Embed Size (px)
Citation preview

Carol Roberts CEO PrescQIPP CICJackie Smith Clinical Pharmacist PrescQIPP Deborah O’Callaghan NICE Implementation Lead
Improving Quality in Care Homes
A PrescQIPP and Eastern Academic Health Science Network Partnership
AHSNs – Improving health& promoting growth
Connecting NHS, academic organisations, local authorities, 3rd sector and industryCatalysts for spreading innovation at pace and scaleCreating an environment for industry to work with the health and care system

How AHSNs are improving health & promoting growth:Innovator Zone• 30 SMEs supported by AHSNs to spread their innovative technologies,
products, systems and processesRoundtable• AHSNs’ key roles in system-wide transformation (Thursday 10am-12pm)Visit our stand• Stand 50, all day Wednesday and Thursday
AHSNs – Expo key partner
Find out how AHSNs are improving health & promoting growth:Pop Up Universities:• Diffusing Innovation: NHS Innovation Accelerator• Improving Patient Safety (Deborah Evans,
Managing Director West of England AHSN, Thurs 1-1.45pm)
• Innovation Pathway: bringing together NHS & Industry (Dr Séamus O’Neill, Chief Executive North East & North Cumbria AHSN , Thurs 11-11.45am)
• Delivering the FYFV: Stroke prevention (Axel Heitmueller, Acting Managing Director Imperial College Health Partners AHSN, Thurs 1-1.45pm)
AHSNs – Expo key partner

Over the past year:• £20 million support for businesses through SBRI
Healthcare• Enabling 33,000 patients to self-manage with Flo
Simple Telehealth• 3 million patients benefiting from NHS
Innovation Accelerator• 800+ jobs created or safeguarded• 500 new products or services co-developed or
supported into the NHS• 365 strokes, one every day, prevented -
saving lives, reducing disability and saving
almost £8.5m to the NHS and social care
AHSNs – our impact

What is the size of the problem?

Where are most people cared for in beds?
• 325,000 older people are in care homes(4% of the over 65 population)
• 50% are estimated not to get the support they deserve from the NHS• 40% to 50% higher rates of emergency admission than in the general
population over 75• 42% admissions are in the last 6 months of life
• There are 134,000 general and acute beds in the NHS

Older people in care homes
• 17,678 care homes in UK• 78% privately owned• 405,000 older people (>65yr)• Average age 85 years• 80% cognitive impairment• 40% depression• 75% severely disabled• Going into care later, sicker and more frail• Median period (admission to death) is 15 months

Workforce
• Half a million employed in care homes
• Care assistants very poorly paid• Lack of funding for training• 66% NVQ2 (4 or 5 GCSEs)• 39% feel unappreciated by public• <25% registered for nursing
(mainly social care workforce)

Understand the context• > 3 x number of care home beds• Caring for some of the most vulnerable citizens in society• Projected to increase significantly
– >85yrs more than double in 23 years– >75yrs more than double in 30 years
• Residents going in later with more complex health problems• Medication safety
– Ave 8 medicines (polypharmacy)– 7/10 patients experience medication errors
• Workforce needs healthcare training and/or better access to health expertise.

NICE: Supporting quality and safety in care homes
Deborah O’Callaghan, NICE Implementation Consultant
Overview
Supporting safety and quality in care homes session overview:
• NICE: who we are and what we do
• Using NICE guidelines in care
homes
• Using NICE Quality Standards in
care homes
• Practical help
• Finding what you need
• Example event programme

