Embed Size (px)
Citation preview

Inpatient Rounding 30 Minutes a Week to Amazing Patient Experiences
Edward Pillar, DO, and Julie Lyall, RN
When we asked hospital administrators what keeps
them up at night …

They ranked patient experience among their
Top 3 Concerns
Experience of care (as measured by the HCAHPS survey) accounted for 25 percent of the federal value-based
reimbursement in 2016.
Experience of care (as measured by the HCAHPS survey) accounted for 25 percent of the federal value-based
reimbursement in 2016.
For a mid-sized hospital, that can translate into tens of thousands of dollars in lost revenue every year.
Emergency Care Is Key HCAHPS is an inpatient survey. However … • Over half of hospital patients are admitted from the
ED. • Patients admitted through the ED tend to be less
satisfied with their hospital experience.
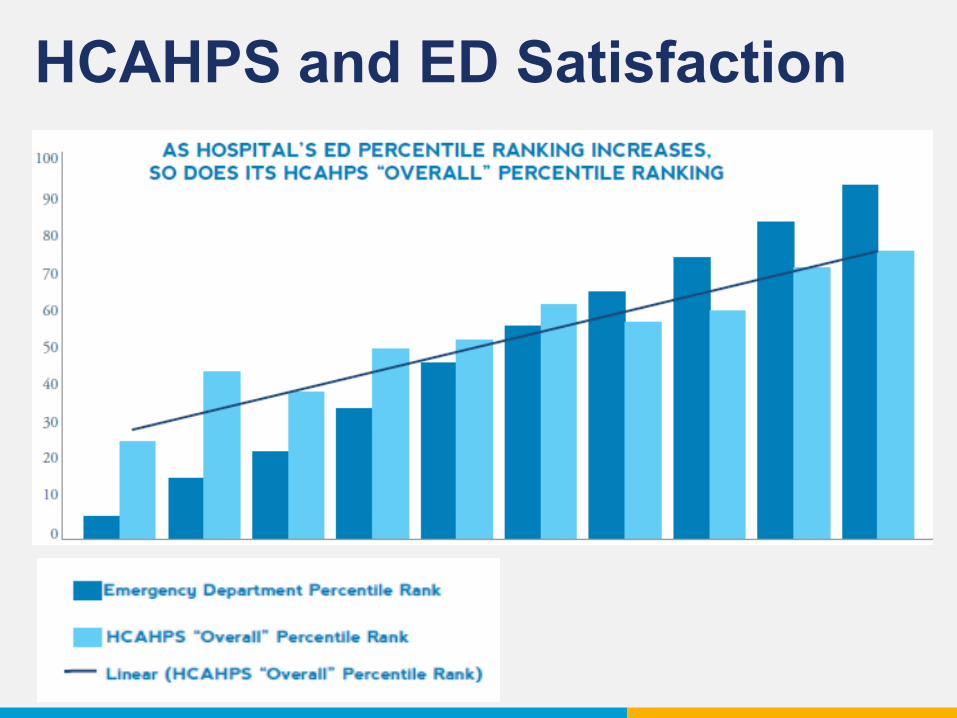
HCAHPS and ED Satisfaction

And it’s not just about data and quality metrics.

Compassion Is Always Right
Patients sacrifice privacy and control over most aspects of their lives when
entrusting themselves to our care.

Compassion Is Always Right
Patients sacrifice privacy and control over most aspects of their lives when
entrusting themselves to our care.
50 percent of patients and physicians say that compassion is missing from the
U.S. healthcare system.
Source: Lown BA, Rosen J, Marttila J. An Agenda for Improving Compassionate Care. Health Affiliate. 2011;30(9):1772-1778
“We can provide the right diagnosis and excellent service every time. But if we don’t serve it up with an experience where
the patient feels valued and cared for, then the patient won’t
want to come back.”
Edward Pillar, DO
So that’s where we come in.
Edward Pillar DO Director of Quality and Performance
Julia Lyall RN Patient Experience Program Manager
Several years ago, we were working together as the ED
Medical Director and ED Nurse Manager of a Level II Trauma
Center in California.
Back then, our admitted patients weren’t scoring us very highly on
HCAHPS.
And we didn’t know why.
After they left our ED, we almost never heard their stories or
concerns.
We felt that something needed to be done to bridge the gap
between the ED and inpatient experiences.

