HJEM, Janssen M, van de Lisdonk EH, et al. Use of Oral Prednisolone or Naproxen for the Treatment of Gout Arthritis: a Double-Blind, Randomized Equivalence Trial. Lancet. 2008;371:1854-60.

Janssens HJEM, Janssen M, van de Lisdonk EH, et al. Use of Oral Prednisolone or Naproxen for the Treatment of Gout Arthritis: a Double-Blind, Randomized Equivalence Trial. Lancet. 2008;371:1854-60.
Janssens HJEM, Janssen M, van de Lisdonk EH, et al. Use of Oral Prednisolone or Naproxen for the Treatment of Gout Arthritis: a Double-Blind, Randomized Equivalence Trial. Lancet. 2008;371:1854-60.

• Mechanism of Action:
– May interfere with the intracellular assembly of the inflammasome complex present in neutrophils and monocytes that mediates the activation of interlukin-1β
– Disruption of cytoskeletal functions through inhibition of β-tubulin polymerization into microtubules which prevents the activation, degranulation, and migration of neutrophils
Colcrys [package insert]. Philadelphia, PA: AR Scientific, Inc; 2012.

Methods Multicenter, randomized, double-blind, placebo-controlled, parallel-group study
Treatment Arms(n=184)
Placebo (n=59)Low-dose colchicine (1.2 mg po with 0.6 mg in 1 hour (1.8 mg total)) (n=74 )High-dose colchicine (1.2 mg po followed by 0.6 mg every hour for 6 hours (4.8 mg total)) (n=52)
Primary Outcome ≥50% pain reduction at 24 hours without rescue medication
Results Low and high-dose colchicine were significantly superior to placebo in reduction of pain at 24 hours (p=0.005, 0.034 respectively)
Overall adverse event rates for high-dose, low-dose, and placebo groups were 76.9%, 36.5%, and 27.1% respectively
Terkeltaub RA, Furst DE, Bennett K, et al. High Versus Low Dosing of Oral Colchicine for Early Acute Gout Flare. Arthritis Rheum. 2010;62(4):1060-68.

• Acute Flare:– FDA Approved: 1.2mg po at sign of first flare,
followed in 1 hour with a single dose of 0.6mg (max of 1.8mg)
– Real Life: FDA Approved dose (1.8mg total) then 12 hours later start prophylaxis dosing (0.6mg po daily or BID) until the end of the gouty attack.
• Prophylaxis: 0.6mg po once or twice daily (max 1.2mg daily)
Arthritis Care Res. 2012:64(10);1454.

• Prophylaxis:– No adjustments for mild-moderate renal impairment– Dose adjust to 0.3mg po daily in severe renal impairment– In patients on HD, the dose is 0.3mg po twice weekly
• Treatment:– No dose adjustments for mild-severe renal impairment– For severe renal impairment, treatment courses should not
be repeated more than once every 2 weeks– In patients on HD, the dose is 0.6mg po once, and
treatment courses should not be repeated more than once every 2 weeks

• Prophylaxis:– No dose adjustment needed for mild-moderate
hepatic impairment– Consideration to dose adjustment for severe
hepatic impairment
• Treatment:– No dose adjustment needed for mild-severe
hepatic impairment– In patients with severe hepatic impairment,
treatment courses should not be repeated more than once every 2 weeks

• Adverse Effects: – GI: Diarrhea, nausea, vomiting, abdominal
cramping/pain– Blood dyscrasias: myelosupression, leukopenia,
granulocytopenia, thrombocytopenia, aplastic anemia
– Neuromuscular Toxicity: myopathy, rhabdomyolysis, muscle weakness/pain
• Contraindication: patients with renal or hepatic impairment should not use colchicine with a p-glycoprotein (PGP) or strong CYP3A4 inhibitor
Colcrys [package insert]. Philadelphia, PA: AR Scientific, Inc; 2012.

• Drug Interactions: Substrate of CYP3A4, PGP; Induces CYP2C8, 2C9, 2E1, 3A4
– 3A4 Inhibitors
– PGP Inhibitors
– HMG Co-A Reductase Inhibitors, fibrates
Colcrys [package insert]. Philadelphia, PA: AR Scientific, Inc; 2012.

