Embed Size (px)
Citation preview

ManualοΙ Glinical
ΡarΠtnff0ntΠΦ$

*B00κPuTE$'A Dreat eift ldea!
Personalize your message!
ManualοΙ Gliniοal
Pefi0dοntics
ffi^,:DΕDιcArroNs
Τo the loves of my life Cheryl, Andrew, and Grace.Τhanks for all of the wonderful things that you have brought to my life. -FGS
To Jean for her encouragement, love, and dedication for so many years. Thank you. -Bud
ACKNOI/VLEDGMENTS
The Manual of CΙinical Periodontics exists in its present form as the result of the concerted efforts of the following individuals:Robert D. Kerscheη pub|isher and president of Lexi_Comp, lnc; Lynn D. Coppinger, managing editor; David C. Marcus, directorof information systems; Brad Bolinski, product manager; and Tracey J. Reinecke, cover art design.
NoτlcEThis handbook is intended to serve the user as a handy, quick reference and not as a complete reference source onperiodontics. While great care has been taken to ensure the accuracy of the information presented, the reader is advised thatthe authors, editors, reviewers, contributors, and publishers cannot be responsible for the continued currency of the informationor for any errors, omissions, or the application of this information, or for any consequences arising therefrom. Therefore, theauthor(s) and/or the publisher shall have no liability to any person or entity with regard to claims, loss, or damage caused, oralleged to be caused, directly or indirectly, by the use of information contained herein. Because of the dynamic nature of clinicaland drug information, readers are advised that decisions regarding treatment and/or drug therapy must be based on independentjudgment of the clinician, changing information about a treatment or drug (ie, as reflected by the literature and drugmanufacturer's most current product information), and changing dental practices. The editors are not responsible for anyinaccuracy of quotation or for any false or misleading implication that may arise due to the text or formulas as used or due to thequotation of revisions no longer official. The editors, authors, and contributors have written this book in their private capacities.No official suppo( or endorsement by any federal agency, educational institution, or pharmaceutical company is intended orinferred. The publishers have made every effort to trace the copyright holders for borrowed material. lf they have inadvertentlyoverlooked any, they will be pleased to make the necessary arrangements at the first opportunity.
Copyright @ 2002by Lexi-Comp, lnc. All rights reserved.
Printed in the United States of America. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior wriftenpermission of the publisher.
,
I
Δ ' Lexi-Comp, lncΖ*E#ξ 11oo τerex RoadllUf Hudson, ohio 44236>'-' τoll free: 1-800-837-5394
Lεxl,CoιηB !πc www.lexi.comtsBN '1-930598-82-3

TABLE OF CONTENTS
About the Authors
Preface. ..-.......4
Chapter 1:Problem-Based Periodontal Diagnosis and Disease Management. ...........5Ηealth and Disease ... ....... 5Disease Categories ... ....... 5Diagnosis and Classification ... ... ... 5Evidence-Based Thinking ......... .. . I
Equivalence Testing ...... 8Superiority Testing ....... 8
Parameters of Care ... ....... I
Chapter 2: Anatomy, Ηistology, and Physiology of the Periodontium. ............ 9Functions of the Periodontium.. ......9Surface Characteristics of the Periodontium. ......... 9Histology of the Periodontium .. . 10
Clinically Healthy Gingiva .... . 10
Supporting Structures Beneath the Gingiva .... ..... 11
Blood Supply ........ 12
lnnervation ..........13Biologicνη/idth.. .....13AttachmentΑpparatus . . 13
Gingival Crevicular Fluid... ..........13
Chapter 3: Etiology and Classification of the Periodontal Diseases 15
Concepts of Etiology . . 15Biofilms. .... . 15Features of Periodontal Pathogens. ......... 16Dental Calculus .... .. .......17Risk Factors - Local and Systemic ...... .. . 18
Classification of Periodontal Diseases. ......221999 Classification System. .........23Distinguishing Characteristics of Gingivitis, Periodontitis, and Other Periodontal Diseases
and Conditions...... ......29
Chapter 4: Clinical Αssessment, Diagnosis, and τreatment Pιanning . . '.. 31RiskΑssessment.... ........31Components of the Clinical Periodontal Examination .. . . 31lnstruments and Materials for Periodontal Assessment ..... 34Radiographic Examination. ..........34Periodontal Screening and RecordingτΜ Examination....... . ''.'' 34Adjunctive DiagnosticTechniques ...........35Periodontal Treatment Planning . .. . . 36SamplePeriodontal ΤreatmentPlans. ..'...36Periodontal Prognosis ....... 39
chapter5: Prevention of Disease and Maintenance of Ηealth ''''.''''' 41
Toothbrushing Methods ..... 41
lnterproximal Cleaning ...... 41Antimicrobial Agents ........ 42Dentifrices . . ..43Therapeutic Endpoints . .. 43Clinical Parameters of Success .43Maintenance of Periodontal Health. ......... 44
Components of the Maintenance Visit. ..........45
Chapter 6: Nonsurgical Treatment: Scaling and Root Planing, occlusal Therapy, and ΑntibioticTherapy .......47
Scaling and Root Planing ......... .. 47occlusal Τrauma ...'..' '.. ' ' 52occlusal τherapy. . '''''52
Force Control ...... .... .. 55Antibiotic τherapy ..... ...... 58Suggested Systemic Αntibiotic Regimens ........... 59Local AntibioticΤherapy. ............60
Chapter 7: Surgical Treatment: Principles .... 61
Basic Principles...... ....61Categories of Surgery ...... ..... 61
When ls Surgery Necessary? .. .... . 61
Flap Surgery ... .... . 63
Basic Approaches .... ...... .... . 63
Types of Flaps .. .... . 63
Anatomic Landmarks ... ..... 66
Wound Closure. ..... 68
Wound Healing . .70
Chapter8: Surgical τreatment: Repair, Resection, and Regeneration .... '.'''.73Gingivectomy. .......7gElectrosurgery ...... .74Apically-Positioned Flap . . .,. 75
Classification of Osseous Defects ...........77Crown Lengthening . ........ 82
Periodontal Regeneration ........... 83
Meοhanisms for Bone Grovvth ....... 83
Materials for Regenerative Therapy . ........ 87
Techniques Used in Regenerative τherapy ..... .... 88
Chapter 9: Surgical Treatment: Periodontal Plastic Surgery ..... 91
Defects Treated by Periodontal Plastic Surgery Procedures ........ 91
Aesthetic Εvaluation. .....91Gingival Recession .. ........ 92
Alveolar Ridge Defects ...... 93
Εxcessive Gingival Display- DiagnosisandTreatment...... '''.''.94Procedures Used in Periodontal Plastic Surgery . .. .... 94
Chapter 10: Periodontal Emergencies . . .. 1ο5
Diagnosis of Periodontal Emergencies . .. 105
Signs, Symptoms, and Treatment of Periodontal Emergencies. ... 105
Periodontal Abscess ... 106
Pericoronitis .... 106
Αcute Herpetic Gingivostomatitis ... . .. 106
Necrotizing Ulcerative Gingivitis . ....... 1O7
Differential Diagnosis of an Endodonticand Periodontal Abscess. .......107
Chapter 11: Considerations in lmplant Dentistry . . . 109
Biomechanics of Modern lmplants . . 109
Signs of a Healthy and Αiling lmρlant ...... 109
Protocol for lmplant Maintenance .......... 110
APPENDIX
Medical Considerations in the Periodontal Patient ......... 114
Calcium Channel Blockers and Gingival Ηyperplasia ....'. 115
Dental Drug lnteractions: Update on Drug Combinations Requiring Special Considerations........ 116
Occupationsl Exposure to Bloodborne Pathogens (Universal Precautions) ......... 121
Predominant Cultivable Microorganisms of the Oral Cavity . . . .. . . . 124
Reference Values for Adults .. . . . 125
Dentifrice Products . .. ...... 128
Oral Rinse Products. .......133Prescription Writing ......134Safe Writing Practices. .....'136lnsurance Coding for the Periodontal Patient .. . . .. 137
Selected Readings - General .......141Selected Readings - Specific .......142

ABoUτ τHE AUτHoRs
ABOUT THE AUTHORS
FRANCIS G. SERIO, DMD, MS
Dr. Francis G. Serio is Professor and Chairman of the Department of Periodontics at the University of MississippiSchool of Dentistry. He is a Diplomate of the Αmerican Board of PeriodontoΙogy. He received his B.A. from TheJohns Ηopkins University, D.M.D. from the University of Pennsylvania, and M.S. and Certifiοate in Periodontics fromthe University of Maryland. Dr. Serio has been involved in education, research, and international volunteer activitiessince 1981 . He has published 30 articles, 3 books, several book chapters, and numerous abstracts. He has lecturedthroughout the United States and in six other countries on various aspects of Periodontics.
Dr. Serio is the founder of the Dominican Dental Mission Project, a volunteer program that provides dental care tothe rural poor in the Dominican Republic. ln 1991 , the project received the President's Volunteer Action Award fromPresident George H.W. Bush, and was named one of the Points of Light in 2001 by President George W. Bush. lnaddition to his academic responsibilities, Dr. Serio maintains a private practice limited to Periodontics and lmplantDentistry.
CHARLES E. HAνVLΕY, DDs, PhD
Dr. Hawley was Professor in the Department of Periodontics, Dental School, University of Maryland from 1982-2001. During that time period, Dr. Haw|ey directed, at one time or another, every eduοational program thedepartment offered to predoctoral and postdoctoral students. He was Director of the Αdvanced Dental EducationProgram in Periodontics from 1996-2001. He is Professor Emeritus in the Department of Periodontiοs at Marylandand also Visiting Professor, Department of Periodontology, Tufts University. Dr. Hawley is a consultant in periodon-tics to the Commission on Dental Accreditation of the Αmerican Dental Association. He has published over 70manuscripts, abstracts, and book chapters.
From 1962-1982, Dr. Hawley νvas a career dental officer in the U.S. Army Dental Corps. Dr. Hawley \Λ,as the firstDirector of the U.S. Army Residency Program in Periodontics at Ft. Gordon, GA. He retired from the Army at therank of Colonel, and at that time, Dr. Hawley was awarded the Legion of Merit.
Dr. Hawley received a Bachelors degree from The Johns Hopkins University, a DDS from the University ofPennsylvania, a Certificate in Periodontics and a Masters degree in Histology from the University of lllinois, and aPhD in Microbiology and lmmunology from the University of Maryland. He is a Diplomate of the American Board ofPeriodontology. During his professional life, Dr. Ηawley was elected to the lnternational College of Dentists, theAmerican College of Dentists, and the Pierre Fauchard Αcademy.

PFEFACE
PREFACE
TheManuatofCtinicatPeriodonticsisu/rittenasaquickreferenceforgeneraldentists,dentalhygienists,dentalstudents, and dental hygiene students. Both basic and clinical science topics.are arranged in a tabular form toallow for easy access to each chapιer.
Each chapter is presented in a "Question & Answer'' format, providing a stepwise approach to thal particular area.This book has been written in a straighforward manner, making it a practical resource both in clinical practice and inan educational setting. Chapters are arranged by basic principles, disease entities, diagnosis, treatment planning,and then various treatment options.
The authors intend that this book be a quick and easy reference to many of the clinical problems that challenge allpractitioners and students of periodontics.
:'.

CHAPτEB 1 -
CHAPTER 1: PROBLEM-BASED PERIODONTALDIAGNOSIS AND DISEASE MANAGEMENT
The framework of effective periodontal therapy includes aworking diagnosis and classifiοation of disease, the identifi-cation of pertinent etiologic factors, and a treatment plan thataddresses eaοh of the etiologic agents in a logical sequence.Τo ignore pertinent etiologic factors in the treatment plan willtranslate to undertreatment and failure in therapy. Treaιment of etiologic factors that either do not exist, or that havebeen incorrect|y identified, wiΙl produce overtreatment andunnecessary financial or physical hardships for the patient.
Problem-based periodontal therapy begins wiih an under-standing ot health and knowing what it means to diagnoseand classify a disease.
What ls Health? \Mhat ls a Normal Periodontium?What ls Meant by the Term "Disease"?
Health is the absence of disease or abnormality. Periodontalhealth then is defined by the absence of marginal periodontalinflammation, the absence of inflammation in the periodontalligament, or evidence of periodontal deformities. Success-fully treated and maintained gingivitis patients may be bothfree of disease and have a normal periodontium.
Periodontitis patients who have received successful perio-dontal and maintenance therapy (ie, patients who are appar-ently free of periodontal inflammation with no ongoing injuryin the periodontal ligament) may, by definition, be consideredhealthy as well. However, these patients may not have anormal periodontium.
DiSeaSe is defined aS a ρrocess that is οharacterized by aseries of morbid pathobiologic events that produce cliniοalsigns and symptoms in the affected host. The processocοurs in response to known or unknown etioΙogic factors.
What Are the Fundamental Periodontal DiseaseCategories? Do These Periodontal DiseasesConform to the Definition of Disease?
The basiο categories of periodontal diseases are:
. Gingivitis. The gingival diseases are periodontaldiseases in which the process is gingival inflammation,the primary etiologic factors may be microbiologic,systemic diseases, or physical injury, and the signs andsymptoms are gingival bleeding, increases in probingdepths, and pain. Loss of periodontal attachment, toothmobility and/or fremitus of teeth, and tooth migration,arenot ordinary features of gingivitis. As it is with all inflam-matory diseases, the pattern and severity of gingivalinflammation in a given patient is affected qualitativelyand quantitatively by local and/or systemic contributingfactors.
. Periodontitis. The types of periodontitis are periodontaldiseases in which the process is periodontal inflamma-tion, the primary etiologic factor may be microbiologiο,systemic diseases, or physical injury, and the signs andsymptoms are gingival bleeding, increases in periodontalprobing depths, destruction of periodontal attachment,pain, and tooth loss. Mobility and/or fremitus and migra-tion of teeth are consequences of forces on teeth withreduced/lost periodontal attachment (see occlusal trau-matism below). The pattern and severity of periodontal
inflammation in a given patient is affected qualitativelyand quantitatively by local and systemic contributingfaοtors.
. Occlusal traumatism. Occlusal traumatism is a perio-dontal disease in which the process is inflammationιΛ/ithin the periodontal Ιigament and the alveolar bone(the lesion of trauma from occlusion), the primary etio-logic factor is force acting on teeth, and the signs andsymptoms are pain, tooth mobility and/or fremitus, andpathologic migration of teeth. The pattern and severity ofthe lesion of trauma from occlusion in a given patient isaffected quantitativeΙy and qualitatively by local andsystemic contributing factors.
Each one of these categories conforms to the definition ofdisease. ln each disease, there is a process, there is a seriesof morbid pathobiologic events that are outcomes of theprocess, and there is a reΙated set of clinica| signs and symp-toms.
What ls Meant by the Expressions "Diagnosis"and "Ctassification"?
F|GURE 1. Photomicrograph of the ρrocess of inflammation in the marginalperiodontium. τhe morbid outcome of the process is histologically repre-sented as evidence of resorbed alveolar bone and the level of attachmenton cementum.
Diagnosis is the aιt of identifying the disease process. lt isthe product of a careful evaluation of the patient's history, thearray of symptoms presented by the patient, and the clinicalsigns revealed during a clinical examination. For instance,the diagnosis of periodontitis is ordinarily achieved bydetecting gingival bleeding with a periodontal probe, destruο-tion of periodontal attachment using radiographs and/or aprobe, mobility and/or fremitus digitally, determining anypathologic migration and/or loss of teeth. Figure 1 representshistologically the process of marginal periodontal inflamma-tion and the morbid outcomes (ie, loss of both alveolar boneand periodontal attachment) of periodontitis.
-

PRoBLEM-BASED PERloDoNτAL D|AGNoSΙs AND D|SEASE MANAGEMENτ
CΙassification is the art of categorizing individual clinicalcases of disease according to treatment requirements. Clas-sification systems are frequently used by third pafty prov-iders to help understand treatment needs. For over 20 years,dentists have been using a classification system developedby the Αmerican Αcademy of Periodontology (AΑP) to facili-tate dialogue among dentists and between third party individ-uals concerning the severity of periodontal diseases, and bydirect extension, treatment needs. This classification systemconsisted of:
. Type l. Gingivitis where gingival inflammation \νaspresent without radiographic evidence of intΘrproΧimaΙbone loss.
FIGURE 2. An artistic represenιation ot gingivitis" There is gingival erythemaand edema. τhe clinical attachment levels are at the cementoenameliunction. The alveolar bone height wilh respect to the cementoenameliunction is normal. Restoraιion of a healthy periodontium without furtherloss of attachment may be predictably achieved with nonsurgicaltherapy. (Couftesy of Kala Addess, MS, RDH)
. Type ll. Early periodontitis where gingival inflammationwas superimposed over clinical evidence of mild boneloss without furοation invasions.
FIGURE 3. An artistic representation of earιy periodon lfis. τherΘ is gingivalerythema and edema. τhere is early loss of clinical attachment andreduclion of alveolar bone height. Furοation invasions wilι probably notbe clinically or radiographically apparent. Periodontal health and func-tion may usually be restored by nonsurgical and/or surgicaΙ therapy.(cour1esy of Kala AddeSS' ΜS' RDH)
. Type lll. Moderate periodontitis where gingival inflam-mation was superimposed over clinical evidence ofmoderate bone loss with early furcation invasions andpossible tooth mobility.
FiGURΕ 4. An artistic representation ot moderate periodontitis. τhere isgingival erythema and edema. τhere is moderate lοss of clinical atιach-ment and reduction of alveolar bone height. Furcation invasions areevident both cιinicaΙly and radiographically. Affected teeth may showdegrees of mobility. Shaded area on the adiacent tooth indicates thatregeneration ot Ιost periodontal tissues may be one outcome ofsuccessful periodontal theraρΥ. (courtesy of Karla AddeSS' Ms' RDH)
. Type lV. Αdvanced periodontitis where gingival inflam-mation was superimposed over severe bone loss withextensive furcation invasions and tooth mobility. Casesof this type could display tooth loss due to periodontitis,pathologic migration of teeth, posterior bite collapse,and/or loss of occluding vertiοal dimension.
FΙGUBE 5. An artistic representation oΙ advanced periodontitis. τhere isgingival erythema and edema. τhere is advanced loss of clinical attach-ment and alveolar bone height. Furcaliοn invasions are θxtensive. τoothmobilily and/or pathologic migration may be seen. τeeth with advancedperiodontitis frequently have a poor prognosis, and decisions abοuttherapy often include the placement of implants. (Couιlesy of ΚarlaAddess, MS, RDH)
While the terms that defined each type were intentionallyvague, the system did provide the framework for dialogueamong therapists, allied personnel, and third party payers

CHAPTER 1
over treatment needs for each case. For instance, a treat-ment plan for a Τype lll moderate periodontitis casedispΙaying the osseous defects and furcation invasionsshown in Figure 6 would be expected to include resectiveand/or regenerative surgical therapy. Τhe treatment plan fora Type ll early periodontitis οase, such as that shown in
Figure 7, would probably not include resective or regenera-tive therapy.
FIGURE 6. A dried human mandible showing periodontaΙ osseous defects andfurcation invasions that are οonsistent with a type lll moderate periodon-titis case.
FIGURE 7. A dried human mandible showing minor periodontal osseousdeformities that are consistent with a type ll early periodontitis case.
As the knowledge base about the patterns of periodontaldiseases improved, this system of classification becameinadequate. Models of periodontitis had emerged sug-gesting that not all cases of periodontitis behaved thesame clinically, that small (<1 mm) changes in attachmentlevel were difficult to detect clinically, and that there wasevidence that all cases of periodontitis did not respond thesame to therapy.
An attempt to overcome many of these shortcomingsoccurred during the 1999 lnternational Workshop for a Clas-sification of Periodontal Diseases and Conditions. Here,scientists and clinicians agreed upon a reclassificationsystem to improve the understanding of periodontal diseasesamong scientists, clinicians, and allied dental healthcare
agencies. Each new or revised category of disease wasbased, in part, upon its etiology and the particular healthcarerequirements to control etiology.
The new System includes eight major οategories of perio-dontal diseases or conditions, and each of the categories issubdivided into specific etiology-based diseases or condi-tions. This new Classification System for PeriodontalDiseases and Conditions was adopted by the AAP in 2000.Τo facilitate its use in every-day periodontiοs, the newsystem would be modified over time.
How Are Scientifically-Based Decisions Made inSuccessful Periodontics? What ls Meant by theExpression "Art of Decision-Making inPeriodontal Therapy"?
Successful periodontal therapy is based upon scientifically-based decisions involving: the disease process, the identifi-cation of aΙl etiologic factors, a correct diagnosis, controllingthe etiologic factors, and correcting deformities produced bydisease.
The arl of decision-making in periodontal therapy involvesthe synthesis of:
1. Clinical experience of the therapist
2. Τechnical ability of the therapist
3. lntuition
4. Experiences of others (type lll information) asreported and presented at professional forums
5. Evidence-based thinking
F|GURE 8. οlinical decision_making in periodontics can be multifaceted.Evidence-based thinking b.ings the outcomes of sοientificalιy soundcΙinicaΙ trials into the process.
While the traditional components of a deοision processremain impoftant ingredients (ie, a clinician will not ordinarilymake a treatment decision that will involve a technique thatis beyond the scope of his/her abilities), the fact remains thatthe knowledge base in a|l aspects of periodontiοs is rapidlyexpanding. lt is incumbent that clinicians keep current withnew science and technology, evaluate reports in the litera-ture criticalΙy, and utilize new information in their practiceswhen appropriate.
PRoBLEM-BASED PERloDoNτAL DlAGNosls AND DlsEAsE MANAGEMENτ
What ls Meant by the Expressions "Evidence-Based Thinking", "Equivalence Testing", and"Superiority Testing"?
Εvidence-based thinking occurs when the therapist logicallyand systematically utilizes scientifically-based clinicalevidence in the process of making decisions about diag-nosis, prognosis, and treatment.
Εquivalence testing in c|inical trials may show that a methodis at least as effective as a commonly employed "gold stan-dard". Superiority testing may show that a given method willproduce outcomes that will be more beneficial than anotherto a patient.
lf there is evidence that a technique or concept of therapy ispredictably equivalent or superior in a given clinical scenario,then, within the scope of experience and ability, it should beconsidered as a treatment option. ln doing so, the number ofoptions available to the patient are increased, and the poten-tial for placebo effects, personal biases, or clinical experi-ences of the therapist that have no controls are kept to aminimum.
The fallout of evidence-based thinking in clinical periodonticswill inevitably be an increased number of treatment options,increased patient confidence, practice gro\λ/th, and improvedtherapeutic outcomes.
What Are the Parameters of Care?
The AAP took a leadership role in developing diagnostic andtherapeutic guidelines for what might be considered the stan-dard of care for periodontal patients. The resulting Parame-ters of Care describe the scope of possible active treatmentplans for the following clinical situations:
ο Plaque-associated gingivitis
o Chronic periodontitis with slight to moderate loss of peri-odontal support
o Chronic periodontitis with advanced loss of periodontalsupport
. Refractory periodontitis
. Mucogingivalconditions
ο Acute periodontal diseases
. Αggressive periodontitis
. Placement and management of the dental implant
. Occlusal traumatism in patients with chronic periodontitis
o Periodontitis associated with systemic conditions
. Systemic conditions affected by periodontal diseases
o Periodontal maintenance
The emphasis of the current parameters is treatment andwhat therapeutic entities might be appropriate for given peri-odontal conditions. Each parameter is inclusive so as to givethe reader (clinician, patient, third party healthcare provider,etc) an appreciation of the scope of acceptable care in eachcategory. The parameters do not prescribe the care thatevery periodontal patient in a given category should receive.The final decision over what will constitute a treatment planin a given case remains, as it should be, in the hands of theclinician and the patient.
Definitions of terms and details of each of these parametersof care may be obtained at the web site of the AmericanΑcademy of Periodontology, www.perio.org.

CHAPτER 2
CHAPTER 2: ANATOMY, HISTOLOGY, AND PHYSIOLOGY OF THEPERIODONTIUM
Α οlear understanding of the structure and function of theperiodontium is necessary in order to appreciate the diseaseprocess and treatment. The periodontium consists primarilyof noncalcified and οalcified connective tissues covered by aprotective layer of epithelium. lt is the destruction of thecalοified conneοtive tissues due to the host response to theexogenous and endogenous periodontal pathogens thatgives rise to a ιoss of periodontal Support and eventua| toothloss.
What Are the Functions of the Periodontium?
. Attach the tooth to the alveolar bone proper
. Resist and dissipate the forces generated by mastica-tion, speech, and deglutition
. Αdjust to οhanges in functional demands through contin-uous remodeling, regeneration, and repair
o Defend against the external pathogenic and environ-mental influences present in the oral cavity
What Are the Surface Characteristics /Landmarks of the Periodontium?
FlGURE 1Α. surface characteristics and Landmarks of the Periodontium.
Free gingivat margin: This is the most coronal edge ofthe gingiva.
Free gingival groove: A groove seen on the facialgingiva that approximates the location of the base of thesulcus. The free gingivaΙ groove is not always present(estimated in only 30% to 40"λ ot adults), nor is it anexact landmark for the base of the sulcus.
Keratinized tissue: The surface of the tissue thatcomprises the free and attached gingiva. Τhe boundariesare from the free gingivaΙ margin to the mucogingivaliunction on the facial and lingual surfaces. Thekeratinized tissue is continuous with the rest of themastiοatory mucosa of the palate. The keratin is found inthe stratum corneum of the epithelium and may beparakeratin (cell nucΙei remaining) or orthokeratin (thicklayer of keratin without remaining cell nuclei). Theepithelium covering is also referred to as the oralepithelium.
Free gingiva: The gingiva from the free gingival marginto the base of the sulοus' This tissue is continuous withthe attached gingiva but is not bound down to anyunderlying structure.
Attached gingiva: Gingiva that is firmly bound down tounderlying tooth structure, periosteum, and bone. Τheboundaries of the attached gingiva are from the base ofthe sulcus to the mucogingival junction. The width offacial attached gingiva ranges from 1-9 mm and isgreatest on the facial surface of the maxillary lateralincisor and narrowest on the facial surfaces of themandibular canine and first premolar. On the lingual,attached gingiva was widest near the first and secondmolars and narrowest adjacent to the incisors andcanines. The thickness of attached gingiva averages1.25 mm + O.42 mm.
Mucogingival junction: The demarcation between theattached gingiva and the alveolar mucosa apical to theattached gingiva. The mucogingival junction oftenappears as a distinct line between the two structures. lfthe mucogingival junction is difficult to see, it may beidentified as the fold area when the alveolar mucosa isgently pushed in a coronal direction.
Alveolar mucosa: Part of the lining muοosa. Thea|veolar muοosa is located apical to the attached gingivaon the facial and lingual surfaces. This tissue is looselyattached to the underlying bone, freely moveable, andrelatively fragile compared to the gingiva. There aremore elastic fibers in the alveolar mucosa. This tissueextends into the vestibule of the mouth and is continuouswith the labial, buccal, and lingual mucosa. There is noalveolar muοosa on the hard palate'
Masticatory mucosa: Keratinized tissue including thegingiva and the tissue covering the hard palate.
Frenum (frenulum): The narrow band of tissue thatattaches the labial and buccal mucosa to the alveolarmucosa. There is also a lingual frenum that attaches theanterior part of the tongue to the lingual aspect of thealveolar process and the floor of the mouth in the anteriorregion.FIGURE '1 B. Surface Characteristics and Landmarks of the Periodontium.
-

ANAToMY, ΗtsτoLoGY, AND PHYsloLoGY oF τHE PERloDoNτlUM
. Rugae: The irregular ridges found on the anterior part ofthe hard palate adjacent to the incisors, canines, and firstpremolars.
. Stippling: The irregular surface texture of the attachedgingiva, similar to the surface of an orange peel, found in40% ot adults. Stippling occurs at the intersection ofepitheΙial ridges that causes the depression and theinterspersing of connective tissue papillae betweenthese intersections giving rise to the small bumps.
. Sulcus: This is the space bounded by the free gingivalmargin, the tooth, and the most coronaΙ attachment ofthe junοtional epithelium. ln health, the sulcus usuallymeasures from 1-3 mm deep. ln disease, this space isreferred to as a pocket.
. Col: This is the saddle-like depression in the interdentalgingiva as seen from buccal to lingual apical to thecontact of two adlacent posterior teeth.
What Are the Layers of Cetls That Comprise theOral Epithelium? What Are a Keratinocyte,Langerhans Cell, and a Melanocyte?
The oral epithelium consists of four layers of cells:
1. Stratum basale: Basal layer of cuboidal cells along thebasement membrane. This is where epithelial οell rep|i-cation occurs. Melanocytes are found in this layer.
2. Stratum spinosum: These cells appear to have cyto-plasmic spines when viewed by Ιight microscopy.Langerhans cells, involved in the processing of antigens,are found in this layer. Keratin synthesis begins in thestratum spinosum.
3. Stratum granulosum: Keratohyalin granules may beseen in this layer. Keratin synthesis is ongoing. Cellsappear to be fΙattened.
4. Stratum corneum: This is the layer where para- ororthokeratinization are found.
Keratinocyte: A cell of the epidermis and parts of themouth that produce keratin. Because of their ability toproduce keratins, epithelial cells are referred to as kerati-nocytes. Keratins are a family of approximately 30proteins that form the intermediate filaments of theepithelial cell cytoskeleton. Keratins may be found eΧtra-celluΙarly in the stratum corneum and contribute to theprotective function of epithelium.
Langerhans cell: A dendritic cell in the epidermis.Thesecells are found in the suprabasal layers of the epithelium,Τhey do not have desmosomal attachments to adja-cent cells. Τhey move in and out of the epithelium, arederived from bone marro\,v, and probablyhave an immu-nologic function for recognizing and processing antigens.
. Melanocyte: Α celΙ of the basal layer that producesmelanin pigment granules (melanosomes) that are trans-ferred to surrounding keratinoοytes for transpoι1' Thereare similar numbers of melanocytes in the epithelium re-gardless of the skin or gingival pigmentation present.
What Does Clinically-Healthy Gingiva Look Like?
FlGURE 2. characteristics of the Heaιthy Pefiodontium. τhe hea,thy periodon-tium is genefally coral pink, possibly with natural pigmentation. τhegingival margins are scalloped to a fine edge. τhe tissue is firm, usuallywith a stippled surface.
Color: The normal οolor of gingiva is often described ascoral pink. Gingiva may also have slight to significantbrown pigmentation from the melanoοytes located in thebasal layer of the epithelium.
Size: Gingival contours generally follow the cemento-enamel junctions of the teeth. Tissue thickness is in the0.25-0.5 mm range. Α wider zone of gingiva is normallyseen in the maxillary anterior region, with the narrowestzone of gingiva on the buccal surface of the mandibularfirst premolars. On the lingual, it is narrowest in themandibular region and widest in the molar area.
Contour: Gingiva has been described as being eitherthin and scalloped, or thick and flatter in contour. Thecontour of the gingiva depends on the οontour of thecementoenamel junction of the teeth, the amount of em-brasure space, and the nature of the contact betweenteeth. The gingiva appears prominent over the tooth rootand may have a slightly concave appearance in the inter-proximal area.
Consistency: Gingiva is generally firm to the touch andattached to the underlying bone and/or tooth.
Surface texture: Gingiva may have either a smooth orstippled surface. Stippling is not an indicator of health noris the absence of stippling an indiοator of disease. Thereappearance of stippling during therapy may be an indi-cation of tissue returning to health.

