Embed Size (px)
Citation preview
Praveen Krishna V. * Vijay Raj * Chandrasekhar B.
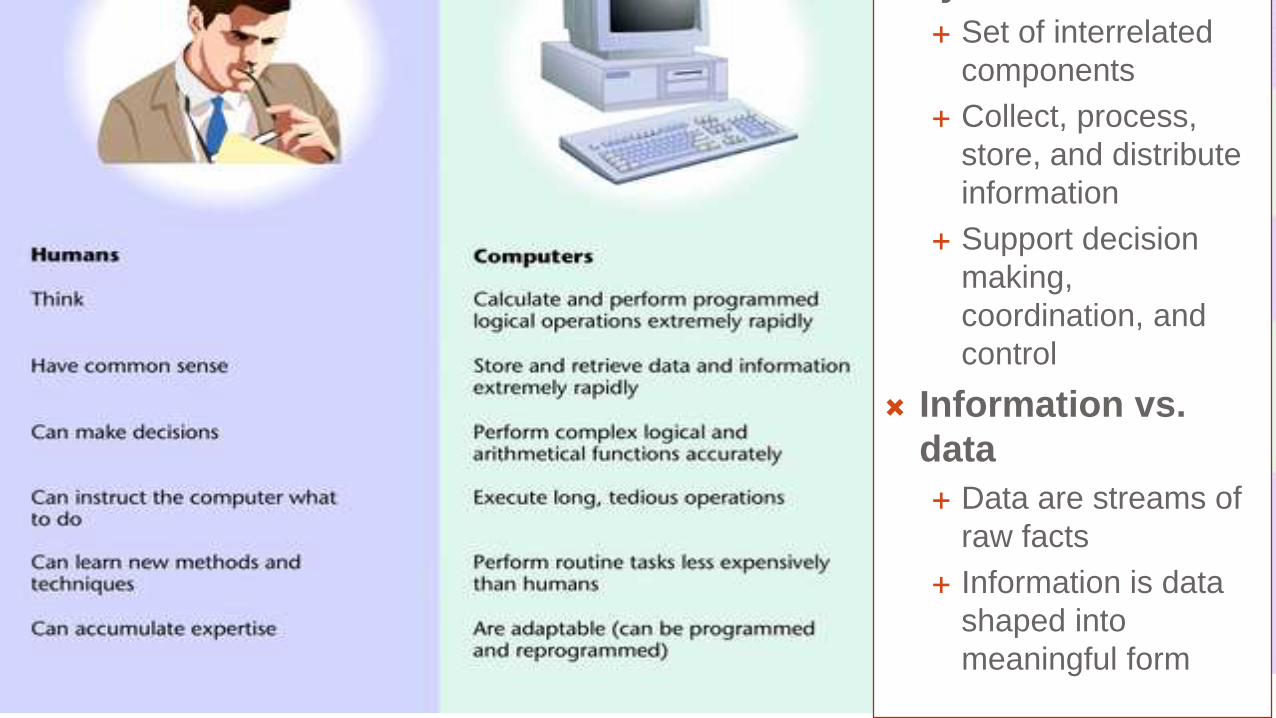
system:
Set of interrelated
components
Collect, process,
store, and distribute
information
Support decision
making,
coordination, and
control
Information vs.
data
Data are streams of
raw facts
Information is data
shaped into
meaningful form
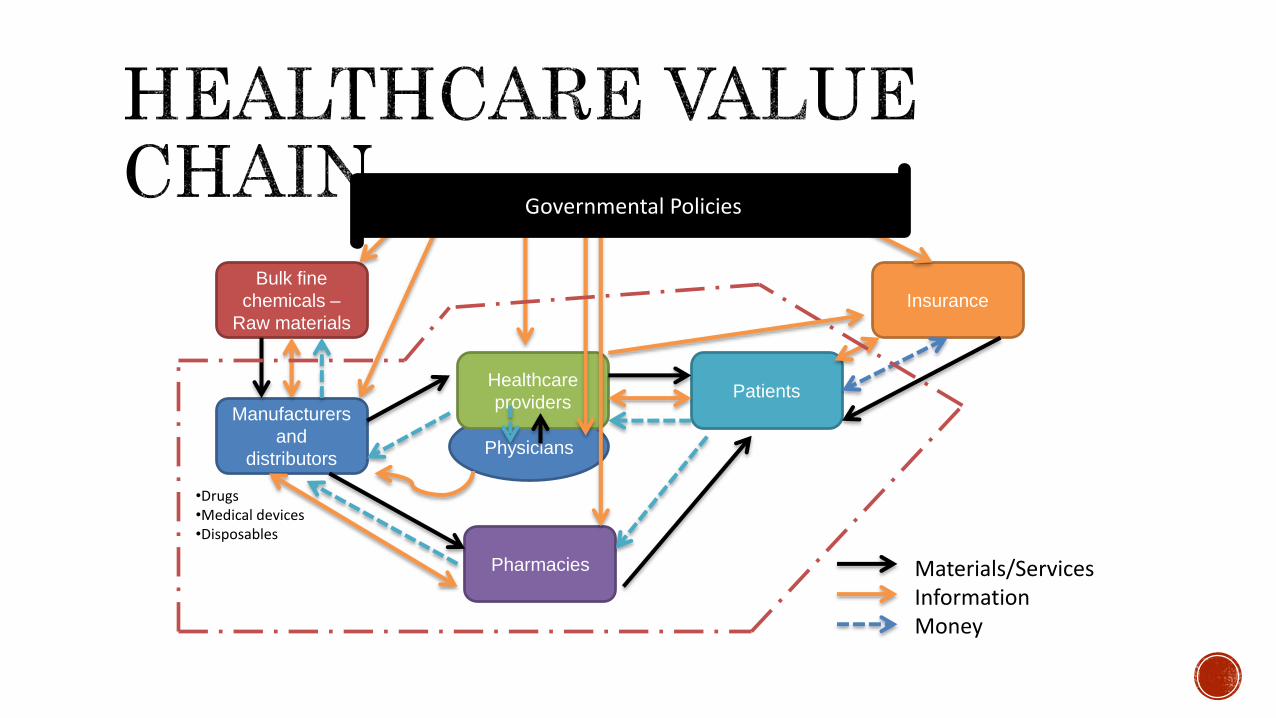
Insurance
Physicians
Manufacturers
and
distributors
Bulk fine
chemicals –
Raw materials
•Drugs•Medical devices•Disposables
Materials/ServicesInformationMoney
Healthcare
providers
Pharmacies
Governmental Policies
Patients
Hospital
s
Primary care
physician
Specialty
physician
Ambulatory
center (e.g.