Colcrys [package insert]. Philadelphia, PA: AR Scientific, Inc; 2012.
Requires dose Requires dose adjustments if currently adjustments if currently
on these meds, or if on these meds, or if recently (w/in the past recently (w/in the past 14 days) on the meds 14 days) on the meds
listedlisted

• Role in Therapy:– FIRST LINE agent for acute gouty attacks w/in 36h
of attack (Evidence A)
– FIRST LINE prophylaxis in patients initiated on urate lowering therapy for up to 6 months (Evidence A)
• Cost: 0.6mg (30 tablets) $196.15
Colcrys [package insert]. Philadelphia, PA: AR Scientific, Inc; 2012.

• MOA:– Anakinra: Competitively inhibits IL-1 from binding
to the IL-1 type 1 receptors– Canakinumab: Recombinant IL-1β monoclonal
antibody • Dose:
– Anakinra: 100mg SQ daily x 3 days– Canakinumab: 150mg SQ once
• Role in Therapy:– Canakinumab is approved in the EU for acute gout– FDA has not approved either in America for gout

Medication BSR EULAR ACRNonsteroidal
Anti-inflammatory
Drugs (NSAIDs)
First line First Line First Line
Corticosteroid Effective Alternative
Effective Alternative
First Line
Colchicine Effective Alternative
First line First Line w/in 36h on attack
onset
British Society for Rheumatology (BSR), European League AgainstRheumatism (EULAR), American College of Rheumatology (ACR)
Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

• Comorbid conditions
• Effectiveness of past treatments
• Patient preference
• Joint involvement
• Severity
• Duration of attack
• Concomitant medications

Severity of Acute Gouty Arthritis Attack (based on 0-10 visual analog scale)
Mild ≤4Moderate 5-6
Severe ≥7
Duration of the gouty arthritis attack since onsetEarly <12h after attack onset
Well-Established 12-36h after attack onsetLate >36h after attack onset
Arthritis Care Res. 2012:64(10);1451.

Extent of acute gouty arthritis attackOne or a few small joints
1-2 large joints (ankle, knee, writs, elbow, hip, shoulder)Polyarticular:
• ≥4 joints w/arthritis involving more than 1 region (forefoot, midfoot, ankle/hindfoot, knee, hip, fingers, wrist, elbow, shoulder, other)
• Acute gout attack involving 3 separate large joints
Arthritis Care Res. 2012:64(10);1451.

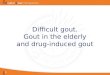
Adequate Response:Adequate Response:•>20% improvement >20% improvement in pain score w/in in pain score w/in 24h24h•≥50% improvement 50% improvement in pain score in pain score ≥ 24h 24h
Adequate Response:Adequate Response:•>20% improvement >20% improvement in pain score w/in in pain score w/in 24h24h•≥50% improvement 50% improvement in pain score in pain score ≥ 24h 24h
Combination Combination Therapy:Therapy:(1)(1)NSAID + NSAID + colchicinecolchicine(2)(2)Corticosteroids + Corticosteroids + colchicinecolchicine(3)(3)Intra-articular Intra-articular steroids + anythingsteroids + anything
Combination Combination Therapy:Therapy:(1)(1)NSAID + NSAID + colchicinecolchicine(2)(2)Corticosteroids + Corticosteroids + colchicinecolchicine(3)(3)Intra-articular Intra-articular steroids + anythingsteroids + anything
Figure 3 from Arthritis Care Res. 2012:64(10);1452.

Date of download: 5/20/2014 Copyright © 2012 McGraw-Hill Medical. All rights reserved.
Algorithm for management of an acute gout attack.
Legend:
From: Chapter 74. Gout and Hyperuricemia
Pharmacotherapy: A Pathophysiologic Approach, 9e, 2014
From: Chapter 74. Gout and Hyperuricemia
Pharmacotherapy: A Pathophysiologic Approach, 9e, 2014

Disease State Considerations for Selection of Acute Gout Therapy
CKD NSAIDs, COX-2 Inhibitors, Colchicine
CHF NSAIDs, COX-2 Inhibitors, Corticosteroids
Peptic Ulcer Disease NSAIDs, COX-2 Inhibitors, Corticosteroids
Anticoagulation/ Antiplatelet Therapy
NSAIDs
Diabetes CorticosteroidsInfection or Infection Risk Corticosteroids
Hepatic Disease NSAIDs, COX-2 Inhibitors, Colchicine

• Self-limiting disease; ~7-10 days of treatment usually required
• Colchicine/NSAIDs/Corticosteroids are all first line
• Select the agent based on insurance/joint involvement/pain severity/co-morbid conditions/concomitant medications/duration of attack
• Appropriate response is a 50% reduction in pain in 24h
• If a patient is on urate lowering therapy, it should not be stopped during the acute attack