NICE: Who we are and what we do
The role of NICE
Produce evidence-based guidance and advice for health, public health and social care practitioners
Develop quality standards and performance metrics for providers, commissioners and practitioners
Provide a range of information services for commissioners, practitioners and managers across health and social care
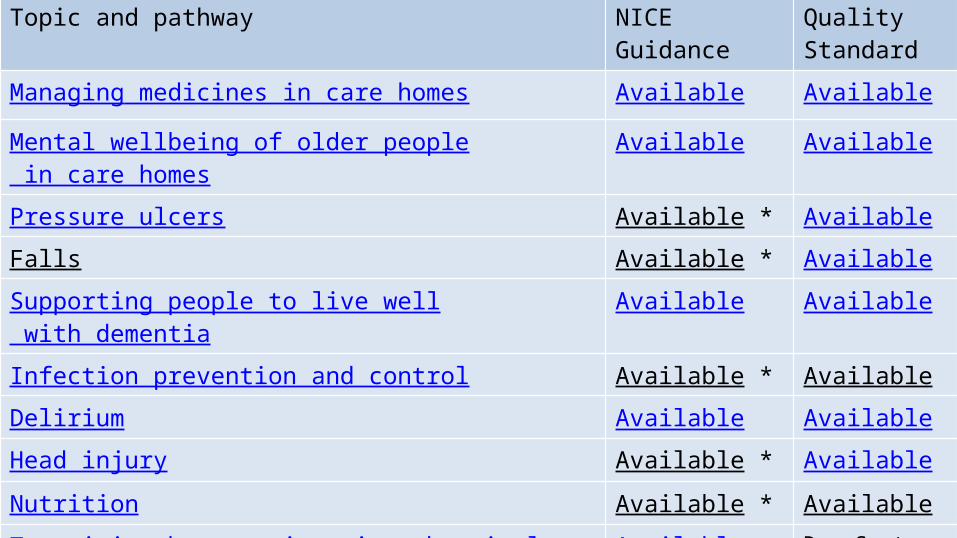
Topic and pathway NICE Guidance Quality Standard
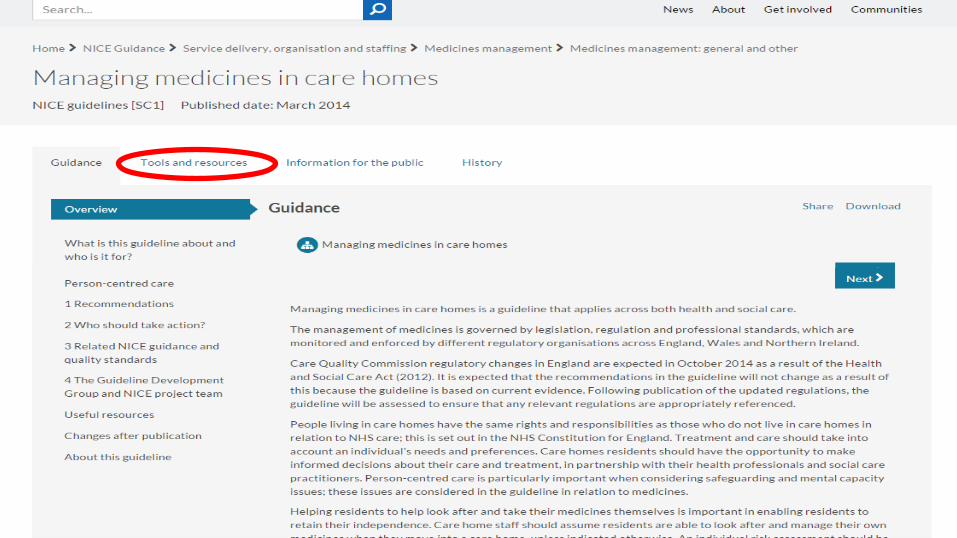
