Embed Size (px)
Citation preview
Making the most of your
PROM data
Jo Partington, Rafael Goriwoda (NHS England)
and Tom Partridge (Northumbria Healthcare NHS Trust)
Pop Up University 5
10am; 2nd September 2015
Appleby and Devlin 2010
“The first health system
internationally to measure what
it produces in terms of health.”
Content
I – Background to the national PROMs programme
What are PROMs? How does the national PROMs programme relate to wider NHS policy.
II – Variation in outcomes (nationally)
How PROMs data can be used to identify good performance or areas for concern.
III – So what?
How provider trusts can investigate their PROMs data to improve outcomes. Northumbria case study.
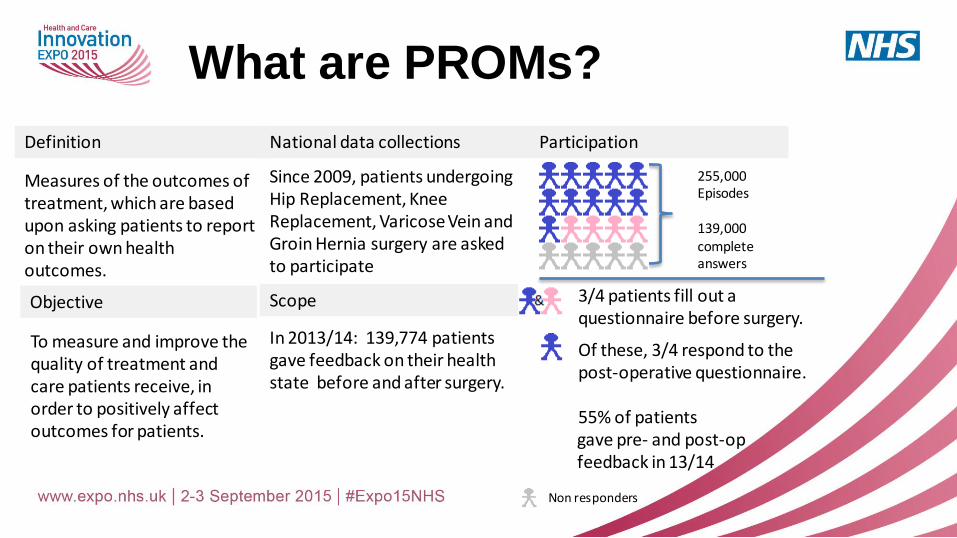
What are PROMs?
National data collections
Since 2009, patients undergoing Hip Replacement, Knee Replacement, Varicose Vein and Groin Hernia surgery are asked to participate
Objective
To measure and improve the quality of treatment and care patients receive, in order to positively affect outcomes for patients.
Definition
Measures of the outcomes of treatment, which are based upon asking patients to report on their own health outcomes. Scope
In 2013/14: 139,774 patients gave feedback on their health state before and after surgery.
255,000 Episodes 139,000 complete answers
Participation
• 3/4 patients fill out a questionnaire before surgery.
• Of these, 3/4 respond to the post-operative questionnaire.
55% of patients gave pre- and post-op feedback in 13/14 Non responders
Wider policy context
• NHS Outcomes Framework: 3.1
• NHS Mandate
• NHS Standard contract
• Five Year Forward View
• Personalised Health and Care 2020 : Using Data and Technology to Transform Outcomes for Patients and Citizens – National Information Board strategy
• Best practice tariff
New developments in PROMs
• Cancers (breast, prostate, bowel, bladder, non-Hodgkin’s lymphoma, womb, ovary and cervix): the pilot PROM report on living with and beyond bladder cancer will be published shortly. Prostate Cancer UK are the first charity to solely fund a UK-wide PROM project.
• Cardiovascular revascularisation: pilot data collected, linkage with NICOR on-going and then the analysis and final report due.
• Renal replacement: Being developed at the UKRR; will look at the link between Patient Activation Measures, Patient Experience and PROMs.