CHAPτER 2
What Supporting Structures Lie Beneath theGingiva?
F|GURE 3A. τhe supporting structures Beneath the Tissue surface. sideview, A. oral epithelium, B. suιcular epithelium, c. Junctional epithelium,D. Dentogingivaι fibers, E. circular fibers, F. Dentoalveolar fibers' G.Acellular cementum, H. Alveolar crestal fibers of the PDL, ι. cellularcementum, J. Horizontal fibers of the PDL, κ. Alveolar bone, L. obliquefibers of the PDL.
FIGURE 38. lnterproximal view. A. Dentogingival fibers, B. Circular fibers, C"τransseptal fibers, D. Alveolar crestal fibers of the PDL, E. Horizontalfibers of the PDL, F. Oblique fibers of the PDL, G. Apical fibers of thePDL' Η. Alveolar bone, lnterradicular fibers not shown.
. Sulcular epithelium: The epithelium that lines thesulοus. ln health, sulcular epithelium does not haveepithelial ridge formation.
o Junctional epithelium: The epithelium that attaches thegingiva to the surface of the tooth, or to compatiblerestorative materials' Τhe special part of the junctional
epithelium that actually provides the attachment is calledthe epithelial attachment. τhis attachment consists of alamina lucida, lamina densa, and hemidesmosomes.
Connective tissue: The predominantly collagenoustissue found beneath the epitheΙium. The connectivetissue contains collagen fibers (60%), fibroblasts (5%),and interfibrillar substanοe οomposed of noncollagenousproteins and mucopolysaccharides, small numbers ofneutrophils and lymphocytes, blood vessels, lymphatics,and nerves (the remaining 35%). Τhe overlying epithe-lium must have intact connective tissue in order tosurvive. Most of the coΙlagen found in the periodontium istype I collagen.
Gingival fibers: These are specially oriented fibers inthe connective tissue. Also known as Ιhe supracrestalconnective tissue fibers, these fibers are designated bytheir orientation: Dentogingival, dentoperiosteal, circular,and transseptal (connecting tνvo adjacent teeth) fibers.Some authors inοlude the transseptal fibers in the prin-cipaΙ fibers of the periodontal ligament, although they areactually tooth-to-tooth and not tooth-to-bone fibΘrs.
Periodontal ligament (PDL): This is the collagenoustissue that surrounds the tooth root and attaches thetooth to the alveolar bone proper. The principal fibers ofthe periodontal ligament have been cΙassified as thealveolar crest, horizontal, oblique, apical, and interradic-ular (in the furcation area of multirooted teeth) fibers. Τheoblique fibers are the most numerous. Fibroblasts, osteo-blasts, cementoblasts, osteoclasts, epithelium, andnerve celΙs are also found in the periodontal ligamentspace. The width of the PDL space is about 0.25 mm innormal function. Α tooth in hypofunction may have anarro\r/er PDL space and a tooth in hyperfunction mayhave a considerably wider PDL space.
FlGURE 4. τhe Attachment Apparatus. From the left: Dentin, cementum, perio-dontal ligament fibers, alveolar bone.
. AIveolar bone: Αlso known as Ιhe alveolar process, thisis the portion of the maxilla and mandibΙe that form andsupport the tooth sockets. The alveolar process givesSupport to the alveoΙi and consists of coιtical bone,cancellous trabeοulae, and the alveo|ar bone proper.
ADc
11
-

Ξ
ANAToMY. HlsτoLoGY. AND PHYsloLoGY oF τHE PERloDoNTlυM
F|GURE 5A. The Alveolar Bone. τhis section shows the relationship of theroots of this molar to the alveolar bone proper and the rest of ιhe alveolarprοcess.
FlGURE 58. τhe Alveolar Bone. ln cross section, corticaι bone can be seen onthe surface of this mandible with trabecular bone within the confines ofthe iawbone. τhe density of the trabeculaιions can vary markedly fromone area of the iaw to another and among individuaΙs.
. Alveolar bone proper: That part of the alveolar bonethat lines the tooth socket. lt is a perforated cribiformplate through which vessels and nerves pass betweenthe PDL and marrow.
. Basal bone: That part of the maxilla and mandible thatsupports the alveolar process. Basal bone is all thatremains once all of the alveolar process is resorbed afterthe teeth are lost from the arch.
. Cementum: The thin, calcif ied tissue of ectomesen-chymal origin covering the roots of teeth in whichembedded collagen fibers attach the teeth to the alveo-lus. There are t\ivo types of cementum: Αcellular andcellular cementum. Acellular cementum does not con-tain cementocytes and is found on the οoronal half of thethe tooth rooΙ. Cellular cΘmentum contains cementocytesand is found primarily on the apical third of the root. lt iscontinuously deposited throughout life.
What ls the Blood Supply to the Periodontium?
FlGURΕ 6Α. Local Blood supply to the Periodontium. supraperiosteal bloodvessels and PDL vessels coalesce into the gingival plexus.
F|GURΕ 68. Loοal Blood supply to the Periodontium. lnterseptal vesselssupply the alveolar bone, PDL, and gingiva.
The blood supply to the periodontium arises from theterminal branches of the internal maxillary aftery. Locally, theblood supply to the gingiva consists of supraperiostealvessels. Vessels from the alveolar bone and periodontal liga-ment also contribute to the coalescence of vessels in thegingival papillae, known as Ιhe gingivaΙ plexus. The alveolar

CΗAPTER 2
bone is supplied by branches of the anterior, middle, andposterior superior arteries to the maxilla and branches of theinferior alveolar artery in the mandible. lntra-alveolar or inteμdental vessels supply the interdental bone. Arterial bloodgenerally flows in an apical-to-coronal direction. Largenumbers of capillary loops that resemble renal glomeruli arefound beneath the iunctional epithelium and sulcular epithe-lium near the surface of the gingiva.
What ls the Innervation of the Periodontium?
Nerve supply to the periodontium is derived from terminalbranches of the maxillary and mandibular branches of thetrigeminal nerve. The periodontium contains sensory recep-tors for pain, touch, and pressure as well as proprioceptors inthe periodontal ligament but not in the gingiva. The sensorynerves have their center in the semilunar ganglion and theproprioceptive nerves are centered in the mesencephaliοnυcleus.
What ls the BioIogic ι,vidth?
duωcτιo*υE
SlλPιeAc'ιee'nLcoilωep-I1ν€
Tι'Sιλ'EΡιB,Ε!LS
FtGURE 7. Biologic νlridth. Junctional epithelium and supracrestal connectivetissue fibers (dentogingival, dentoalveolar, circular, transseptal) must bemaintained in health.
The biologic width is the apicocoronal distance that the junc-tional epithelium and supracrestal connective tissue(gingival) fibers are attached to the tooth. This distance ismeasured histologically from the most coronal part of thejunctional epithelium (base of the sulcus) to the crest of thealveolar bone. The average measurement of the biologicwidth is 2.04 mm, approximately 1 mm for the junctionalepithelium and 1 mm for the supracrestal connective tissuefibers. The sulcus depth is nof part of the biologic width.
ΨVhy Is the BioIogic Vvidth lmportant?
The body maintains the biologic width as a stable dimension.When the biologic width is encroached upon and iniured byextension of restorative preparations and materials into thisarea, uncontrolled inflammation may result as the body triesto reestablish this dimension. ln areas of thin gingiva, thismay result in recession or bleeding upon gentle probing evenwhen the patient has good plaque control and recession.
What ls the Attachment Apparatus?
The attachment apparatus is the alveolar bone proper, perio-dontal ligament fibers, and cementum that attach the root tothe alveolar bone. Regeneration of the attachment apparatusis one of the surgical goals in periodontal therapy. Regenera-tion of the attachment apparatus is the only treatment proce-dure in dentistry where new tissue is histologically identicalto that which has been lost due to the disease process.
ΨVhat ls Gingival Crevicular Fluid?
ln health, gingival crevicular fluid (GCF) is a transudate thatemerges from the gingival sulcus. The gingival crevicularfluid may contain a variety of enzymes and cells, particularlydesquamating epithelium and neutrophils, that are beingshed through the sulcus. An increase in gingival crevicularfluid flow is the first detectable sign of inflammation. Onceinflammation has ocοurred, the GCF is referred to aS aninflammatory exudate. This exudate contains higher levels ofserum proteins and leukocytes.
o', o.
u cιd_.'o'
gto
η
q: )t
itζ
Zι
ζ

Ξ

CHAPτER 3
CHAPTER 3: ETIOLOGY AND CLASSIFICATION OF THEPERIODONTAL DISEASES
The etiology of the periodontal diseases is multifactorial, butbacterial plaque is necessary for the initiation and progres-sion of infΙammatory periodontal disease. Αs indicated by theneνι Ctassification System for Periodontal Diseases andConditions, etiologic faοtors have become the framework forperiodontal diagnosis and classification
What ls lnflammation?
lnflammation is a soft tissue cellular and vascular response tolocal iniury of physical, thermal, chemical, or microbial origin.lnflammatory periodontal diseases are no exception to thisparadigm as local periodontal etiologic factors may be phys-ical (factitial habits such as toothbrush abrasion or occlusaltrauma), thermal, chemical (epithelial disorders associatedWith some mouth\ivashes, smokeless tobaοco, aspirin, andcoοaine), and microbial (dental plaque induced gingivaldiseases). The most common inflammatory periodontaldiseases are caused by a locaΙ accumulation of baοteria.
What ls Meant by EtiologY?
ΕtioΙogy is "the study or theory of the causation of anydisease; the sum of knowledge regarding causes." Therefore,etiology is a noun that defines the science of disease causa-tion, but in common usage, etiology is a cluster of faοtors thatcontribute to disease (ie, the etiology of periodontaldiseases).
What Are the Microbiologiο Etiologic Factors inPeriodontal Diseases?
Τhe microbiologic etiologic factor in periodontal diseases isdental plaque with dental calculus as probably the mostsignificant local contributing factor. Food debris and thebacteria it contains is probably a major etiologic factor in rootcaries.
F|GURE 1. A photomicrograph showing severe marginaΙ inllammation andlocal etiologic factors of bacteriaι origin.
There is littΙe dispute over the concept that bacteria are theprimary etiologic factors in inflammatory periodontaldiseases. ln 1965, Loe and co-workers published their classic
work that demonstrated that gingival health could be reliablyachieved with immaculate oral hygiene and that gingivalinflammation could be caused by the aοcumulation of plaqueon the teeth. Light microscopiο examination of tooth scrap-ings revealed that plaque \ivas an adherent mat of bacteria,epithelial cells, and leukocytes encased in an amorphousprotein and polysaccharide matrix, and that cocci, filamen-tous bacteria, spirochetes, and vibrios accumulated on teethin an ordered sequence. The knowledge produced in this andlater studies of plaque morphology and microbiologyemphasied that plaque was a heterogeneous community ofbacteria (see Figure 2).
Generally speaking, bacteria assoοiated with periodontalhealth are characterized as Gram-positive, nonmotile faculta-tive anaerobes. Bacteria assoοiated with disease are gener-ally Gram-negative, motile, Strictly anaerobiο speοies. Τhecell wall of Gram-negative bacteria consists of a lipopolysac-charide base, aΙso known as endotoxin, that has significantpathogenic potential. νγhile over 350 distinct speοies ofbacteria have been isolated from the oral cavity, relativelyfew are associated with gingival or periodontal inflammation.The list of strongly associated pathogenic bacteria includes:
ο Actinobacillus actinomycetemcomitans
ο Bacteroidesforsythus
. Fusobacteriumnucleatum
. Peptostreptococcusmicros
o Porphyromonasgingivalis
o Prevotella intermedia/nigresens
What ls Meant by the Term "Biofilm"?
B
FIGURE 2. A thin section eleclron photomicrograph of supragingival plaque(biofilm) showing a heterogeneous popu|ation of resident bacteriaΙmorphοtypes and bacterial debris. τhe interbacterial matrix permits theexchange of nutrients between microorganisms.
-

I
I
ι
I
ET|oLoGY AND cLASslFlcATloN oF τΗE PERloDoΝτAL DlsEAsEs
Biofilms form on inert surfaces where bacteria to bacteriacohesive interactions or bacteria to surface adhesive interac-tions are allowed to occur. Biofilms are heterogeneouscomposites of bacterial communities within a nonbaοterialprotein, polysaccharide, and glycoprotein matrix of bacterialand salivary origin. The matrix allows for a "circulation" ofnutrients and baοterial metabolites betνveen communities andthe environment outside the biofilm. τhere are extreme varia-tions in oxygen levels ranging from highly aerobic areaswithin fluid channels to almost completely anaerobic areas inmicrocolonies.
What ls the "Nonspecific Plaque Hypothesis"?
The basic tenets of the nonspecific plaque hypothesis statethat inflammatory periodontal diseases (and possibly caries)are caused by composite effect of bacterial colonization andmaturation on the surfaces of teeth, not by specific bacteriathemselves. Gingival disease is the outcome from release ofbacterial metabolites (such as butyrate or other short chainfatty acids) and immunogenic bacteriaΙ antigen components,such as lipopolysaοcharide (endotoxin) from Gram-negativecell walls during plaque growth. lnflammatory disease is theoutcome of a microbial mass that is in excess of the localdefense mechanisms of the host.
What ls the "Specific PIaque Hypothesis"?
The specific plaque hypothesis states that periodontitis is aninfection caused by a limited number of periodontal microor-ganisms, and that these microorganisms characterize theplaque biofilms associated with periodontitis but not gingivitisor gingival health. lt appears that of the 300+ identifiablespecies found in the oral cavity, only a small proportion (10-12 species) are actually found in active periodontitis sites.
The bacteria believed to be pathogens in periodontitis do notconform to the classic dogma for microbial pathogenicity (ie,Koch's Postulates). The current understanding of mixedinfections, bacterial invasion, virulence factors, conducivebacteria habitats, the role of so-called "beneficial species",and the susceptibility of the host have rendered Koch'sPostulates obsolete when it comes to periodontitis.
What ls Meant by "Putative PeriodontalPathogen"?
The criteria for implicating oral microorganisms as perio-dontaΙ pathogens are:
1. The microorganism must be associated in high numbersin active periodontitis lesions and either absent (not culti-vable) or in low numbers in gingivitis or healthy sites. Thenumbers of the microorganism should have increased toa threshold level before the onset of disease.
2' Ιhe elimination of the microorganism, or its numericalreduction below threshold levels, should parallel remis-sion of active disease.
3. There should be a specific host immune responseagainst the organism (ie, elevated serum, salivary, andcrevicular fluid antibody titers).
4. The microorganism should evoke virulence factors thatcontribute to its pathogenicity or explain disease pathobi-ology.
5. The microorganism should produce periodontitis inanimal model systems.
What Features Do Most Periodontal PathogensHave in Common? What Are the Exceptions tothe Paradigm?
This smalΙ group of putative periodontal pathogens possessescertain features in common. Most of them have a Gram-negative cell wall. The outer membrane of the Gram-negativecell wall contain lipopolysaccharide (LPS) \Λ/hich has endo-toΧin activity (see Figure 3). Typically, LPS οontaining Gram-negative cell waΙl extracts are capable of promoting boneresorption, inhibiting osteogenesis, οhemotaxis of neutrophils,and other events associated with active periodontitis. Somepathogens release a LPS that suppresses the innate immuneresponse. Many periodontal pathogens are strict or faculta-tive anaerobes and are asaccharolytic, permitting survival inthe restricted ecosystem of the periodontal pocket. Amongthe strict anaerobes is the only presumptive periodontal path-ogen with a Gram-positive οell ν'ιall, Peptostreptococcusmicros.
F|GUHE 3- A terminaΙ outer membrane vesicle at the tip of Fusobacteriumnucιeatum. High concentrations of lipopolysaccharide (endotoxin) arepresent in the outer membrane of Gram-negative cell walls,
Actinobacill us actinomycetemcomitans and Porphyromonasgingivalis are the best studied and have been designated,along with Bacteroides forsythus, as true etiologic agents inperiodontitis because of the host of virulence they produceand their ability to invade gingival tissues. Prevotella inter-media/nigrescens and Fusobacterium nucleatum have beenwidely studied as well, and appear to satisfy all criteria forperiodontal pathogenicity. Because P. intermedia and strainsot F. nucΙeatum have also been found in areas of Severegingival inflammation without evidence of attachment loss,controversy exists as to their true periodontal pathogenicity.
Campylobacter rectus, Εikeneila corrodens, Εubacteriumspecies, SeΙenomonas species, enteric rods/Pseudomonasspeοies, and Treponema species satisfy some, but not all,criteria with any degree of confidence. Nonetheless, theyremain among the list of periodontal pathogens, and microbi-ology testing serviοes commonly report their presenceamong cultivable flora.
Relative risk values of periodontal pathogens in periodontalsites have emerged from archival reviews of data baseslocated in commercial testing facilities. The relative risk of a

CHAPτER 3
microorganism as a pathogen is often expressed as percentof total cultivabιe bacteria in a given culture. For example, thecultivability of A. actinomycetemcomitans at levels at orabove 0.01% indicates a periodontal site at risk for activedisease. The risk for P. gingivalis, C. rectus, P. intermedia,and P. micros in periodontal sites is 0.1%, 2%,2.5%, and 3"/",
respectively.
What ls Dental Calculus?
Dental calculus is mineraΙized, mature plaque covered on itssuface with nonmineralized plaque, material alba, desqua-mated epithelial cells, and formed blood elements. Thebacterial components are largely branched and unbranchedfilamentous microorganisms that are usually nonvital ordisplay minimal metabolic activity. These bacteria probablyplay a role in the mineralization of calculus as inorganic crys-tals are frequently found within and around microorganisms.Structurally, calculus retains much of the histologicmorphology of its plaque precursor.
Calculus may be classified as supragingival or subgingivalbased on location. lt may also be classified as salivary orserumal based on the source of inorganiο salts that comprisecalculus. Root calculus is usually more strongly adherent totooth surfaces than that found on enamel sudaces (seeFigures 4 and 5).
The inorganic components of calculus deposits are primarilyorganized into crystalline struοtures that vary according to theage of the deposit. For instance, in mature calculus (>6
months), the major crystalline structure is hydroxyapatite(Ca16[PO4]6(OH)r) with lesser amounts of octacalcium phos-phate (Cas[HPOa]a), whitlockite (Ca3[POo]r), and brushite(Ca[HPOo]2HrO). ln younger deposits (<3 months), brushitepredominates, but with progressive aging, octacalcium phos-phate, whitlockite, and finally hydroxyapatite become moreabundant.
FlGURE 4. A heavy deposit of suρragingival, salivary calculus on the buccaland occlusal surfaces of nonfunctional maxillary premolar and molarteeth.
Calculus deposits have also been desοribed as radiographi-cally apparent. The radiographiο detection of calculus is posi-tively influenced by the thickness of the deposit, the amountof surface area covered by the deposit, and the anatomy of
the tooth. Only 40% to 50% of calculus deposits will be radio-graphicaΙly apparent. Therefore, radiographs should notsolely be used to measure the presence or absence ofcalculus.
How Does Calculus Attach to Teeth? Do theAttachment Mechanisms Have Any ClinicalSignificance?
Calculus will attach to tooth suι'faces by several mechanisms.The most common mechanism of supragingival calculusattachment to smooth enamel surfaces is salivary pellicle,and it is usually easily removed using ultrasonic or handinstrumentation. The irregularities of unrestored caries anddefective dental restorations complicate the removal ofsupragingival calculus. The attachment of subgingivalcalculus is further complicated by microscopic irregularities incementum such as cementaι tears, cemental voids onceoccupied by Sharpey's fibers, resorption bays, and othersurfaοe cemental defects. lt is for these reasons that clini-cians will further designate calculus deposits as eithercoronal or radicular to reflect the relative tenaciousness ofradicular and coronal calculus, and in the οase of radicularcalculus, the difficulty they may have in achieving totalcalοulus removal during root planing.
FlGURE 5. serumnaι calculus deposits that have become supragingival due togingival reοession caused by advanced periodontitis. Note the moregeneralized distribution of the deposits with no apparent relationship orproximity to ma,or salivary ducts.
What ls the Pathogenic PotentiaΙ of Calculus?
The current view is that calculus exerts its pathogenic poten-tial as a contributing factor that fosters plaque formation andpromotes its retention on teeth. Also, there is little questionthat the microbiaΙ composition of calculus provides bacterialfactors that, by themseΙves, produce an inflammatory reac-tion in tissue. Bacterial οomponents (outer membrane vesi-cles containing LPS, cell \ivall material containing lipoteichoiοacids, periplasmic and cytopΙasmic enzymes, and bacterialmetabolic factors) are all suspect pathogenic factors in dentalcalculus. The persistent inflammation in gingival tissuepredictably seen adjacent to reasonably plaque free calculusis unequivocal evidence of the pathogenic effect of calculus.
17
-

EτloLoGY AND clAsslFlcAτloN oF τHE PEBloDoNτAL DlsEAsEs
F|GURE 6. τhe exposure of subgingival' serumnal calculus aΙter a period ofimproved plaque control. Marginal inflammation has been reduced buterythema and edema persist. τhis is the same patient as seen in Figure 1'
Aside from this, the rough surface of dental calculus isusually covered with a layer of plaque biofilm. Αs such,calculus tends to "present" plaque to periodontal soft tissuesand interfere vvith efforts to improve plaque control. The phys-ical removal of dental calculus remains a critical componentof mechanical periodontal inflammatory disease control.
What Are the Risk Factors for PeriodontalDiseases? What ls Meant by "Risk"?
The expression risk in this context means that, in the pres-ence of a given factor, injury to or loss of periodontal tissue isa possibility. Risk factors may be local or systemic in nature.
Local contributing factors to the etiology of periodontaldiseases fall into two general categories: Anatomic or iatro-genic. They share in common their ability to either facilitatebacterial plaque, and therefore calculus, accumuΙation/reten-tion or their ability to interfere with plaque/calculus removal.
Τhe loca| anatomic risk factors include:
1. Furcation anatomy. ln many instances, the entranceof bifurcations or trifurcations is restricted enough tolimit access for mechanical root instrumentation.once access to the intrafurcaΙ space has beenachieved, concavities in the furcal aspects of molarroots wiΙl limit instrumentation as well (see Figure 7).
2. lntermediate bifurcation ridges extending from themesial furcation surfaοe of the distal root across theroof of the bifurcation to the distal sudace of themesial root of mandibular molars. Τhese commonanatomic deformities interfere with a patient's abilityto effeοtively remove plaque biofilm.
3. Cervical enamel projections (CEP). CEPs are toothdevelopmental deformities of the CEJ found onmolars. They are classified according to their involve-ment in tooth furcations. Α Grade l CEP presents withminimal projection of enamel tov/ard the entrance of
the furcation. Α Grade ll οEP approximates theentrance of the furcation, and the tip of a Grade lllCEP is well within the furcation (see Figure 8).
FlGURΕ 7. A maxiΙlary moΙar displaying a buccal to distal furcation invasionwith a Nabers probe in place. The narrowness of the furcation entrancesand the tortuousness of the furcation invasion mitigate against access forscaling and root planing. (Courtesy of Dr. Jeanne Salcetti)
F|GURE 8. A human dried maxilla with a grade ll cervical enamel proiΘction(cEP) in the buccal furcation of the maxilΙary sΘcond molar. τhe cEPcould have been partially responsible tor the furcation invasion and local-ized severe bone loss around the tooth.
4. Palato-gingival grooves (PGG). PGGs are toothdevelοpmenta| deformities of maxilΙary central andlateral incisors. They begin in lingual piis and extendvertically onto root suιJaces. PGGs could, on rareoccasions, extend to the root apex. PGGs arecommonly associated with increased gingival inflam-mation, plaque aοcumulaiion, and probing depth (seeFigure 9).

CHAPτER 3
FlGURE 9. A palatogingival groove on a maxillary lateral incisor. τhe gfoovecouΙd have been partially responsible for the sΘvere attachment lossaround the tοoth. Note that because of its loss of support, the lateralincisοr has undergone pathologic migration.
5. Open contacts and food impaction. Open contactsbetween teeth may be anatomical in origin, iatrogenicin origin, or be due to caries and pathologic migrationof periodontally involved teeth. Food impaction isdefined as the forceful wedging of food betweenteeth. Any other accumulation of food or food debrisaround teeth should be categorized as food retentionand is probably less threatening to the periodontium.Food impaction and subsequent retention maycontribute to root caries in individuals who do notperform proper oral hygiene interdentalΙy. opencontacts by themselves probably do not contribute toperiodontal pathology, but, in the presence of foodimpaction, open contacts have been associated withperiodontal destruction. This may be particularlynoticeable in periodontitis cases where the progressof disease is in its early stages or particularly obviouswhere periodontitis is isolated to sites of opencontacts/food impaction.
F|GURE 10. surgical exposure of an anomalous maxillary first moΙar. Thepalatal root is bifurcated and the distopalatal root curues into the mesialfurcation of the second molar. on the bucca| aspect, the mesiobuccaΙroot of the second molar is in close approximation to the distobuccal rootof the first molar. Access for effective scaling and root planing isextremely limited.
6. Other anatomic risk factors of potential etiologicimportance are: The width of the space betweenteeth and root proximity (so-called "kissing roots").
The iatrogenic risk factors are:
1. Overhanging dental restorations. Since dentalrestorations remain the mainstay of dental practice, it
is not surprising that overhanging dental restorationsare arguably the most common form of iatrogeny toaffect marginaΙ periodontal health (see Figure 11).Overhanging and improperly placed dental restora-tions can be physicaΙly irritating' be pΙaque retentive,foster the growth of periodontal pathogens, alter themorphology of the interdental space, and violate thedentogingival junction (see 2 below). By virtue of theirroughness and overall bulk, they may also interfere\ivith interdentaι plaque control.
FIGURE 11. A maxillary first molar with a mesial amalgam overhang thateπends into the furcation. lt is probable that the preparation Ιor thisrestoration impinged upon the biologic width. Note how the attachmentlevel on the tooth parallels the extension of the overhang onto thecementum and into the furcation.
Violation of the "biologic width". After overhangingrestorations, iatrogenic invasion of the biologic widthmay be the next more serious insult to the periodon-tium a dentist can make. The impact of this insult isusually permanent as the margins of dental restora-tions are inevitably placed in the wake of the insult.The biologic width is one of nature's constant dimen-sions. lt is most constant within individuals and lessconstant bet\Λ/een individuals. lf it is injured, it willrepair. lf however, restorative materials render theinvasion of the biologic width permanent, periodontitiswilΙ produce apical migration of the .iunctional epithe-lium, resorption of crestal alveolar bone, loss of perio-dontal attachment, and possible vertical osseousdefeοts (Figure 1 1). Α new bio|ogic width will repair afew mms apical to its original position on the tooth.This represents a net loss of attachment on the tooth.
Open contacts and food impaction related toinadequate restorative dentistry. The impact offood impaction through open contacts created by
2.
3.
Ξ