Managing medicines in care homes Available Available
Mental wellbeing of older people in care homes Available Available
Pressure ulcers Available * Available
Falls Available * Available
Supporting people to live well with dementia Available Available
Infection prevention and control Available * Available
Delirium Available Available
Head injury Available * Available
Nutrition Available * Available
Transition between inpatient hospital settings and community or care home settings
Available Due Sept 2016
Oral health for adults in care homes Available Due July 2017
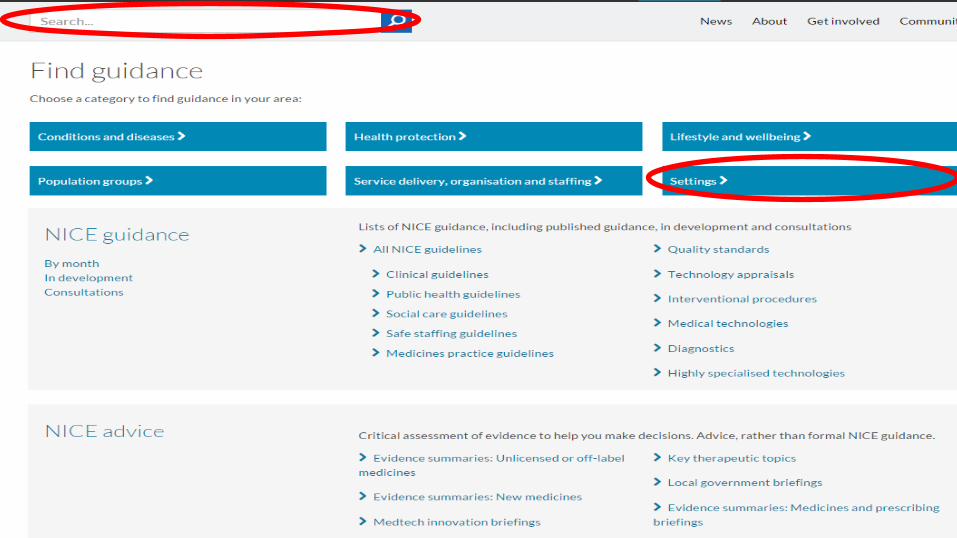
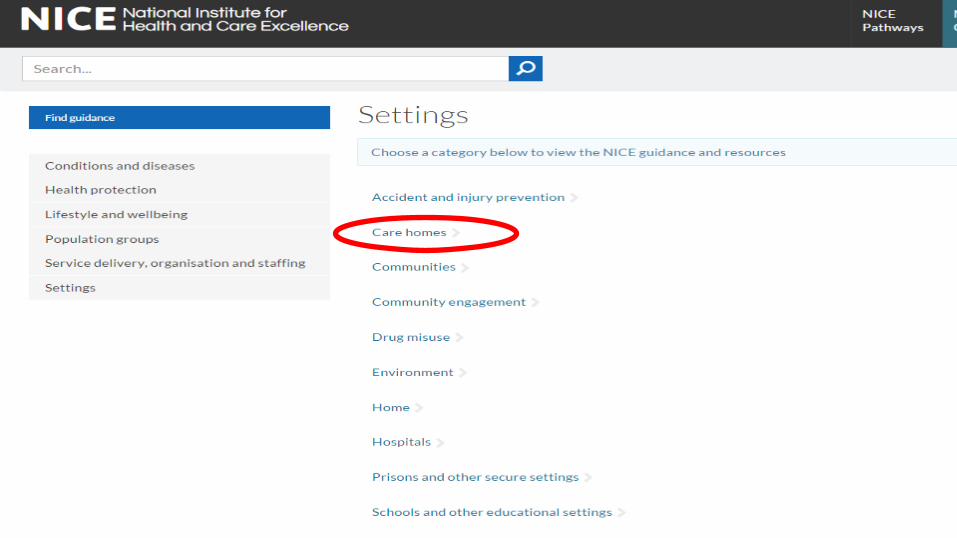
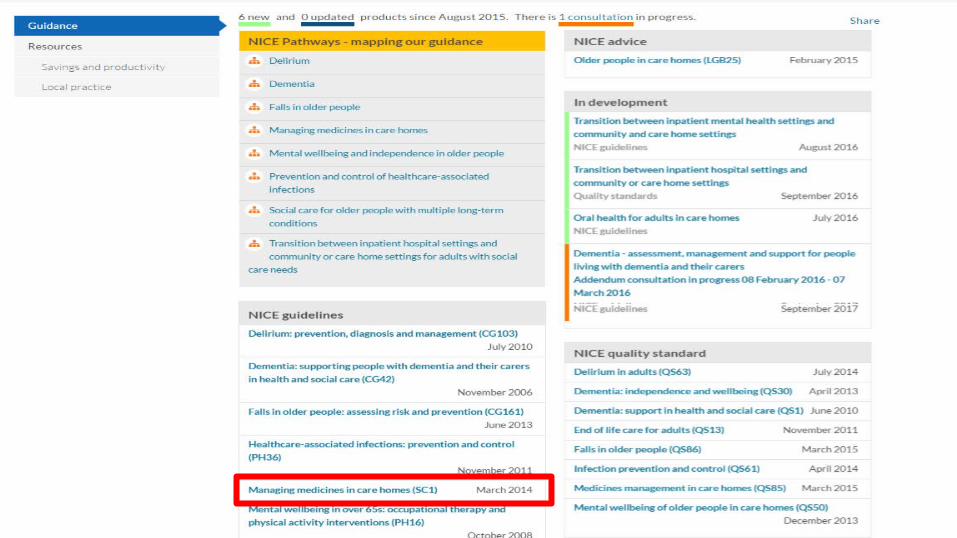
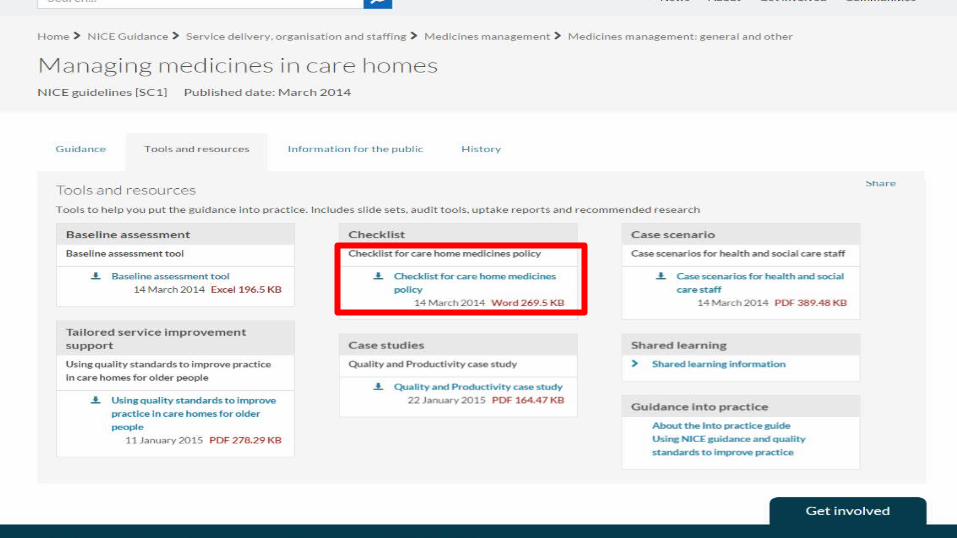
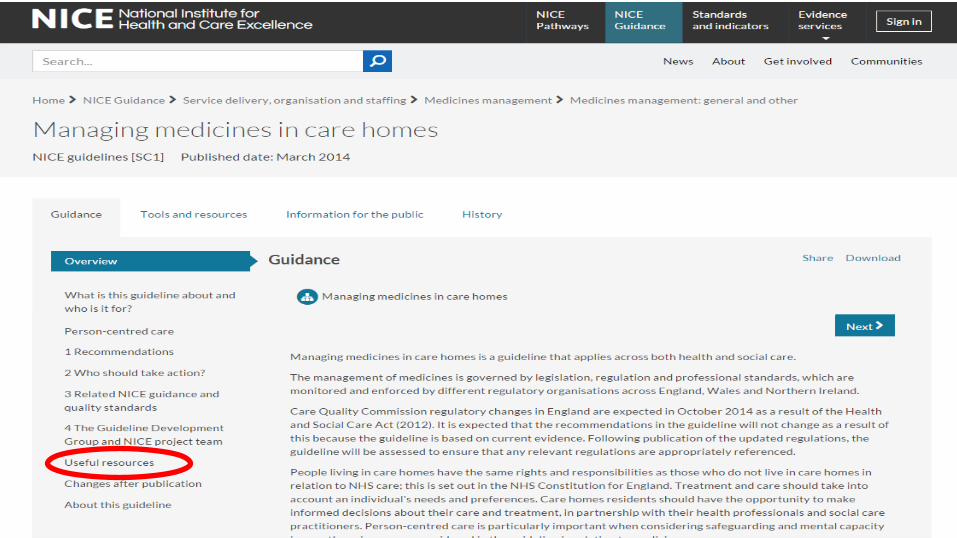
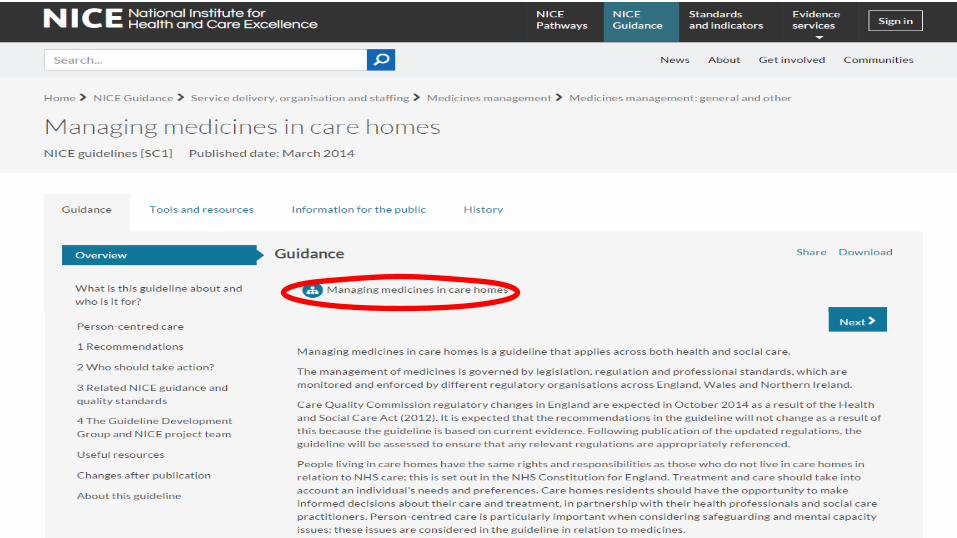
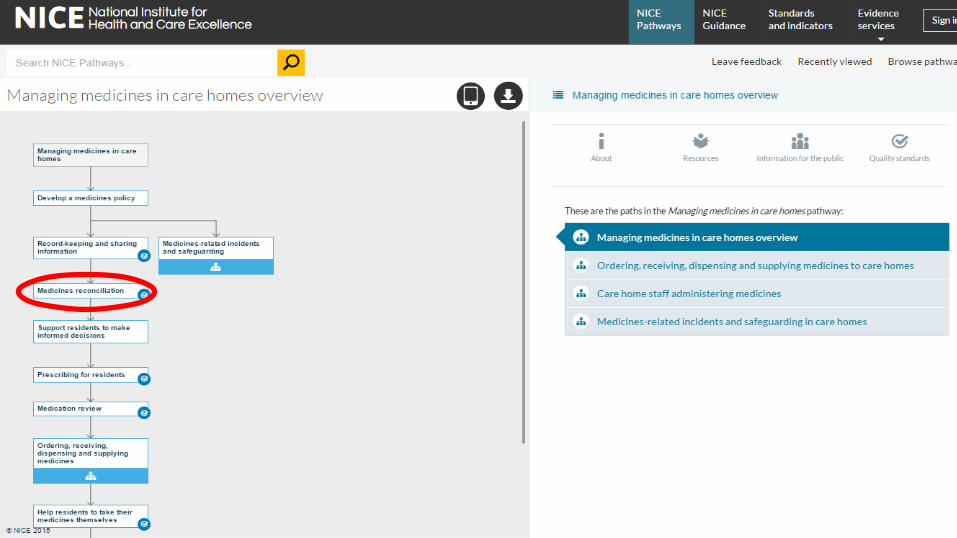
Using NICE guidance in care homesFinding what you need and practical help
www.nice.org.uk