• Major Trauma – Pilot sites already collecting data – some investment from the Medical Directorate
• Dementia: DEMQoL development through National Institute for Health Research (NIHR)
• Long-term conditions: As for dementia, development through NIHR.
PROMs pilots beyond the national programme
• Publication on MyNHS and NHS Choices
• Upcoming “Insight Strategy Short Guide
to PROMs”
• Work with ISIS Outcomes at the
University of Oxford to support the
development of electronic PROMs
Making better use of what we have
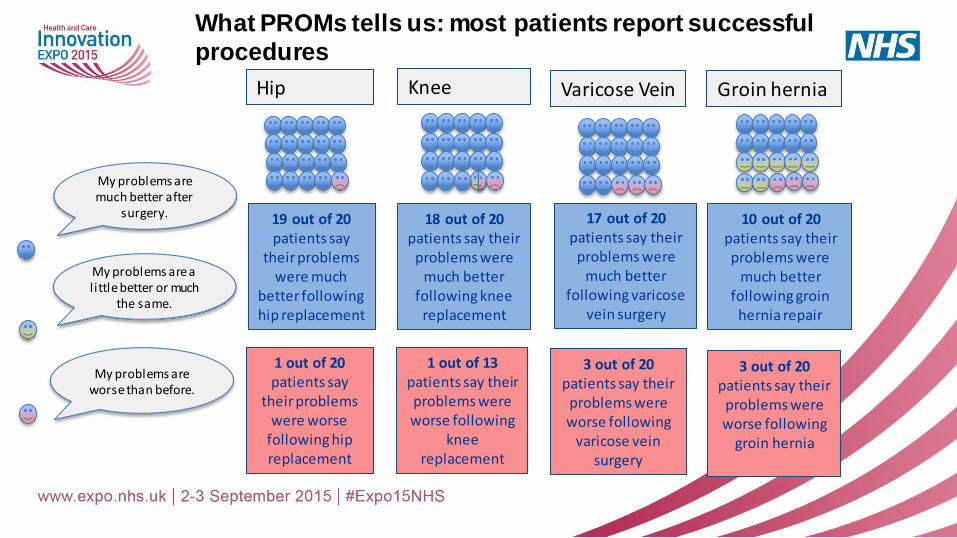
My problems are much better after
surgery.
My problems are a l ittle better or much
the same.
My problems are worse than before.
19 out of 20 patients say
their problems were much
better following hip replacement
18 out of 20 patients say their
problems were much better
following knee replacement
1 out of 20 patients say
their problems were worse
following hip replacement
1 out of 13 patients say their problems were worse following
knee replacement
17 out of 20 patients say their
problems were much better
following varicose vein surgery
10 out of 20 patients say their problems were
much better following groin