RT is a 48 year old male with PMH significant for HTN, Type II DM, CHF
Patient presented to the emergency room with a 12 hour history of acute tenderness, and redness of his left big toe.
Pain Score: 4/10 on visual analog scaleBP 178/92 mmHg in ER
145 105 22
1263.8250

A. Naproxen 500mg po BID
B. Colchicine 1.2mg po once, then 0.6mg po one hour later
C. Prednisone 30mg po daily

A. Naproxen 500mg po BID
B. Colchicine 1.2mg po once, then 0.6mg po one hour later
C. Prednisone 30mg po daily
D. Intra-articular steroids


• Presentation:– Tophus: urate deposits– Fingers>olecranon bursae>forearm>achilles
tendon>knees>wrists>hand
• Late complication of gout, uncommon in the general population
• Complications:– Joint deformities and destruction– Pain– Damage to surrounding tissue– Nerve compression

Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

Upon discussion with RT in the ER, the physician discovers this is the third exacerbation RT has had this year.
Is RT indicated for urate lowering therapy?
A. Yes
A. No

LOW DOSE LOW DOSE Colchicine, NSAIDs, Colchicine, NSAIDs,
CorticosteroidsCorticosteroids

Image from: www.goutrx.com

Methods Randomized, prospective, double-blind, placebo controlled trial
Treatment Arms(n=43)
Colchicine 0.6 mg po BID (n=21)Placebo po BID (n=22)
Primary Outcome Number of gout flares during the initiation of allopurinol
Results Reduction in the number pts with acute gout flares (33% of colchicine pts versus 77% placebo pts (p=0.008))Reduction in the number of pts with multiple gout flares (14% of colchicine pts vs 63% placebo pts (p=0.004))
Borstad GC, Bryant LR, Abel MP, et al. Colchicine for Prophylaxis of Acute Flares When Initiating Allopurinol for Chronic Gouty Arthritis. J Rheumatol. 2004;31(12):2429-32.

• First Line: Colchicine or low dose NSAIDs– Colchicine 0.6mg po daily or BID – Low Dose NSAIDS (i.e. Naproxen 250mg po BID)
• Second Line: Corticosteroids– Prednisone or prednisolone ≤10 po mg/day
• Role: Initiated just prior to/at start of urate lowering therapy to prevent acute gouty attacks
Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.
Keep in mind to Keep in mind to check the need for check the need for GI prophylaxis with GI prophylaxis with long term NSAIDslong term NSAIDs

Figure 5 from Arthritis Care & Research. 2012;64(10):1457.
Signs/Symptoms of Signs/Symptoms of Gout: acute gouty Gout: acute gouty
arthritis in the past 3 arthritis in the past 3 months, presence of months, presence of
palpable tophus or tophi, palpable tophus or tophi, chronic tophaceous chronic tophaceous
gouty arthropathy (with gouty arthropathy (with chronic synovitis) in the chronic synovitis) in the
past 3 monthspast 3 months

RT is a 48 year old male with PMH significant for HTN, Type II DM, CHF
Patient presented to the emergency room with a 12 hour history of acute tenderness, and redness of his left big toe.
Pain Score: 4/10 on visual analog scaleBP 178/92 mmHg in ER
145 105 22
1263.8250

What prophylactic therapy would you want to use in RT and why?
A. Colchicine
B. Naproxen
C. Prednisone

Allopurinol, Allopurinol, Febuxostat, Febuxostat, Probenecid, Probenecid,
Pegloticase…Pegloticase…

• Mechanism of Action: Competitively inhibits the postsecretory renal proximal tubular reabsorption of uric acid
• Dose:
• Avoid use with renal impairment (CrCl <50)Probenecid. Lexi-Drugs Online, Lexi-Comp Inc. Hudson, OH. http://www.crlonline.com/crlonline. Accessed July 1, 2014.
Medication Dose
Probenecid 250mg po BID, titrated up to 500-2000mg/day
Sulfinpyrazone 50mg po BID, titrated to 100-400mg /day

• Adverse Effects:– Cardiovascular: Flushing– CNS: Dizziness, fever, headache– Dermatologic: Alopecia, dermatitis, pruritis, rash– Gastrointestinal: Anorexia, dyspepsia, GERD,
nausea– Hematologic: Anemia, aplastic anemia, hemolytic
anemia (in G6PD deficiency), leukopenia– Skeletal: Precipitation of acute gouty arthritis, – Other: rash, hypersensitivity, uric acid
nephrolithiasis