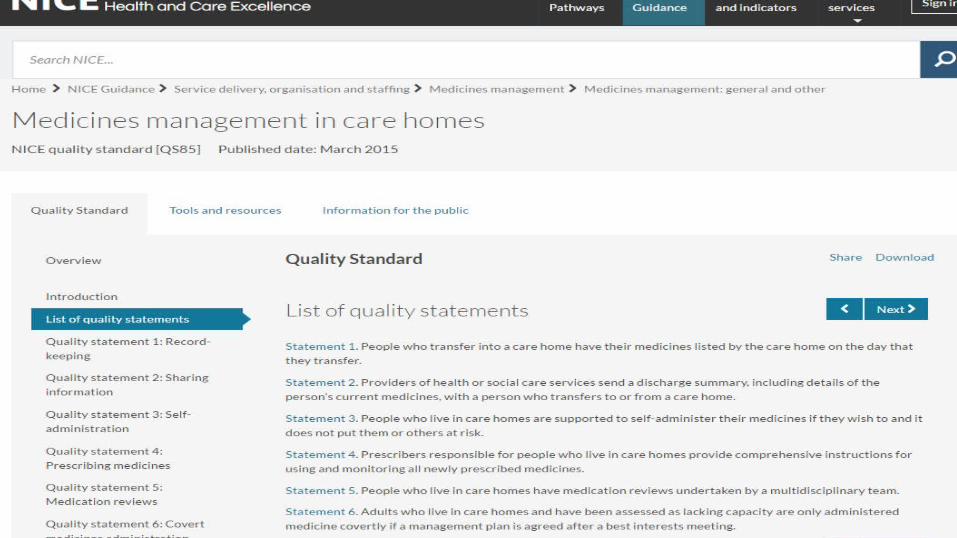
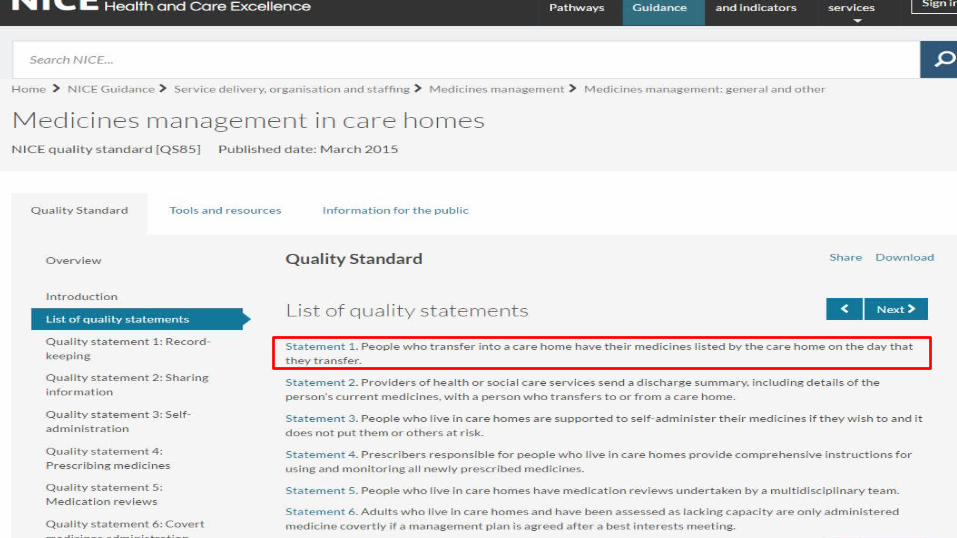
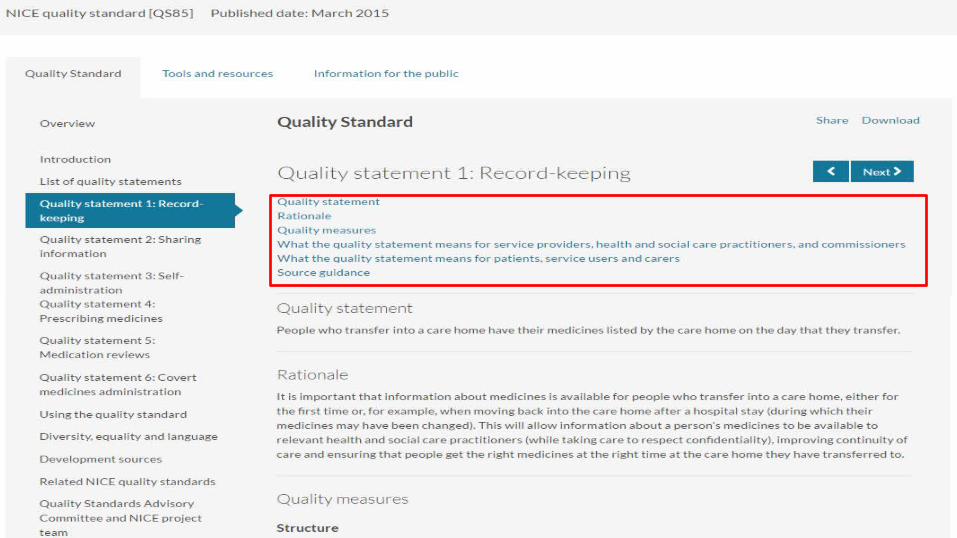
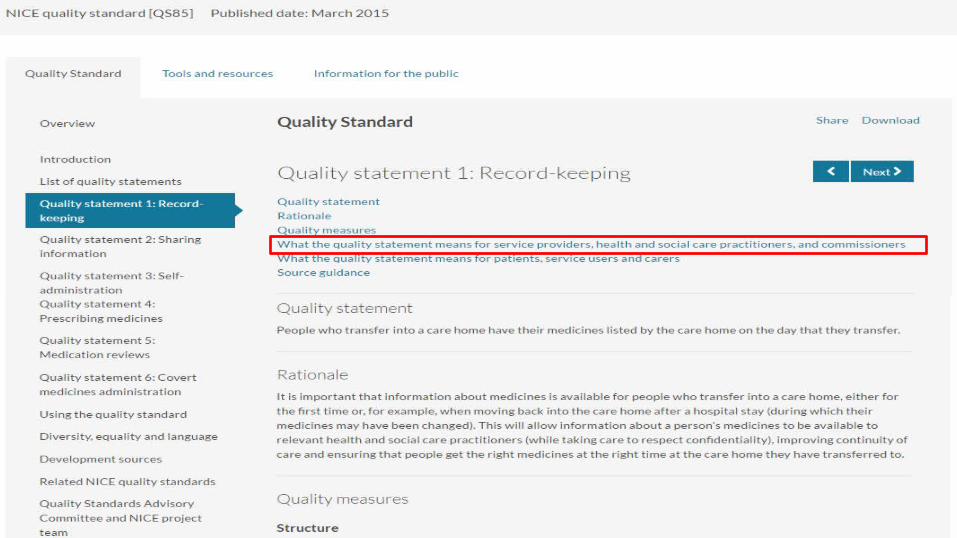
Using NICE Quality standards in care homes