imaging centers)
Payers
Pharmacy
Laboratory
Public
health
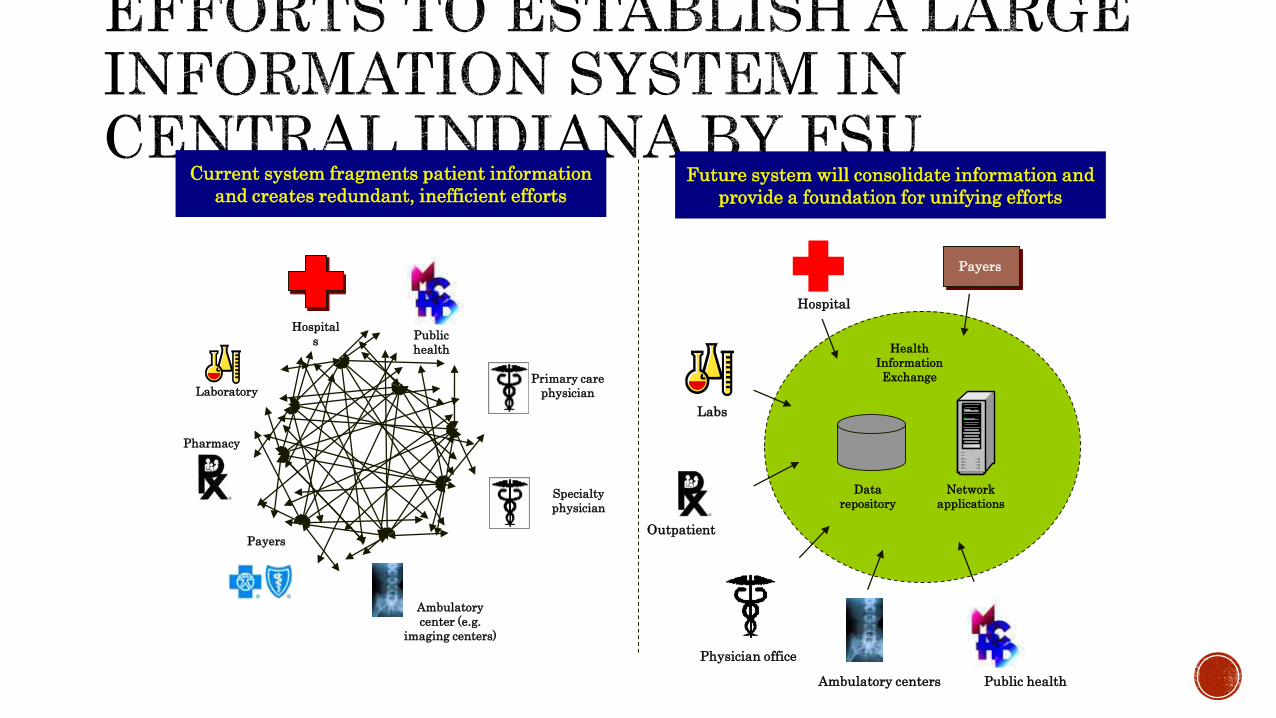
Current system fragments patient information
and creates redundant, inefficient effortsFuture system will consolidate information and
provide a foundation for unifying efforts
Hospital
Data
repository
Health
Information
Exchange
Network
applications
Server
Payers
Labs
Outpatient RX
Physician office
Ambulatory centers Public health
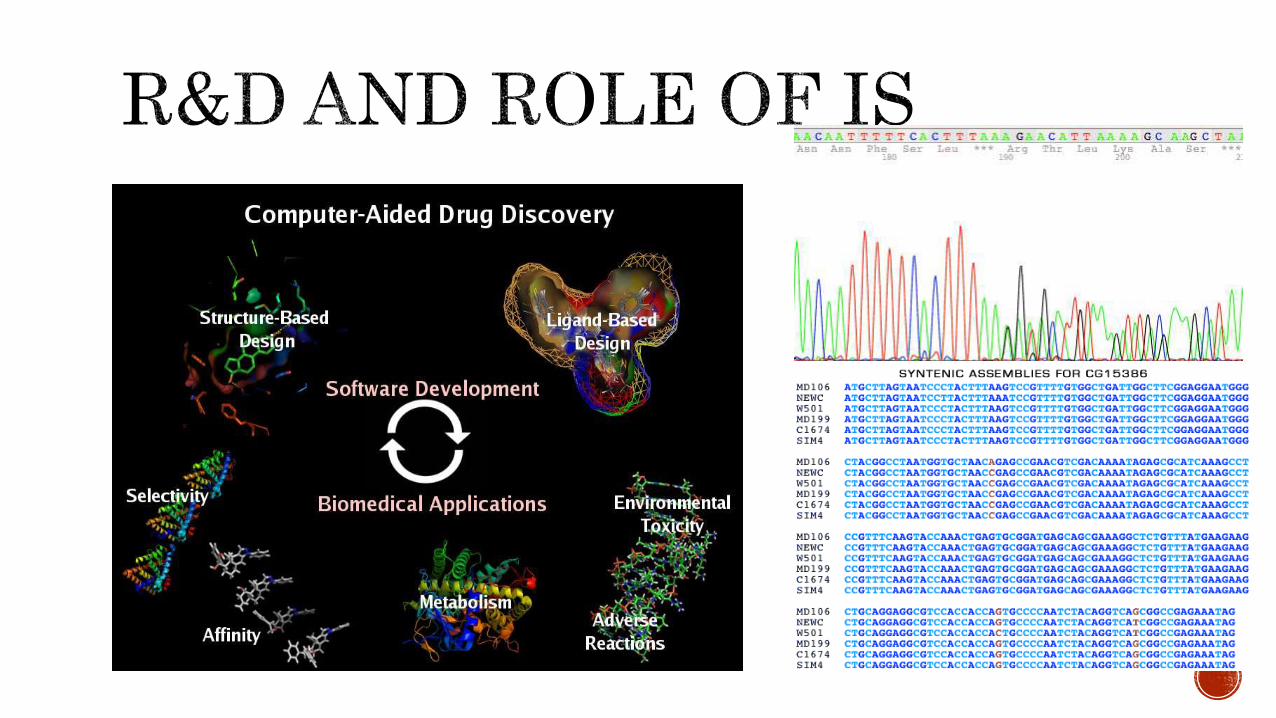
• Operational excellence• New products, services, and business models• Customer and supplier intimacy• Improved decision making• Competitive advantage - Survival
•Information to help the government frame policies
•Assist drug and devices manufacturers in forecasting diseases that in turn define the
demand for their products
•Aid medical practitioners in studying patients and in defining and curing ailments better.