• Contraindication: History of urolithiasis, overproducers of uric acid, hypersensitivity to probenecid, small or large dose aspirin therapy, blood dyscrasias, <2 years of age, initiation during an acute gout attack
• Precautions:– Disease-related: G6PD, peptic ulcer disease, renal
impairment– Drug-related: Methotrexate, penicillin, salicylates

• Drug Interactions: – Salicylates– Penicillins/cephalosporins/carbapenems– Methotrexate– Pegloticase
• Monitoring: serum uric acid, urine uric acid, renal function
• Pt Education: Increase fluid intake ± urinary alkalization

• Place in Therapy:– “ALTERNATIVE” FIRST LINE therapy to xanthine
oxidase inhibitors (XOI)– May be used in conjunction with XOI in patients
not fully controlled on XOI alone
• Cost: Probenecid 500mg (100 tablets) $114.56

• If patient has HTN or hyperlipidemia consider the use of losartan and fenofibrate
• Both have uricosuric properties
• Place in Therapy: add-on to XOI in pts not controlled on single agent
Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

• Mechanism of Action: Xanthine Oxidase inhibitor which causes reduced uric acid production
• Dosing: Start at 50-100mg po daily– Titrate up every 2-5 weeks until a goal SUA <5-6
mg/dL– Doses >300mg usually given in divided doses– Max Dose=800mg/d
Allopurinol. Lexi-Drugs Online, Lexi-Comp Inc. Hudson, OH. http://www.crlonline.com/crlonline. Accessed July 1, 2014.Dalbeth N, Kumar S, Stamp L et al. Dose Adjustment of Allopurinol According to Creatinine Clearance Does Not Provide Adequate Control of Hyperuricemia in Patients with Gout. J Rheumatol. 2006;33(8)1646-50.

Dose Adjustment of Allopurinol According to Creatinine Clearance Does Not Provide Adequate Control of Hyperuricemia in Patients with Gout.
Methods Retrospective chart review of 250 patients attending rheumatology clinics in South Auckland between 2001 and 2004 diagnosed with gout
Analysis Groups(n=250)
•No allopurinol (n=23, 9.2%)•Lower than recommended allopurinol dose (n=22, 9.7%)•Recommended allopurinol dose (n=161, 70.9%)•Higher than recommended allopurinol dose (n=44, 19.4%)
Inclusion Criteria American College of Rheumatology diagnostic criteria for gout
Exclusion Criteria End stage renal failure receiving renal replacement therapy
Dalbeth N, Kumar S, Stamp L et al. Dose Adjustment of Allopurinol According to Creatinine Clearance Does Not Provide Adequate Control of Hyperuricemia in Patients with Gout. J Rheumatol. 2006;33(8)1646-50.

Group SUA Number of patients achieving SUA ≤6mg/dL (0.36mmol/L)
No allopurinol 0.57 mmol/L 1/23 (4%)
Lower than recommended
allopurinol dose
0.53 mmol/L 3/20 (15%, p=0.7 vs recommended allopurinol dose)
Recommended allopurinol dose
0.48 mmol/L 29/152 (19.1%)
Higher than recommended
allopurinol dose
0.48 mmol/L 16/42 (38%, p<0.01 vs recommended allopurinol dose)
Dalbeth N, Kumar S, Stamp L et al. Dose Adjustment of Allopurinol According to Creatinine Clearance Does Not Provide Adequate Control of Hyperuricemia in Patients with Gout. J Rheumatol. 2006;33(8)1646-50.

Dalbeth N, Kumar S, Stamp L et al. Dose Adjustment of Allopurinol According to Creatinine Clearance Does Not Provide Adequate Control of Hyperuricemia in Patients with Gout. J Rheumatol. 2006;33(8)1646-50.

• Renal:– Initiation of Therapy:
• 50mg for people with CKD stage ≥ 4• 100mg for everyone else
– Chronic Therapy:• “Dose can be raised above 300mg daily even with renal
impairment as long as it is accompanied by adequate education and monitoring for drug toxicity (e.g., puritis, rash, elevated hepatic transaminases; evidence B).
• The ACR guidelines do not recommend the non-evidence based renal dose adjustment algorithm for maintenance dosing
• Hepatic: no dose adjustments givenArthritis Care Res. 2012:64(10);1431-1446.