So we created an
Inpatient Rounding Pilot Program

It’s Super Simple.
Each week, providers and nurses round on their admitted patients.
Why? • Learn about patients’ transitions of
care experience. • Identify opportunities for closer
integration between the ED and hospitalist teams.
• Provide real-time service recovery. • Gain feedback on initiatives and
outstanding providers.
And most of all …
Exceed the expectations of
patients and families.
At first, it was just two of us.
We didn’t spend a lot of time seeking buy-in or forming a committee.
We just started knocking on doors.

Eventually, others joined in.
It started with a few volunteers. But once they tried it, they were hooked.

From the first day of rounding, it became apparent that this process
provided feedback that was overwhelmingly positive.
From the first day of rounding, it became apparent that this process
provided feedback that was overwhelmingly positive.
That was powerful. No one gets enough positive reinforcement in
emergency medicine.
“One woman ran into my arms when we came to visit her
husband. He had just received a terminal diagnosis and was
going into hospice. Knowing we cared meant a lot to her.”
Edward Pillar, DO
Soon we were rounding as a team. • Patient’s PA/NP • Patient’s Primary ED Nurse • Representative from hospital administration • Hospitalist Provider • Case Manager
Any feedback, positive and negative, was circulated back to individual providers and staff in order to:
• Further hardwire our culture of caring • Reinforce positive behavior • Provide counseling and support for
negative behavior
Negative patient experiences were communicated in concept (no names mentioned) in our daily shift huddles.

While we got tons of positive feedback, we also found that
Service Failures Happen.

While we got tons of positive feedback, we also found that
Service Failures Happen. That’s a guarantee. So you’d better go
find them!
Here are just a few we identified during the 6-month pilot period:
• Poor communication • Lack of introductions • Inappropriate conversations • Cleanliness issues • Unexplained delays • Noise • Inadequate pain control
How to spot more service failures:
• Make an authentic connection • Watch for nonverbal cues • Practice active listening
Rounding gave us a chance to validate patient and family concerns.
Rounding gave us a chance to validate patient and family concerns.
I can see how that would be
frustrating.
Rounding gave us a chance to validate patient and family concerns.
Anyone in your situation would feel that way.
I can see how that would be
frustrating.
If you identify a failure …
• Try not to take it personally. • Diffuse negativity by acknowledging
the concern and taking responsibility.
If you identify a failure …
• Try not to take it personally. • Diffuse negativity by acknowledging
the concern and taking responsibility.
It may not be my fault, but it’s my problem. Thank you for bringing
this issue to my attention.

