Embed Size (px)
Citation preview

HERITABLE EFFECTS OF RADIATION
ByDr.Ayush Garg

GERM CELL PRODUCTION AND RADIATION EFFECTS ON FERTILITY

BASICS OF GENETICS
• CHROMOSOME
- Contains long threadlike structures called DNA- Carries all the information that specifies a
particular human with his/her individual characteristics
- 22 pair of autosomes + 1 pair of allosomes

DNA
• Double helix
• Organic bases
• Sugar-phosphate backbone

• Gene – Finite segment of DNA specified by an
exact sequence of bases.
• Locus – Position of a gene
• Human genome – DNA of chromosomes +
DNA of mitochondria.
• 6 billion base pairs of DNA.
• Total no of protein encoding genes – 25,000 to
50000/haploid set of chromosomes.

MUTATION
• Any change in chromosomes, their genes, and their DNA.
• Include an array of changes in DNA, such as deletion, rearrangement, breakage in the sugar-phosphate backbone, and base alterations.

HERITABLE EFFECTS OF RADIATION
• Adverse health effects in descendants due to mutations induced in germ cells.
• Radiation does not produce new unique mutations, but increases the incidence of the same mutations that occur spontaneously.
• Information on the genetic effects of radiation comes almost entirely from animal experiments.


HERITABLE DISEASES
Mendelian
Chromosomal
Multifactorial


MENDELIAN INHERITANCE
• Autosomal Dominant• Autosomal Recessive• X-linked
Mendelian Diseases

Autosomal Dominant
• Expressed in the first generation after its occurrence.
• Eg’s - Polydactyly, achondroplasia, Marfan’s syndrome and Huntington's chorea.

Autosomal Recessive
• Require that the gene be present in duplicate to produce the trait
• Mutant gene must be inherited from each parent
• Eg’s - Sickle-cell anemia, cystic fibrosis, and Tay-Sachs disease.

X-Linked
• Mutations in genes located on the X-chromosome.
• Eg’s - Hemophilia, color blindness, and a severe form of muscular dystrophy

• 67% are caused predominantly by point mutations (base-pair changes in the DNA)
• 22% by both point mutations and DNA deletions within genes (i.e., they are intragenic)
• 13% by intragenic deletions and large multilocus deletions.

CHROMOSOMAL CHANGES• Abnormalities either in the structure of the
chromosomes or in the number of chromosomes• Down's syndrome• 40% of the spontaneous abortions• 6% of stillbirths• Radiation is much more effective at breaking
chromosomes than in causing errors in chromosome distribution.

MULTIFACTORIAL• Known to have a genetic component• Transmission pattern not simple Mendelian• Congenital abnormalities: cleft lip with or
without cleft palate; neural tube defects• Adult onset: diabetes, essential hypertension,
coronary heart disease• Interaction with environmental factors

RADIATION-INDUCED HEREDITARY EFFECTS IN FRUIT FLIES
• 1927 – Müller - exposure to x-rays could cause readily observable mutations in the fruit fly, Drosophila melanogaster.
• Included a change of eye color from red to white, the ebony mutant with its jet-black color, the “vestigial wing” mutant, and the recessive lethal mutation.

• Hereditary changes were considered the principal hazard of exposure to ionizing radiation because
– A low doubling dose (5-150 R) for mutations
– Hereditary effects were cumulative
– Little was known of the carcinogenic potential of
low doses of radiation.• The doubling dose is the dose required to
double the spontaneous mutation rate.

RADIATION-INDUCED HEREDITARY EFFECTS IN MICE
• Russell and Russell - Oak Ridge National Laboratory
• To determine specific locus mutation rates in the mouse
• Megamouse project - 7 million mice• An inbred mouse strain was chosen in which
seven specific mutations occur, 6 involving change of coat color & 1 as stunted ear.