• Adverse Effects: – Dermatologic: Rash (<1%), Allopurinol hypersensitivity
syndrome (AHS)– Hematologic: agranulocytosis, aplastic anemia,
myeulosupression, thrombocytopenia– Renal: renal failure (<1%)
• Contraindications: allopurinol sensitivity, concurrent didanosine
• Drug Interaction: azathioprine, 6-mercaptourine (MUST reduce the dose of azathioprine or 6-MP when used in combination with allopurinol), theophylline, pegloticase, loop/thiazide diuretics, didanosine

• Monitoring: SUA every few weeks initially, HLA-B*5801 prior to initiation in high risk subpopulations (Koreans with stage 3 CKD or worse, and patients of Han Chinese or Thai descent).
• Place in Therapy: FIRST LINE agent for chronic gout
• Cost: 100mg (100 tablets) $24.24, 300mg (100 tablets) $60.81

• MOA: non-purine inhibitor of xanthine oxidase (XO)
• Dosage: – Initiate at 40mg po daily; if goal SUA is not achieved
by 2 weeks, increase to 80mg po daily– No renal/hepatic dosage adjustment in mild-
moderate impairmentUloric [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Inc; 2012.

• Adverse Effects: – Hepatic: abnormal LFTs– GI: nausea– Rheumatologic: Gout flares due to mobilization– Others: arthralgia, rash
• Contraindications: Concomitant use of azathioprine/6-mercaptopurine

• Precaution: – Acute gout flare
– Cardiovascular events
– Hepatotoxicity
• Drug-Interactions: azathioprine/6-mercaptourine, theophylline, pegloticase

• Monitoring: SUA after 2 weeks of treatment; LFTs at baseline and repeated if signs of hepatic injury
• Place in Therapy: FIRST LINE alternative to allopurinol
• Cost: – 40 mg (30 tablets): $256.99– 80 mg (30 tablets): $256.99

Febuxostat Compared with Allopurinol in Patients with Hyperuricemia and Gout.
Methods Randomized, multi-center, double-blind, phase 3 trial over a 52 week period
Treatment Arms(n=760)
•Febuxostat 80mg po daily (n=256)•Febuxostat 120mg po daily (n=251)•Allopurinol 300mg po daily (n=253)
Primary Outcome Serum urate concentration of <6mg/dL at the last three monthly measurements
Secondary Outcomes
Proportion of subjects with SUA <6mg/dL at each visit, percentage reduction of SUA from baseline at each visit, reduction in the incidence of gout flares, reduction in tophus
area, reduction in the number of tophi
Becker MA, Schumacher HR, Wortmann RL et al. N Engl J Med. 2005;353:2450-61.

Febuxostat Compared with Allopurinol in Patients with Hyperuricemia and Gout.
Results • Percentage of patients with SUA <6% at last 3 monthly visits• Febuxostat 80mg (53%)*• Febuxostat 120mg (62%)*• Allopurinol 300mg (21%)
• Incidence of gout flares (day 1-week 8)• Febuxostat 80mg (22%)• Febuxostat 120mg (36%)*• Allopurinol 300mg (21%)
Authors’ Conclusion Significantly more subjects receiving febuxostat v allopurinol achieved the serum urate concentrations <6mg/dL
* p<0.001 compared to allopurinol

• MOA: pegylated recombinant modified mammalian urate oxidase (uricase)
• Dose: 8mg IV infusion over 2 hours Q2 weeks; with corticosteroid and antihistamine pre-medication
Krystexxa [package insert]. East Brunswick, NJ: Savient Pharmaceuticals, Inc; 2012Sundy JS, Becker MA, Baraf HS, et al. Reduction of Plasma Urate Levels Following Treatment With Multiple Doses of Pegloticase (polyethylene Glycol-Conjugated Uricase) in Patients With Treatment-Failure Gout. Arthritis Rheum. 2008;58(9):2882-2891

• Adverse Effects: Gout flares, infusion reactions, nausea, vomiting, bruising, nasopharyngitis, constipation, chest pain, anaphylaxis
• Contraindication: Glucose-6-phospate dehydrogenase deficiency
Krystexxa [package insert]. East Brunswick, NJ: Savient Pharmaceuticals, Inc; 2012

• Precautions:– Anaphylaxis: Most often occurs within 2 hours of
the infusion; pre-medicate patients and observe them
– Infusion reactions: Give the infusion over no less than 120 minutes; if a reaction occurs, the infusion should be slowed or stopped and restarted at a lower rate
– Gout flares: Start gout flare prophylaxis with low dose NSAID or colchicine at least 1 week prior to starting pegloticase
– Congestive heart failure: Some patients in clinical trials have demonstrated CHF exacerbations

