Embed Size (px)
Citation preview

Less Pain, More Gain: Palliative Care Strategies for
Recurrent Ovarian Cancer
Carolyn Lefkowits, M.D. M.P.H. M.S.Assistant Professor, Gynecologic Oncology & Palliative Care
University of Colorado Denver
SHARE Webinar Sept 27, 2017
Objectives• Define palliative care & differentiate it from
hospice
• List at least 3 evidence-based benefits of palliative care
• Differentiate between primary & specialty palliative care
• Leave with homework
Outline: Palliative Care
• What is it?
• Why do we need it?
• How can you get it?
• Barriers
• Next steps
What is Palliative Care?
Palliative Care (PC): “therapies that address the
multiple issues that cause suffering for patients and
their families and impact their quality of life”
NOT synonymous with end-of-life care/hospice
Can be offered concurrently with curative therapy
Smith et al JCO 2012
What is Palliative Care?
“Palliative care is specialized medical care for
people living with serious illness. It focuses on
providing relief from the symptoms and stress of a
serious illness. The goal is to improve quality of life
for both the patient and the family…It is appropriate
at any stage in a serious illness and can be provided
along with curative treatment.”
“an extra layer of support”
Center to Advance Palliative Care
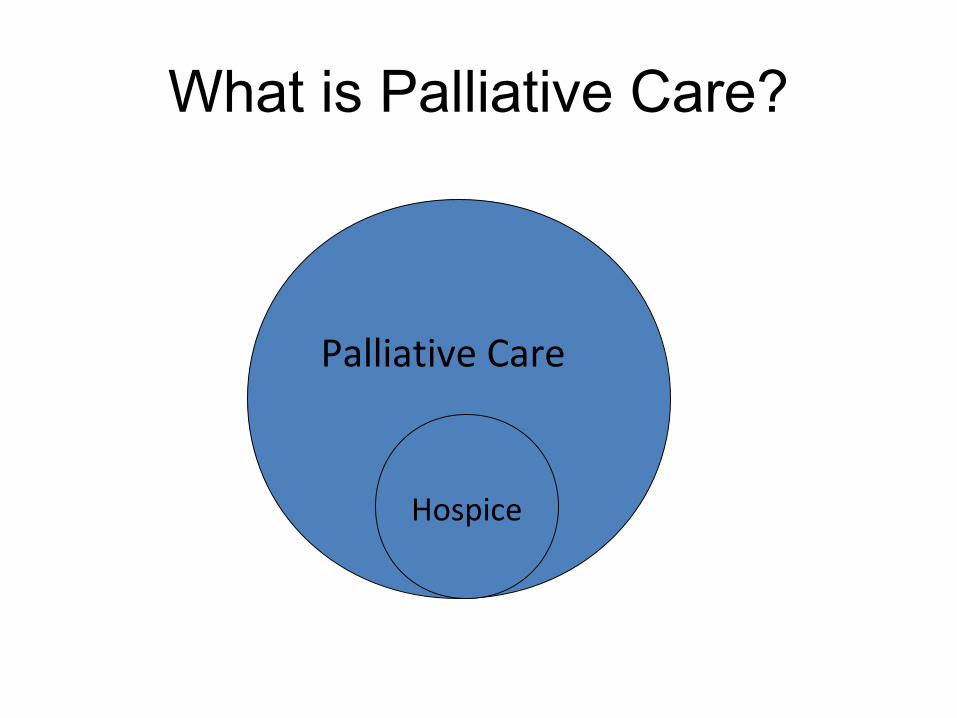
What is Palliative Care?