• Five major conclusions1. The radiosensitivity of different mutations varies
by a significant factor of about 352. Dose rate effect was evident.
– Chronic dose exposure induces fewer mutations– Acute dose exposure induces more mutation– This is in contrast with Drosophila
3. The oocytes are exquisitely radiosensitive.4. The genetic effects of a given radiation dose can
be reduced greatly if a time interval is allowed between exposure and conception.
5. The estimate of the doubling dose adopted by BEIR V and UNSCEAR 88 is 1 Gy.

RADIATION-INDUCED HEREDITARY EFFECTS IN HUMANS
• Two basic pieces of data are needed:– Base-line spontaneous mutation rate in
humans – 738,000 per million.
– Doubling Dose (1 Gy, or 100 rad).

RADIATION AND SEX CELLS
• Resistant– Post-spermatogonial cells
• Sensitive– Stem cells
• Temporary sterility– 15 rad (0.15 Gy)– 40 rad/year (0.4 Gy/yr)
• Permanent sterility– 350-600 rad (3.5 to 6 Gy)– 200 rad/yr (2 Gy/yr)
• No significant hormonal imbalance
• Resistant– Post-oogonial cells
• Sensitive– follicles
• Permanent sterility– 250-600 rad (2.5 to 6 Gy)– 20 rad/yr (0.2 Gy/yr)
Pronounced hormonal imbalance
Males Females

Two Correction Factors
• Not all mutations lead to disease.• The mutation component (MC):
– 0.3 for autosomal dominant.– 0.0 for autosomal recessive.– 0.01-0.02 for chronic multifactorial.
• The 7 specific locus mouse mutations are not representative; they are genes not essential for viability. Only a small proportion of human genes, when mutated, would result in live births.


1. Assuming an average life expectancy of 75 years, with mean reproductive age stopping at 30 years
2. The risk coefficients for a total population of all ages will be 30/75, that is, 40% of that for a reproductive population.
3. This rounds out at 0.2% per sievert.
4. For a working population, the age range is only from 18 to 30 years because of the fact that no one is allowed to be a radiation worker before the age of 18 and the reproductive cycle is assumed to end at the age of 30
5. Consequently, the risk coefficients will be 12/75, or 16% of that for a reproductive population, which rounds out at 0.1% per sievert.

Hereditary Effects of Radiation - Human
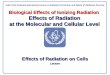
• Children of the survivors of Hiroshima and Nagasaki have been studied for untoward pregnancy outcomes, death of live-born children, sex chromosome abnormalities, electrophoretic variants of blood proteins.
• Though no genetic indication is statistically significant, the average doubling dose is 156 rem (1.56 Sv).

MUTATIONS IN THE CHILDREN OF THE A-BOMB SURVIVORS

CHANGING CONCERNS FOR RISKS• Dose limit of radiation workers reduced to
50mSv per year(by ICRP in 1956)• The level of concern regarding genetic effects
has declined steadily – as a consequence the percentage of radiation detriment attributed to the genetic component in view of ICRP has declined from 100% in 1955 to 4% in 2007
• The level of concern involving radiation carcinogenesis has increased as more and more solid tumours have appeared in the Japanese A-bomb survivors


EPIGENETICS• Changes in gene expression that takes place
without a change in the DNA sequence• The changes result from mainly these
molecular modifications - DNA methylation which takes place at the carbon – 5 position of cytosine in CpG dinucleotides - Changes to chromatin packaging of DNA by post translational histone modifications

• Pre natal and early postnatal environmental factors can result in altered epigenetic programming and subsequent changes in the risk of developing disease later in life
• Environmental changes studied include nutritional supplements, xenobiotic chemicals and exposure to ionizing radiation

• Radiation studies showed that exposure of adult mice led to transgenerational genome instability in the offspring resulting from a significant loss of DNA methylation in somatic tissue.
• In addition there is some evidence from animal studies that epigenetic alterations may be inherited trans- generationally thereby affecting the health of future generations