•A better and safer healthcare experience for the patients
Obsolescence
– loss of $19-
27 billions
Warehousing
woes
$10-14 billions
Drugs * Devices and implants * Instruments * Consumables
•Ardently tie the supply chain with business strategy
•Formulate robust custom-made supply chains using segmentation and end-to-end thinking
•Establish responsive supply chain that could capture the market demand
•Effect informed choices on network (internal/external) also with strong supplier management
•Establish new levels of collaboration with partners for streamlined performance
This, it is suggested, would help bridge the technological and performances gaps of thirty years between the pharmaceutical supply chain (worth over half a billion dollars in 2013) and the nimble FMCG (fast moving consumer goods) segments.
Ebel et al, 2012
(Mckinse
y white
paper)
•Enable efficient recall administration (recall of expired or unsafe products) by the suppliers
at various point of administration of drugs/devices;
•Medication authentication to help pharmacies, hospitals and physicians to enable
identification of counterfeit drugs being sold and reimbursement frauds that aim to fool
insurers;
•Inventory management collaboration between the manufacturers, distributors and end
users and administrators of the products. This can allow for seamless flow of data allow and
allow for product warehouse management; and
•Automated transaction and data-sharing has the potential to reduce errors and expenses
twined with paper records and physical data entry and validation.
Health Information Technology usescomputers and computer programs tostore, protect, retrieve, and transferclinical, administrative, and financialinformation electronically.
Health Information Technology (HIT)has the potential to improve the healthof individuals and the performance ofproviders, yielding improved quality,cost savings of patients in their ownhealth care. There are seven types ofHIT
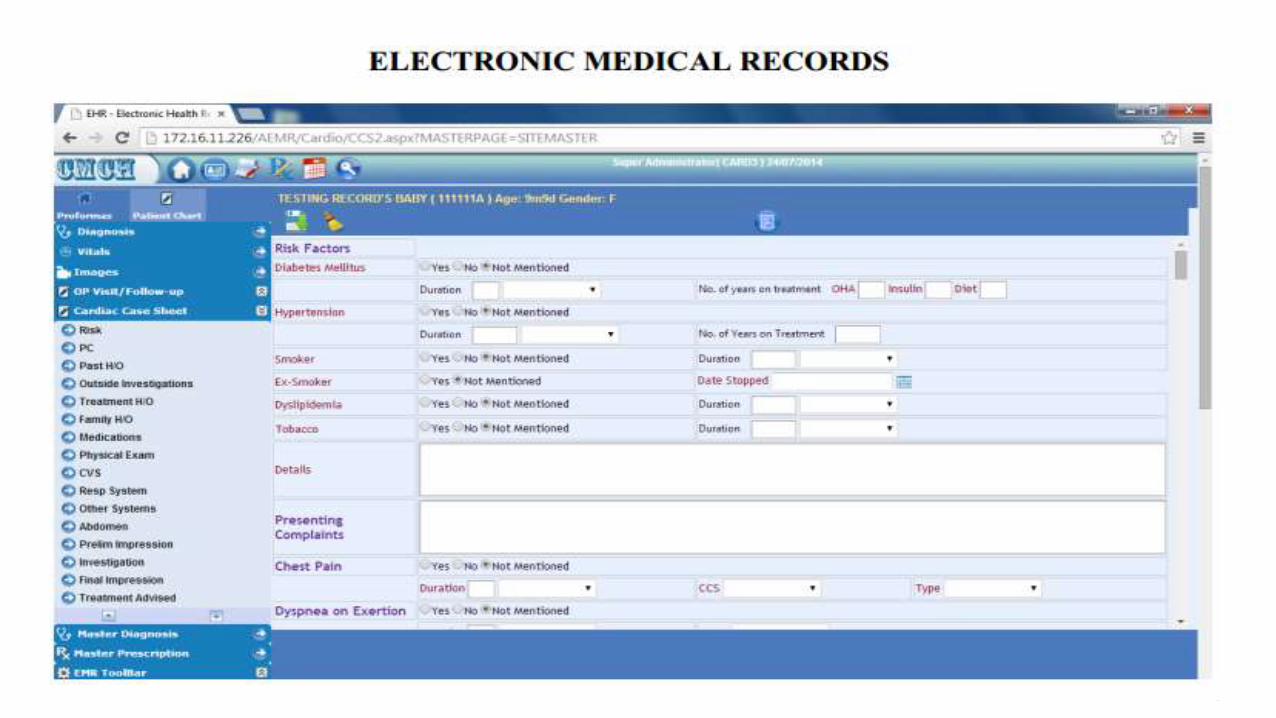
1. Electronic Medical Records (EMR)
2. Electronic Health Records (EHRs)
3. Personal Health Records (PHRs)
4. Payer-based Health Records (PBHRs)
5. Electronic Prescribing (e-Prescribing)
6. Financial/Billing/Administrative Systems
7. Computerized Practitioner Order Entry (CPOE) Systems
The IOM 2003 Patient Safety Report describes an EMR as
1. A longitudinal collection of electronic health information for and about persons
2. Immediate electronic access to person- and population-level information by authorized users;
3 Provision of knowledge and decision-support systems that enhance the quality, safety, and efficiency of patient care
4. Support for efficient processes for health care delivery
Capabilities of EMR
To capture data at the point of care
To integrate data from multiple internal and external sources
To Support care giver in making decisions
Objectives for Implementing EMR
Improve Quality Care
Avoid Adverse Drug Events
Improve Quality Measures
Enhance Resident Safety
Improve Operational Efficiencies and Reallocate Staff
Increase Reimbursements
Electronic Health Record (EHR)
EHR (Electronic Health Record) is term applied to electronic patient care systems
Primary uses
Patient care delivery
Patient care management
Patient care support processes
Financial and other administrative processes
Patient self-management
Secondary uses
Education
Regulation
Research
Public Health and Homeland Security
Policy Support
Health information and data
Patient support
Results management
Administrative processes
Order entry/management
Reporting & population health
Decision support management
Electronic communication and connectivity
Telemedicine
Telemedicine is an umbrella term used for the diagnosis and medicaladvice at a distance.