EτloLoGY AND clAsslFlcAτloN oF τHE PERloDoNτAL DlsEAsEs
4-
5.
iatrogeny offers the same threat to the periodontiumas food impaοtion associated with open contacts thathave resulted from growth and development orocclusal \Λrear.
Occlusal traumatism associated with inadequatedentistry in 1, 2, and 3 above.
Additional local iatrogenic risk factors for perio-dontal diseases include: Removable partial 2.dentures and overdentures, fixed bridges, removal ofthird molar teeth in older adults, placement of fixedorthodontic appliances, and orthodontic movement ofperiodontally involved teeth.
Uncontrolled diabetics, poorly controlled diabetics, ordiabetics whose control is unknown should onlyreceive emergency periodontal therapy, and thattreatment should be performed \,vith intraproceduraland/or postoperative antibiotic coverage. Thepatient's physician may also prescribe insulin or otherantihyperglycemic agents to help limit post-operativeinfections or complications in wound healing.
Ηlv/AlDs. Given the immunosuppressed state ofthese individuals (decreased CD4 lymphocytes), anexpectation for severe periodontitis in patients withHIV/AIDS is reasonable. lndeed, these individualssuffer from other bacterial, viral, and fungal diseasesmore than those νvithout HIV infection. Manysucοumb to these infections. Early studies of the peri-odontal status in AIDS patients indicated that theseindividuals showed increased severity of periodontaldiseases. H|V-gingivitis (linear erythema) and HIV-periodontitis (necrotizing ulcerative periodontitis)categories of periodontal diseases were quicklyproposed to designate the unique cΙinical characteris-tics of periodontal diseases in this group. RecentΙy,the issue has been challenged by those who reportno increases in the prevalence or extent of perio-dontal diseases among HlV-positive individuals.
Smoking. Due to the vasoconstrictor effect of nico-tine and the paralysis by carbon monoxide on theability of hemoglobin to transport oxygen, it is under-standable that smoking is a serious environmentalrisk factor for periodontal diseases. The length of timean individual has been smoking and the frequency ofsmoking play contributory roles in the severity of peri-odontal disease in smokers. Smokers also have agreater accumulation of plaque and οaΙcu|us thannonsmokers and may be more at risk to harbor perio-dontal pathogens.
While probing depth reduction following conventionalnonsurgical and surgical periodontal therapy hasbeen reported in smokers, the amount of reductionhas been reported as less than that achieved innonsmokers. A growing body of evidence suggestsstrongly that the failure rate of implant therapy ishigher in patients who smoke. lt is not uncommon fora therapist to recommend against the placement ofdental implants in smokers. Patients must be coun-seled in this regard and supported in their attempts toovercome their addiction.
Sex hormone imbalances. The most notablechanges in the periodontium that are affected in partby hormonal changes occur in \Λ/omen in their child-bearing years. ln the case of pregnancy, proges-terone and estrogen levels increase to levels that areseveral orders of magnitude greater than those seenduring a normal menstrual cycle. Varying degrees ofa reversible "pregnancy gingivitis" are commonduring pregnancy. The biologic impact of hormonechanges range from the release of inflammatorymediators that increase vascular permeability (pros-taglandins), the alterations in immunoregulation andpro-inflammatory reguιators, the imbalances in thefibrinolytic system, and the abundant growth of theperiodontal pathogen, P. intermedia. Because theduration of pregnancy is relatively short, hormonalchanges associated with pregnancy have little effecton the more irreversible progress of periodontitis.
What Are the Systemic Diseases and/orConditions That Are Contributing Factors forPeriodontal Diseases?
Aside from the medications that affect the clinical presenta-tion of plaque-induced gingival diseases (nifedipine forcontrol of hypertension, phenytoin for control of epilepticseizures, and cyclosporine to control organ transplant rejec-tion), most systemic diseases and conditions that may affeοtperiodontal diseases generally alter host barrier and hostdefense mechanisms. The impact of diminished host suscep-tibility, along with the diverse virulence mechanisms invadingmicroorganisms possess, help to explain the individual varia-tions in periodontal disease patterns \Λ,e See in systemically ill
periodontal patients. An assessment of systemic contribu-tions to periodontal diseases in our patients is critical to perio-dontal diagnosis and/or treatment planning.
The systemic diseases and conditions that commonly affectperiodontal diseases are: Uncontrolled type I and type lldiabetes mellitus, HIV/AIDS, hormone imbalances, geneticpredisposition, medications, smoking, and malnutrition.
1. Diabeιes mellitus. Diabetes mellitus (DM) isatfecting a growing number of Americans. The inci-dence of the disease seems to vary according toethnic origin, but it is estimated that 5% to 10% ofindividuals in the United States are affected withdiabetes. DM is an aberration in carbohydrate, lipid,and protein metabolism. Most of the morbid compli-cations of DM stem from longterm impaired glucosemetabolism. The characteristic hyperglycemia ofuncontrolled DM is the basis for most of the vascular,cellular, and immune changes assoοiated with thedisease.
Epidemiologic data has made clear associationsbetween increased severity of periodontal diseasesand uncontrolled type I and type ll diabetes mellitus.Type I and type ll uncontrolled diabetics tend topresent with more gingiva! inflammation, more loss ofperiodontal attachment, and radiographic evidence ofmore bone loss than controlled or nondiabetic individ-uals. There is agreement that periodontal patientswhose DM is welΙ controlled may receive periodontaltherapy without restriοtions' incΙuding periodontalsurgery and implant placement.
3.
CHAPτER 3
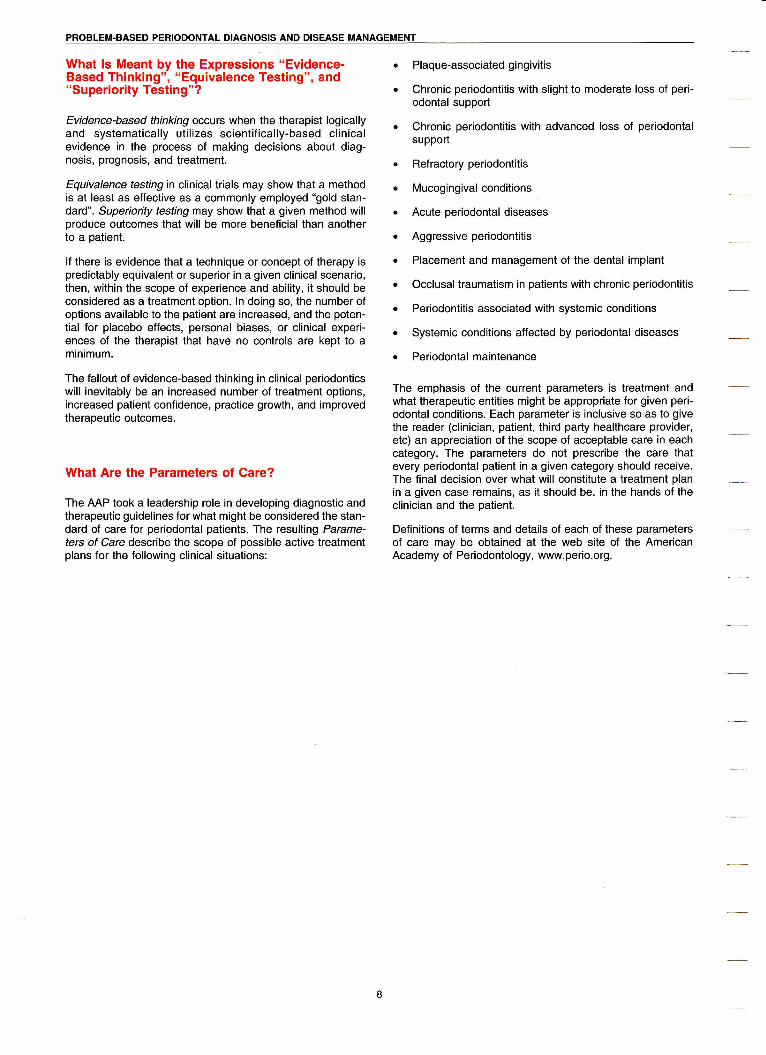
Oral contraceptives mimic the hormonal levels seenduring pregnancy, and it is not uncommon to findpregnancy-like changes in patients using birth οontrolpills (BCP). Because gingivaΙ sex hormone concen-trations tend to be lower during normal menstruation,it is not unexpected that women in their childbearingyears may present with "cyclic" episodes of increasedgingival inflammation.
F|GURE'12. τhis lesion is a pyogenic granuloma in a 17-year-oιd femaΙepatient as a result in changes in sex hormone levels and plaqueaccumuιation.
The most important οoncern of the dentist inmanaging patients who present with gingival diseaserelated to hormone imbalances is to be certain thatinflammatory disease control measures are effective(Figure 12).
This is particularly important in women who are preg-
nant because data exists to suggest a relationshipbet\Λ/een periodontal infections (periodontitis) andpreterm low birth weight babies. Antibiotiοs should beused only after a medical consultation in patients whoare pregnant. Although οontroversial, there arereports of decreased effectiveness of oral οontracep-tives in individuals taking certain antibiotics. lndivid-uals who are taking BCPs should be advised that theuse of prescribed antibiotics such as tetracyclinesand some penicillins may interfere with the action ofBCPs. To avoid unwanted pregnancy, these individ-ua|s should be so warned and use aΙternativemethods of birth control \ivhile taking antibiotics.
5. Genetic predisposition for periodontal diseases.There is general agreement that individual responsesto plaque bacteria vary. lt has been suggested thatdisease pattern variations could be based, in part, onunderlying genetically based differenοes in immunefunction. lndeed, the association of:
a. Neutrophil receptor defects
b' Αntibody responses (lgGr) to periodontal patho-gens
c. οertain histoοompatibility antigens (HLΑ)
d. Lymphocyte immune regulatory defeοts in patientswith aggressive periodontitis adds credibility to thisconοept.
Studies in twins indicate that many of the clinicalvariations seen in chronic periodontitis can be attrib-uted to individual genetic differenοes. Recent reportsof genetic pleomorphism in lL-1 genes and theelevated production of proinflammatory mediators,such as lL-1 , add another dimension to the impactgenetic variations among individuals have on thepatterns of chronic periodontitis.
-

EτloLoGY AND cLAsslF|cATloN oF TΗE PERIoDoNτAL DlsEAsEs
CLASSIFICATION OF PERIODONTAL DISEASES
Concepts about the etiology, pathogenesis, and treatment ofthe periodontal diseases have changed significantly over theyears. Ne\Λ/ levels of understanding are reflected in the clas-sification systems for these diseases and conditions. Thet\Λ/o most recent widely accepted classification Systems ofthe periodontal diseases and conditions were developed in1989 and 1999. The current system, more comprehensivethan any of its predecessors, is admittedly still a work inprogress.
Ηoνv Has the Understanding of PeriodontalDiseases Changed Over the Years?
For many years, the periodontal diseases were thought of asdegenerative diseases. Early confirmation of the role ofbacterial plaque in the initiation and progression of gingivitiswas only presented in the 1960s. Since that time, many ofthe earlier tenets have fallen by the wayside. Currently, it isclear that both gingivitis and periodontitis in their variedforms are caused by the accumulation of a bacterial plaquebiofilms on the teeth and in the subgingival area, the hostresponse to that aοcumulation, and the various systemic andlocal factors that may affect the host response. lt is also clearthat only a relatively few bacteria are associated with inflam-matory periodontal disease. The exact role of these bacteria,their relationship with each other and their interaction withthe immune system in the initiation and progression ofdisease is still not clearly understood. There also appears tobe a genetic component to the initiation and progression ofdisease in some patients. At this iuncture, controlling theacοumulation of plaque is the first line of defense inpreventing disease, no matter what other factors may bepresent.
What ls the Difference BetιΛreen Gingivitis andPeriodontitis?
FlGURE '|3. Gingivitis in a 12-year-old female. τhe severe gingivitis was due tothe interaction of increased levels of progesterone and plaque.
Gingivitis is inflammation of the gingival tissues in theabsence of οlinical attachment loss (Figure 13). lt may beοharacterized by edema, erythema, increased gingivaltemperature, and oοcasionally pain. As the inflammation andloss of connective tissue is confined to the soft tissues, teethare not in jeopardy of being lost. Gingivitis is ordinarily
reversible with appropriate therapy. Periodontitis is infΙam-mation that affects and destroys the attachment apparatus(Figure l4). The histology is marked by apical migration ofthe junctional epithelium from the οementoenamel junction,Ιoss of connective tissue attachement, loss of periodontalΙigament, and destruction of bone. lncreased probing depthsmay occur or the gingiva may recede as attachment is lost.Continuation of this loss of attachment will eventually lead tothe loss of the tooth. The progress of periodontitis may bearrested \Λ/ith proper therapy. ln certain Situations, lostattachment apparatus may be surgicaΙly regenerated.
FIGURE 14. Periodontitis in a 37-year-old male. Note the significant calculusand plaque accumulations, severe gingival inflammatiοn, and recessionassociated with the mandibular anterior teeth.
What ls the "Traditional" Classification of thePeriodontal Diseases?The 1989 World Workshop in Clinical Periodontics recom-mended the following categories of periodontitis. This systemiS the one most familiar to a majority of cliniοians'
l. Αdult periodontitis
ll. Early-onset periodontitis
A. Prepubertal periodontitis1. Generalized2. Localized
B' JuveniΙe periodontitis1. Generalized2. Localized
C. Rapidly progressive periodontitis
lll. Periodontitis associated with systemic disease
lV. Necrotizing ulcerative periodontitis
V. Refractory periodontitis
One of the generally accepted classifications for gingivitisvι/as:
l. Plaque-associated gingivitis
ll. Αcute necrotizing ulcerative gingivitis (ANUG)
lll. Hormonal gingivitis
lV. Drug-induced gingival overgrowth
V. Desquamative gingivitis (associated with vesiculo-bullous diseases)

CHAPτER 3
During the ensuing decade, it \Λ/as determined that thisdisease classification system exοluded many of the diseasesand conditions of the periodontium that clinicians andresearοhers confront on a dai|y basis. Further work wasnecessary to develop a neνv, more inclusive system.
VVhat Is the 1999 Classification of PeriodontalDiseases?
The American Academy of Periodontology convened the1999 lnternational Workshop for a Classification of Perio-dontal Diseases and Conditions to reassess the diseaseclassification system that \ivas developed by the 19B9 νvorldWorkshop in Clinical Periodontics. Based on current knoννΙ-
edge and philosophies, a more comprehensive classificationsystem of diseases and conditions that affect the periodon-tium \Λ/as proposed. Major οhanges include the addition of asection on gingivaΙ diseases, changing the names of adultperiodontitis to chronic periodontitis, early onset periodontitisto aggressive periodontitis, and the elimination of refractoryperiodontitis as a distinct disease class. Periodontitis as amanilestation of systemic disease has been further clarified,new categories added on periodontal absοesses, perio-dontic-endodontiο lesions, and the developmental oracquired deformities and conditions, and the replacement ofnecrotizing ulcerative periodontitis with necrotizing perio-dontal diseases.
l. Gingival Diseases
A. Dental Plaque-lnduced Gingival Diseases.l . Gingivitis associated with dental plaque only
a. Without Ιocal contributing factors (Figure 15)
FIGURE 15. Gingivitis associated with dental plaque only. Note that thegingival inflammation is worse on the maxillary left side than theright side. τhis may be relatθd to the hand with which the patientbiushes his teeth. As the patient turns his hand to maneuver thebrush, the lateral incisor and canine are ofιen missed.
b. V/ith local contributing factors
2. GingivaΙ diseases modified by systemic factors
a. Αssociated with the endocrine System
1. Puberty-associated gingivitis (Figure 16)
FIGURE 16. Puberty-Associated Gingivitis. τhis is related to the patient inFigurΘ 13.
2. Menstrual cycle-associated gingivitis
3. Pregnancy-associated
- Gingivitis
- Pyogenic granuloma (see Figure 12)
4. Diabetes mellitus-associated gingivitis
b. Associated with blood dyscrasias
1. Leukemia-associated gingivitis
2. Other
3. Gingival diseases modified by medications
a. Drug-influenced gingival diseases
1. Drug-influenced gingival enlargements(Figure 17)
FlGURE'17Α. Drug-lnfluenced Gingival Enlargements. Gingival enlarge-ment due to phenytoin the,aPy.
23
-

EτloLoGY AΝD cLAsSlFlcATloN oF THE PER|oDoΝTAL DlSEASES
FIGURE 178. Drug-lnfluenced Gingivat Enlargements. Gingival enlarge-ment due to nifedipine therapy superimposed on chronic periodon-titis.
2. Drug-influenced gingivitis
- Oral contraceptive-associatedgingivitis
- Other
4. Gingival diseases modified by maιnutrition
a. Αscorbiο acid-deficiency gingivitis
b. Other
B. Nonplaque-lnduced Gingival Lesions
1. Gingival diseases of specific baοterial origin
a. Νeisseria gonorrhea-associated lesionsb. Treponema pallidum-associaied lesionsc. Streptococcal species-associated lesionsd. Other
2. Gingival disease of viral origin
a. Herpesvirus infections
1. Primary herpetic gingivostomatitis
2' Reοurrent oraΙ herpes (Figure 1B)
FIGURE 18A. Recurrent Oral Herpes. General herpetic outbreak on thegingival tissues.
F|GURE 188. Recurrent oraι Herpes. Herpes outbreak localized to oneside of the hard palate several days after periodontal surgery on thesame side ot the maxilla.
- VaricelΙa-zoster infectionS
b. Other
3. Gingival diseases of fungal origin
a. Candida-sρecies infections
- Generalized gingival candidiasis
b. Linear gingival erythema (Figure 19)
FIGURE '19. Linear Gingival Erythema. Seen in some HIV+ patients.
ο. Ηistoplasmosis
d. Other
Gingival lesions of genetic origins
a. Ηereditary gingival fibromatosis
b. Other
Gingival manifestations of systemic conditions
a. Mucocutaneousdisorders
5.

CΗAPτER 3
'1 . Lichen planus (Figure 20)
F]GURΕ 20. Erosive Lichen Planus. Ιn its ulcerative form, this diseasecan be quite painful for the patient.
2. Pemphigoid (Figure 21)
fe #j
FlGURΕ 21Α. Benign Mucous Membrane (cicatricial) Pemphigoid. A posi-tive Νikolsky sign is seen over the maxillary right lateral incisor.τhis indicates that a vesiculobullous disease is present.
FlGURE 21B' Benign Mucous Membrane (cicaιricial) Pemphigoid. lmmu-notluorescence contirms the diagnosis ot pemphigoid.
3. Pemphigus vulgaris
4. Erythema multiforme
5. Lupus erythematosus
6. Drug induced
7 " Other
b. Αllergic reactions
1. Dental restorative materials
- Mercury
- Nickel
- Acrylic- Other
2. Reactions attributable to
- Toothpastes/dentifriοes
- Mouthrinses/mouthwashes
- Chewing gum additives
- Foods and additives (Figure 22)
3. Other
FlGURΕ 22Α. Allergic Reactions Attributable to Food. This patientpresented With severe gingival infΙammation associated with perio-dontal disease. The patient had no history or cΙinical findingssuggesιive of sysιemic disease.
9q
FΙGURΕ 22B' AΙlergic Reactions Atlributable to Food' After contrοl oflocal factors, there was still a signiricant amount of inflammation.
-

EτloLoGY AND cLAsSIFlcAT|oN oF τHE PER|oDoNTAL DlsEAsEs
FIGURE 22C. Allergic Reactions Attributable to Food. An incisionalbiopsy revealed a diagnosis of plasma ceΙl gingivitis (allergic reac-tion)-
FIGURE 22D. Allergic Reactions Attributable to Food. After eliminatingcurry peppers from her diet, this patient's gingiva returned tohealth.
6. Traumatic lesions (factitious, iatrogenic, acci-dental)- Chemiοal injury- Physical injury- Thermal injury
7. Foreign body reaction8. Noi other\ffise specified (NOS)
ll. Chronic Periodontitis (Figure 23)-
FlGURΕ 23Α. Generalized chronic Periodontitis. A' ln spite of significantplaque and calculus accumulations in the mandibular arch, ιhispalient had minimal gingival intlammation.
FiGURE 23B. Generaιized chronic Periodontitis. τhe right buccalsegment showed minimal soft tissue infΙammation buι probe depthsranged from 7-10 mm.
FlGURE 23c. Generalized chronic Periodontitis. τhe radiographsshowed significant bone loss in this area.
F|GUΗΕ 23D. Generalized chronic Periodontitis. once a full thicknessmucoperiosteal flap was reflected, the extent of bone loss wasapparent.
Α. LocalizedB. Generalized
26
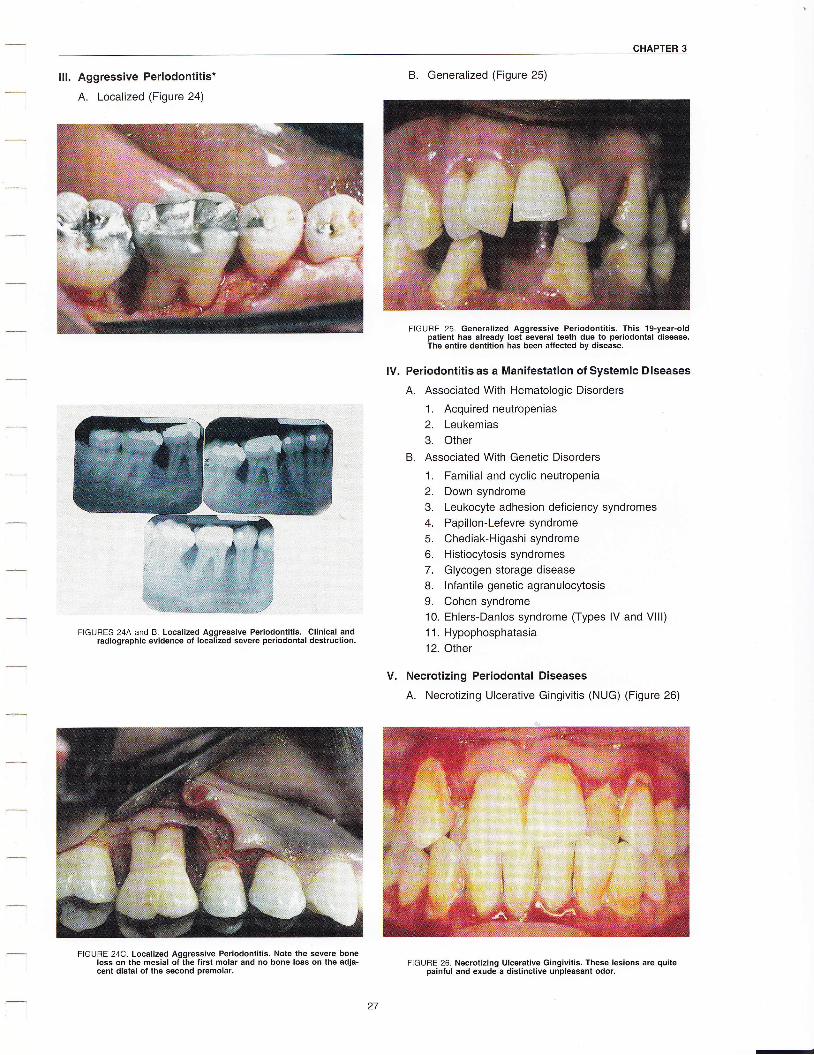
CHAPτER 3
ll!. Aggressive Periodontitis*
A. Localized (Figure 24)
FιGURES 24A and B. Localized Αggressive Periodontitis. clinical andradiographic evidence of localized severe periodontal destruction.
FlGURΕ 24ο. Localized Aggressive Periodontitis. Note the severe boneloss on the mesial of the tirst molar and no bone loss on the adia-cent distal of the second premolar.
B. Generalized (Figure 25)
FΙGURE 25. Generalized Aggressive Periodontitis. τhis 1g-year-oldpatient has already lost several teeth due to periοdontal disease.τhe entire dentition has been affected by disease.
Periodontitis as a Manifestation of Systemic Diseases
Α. Αssociated With Ηematologic Disorders
1. Acquired neutropenias2. Leukemias3. Other
B. Αssociated With Genetic Disorders
1. Familial and οyοιic neutropenia2. Down syndrome3. Leukocyte adhesion deficiency syndromes4. Papillon-Lefevre syndrome5. Chediak-Higashisyndrome6. Histiocytosis syndromes7. Glyοogen siorage disease8. lnfantile genetic agranulocytosis9. Cohen syndrome10. EhΙers-Danlos syndrome (Types lV and VlΙl)1 1. Hypophosphatasia12. Other
Necrotizing Periodontal Diseases
Α. Necrotizing Ulcerative Gingivitis (NUG) (Figure 26)
FlGURΕ 26. Νecrotizing Ulceraιive Gingivitis. These lesions are quitepainful and exude a distinctive unpleasant odor.
tv.
v.
-
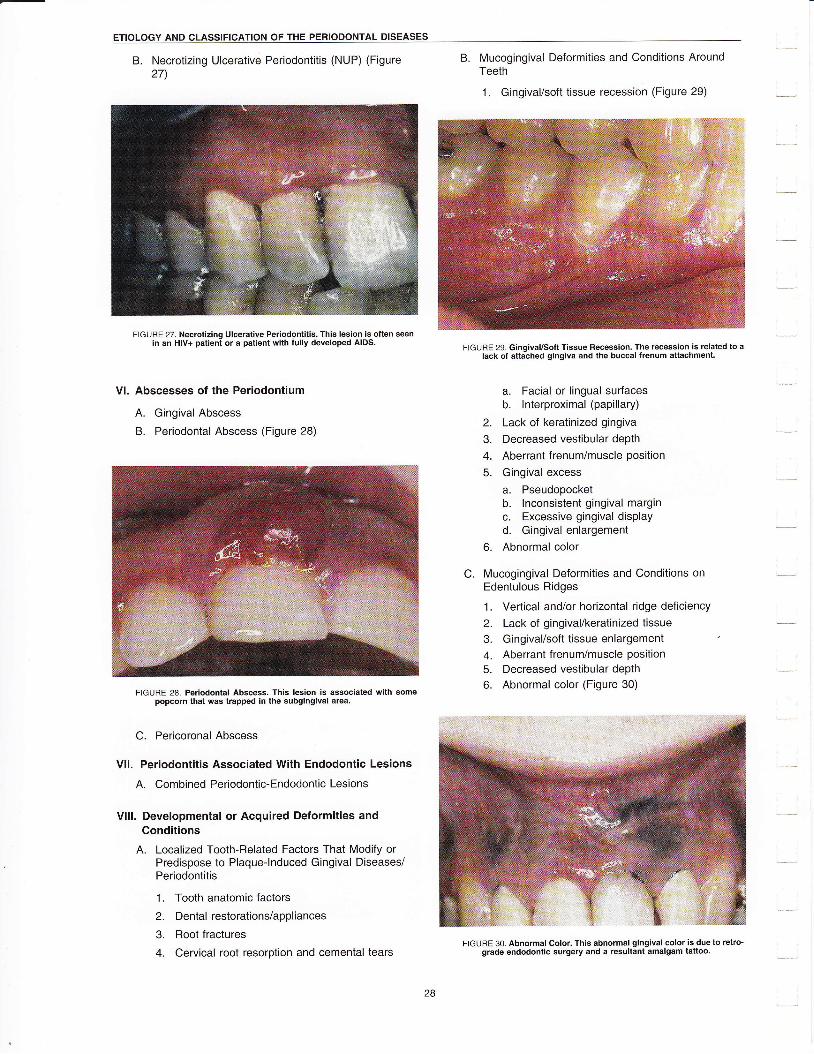
EτloLoGY AΝD cLAsslFιcAτloN oF THE PΕRloDoNτAL D|SEASES
B. Necrotizing Ulcerative Periodontitis (NUP) (Figure27)
FlGURE 27. Necrotizing Ulcerative Periodontitis' τhis lesion is often seenin an Hlv+ patient or a patient with fully developed ΑlDs.
Vl. Abscesses of the Periodontium
A. Gingival Abscess
B. Periodontal Αbscess (Figure 28)
FiGURE 28. Periodontal Abscess. τhis lesion is associated with somepopcorn that was trapped in the subgingival area.
C. Pericoronal Abscess
Vll. Periodontitis Associated With Endodontic Lesions
Α' Combined Periodontic-Endodontic Lesions
Vlll. Developmental or Acquired Deformities andConditions
A. Localized Tooth-Related Factors That Modify orPredispose to Plaque-lnduοed Gingival Diseases/Periodontitis
1. Tooth anatomic factors
2. Dental resiorations/appliances
3. Root fraοtures
4' Cervical root resorption and οemental tears
B' Muοogingival Deformities and Conditions AroundTeeth
1. GingivaΙ/soft tissue recession (Figure 29)
F|GURE 29. Gingival/soft Tissue Recession. τhe recession is related to alack οf attached gingiva and the buccaι frenum altachment.
a. Facial or lingual surfacΘsb. lnterproximal (papillary)
2. Lack of keratinized gingiva
3. Decreased vestibular depth
4. Αberrant frenum/muscle position
5. Gingival excess
a- Pseudopocketb. lnconsistent gingival marginc. Excessive gingival displayd. Gingivalenlargement
6. Abnormal color
C. Mucogingival Deformities and Conditions onEdentuΙous Ridges
1. Vertical and/or horizontal ridge deficiency
2. Lack of gingival/keratinized tissue3. Gingival/soft tissue enlargement
4. Aberrant frenum/muscle position5. Decreased vestibular depth
6. Abnormal color (Figure 30)
FTGURE 30. Abnormal Color. This abnormal gingival color is due to retro-grade endodontic surgery and a resultant amalgam tattoo.
CHAPτER 3
D. occΙusal Trauma
1. Primary occlusal trauma2. Secondary occlusal trauma
"Cases of chronic and aggressive periodontitis may begenerally described by the extent and severity of thedisease. Localized disease would be <30o/o of sites involvedand generalized disease as >30% of sites involved. Slightdisease would have 1-2 mm of clinical attachment loss(CAL), moderate disease 3-4 mm CAL, and severe disease>5 mm CAL.
What Are Some of the DistinguishingCharacteristics of the New Classifications ofGingivitis?
Gingivitis associated νιrith dental plaque only. As thename implies, bacterial plaque must be present to initiate thegingival infΙammation. This inflammation may be character-ized by changes in gingival color, contour, and possiblyconsistenοy; slight elevation of intrasulcular temperature;bleeding on gentle probing; an increase in gingival crevicularfΙuid flow (now as an exudate); and the inflammation isconfined to the soft tissues. Local factors may include resto-ration overhangs, open contacts, and other plaque traps andimpediments to good oral hygiene.
Gingival diseases modified by systemic factors:Pubefiy-associated gingivitis, menstrua! cycle-associ-ated gingivitis, and pregnancy-associated gingivitis.These conditions are all associated with changes in steroidhormone levels, primariΙy progesterone and estrogen. Τheyhave been associated with increased levels of Prevotellaintermedia in the infΙamed sites. ln puberty-associated gingi-vitis, the inflammation may be exaggerated even with appar-ently minimal amounts of plaque. Menstrual cycle-associatedgingivitis may appear in a very mild form. lncreased gingivalcrevicular fluid flow has been seen in a majority of subjectsduring ovulation. Pregnancy-associated gingivitis hasperhaps the most radical changes, \rvith the possible appear-ance of a pyogenic granuloma. lt is an extreme response togingival inflammation, characterized as a painless protuber-ance of the gingiva that bΙeeds readily at slight provocation.
Gingival diseases modified by medications. There arethree major drugs that can induce an overgro\Λ/th of gingivaltissues. Phenytoin is used as an antiseizure medication,nifedipine and several of the other calcium channel blockersare antihypertensive/antiarrhythmic drugs, and cyclosporineΑ is an immunosuppressant. overgrowth appears to berelated to the level of plaque accumulation. Approximately50% of phenytoin patients are susceptible to this overgro\,νth.lt has been estimated Ιhat 2o"/" of patients on calcium_channel blockers, and 2O/" to 30% of patients on cyclo-sporine A are susceptible to drug-induced gingival over-growth.
Nonplaque-induced gingival lesions. Many of theselesions are relativeΙy rare with the exception of the herpes-virus and Candida infections. Herpesvirus infections must becautiously treated due to their contagious nature \Λ/hile thelesions are shedding virus. Treatment must be deferredνvhen the patient presents with a weeping lesion. Candidainfections may be problematic if there is no apparent cause(reοent antibiotic use' illness) for the infeοtion. Candidaintec-tions have a high association \r/ith human immunodeficiency
virus (HlV) infection, so a thorough patient work-up may benecessary in the face of an unexplainable Candida infection.
Gingival manifestations of systemic conditions. Muco-cutaneous disorders: These disorders include the dermato-logic/autoimmune diseases of lichen planus, pemphigoid,pemphigus vulgaris, erythema multiforme, lupus erythema-tosus, and drug-induced disorders. These disorders at onetime were classified as desquamative gingivitis, a descriptiveterm signifying desquamation or falling away of the surfaceepithelium of the gingiva. These disorders are actually auto-immune in nature with no clear etiology. lt is critical that adefinitive diagnosis be obtained, for while they all may havea similar appearanοe, pemphigus has a higher morbidity,while the mucocutaneous disorders are difficult to managefor patient comfort.
Gingival manifestations of systemic conditions: Lineargingival erythema. This lesion is characterized by a brighterythematous margin of the free gingiva. lt is associated withimmunosuppression, particularly ΗlV infection. Theerythema does not resolve with the removal of plaque.
Gingival manifestations of systemic οonditions: Aller-gies' Αllergic reactions may take on a Variety of forms frommild erythema and edema to severe inflammation to anapparent lichenoid appearance. The challenge is to be surethat the inflammation is not plaque related. A diagnosis ofplasma cell gingivitis may be made by biopsy. The allergenmust then be identified and, if possible, eliminated from theoral cavity. Allergens incΙude amalgam, base metals used infixed prosthodontics, flavoring agents in dentifrices andcheνving gum' chili peppers, and other foodstuffs. lt may bedifficult to identify the offending agent. Changes must bemade one at a time, often a time-consuming process, inorder to identify the allergen.
What Are Some of the DistinguishingCharacteristics of the New Classifications ofPeriodontitis?
The new classifiοation system for periodontitis is moredescriptive and not temporal as νvas the previous system.The terms adult, juvenile, early onset, and prepubertal havebeen replaced with various forms of chronic and aggressivedisease. ln addition, many periodontal conditions that νverenot addressed in any previous classification system havebeen described. The term refractory periodontitis has beenremoved as a distinct disease entity, as the current thinking isthat any type of periodontitis may be refractory.
Chronic periodontitis. As the name implies, this type ofperiodontitis has a relatively long-standing history in apatient. This disease is characterized by relatively slowprogress, loss of attachment and underlying bone withincreased pocket depth. lt may have periods of rapid attach-ment Ιoss foΙlowed by prolonged periods of inactivity. Ιt isrelated to the presence of plaque and calculus, \ι/ith a varietyof associated bacteria involved. There may be modifyinglocal factors, such as restorative overhangs, food impaction,or open contaοts, and systemic factors, such aS uncontrolΙeddiabetes mellitus or cigarette smoking. Most often, chronicperiodontitis is responsive to mechanical therapy. lt is nolonger referred to as adult periodontitis as this disease may,albeit rarely, be seen in οhildren.