IMPRINTED GENES
• Expression is from only one parental allele with the other allele silenced – this leads to a non mendelian germ line inherited form of gene regulation that involves heritable DNA methylation and histone modification
• Expression of an imprinted gene in the present generation depends on the environment that it experienced in the previous generation

EFFECTS OF RADIATION ON THEEMBRYO AND FETUS

Commonly used measurements for ionizing radiation and their units
(Nuclear Wastelands, Makhijani et al., eds., Cambridge: MIT Press, 1995)
Units Description equivalent
Rem(roentgen equivalent man)
A unit of equivalent absorbed dose of radiation with relative biological effectiveness
rem = rad x Q
Sievert (Sv) A unit of equivalent absorbed dose equal to 100 rem.
1 Sv = 100 remSv = Gy x Q
Rad(radiation absorbed dose)
A unit of absorbed dose of radi-ation. Rad is a measure of the amount of energy deposited in tissue
1 rad = 100erg/gram
Gray (Gy) A unit of absorbed radiation dose equal to 100 rad. Gray is a measure of deposition of energy in tissue
1 Gy = 100 rad

Health impact of high-dose radiation from a nuclear disaster
• Cell death– Alter DNA of normal cells– Uncontrolled cell divisions– Induce cancer
• Damage organs– Acute radiation sickness (coagulopathy, immunity
disorders)– Diarrhea– Fever, burns, coordination & equilibrium disturbances

Ionizing radiation from Natural source

Ionizing radiation from Natural source
(World Nuclear Association)

Effects of Prenatal Radiation
Exposure

Effects of radiation in pregnancy
• Pregnancy loss• Malformation• Neurobehavioral abnormalities• Fetal growth restriction --- deterministic effect --- Threshold or NOAEL (No-Adverse-Effect Level)
• Cancer --- Stochastic effect --- More radiation, greater the chance of the disease --- No defined threshold

Effects of radiation in pregnancy
- Deterministic effect• Radiation dose, the trimester of the pregnancy
Ex) Pregnancy loss• During the 1st 2 weeks after conception, 100-200mGy (10-20 rad)• Shortly thereafter, 250-500 mGy (25-50 rad)• 18weeks, 5000mGy (500 rad)• At term, 20, 000mGy (2000rad)

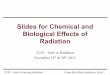
EffectMost sensitive pe-riod after concep-tion(d)
Threshold dose at effect was observed (mGy) Absolute
inci-dence
Animal studies Human studies
Perinatal death Preimplantation Postimplantation 0-8 50-100
250ND ND
Growth retardation 8-56 10 200 ND
Organ malformation 14-56 250 250 ND
Small head size 14-105 100 No threshold observed 0.05-0.1%
Severe mental re-tardation 56-105 ND 100 0.04%
Reduction of IQ 56-105 ND 100 ND
Childhood cancer 0-77 No threshold No threshold 0.017%
Fetal Effects from Low-level Radiation Exposure
(Wagner LK, 1997)

Radiation and mental retardation
• 8-15 weeks, : Risk of impaired CNS
development > 5 times than 16~25 weeks
• < 8 weeks, or > 25 weeks– No increased risk of
mental retardation

OVERVIEW OF RADIATION EFFECTSON THE EMBRYO AND FETUS

LETHAL EFFECTS
• These are induced by radiation before or immediately after implantation of the embryo into the uterine wall or are induced after increasingly higher doses during all stages of intrauterine development, to be expressed either before birth (prenatal death) or at about the time of birth (neonatal death).

MALFORMATIONS
• These are characteristic of the period of major organogenesis in which the main body structures are formed, and especially of the most active phase of cell multiplication in the relevant structures.

GROWTH DISTURBANCES AND GROWTH RETARDATION, WITHOUT MALFORMATIONS• These are induced at all stages of development
but particularly in the latter part of pregnancy.
• The principal factors of importance are the dose and the stage of gestation at which it is delivered.