It uses telecommunication to enable the doctors to interact with theirpatients.
It is more applicable in remote places or in places where hospitals are faraway; for example, Australians use this technology more because healthcenters are far off.
It has benefits of providing timely medical attention in such cases. Thedriving factors for telemedicine are the advent of seamless networkingcapabilities, high bandwidth availability and decreased costs of medical andnon-medical devices and technologies
Christian Medical College, Vellore (CMC) is an unaided, Christian minority health care institution which is committed to delivering world class health care to all sections of society, aided by the use of caring, cost effective technology.
From its humble beginnings as a one-bedded clinic over a hundred years ago, CMC has blossomed into a large institution catering to over 6000 outpatients and 2600 inpatients daily, and home to 10,500 staff and students.
An institution of this magnitude brings with it a raft of administrative and organizational complexities, which need to be continuously addressed in order to facilitate CMC’s goal of excellence in education, service and research.
In order to integrate the functions of various sections of the
hospital – Laboratories,
Medical Records Department (MRD),
Pharmacy, Dietary, in-patient (IP)
and out-patient (OP) areas,
CMC required a fully integrated Hospital Information System (HIS) for the Main Hospital and peripheral centres.
Since it would have been prohibitively expensive to outsource the development of a user friendly program that would be sophisticated enough to meet the needs of an ever expanding institution, CMC’s Department of Centralised Hospital Information Processing Systems (CHIPS) took up the challenge of developing, in-house, a program with the desired specifications.
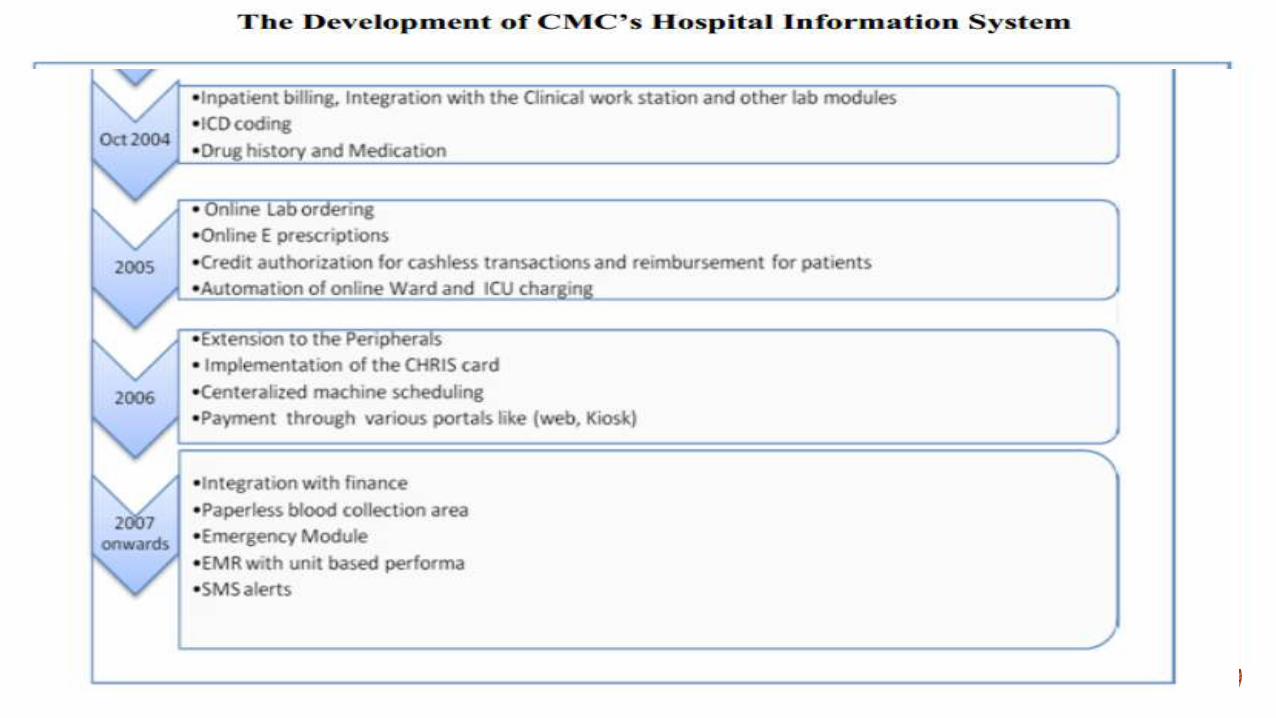
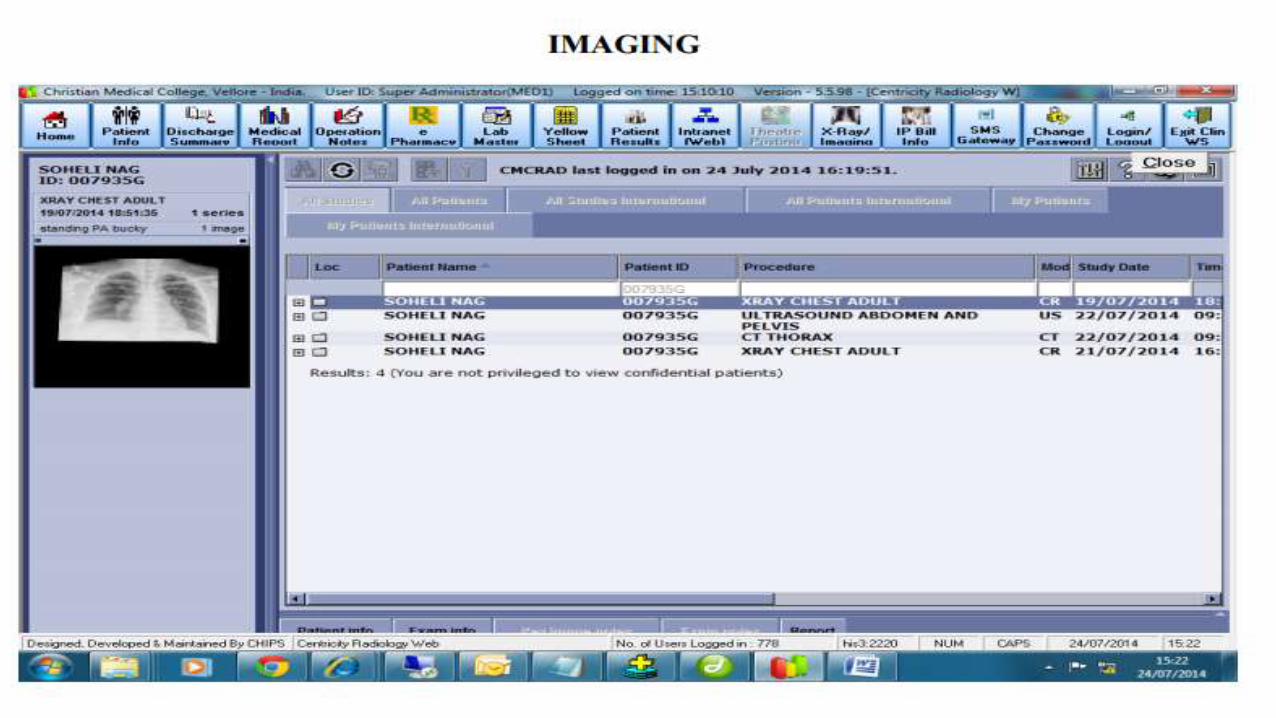
This HIS covers the
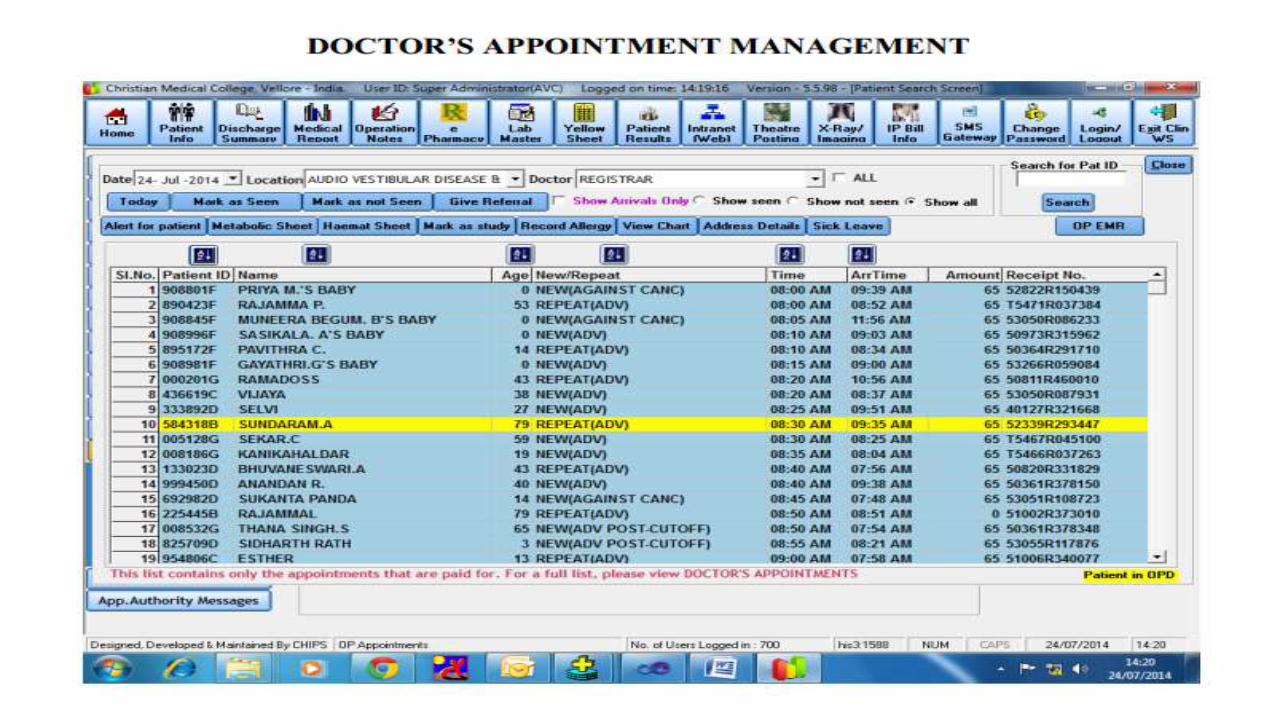
patient registration and appointment system,
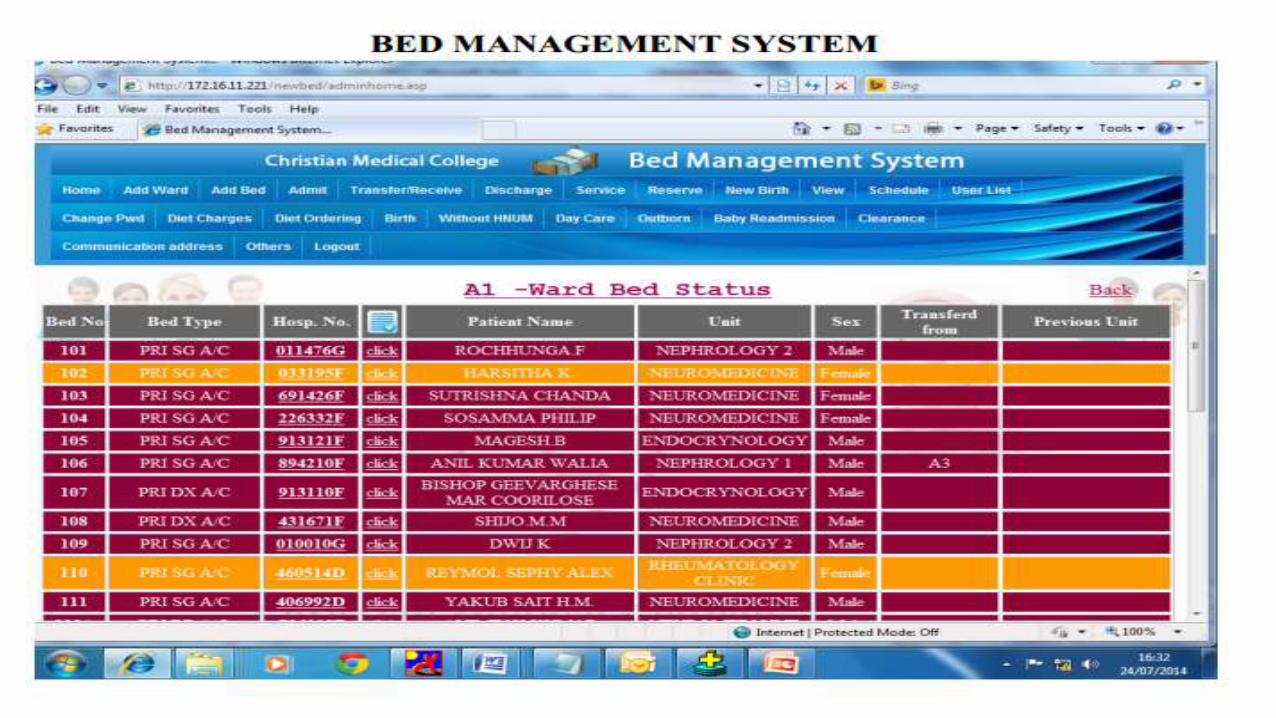
admission-discharge-transfer (ADT) process,