hernia repair
3 out of 20 patients say their
problems were worse following
varicose vein surgery
3 out of 20 patients say their
problems were worse following
groin hernia
Hip Knee Varicose Vein Groin hernia
What PROMs tells us: most patients report successful
procedures
-15
-10
-5
0
5
10
15
20
25
0 100 200 300 400 500 600 700 800 900
Ad
jus
ted
He
alt
h G
ain
Number of Modelled Records (Trust Size )
95% control limits
99.8% control limits
England
All
Trust A Trust B
Trust C
Trust D
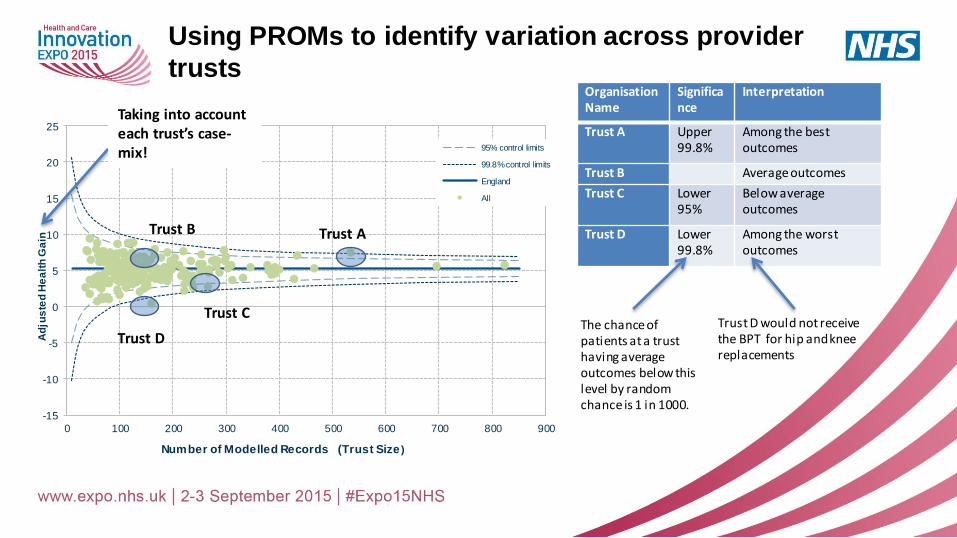
Using PROMs to identify variation across provider
trusts Organisation Name
Significance
Interpretation
Trust A Upper 99.8%
Among the best outcomes
Trust B Average outcomes
Trust C Lower 95%
Below average outcomes
Trust D Lower 99.8%
Among the worst outcomes
Trust D would not receive the BPT for hip and knee replacements
The chance of patients at a trust having average outcomes below this level by random chance is 1 in 1000.
Taking into account each trust’s case-mix!
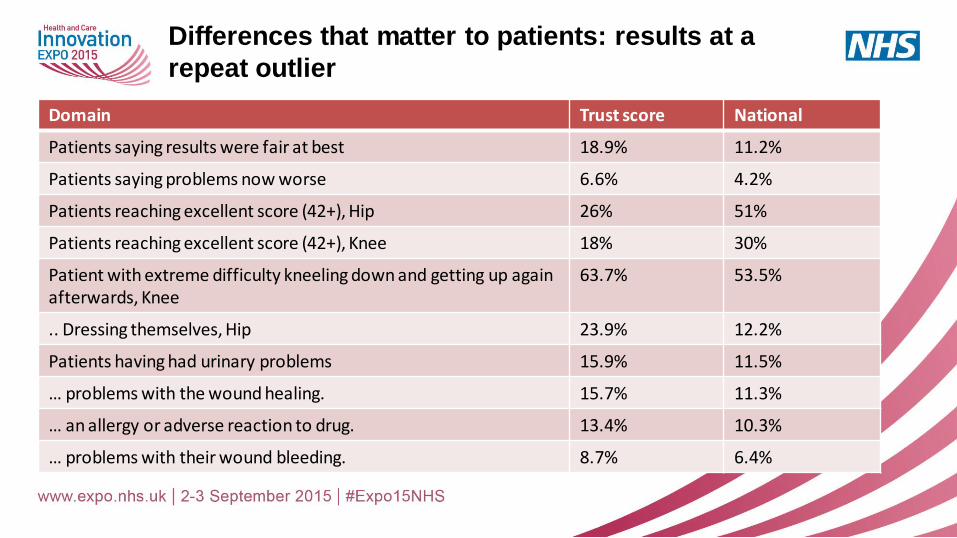
Differences that matter to patients: results at a
repeat outlier
Domain Trust score National
Patients saying results were fair at best 18.9% 11.2%