Evidence Guidance Quality
Standards
A NICE quality standard is a concise set of statements designed to drive and measure priority quality improvements.
A set of systematically developed recommendations to guide decisions for a particular area of care or health issue
Research studies - experimental and observational, quantitative and qualitative, process evaluations, descriptions of experience, case studies

Evidence sources• Managing medicines in care homes (2014) NICE guideline SC1• Care Quality Commission (2015) Guidance for providers on meeting the regulations• Royal Pharmaceutical Society (2014) Pharmacists improving care in care homes• Department of Health (2013)
Best practice for ensuring efficient supply and distribution of medicines to patients• General Medical Council (2013)
Good practice in prescribing and managing medicines and devices• National Care Forum (2013) Safety of medicines in the care home• National Care Forum (2013)
Safety of medicines in care homes: Framework: Making the best use of medicines across all care settings
• Royal Pharmaceutical Society (2013) Medicines optimisation: helping patients to make the most of medicines
Evidence sources cont.• Care Quality Commission (2012) Meeting the health care needs of people in care homes• Department of Health (2012)
Action plan for improving the use of medicines and reducing waste• Royal Pharmaceutical Society (2012) Improving pharmaceutical care in care homes• Royal Pharmaceutical Society (2012)
Keeping patients safe when they transfer between care providers – getting the medicines right• Social Care Institute for Excellence's (SCIE) (2012)
Commissioning care homes: common safeguarding challenges• Centre for Policy on Ageing (2011)
A report for the project: Working together to develop practical solutions – an integrated approach to medication in care homes
• Report to the Patient Safety Research Portfolio, Department of Health (2009) Care home use of medicines study (CHUMS): prevalence, causes and potential harm of medication errors in care homes for older people
• National Prescribing Centre (2009) A guide to good practice in the management of controlled drugs in primary care (England)