Outpatient and Inpatient billing,
Company & Insurance billing
and Reimbursement procedures,
and is integrated with MRD, Laboratories,
Pharmacy Department,
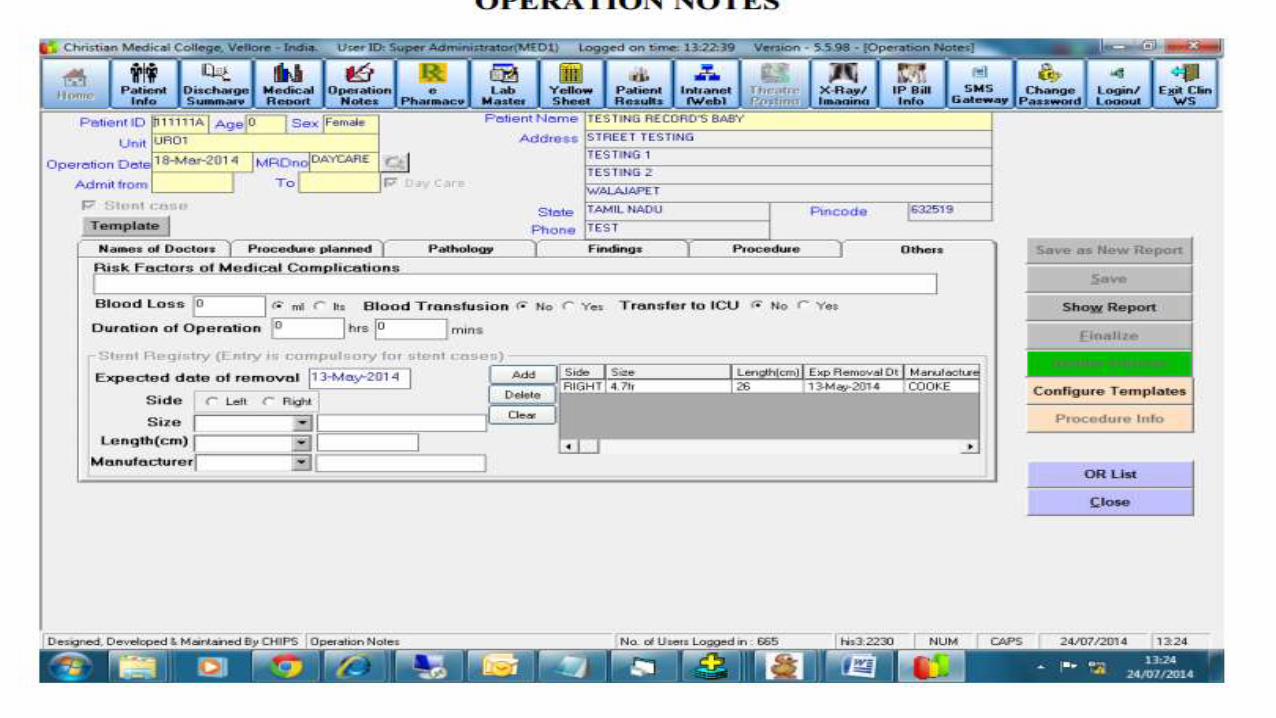
Operation Theatre,
Anaesthesia Department,
Dietary and Laundry.
it includes the Clinical Workstation that is an interface by which doctors can view and manipulate patient data.
The HIS has resulted in a tremendous increase in efficiency at all levels of the health care delivery process within CMC –
allowing prompt service,
reducing costs,
minimizing the margin for human error
and providing a tool for Continuous Quality Improvement (CQI) strategies by CMC.
CMC started with stand-alone microcomputers to perform Billing and Accounts procedures.
However, as the services of the hospital expanded and the number of patients soared, so also did the need for storage and sharing of data.
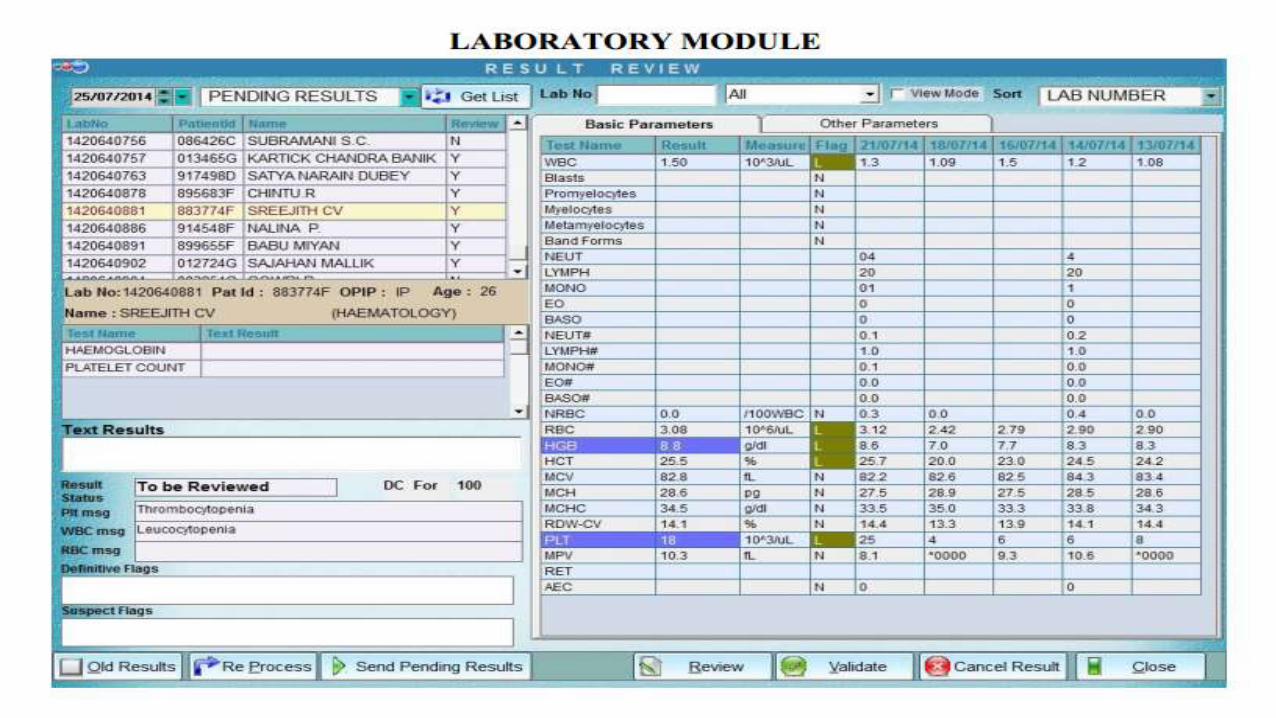
Results entered in the labs would previously take at least a day to reach the doctors desk based on which treatment would be modified.