• Drug Interactions: No studies of pegloticase with other drugs have been conducted
• Monitor: SUA levels, G6PD screening prior to initiation in high risk patient populations (African and Mediterranean ancestry)
• Place in Therapy: – Refractory disease– Must have all other forms of urate lowering therapy
discontinued prior to its use
• Cost: $10026 (8mg/mL, 1mL)

XO inhibitors: allopurinol, febuxostat
XO inhibitors: allopurinol, febuxostat
Uricosurics: probenecid, losartan, fenofibrate
Recombinant uricase enzyme: Pegloticase
X
X

BSR EULAR ACRGoals of Therapy
≤ 5mg/dL ≤ 6mg/dL ≤6 mg/dL, and often ≤5 mg/dL
Prophylaxis for Acute
Gout
Colchicine for up to 6 months;
NSAIDs or COX-2 inhibitors in
patients who cannot take
colchicine for up to 6 weeks
Prophylaxis in the first months of urate lowering therapy can be achieved with
colchicine and/or NSAID
First Line: NSAIDs or colchicine
Second Line: Corticosteroids
Uricosurics (i.e.
probenecid)
Second line drug in under-excretors
or in patients resistant to allopurinol
Alternative to allopurinol in patients with normal renal
function
“Alternative” first line tx w/appropriate renal
function and intolerance or contraindication to
XOI; add-on to xanthine oxidase inhibitors when
not fully controlled
Ann Rheum Dis. 2006;65:1312-24. Rheumatology. 2007:1-17. Arthritis Care & Research. 2012;64(10):1431-1446.

BSR EULAR ACRAllopurinol Drug of choice;
Initial treatment starting at 50-
100mg/day and adjusted for renal
function if necessary, to reach a therapeutic target of
SUA <300μmol/L
Appropriate therapy; start at a
low dose (100mg/day), the
dose must be adjusted for renal
impairment
First Line
Febuxostat Not addressed Not addressed First Line
Pegloticase Not addressed Not addressed Refractory disease
Fenofibrate/losartan
Uricosuric Uricosuric Add on to appropriate XOI therapy
Initiation of Therapy
NOT during acute attack
NOT during acute attack
May start during acute attack if on
prophylaxis
Ann Rheum Dis. 2006;65:1312-24. Rheumatology. 2007:1-17. Arthritis Care & Research. 2012;64(10):1431-1446.

• Historically, we do not initiate urate lowering therapy during the acute attack due to risk of worsening the attack
• New guideline recommendation from ACR states “pharmacologic ULT could be started during an acute gout attack, provided that effective antiinflammatory management has been instituted (level C)”
• In practice, we are still waiting 1-2 weeks after the acute attack to start ULT
Arthritis Care & Research. 2012;64(10):1431-1446.

Figure 3 from Arthritis Care & Research. 2012;64(10):1437.
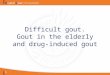
Long Term Long Term Monitoring:Monitoring:•SUA Q2-5 SUA Q2-5 weeks during weeks during ULT initiationULT initiation•SUA Q6 SUA Q6 months when months when stablestable

Table 4 from Arthritis Care & Research. 2012;64(10):1441.

• Unclear etiology of hyperuricemia
• Refractory signs/symptoms of gout
• Difficult to control and reach target SUA
• Multiple/serious medication related adverse events
Ann Rheum Dis. 2006;65:1312-24. Rheumatology. 2007:1-17. Arthritis Care & Research. 2012;64(10):1431-1446.

• Patient should be started on prophylaxis (low dose colchicine, NSAID, prednisone) just prior to or with the start of ULT
• XOI (allopurinol/febuxostat) are first line
• Uricosurics are usually second line or add on therapy, and should be avoided in over-producers
• Pegloticase is used in refractory disease. All other ULT must be stopped prior to starting pegloticase.
• Once on ULT, they should be maintained on ULT indefinitely. Should an acute exacerbation occur, the ULT should remain on.

These are being performed at the These are being performed at the same time. We look to see if they same time. We look to see if they need ULT, start the prophylactic need ULT, start the prophylactic therapy, and then start the ULT.therapy, and then start the ULT.