Evidence sources cont.
• Department of Health (2008) Medicines management: everybody's business• National Prescribing Centre (2008)
Medicines reconciliation: a guide to implementation• Nursing and Midwifery Council (2007) Standards for medicines management• Royal Pharmaceutical Society (2007) The handling of medicines in social care• Department of Health (2003)
National service framework for children, young people and maternity services: medicines for children and young people

2
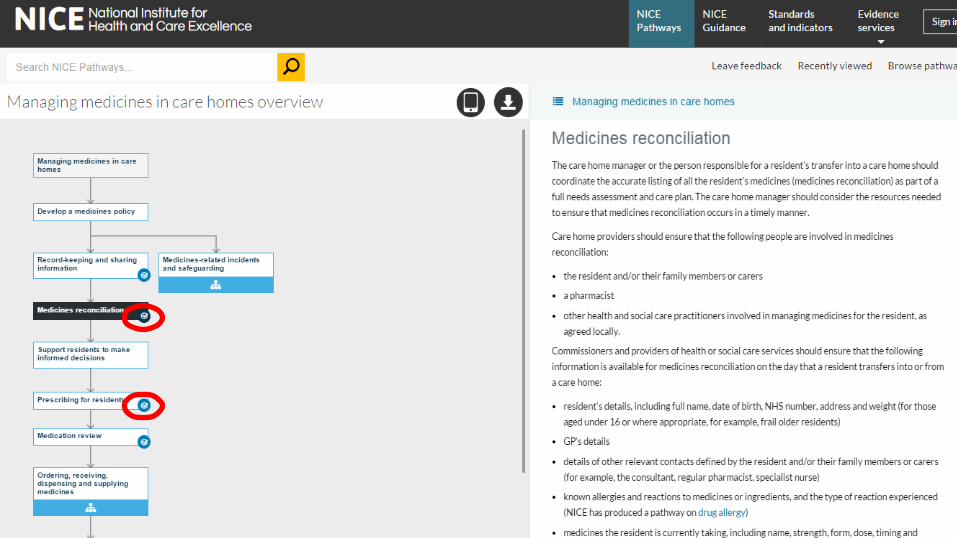
Suggested service review questions:How do we ensure that a list is made of a person’s medicines on the day that they transfer into our care?1. Who is responsible for listing a person’s medicines on the day that they transfer into our care?2. At what stage is the list made?3. Do we use a template?4. Does the person completing the list of medicines routinely provide their details (name, job title)
and the date the list was recorded?5. Once written up, where is the list kept?

Regulation - CQC
Andrea Sutcliffe, Chief Inspector for Adult Social Care at the CQC“At the CQC we are asking the questions that matter to people. We’re asking whether services are safe, caring, effective, responsive to people’s needs, and well led.
“And the way that we can do this is by identifying key lines of enquiry – so the questions that we will ask when we go out on inspections. We will also identify what the characteristics are of the services that we see, so whether they are good, outstanding, require improvement or are inadequate.
“This quality standard will inform the questions that we ask, and help us to provide the understanding of what ‘good’ and ‘outstanding’ practice looks like in this area.”
https://www.youtube.com/watch?v=RxwHM0JsdyI

Event programme10.00 Welcome and introductions (Carol Roberts)10.15 What is the size of the problem? (Carol Roberts) 10.30 Managing medicines in Care Homes – NICE guidelines and supporting resources
(Deborah O’Callaghan) 11.15 Refreshment break 11.30 Workshop – Case scenarios (Jackie Smith) 12.00 Feedback and discussion around case scenarios (Jackie Smith) 12.30 Common problems in medicines management (Jackie Smith) 13.00 Lunch and networking 13.45 Using NICE Guidelines and Quality Standards to support quality in Care Homes 14.15 Workshop – using quality standards to inform service review and improvement
(Deborah O’Callaghan and Jackie Smith)15.00 Refreshment break 15.20 Future work – Acute Kidney Injury (Joanne Lowe) 15.40 Summing up and next steps (Carol Roberts)
Keeping up to date
• Sign up for the NICE News• Log on to the website and register
your details at www.nice.org.uk• Register as a Stakeholder for Social
Care Guidance and Quality Standards: [email protected]
• Email: [email protected]