The lack of integration caused significant delays in patient billing, increased waiting time, and incurred additional costs in terms of finance and resources.
Retrieving patient and financial information was difficult, thereby limiting decision-making processes.
Manual processes were subject to entry errors. Information was available at limited areas and sometimes could not be provided in real-time.
Gathering information for statistics and research was a complex operation. Generating financial statements was a phenomenal task.
1. To develop a fully integrated HIS for various areas of the hospital – Emergency Services, Pharmacy, Labs, MRD (Patient registrations, doctor schedules and OP/IP charts), IP areas (wards & intensive care units, billing, reimbursement and credit authorizations), OP areas (OPDs) and Dietary services.
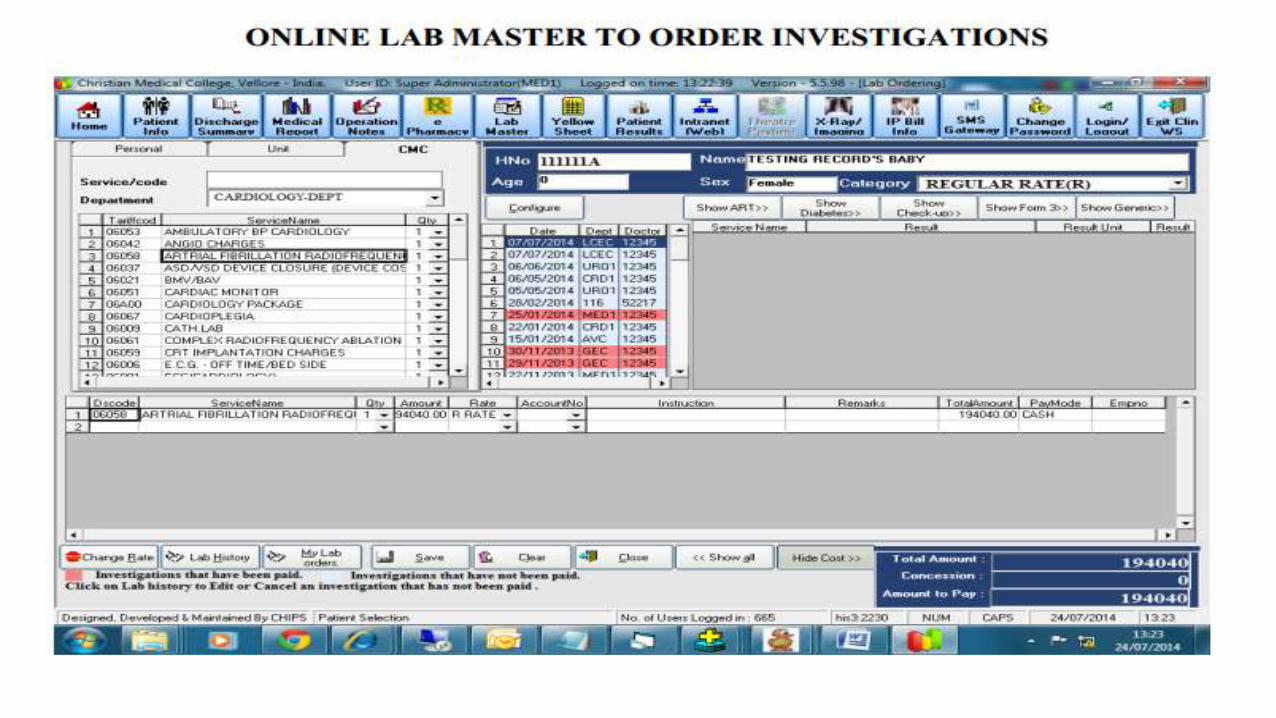
2. To develop an integrated, user friendly Clinical workstation for doctors to view appointments, results, clinical images, theatre postings and inpatient lists; schedule doctor appointments & procedures; order investigations and prescriptions; and generate medical reports and discharge summaries – all at a single click.
3. To allow acquisition and availability of relevant real-time information and allow billing to be automated with data entry.
4. To ensure transaction security and minimize human errors.
5. To incorporate a Self-Service Module allowing ease of access to an individual’s information.
Software: Oracle and VB, VB.net, ASP, ASP.net.
Hardware: RAC (Real Application Cluster) 3 Node environment with a two node RAC for business continuity (Disaster Recovery) and a separate data mining server.
Other technologies/solutions employed:
CMC debit card (CHRIS card), which can be used for payments at cash counters and kiosks within hospital, for online payment and payment through the CMC Call Centre
Machine interfaces in labs
Security implemented via passwords and/or contactless security card
Customized SMS Gateway for alerts to employees and patients
Web paging, multi-line telephonic paging and CART (Cardiac Arrest Resuscitation Team) paging for priority paging
Complete CISCO switched network with Virtual Private Networks and security walls was put in place, which extended Clinical services to the entire CMC residential campus through broadband or LREs
Audit vault
The development of the HIS brought about a sea change in the organizational capabilities of the institution, besides boosting efficiency at every level.