Palliative Care
Hospice
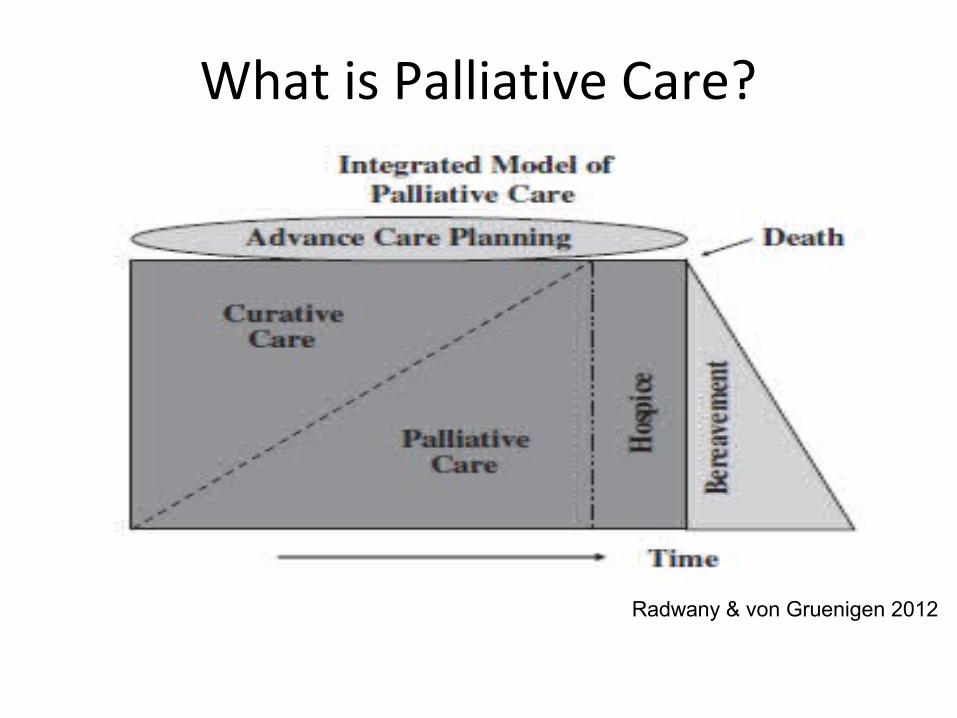
What is Palliative Care?
Radwany & von Gruenigen 2012
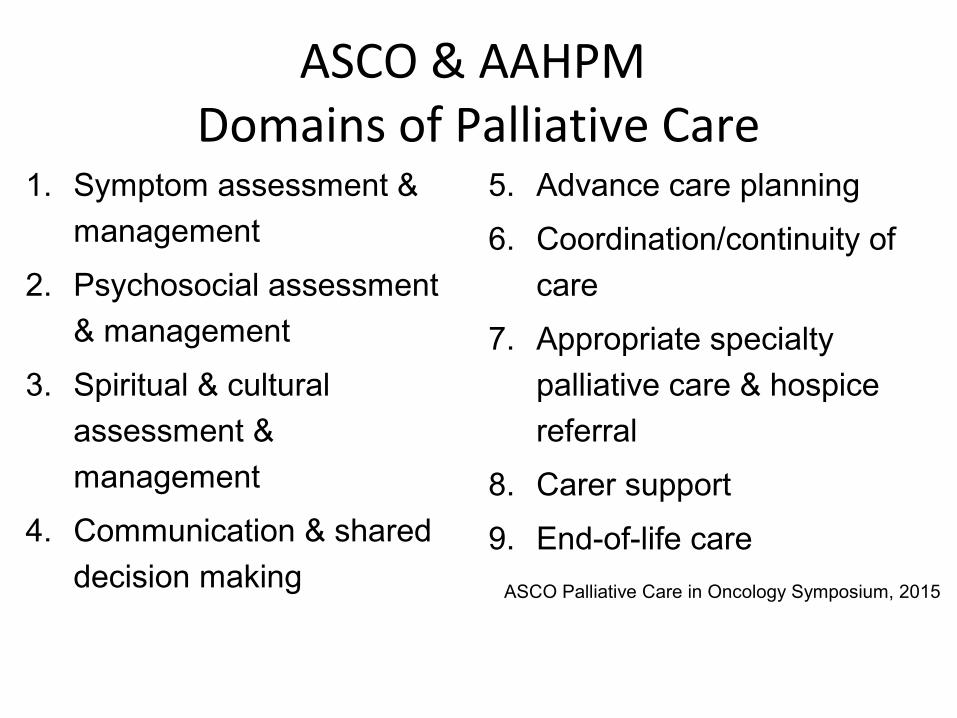
ASCO & AAHPM Domains of Palliative Care
1. Symptom assessment &
management
2. Psychosocial assessment
& management
3. Spiritual & cultural
assessment &
management
4. Communication & shared
decision making
5. Advance care planning
6. Coordination/continuity of
care
7. Appropriate specialty
palliative care & hospice
referral
8. Carer support
9. End-of-life care
ASCO Palliative Care in Oncology Symposium, 2015
Outline: Palliative Care
• What is it?