Patients saying problems now worse 6.6% 4.2%
Patients reaching excellent score (42+), Hip 26% 51%
Patients reaching excellent score (42+), Knee 18% 30%
Patient with extreme difficulty kneeling down and getting up again afterwards, Knee
63.7% 53.5%
.. Dressing themselves, Hip 23.9% 12.2%
Patients having had urinary problems 15.9% 11.5%
… problems with the wound healing. 15.7% 11.3%
… an allergy or adverse reaction to drug. 13.4% 10.3%
… problems with their wound bleeding. 8.7% 6.4%
So What? Putting PROMs into practice
• PROMs is used in a variety of ways: • Audit & Effectiveness Committees – local
• Quality Boards - local
• Best Practice Tariff
• Care Quality Commission “Intelligent Monitoring”
• “Beyond Compliance”
• “Getting It Right First Time”
• Examples from HSCIC benefit realisation study: • Enhanced recovery pathways implemented; PROMs used to evaluate success of
components
• Revised pain management regimes => earlier mobilisation; improved rehab ++ = better outcomes
• Analysis of themes where people struggled post-operatively, and exercises included in post-op appointments
• Better wound management protocols
• Altered mode of knee surgery treatment
QUALITY IMPROVEMENT USING
PROMS IN TOTAL KNEE
REPLACEMENT Presenter: Mr T Partridge MBBS, MRCS
Northumbria Healthcare NHS Foundation Trust
Co-authors: Muller S, Emmerson KP, Carluke I, Partington PF, Reed MR
Large provider
Vast geography
4 main sites
Over 2000 hip and knee
replacements/year (3rd
largest nationally)
INTRODUCTION
PROMs introduced in 2009
Evaluate quality of care
Drive patient choice
Empower commissioners
Total Knee Replacement
Pre and 6 month post procedure OKS and EQ5D
Remuneration on compliance and outcome
QUALITY IMPROVEMENT USING PROMS
IMPROVING PROMS IN TOTAL KNEE
REPLACEMENT BY CHANGING IMPLANT: A
QUALITY IMPROVEMENT PROJECT
DOES PRESERVATION OF THE INFRAPATELLA
FAT PAD IMPROVE PROMS IN TOTAL KNEE
REPLACEMENT?
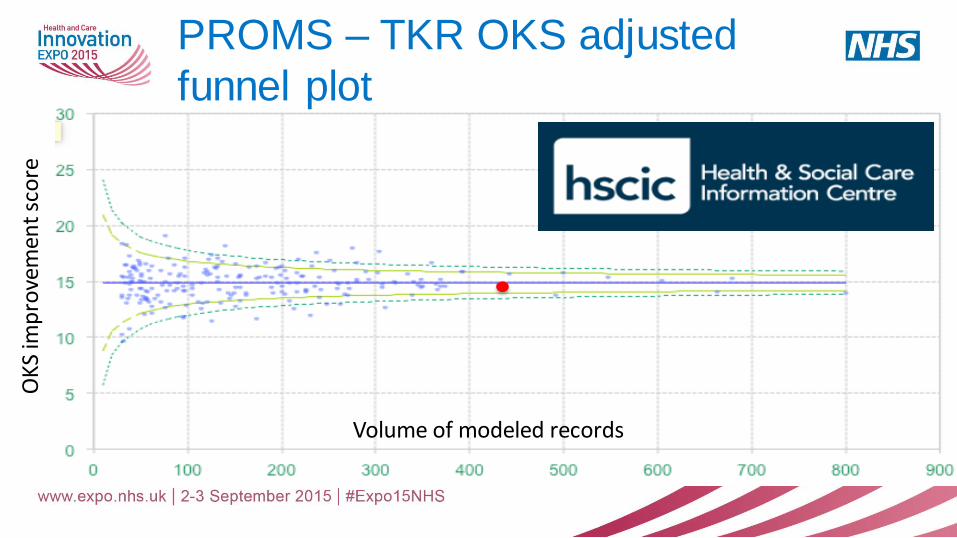
PROMS – TKR OKS adjusted
funnel plot
Volume of modeled records
OK
S im
pro
vem
ent
sco
re
BACKGROUND
Significant variation in PROMs improvement
scores between TKR brands
METHODOLOGY
• Mass move to ‘best’ TKR brand
– 6 month transition period
– Re-training
• Retrospective cohort study using PROMs database
– April 2009 to March 2014 Northumbria Healthcare TKR
– Incomplete records/transition period excluded