Speed of service has increased significantly
Patient billing delays have decreased dramatically
Secure, real-time, relevant information is now available anywhere on the institutional campuses
MIS for Administration and Auditors
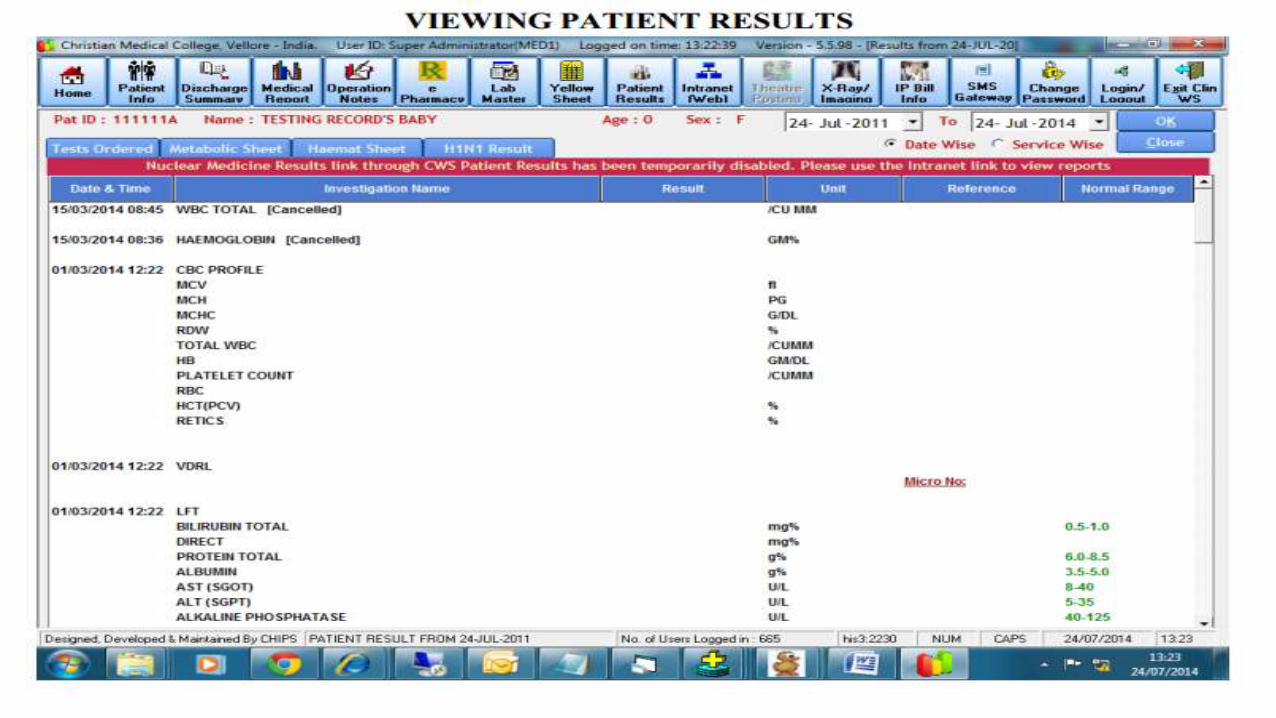
Online investigation results available as soon as they are ready, thus aiding clinical decision making. Trend of lab investigations over a time period can be studied using graphical displays.
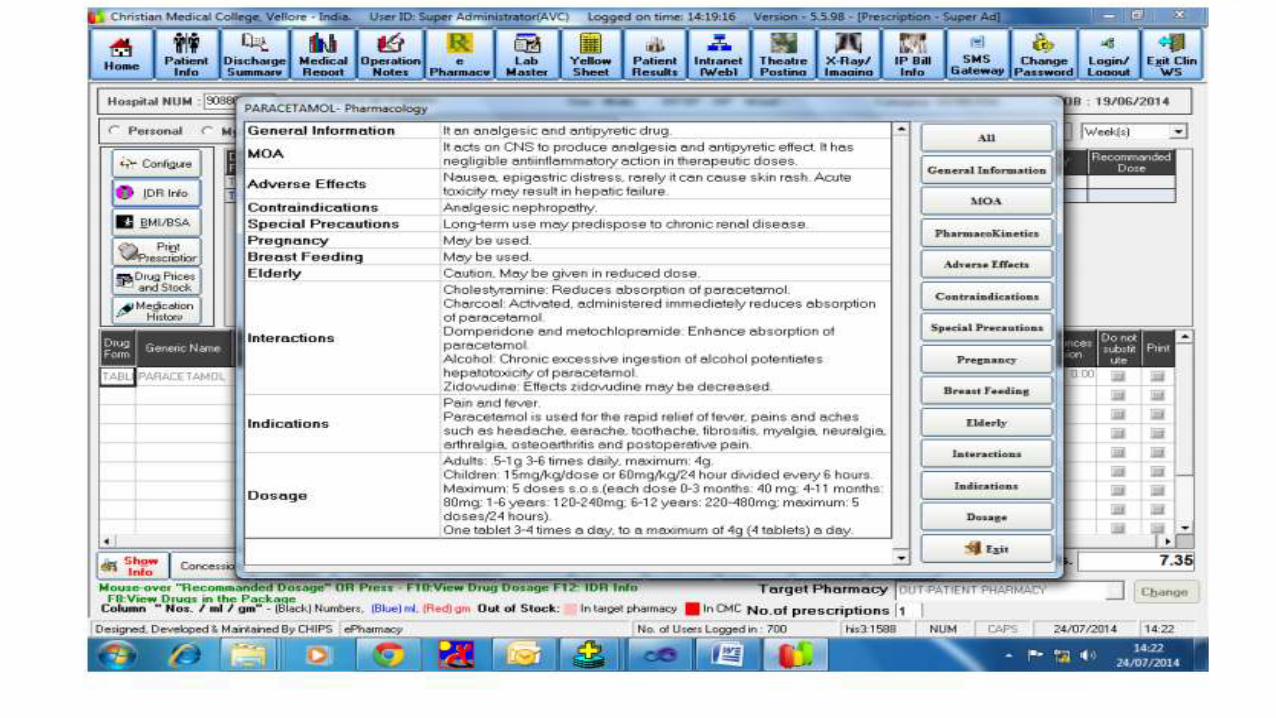
Information regarding drug interactions is available in real-time, as a prescription is being written
Patient billing delays have decreased dramatically
Patient reports are generated quickly without needing re-entry of data.
Research information is easily retrievable; alerts can be generated for study participants and patients enrolled in clinical trials
Change in workflow can be easily managed since an in-house team has developed the solution
In conclusion, at long last Clinical Information Systems have come of age and this technology is fast bringing about a revolution in healthcare, just like information technology brought about a revolution in other fields like finance, banking and travel.
Those healthcare organizations that wish to be of international caliber will have to embrace this technology and implement it, as this technology will be a benchmark criterion in qualifying as a healthcare organization of international standard