• Why do we need it?
• Barriers
• How can you get it?
• Next steps

Why do we need palliative care?
You are a Bridge: Palliative Care
1 min 40 sec youtube video
(https://youtu.be/lDHhg76tMHc)
Benefits of palliative care
Nonrandomized studies have shown the following benefits without decreased survival
• Reduced pain & other distress
• Improved health-related QOL
• High patient & family satisfaction with care
• Increased likelihood of location of death being outside of hospital
• Reduction in hospital & ICU length of stay Meier et al 2006
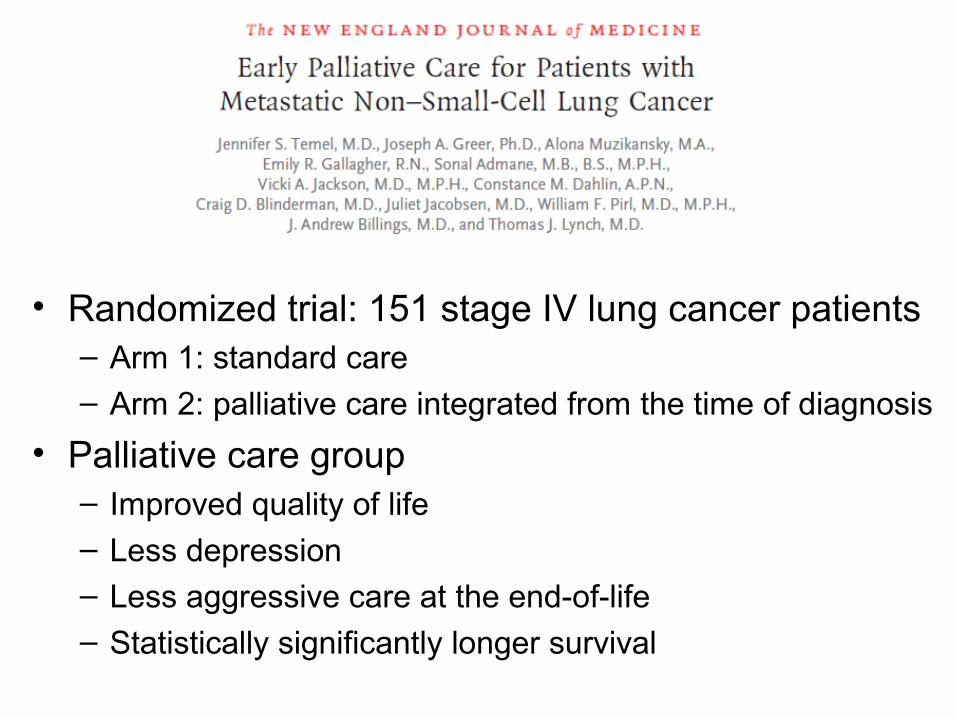
• Randomized trial: 151 stage IV lung cancer patients– Arm 1: standard care
– Arm 2: palliative care integrated from the time of diagnosis
• Palliative care group– Improved quality of life– Less depression– Less aggressive care at the end-of-life
– Statistically significantly longer survival
“It is the panel’s expert consensus that
combined standard oncology care and palliative
care should be considered early in the course
of illness for any patient with metastatic
cancer and/or high symptom burden”

• n=87 patients discontinuing anti-cancer therapy
• Integrated Care Model (ICM) patients had seen PC prior to decision to d/c anti-cancer therapy
• ICM patients
– Better QOL
– Less depression
– Less chemo within last 6 wks of life (40% vs 6%, p=0.001)
– Improved median survival (HR 0.48, p=0.46)
• n=95 patients with gyn malignancy & inpatient PC consultation for
symptom management
• Improvement in prevalence moderate to severe symptom
intensity
– between PC consult & discharge for: pain, anorexia, fatigue & nausea
(magnitude 58-66%)
– within one day of PC consult for: pain, fatigue, nausea (magnitude 50-55%)
• Majority of improvement that occurred between consult &
discharge happened within 24hrs of consult
• Model of routine care vs routine care + PC referral at time of diagnosis of recurrent platinum-resistant disease
• Data from Temel et al informed creation of model
• Early palliative care associated with – Cost savings $1285 per patient over routine care
– ICER <$50,000/QALY
– Assuming no clinical benefit other than QOL improvement, remained highly cost-effective
Palliative Care & The Society of Gynecologic Oncology (SGO)
Palliative Care & Ovarian Cancer: Christine’s Story
https://soundcloud.com/get-palliative-care/a-quality-life-episode-1-christines-story
Outline: Palliative Care
• What is it?