Date of download: 5/20/2014 Copyright © 2012 McGraw-Hill Medical. All rights reserved.
Algorithm for management of hyperuricemia in gout.
Legend:
From: Chapter 74. Gout and HyperuricemiaPharmacotherapy: A Pathophysiologic Approach, 9e, 2014
From: Chapter 74. Gout and HyperuricemiaPharmacotherapy: A Pathophysiologic Approach, 9e, 2014

Upon discussion with RT in the ER, the physician discovers this is the third exacerbation RT has had this year. He has only been given is 1.8mg total of colchicine thus far.
What is the next thing that should be given to RT?
A.Nothing—he is still in an acute exacerbationB.Probenecid 250mg po BIDC.Colchicine 0.6mg po BIDD.Naproxen 250mg po BID

What Urate Lowering Therapy would you want to start in RT, and why?
A. Allopurinol
B. Febuxostat
C. Probenecid
D. Nothing

When would you want to start urate lowering therapy in RT?
A.Immediately, he is already on prophylactic therapy
B.After he demonstrates appropriate response to his current treatment, which can double as prophylactic therapy
C.1-2 weeks after his current flare subsides while he is on concurrent prophylactic therapy

• Should always be considered alone or in combination with pharmacologic therapy
• Smoking cessation• Patient Education
• Exercise
• Weight loss
• Avoidance of risk factors (dietary, medication)
~10-18% ~10-18% decrease in decrease in
SUASUA

Rheumatology. 2007;46:1372-1374. Ann Rheum Dis. 2006;65:1312-24. Arthritis Care Res. 2012:64(10);1431-1446.

Avoid Limit Encourage
• Organ Meats high in purine (eg, sweetbreads, liver, kidney)
• Serving Sizes of:• Beef, lamb, pork• Seafood with high purine
content (eg, sardines, shellfish)
• Low-fat or non-fat dairy products
• High fructose corn syrup-sweetened sodas, other beverages, or foods
• Servings of naturally sweet fruit juices
• Table sugar, and sweetened beverages and desserts
• Table salt, including in sauces and gravies
• Vegetables
• Alcohol overuse (defined as more than 2 servings/day for males and 1 serving/day for females) in ALL gout patients
• Any alcohol use in gout during periods of frequent gout attacks, or advanced gout with poor control
• Alcohol (particularly beer, but also wine and spirits) in all gout patients
Figure 4 from Arthritis Care & Research. 2012;64(10):1439.

Given the following patient case, identify the options for non-pharmacologic treatment of gout:
• RT is 6’4” and 240lbs• He exercises some mornings during the week• RT generally has coffee for breakfast, a pepsi
with a roast beef sandwich for lunch, and scallops or steak with vegetables and beer for dinner.

• RT is 6’4” and 240lbs• Current Medications: metoprolol XL 50mg po
daily, aspirin 81mg po daily, lisinopril 20mg po daily, metformin 1000mg po BID, furosemide 40mg po daily
What medication risk factors does RT current have, and can we change any of his medications?

• Royal Pains: Season 2 Episode 10 (available on Netflix)– 13:20-14:33– 28:37-29:45– 33:25-35

• What would be in your differential diagnosis for this patient?
• What signs/symptoms of gout does this patient present with?
• Is this a typical acute gouty presentation?


A. Treatment plan is appropriate
B. Treatment plan is inappropriate


A. Start the allopurinol as planned.
B. Treat the acute attack, then start allopurinol
C. Treat the acute attack, then start low dose colchicine and allopurinol concurrently
D. Treat the acute attack and modify risk factors

• Acute– Non-Pharmacologic: rest, ice– Pharmacologic:
• NSAIDs, colchicine, corticosteroids to treat (~7-10 day)• CONTINUE ULT during the acute gouty attack!
• Evaluate if indicated for ULT: Tophi, CKD Stage ≥2, Urolithiasis, ≥2 acute gout attacks/year

• Chronic– Non-Pharmacologic: diet, fluids,
weight loss, smoking cessation, avoidance of risk factors
– Pharmacologic: • Prophylactic therapy: LOW DOSE
colchicine, NSAIDs, corticosteroids during initiation or just prior to initiation of ULT
• Urate lowering therapy (ULT) for indefinite duration dosed to SUA– Allopurinol/febuxostat> probenecid– Probenecid/losartan/fenofibrate may
be add on therapy– Pegloticase last line for refractory
cases
Neoni T. Gout. N Engl J Med. 2011;364:443-52.


• We probably wont have time to work on these during class, but Elizabeth Akselrod, PharmD Class of 2015, and I made some practice cases and questions for you to work on at home while studying for the quiz/exam.
• I will post our keys to the questions at the end of my version of the ppt slides after our lecture.