EτloLoGY AND clAsslFlcAτloΝ oF τHE PER|oDoNTAL DlsEASEs
Aggressive periodontitis. This category replaces whatused to be known as the early-onset periodontal diseases.Localized aggressive periodontitis replaces the older term,juvenile periodontitis, that is manifest by rapid and severeattachment loss in the incisor and permanent first molarregions. Actinobacillus actinomycetemcomitans is assoοi-ated with a majority of cases. Τhese patients have shownabnormalities in neutrophil function that may be related to ahyperimmune effect of their macrophages. This type ofaggressive periodontitis has a fairly clear inheritance pattern.
Τhe loοalized ρattern affects 14 or fewer teeth, mostlyconfined to the incisors and first molars. The generalizedform of aggressive periodontitis, formerly known as rapidlyprogressive periodontitis, affects 15 or more teeth withpossible immunologic changes as well. lt is characterized byepisodic, rapid, and severe attachment loss. At times, thisdisease may be difficult to control.
Periodontitis as a manifestation of systemic diseases.\Λ/ith the exception of Down syndrome, most of the listedgenetic disorders are relatively rare. τhe Down syndromepatient is a challenge because of the difficulty in maintaininggood oral hygiene. The prevalence and severity of periodon-titis is high compared to unaffected siblings, and attaοhmentloss may appear in the deciduous dentition. As the roots ofteeth are often short, these patients may lose teeth earlierdue to the early onset of disease and the root anatomy.
What Are Some of the DistinguishingCharacteristics of Some of the Other PeriodontalDiseases and Conditions?
Necrotizing periodontal diseases. Τhis οategory includesboth necrotizing ulcerative gingivitis (NUG) and necrotizingulcerative periodontitis (NUP). NUG and NUP have beenclassified together as they may be different stages of thesame disease. NUG is characterized by necrosis of the tipsof the interdental papilla with a pseudomembrane appear-ance, pain, foul odor, spontaneous bleeding, and possiblefever and lymphadenopathy. There is no attachment lossassociated with NUG. Fusiforms and spirochetes, as well asPrevotella intermedia,haνe been implicated in the etiology ofNUG. Significant contributing factors include stress, fatigue,poor oral hygiene, smoking, and poor nutrition, basicallyfactors associated with immunosuppression. NUG and NUPare also associated with HIV infection. NUP shares many ofthe clinical characteristics of NUG along \Λ/ith attachmentloss.
Abscesses of the periodontium. Periodontal abscessesare local infections of the gingival or periodontal tissues. Theetiology may be a foreign object such as a popcorn hull orloose piece of calculus. This type of abscess is marked bylocalized swelling and tenderness or pain. As the marginalgingiva begins to heal ιΛ,ith treatment, the orifice to deeperdrainage of infection may be closed off. lt may be drainedeither externally or through the wall of the periodontal pocket.
Periodontitis associated with endodontic lesions. Endo-dontic and periodontal Iesions may coexist separately asso-ciated with the same tooth or may communicate with each
other. Two separate lesions may coalesce or there may be aroot fracture or root perforation. Occasionally, an isolatedendodontic lesion may masquerade as a periodontal lesion,such as in an isolated furcation defect on a mandibular firstmolar. ln this case, proper endodontic therapy will heal thefurοation lesion as weΙl. ln a true combined lesion, the endo-dontic therapy must be performed first in order for the even-tual periodontal therapy to succeed as well.
Developmental or acquired deformities and conditions.Most of the deformities and conditions classified here areself-explanatory by name. Specific conditions such asmucogingival deformities, edentulous ridge deficiencies, andocοlusal trauma are described elsewhere in Ιhis Manual.
How ls a Periodontal Case Type FormulatedUsing the American Academy of PeriodontologyCase Type System?
The case type refers to the level of disease sΘverity, not thespecific diagnosis. Case type may be applied to each type ofgingivitis and periodontitis (also see Chapter l).
Case Type 1: Gingivitis. lnflammation confined to thesoft gingival tissues only. All gingivitis, irrespeοtive ofthe level of inflammation, is considered to be in thiscategory.
Case Type 2: Mild Periodontitis. This category signifiesthe beginning of attachment loss, up to approxi-maΙely 2o"/" of the attachment apparatus on the root.
τhere may be some pocketing and initial mobility.Furcation involvement, when present, is confined toa Class I involvement.
Case Type 3: Moderate Periodontitis. This categorysignifies further loss of the attachment apparatus, upto approximately 40% Ιo 45"/o. There is increasedbone loss, pocket depth, mobility, and furcationinvolvement. Furcas may have Class ll involvement.
Case Type 4: Severe Periodontitis. There is severeattachment loss, deep pocketing, mobility, pathologicmigration of teeth, and Class ll and possibly Class lllf urcation involvement.
30

CHAPTER 4
GHAPTER 4: CLlNlcAL ASSESSMENT, DlAGNoSlS, AND τREATMENTPLANNING
A comprehensive periodontal examination is necessary toascertain the presenting condition of the patient. ln additionto examining the patient's periodontal status, informationregarding the patient's medical history, past dental history,and a thorough soft and hard tissue examination will allow thepractitioner to formulate a complete set of diagnoses and acomprehensive treatment plan.
What ls the Risk Assessment in the Examinationand Diagnosis of the Periodontal Diseases?
Risk is defined as the possibility of loss or iniury. While it iswell established that bacterial plaque is the etiology of inflam-matory periodontal disease, there are many factors thatincrease risk of periodontal attachment loss. These contrib-uting factors may alter the host response to the bacterialοhallenge. Contributing factors may be systemic or local in
nature. Uncontrolled diabetes, smoking, or the use of certainmedications may adversely affect periodontal health. Openinterproximal οontacts, caries, restorative overhangs, andinvasion of the bioΙogic width may contribute to periodontalinflammation. The combination of these factors in coniunctionwith the host response is responsible for the manifestationsof disease. As risk is assessed, the resulting periodontalcondition must also be assessed.
What Are the Components of the ClinicalPeriodontal Examination? How ls EachComponent Completed?
Patient interview. The patient interview would elucidate thepatient's chief complaint and desired outcomes of treatment.The patient's state of mind relative to dental treatment mayalso be determined. Often, the patient will relate previousdental experiences, both positive and especially negativeexperiences that have shaped their perception of dentistryand dental care. Soοial habits such as smoking andfrequency and technique of oral hygiene may also bediscussed.
Medical history. A complete medicaΙ history must beobtained. The adage, "Never treat a stranger," is appropriateto remember. Medical problems such as uncontrolleddiabetes, smoking, arthritis, uncontrolled hypertension, infec-tious diseases such as hepatitis or HlV, allergies, bleedingdisorders, anticoagulation therapy, prophylaxis vs subacutebacterial endocarditis, and certain medications may alter thecourse or treatment of periodontal disease. A complete list ofmedications must be obtained. lnformation on medicationsmay be obtained from the Drug lnformation Handbook forDentistry, Tth ed, a companion Lexi-Comp book to thismanual. Often, the dentist may be the only healthcareprovider who has a complete picture of a patient's medicalcare. Αs more patients live longer and see multiple health-care providers, polypharmacy (concurrent use of manydrugs) of both prescribed and self-administered medicationswill be an increasing problem.
Dental history. The dental history will provide a picture ofboth the progress of the current conditions and the patient'sprevious efforts at maintaining their oral health. A history ofbleeding gums, change in tooth position, pain, halitosis or abad taste, oral habits, and previous periodontal care andmaintenance may all οontribute to a proper diagnosis anddetermination of prognosis. Copies of previous records and
radiographs will also contribute to a more complete picture ofthe patient's clinical condition.
Extraorat and intraorat examination. Both the externalsurfaces of the head and neck and internal suι'faces of themouth are examined for abnormal growths, lumps, bumps, orother signs of pathology. A complete bimanual and visualexamination will uncover unusual gro\Λ/ths or lesions forfurther analysis. Baseline vital signs: Blood pressure, respira-tions, and pulse should be obtained. Α complete muscle andTMJ examination should be completed for patients withtemporomandibular dysfunction signs and/or symptoms.
Dental examination. Numbers of teeth, missing teeth, resto-rations and their condition, caries, tooth position, and pulpalstatus \Λ/hen indicated should all be recorded"
FIGURE 1. Severe Caries. A hard tissue and dental examination are part of thecomprehensive periodontal examination. Caries such as this cancontribute to the gingival inflammation sΦn here by harboring pΙaque.
Plaque score. There are many methods by which to quantifyplaque accumulation on the teeth. One of the simplestmethods is to use a plaque disclosing dye that visualizes theplaque and then count the percentage of surfaces that haveplaque accumulated or those surfaces without plaque.Sequential recording of plaque and bleeding scores may beused to show patients improvement in their level of oralhygiene and clinical health.
F|GURE 2. Disclosing Dye. Red dye may bΘ used to help visualize plaque forthe patient and practitioner.
-

cLlNlcAL ASSESSMENτ, DlAGNosls, AΝD TREAτMENT PLANN|ΝG
Bleeding scores. BΙeeding is still the most reΙiable indicatorof the presence of gingivaΙ or periodontal inflammation.Bleeding on gentle skimming examines the health of themarginal gingiva. Bleeding on probing examines the health atthe base of the sulcus or pocket. The amount of bleeding andthe time bet\,veen stimulation and the appearance of bloodmay also be used to judge the severity of inflammation.Bleeding scores may be οaΙcuΙated as a percentage of sitesaround a tooth that bleed or do not bleed.
Periodontal pocket probing. Α periodontal pocket is a path-ologic space between a tooth and pocket wall and its depthmeasured from the gingival margin to the οlinical attachmentlevel. The depth of a periodontal pocket may only beis measured by using a calibrated periodontal probe (seeFigures 3A and 38). The probe is inserted along the long axisof the tooth into the pocket \,γith gent|e (approximately 25grams) of force until resistance is met. τ\Λ/enty-five grams offorce is necessary to indent the pad of the thumb about 1-2mm (see Figure 4). The probe is walked around each sur-face of the tooth. Errors in probing may arise from stoppingthe probe on a piece of calculus coronal to the base of thepocket, using excessive probing force, using a probe greaterthan 0.5 mm in diameter at the tip, the angulation of theprobe, and the health of the tissue.
F|GUΒE 3Α. PeriodontaΙ Probes. Periodontal probes come in a variety ofdesigns and markings. lt is important to have uniform instrumentsthroughout the practice as the same style probe may have differentdimensions from different manufacturers.
Figure 38. Periodontal Probes. Plastic probes may be used to examine aroundimplants. τhe probe on the left has PsB markings. τhe probe on the rightis a pressure-sensitive probe set at 25 g of force.
FlGUHE 4. Probe νιrith Gently Pressure. τhe correct probe force depresses theιhumb pad approximately 1_2 mm as seen here.
Εach tooth is examined at 6 locations: The mesiobuccal,buccal, distobuccal, distolingual, lingual, and mesiolin-gual surfaces. The probe may be angled approximately10" on each interproximal surface so that the tip of theprobe is placed apical to the contact point of adjacentteeth and may deteοt any interdental crater but, in mostinstances, the direction of probing is paralΙel to the longaxis of the tooth. ln a healthy site, the tip of the probestops v/ithin the junctional epithelium and in a diseasedsite it penetrates into the connective tissue. ln severedisease, the probe tip may penetrate to the alveolarbone. Therefore, the cliniοal probing depth is alwaysgreater than the histologiο sulcus or pocket depth. Amongexaminers, or from one time point to another, probingacοuracy is only within + 1 mm (see Figure 5).
FlGURE 5. Probing' τhe periodontaΙ probe is angled to the intefproximal underthe contact point to dΘtect any interproximal pocketin9.
Recession measurements, Recession is the measurementof the migration of the free gingival margin apiοal to thecementoenamel junction of the tooth. Recession is measuredas a positivΘ value. The recession measurement added tothe probe depth at a particular site indiοates the amount ofperiodontal attachment that has been lost at that site. Whenthe gingival margin is οoronal to the cementoenamel junction,the recession measurement has a negative value.Progressive recession from one examination to the next mayindiοate the need for surgical intervention.
δz

cHAPτER 4
Amount of attached gingiva. The attached gingiva ismeasured from the projection of the base of the sulcus orperiodontal pocket onto the suι'face of the gingiva to themucogingivaΙ junction. Τhe amount of attaοhed gingiva maybe calcuΙated by Subtracting the sulcus/pocket depth from thewidth of the gingiva from the free gingival margin to themuοogingival junction' The mucogingival .junction may beidentified by sight, by moving the lip or cheek laterally anddetecting where the alveolar mucosa stops moving, or byusing the side of a periodontal probe or other instrument andgently pushing in a coronal direction. The mucogingival junc-tion is located where the tissue folds (see Figure 6).
FlGURE 6. ldentification of the mucogingivaΙ iunction. τhe alveolar mucosamay be gently displaced in an occlusal direction to identΙfy ιhe muco-ginqival iunction.
Furcation examination. The furοation, the anatomic area ofa multirooted tooth where the roots diverge, may be exam-ined with a furcation probe such as the Nabers 2N probe. Thefurcation probe is curved with a rounded end (see Figure 7).The furcation probe should not be confused with the pigtailexplorer in which the probe is shorter than a furcation probe\νith a sharp tip.
F|GURΕ 7. Furcation Probes. τhe curued furcaιion prοbe has a long shaft andblunted tip.
Furcations are probed by placing the tip of the Nabersprobe against the tooth and moving it in an apical direc-tion. Τhe depression of the furca may be felt in thismanner. Maxillary premolars would have the mesialfurcation examined, maxillary molars would have thebuccal, mesial, and distal furcas examined, and mandib-ular molars would have the buccal and lingual furcas
examined. The mesial furcation of maxilΙary molars mustbe approached from the palate due to the shape of themesial and palatal roots (see Figures 8Α and BB). Thedepth of the furcation may be measured with a perio-dontal probe or specially marked furοation probe.
FIGURE 84. Examining Furcations.The buccal and lingual furcas are examinedin both a vertical and horizontal direction.
F|GURE 88. Examining Furcations. Τhe mesial furcation of the maxillary firstand second molars may only be detected from a palatal approach.
Glickman furcation classification:
Grade l: lncipient bone loss. The furcation probecan feel the depression of the furcationopening.
Grade ll: Partial bone loss (Cul-de-sac). The furca-tion probe tip enters under the roof of the furca-tion.
Grade lll: Total bone loss with through-andthroughopening of the furcation. The furcation entranceis not visible.
Grade lV: Α Grade lll furcation \Λ/here the furcationentrance is visible.
Other furcation systems may measure the horizontal(Lindhe and Nyman) or vertical (Tarnow and FletcheQοomponents of furcation involvement.
Mobility. Τhe movement of a tooth in its socket as a result ofan externaΙly applied force. Mobility is measured by theexaminer pushing the tooth gently in a faciolinguaΙ direοtion
-

cltΝlcAL AssEssMENτ- DιAGNosls" AND τREAτMENτ PLANNlNG
using the blunt ends of two metal instruments, usually amirror handle and handle of a periodontal probe. The use of afinger is not acceptable when assessing mobility. Mobilitymay be recorded on a 0-3 scale, although this scale may bemodified by individual practitioner preference.
Mobility scale:0: No mobility1: Mobility that is perceptible2: Mobility <1 mm faciolingually but no apical move-
ment3: Αpica! movement as well as lateral movement >1
mm
FIGURE 9. Mobility is measured using gentle force and the handles of twoinstruments. A finger should not be used to measure mobility.
Fremitus. A palpable δr visible movement of a tooth whensubjected to occlusal forces. Fremitus may be deteοted bothin centric occlusion and in lateral excursive movements(lateral fremitus). Fremitus may be detected by placing afingertip on the tooth in question or by looking as the teethcome together or are moved. lt is easier to detect fremitus ofthe maxillary teeth than the mandibular teeth. Fremitus isrecorded aS +. τhere is no numerical fremitus scale.
Occlusal analysis. Centric relation, CR-CO slide, excursivecontacts: The centric relation contact may be obtained usingthe chin point manipulation, bimanual manipulation, or thepower bite technique. The CR-CO sΙide and excursiveοontacts may be detected using articulating ribbon orocclusal indicator wax. lf these contacts, particularlynonworking οontacts, are associated with occlusal pathology(mobility, fremitus, widened PDL on radiographs), an occlusaladjustment to minimize excursive forces on each tooth maybe indicated.
What lnstruments and Materials Are Necessaryfor a Complete Periodontal Assessment?
Mouth mirror. A front surface mouth mirror is necessary tosee areas that may not be accessible by direct vision, reflectthe lips, buccal mucosa, and tongue, and in the assessmentof mobility. The mirror may also be used to depress thetongue during the soft tissue examination.
Periodontal probe. The calibrated periodontal probe shouldhave a tapered shaft approximately 0.5 mm in diameter at thetip. The tip may be smooth or have a small ball at the end(PSR probe, Maryland/Moffitt probe) useful for detectingcalculus and root irregularities. ln any practice, all periodontal
probes should be of the same design and from the samemanufacturer in order to ensure as much standardization aspossible (see previous Figure 3).
Furcation probe. Furcations are best examined using afurcation probe suοh as the Nabers 2N or Hamp probe. Thelf23 exρlorer, periodontal probe, and pigtail explorer are notproperly shaped to adequately explore a furcation (seeprevious Figure 7).
Articulating ribbon and articulating ribbon forceps(holder), occlusal indicator wax. Occlusal contacts must behighlighted in order to be properly identified. This may bedone either with articulating ribbon or occlusal indicator wax.Occlusal indicator wax has the advantage of beingcompletely perforated only where opposing teeth are in
contact. Often, articulating paper leaves stray marks thatmakes proper interpretation more diffiοult.
What ls Necessary for a PeriodontalRadiographic Examination?
Α periodontal radiographic examination consists of a fullmouth series of radiographs including vertical bitewing films.A long cone paralleling technique is utilized and the apices ofall roots must be visible. ln many instances, particularly whenthere is significant bone loss or the films are misaligned,standard horizontal bitewing films do not adequately eΧposethe interproximal bone between the posterior teeth. Boneloss, widened periodontal ligaments, caries, calculus, rootproximity, and unusual radioluοencies and radiopacities maybe detected. The true topography of vertical osseous defeοtscannot be determined by radiographic examination alone.
F|GURΕ '10. vertical bitewing radiographs, seen here with well-executedposterior periapical films, will show the interproximal crest of the alveolarbone that is often missed on horizontal bitewing films.
VVhat Is a Clinical Periodontal ScreeningExamination?
The Periodontal Screening and RecordingτM (PSR) Examina-tion \Λ/aS developed in order to streamline the data gatheringand recordkeeping for the screening periodontal examina-tion. The PSR Exam is patterned after the Community Perio-
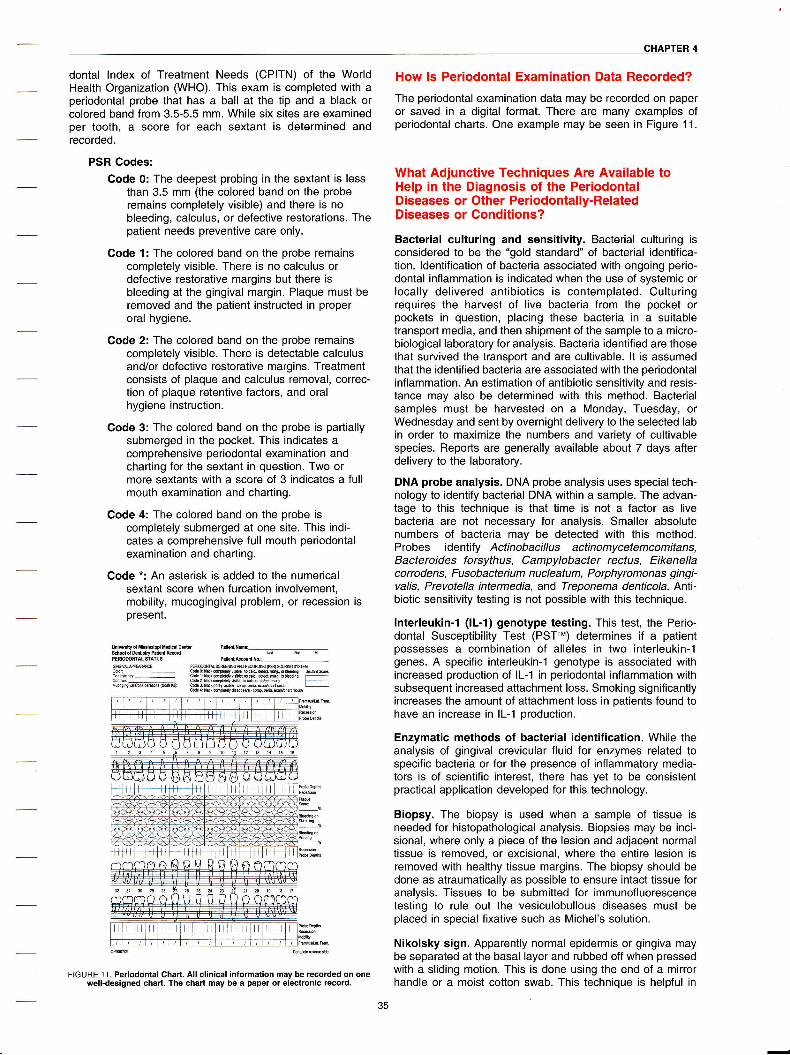
CHAPτER 4
dontal lndex of τreatment Needs (CPITΝ) of the WorldHealth organization (\Λ/Ho). This exam is completed with aperiodontal probe that has a ball at the tip and a black orcolored band from 3.5-5.5 mm. While six sites are examinedper tooth, a score for eaοh sextant is determined andrecorded.
PSR Godes:Code 0: The deepest probing in the sextant is less
than 3.5 mm (the colored band on the proberemains completely visible) and there is nobleeding, οalοulus, or defeοtive restorations. Thepatient needs preventive care only.
Code 1: The colored band on the probe remainscompletely visible. There is no calculus ordefective restorative margins but there isbleeding at the gingival margin. Plaque must beremoved and the patient instructed in properoral hygiene.
Code 2: The colored band on the probe remainscompletely visible. There is detectable calculusand/or defective restorative margins. Treatmentconsists of plaque and caΙculus removal, correc-tion of plaque retentive factors, and oralhygiene instruction.
Code 3: The colored band on the probe is partiallysubmerged in the pocket. This indicates acomprehensive periodontal examination andcharting for the sextant in question. Two ormore sextants with a score of 3 indicates a fullmouth examination and chaιting.
Code 4: The colored band on the probe iscompΙete|y submerged at one site. This indi-οates a comprehensive full mouth periodontalexamination and charting.
Code *: An asterisk is added to the numericalsextant score when furcation involvement,mobility, mucogingival problem, or recession ispresent.
υniνriιydMiΦi38ippi Eld cσιg$δddMUΦ PddRΦ
Cdor
-
ω1sbEΦyj
-
cΦur
-
MιΦoho va] ΦmrσΦm {bob h)
PRoWtrsRΦlΦMRΦΦDM ffi )Φrewffiωe0 ilaιΦΦΦ!y'ii ΦΦ...ffiωωΙ urιΦdΦii*:Φc* ffiΦ !fuσiq rτΗ:l}affi"yfu"ft"*tr#&-:-''Φω 4: il* ΦΦω, dMΦ.* .Φm. Eio εΙftιa( ΦΦ
How ls Periodontal Examination Data Recorded?The periodontal examination data may be recorded on paperor saved in a digital format. There are many examples ofperiodontal charts. One example may be seen in Figure 11.
What Adiunctive Techniques Are Available toHelp in the Diagnosis of the PeriodontalDiseases or Other Periodontally-RelatedDiseases or Conditions?
Bacterial culturing and sensitivity. Bacterial culturing isconsidered to be the "gold standard" of bacterial identifica-tion. ldentification of bacteria associated with ongoing perio-dontal inflammation is indicated when the use of systemic orlocally delivered antibiotics is contemplated. Culturingrequires the harvest of live bacteria from the pocket orpockets in question, placing these bacteria in a suitabletransport media, and then shipment of the sample to a micro-biological laboratory for analysis. Bacteria identified are thosethat survived the transport and are οultivable. lt is assumedthat the identified bacteria are associated with the periodontaΙinflammation. An estimation of antibiotic sensitivity and resis-tance may also be determined with this method. Bacterialsamples must be harvested on a Monday, Tuesday, orWednesday and sent by overnight delivery to the selected labin order to maximize the numbers and variety of cultivablespecies. Reports are generally available about 7 days afterdelivery to the laboratory.
DNA probe analysis. DNA probe analysis uses special tech-nology to identify bacterial DΝA within a sample. The advan-tage to this technique is that time is not a factor as livebacteria are not necessary for analysis. Smaller absolutenumbers of bacteria may be detected with this method.Probes identify ActinobacilΙus actinomycetemcomitans,Bacteroides forsythus, Campylobacter rectus, Εikenellacorrodens, Fusobacterium nucleatum, Porphyromonas gingi-valis, PrevoteΙΙa intermedia, and Treponema denticola' AnΙi-biotic sensitivity testing is not possible with this technique.
lnterleukin-1 (lL-I) genotype testing. This test, the Perio-dontal Susceptibility τest (PSττ") determines if a patientpossesses a combination of alleles in two interleukin-1genes. A specifiο interleukin-1 genotype is associated withincreased production of lL-1 in periodontal inflammation withsubsequent increased attachment loss. Smoking significantlyincreases the amount of attachment loss in patients found tohave an increase in lL-1 production.
Enzymatic meιhods of bacterial identification. While theanalysis of gingival crevicuΙar fluid for enzymes related tospecific bacteria or for the presenοe of infΙammatory media-tors is of scientific interest, there has yet to be οonsistentpractiοal application developed for this technology.
Biopsy. The biopsy is used when a sample of tissue isneeded for histopathological analysis. Biopsies may be inci-sional, where only a piece of the lesion and adjacent normaltissue is removed, or excisional, where the entire lesion isremoved with healthy tissue margins. The biopsy should bedone as atraumaticaΙly as possible to ensure intact tissue foranalysis. Tissues to be submitted for immunofluorescencetesting to rule out the vesiculobullous diseases must beplaced in special fixative such as Michel's solution.
Nikolsky sign. Apparently normal epidermis or gingiva maybe separated at the basal layer and rubbed off when pressedwith a sliding motion. This is done using the end of a mirrorhandle or a moist οotton swab. Τhis technique is helpful in
cP000709 ΦΦΦs*
FIGURE 1 1. Periodontal Chart, All clinical information may be recorded on onewell-designed chart. The chart may be a paper or electronic record.