The Good News
Most service failures were recovered in real-time by the inpatient rounding team.
(We got great backup from our hospital’s
service recovery team.)
So we know you’re probably wondering
Does this get results?
So we know you’re probably wondering
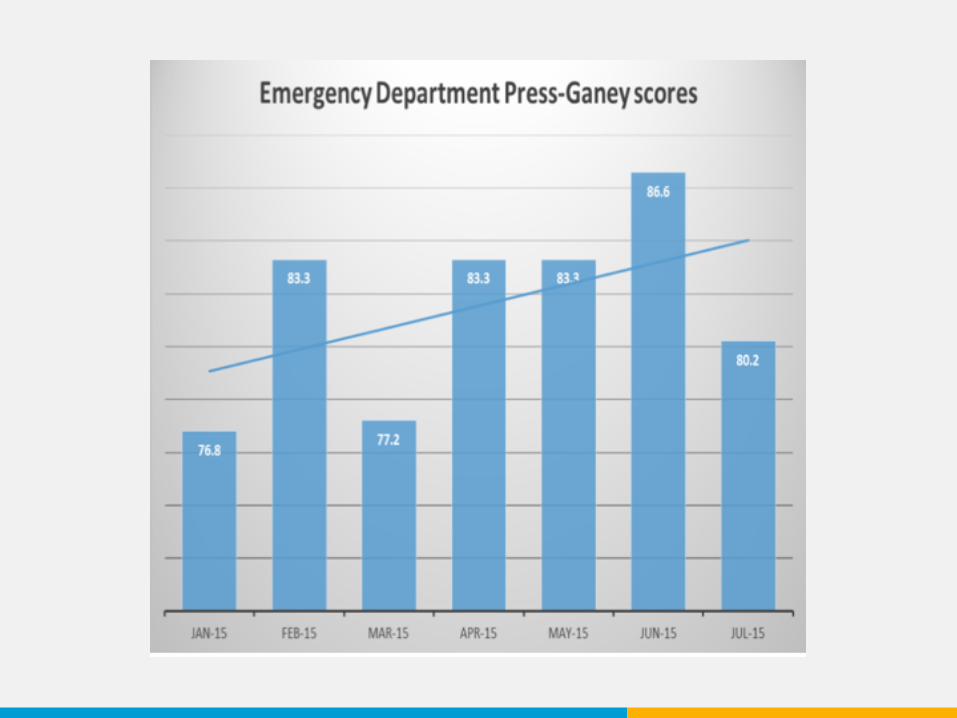
Does this get results? Well, during our pilot ...

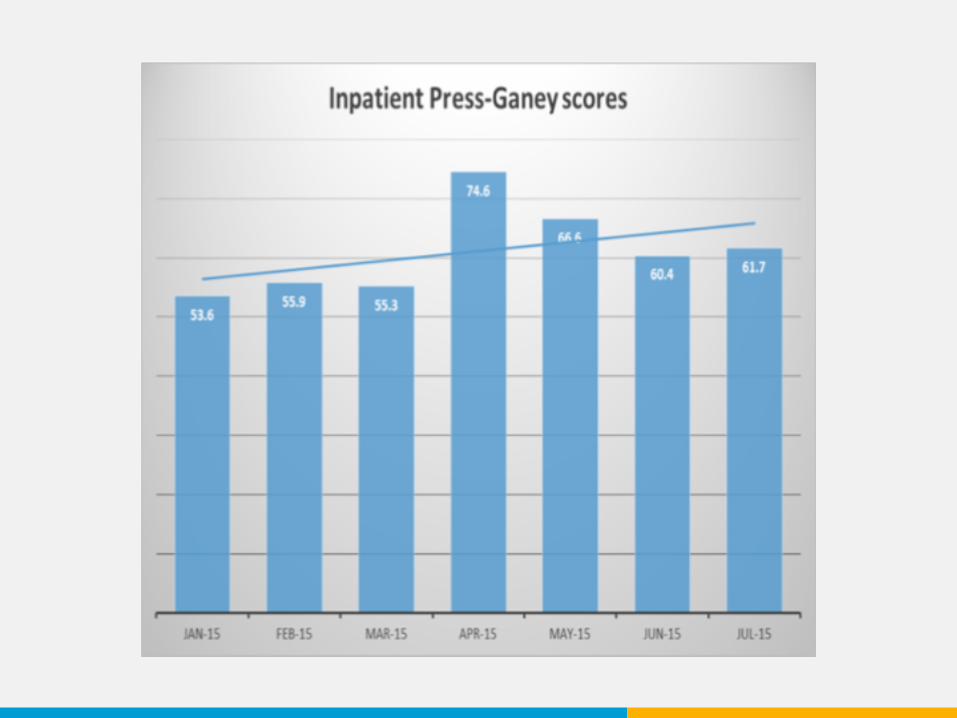
We saw improvement in both our ED and inpatient
satisfaction scores.
Patients weren’t the only ones satisfied.
The entire hospital saw the momentum of positivity and energy
that resulted from the project.
“The ED nurses and physicians were seen as leaders and role
models in the patient experience. We became known as the team to call upon when there was a
difficult situation with a patient.”
Julia Lyall, RN

People were just really fascinated.
Even some of our hospital board members requested to round with us
and share the experience.