Preimplantation, which extends from
fertilization to the time at which the embryo
attaches to the wall of the uterus
Organogenesis, the period during which the
major organs are developed
The fetal period, during which growth of the structures already
formed takes place.
Russell and Russell divided the total developmental period in utero into three stages:



Preimplantation

Organogenesis


EXPERIENCE IN HUMANS

Survivors of the A-Bomb Attacks onHiroshima and Nagasaki Irradiated In Utero

Exposure to Medical Radiation
• Dekaban surveyed the literature for instances of pelvic x-irradiation in pregnant women. Based on the available data, the following generalizations were proposed:
• 1. Large doses of radiation (2.5 Gy) delivered to the human embryo before 2 to 3 weeks of gestation are not likely to produce severe abnormalities in most children born, although a considerable number of the embryos may be resorbed or aborted.

• 2.Irradiation between 4 and 11 weeks of gestation would lead to severe abnormalities of many organs in most children.
• 3.Irradiation between 11 and 16 weeks of gestation may produce a few eye, skeletal, and genital organ abnormalities; stunted growth, microcephaly, and mental retardation are frequently present.

• 4. Irradiation of the fetus between 16 and 25 weeks of gestation may lead to a mild degree of microcephaly, mental retardation, and stunting of growth.
• 5. Irradiation after 30 weeks of gestation is not likely to produce gross structural abnormalities leading to a serious handicap in early life but could cause functional disabilities.

COMPARISON OF HUMAN ANDANIMAL DATA

63
Fetal Radiation Risk
• There are radiation-related risks throughout pregnancy which are related to the stage of pregnancy and absorbed dose
• Radiation risks are most significant during organogenesis and in the early fetal period somewhat less in the 2nd trimester and least in the third trimester
Less LeastMost risk

This table summarizes the lowest doses atwhich effects on the embryo and fetus havebeen observed.

CANCER IN CHILDHOOD AFTER IRRADIATION IN UTERO
The Oxford Survey of Childhood Cancers, published by Stewart and Kneale in the 1950s, suggested an association between the risk of cancer, principally leukemia, up to 15 years of age and exposure inutero to diagnostic x-rays. This was a retrospective case-controlled study and is summarized in this table

Radiation exposure on infants and lactating women
• Direct exposure to radiation on breast• Ingestion of radioactive pharmaceuticals
• Mammogram ---- breastfeeding (O)
• The highest radiation conc. in breast milk– 3-4 hours after adm. of radioactive pharmaceuticals– radiation absorbed by fetus < 3-10% of the total dose absorbed by a
woman– But, no negligible dose !– 1 Gy in infant :thyroid cancer(x10)
• CDC: if radioactive iodine ----stop breastfeeding !

Protection of pregnant women and fetuses from radiation exposure
• Maintaining a safe distance• Shielding one’s body from exposure• Avoiding ingestion of food and water contaminated with
radioactive particles in the air, rain, or soil
• In disaster, minimize the exposure• Lead-containing vest• In radioactive pharmaceuticals, hydration + voiding!
• If safe protocol, < 1mSv /year

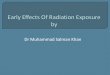
Probability of birth with no malformation and no childhood cancerDose to concep-
tus (mGy)No malforma-
tion (%)No childhood
cancer(%)No malforma-tion and No
childhood can-cer (%)
0 96.00 99.93 95.930.5 95.999 99.926 95.9281.0 95.998 99.921 95.9222.5 95.995 99.908 95.915.0 95.99 99.89 95.8810.0 95.98 99.84 95.8350.0 95.90 99.51 95.43100.0 95.80 99.07 94.91
(Wagner LK et al. 1982)

Thus…• ICRP (The International Commission on Radiological Protection)
– < 100mGy (10 rad) : Not medical ground for termination
• ACOG – Threshold for medical concern ~ 50mGy (5 rad)– > 1000mGy (100 rad) : Serious risk to fetus’ CNS---severe mental retardation– Single diagnostic radiation exposure? –10rad? 5 rad?

70
Research on Pregnant Patients
• Radiation research involving pregnant patients should be discouraged

THA
NK
YOU