Ξ
cLlNlcAL AssESsMENτ. D|AGNosls. AΝD TREAτMENτ PLANN|NG
identifying the vesiculobullous diseases. Distinction amongthe diseases may be made only by biopsy.
Exfoliative cytology. This technique may be used to identifyabnormal cells on the surface of a lesion. Several commer-οially available tests can be used to sample suspicious-looking red lesions.
What Are the Dento-Legal Considerations of aComplete Examination and Diagnosis inPeriodontal Therapy?
The patient record should contain a complete periodontalcharting, diagnosis, and treatment plan for all patients withperiodontal disease. Studies have shown that fe\r/er than20% ot records in general practice οontain these necessaryelements. lt is significantly easier for a practitioner to supportclaims of a complete examination, diagnosis, treatment, and/or specialty referral if this documentation is present. "lf it isn'twritten down, it didn't happen," and that a "Short pencil iswofth more than a long memory," should be remembered atall times.
PERIoDoNTAL TREAτMENτ PLANNING
Periodontal diagnosis and treatment planning are criticalsteps in the process of periodontal disease management.Diagnosis and treatment planning are the direct outcomes ofa periodontal assessment. An accurate diagnosis and aneffective treatment plan should be based upon a comprehen-siye assessment of periodontaΙ signs and patient Symptoms.The aft of decision-making in periodontal therapy involves asynthesis of 1) the cΙinicaΙ experience of the therapist, 2) thetechnical ability ot the therapist, 3) intuition, 4) the experi-ences of others as recorded in texts or presented in profes-sional forums, and 5) evidence-based thinking.
What ls a Working Diagnosis? How Does aWorking Diagnosis Differ From a DifferentialDiagnosis?
A working diagnosis is the "pencil" diagnosis generated bythe cΙiniοian that is based upon the scientific signifiοance ofthe signs and symptoms recorded during the comprehensiveexamination. lt is the οlinician's best estimate of the patho-logic process, the etiologic factors for that process, and themorbid outcomes of the process present at the time of theexamination. Τhe working diagnosis is the basis of thepatient's initial treatment plan. lf later assessments are madeat the re-evaluation of initial therapy, or for that matter,assessments are made at any time during therapy indicatethat the working diagnosis may be incorrect, the workingdiagnosis may be changed to reflect the new information.
A differential diagnosis is one that includes t\ivo or morepossible processes that may be consistent with initial clinicalassessments. Rather than commit to one νvorking diagnosis,the clinician may choose to provide a differential diagnosisand either perform or request additional diagnostic testing. lnthis instance, the clinician fully expects that a working diag-nosis will emerge from the differential diagnosis.
The initial treatment plan is based upon the periodontal diseaseidentified in the working diagnosis. The treatment planaddresses itself to each etiologic agent in a logical sequence.Pertinent etio|ogic factors that are not addressed in the treaιment plan result in undertreatment and failure of therapy.
The treatment of etiologic factors that either do not exist, orhave been incorrectly identified by the clinician, leads to over-treatment, which prolongs treatment, or in the οase of anincorrect assessment, undertreatment, which preventsdisease οontrol. Both oveftreatment and undeιtreatment areoutside the standard of care for any patient. Assuming thatthe clinical assessments are complete, control of the etiologicfactors should effectively manage the periodontal disease(identified in the working diagnosis). Simply stated, οontrol ofetiologic factors translates to disease control.
SAMPLE PERIODONTAL TREATMENT PLANS
While all periodontal treatment plans share a common goal(ie, control of inflammatory periodontal diseases), thepath\Λ/ay to that goaΙ from patient to patient is rarely thesame. For discussion purposes, models of treatment planswill be presented for each of the three basic periodontaldisease categories: Gingivitis, periodontitis, and occlusaltraumatism.
Gingivitis. The presence or absence of dentaΙ plaque as theprimary etiologic factor distinguishes the two major catego-ries of Class I Gingival Diseases. There are four categories ofdental plaque-induced gingival diseases and eight categoriesof nonplaque-induced gingival lesions. Since the majority ofgingival diseases seen in a dental practice are related to thepresence of pΙaque, the framework of a treatment plandesigned to manage these common disorders is includedhere.
The correct working diagnosis is the critical first step in thetreatment planning process. The therapeutic "mindset" of theprovider should be based upon that diagnosis. For example,a diagnosis of gingivitis associated with dental plaqueonly should ordinarily not include resective periodontalsurgery, but a diagnosis of drug-influenced gingivalenlargement might include a gingivectomy, apiοally posi-tioned flaps, or systemic antibiotics as a therapeuticpossibility if the gingival enlargement persists followingnonsurgical mechanical therapy and/or attempts to modifythe patient's medication protocol.
AcTlvE TREATMENτ oF A DENTALPLAQUE-INDUCED GINGIVAL DISEASE
Working diagnosis. Gingivitis associated \Ιvith dental plaqueonly.
FIGUFIE 12. Gingivitis Associated livith Dental Plaque Only. Severe gingivitisthat displays the clinical signs of necrotizing ulcerative gingivitis ispresent in the maxillary incisor and canine area.
JO

cHAPτER 4
The patient is a well-kempt 26-year-old systemiοally healthyfemale. She sees a physician annually and has been on oralcontraceptives for 2 years. She is married and works as avice-president in a local banking institution. Her chiefcomplaint is "bleeding gums." She also presents with severegingival inflammation consistent with localized necrotizingulcerative gingivitis (NUG) around the maxillary right incisorsand canine. With treatment, the prognosis for keeping herperiodontium in health and comfortable function for a lifetimeis good to excellent.
TREATMENτ PLAN
lnitial τherapy
ο Presentation and discussion of diagnosis and treatmenιplan.Ιhis step will ensure that the patient understandsher condition and the rationale of therapy. Because somuch of periodontal therapy requires patient involvementand behavior modification, understanding her disease willbe critical. Commonly, points made here will need to bere-enforced during the course of therapy.
. Medical consuΙtation. Probably unneοessary in this case.
. Oral physiotherapy. The patient's methods of plaquecontrol are evaluated and, as probably will be the case,modifications wiΙl be made. Special emphasis should beplaced on improving plaque control in the maxillary right.
o Coronal debridement. Hand and power-driven scalers νvill
be used to remove coronal calοulus. Since this is a gingi-vitis case, there will not have been loss of periodontalattachment to permit root planing.
. Correction of plaque and food retention factors such asoverhanging restorations and open contacts. The clinicalcroνvns will be polished with a fluoride-containing mildabrasive.
. Re-evaluation of inΙtial therapy. After a minimum of 4weeks (the time for healing and maturation of the dento-gingival junction), the patient is re-examined and theresults of that examination will be compared νvith thoserecorded at the initial examination. Decisions about theworking diagnosis, continuation of periodontal therapy, ora periodontal maintenance program will depend upon theanswer to the following two questions:
Are thΘre any persistent signs and symptoms ofgingivitis present?
lf so, is there anything that can be done to improvethis patient's gingival health?
lf the answer to both questions is"no", the working diagnosisis confirmed. The patient's final diagnosis is then: Gingi-vitis associated with dental plaque only with local con-tributing faοtors.
lf, however, the answer to the both questions is "yes", thenconsiderations for improving the patient's oral hygiene, anti-microbial therapy in the form of antimicrobial mouthrinses,additional correction of plaque retentive factors, and discus-sions concerning the effect of oral contraceptives on gingivalhealth might be appropriate. A gingivoplasty in the maxillaryincisor/canine area may be required if the gingival deformitiescontinue to be worrisome.
F|GUBE 13. Gingivitis Associated ι,vith Dental Plaque onΙy After Plaquecontrol, scaling, and Polishing. Residuaι disease and deformities mayrequire local deΙivery of antibiotic, additional emphasis on plaque control'and/or gingivoplasty,
AcτlVE τREATMENT oF cHRoNlc PERloDoNτlTls
Periodontitis. Periodontal diseases and conditions thatfeature loss of periodontal attachment include chronic perio-dontitis, aggressive periodontitis, periodontitis as a manifes-tation of systemic disease, necrotizing periodontitis, andperiodontitis associated with endodontic lesions. Since themajority of gingival diseases seen in a dental practice arerelated to the presence of plaque, the framework of a treat-ment plan designed to manage these common disorders isincluded here. Since chronic periodontitis is a relativelycommon disorder, a typical treatment plan for chronic perio-dontitis will be presentΘd here.
Working diagnosis. Generalized moderate chronic perio-dontitis with occlusal traumatism.There are >30% of perio-dontal sites with >3-4 mm loss of periodontal attachment.Generalized mobility and fremitus patterns are present.There are areas of gingival recession.
FIGURE 14. Generalized Moderate οhronic Periodontitis lΙvith occlusal τrau-matism. τhe patient has a 2s-pacιΦear history of cigarette smoking,Results of a recent medical evaluation were unremarkable.
τhe patient is a robust 47-year-old male \ivho works as aconstruction foreman with a chief complaint of "looseteeth." He reports that the outcomes of a recent physicalexamination \Λ/ere unremarkable. He has been divorcedfor 3 years and has a 25 pack/year history of cigarettesmoking. His dental treatment has been infrequent. Hislast dental appointment was for a "cleaning" four yearsago. \Λ/ith treatment and regular periodontal mainte-
1.
2.
cllNlcΔL ΔssEssMENτ- DlAGNοsls- AND τREAτMENτ PLANN|NG
nance, the prognosis for keeping his dentition in healthand comfortable function is excellent for 5 years andgood forl0 years.
TREAτMENτ PLAN
lnitial Therapy
. Presentation and discussion of diagnosis and treatmentplan. Ιhis step will ensure that the patient understandshis condition and the rationale of therapy. Because somuch of periodontal therapy requires patient involvementand behavior modification, understanding his disease willbe critical. Α concept of co-therapy bet\Λ/een dental health-care professionals and the patient is stressed because ofthe expected lifetime duration of active and maintenancetherapy. The timing and sequence of any endodontictherapy, minor tooth movement, and/or restorativedentistry is presented at this time as well. The patientshould be presented with the rationale for periodontalsurgery that will most likely be necessary. Commonly,points made here will need to be re-enforced during thecourse of therapy.
o Medical consultation. Because of the recent physicalexamination, it may not be necessary to send the patientfor an evaluation. Α letter to the patient's physicianrequesting a copy of recent medical laboratory testresults for his dental record is appropriate. The lettercould also describe the patient's periodontal condition,outline the periodontal treatment plan, and request anypertinent medical recommendations.
. Counseling in methods for smoking cessation. Ιhepatient needs to understand clearιy how continuedsmoking u/ill abrogate the effects of periodontal therapy.Τhe letter to the patient's physician might solicit strate-gies for smoking cessation. Because smoking is such asignificant etiologic factor, smoking cessation will be amajor element in infΙammatory disease control for thispatient.
. Oral physiotherapy. The patient's methods of plaquecontrol are evaluated and, as probably will be the case,modifications will be made.
. Scaling and root planing. Hand and power-driven scalerswill be used to remove coronal and radicular calculus.Since this is a periodontitis case, there will have beenloss of periodontal attachment.
Because of anatomical limitations (probing depths >4mm, furcation invasions, root grooves etc), it is under-stood that surgical access may be required to completeroot debridement. Thermal sensitivity is a commonoutcome of scaling and root planing. Desensitizingagents may be prescribed, but often, "tincture of time" isadequate.
. Correction of plaque and food retention factors such asoverhanging restorations and open contacts. The clinicalcro\Λ/ns will be polished with fluoride containing mild abra-sives and desensitizing agents.
. Re-evaluation of inflammatory disease controι' After aminimum of 4-6 weeks (the time for repair of the dento-gingival junction), the patient is re-examined and theresults of that examination are compared with thoserecorded at the initial examination. This is a critical stagein treatment as decisions about the working diagnosis
and continuing active therapy are made depending uponthe answers to the following questions:
1. Are there any persistent signs and symptoms ofgingival inflammation or debris present?
2. lf so, is there anything short of periodontal surgerythat can be done to improve the conditions?
3. ls there any residual tooth mobility/fremitus?
lf the answer to the first and second question is "no" and theansνver to the third question is "yes", the patient's workingdiagnosis o't generalized moderate chronic periodontitis withocclusaΙ traumatism iS Supported, and treatment shouldproceed to the occlusal therapy phase.
lf, however, the answer to the first and second question is"yes"' then considerations for improving the patιent's oralhygiene, refining scaling and root planing, instituting antimi-crobiaΙ therapy, additional correction of plaque retentivefactors, and discussions concerning progress made insmoking cessation might be appropriate. Because anyresidual inflammation may contribute to mobility/fremitus, it isinappropriate to proceed to occlusal therapy vι/ith persistentgingival inflammation. The working diagnosis cannot beconfirmed or, for that matter changed, without optimalnonsurgical inflammatory disease control.
occLUSAL τHERAPY
. Persistent mobility and fremitus patterns should be re-evaluated following inflammatory disease control. lfpresent, selective grinding of nonworking and workingfunctional tooth contacts that are contributing to occlusaltraumatism should be adjusted. Ιn addition, parafunc-tional habits of compulsion, such as bruxism, should becontrolled with occlusal appliance therapy. Force control,like inflammatory disease control, is an ongoing processin both active and maintenance periodontal therapy.
RE-EVALUAT|oN oF lNlτlΑL THERAPY
. After all of the items on the initial therapy treatment planhave been addressed, decisions about the working diag-nosis and the need for additional treatment are madebased upon the ansνver to the following questions:
'l . ls there any additional therapy required to controlthis patient's periodontitis?
2. ls there anything that needs to be done for thispatient other than periodontal surgery to controι hisperiodontitis?
3. Are the outcomes of inflammatory disease controland force control therapy consistent with theworking diagnosis of generalized moderate chronicperiodontitis with occlusal traumatism?
lf the ans\Λ,er to the first question is "no" and the ans\iver tothe third question is "yes", no additional active treatment isrequired and the patient should be placed in periodontalmaintenance. Question 2 is irrelevant.
lf the answer to Questions 1 and 3 are both "yes", and theansνver to Question 2 is "no", treatment should progress tothe surgical phase.
38
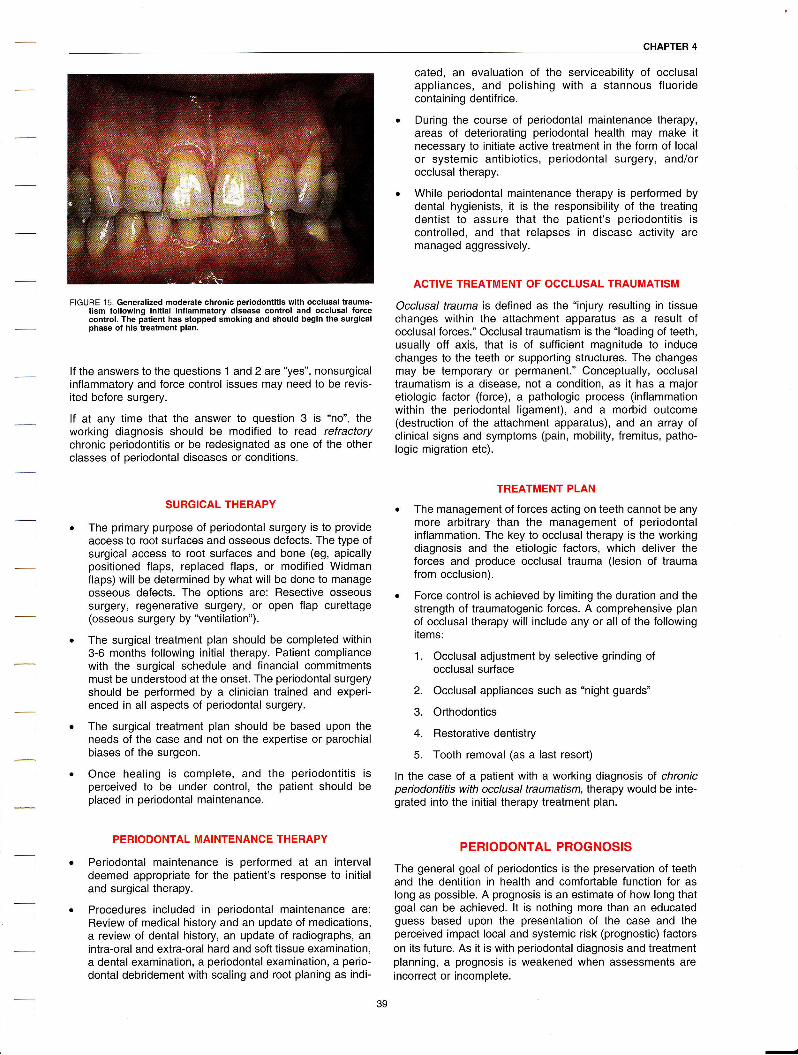
CHAPτER 4
FIGURE 1 5. Generalized moderate chronic periodontitis with occlusal trauma-tism following initial inflammatory disease control and occlusal forcecontrol. The patient has stopped smoking and should begin the surgicalphase of his treatment plan.
lf the answers to the questions 1 and 2 are "yes", nonsurgicalinflammatory and force control issues may need to be revis-ited before surgery.
lf at any time that the answer to question 3 is "no", thevvorking diagnosis should be modified to read refractorychronic periodontitis or be redesignated as one of the otherοlasses of periodontal diseases or conditions.
sURGlcAL THΕRAPY
The primary purpose of periodontal surgery is to provideaccess to root surfaces and osseous defects. The type ofsurgical access to root surfaces and bone (eg, apicallypositioned flaps, replaced flaps, or modified \iηlidman
flaps) will be determined by what will be done to manageosseous defects. The options are: Resective osseoussurgery, regenerative surgery, or open flap curettage(osseous surgery by "ventilation").
The surgical treatment plan should be completed within3-6 months following initial therapy. Patient compliancewith the surgical schedule and financial commitmentsmust be understood at the onset. The periodontal surgeryshould be performed by a clinician trained and experi-enced in all aspects of periodontal surgery.
The surgical treatment plan should be based upon theneeds of the case and not on the expefiise or parochialbiases of the surgeon.
onοe healing iS complete, and the periodontitis isperceived to be under controι, the patient should beplaced in periodontal maintenance.
PERIoDoNTAL MAlNτENANGΕ THERAPY
Periodontal maintenance is performed at an intervaldeemed appropriate for the patient's response to initialand surgical therapy.
Procedures included in periodontaι maintenance are:Review of mediοal history and an update of medications,a review of dental history, an update of radiographs, anintra-oral and extra-oral hard and soft tissue examination,a dental examination, a periodontal examination, a perio-dontal debridement with scaling and root planing as indi-
cated, an evaluation of the serviceability of occlusalappΙiances' and polishing with a stannous fluoridecontaining dentifrice.
During the course of periodontaΙ maintenanοe therapy,areas of deteriorating periodontal health may make it
necessary to initiate active treatment in the form of localor systemic antibiotics, periodontal surgery, and/orocclusal therapy.
While periodontal maintenance therapy is performed bydental hygienists, it is the responsibility of the treatingdentist to assure that the patient's periodontitis isοontrolled, and that relapses in disease activity aremanaged aggressively.
AcTlvE τREAτMENT oF occLUSAL τRAUMATιSM
Occlusal trauma is defined as the "injury resulting in tissuechanges within the attachment apparatus as a result ofocclusal forces." Occlusal traumatism is the "loading of teeth,usually off axis, that is of sufficient magnitude to induοechanges to the teeth or supporting structures. The changesmay be temporary or permanent." Conceptual|y, occΙusaltraumatism is a disease, not a condition, as it has a majoretiologic factor (force), a pathologic process (inflammationwithin the periodontal Ιigament), and a morbid outcome(destruction of the attachment apparatus), and an array ofclinicaΙ signs and Symptoms (pain, mobility, fremitus, patho-logic migration etc).
τREATMENT PLAN
. Τhe management of forces acting on teeth cannot be anymore arbitrary than the management of periodontalinflammation. The key to occΙusal therapy is the workingdiagnosis and the etiologic factors, which deliver theforces and produce occlusal trauma (lesion of traumafrom occlusion).
. Force control is achieved by limiting the duration and thestrength of traumatogenic forces. A comprehensive planof occlusal therapy wilΙ include any or aΙl of the followingitems:
1. Occlusal adiustment by selective grinding ofocclusal surface
2. Occlusal appliances such as "night guards"
3. Orthodontics
4. Restorative dentistry
5. Tooth removal (as a last resort)
ln the case of a patient with a working diagnosis of chronicperiodontitis with occΙusal traumatiSm, therapy would be inte-grated into the initial therapy treatment plan.
PERIODONTAL PROGNOSIS
The general goal of periodontics is the preservation of teethand the dentition in health and comfortable function for aslong as possible. Α prognosis is an estimate of hoνv long thatgoal can be achieved. lt is nothing more than an educatedguess based upon the presentation of the case and theperceived impact local and systemic risk (prognostic) faοtorson its future. Αs it iS \Λ/ith periodontal diagnosis and treatmentplanning, a prognosis is weakened when assessments areincorrect or incomplete.
39

cLlNlcAL AssEssMENτ. DlAGNosls. AND τBEAτMENτ PLANN|NG
What ls Meant by Prognosis? ls a PrognosisRelated to the Oltcori'e of a Disease Witn r A "poor" prognosis will suggest that the goal is
Treatment or Without Treatment? unachievable for any significant length of time andthat major changes in periodontal health will probably
A prognosis is a forecast of the probable result of an attack of occur'
a disease - the prospect as to recovery from a disease asindicated by the nature and symptoms of the (#ftirδ ' A.hopeless" prognosis will offer no chance of main-
case. ln periodontiοs, a prognosis \,lι,ill οommonly n" "ircrΞi taining the dentition in health and comfortable func-
for individua| teeth and the complete dentition depending τlon'
upon whether or not treatment is rendered.A periodontal prognosis \ivill be rooted in assessments of the
Α prognosis is usually expressed in terms of a finite time initial status of the case (eg, degree and extent of inflamma-period during which the goal of health and comfortable func- tion, pocket depths, attachment loss, the amount of bonetion can be maintained. Typically, a 5- to 1O-year timeframe loss, the number of teeth lost due to periodontal disease, andis typical of a "long-term prognosis", while a 2- to s-year time- the severity of mobility/fremitus patterns). To this information,frame is typical of a "short-term prognosis". Within each time- an overlay of the systemic, local, and intangible risk (prog-frame, graded qualitative estimates of success for achieving nostic) factors will be added.the goal are also made. For example:
Clearly, there is little true science involved in formulating a
o An ,,excellent,,prognosis will forecast that goal with no prognosis- Too many prognostic factors are out of the direct
significant change in periodontal health. control of the therapist and the patient. ln addition, thepredictability of treatment outcomes is almost always weak-
. A ,,good,, prognosis will forecast that goal with only ened by the severity of the disease. A prognosis can be
minor changes in periodontal health. helpful to the patient in decision-making vis-a-vis time andcosts of treatment. ln every case, the patient should/must
. A "fair" prognosis will forecast that goal, but changes understand that for anything other than a "good" prognosis orin periodontal health might occur that will either a "poor'' prognosis, forecasts for treatment outcomes can bedowngrade or reduce the timeframe of the forecast. extremely unreliable.
40

CHAPτER 5
CHAPTER 5: PREVENTION OF DISEASE AND THE MATNTENANCE OFHEALTH
Prevention of disease and the maintenance of health oncethe disease process has been controlled are the corner-stones of periodontal therapy. As plaque is the primary etio-logic agent of gingivitis and periodontitis, personal plaquecontrol is the s,ne qua non of dental therapy. A patient mustbe able to control the etioΙogiο agents of both caries andperiodontal disease on a daily basis for therapy to besuccessful. As plaque can reorganize on the teeth and sub-gingivally within 24 hours, daily plaque removal is essential.
What Are the Components of Personat PIaqueControl?
Personal plaque control consists predominantly of themechanical disruption of plaque on the facial, lingual, andinterproximal surfaces of the teeth. This disruption may beachieved using a manual toothbrush, powered toothbrush,floss, interdental brush, specialized brushes, and otherinstruments. Antimicrobial agents such as chlorhexidine orthe essential oils may be used as adjuncts to mechanicalplaque removal.
VVhat Methods of Toothbrushing May BeRecommended to a Patient?
The toothbrush can remove plaque on accessible surfaces.No matter what toothbrushing method is chosen, the manualtoothbrush should have soft nylon bristles and a small head,either a child's size brush or a size 20 or the equivalent. Asmaller brush head allows the brush to be properly adaptedto the irregularities of tooth anatomy and arrangement. ASmalΙer head also lessens the potential for activating the gagreflex and may reach posterior surfaces more comfortablyand effectively than a larger headed brush. For use in deli-cate areas, the bristΙes may be softened by running the brushhead under hot νvater before use.
There are many toothbrush designs available today. Eachbrush manufacturer presents claims νVhy that particuΙar brushis superior to others. ln reality, brushes of many differentdesigns will effeοtively remove plaque when used properΙy.
Bass Method. The bristles of the toothbrush are placed at a45" angle to the tooth surface at the gingival margin, trying toget the bristles into the gingival sulcus. The brush is thenmoved in short back-and-forth motions for about 20 strokes.The brush head is then moved around the arch, both on thefacial and lingual surfaces. The occlusal surfaces are cleanedby manipulating the bristle ends into the pits and fissures ofthe tooth crown. This is the currently preferred method ofmanual brushing.
Other Methods:
Modified Stillman Method. The brush bristles areresting partially on the cervical area of the teeth andpartially on the gingiva pointing toward the gingivalmargin. Pressure is applied to the brush to cause thegingiva to blanch. The brush head is then moved in shortback-and{orth strokes with the brush moving οoronally atthe same time. The sides of the bristles, instead of thebristle tips, are used to disrupt the plaque. This method isclassified as a "roll" technique.
Charters' Method. The brush is placed against thesurface of the teeth with the bristles pointing away fromthe gingival margin. The back-andJorth motion is amassaging stroke for the gingiva. This method may beused for gentle plaque removal.
What Methods of Interproximal Cleaning May BeRecommended to a Patient?
For the patient with no or minimal attachment loss, flossing isthe interproximal technique of choice. There is no clear-cutdifference in effectiveness between waxed and unwaxedfloss. lt should be stressed to the patient that fιoss be used inan up-and-down motion, not in a "shoeshine" motion. Manypatients will revert to improper technique even after properinstruοtion. Dental tape, basically a wider version of floss,may also be used.
Once attachment loss has occurred and root concavities areaccessible, floss loses its effeοtiveness. lnterproximalbrushes, toothpicks, and rubber tips may be used in thesecircumstances. With moderate to severe attachment loss, amanual brush and an interproximal brush will outperform themanual brush and floss in plaque removal.
Interproximal brushes may be cylindrical or conical in shape.The advantage of an interproximal brush is that the bristlesmay be worked into root concavities and furcation areasexposed by attachment loss. The interdental brush should beused in both a back-and{orth and rotary motion to ensuremaximum adaptability of the bristles. The brush should beused from both a facial and lingual or palatal approaοh toremove all plaque.
FIGURE 1. lnterproximal Brushes. Either cylindrical or cone shaped are moreeffective in removing plaque that is lodged in the exposed concavities orfurcations of tooth roots.
The end-tuft brush (Figures 2Α and 28) may be used oninterproximal surfaces \Λ/here there is no adjacent tooth andon the distal areas of the most posterior teeth. With a bend in
the handle and tapered bristles, the end-tuft brush fits almostperfectly in the distal furcation of the most posterior maxillarymolar.
-

PREvENτloNoFDl
manual brushing along with appropriate interproximalcιeaning with floss or an interproximal brush'
Powered brushes may be useful as a motivationaι tool to
assist patients in cleaning their teeth on a daily basis' Thesebrushes may also assist patients with arthritis or other debili-
tating conditions that make holding or manipulating a manual
brush difficult or impossible. While there are several distinc-
tive designs of po\Λ/ered brushes, each design has its strongpoints and weaknesses, but all of these brushes perform at
similar levels of effectiveness.
FlGURES 2A and 2B' End-Tuft Brush. τhe end-tuft brush, particu|ar|y When the'- - nanαε is υent approximately 3o", is quite effective at removing PlaqΨ9 9ηiii;'li;gr;i;r;i;ces of th6 mandi6ular anterior teeth and the distalsurtaces οf the most posterior teeth.
What Role Do Powered Toothbrushes Have inPersonal Plaque Control?
F|GURE 38. τhe smalι head of this powered brush adapts wsmoolh surface and interproximal areas ot teeth'
What Antimicrobial Agents Can Assist inControlling PIaque ani Gingival lnflammation?
When seleοting a chemotherapeutic agent, it is important to
distinguish bδtween the ability to remove plaque andsubstΞntiated evidenοe of a therapeutic effect' Manymouthrinses οan reduce the amount of plaque over rinsing
with water, but wiihout a positive therapeutic effect, the justifi-
cation for recommending such an agent is minimal'
To date, two basic agents have been shown to have a signifi-
cant therapeutic effect on gingivitis over a 6-month period'
Chlorhexidine gluconate, O.12Yo' in an alcohol-containingvehicle, now aviilable in generic as well as brand name form'
and phenolic compound/essential oil-based mouthrinses canbe used to help control gingivitis. Chlorhexidine kills bacteria
rn sifu when used for 30 seconds twice daily' Side effects
include increased calculus formation, staining of teeth and
restorations, and altered taste. Caution should be taken \νhen
recommending a chlorhexidine rinse for a patient with
composite resin restorations.
The essential oils, thymol, menthol, and eucalyptol, along
Vvith methyl sa|icylate for flavoring, constitute the aοtive ingre_
dients in most phenol-based mouthrinses. These rinses alsocontain betv/een 20"λ Ιo 27"/" alcohol in the vehicle' Discre-
tion should be taken in recommending these rinses to recov-
ering alcoholics.
There are other mouthrinses and mouthwashes that show a
therapeutic effect for periods of time shorteτ than the 6montλs stipulated by the U.S. Food and Drug Administration
for approval as a therapeutiο agent. Some agents have adetergent effect to remove plaque and contain glycerin or
other compounds that leave teeth feeling smooth to the
tongue. These agents have noi been shown to have any
significant therapeutic benefit to the patient'
42
F|GURE 3Α. Powered toothbrushes come in a variety ot shapes and with
different plaque disruption principles.
It has been demonstrated that powered toothbrushes remove
more plaque than manual toothbrushing alone, when both
are used properly. There is no evidence to suggest that the
use of a powered brush alone is as effective as appropriaie