• Why do we need it?
• How can you get it?
• Barriers
• Next steps
Where can you get palliative care?
• Primary palliative care: delivered by non-palliative care specialists
• Specialty palliative care: delivered by palliative care specialists– In the hospital– In an outpatient clinic– At home
• Home palliative care• Hospice care
What actually happens at a palliative care appointment?
• n=67 patients with advanced lung cancer
• 1st palliative care visit median 55 minutes
(range 20-120 min)
• Mean minutes spent (range)
– Symptom management 20 mins (0-75)
– Patient & family coping 15 mins (0-78)
– Illness understanding & education 10 mins (0-35)
Jacobsen et al JPM 2011
Center to Advance Palliative Care(getpalliativecare.org)
• Quiz – “is palliative care right for you?”
• Searchable provider directory
Outline: Palliative Care
• What is it?
• Why do we need it?
• How can you get it?
• Barriers
• Next steps
Barriers to Palliative Care Integration
• Limited availability
• Poor reimbursement
• Lack of provider education
• Palliative care has a branding problem
Barriers: Lack of Provider Education
• Survey 327 practicing gyn oncologists– Only 45% said training helped them relate to
terminally ill patients & families
• Survey 103 gyn oncology fellows– Quality & quantity of palliative care training
rated lower than other common oncologic topics
• Survey 29 gyn onc fellowship directors– 14% written pall care curriculum– 48% elective/required pall care rotation
Ramondetta et al 2004Lesnock et al 2013Lefkowits et al 2015

Palliative Care Has a Branding Problem
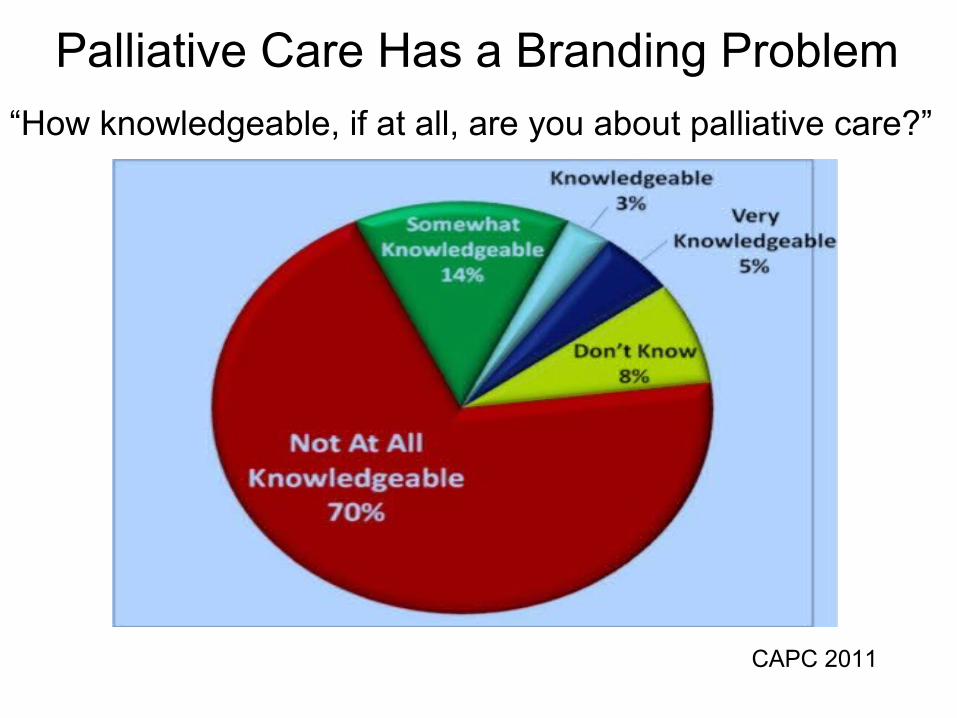
Palliative Care Has a Branding Problem
“How knowledgeable, if at all, are you about palliative care?”