1. Which of the following is the goal of urate lowering therapy?A. SUA <6mg/dLB. SUA <4 mg/dLC. SUA <7mg/dLD. Lower the SUA until the tophi resolve
2. Which medication(s) work on xanthine oxidaseA. AllopurinolB. FebuxostatC. PegloticaseD. ProbenecidE. Both A and B

3) There is new evidence to support dosing allopurinol to a target serum uric acid, instead of renal dose adjustmenta) Trueb) False
4) Low dose colchicine is less effective than high dose colchicinea) Trueb) False

5) Patients being treated for gout should receive pharmacologic treatment only
a) Trueb) False
6) When initiating urate lowering therapy, which of the following can be given to prevent acute gout attacks
a) NSAIDsb) Colchicinec) Corticosteroidsd) All of the above

• MC is a 21 yoF who presents to her PCP for an annual checkup. Her parents have been concerned because lately she hasn’t been taking good care of herself. She’s been staying up late, eating lots of processed foods, drinking excessive alcohol since her 21st birthday, and has developed a “strange obsession with sticking her tongue out at people.” She presents with no symptoms and simply wants to “get this appointment over with so she can go party in the USA.”
• PMH: N/A• SH: Drinks 3-4 mixed drinks per day, quit smoking 4 weeks ago (1 pack per day)• Vitals: 98.6 F, BP 115/76, HR 80, RR 18, O2 Sat 98• Medications: Women’s MVI, daily laxative use to help with weight loss• Abnormal labs: SUA 7.2 mg/dL
• List all MC’s risk factors
• Does MC need treatment for gout? If yes, what would you recommend? If no, explain.

• RW (prefers to be called Fat Amy) is a 28 yoF who was shooting a film in Hollywood when all of a sudden she felt pain in her right big toe which was red and inflamed. She presented to the ER 3 hours later and stated that her pain was a 4/10. She has no history of acute gouty attacks.
• PMH: Type II DM, Obesity, GERD (no ulcers)• SH: 2 beers per night• SUA: 6.5 mg/dL; no tophi present• CrCl: 60 mL/min
• What treatment options can you recommend for RW?
• Does RW need chronic gout treatment? Prophylaxis? Explain.
• Provide one counseling point using patient-specific language.

• TS is a 59 yoM who presents to the ER for the 4th time this year with an acute gouty attack. He rates his pain as a 6/10 and says it started 24 hours ago. His history is significant for HTN (refuses to take his Lisinopril because it makes him cough), DMT2, s/p MI in 2009, migraines, gouty attacks with tophi, and s/p vehicle accident with fractured femur. SUA: 8. G6PD (-) and HLA-B*5801 (-).
• Recommend a plan for TS. Include drug name, dose, route and duration.
• If the patient was HLA-B*5801 (+), which medication would you have to avoid?
• Which medication(s) is contraindicated in G6PD deficiency?

• SN is a 63 yoM who has no significant PMH except has been taking Allopurinol 300 mg PO daily for 1 year due to frequent gouty attacks starting in 2005. At his annual physical, the doctor notes that SN has chronic knee pain and an SUA of 8.5 mg/dL. The doctor asks for your advice. Since you’re a gout expert, you know exactly what options are available and you recommend:
• List 3 non-pharmacologic options to educate SN about:

• HR is a 45 yoF who has had breakthrough gouty attacks despite Allopurinol treatment. Her PMH is significant for HTN, DMT2, hyperlipidemia, s/p kidney donation in 2010, and recent start on Azathioprine for RA. She tells the doctor that she has heard of an alternative to Allopurinol that also doesn’t require renal dosing. What is this drug? Is HR eligible to receive this medication? Why/why not?

• Dr. Sampson is a new resident and wants to start a patient on Allopurinol for chronic gout treatment. He asks you for help to make sure the patient is eligible to take this medication. What test should be ordered prior to starting the patient on Allopurinol?
• Which medications should you beware in the patient’s profile that interacts with Allopurinol?

• TY comes into your pharmacy to pick up his newly prescribed probenecid. He has never heard of this medication and knows nothing about it. You check his profile and confirm that he doesn’t have renal impairment and you approve the order. What important points should you make TY aware of?

• RC 67 year old African American male comes is a regular patient at your pharmacy. His past medical history includes Hypertension, diabetes, and atrial fibrillation. His current medication list includes: chlorthalidone 25mg po daily, metformin 1000mg po BID, aspirin 81mg po daily, verapamil 80mg po TID, and warfarin 5mg po daily.
• VS: within normal limits; BG: 150 (fasting this AM)
• He comes to your pharmacy with the following prescription. What would you want to do?

Colcrys 1.2mg po once followed by 0.6mg 1 hour later, then 12 hours later start 0.6mg po BID x 7 days.
RC 67
7/6/14