CHAPτER 5
What Are the Ingredients in a Dentifrice(Toothpaste)?
Toothpaste, in conjunction with toothbrushing, serves to:
. Minimize plaque buildup
. Provide an anticaries effect
. Remove stainr Freshen breath
Τhe ingredients found in most toothpastes include:
ο Polishing or abrasive agent. May be silica, calciumcarbonate, alumina, or other mild abrasive. Thepolishing agent removes stain, stained pellicle,and plaque.
. Binder or thickener. May be the carrageenates,alginates, or carboxymethyΙcellulose. Τhesebinders give the toothpaste its consistency andflowability when expressed from the tube.
. Surfactant. Detergent such as sodium lauryl sulfatethat foams to aid in debris removal. Detergentsmay also have inherent antimicrobial propertiesthat contribute to plaque control.
. Ηumectant. May be glycerin, sorbitol, or polyethy-Ιene glycol. Provides moisture to the paste andkeeps it from drying out, even when left exposedfor short periods of time.
ο F]avoring. May be spearmint, Wintergreen, orpeppermint. Some patients may have allergicsensitivity reactions to certain flavoring agents,particularly those νvith a cinnamon base.
. Active (therapeutic) ingredient. May be fluoride forcaries protection, triclosan as an antiplaqueagent, pyrophosphate as an anticalculus agent,potassium nitrate as a desensitizing agent, orperoxide compounds as whitening agents.
\tVhat is the American Dental Association Seal ofAcceptance?
The American Dental Αssociation (ADΑ) Seal of Acceptanceis earned by product manufacturers after submitting theirproducts to rigorous testing under standards defined by theΑDA. As this is a costly and lengthy process, manufacturersof consumer products more often seek approval than those ofprofessional products. This Seal may be carried on productpackaging.
THERAPEυτIc ENDPolNTsΗow much treatment is enough? Τhe answer to that questionis found in an understanding of the endpoints of therapy.These endpoints must be practical and realistic for each indi-vidual patient. Once the goals of therapy have beenachieved, frequent and regular re-evaluation and periodontalmaintenance become integral parts of periodontal therapy. lthas been well documented that patients retain more teeth forlonger periods after therapy with appropriate maintenancecare than \λ/ithout that care.
ls Periodontal Therapy Successful?This question goes to the core of periodontics as a disciplinein dentistry. There are many studies that have proven thatperiodontal therapy, when appropriately executed and withgood patient compliance to oral hygiene regimens andscheduled maintenance wbifs, can reduce tooth loss due toperiodontal disease by up to 7o"λ. ln one group of treatedpatients with periodontal disease followed an aνerage ot 22years, overall tooth loss νιas7.1"/o. occasionally, teeth Will belost in even the most compliant patient. Those few patients(<10% of the total) that fall into the "extreme downhill" group,may continue to lose attachment and subsequently lose teethin spite of all efforts.
What Are the Goals of Periodontal Therapy?
The primary goal of periodontal therapy is the maintenance ofthe natural dentition in health, comfortable funοtion, withpleasing aesthetics and satisfaction for the life of the patient.This goal persists even in the face of the expanding use andsuccess of endosteal implants. lmprovements in implanttherapy have given the practitioner neνv treatment planningand decision-making challenges regarding the retention orremoval of natural teeth. ln spite of these successes, theoverarching goal must still be the prevention of disease andmaintenance of the natural dentition when practicallypossible.
What Teeth Can Be Expected to Ηave theGreatest Longevity and \Ιvhich Teeth Are LostMost Frequently Due to Periodontal Disease?
Excluding third molars, maxillary second molars are lost mostoften to periodontal disease. This would be expected bothdue to complex root anatomy and the difficulty in performingeffective oral hygiene because of the tooth's location.Mandibular canines and first premolars are the teeth mostlikely to be retained.
What Clinical Parameters May Be Used to Judgethe Success of Periodontal Therapy?
There are several clinical and radiographic parameters thatmay be used to judge the success of periodontal therapy,including:
Reduction or absence of bleeding on probing.Bleeding on gentle probing (25 g of force) is still the bestprognostic indicator of the potential for future attachmentloss. Absence of bleeding on probing is a g8% negativepredictor that the site will lose attachment in the future.Conversely, approximately 3O/" ot sites that bleed atconsecutive maintenance visits over one year are at riskfor future attachment loss. Since it is impossible to predictexactly which site will lose attachment, the thrust oftherapy is to control inflammation at all sites.
Reduction of probing depth and gains in periodontalattachment. Periodontal therapy is focused on theremoval of etiologic agents and contributing factors andthe subsequent maintenance of health. One way toimprove this possibility for both the patient and practi-tioner is to reduce probing depths. Greater success isachieved in creating and maintaining a plaque-free envi-ronment with shallow pockets compared to pocketsgreater than 5 mm in depth. Persistence of periodontalpathogens and progressive loss of attachment is associ-ated \Λ,ith deeper pockets' Pocket depth may be reduced

Ξ
PREvENτloN oF DlsEAsE AΝD τHE MA|ΝτENAΝcE oF HEALτH
by inflammatory control achieved with initial therapy,resective surgery (eg, gingivectomy, apically positionedflap with osseous surgery), or by repair or regeneration oflost periodontal attachment.
Positive radiographic changes. Positive radiographicchanges related to the success of periodontal therapyinclude the reappearance of a crestal lamina dura at theinterproximal osseous crests, evidenοe of bone fill inareas of regenerative therapy, narrowing of the perio-dontal ligament Spaοe in teeth subiect to occlusal trauma,and the absence of calculus on coronaΙ and rootsurfaces. While radiographs made in clinical practice arenot standardized, valuable comparisons may still bemade betνveen pretreatment and post-treatment films-
Occtusal stability. Tooth mobility is caused by the pres-ence of edema in the gingival and periodontal tissues,loss of attachment, and the effects of occlusal forces onthe attachment apparatus. Αfter inflammatory control iSοompleted, teeth often exhibit decreased mobility. This isdue to the elimination of edema and the reformation ofthe supragingival connective tissue fibers that contributeto tooth stability' particularly when there has been attaοh-ment loss. Judicious occlusal adjustment by selectivegrinding to relieve fremitus may also contribute toincreased tooth stability. Mobile teeth may be success-fully maintained in a state of health. lncreasing mobility orhypermobility are indicators that an occlusion remainsunstable even after therapeutic intervention. Τargetedocclusal therapy, removable or fixed splints, may be indi-cated in this case.
What Are the Limitations of Periodontal Therapy?
There may be significant limitations to \ivhat periodontaltherapy can accomplish. First and foremost, the patient mustbe dedicated to a daiΙy ritual of personal plaque control.Without this, successful treatment becomes an uphill battle.There may be limitations due to the amount of attachmentΙoss, root anatomy, uncorrectable local or systemic factors,uncontrollable occlusal forces, mobility, and last but not least,the diagnostic aοumen and skiΙl of the c|inician.
What Can Be Done for the Patient Who Fails toRespond to Periodontal Therapy?
It is important to identify those factors that may contribute to apatient's continued attachment loss. Failures in therapy maybe related to either diagnostic or therapeutic shortcomings.Even with accurate diagnoses and flawless treatment, theoccasional patient \Λ/ill continue to lose attachment.
Diagnostic def iciencies:
o Related to health history: Undetected diabetes,immune compromise, or other systemic disorder
. lmproper use, or nonuse, of the periodontal andfurcation probe
. lmproper radiographic examination: Particularly theuse of bitewing films of less than a diagnostic qualityto detect interproximal bone loss; vertical bitewingfilms are recommended to adequately visualizeposterior interproximal bone height
ο Abnormal anatomy rendering complete root detoxifi-cation impossible
o Unidentified microbes not eradicated by conventionalmechanical therapy
ο Undeteοted traumatic occlusion
. Pulpal pathosis
Therapeutic deficiencies, failure to:
. lnstruct the patient adequately in plaque control
o Formulate a comprehensive treatment plan
ο Control the etiologiοal agents
o ldentify and correct loοal contributing factors
o Treatment failures related to diagnostic defiοiencies
. Select proper of therapeutic modalities
ο Execute proper initial therapy vvith adequatefollow-up
. Provide adequate surgical techniques
. Utilize an effective maintenance program
How ls Prognosis Determined?
Patients are extremely interested in \Λ/hether or not theproposed treatment is going to be effective. lt would bebeneficial for clinicians to give their patients a reasonablyaccurate prediction of treatment success. Unfortunately,prognostic acumen is limited. Except for those teeth thatoriginally have a "good" prognosis, projections were ineffec-tive at projecting the fate of teeth, acοuraοy in predicting wasin about Ιhe 40"λ range. lnitial mobility, increasing mobility,and smoking \ivere seen as factors negatively affecting prog-nosis.
MAINTENANCE oF PERloDoNτAL HEALTH
How Important ls Maintenance in PeriodontalTherapy?
lt is cΙear that regular maintenance visits are a key compo-nent to successful periodontal therapy. There is a demon-strated 70% reduction in lost teeth comparing untreatedpatients to those who received treatment and followedthrough with regular maintenance. Τhere is a 50% improve-ment in tooth retention when comparing treated patientswithout maintenance therapy to those who were both treatedand well maintained. Some studies suggest that with aregular 3-month maintenance interval, attachment levels maybe maintained even in the face of a patient's poor oralhygiene.
What Are the Therapeutic Goals of PeriodontalMaintenance?
. To minimize the recurrence and progression of perio-dontal disease in patients who have been previouslytreated for gingivitis and periodontitis
. To reduce the incidence of tooth loss by monitoringthe dentition and any prosthetic replacements of thenatural teeth

CHAPτER 5
. To increase the probability of locating and treating, ina timely manner, other diseases or conditions of theoral cavity
What Are the Components of the PeriodontalMaintenance Visit?
Τhe basic maintenance appointment should have thefollowing components:
Update and review the medical history. Τhis aspect isparticularly important related to the onset of Type 2diabetes mellitus in adult patients, and changes in patientmedications, both prescribed and self-administered.Queries to the patient must take more than one form, forsimply asking the question, "Has anything related to yourhealth changed since your last visit with us?" may notgarner the necessary information. Asking patients to listtheir current medications, whether or not they are contin-uing to take previously reported medications, andinquiring about recent visits to the physician may all elicitmore meaningful answers.
Update the dental history. This review may seemunnecessary for the patient being treated solely in oneoffice. Unfortunately, for \ivhatever reason, some recom-mended treatment may not have been completed and aperiodic review of patient treatment will uncover anyincomplete treatment needs. The patient νvho sees both ageneralist and a specialist or specialists must updatehis/her dental history to acknowledge the following, ordecide not to follow treatment recommendations.
Extraoral and intraoral hard and soft tissue examina-tions' Τhis step will uncover any clinically evident hardand soft tissue lesions that may require some follow-upattention.
Dental examination. This step will reveal clinicallyevident decay and/or restorations that have outlived theirusefulness.
Periodontal evaluation. This step includes review oforal hygiene effectiveness (best accomplished beforeplaque and οalculus is removed), marginal inflammatorycontrol as demonstrated by bleeding on gentle skimming,and reduction or maintenance of probe depths. Use ofthe Periodontal Screening and Recording (PSR) systemmay simplify documentation of this review.
Radiographic review. Review of existing radiographscan corroborate clinical findings and the decision for newradiographs may be made. Vertical bitewing films shouldbe exposed for patients with posterior interproximal boneloss.
Removal of supra- and subgingival plaque
Scaling and root planing where indicated
Polishing the teeth. Selective polishing, using a rubbercup and abrasive prophylaxis paste only where plaqueand stain are evident, has been advocated to maintaintooth structure, particularly the fluoride-rich layer ofenamel on the surface of the crown. An air abrasive typeof polishing unit may be used as long as the abrasivestream is not directed onto root surfaces or compositeresin restorations.
Topical fluoride application. This step helps to restorethe fluoride-rich surface that may have been removedduring the polishing step.
Final oral hygiene instructions and the dispensing ofappropriate personal hygiene implements
How ls the Patient's Maintenance lntervalDetermined?
The maintenance interval should be determined on an indi-vidual basis' Αmong the factors to be considered are theinitial level of disease, the aggressiveness of the attachmentloss, the patient's response to therapy, the patient's ability toperform effective plaque control, and the post-treatmentstability of gingival inflammation and attachment levels. Main-tenance intervals may be as shoιt as 1-2 months, up to about6 months bet\Λ/een appointments. Patients who have alreadydemonstrated a susceptibility for attachment loss should beseen no less often than every 4 months.
How Compliant ls the Average PeriodontalPatient?
One study suggests that only about 16% of patients receivingperiodontal therapy comply with recommended maintenanceintervals. other studies have demonstrated a similar Ιack ofcompliance. Behavior modification is difficult even when thepatient is faced with a life{hreatening disease. There aremany factors contributing to a lack of compliance including:
. Denial and negligent attitude towards own health
. Αcknowledging the problem means the patient mustparticipate in his own care
o Many patients \ivant the dental profession to takeresponsibility for and fix their problems
. Compliance decreases as treatment time or thecomplexity of the required behavioral changeincreases
Several steps to improve patient compliance have beenproposed:
. Simplify behavioral change
o Accommodate the patient
. Remind patients of appointments
o Keep compliance records
. lnform the patient about the necessity for and consis-tency of keeping maintenance appointments
. Provide positive reinforcement
. Ensure the dentist's involvement
What Type of Biological Modulation May Be Usedto Control Recurrent Periodontal Disease in theMaintenance Patient?
Maintaining stable post-treatment attachment levels may bedifficult. There are several approaches to treating new areasof attachment loss or to prevent new attachment loss. lnsituations where the attachment loss is localized, localdelivery of antibiotics or antimicrobial agents such as doxycy-cline, minocycline, or chlorhexidine is possible. For situationswhere new attachment loss may be more widespread, theuse of systemic antibiotic therapy may be warranted.

PREvENTloN oF DlsEAsE AND τHE MA|NτENANGE oF HΕALτH
Systemic administration of a subantimicrobial dose of doxy-cycline (SDD) has been advocated to help prevent attach-ment loss. SDD has been shown to stabilize the activity ofcollagenase and other matrix metalloproteinases and there-fore slow down the destructive inflammatory process. lnitialcliniοal studies to receive U.S. Food and Drug Administrationapproval were of 9 months duration. There is minimalevidence of the effect of SDD over longer time periods. lt hasbeen suggested that SDD may be effective in controllingother collagenase-based inflammatory disorders.
When Should a Patient Be ComprehensivelyRetreated for Recurring Periodontal Disease?
Τhere are no clear-cut guidelines as to \Λ/hen a patient shouldre-enter comprehensive periodontal treatment. Fortunately,in most cases, only localized sites remain a problem. Onerule of thumb would be that if the patient's recurrent problemscannot be addressed in 2-3 appointments, considerationshould be given toward a new round of comprehensivetherapy. ln addition, a patient who has recently completedsurgical therapy but οontinues to have difficulty should betreated with alternative therapies, such as antibiotics, andfurther control of risk factors, with additional surgical therapyheld in abeyance.
When Should a Patient Be Referred for SpecialtyPeriodontal Care?
Τhe decision on when to refer a patient for specialty caremust be made between the general practitioner and patient,with the periodontist available to provide the necessary treat-ment. ln general, most periodontists prefer to treat the patientfrom the beginning of initial therapy through advancedtherapy. ln certain situations, particularly when the generalpractitioner's office can provide high quality initial therapy orwhen there is a questionable need for referral, the patientmay be referred for specialty care after the results of initialtherapy have been evaluated. This arrangement should beworked out in advance as it is uncomfoιtable for both thepatient and periodontist if additional initial therapy is recom-mended by the specialist. ln most cases, third party carrierswill not provide benefits for this additional treatment. Thissituation also begs the question in the patient's mind as to thequality of the care received in the generalist's office. Effectivecommunication between the general dentist and periodontistis paramount to a clear understanding of the overall course ofthe patient's treatment.
46

CHAPTER 6
CHAPTER 6: NONSURGICAL THERAPY: SCALING AND ROOTPLANING, OCCLUSAL AND ANTIBIOTIC THERAPY
What ls Nonsurgical Therapy?
Τhe expression nonsurgical therapy suggests that thenonsurgical procedure so designated is performed in aclosed environment and, therefore, is not invasive (eg, it doesnot break the epithelial seal of the sulcular or iunοtionalepithelium). While the οoncept of scaling and root planingmay be, indeed, nonsurgical, the gingival soft tissue is ofteninadvertently invaded. Local anesthesia will often be requiredfor patient comfoft during scaling and root pΙaning proce-dures.
Oral hygiene and local antimicrobial procedures, the removalof iatrogenic factors, occlusal therapy, and systemic antibioticprocedures are not invasive and, therefore, conform tononsurgical concepts.
The term surgical treatment is reserved for those periodontalprocedures that are performed in a deliberately open environ-ment where incisions are made, periodontal soft tissue iselevated to expose tooth roots and alveolar bone, and thesoft tissue is either rep|aοed or repositioned over the rootsand bone. During surgiοal access, resective or regenerativeprocedures may be performed on the bony defects producedby periodontitis.
SCALING AND ROOT PLANING
Scaling and root planing are the cornerstones of almost allinitial therapy treatment plans for periodontitis and may bethe only mechaniοal therapy required for the management ofmild (1-2 mm clinical attachment loss) chronic periodon-titis. WhiΙe sca|ing and root planing procedures are utilizedroutinely they remain among the most technically demandingprocedures performed in periodontics. When performedwith optimal access and skill, scaling and root planing wilΙ pro-duce a decrease in gingival inflammation, a reduction inperiodontal probing depths, and a gain in periodontal attaοh-ment. With less than optimal access and skill, the outcomesfrom scaling and root planing will, by extension, be lessthan optimaΙ.
What ls Scaling and Root Planing? What Are theGoals and Objectives of Scaling and RootPlaning?
Scaling and root planing are tνvo technically similar perio-dontal procedures. Both involve the mechanical application ofhand- and/or power-driven instruments to tooth suι'faces toremove plaque, stain, and calculus. Clinically, it is frequentlydifficult to separate one from the other. Scaling may beper{ormed on eithΘr coronal or radicular surfaces in periodon-titis cases, but in gingivitis cases, scaling should be limited tocoronal surfaces. Root planing is only performed on rootsuι'faces that have been denuded of periodontal attachmentby periodontitis. ln addition to the removal of plaque, stain,and calculus, it also includes the removal of "diseaseaffected" cementum containing imbedded calculus, wholebacteria, and toxic bacterial debris such as endotoxin.
The goals and objectives of scaling and root planing are bothtechnical and biologic. The technical goals and objectives ofscaling and root planing (ie, the mindset of the clinician at thetime), are to produce hard, smooth tooth surfaces free ofcalculus and cementum affected with endotoxin and/or otherbacterial contaminants. ln the process, the bacterial loadadjacent to periodontal tissues is reduced.
The biologic aoals and objectives of scaling and root planingare to produce a tooth surface and sulcular ecosystem that isbiocompatible with periodontal epithelial cell and connectivetissue adhesion. Decreases in gingival inflammation, reduc-tions in periodontal probing depths, the presence of Gram-positive beneficial bacterial species, and gains in periodontalattachment are the outcomes by which effeοtive scaling androot planing are measured (see below).
What ls Disease-Affected Cementum? What lsEndotoxin and Where Does it Come From?
Disease-affected cementum is cementum that has beenstripped of periodontal attachment by periodontitis and hasbeen exposed to the septic contents of the periodontalpocket. lt contains remnants of embedded calculus, wholebacteria, and the products of microbial life. Τhe most studiedof these is bacterial endotoxin. Endotoxin and whole bacteriamay be found as deep as 12 microns beneath the cementalsurfaοe (see Figure 1).
F|GURΕ 1. A Photomicrograph of Marginal Periodontitis. τhe associateddeposits o' subgingival, serumnaΙ calculus are firmly attached to andinterlocked with surface irregularities in dentin and cementum.
Εndotoxin is the lipopolysaccharide component of the outermembrane of Gram-negative cell walls. lt is exported asmembrane vesicles during the lifespan of most Gram-nega-tive bacteria. The biologiο activity of endotoxin includesattraction of inflammatory οells, activation of the complement
E

NoNsURGlcAL THERAPY: scALlNG AND Rooτ PLANING' occLUsAL AND ANTlBloτΙc τHERAPY
System, Stimulation of bone resorption, fibroblast οytotoxicity,pyrogenicity, and mitogenic activity with B-lymphocytes.Endotoxin Will produce a Severe local infΙammatory reaction\,vhen injected experimentally in tissue (see Figure 2).
FlGURE 2. An electron micrograph of negatively stained Fusobacterium nucιe-a,Um. The corrugaιed surface is a typical morphological feature of Gram-negative bacteria. τhe oιher membrane vesicle at the tip of the organismis a possible source of endotoxin.
What Are the lnstruments Used in Scaling andRoot Planing? \Mhat Techniques Are Employed?
Calculus detection and removal are learned skiΙls that gradu-ally improve with experienοe. Εxquisite tactile sensitivity,mediated by hand, sonic, and ultrasonic instruments isessential. Correct instrumentation is then an essentialprerequislte to detection and removal. There are manydifferent instruments specifically designed for scaling androot planing, and there are probably as many personal prefer-ences for instruments as there are instruments. The followingis a guide to the four general categories of instruments usedin scaling and root planing.
F|GURE 3. τhis is a Moffitt-Maryland periodontal probe detecting subgin-gival calculus in a narrow subgingival pocket. Calculus removal at thissite will be difficuΙt.
PeriodontaΙ probes and explorers are used to detect calculusdeposits. Probes will also confirm that deposits have beenremoved and that the roots have been planed to hard and
smooth surfaces. The uΙtralight Moffitt-Maryland periodontalprobe with Williams markings is an excellent choice forsubgingival calculus detection (Figure 3). The 3A curvedexplorer or the Nabers furcation probe may also be used forοalculus detection and are particularly helpful in root concavi-ties or furcation invasions.
Scalers are the instruments of οhoice for visible supragingivalcalculus removal. Scalers have a bulky working end and a rigidshank. Both tend to limit their tactile sensitivity. ln crossseοtion, the most popular scalers (sickle scalers) have atriangle shaped blade with 2 opposed οutting edges. ScalersshouΙd not be used in deep (>4 mm) pockets so as to mini-mize injury to gingival tissues.
Hoes and flles belong with scalers as instruments whosecutting edges are designed to function at right angles to thetooth surface and they shouΙd be used almost exclusively forheavy supragingival deposit removal. Frequently, calculusremoval with sοalers, hoes, and files will be incomplete, andmore delicate instruments with greater tactile sensitivity andaοcess capability will be required to remove residual depositsand smooth cementum or dentin. Scalers, hoes, and files areused with a verlical pulltype stroke.
FIGURE 4. A Gracey curette with calculus and soft tissue debris removed froma deep periodontal pocket. lncidental tissue removal is common duringsubgingival scaling and root pιaning.
Curettes are the instruments of choice for subgingival instru-mentation and root planing. They are generally smaller thanscalers and are designed to permit atraumatic entry to thesubgingival space. The tactile sensitivity of most curettes isgreater than scalers and, as such, curettes are well suited forsubgingival calculus detection, calοulus removal, and rootplaning. Area specific curettes (Gracey and Goldman-Fox)have a single cutting edge at 60'to the root surface and aredesigned to instrument specific tooth surfaces in specificregions of the mouth. For example, the Gracey 13/14 isdesigned to instrument the distal surfaces of molar andpremolar teeth, while the Gracey 9/10 is designed to instru-ment the buccal or lingual surfaces of the same posteriorteeth. Gracey curettes have been modified for improvedaccess and reduced tissue injury. Universal curettes (Crane-Kaplan 6, McOall's 17sl18s, Columbia 4Rl4L) have 2 cuttingedges at 90" to the root surface and may be used in any
48

CHAPTER 6
Application
Supragingival calculus removal
Universal scaling and root planing
BuccaΙ and lingua| surfaces
lnterproximal surfaces of anterior teeth
lnterproximal surfaces of posterior teeth
lnstrument
Scalers - Jacquette 34135, τay1or
colUmbia 4Fy4L or 13/14, ΝΙccall's17sl18s
Gracey 9/1 0
Gracey 112, 314
Gacey 11112 (mesial), Gracey 13/14 or 15/16 (distal)
region of the mouth. Curettes may be used νvith vertical,oblique, horizontal, or circumferential pull-type strokes(see Figure 4).
SUGGESTED SCALING AND ROOT PLANINGlNSTRUMENTs AND APPLlcAτloNs
ments be kept adequately cooled, that the instruments bekept in constant motion, and that the side (not the tip) of theinstrument be used against tooth structure at all times. Manyultrasonic units may be used \Λ,ith a variety of irrigants suchas chlorhexidine or povidone-iodine.
Are There Any Medical Risks to the Patient and/or the Provider When Power-Driven lnstrumentsAre Used to Debride Teeth?
Magnetostrictive ultrasonic instruments may "de-program"some οardiac pacemakers. Αs it is not in the province ofdental health professionals to decide whether or not a patientwith a cardiac pacemaker may be at such a risk, it is recom-mended that a medical consultation be obtained beforemagnetostrictive ultrasonic instrumentation is performed.
Cultivable oral bacteria are present in aerosols created bysonic and ultrasonic instruments, and there seems to be nodifference in the number of colony-forming units producedfrom aerosols generated by magnetostrictive, piezoelectric,or turbine driven instruments. Antimicrobial mouthrinsesbefore power-driven instrumentation \Λ/ill reduce the numberof cuΙtivabΙe baοteria in aerosols.
It is beyond the intended scope of this manual to describe thetechnical aspects of scaling and root planing. It is recom-mended that the reader consult one of the textbooks devotedto the subject listed in the "Selected Readings" section.
How Do Power-Driven Instruments Perform WhenCompared to Conventiona] Ηand lnstruments?
Comparison studies of the performance of power-driveninstruments \,vith hand instruments on extracted teeth haveproduced equivocal data. Both are partially effective inremoving calculus and cementum. Tests on extracted teethsuggest that both methods are equally effective in removingdebris from teeth, but that hand instruments alone, orfollowing power-driven instrumentation, produced thesmoothest tooth surface. Other reports have presentedcontrasting data indicating the superiority of power-driveninstruments in producing smooth tooth surfaces.
What Are the Expected Outcomes andLimitations of Scaling and Root Planing? HowSuccessful ls Scaling and Root Planing inAchieving lts Goals and obiectives? ν\rhat Arethe Guidelines for Decision-Making vis-a-visSurgical Access for Root Debridement?
Catculus removal. Both hand- and power-driven instrumentshave limited utility in calculus removal from periodontalpockets. As a guideline, calculus removal becomes progrΘs-sively more inefficient in sites with probing depths greaterthan 3 mm, and the limit of any effective instrumentationoccurs in probing depths over 6 mm. These reports supportthe notion that closed (nonsurgical) access for scaling androot planing in pockets less than 3 mm may be as effective asopen (surgical) acοess. When probing depths are greaterthan 6 mm, residual calculus is inevitable. These sites wiΙlrequire surgical access for effective root debridement.
What Are Power-Driven Scalers? How Are TheyUsed?
Power-driven scalers are usually used to provide a rapidcalculus and stain removaΙ with a minimum of discomtort tothe patient or trauma to hard or soft tissues. Power-drivenscalers use either ultrasonic or sonic energy for debridement.
Ultrasonic instruments use either magnetostrictive or piezo-electric technology to convert electrical energy to physicalenergy at the instrument tip. lnstrument tips vibrate from25,000-40,000 cycles per second at an amplitude betvveen10-30 μm. The heat generated by magnetostrictive instru-ments requires copious amounts of water for cooling. ln thecooΙing process, \ivater "cavitation" (similar to the effectproduced by a propeller in water) occurs which releasesdissolved gases. The resulting spray, along with the wateritself, facilitates the removal of dislodged debris. Recentadvances in ultrasonic instrument design, such as thinneruιtrasonic tips, have improved access in deep pockets andprovide subgingival delivery of antimicrobial agents (Figure5).
FIGURE 5. An ultrasonic scaler with water cavitation at the tip.
Sonic instruments are classified as air-turbine instruments.They use the air pressure from high-speed handpiece lines toproduce tip vibrations from 2,000-6,000 cycles per second.
Power-driven instruments may be used in both supragingivaland subgingival areas. lt is recommended that the instru-
49