We’ve presented posters on inpatient rounding at the
conferences of:
We also wrote about it for FierceHealthcare.
So why exactly does this work?
Here are a few thoughts.
Maximizing the patient experience requires providing authentic connections
at every touch point throughout the patient’s journey.
Inpatient rounding meets this need.
Care Should Be Personal
Maintaining a culture of caring requires constant feedback to staff.
Inpatient rounding helps you provide this
feedback in real time.
Culture Takes Work

Feedback on patient and family perceptions of their experience is a
powerful tool for nurturing an empathetic and engaged staff.
We Really Care About Patients

An effective service recovery program will actually increase patient and
family loyalty.
Service Recovery Is a Gift
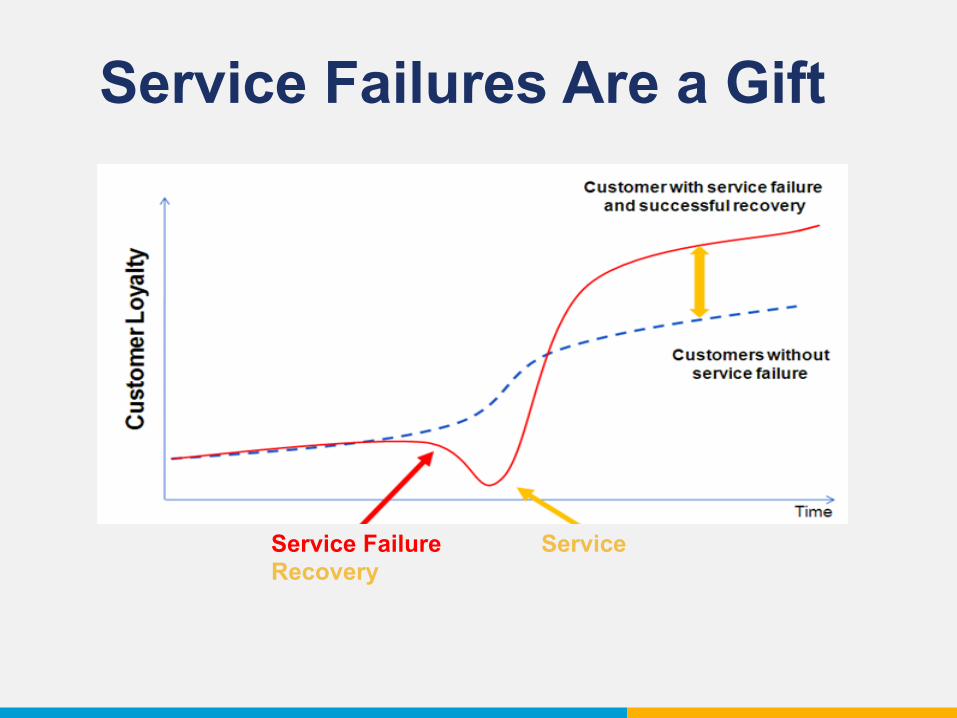
Service Failures Are a Gift
Service Failure Service Recovery
We really hope you do. And it’s easy to get started.
Ready to Give It a Try?
The great thing about inpatient rounding is that it doesn’t take a lot of money or
resources.
Culture change. Leading by example.
Getting out of your comfort zone. Opening yourself to possible criticism.
What It Does Take
It’s not always comfortable.
But at the end of the day, you’re building a better patient experience — the kind of experience you’d want for yourself and
your family members.

Learn more about improving the patient experience at the CEP America blog.
Thank You!