CAPC 2011
Branding Problem: Providers
• Lack knowledge of specialty palliative care services & their benefits
• Equate palliative care with end-of-life care
• Patients unlikely to request palliative care referral, but open to it when recommended by oncologist
CAPC 2011Schenker et al JOP 2014Schenker et al JPM 2014
Palliative Care Has a Branding Problem
“One of the greatest remaining challenges is the
need for better understanding of the role of
palliative care among both the public and
professionals across the continuum of care so that
hospice and palliative care can achieve their full
potential for patients and their families”
Institute of Medicine (IOM)
Dying in America 2014
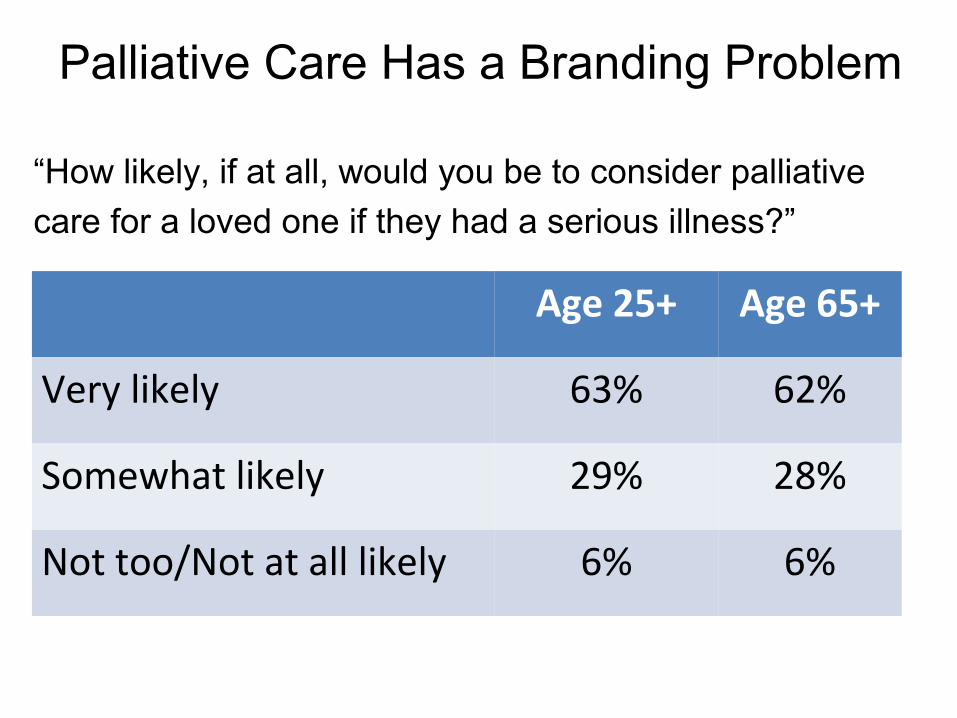
Palliative Care Has a Branding Problem
Age 25+ Age 65+
Very likely 63% 62%
Somewhat likely 29% 28%
Not too/Not at all likely 6% 6%
“How likely, if at all, would you be to consider palliative
care for a loved one if they had a serious illness?”
Outline: Palliative Care
• What is it?
• Why do we need it?
• How can you get it?
• Barriers
• Next steps
Next Steps to Improve Palliative Care Integration for Women with Ovarian
Cancer
• Education
• Research
• Policy
Objectives• Define palliative care & differentiate it from
hospice
• List at least 3 evidence-based benefits of palliative care
• Differentiate between primary & specialty palliative care
• Leave with homework – familiarize yourself with palliative care resources near you (getpalliativecare.org)
Take Home Points
• What is palliative care – “an extra layer of support”
• Why palliative care– Because it improves clinical outcomes without
adversely affecting survival
• How palliative care– Getpalliativecare.org
• When palliative care– Why not now?
Thank you!