NoNsURGlcAL THERAPY: scALlNG AND Rooτ PLANING. occLUSAL AND AΝτiBloτlc τHERAPY
The limitations in achieving the goals and ob.iectives ofscaling and root planing may be a function of either:
o Probing depth at the time of instrumentation
. The method of access to root surfaces (eg, surgicalversus nonsurgical)
o Root grooves and concavities
o Furcation involvements (Figure 6), and/or
o Technical ability of the operator
F|GUFiE 6. A maxillary premoιar showing retained calculus in the rootconcavity and bifurcation. Anatomic features of tΦth frequently limit theeffectiveness and efficiency of calculus remoνal (couι7esy of Dr. JeanneSaιcetti)
Scaling and root planing will reduce the biomass of patho-genic bacteria and calculus in periodontal pockets. Thereduction in bacterial Ιoad will allow improved periodontalhealth in most cases of chronic periodontitis. MiΙd cases ofperiodontitis may not require additionaΙ surgical therapy. lnmore advanced οases, repeat sessions of scaling and rootplaning are not indicated, as they probabΙy will not improvesoft tissue health beyond that achieved by one or two sessionsof therapy. Still, where surgery is indicated, presurgicalscaling and root planing will improve tissue health andenhance surgical outcomes.
Removat of disease affected cementum. The cementum ofthe coronal third of the root ranges from 10-150 μm. lt isthinnest nearest the cementoenamel junction and becomesprogressively thiοker toνvard the root apex. Because it iS thinand is readily aοcessibΙe to instrumentation, all cervicalcementum is usually removed in 1-4 strokes of a curette. lnadvanced cases of periodontitis that involve the thickercementum at the mid-root, and where cΙinical access may bereduced by deeper pocket depths or root anatomy, theremoval of cementum is predictably less complete. Otherfaοtors that affect the amount of tooth structure removedduring scaling and root pΙaning are the forces applied at theworking end of the instrument and the number of strokes νvith
an instrument against a given root surface. Ultrasonic instru-ments remove less tooth structure than do hand curettes.
Both hand curettes and power-driven instruments removeaffected cementum containing endotoxin. Curettes are moreeffective than ultrasonic instruments in removing endotoxinfrom root surJaces, and under ideal conditions, hand curettesare capable of rendering root surfaces previously in contactwith diseased periodontal tissues totally free of endotoxin.
Decreased probing depths and gains in periodontalattachment. As a general rule, subgingival scaling and rootplaning \Ιvith hand- and/or power-driven instruments wil| yielddecreases in probing depths and, in most cases, gain inperiodontal attachment. Deeper periodontitis sites are morelikely to gain attachment than shallow sites, and there doesnot Seem to be a Ιimit to pocket depth where these effectswill not be observed to one degree or another. These changesusually ocοur within thΘ first month following treatment andcan be maintained with good oral hygiene and monthlysupragingival cleanings for up to three months (Figures7 and 8).
FIGURE 7. The effect of scaling and root planing on pocket depth. Greaterreduction in pocket depth may be expected following instrumentation ofdeeper pockets. (With permission, cercek, et aι, J cιin Periodontol, 1983,10:46-56)
FlGURE 8. τhe effect of subgingival scaling and root planing on subgingivalattachment levels. Greater gains in attachment may be obtained byscaling and root planing in deeper pockets. (with permission, Cercek, et al,J clin Periodontoι, 1983, 10:4σ56)
What ls Meant by Critical Probing Depth?
The downside of scaling and root planing is the observationthat a |oss of οlinical attachment will invariably occur whenshallow pockΘts are mechanically instrumented. Concepts ofcritical probing depths have emerged as decision-makingguidelines for nonsurgical and surgical periodontal therapy.Scaling and root planing initial probing depths <2.9 mm will
50

result in a net loss of periodontal attachment \Λ/hile performingthe same proοedures on pockets >2.9 mm will resu|t in a netgain in periodontal attachment. Similarly, the critical probingdepth for surgical treatment is 4.2 mm.
Judiοious instrumentation to control inadvertent tissue injuryis appropriate in shallow periodontal pockets. Since the injuryproduced by instrumentation is a painful blunt tearing of thetissues of the dentogingival junction, the use of locaΙ anes_thesia for patient comfort should be avoided to minimizeunwanted soft-tissue injury. Local anesthesia should bereserved for periodontitis cases where deep pockets (>6
mm) are the rule and where instrument efficiency and effec-tiveness is limited.
Reduce the load of pathogenic bacteria. Visual clinicalmeasures of supragingival plaque accumulation on teeth areusually affected most by supragingival instrumentation andoral hygiene practices by the patient. Subgingival instrumen-tation is not a requirement for changes in visual measures.Subgingival scaling and root planing are effective in reducingthe number of bacterial morphotypes associated with inflam-matory disease (motile rods and spirochetes) as seen in dark-field or phase contrast microscopy. Hand, sonic, and ultra-sonic instrumentation appear to be equally effective in pro-ducing these changes and in creating an environment \η/here
morphotypes associated with periodontal health (nonmotilecocci and rods) will predominate. However, these changesare not permanent, and the proportions of pocket bacterialmorphotypes will return baseline levels in 2-3 months.Frequent professionally performed supragingival debride-ments will have little effect on this trend. lt is clear thatsubgingival instrumentation is a critical guideline in achievingthe clinical goals and obiectives of scaling and root planing(Figure 9).
FΙGURE 9. τhe effect of subgingival scaling and root planing on supragingivalplaque scores. lnitial reductions gained following oral hygiene instructionwerδ the same as those obtained by subgingival instrumentation. rwithρemission, cercek, et al, J clin Periodontol, 1983' 10:46'56)
The effect of subgingival instrumentation on the cultivability ofplaque microorganisms is limited by the degree of invasive-ness of P gingivalis and A. actinomycetemcomitans.These t\Λ/o
exogenous periodontal pathogens tend to resist eradicationby scaling and root planing. Because their persistence in highnumbers after mechanical therapy is associated with contin-uing periodontaΙ deterioration, the eradication of these andendogenous periodontal pathogens is viewed as a majorcriteria for successful periodontal therapy. Systemic antibi-otics may be used as adjuncts to mechaniοal periodontaltherapy to reduce the levels of periodontal pathogens belo\Λ/
detectabΙe levels.
The requirement for the elimination of periodontal pathogensdoes not appear to be absolute as clinical improvements inplaque levels, inflammation, probing depths, and attachmentlevels may be achieved \Ιvith scaling and root planing whenpathogens are reduced, but not necessarily eradicated. Theobservations that the goals and obleοtives of scaling and rootplaning can be achieved by only reducing the numbers ofperiodontal pathogens supports the notion that a critical massof pathogenic bacteria are required before the host becomessusceptible to pΘriodontal diseases.
Control gingival inflammation. Scaling and root planing willpredictably reduce gingival inflammation. As it has been withother clinical measures of successful scaling and rootplaning, the instrumentation must be subgingival to achievethis outcome. Hand, sonic, and ultrasonic instruments appearto be equally effective in reducing gingival inflammation(Figure 10).
F|GUFiE 10. The effect of subgingival scaΙing and root planing on gingivalinflammation (bleeding). Greater reductions in gingivai inflammation maybe expected after the instrumentation of deeper pockets. (With ρermission,cercek, et al, J clin Periodontoι, 1983' 10:46-56)
What ls Soft Tissue Management (STM)?
ln its broadest sense, STM refers to local mechanical andchemotherapeutic approaches to improving and controllingperiodontal health. Αs such, oral hygiene instructions, the useof antimicrobial agents as mouthrinses or crevicular irrigants,subgingival scaling and root planing with hand- and power-driven instruments, correcting unserviceable dental restora-tions, and supragingival coronal polishing are importantelements of STM. STM bears striking resemblance to thetypical initial therapy periodontal treatment plans that havebeen used successfully for inflammatory periodontal diseasecontrol and that are included inthe Parameters of Care. STΜshould be limited to the management of gingivitis and slightperiodontitis with <2 mm of clinical attachment loss wherebacterial deposits on teeth are usually accessible and can beremoved efficient|y and effectively. Root οoncavities, rootgrooves, furcation invasions, and other anatomical factorsthat could affect the completeness of debridement are usuallynot an issue in these cases. Moderate periodontitis (3 or 4mm of clinical attachment loss) and severe periodontitis (>5
mm clinical attachment loss) cases should be οonsidered forreferral to a periodontist vι/here issues of force control,surgical access, pocket elimination, regeneration of lostattachment, and gingival augmentation can be addressed byclinicians trained and experienced in the management ofadvanced periodontitis.
-

NoNsURGlcAL THERAPY: scALlNG AND Rooτ PLANING. occLUsAL AND ANTlBloτlc τHERAPγ
Chairside diagnostic instruments that measure volatiΙe sulfurcompounds, periodontal pocket temperatures, and themotility of pocket bacteria have been used in patient educa-tion STM. These methods are not described inΙhe Glossaryof Periodontal Termsnor are they included inthe Parametersof Care.
Scaling and root planing are fundamental procedures innonsurgiοal periodonta| therapy. The target of sca|ing androot planing is the removal of subgingival bacteria and theremoval of affected cementum. The effectiveness of scalingand root planing is limited by root anatomy, pocket depths,the skill and experience of the provider, and the overallsystemic health of the patient. Τhe outcomes of scaling androot planing include lowered plaque scores, reduοed gingivalbleeding scores, gain in periodontal attachment, gingivalrecession, and reductions in probing depths. lnstrumentationof root surfaces must be subgingival in order to aοhieve theseresults.
ln mild and some moderate chronic periodontitis cases, theclinical outcomes of scaling and root planing may precludethe need for periodontal surgery.
OCCLUSAL THERAPY
What ls Occlusal Traumatism? How DoesOcctusal Traumatism Conform to the Definitionof a Disease?
ln occlusal traumatism, the etiologic factor is any force inexcess of the adaptive capacity of the periodontium, themorbid pathobiologic event is injury within the periodontalligament and alveolar bone, and the signs and symptoms arepain, mobility and/or fremitus, pathologic migration of teeth,excessive occlusal wear, and widening of the periodontalligament space in radiographs.
Αs defined in the G/ossary of Periodontal Terms, occlusaltraumatism is the "functional loading of teeth" (force isprimary etiologic factoQ, usually off-axis, that is of sufficientmagnitude (excess of the adaptive capacity) to inducechanges to the teeth (eg, fractures, occlusal wear) orsupporting structures (inflammation in the periodontal liga-ment and alveolar bone, also known as the "lesion of traumafrom occlusion"). The changes may be temporary (reversible)or permanent (irreversible).
What is Adaptive Capacity? What Factors Affectthe Adaptive Capacity?
Adaptive capacity is the ability of the teeth and tissues of theperiodontium to sustain the effects of, or adapt to, forcesacting on the periodontium νvithout injury. The adaptivecapacity is affected quantitatively and qualitatively by localand systemic contributing factors. When it is exceeded,occlusal traumatism occurs.
Τhe etiologic forces that produce occlusal traumatism maynot always be occlusal in nature, but they may be generatedby orthodontic or prosthodontic appliances and/or habits of
compulsion, such as pipe smoking or fingernail biting. Themore inclusive designation, periodontal traumatism, ispreferred by some over occlusal traumatism because it
allows for nonocclusal forces and occlusal forοes as etio|ogicfactors.
What ls the Nature of the lnjury to thePeriodontal Attachment Apparatus Produced byForces Acting on τeeth? What ls PrimaryOcclusal Trauma and Secondary OcclusalTrauma?
The injury to the periodontium caused by forces acting onteeth is called the lesion of trauma from occlusion or moresimply, occlusal trauma.
o Τhe lesion of trauma from occlusion is located withinthe periodontal ligament in areas \Λ/here the ligamentis either under pressure (crushed) or under tension(torn) (Figure 11). The οrush or tear produces a phys-ical injury resulting in local necrosis of the periodontalligament and a typical inflammatory response. Thehistologic appearance of the periodontal ligament isdesοribed as "hyalinization", or a decrease in thecellular component of the tissue. Resorption ofnearby alveolar bone also occurs as an outcome ofthe inflammation. The resorption will occur on theperiodontal ligament side of the alveolar bone properwith mild injury (frontal resorption) and/or on themarroνv surfaces of the supporting alveolar bone(rear resorption). The degree of necrosis, inflamma-tion, and resorption will depend upon the amount offorce acting on the teeth and the adaptive capacity ofthe periodontium (see Figure '12).
FIGURE 11. A line drawing showing the reciprocal areas of crush and tear(ιightnin9 bolts) of a p€riodontal ligament when excessive nonaxial forcesare applied to a tooth. τhe tooth rotates within the alveolus around a pointcenter of rotation located within the root.
52
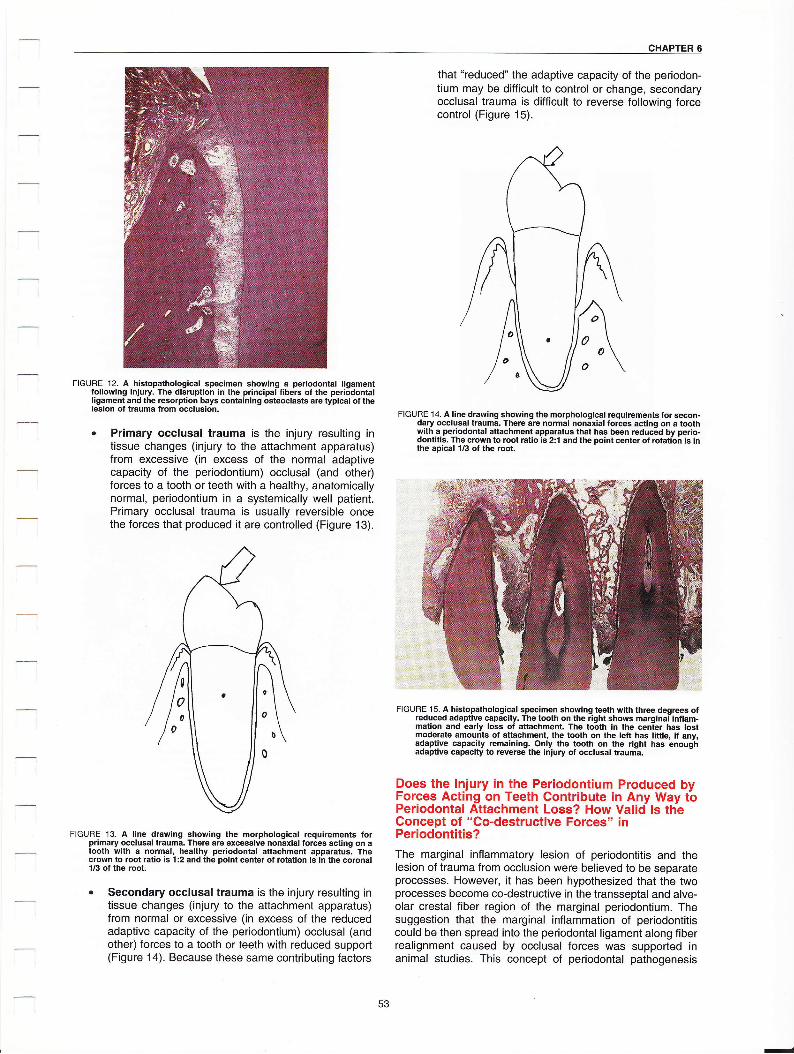
CHAPτΕR 6
that "reduced" the adaptive capacity of the periodon-tium may be difficult to control or change, secondaryocclusal trauma is difficult to reverse following forcecontrol (Figure 15).
F|GURE 12. A histopathologicaΙ specimen showing a periodontal ligament,ollowing iniury. τhe disruption in the principal fibe.s of the periodonta|ligament and the resorption bays containing osteoclasts are typical o, thelesion of trauma from occlusion.
. Primary occtusal trauma is the injury resulting intissue changes (injury to the attachment apparatus)from excessive (in excess of the normal adaptivecapacity of the periodontium) occlusal (and otheQforces to a tooth or teeth With a healthy, anatomiοallynormal, periodontium in a systemically well patient.Primary occlusal trauma is usually reversible oncethe forces that produced it are controlιed (Figure 13).
FIGURE 13. A line drawing showing the morphological requirements folprimary occlusal trauma. τhere are excessive nonaxial forces acting on atooth with a normal, healthy periodontal attachment apparatus. τhecrown to root ratio is 1:2 and the point center ot totation is in the coronal1/3 ot the root.
ο Secondary occlusal trauma is the injury resulting intissue changes (injury to the attachment apparatus)from normal or excessive (in excess of the reducedadaptive capacity of the periodontium) ocοlusal (andotheQ forces to a tooth or teeth with reduced support(Figure 14). Because these same contributing factors
FIGURE '14. A line drawing showing the morphological requirements for secon-dary occlusal taauma. τhere a.e normal nonαial forces acting on a toothwith a periodontal attachment apparatus that has been reduced by perio-dontiιis. τhe crown to root ratio is 2:1 and the point center of Joιation is inthe apical 1/3 of the .oot.
F|GURE 15. A histopathological specimen showing tΦth with lhree degrΦs ofreduced adaptive capacity. τhe tooth on the right shows marginal inflam-mation and earΙy loss of attachment. τhe tooth in the cenier has lostmoderate amounts of attachmeπt, the tooth on the left has little, if any,adaptive capacity remaining. Only the tooth on the right has enoughadaptive capacity to reverse the iniury of occlusal trauma.
Does the lnjury in the Periodontium Produced byForces Acting on τeeth contribute in Any Way toPeriodontal Attachment Loss? How Valid ls ttieConcept of "Co-destructive Forces" inPeriodontitis?The marginal inflammatory lesion of periodontitis and thelesion of trauma from occlusion were beΙieved to be Separateprocesses. However, it has been hypothesized that the tνvoprocesses become co-destructive in the transseptal and alve-olar crestal fiber region of the marginal periodontium. Thesuggestion that the marginaΙ inflammation of periodontitiscould be then spread into the periodontal ligament along fiberreaΙignment caused by occlusaΙ forces was supported inanimal studies. This concept of periodontal pathogenesis
53

Ξ
NoNsURGlcAL THERAPY: scALlNG AND Rooτ PLANING. occLUsAL AND ANτlBloTιc τHΕRAPY
conflicted οritically \Λ/ith the c|assic periodontitis model \Λ/here
marginal inflammation was depicted as following perivascularconnective tissue directly into alveolar bone marrow, andwhere the periodontal ligament \Λ/as typically free of inflam-mation.The projected outcomeof this "co-destructive" processwas the formation of angular bony defects and infrabonypockets Seen οommonly in periodontitis (Figure 16)'
FIGURE 1 6. A photomicrograph showing an angular orientation of transseptalfiber apparatus and a corresponding anguιar pattern of interdental boneloss. According to the co-destructive model, marginal inflammation andocclusal trauma could have been cofactors in its pathogenesis.
Studies in both animals and humans have not been able tocompletely demonstrate the role of occlusal trauma in perio-dontitis' While it is unclear νvhether potentialΙy destructiveocclusal contacts have any impact on the severity of perio-dontitis, there is agreement that two of the recognized signsof occlusal traumatism (eg, mobility and widened PDLspaces) are associated with greater amounts of attachmentloss, pocket depth, and bone loss.
What Are the Clinical Signs and Symptoms ofocclusal Τraumatism?
The cliniοal signs and symptoms of injury in the periodontalligament are commonly:
1. Pain or discomfort around one or more teeth onpercussion, function,and/or parafunction. Pain is oneof the four cardinal signs of inflammation (doΙor/pain,οalor/heat, rubor/redness, and tumor/swelΙing). Painthen is a sign of inflammation in the periodontal liga-ment.
2. Tooth mobility as determined with bidigital manipu-lation of teeth using the handles of 2 hand instru-ments. One handle is placed on the buccal surfaceand the other is placed on the lingual surface of clin-ical crowns. Tooth mobility is defined as "visiblyperceptible movement of a tooth away from its normalposition when a light force is applied."
Tooth mobility may be physiologic (ie, horizontalmovement limited to the width of the periodontal liga-ment), or pathologic (ie, horizontal and/or verticalmovement beyond the expected boundaries of theperiodontal ligament). Mobility occurs when fibers of
the periodontal ligament are injured or destroyed byinflammation resulting from excessive forces actingon teeth' lt will also oοcur when the adaptive capacityof the periodontium has been altered by marginalinflammation or systemic disease. Mobility iscommonly observed when a tooth has reduced perio-dontal attachment.
The Miller cΙassification scheme for tooth mobility isas follows:
- Grade (degree) Ι. The slightest distinguishablemovement in a horizontal direction. Tooth mobilityis classified as physiologic mobility.
- Grade (degree) ll. Movement in a horizontal direο-tion of a tooth within t mm of its normal position.
- Grade (degree) lll. Movement of a tooth in a hori-zontal direction greater than 1 mm from its normalposition. Grade lll mobility also includes teeth thatare depressible and/or can be rotated in theirperiodontal support.
Fremitus as determined by palpable or visible move-ment of teeth under verticaΙ (axial) or horizontal(nonaxial) occlusal forces. Fremitus is detected usingfingertips placed on the crowns of teeth while thepatient occludes. Fremitus is "functional mobility."
Pathologic migration of teeth. Pathologic migrationof teeth usually occurs when teeth have lost theirnormal periodontal support due to periodontitis andsubsequently migrate from their normal position inthe dentition in response to occΙusal and nonocclusalforces (Figure 17).
FIGURE 17. A case of severe chronic periodontitis with secondaryocclusal traumatism. Loss of adiacent teeth and periodontal supportallow teeth to migrate away from forces acting upon them. Posteriorbite collapse and loss of vertical dimension of occlusion are alsosigns of advanced secondary occlusal traumatism.
5. Tooth loss
6. Posterior bite collapse. Posterior bite collapse isthe product of tooth loss and pathologic migration.
7. Widened periodontal ligament spaces aroundaffected teeth in radiographs. Widened periodontalligament (PDL) spaces usually indicate that an adap-tive response has occurred either to excessive forceon a normal periodontium or to normal or excessiveforces on a reduced periodontium. Widened PDLspaces together \ivith an intact laminadura suggestthat repair occurred following injury (Figure 18).
3.

CHAPτER 6
F|GURE 18- A radiograph of mandibuιar molars with severe bone loss.νιridened periodontal ligament spaces in radiographs are signs ofocclusal traumatism. The retained third molar is probably a contrib-uting factor to the degree of periodontal attachment loss.
What ls the Basis for Force Control and OcclusalTherapy?
The essence of occΙusal therapy is to treat the lesion oftrauma from occlusion and to create an environment that willallow the injured attachment apparatus to repair itself withinthe limits imposed by the adaptive capacity of the host. lt isnot a form of therapy for periodontitis. There is someevidence to suggest that periodontitis patients who receiveperiodontal inflammatory disease control therapy along withocclusal adjustment will display minor (<l mm) gains inattachment compared to those who did not receive oοcΙusaladjustment.
Repair to the attachment apparatus will depend directly uponthe effectiveness of force control and indirectly upon theeffectiveness of improvements in the adaptive capaοitybefore force control (ie, control of marginal inflammation andcontrol of diabetes mellitus).
What Are the Components of a Force ControlTreatment Plan for a Periodontal Patient? WhatDetermines Which Component Is Appropriate ina Given Case? How Are the GomponentsSequenced?
A typiοaΙ force control treatment pΙan for a patient with thediagnosis of generaΙized moderate chronic periodontitis withocclusal traumatism would be:
. Re-evaluation of inflammatory disease control. Αfter aminimum of 4-6 weeks (the time for repair of the dento-gingival junction), the patient is re-examined and theresults of that examination are compared with thoserecorded at the initial examination. This is a critical stagein treatment as decisions about the working diagnosisand continuing active therapy are made depending uponthe answers to the foΙlowing questions:
1. Are there any persistent signs and symptoms ofgingival inflammation or debris present?
2. lf so, is there anything shott of periodontaΙ surgerythat can be done to improve the conditions?
ls there any residual tooth mobility/fremitus?
lf the answer to the first and second question is "no" andthe answer to the third question is "yes", the patient'sworking diagnosis of generalized moderate chronic perio-dontitis with occlusal traumatism is supported, and treat-ment should proceed to the occlusal therapy phase.
Ιf, however, the answer to the first and second question is"yes", then considerations for improving the patient's oralhygiene, refining scaling and root planing, institutingantimicrobial therapy, additional correction of plaqueretentive factors, and discussions concerning progressmade in smoking cessation might be appropriate.
Αssuming that the ansνvers to the first and second ques-tions are "no" and the answer to the third question is"yes", the next Step in treatment is to determine \Λ/hat isresponsible for the mobility and fremitus.
o Assessment of parafunctional occlusal habits of compul-sion.
What ls Meant by Parafunction? ts Bruxism aForm of Parafunction?
Parafunction is "abnormal function, as in bruxism". Bruxism(tooth grinding, occlusal neurosis) is "a habit of grinding,clenching, or clamping the teeth. The force generated maydamage both tooth and attachment apparatus." lt should beemphasized that bruxism occurs during vertical (clenching)and horizontal (grinding) nonfunctional movements of themandible. lt may occur during sleep (nocturnal bruxism) orduring waking hours (diurnal bruxism). Parafunctional toothcontacts tend to be repetitive and of greater force and dura-tion than the more random and 'Tleeting" functional toothcontacts.
ο Parafunction may have been established during thedental history. Not all patients are a\,vare of parafunctionalactivity, and therefore, an interview with the patient rarelyprovides reliable diagnostic information vis-a-visparafunction. lt has been estimated that only a fewpatients (20%) know they engage in parafunction. Mostpatients deny the activity, but when asked to duplicatejaw movements associated with parafunction, they willduplicate them easily. Stressful lifestyles, heavy occlusalwear facets on nonfunctional tooth surfaces, fracturedcusps, tooth mobility, hypercementosis, tenderness and/or hypertrophy of masticatory muscΙes, and |imitedmandibular opening are frequent "bedfellows" ofparafunction, and their presence in a given case couldhave diagnostic ramifications (Figure 19).
3.
-

NoNsURGlcAL THERAPY: SOAL|NG AΝD Rooτ PLAN|NG. occLUsAL AND ANτlBloτlc τHΕRAPY
ffir;..,r]r..:,r,L:.,.::, :::: L:;;. ' ,'.; 1:, I l:',1, .:l:',il::,ir'
FIGUFIE 19. A dried specimen of mandibular posterior teeth showingheavy Wear on supporting and nonsuppofting cusps. τhese wearfacets provide enlarged surface areas for occlusal contact and,thereby, potentially increase the forces acting on teeth duringparafunction.
. Occlusal analysis. ldeally, the occlusal analysis shouldbe carried out on an adjustable articulator \Λ/ith the maxil-lary cast mounted on the hinge axis on an anatomical arti-culator, and the mandibular cast should be mountedin centric relation.Alternatively, the analysis may beperformed in the mouth' ln either case' occΙusal contactsshould be recorded along the operator-guided, patient-generated, movements of the mandible that originate incentric relation.
How ls Force Control Achieved for a PeriodontalPatient?
Force control in a patient with occlusal traumatism may beachieved by occlusal adjustment of the natural dentition(occlusal adjustment), removable appliance therapy (nightguards), removable and fixed provisional splint therapy,orthodontics, and fixed restorative dentistry. Τhis chapter willdiscuss general guidelines for occlusal adjustment and appli-ance therapy for cases of moderate chronic periodontitis withocclusal traumatism that can usually be managed effectively\Λ/ith these two traditional forms of force control. The occlusalmanagement of advanced periodontitis cases that displayposterior bite collapse, loss of occluding vertiοal dimension,and skeletal malocclusions that will require the coordinatedefforts of combined periodontal, prosthodontic, and ortho-dontic providers will not be discussed here.
What Are Occlusal Adlustment and OcclusalAppliance Therapy?
Occlusal adjustment is the reshaping of occlusal surJaces ofteeth by grinding to create harmonious contact relationshipsbetνveen upper and lower teeth. This process is also knownas occlusal equilibration or seΙective grinding' The term odon-toplasty is commonly used to describe the act of ocοlusaladjustment/oοclusal equilibration/selective grinding. Theguiding principals of occlusal adjustment are the preservationand refinement of supporting cusp tips in centric ocοlusionand the elimination of lateral interfering centric and excursivecontacts. Wear facets are also eliminated by vertical groovingand rounding of edges to reduce the tooth contact surfacearea during parafunction.
. Occlusal adiustment. lt is axiomatic that the muscles ofmastication be free of myospasm or other functionaldisorders before occlusal adjustment is performed.Spastic, splinted muscles occur in response to noxious orinjurious tooth contacts and result in neuromuscularpatterns of jaw movement that "avoid" the offending toothcontact(s). These same οontacts may be the targetcontacts of occlusal adjustment, and it is pointless toadjust an occlusion νvhen target contacts cannot berecorded. Stressful life-styles or events commonlyprovide a psychic background for myospasm (Figure 20).
FIGURE 20. A clinical photograph showing occlusal adiustment of acentric interference by coronoplasty. Flame shaped or conical highspeed rotary instruments are ideal for the reduction of inclines andfacets.
Pain or tenderness in the masseter, temporalis, or lateralpterygoid muscles, hypertrophy of the masseter muscles,limitation in opening the ja\Λ/S, and/or Subconscious resis-tance to movement of the mandible in hinge-axis andborder movements are signs of myospasm. The applica-tion of heat to the affected muscles, and the use of ananterior bite-plane appliance for 1-2 weeks is usually allthat is required to "deprogram" avoidance patterns andultimately relieve the myospasm. Patients who are refrac-tory to this noninvasive therapy may have a more seriousform of myofascial pain dysfunction (MPD) syndrome orother temporomandibular joint (ΤMJ) disease' Patientsvι/ith refractory pain and dysfunction will require care by aspecialist and should be referred for treatment as soon aspossible.
Detailed methods of occlusal adjustment are presented instandard periodontics and occlusion textbooks.
Occlusa! appliance therapy.
1. The primary function of appliance therapy in perio-dontal patients is force control in secondary occlusaltrauma. Αdditional benefits from occlusal appΙiancesin periodontitis patients incΙude splinting of teeth inthe appliance, control of super-eruption, andanchorage for minor tooth movement. Typically, theforce control appliance will provide fulΙ occlusalcoverage of either the maxillary or mandibular teeth.The decision over which arch will be chosen for appli-ance therapy will be affected by Angle's classifica-tion, the location of teeth that might require splinting,and the location of teeth that need to be controlled forsuper-eruption. Wrought wire clasps and the anteriorHawley appliance wire are unnecessary unless the
56

CHAPTΕR 6
appliance is modified to accomplish anchorage fororthodontics. Τhe occlusal scheme for full occlusalforce control appliances is maximum οuspal contacton the flat occlusal surfaces of the guard in centricrelation and all excursions. Because there are noindentations for cuSp interdigitation, full occΙusaΙappliances do not have a centric occlusion. As suοh,they have been proven io be effeοtive in the long-term maintenance of muscle "deprogramming." Theyare not recommended for initial deprogramming ofsplinted muscles of mastication (Figures 21Α and B).
FΙGURE 21Α' A clinical photograph of a fuιl occlusal maxillary appliancefor force control. The appliance is designed to produce a minimalincrease in the vertical dimension of occlusion.
F|GυRE 21B. The appliance Will provide maximum occlusaΙ contact in allexcursiοns. Ιt will also provide intra-arch splinting of teeth duringparafunction,
2. ln patients who have a normal periodontium anddemonstrate heavy occlusal wear of parafunctionalorigin, or who have a history of fracturing restorationsor teeth, an occlusal/night guard may be prescribedaS an ablative shield. Force controΙ may not be aSmuch of an issue in these patients as tooth protec-tion, particularly in cases where teeth have normalamounts of periodontal support. This applianceallows the patient io continue engaging in parafunc-tional aοtivity withoui additional occlusaΙ wear.lnstead of irreversible tooth \η/ear as a consequenceof parafunction, the appΙianοe is ablated.
3. ln patients who have mild MPD and where muscledeprogramming is required before occlusal adjust-ment, an anterior bite plane may be constructed
covering the lingual surfaces of the six maxillary ante-rior teΘth. A Hawley labial wire is οommonΙy includedin the appliance to stabilize tooth position. A lingualplatform establishes occlusal contact with the sixmandibular anterior teeth, increases the occludingvertical dimension, and "discΙudes'' all posterior teeth.The net effect of this appliance is that noxious toothcontacts are prevented while the patient wears theappliance. The expected outcome should be thereduοtion of myospasm in the muscles of mastication(Figures 22A and 228).
F|GURE 22Α. A clinical photograph of an occlusal appliance with aHawley wire. τhis appliance is best suited for short periods ofmuscle deprogramming.
F|GURE 22B. τhe anterior bite plane makes contact with ιhe mandibularanterior teeth only. Poslerior teeth not contained in the appliance aresubiect to supraeruption.
Because anterior bite plane appliances are reasonablysimple to fabricate and usually require less chair time toadjust than the full occlusal appliances, it is tempting touse these appliances for longterm force control. Oneconsequence of this approach may be the extrusion of un-opposed teeth and unexpected additional occlusal prob-Ιems. Ιt is recommended ihat anterior bite-planeappliances be used only for short{erm muscle depro-gramming.
Force control has been a tradition in the treatment ofperiodontitis. lnitially, it was believed that forces acting onteeth produced gingival recession and attachment lossand that periodontal therapy was incomplete unlessthese forces were eΙiminated or at least οontrolled.Today, the paradigm is that occlusaι trauma and marginal
57