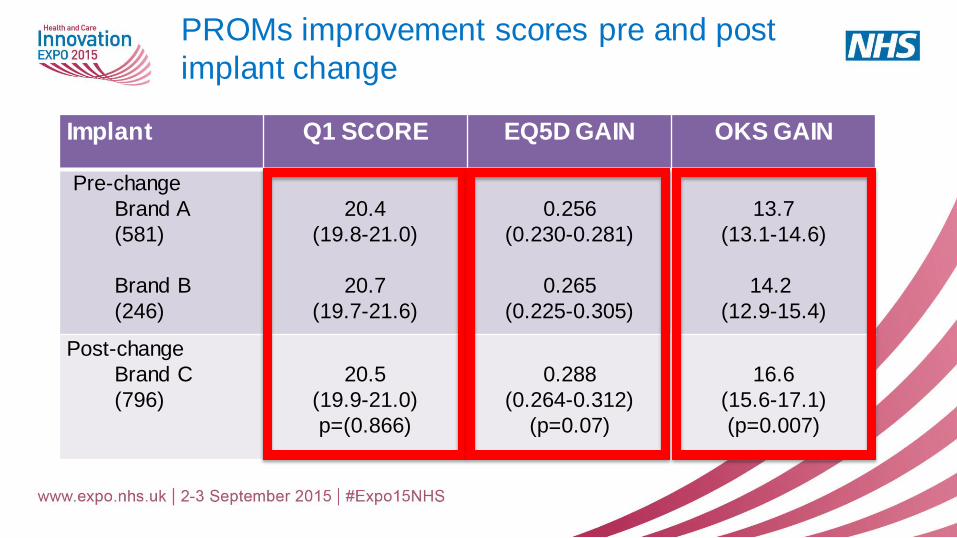
PROMs improvement scores pre and post
implant change
Implant Q1 SCORE EQ5D GAIN OKS GAIN
Pre-change
Brand A
(581)
Brand B
(246)
20.4
(19.8-21.0)
20.7
(19.7-21.6)
0.256
(0.230-0.281)
0.265
(0.225-0.305)
13.7
(13.1-14.6)
14.2
(12.9-15.4)
Post-change
Brand C
(796)
20.5
(19.9-21.0)
p=(0.866)
0.288
(0.264-0.312)
(p=0.07)
16.6
(15.6-17.1)
(p=0.007)
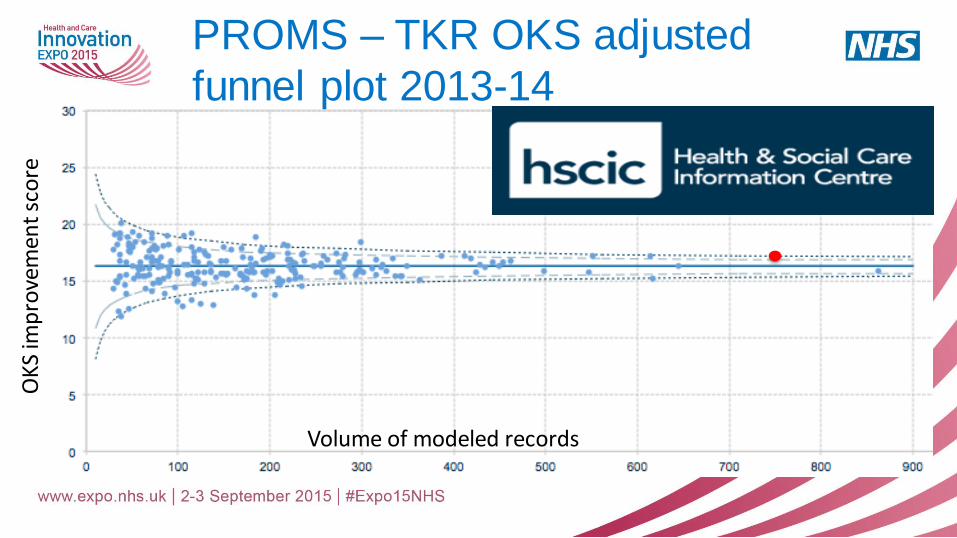
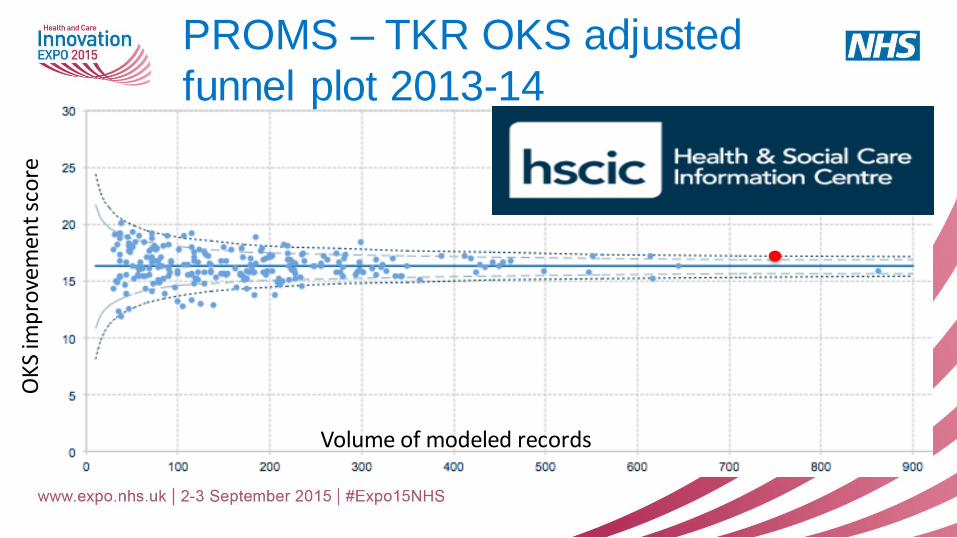
PROMS – TKR OKS adjusted
funnel plot 2013-14
Volume of modeled records
OK
S im
pro
vem
ent
sco
re
STUDY CONCLUSIONS
• Significant improvement in TKR outcome by change of TKR brand
• Evidence based practice - highlighted by PROMs/NJR project
• Showcase national PROMs agenda
DOES PRESERVATION OF THE
INFRAPATELLA FAT PAD IMPROVE
PROMS IN TOTAL KNEE REPLACEMENT
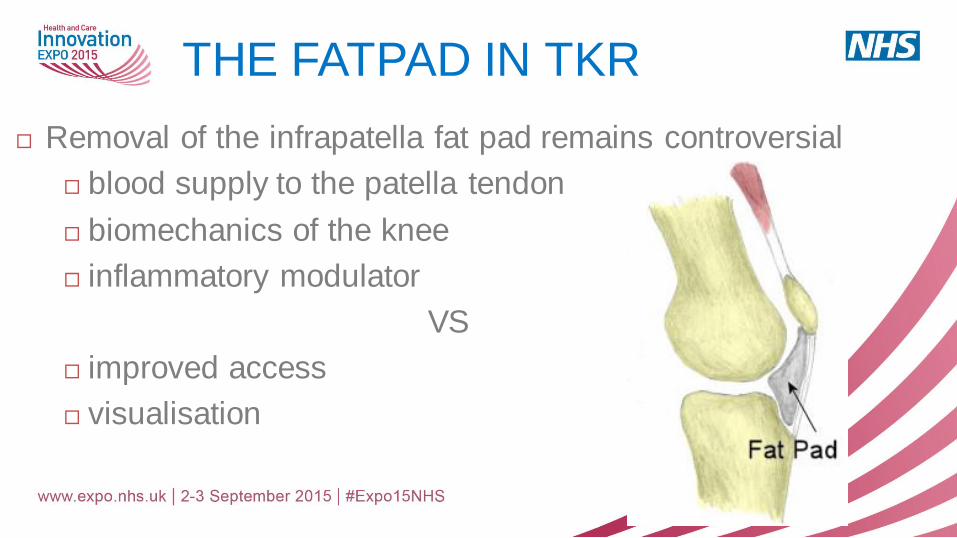
THE FATPAD IN TKR
Removal of the infrapatella fat pad remains controversial
blood supply to the patella tendon
biomechanics of the knee
inflammatory modulator
VS
improved access
visualisation
AIM AND METHODOLOGY
To determine if the default removal of the infrapatella fat pad
affects patient outcome in TKR.