Practical medication issues encountered in Care Homes
Jackie Smith Clinical Pharmacist
Who am I?Care Homes Lead pharmacist
BCCG 2008-2015- eyes of a commissioner
Complex care team pharmacist 2010-11 –eyes of a provider (patient focussed)– still in this role- team support- not just about medication
GP clinical pharmacist- through the eyes of the prescriber
Sessional pharmacist for care provider- systems focused + eyes of the carers/nurses
Responsibilities to our patients/residents
“Residents have the right to access their medicines at the times they need them, and in a safe way” (CQC Essential standards of quality and safety Outcome 9).This means that they must be available, stored safely, administered as prescribed and recorded appropriatelyWould appear to be a simple requirement….. BUT
The role of CQCCQC are regulatorsSafety in all aspects of medicine
management Dignity and respect- mental
capacity issues, the right of refusal, best interest decisions
Processes and patient centred care
Meeting the needs of the individual
There are no shades of grey!!!-
The role of the care workersTo meet the needs of each
individual resident to manage their medication safely
To provide evidence that this is being carried out at every stage through record keeping
To deliver this aspect of care in a timely manner
To respect dignity and capacity to make decisions
Medicines management isn’t just giving medication…….
Ordering- time it takes!!, variety of methods, complexity, stock management,
prescription issuesSupply issues-timely
deliveries, availability of stock Receipt of stock-missing
items, caring time checking in, unwanted items received,
medication has changed ……
Respecting individualsEncouraging independence
understanding the risk/benefit issues
risk assessments for self administration
mental capacity assessments for refusalManaging expectations of relatives Respite care
Record Keeping
Not just administration…stock levels- carried
forward stock+ drugs for destructionchanges in medicationaccurate and consistent
recording- (no standard MAR chart)
evidencing prn prompts
The real world of the carer in a 50 bed homeMedication round starts at 8am. 2
carers responsible for medication. They are wearing “do not disturb” tabards
Some of the residents are still asleep, some are at breakfast, some are refusing to take their medicines, some have 10+ medicines and want them individually, some have advancing dementia and need gentle encouragement
One resident arrived 2 weeks ago and no-one has re-ordered their medicines- there is none to give this morning
It gets worse!!!- it is now 10amThe phone rings- it’s the GP
surgery Two doctors arrive for visitsA relative has a complaint and
will only speak to the seniorJust when you thought it couldn’t get worseSomeone is asking for “prn”
analgesia which was forgottenA new admission arrives with
their medicationIts now 11.15. The “do not disturb” tabard is meaningless!!
The reality of our demandsA morning drug round should not
finish later than 10.30?A 50 bed home – 25 residents
each carer2.5 hours=150mins. This gives
a carer 6 minutes for each resident.
This includes selecting the correct medication safely, finding the resident, watching them take the medicines without rushing them, recording the process
What about inhalers, patches, creams, PEG feeds, CDs?
Time for monthly ordersThis home has 15 surgeries
supporting the 50 residentsFor each resident the current
MAR chart must be checked against the repeat prescription to ensure no changes have occurred
The stock levels should be checked for prn medication
Emollient creams are kept in each residents room…
Pressures…Social care funding reductions
presenting staffing issuesHome managers seeing convenient
compliance aids as a way of reducing time for drug rounds
More complex health needs managed by non-clinical staff
More evidence for every stage of medication management
Medicines optimisation- effective use of our medicines
Stock management- reduced waste
Additional demandsManaging pain-use of pain
assessment toolsManaging swallowing difficulties-
correct use of thickeners, appropriate liquids
Managing dementia-refusal, pain, antipsychotics
Managing specific conditions e.g Parkinson’s-specific times
Managing bowels-appropriate use of laxatives
Managing “prn” medication- with no clinical knowledge
Clinical aspects - what about healthcare responsibilities!!!
GP communication-poor transfer of information, remote prescribing processes, updating records
Communication between professionals-no links, still paper driven, poor pathways
Supporting non-clinical staff -ensuring staff can deliver what is required safely, respecting their knowledge of residents
Documentation of all interventions in care plans and MAR sheets
Risks –where does it go wrong?
We must not put non-clinical staff in situations which require clinical decisionsTransfer of care & information
Hospital dischargeRegistering with new GPMoving from one
environment to anotherCommunication between
professionalsPharmacists, community
services, GPs -Working togetherCommissioning must recognise the increasing demands

Role of NICE quality standardsEvery manager wants their service to be the best. Using the NICE tools will……Help to provide evidence that the service is well-led, with a focus on quality improvementHelp to assess the performance of the care home against the quality statements Help to develop an action plan to achieve the levels of quality outlined in each statement Help to continuously monitor performance and strive for improvement

Over to you….
How can we support safe and effective medicines management?Two questions for discussion:1.What can we introduce to make the
process driven tasks in medicines management less time consuming thereby enabling carers to optimise medication use safely?
electronic systems?standardised MAR charts?one GP supporting a home?
….. other ideas….
And…
2. Consideration is being given to utilising clinical pharmacists to support care homes. The focus is very much on medication reviews. What other roles do you think pharmacists could provide?
Carol Roberts [email protected] Deborah.Ocallaghan [email protected] Smith [email protected]
Contact for further information