Retrospective cohort study using PROMs database
OKS and EQ5D pre-operatively and at 6 months.
Correlated with consultant default practice of
excising
partially removing
preserving the infrapatella fat pad.
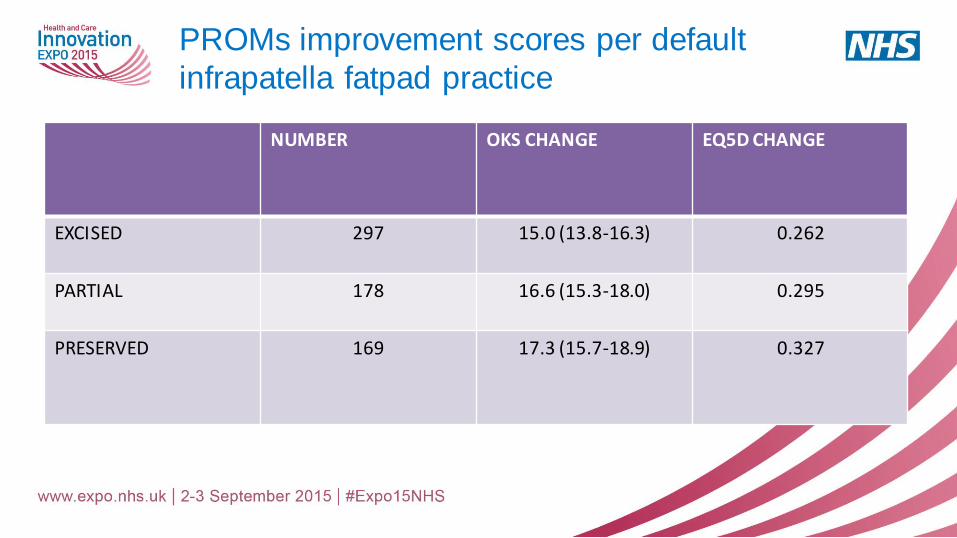
PROMs improvement scores per default
infrapatella fatpad practice
NUMBER OKS CHANGE EQ5D CHANGE
EXCISED 297 15.0 (13.8-16.3) 0.262
PARTIAL 178 16.6 (15.3-18.0) 0.295
PRESERVED 169 17.3 (15.7-18.9) 0.327
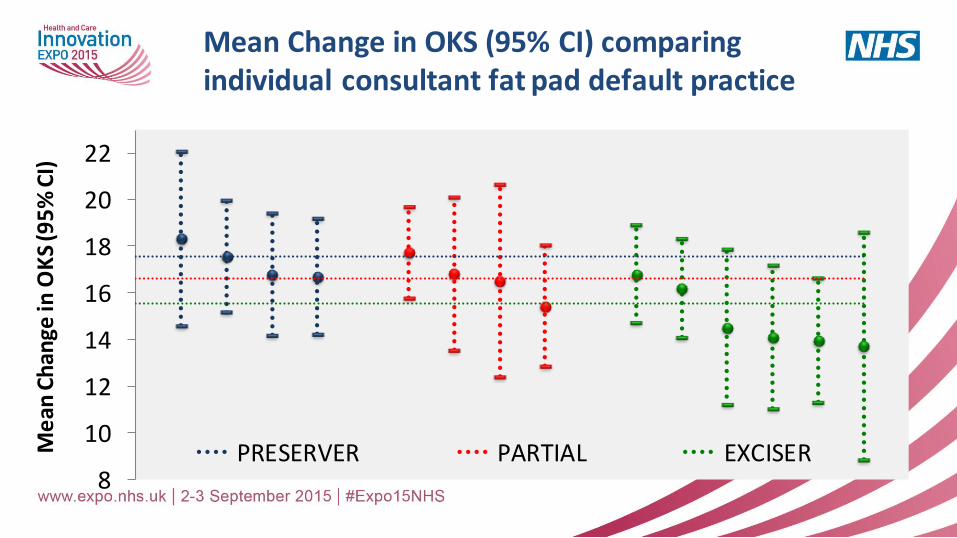
Mean Change in OKS (95% CI) comparing individual consultant fat pad default practice
8
10
12
14
16
18
20
22
Me
an C
han
ge in
OK
S (9
5%
CI)
PRESERVER PARTIAL EXCISER
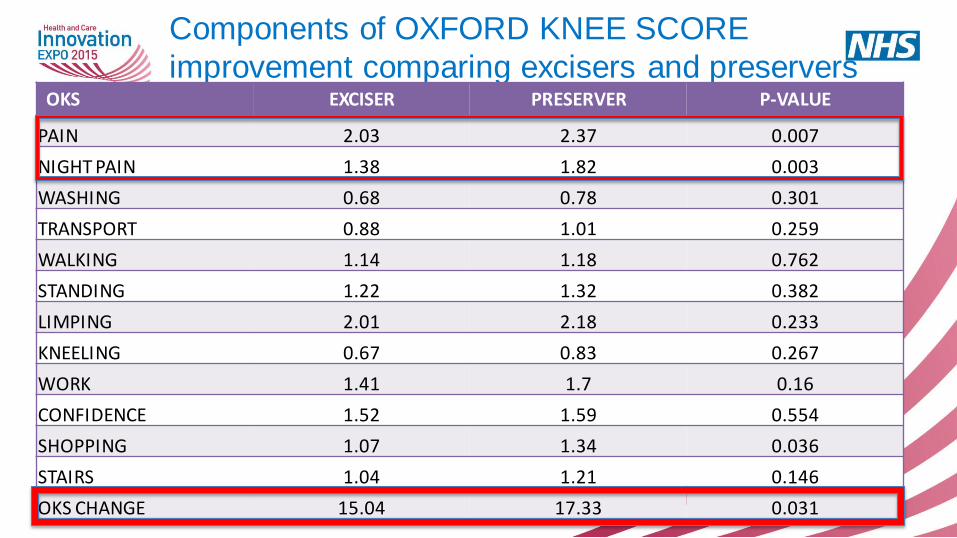
Components of OXFORD KNEE SCORE
improvement comparing excisers and preservers OKS EXCISER PRESERVER P-VALUE
PAIN 2.03 2.37 0.007
NIGHT PAIN 1.38 1.82 0.003
WASHING 0.68 0.78 0.301
TRANSPORT 0.88 1.01 0.259
WALKING 1.14 1.18 0.762
STANDING 1.22 1.32 0.382
LIMPING 2.01 2.18 0.233
KNEELING 0.67 0.83 0.267
WORK 1.41 1.7 0.16
CONFIDENCE 1.52 1.59 0.554
SHOPPING 1.07 1.34 0.036
STAIRS 1.04 1.21 0.146
OKS CHANGE 15.04 17.33 0.031
STUDY CONCLUSION
Patients report better outcomes if their surgeons default to
preserving the infrapatella fat pad
Pain is reported difference
In the absence of a randomised trial surgeons should consider fat
pad preservation
PROMS – TKR OKS adjusted
funnel plot 2013-14
Volume of modeled records
OK
S im
pro
vem
ent
sco
re
PROMS
• Show case PROMs agenda
• Local projects vs national projects
• Publication of trust PROMs and the possibility of performance based
remuneration makes self-evaluation of practice ever more important.
• Excellent opportunity for quality improvement
Thank you

![2012-13 Prom Dress Code[2] › userfiles › 127 › 2012-13 Prom Dress Code(1).pdfForest Park High School Prom 2013 Prom Dress Code To: Prom participants From: Jeff Jessee, Principal](https://img.pdfslide.net/doc/110x75/5f284715184c880cdb06d74d/2012-13-prom-dress-code2-a-userfiles-a-127-a-2012-13-prom-dress-code1pdf.jpg)