Ξ
NONSURG|CAL τHERAPY: SCAL|ΝG AND RooT PLANING, OCCLUSAL AΝD ANτlBloTlC THERAPY
periodontal diseases are probably distinct clinical entities.occlusal trauma iS treated !η/ith force control and perio-dontitis is treated by infection control.
The sequence of treatmΘnt for each is critical. Effeοtivetreatment of marginal periodontal inflammation maydecrease some of the Signs and symptoms of oοc|usaltrauma. ln addition, reactive repositioning (closure ofopen contacts) may take place after inflammatorydisease control. There is also evidence that untreatedinflammatory disease may impact negatively on therepair of occlusaΙ trauma. |n some cases, occlusaltherapy may not be necessary after inflammation control.
ANTIBIOTIC THERAPY
What ls Anti-infective Periodontal Therapy?
Anti-infective theraρy is the use of local and systemicagents to control the bacterial etiology of the inflamma-tory periodontal diseases. τhese agents include bothlocally and systemically delivered antibiotics and chemo-therapeutic agents.
When Are Antibiotics lndicated in PerΙodontalTherapy?
lndications for the use of antibiotics in periodontal therapyinclude the following:
ο PeriodontaΙ abscess (see chapter on "PeriodontalEmergencies" on page 105.)
. Aggressive periodontitis
- Juvenile periodontitis
- Rapidlyprogressiveperiodontitis- Prepubertal periodontitis
ο Chronic periodontitis with persistent severe gingivalinflammation
ο Refractory forms of chronic or aggressive periodon-titis
o Protection vs subacute bacterial endocarditis
. When surgical therapy is contraindicated
ο To control local sites of inflammation
ο As an adjunct to conventional mechanical therapy
ο Subantimicrobial dose of doxycycline to stabilizecollagenase activity
What Antibiotics Are Commonly UsedSystemically in Periodontal Therapy?
Τhe most commonly used antibiotics in periodontaltherapy are:
. Αmoxicillin (with or without οlavulanic acid -AugmentinΘ)
. Metronidazole
. Ciprofloxacin
o Clindamycin. Doxycycline
. Azithromycin
What Are Some of the Risks of UsingSystemic Antibiotics in Periodontal Therapy?
There are general and specific risks in the use of antibi-otics in periodontal therapy. These include:
ο AΙlergic reactions (delayed or immediate hypersen-sitivity)
o Gastrointestinal problems
ο Development of superinfections by unaffected orga-nisms
. Development of resistant bacterial strains
How ls the Appropriate Antibiotic RegimenChosen?
It is preferable that the bacteria associated with theinflamed sites have been identified before the selection ofantibiotic therapy. Bacterial identification may be accom-plished by culturing the bacteria from within the pocket orby using DNΑ probe identification technology. Theadvantage of culturing is that sensitivity of the identifiedbacteria to specific antibiotics can also be reported. Themajor advantage of DNA probe technology is that viablebacteria are not needed to identif y the peri-odontopathogens.
Antibiotics are prescribed without identifying the asso-ciated microorganisms and the patient is monitored forfor clinical success. The major risks in this approachare the selection of an antibiotic to which the pathogenis resistant or the development of a superinfection causedby an unidentified and unaffected bacterial strain.
What Are the PrincΙpIes of Antibiotic Dosing?
. Employ high doses for a short duration
. Use an oral antibiotic loading dose, especially withthe tetracyclines or \Λ,ith an acute infection
ο Achieve blood levels of the antibiotic at 2-8 timesthe minimal inhibitory concenιration
. Use frequent dosing intervals, particularly with anti-biotics with a relatively short half-life
ο Determine the duration of therapy by the remissionof disease
What Are the Potential Problems With Druglnteractions?
Depending on the mechanism of antibiotic action, combi-nations of antibiotics may have an additive, synergistic, orantagonistic effect. Static antibiotics used in combinationgenerally exhibit an additive effect, bacteriocidal antibi-otics exhibit a synergistic effect, and the combination ofbacteriocidal and bacteriostatic agents exhibit an antago-nistic effect. Antibiotics may also react \Λ,ith other medica-tions the patient may be taking or interact with certainfoods (eg, tetracycline chelating with calcium or otherdivalent cations). lndividual drug interactions can befound in the section on specific agents below.

cHAPτER 6
What Are Some Gommon Dosing Regimensfor Systemic Antibiotic Use in PeriodontalTherapy?
Arriving at an appropriate antibiotic selection and dosingregimen is an inexact science. lndividual antibiotics orcombination therapy may be selected depending onwhether or not the infection seems to be οaused by onebacterial species or is a mixed infection, as most perio-dontal infections tend to be. ProtocoΙ selection maydepend on the practitioner's knowledge, previous experi-ence, and perhaps by the most recent advertisement orsales representative to speak with the practitioner. Thesuggested regimens that follow are taken from recom-mendations of Dr. Thomas Rams, Director of the OralMicrobiology Testing Service at Τemple University and along-time researcher in the field of antibiotic therapy inthe treatment of the periodontal diseases. While there areother suitable regimens, these recommendations are agood starting point for those practitioners in need of guid-ance.
GUlDELlNEs lΝ τHE sELEcTloN oF sYsTΕMlcANTlBloτlcs lN PER]oDoNTAL THERAPY
Thomas E. Rams, DDS, MHSOral Microbiology Testing Service
Department of PeriodontologyTemple University School of Dentistry
Philadelphia, PΑ1-800-788-OMTS
Possible Antibiotic RΘcommendations for SpecificMicrobiological Test Findings*For οombinations of anaerobic and facultative perio-dontal pathogens:
1St choice: Metronidazole + amoxicilΙin or Augmentino(250 mg each TID for 5-7 days, or metronidazole 500mg and Αugmentin@ 875 mg each BlD for 5-7 days)
2nd choice: Metronidazole + ciprofloxacin (500 mg eachBID for 5-7 days)
(Note: Combination drug regimens are generallypreferred to single antibiotic administration)
* F or ActinobacilΙus actinomycetemcomitans:
1st choice: Metronidazole + amoxicillin or AugmentinΘ(250 mg each TID for 5-7 days, or metronidazole 500mg and Augmentino 875 mg each BID for 5-7 days)
2nd choice: Ciprofloxacin (adults only) alone or withmetronidazole (500 mg each BID for 5-7 days)
3rd choice: Azithromycin (500 mg/day for 3-5 days)
4th choice: Doxycycline (100 mg BID for 14-21 days)
*For anaerobic pathogens (Porphyromonas gingivalis,Prevotella intermedia, Bacteroides forsythus, Fuso-bacterium species, Peptostreptococcus micros, andCampylobacter speοies):
1st choice: Metronidazole + amoxicillin or AugmentinΘ(250 mg each TID for 5-7 days, or metronidazole 500mg and Augmentino 875 mg BID for 5-7 days)
2nd choice: Augmentin@ (250-500 mg TlD, or 875 mg BIDfor 7 days)
3rd choice: Metronidazole (500 mg BID for 7 days)
4th choice: Clindamycin (150 mg TID for 5-7 days)
5th choice: Αzithromyοin (500 mg/day for 3-5 days)
6th choiοe: Doxycycline (100 mg BlD for 14-21 days)
(Note: Some Fusobacterium strains may metabolizemetronidazole and reduce its efficacy; some Peρto-streptococcus mrbros strains are resistant to tetracy-clines, metronidazoΙe, and azithromycin; Prevotellaintermedia is often resistant to tetracycline antibi-otics.)
*For enteric rods, Pseudomonads, Εnterococci, andlorStaphylococci.
1st choice: Ciprofloxacin (usually given with metronida-zole - 500 mg eaοh BlD for 5-7 days)
2nd choice: Variable depending on strain susceptibility
-For beta-hem olyΙilc Streptococci.
1st choice: Augmentino (250-500 mg TID or 875 mg BIDfor 7 days)
2nd choice: Clindamycin (150 mg TID for 5-7 days)
What Are Some Common Reasons forAntibiotic Failure in Periodontal Therapy?
. lnappropriate choice of antibiotics (the microor-ganism is not susceptible to the antibiotic of choice)
ο lncorrect / inadequate doses
ο Emergenceof antibiotic-resistant microorganisms
o Too low a blood concentration of the antibiotic
. Slo\ν gro\Λ/th rate of the microorganisms
. lmpaired host defenses
ο Patientnoncompliance
ο Antibiotic antagonism (eg, using bacteriocidal andbacteriostatic antibiotics togethe0
o lnability of the antibiotic to penetrate to the site ofinfection
. Limited vascularity or decreased blood flow
ο Unfavorable local factors
o Failure to eradicate the source of infection
What ls Subantimicrobial Antibiotic Usage?
It has been demonstrated that tetracycline and the tetra-οycline derivative doxycycline (subantimiοrobial dose ofdoxycycline - SDD) can reduce collagenase activity \Λ/hen
used in doses too low to have any antimicrobial effect.The use of SDD has been shown to reduce the rate andamount of attachment loss associated with advancingperiodontal disease. SDD is currently used as a 20 mgdose of doxycycline t\ivice a day. Long-term studies have

NoΝsURGlcAL τΗERAPY: scALIΝG AND Rooτ PLANING. occLUsAL AND ANτlBloτlc τHERAPY
been for g-month durations. There is little data on the manufacturers provide detailed instructions, there is aeffectiveness of SDD therapy for longer periods of time. learning curve to developing an efficient technique for the
use of eaοh product.
What Are the lndications for the Use ofLocally Delivered Antibiotic and AntimicrobialTherapy? What Therapeutac Mouthrinses Are Available
to Reduce PIaque and Help Control Gingivalo Local site(s) with signs of inflammation that have not lnflammation?
responded to conventional mechanical therapy rt shourd be remembered that a mouthrinse must not onry
. Local site that has recurrent signs of inflammation at reduce plaque but also have a therapeutic effect.a maintenance visit Currently, long-term, 6-month studies support only the
use of mouthrinses containing 0.12% chlorhexidine. Buying time for a so-called hοpeless tooth before gluconate or the "essential oils" (phenolic compounds
extraction thymol, menthol, eucalyptol, methyl salicylate) to reduceplaque and gingivitis. These mouthrinses are available to
. Resolving marginal inflammation when oral hygiene consumers through a variety of manufacturers andhas reached maximum effectiveness distributors. τhese mouthrinses must be used appropri-
ately, usually a 3O-second rinse twice daily to be effec-tive. These rinses have an alcohol vehicle ranging from
What Are Some Common LocaI Antibiotic and 17"/o Ιo 26'7%'
Antimicrobial Delivery Systems?
ActisiteΘ - Tetracycline in a nonresorbable ,ethY| What Are other Periodontat Conditions That
-acetate fiber (1st generation' no longer availabie; r,,ray nequire Crremoillerapeuiic Treatment?
ArestinΘ - MinocycΙine in a resorbable bead vehicle . Vesiculobullous diseasesAtridox@ - Doxycycline in a resorbable polylactide gel - Benign mucous membrane (cicatriciar) pemphi-
PerioChipΘ - Chlorhexidine in a resorbable gelatin goid
wafer - Erythema multiforme
- Lichen planus
How Are These Local Antibiotics Delivered to * Pemphigus vulgaris
the Site of Choice? ο Viral infections
Each product is delivered in a different manner - Herpes simplexdepending on the delivery vehicle. Even though the - Human immunodeficiency virus
60

cHAPτER 7
CHAPTER 7: SURGICAL TREATMENT: PRINCIPLESThe treatment of periodontal disease has included someform of surgery for over 100 years. Early on, periodontalsurgery was performed to remove infected and/ornecrotic bone. By the middle of the 20th Century, thera-pists vvere more intent on performing periodontal surgeryfor pocket elimination or reduction. lndeed, most perio-dontal surgery performed during the 1950s and 1960swas resective in nature. The dominant philosophy of thetime \ivas that removal and reshaping of alveolar bonewas essential to assure that the pocket eliminationachieved during surgery would remain stable. ln the1970s, concepts of bone grafting emerged that chal-lenged the wisdom of removing bone to maintain shallowpockets when pocket reduction might be achieved bygraft mediated regeneration of lost periodontal tissues.Regeneration has become a predictable periodontalsurgical procedure and has eroded the once dominantrole of resective surgery in periodontics.
νvhat Are the Basic Principles of PeriodontalSurgery?
The basic principles of periodontal surgery are nodifferent than any other form of surgery.
Αbove all, periodontal surgery should do no harm to thepatient. ln addition, the surgery should:
. Be discussed, in alΙ aspects, in advance with thepatient
. Be understood, in all aspects, by the patient and thatunderstanding should be acknowledged as writtenconsent
ο Be as atraumatic as possible
. Be conducted in an aseptic environment
o Not exceed the limits of physical tolerance of thepatient in terms of discomfort, blood loss, and stress
. Produce a benefit for the patient
. Be actively monitored postoperatively to assureuneventful healing
What ls Meant by Periodontal Surgery? WhatAre the Categories of Periodontal Surgery?
The term surgery describes that branch of medicalscience that is concerned with the treatment of diseasesor injuries by means of manuaΙ or operative methods.Periodontal surgery is any surgical procedure/operationused to treat periodontitis or modify the morphoΙogy ofthe periodontium. Subcategories of periodontal surgerybased upon expected outcomes incΙude:
. lmplant surgery, defined as operations concernedwith the placement, uncovering, and removal ofdental implants. τhe repair and modification of softand hard peri-implant tissue are viewed as implantsurgery.
. Osseous surgery, defined as operations that modifybone aΙtered by periodontal diseases by eitherreshaping or removing alveolar bone. The relation-
ship of the cementoenamel junction to the crest of thealveolar bone is usually changed by osseous surgery.
o Reconstructive surgery, sometimes called regenera-tive surgery, defined as operations that restore abody part to a more normal appearance or funοtion.
. Mucogingival surgery, defined as proceduresdesigned to correct defects in the morphology orposition of the dentogingival junction. Mucogingivalsurgery is also used to augment the dimensions ofthe dentogingival junction.
o Re-entry surgery, defined as a second stage opera-tion performed to improve, enhance, or evaluate theresults obtained from a previously performed proce-dure.
When ls Periodontal Surgery Necessary?What Are the Diagnostic and Therapeuticlndications of Periodontal Surgery? Are ThereAny Contraindications to PeriodontalSurgery?
The necessity for periodontal surgery is outlined in thefollowing three basic goals/objectiyes. Periodontalsurgery wil!:
. Provide access to root surfaces exposed to periodon-titis for root debridement
ο Provide access to periodontal bony defects forcorreοtion by osseous or regenerative procedures
o Provide an opportunity to remove periodontaΙ tissueinfected by periodontal pathogens
The therapeutic indications tor periodontal surgical proce-dures may be any combination of the following:
ο Allow more efficient and effective Scaling and rootplaning
. Reduce or eliminate periodontal pockets
o Remove inflamed periodontaΙ tissue
. Remove gingival overgrowths
ο Create an environment that will Support regenerationof new attachment or a new attachment apparatus
ο Correct mucogingival deformities that require rootcoverage or gingival augmentation
. Create a periodontal environment that will fosteroptimal oral hygiene
. lmprove periodontal aesthetics
. Establish a periodontal environment that supportsfixed and removable restorations in health andcomfort
The diagnostic indications of periodontal surgery are:
. Biopsies
. Exploratory fΙap procedures
Periodontal surgery is contraindicafed when:
. The surgery that has been proposed is not in the bestinterest of the patient. Recommendations for surgery
61
-

sURGlcAL TREATMEΝT: PRlNclPLES
should be based upon the patient's needs and not onthe experience or skill leveΙ of the provider. lf theprovider cannot satisfy those needs, the patientshould be referred to a qualified provider.
There will not be enough time following the surgery toperiodically monitor healing and therapeutiοoutcomes. Postsurgical treatments and evaluationsshould ocοur regularly during the first 3 months ofhealing.
There are significant health considerations for thepatient.
The patient has a history of cigarette smoking.Smoking remains the number one environmental riskfactor in periodontitis. lt is also associated \Λ/ith pooroutcomes from periodontal regeneration and dentalimplant surgery. The decision to perform periodontalsurgery for a smoker should be made only after thepatient ackno\Λ/ledges the surgical risks on aninformed consent document. Counseling on smokingcessation is an essential component of initial perio-dontal therapy.
Following initial therapy, inflammatory disease andplaque control are inadequate. Surgery should not beperformed in a plaque-infected periodontium!
The periodontitis has been so severe that the sur-gical risks exceed expected benefits. Surgery tosave hopeless teeth may affect the prognosis ofpotentially salvageable teeth. Τooth removal may bea more reasonable option.
What ls Aseptic Technique? Can Asepsis BeAchieved in the Oral Cavity?
Asepsis means free from infection or septic material. ltalso means sterile (ie, without life). Αseptic techniquerefers to a method/protocol whereby asepsis is achievedand maintained during a surgical procedure. Rigidaseptic protocols as practiced in hospital operating roomscannot be achieved in periodontics, or for that matter, inany discipline that involves the oral cavity.
The purpose of an aseptic technique in periodontalsurgery is to prevent the introduction of environmentalbacteria into periodontal surgical !η/ounds. The potentialsourοes of contaminating organisms are the operatory,the personnel who perform the surgery, the patient, andthe instruments used during the surgery. τo assure thatthese potential sources of contamination are controlΙed,the aseptic teοhnique for periodontal surgery must occurat 4 levels. They are:
. Preparation of the personnel. lndividuals involvedin periodontal surgical procedures should be trainedin the rationale and the teοhnical aspects of theaseptic technique. The training should incΙude: Αnunderstanding of barrier protection, gowning andgloving teοhniques, and the discipline of maintaining
sterility of barriers and instruments. Principles of theaseptic technique should be formally reviewed andupdated at least annually.
lndividuals directly involved in the procedure chair-side should vvear a clean surgical mask, a cleansurgical cap, a sterile surgical gown, and sterilesurgical gloves. Once gowned and gloved, thesurgeon and the chairside assistant must not lo\,vertheir hands below their \ivaists or contact nonsterilesurfaces (Figure 1). lndividuaΙs who will "circulate" orassist in the operatory to adjust Mayo stands andinstrument trays, "drop" instruments and supplies,adjusVregulate power-driven instruments, etc mustWear a clean οap, mask, and examination gΙoves.Circulating assistants must also be alert for acci-dental breaches in aseptic technique anywhere in theoperatory.
F|GUHΕ 1. Aseptic τechnique for surgical Personnel. τhe surgeon andthe assistant must wear a clean mask, a clean hair cover, and sterilesurgical gloves. τhe patient's chest and abdomen are covered withsterile surgical drapes. Light handles must be covered with sterilealuminum foil.
. Preparation of the operatory. The dental operatorymust be as clean as any hospital operating room.Surfaces, including the floor, must be cleaned anddisinfected before and after each procedure. Theantiseptic agent must be used according to theprotocol suggested by the manufacturer andapproved by state and local health agencies.Surfaces that will be touched by the surgeon or assis-tant during the surgery (eg, light handles, watersyringes, handpieces, hoses, etc) must be wiped withantiseptic and wrapped with sterile aluminum foilbefore the procedure begins.
The water used to irrigate the wound or cool instru-ments should be sterile, and dental unit water linesshould be treated regularly \Λ,ith antiseptic agents toprevent biofilm formation (Figures 1, 2, and 3).
. Preparation of the patienι. τhe patient should bedressed in loose-fitting, comfortable clothing. Whenthe patient is seated in the chair, the perioral tissuesshould be washed \,vith an antiseptic soap. Oncepositioned for the procedure, the patient's head, hair,and eyes should be wrapped and covered with steriledrapes. The patient's torso, shoulders, arms, andhands shouΙd be covered with sterile drapes duringthe surgery (Figures 1, 2, and 3).

CHAPτER 7
FIGURE 2. Aseptic Technique for the Patient and Operatory. The patient'shair and eyes are covered with sterile surgical drapes. Air and waterlines must be covered with sterile aluminum foil.
FlGURE 3. Aseptic τechnique for the operatory. Working surtace such asMayo stands and bracket tables must be covered with sterilesurgical drapes" Ηand pieces and ultrasonic instruments must becovered with sterile aluminum foil. τhe water used in high-speedrotary and ultrasonic instrumentation must be steriΙe as well.
o Preparation of the instruments. All instrumentsused in the surgical field must be individually wiped toremove debris and then ultrasonically cleaned in anantiseptic solution. They must then be dried, pΙacedin cassettes, wrapped, and autoclaved.
What ls a Periodontal Flap? What Are theTechnical Features That Are Shared by AllPeriodontal Flap Procedures?
A periodontaΙ flap is a Segment of marginal periodontaltissue that has been surgically separated coronalΙy fromits underlying support and blood supply and attachedapically by a pedicle of supporting vascular connective
tissue. All periodontal flaps have four critical sιages incommon. They are:
lncision of marginal attachment
Elevation by sharp or blunt dissection
Placement or repΙacement
Protection
What Are Partial Thickness and Full ThicknessPeriodontal FIaps?
FuΙl thickness periodontaΙ flaps include the surfacemucosa (defined as epithelium, basement membrane,and connective tissue lamina propria) and the οontiguousperiosteum of the underΙying alveolar bone. FulΙ thick-ness flaps are usually elevated by blunt dissection usinga periosteal elevator, and alveolar bone is temporarilyexposed during the procedure. ln the process, the bloodsupply to bone provided by the periosteum is severed.νvhile the blood supply is re-established during healing,infΙammation and associated bone resorption (locaΙizedalveolar osteitis) may produce a permanent deformity inalveolar bone height and width. Full thickness periodontalflaps are used for osseous resection and periodontalregeneration procedures (Figure 4).
FIGURE 4. A Clinical Photograph of a Full-Thickness Mucoperiosteal Flap.A scalloped internal bevel envelope incision was used and all of thegingiva was preserued to facilitate wound closure. Alveolar bone isdenuded temporarily. τhe full-thickness periodontal flap providesoptimal access for scaling, root planing, and debridement of perio-dontal deformities.
A paιtiaΙ thickness f/aρ includes only the mucosa, whichiS separated from the periosteum by Sharp disseοtion.Alveolar bone is not exposed. Τhe major advantage of apaιtial thickness flap is that the blood suppΙy to the alve-olar bone surface is not disturbed, and, the localizedosteitis and bone resorption observed during the healingof fu|l thickness flaps is minimized. Τhe major disadvan-tages of paιiial thickness flaps are the technical difficultyrequired to perform the procedures successfulΙy and thehigh probability of perforation. The vascularity of theretained periosteum is a frequent source ofintraprocedural bleeding and the limited visibility of perio-dontal defeοts it produces (Figure 5)'
a
o
a
o

sURGlcAL TREATMENT: PRlNοlPLES
FlGURΕ 5. A clinical Photograph of a Partiaι τhickness Mucosal Flap. Αscalloped internal beveΙ incision was used to separate mucosa tromunderlying periosteum. Alveolar bone remains covered with retainedperiosteum. The partial lhickness flap provides adequate access toroot surfaces for scaling and root planing. Partial thickness flaps areprone to perforation and tears.
A variant of the partial thickness flap is the periostealretention procedure. PeriosteaΙ retention is basic to recip-ient sites for free autogenous sofi-tissue grafts andvestibular deepening procedures, such as the periostealfenestration or the periosteal separation (Figure 6).
FIGURE 6. A Clinical Photograph of a Periosteal Retention ProcedureUsed to Prepare a Recipient site for a Free Autogenous Soft-τissueGraft' τhe incision for the mucosal flap in this case was made at themucogingival junction and the remnants of the marginaΙ gingivahave been removed. lniury to the mental nerve is always a riskduring periosteal retention procedures in the mandibular premolarregion.
What Types of lnitial lncisions Are Made inPeriodontal FIap Surgery? What ls anEnvelope Flap? What ls Crestal Anticipation?lnitial incisions in periodontal flap surgery are horizontaΙinternal beyel incisions. The incision line will begin eitherin the sulcus, at the gingival margin, or at a submarginalpoint in the keratinized gingiva. lnternal bevel incisionsend on the facial surface of the underlying alveolar boneand are designed to thin the buccal lingual dimensionsof the flap margin. lnternaΙ bevel incisions that end atthe aΙveolar crest are used \η/hen fuΙl gingival retentionis required.
SulcuΙar Incision. The initial incision is a scallopedincision that is made into, and follows, the gingivalsulcus (Figure 7).
Marginal lncision. Τhe initial incision is a sοallopedincision at the gingival margin (Figure 7).
Submarginal lncision. Τhe initial incision is madeapical to the gingival margin but sufficientΙy corona| tothe mucogingival junction to preserve gingiva on thefΙap (Figure 7).
FΙGURΕ 7. A line drawing showing three possible orientations of initialinternal bevel incisions. sulcular inοisions (A) and marginaΙ inci-sions (B) are used when the zone of keratinized gingiva is narrowand preservation of gingiva is criticaι. submarginal incisions (c) areused when the zone of keratinized gingiva is wide and where the flapmust be thinned internally.
FIGURE 8. A clinical photograph showing a partial thickness lateralpedicΙe flap placed over the mesial buccal root ot a maxillary firstmolar. τhe releasing incision was made over interproximal bone topreserve enough papillary tissue on the flap for suturing and tominimize surgical trauma to the thin bone over the root prominenceof the second premolar.
b4

Access to roots, marginal alveolar bone, and bonydefects can be adequately achieved in most instancesυsing envelope flaps (ie, flaps produced by horizontal
sulcular, marginal, or submarginal incisions). ln somecases where acοess is difficult to achieve or where the
risk for undue surgical trauma is high, flaps may be"relaxed" using vertical and/or cutback ("hockey-stick")
releasing incisions. Vertical incisions are made parallel
with the long axis of the teeth in the area^ They must beplaced at line angles of teeth to minimize postsurgical
marginal deformities and through the muοogingival junc-
tion to permit adequate flap "relaxation". The cardinalprinciple in planning vertical or cutback releasing inci-
sions' is that the blood supply to the flap margin ispreserved. To do so, the flap should be at least as wide at
its base as it is coronally (see Figure 8).
Crestat anticipation incisions are variants of the submar-ginal incision and are indicated in areas where the
mucogingival junction is absent and the flap cannot be
repositioned. The best example of this scenario is wherepalatal flaps are used for access in osseous surgery.These inclsions require abundant keratinized gingiva bepresent, they are peι'formed to "antiοipate" the position of
ihe future gingival margin in relation to the future crest of
the alveolar bone when apical positioning of the flap is
not possible (Figure 9).
achieved mainly by gains in clinical attachment mediatedby repair.
1. Replaced Flap (RF). The RF is a full-thickness, full
gingival retention mucoperiosteal flap. lt is a "work-horse"of periodontal surgery as it can be employed in one ormore of the following periodontal applications:
. Access to roots and bony defects in regenerativesurgery procedures
. Αccess to roots in open flap debridement proce-dures
. Aοοess in diagnostic exploratory procedures
. Access for treatment of periodontal emergencies
RFs are full gingival retention procedures. The initial inci-sions are always sulcular in origin and include as muchinterdental tissue as possible (Figure 10).
FIGURE 9. A clinical photograph shosring a crestal anticipation incision_ -on tne palate. The giigii/al tissue ioronal ιo the incision will be
δ.or.i fo, ucc."s ib b,-one and roots. crestal anticipation incisionsa.J ,seα to "anticipate" the apical Position ot the flap margin at theaiveoiir οrest wneλ the tιap iiself cannot be aρically positioned'
VVhat Is Meant by Positioned andRepositioned FIaPs?
Periodontal flaps may be categorized acοording to
whether they will, at the conclusion of the procedure, be
either repositioned back to their presurgical location orpositioned to a nevv, alternative location'
Repositioned ftaps are "open and close" procedures\Λ/here the coronal fΙap margins, keratinized gingiva, and
the mucogingival junction are returned to the same rela-
tive position on the teeth and bone that they occupiedbefore flap elevation. Repositioned flaps, as a category'include replaced flaps, modified Widman flaps' and exοi-
sional new attachment procedures. They all heal byrepair (ie, by a long junctional epithelium and conneοtivetissue adhesion or attachment) and are consideredpocket reduction procedures. The pocket reduction is
FlGURE 1o. A line drawing showing the initial sulcular incisioΠs.(dottedlines) for a replaced fιap. Diagonal incision lines that extend acrossthe iilerproxi'mal spacd from the distal lingual ιine an9les to mesialfacial lin; angles iicrease the chances of primary wound cιosure'
The flaps are raised by blunt dissection from the under-lying alveolar bone. Conceptually, RF reflection does not
extend apical to the mucogingival iunction, and the RFοannot be positioned apically, coronally, or laterally. RFsare "replaced" back to their presurgical location and are
sutured to achieve primary wound closure interdentally.Repositioning of the RF minimizes postsurgical reces-sion. RFs are the flap of choice in aesthetically sensitiveregions of the dentition. RFs are indicated for the treat-ment of suprabony pockets or where periodontal repair ispossible. They are also indicated for aοcess to intraos-seous defects for periodontal regeneration. ln reality,
many RFs are etevated apical to the mucogingival .iunc-tion to achieve required access (see previous Figure 4).
Modified Widman Flap (MWF). The MWF is a modifica-tion of the replaced flap. lt is a full{hickness flap that maybe used in open flap debridement and regenerative perio-
dontal procedures. Unlike the RF, the M\,VF is not a full
gingival retention procedure. Submarginal, scalloped,
2.
65

Ξ
SURGICAL TREATMENT: PRINCIPLES
internal bevel horizontal incisions are used to produceprominent interdental extensions of tissue that ensureprimary flap closure (Figure 11). The MWF is indicatedwhen access to roots and intraosseous defects fordebridement is needed. Because of its greater opportu-nities for primary closure that ensures graft retention, theMWF is also indicated in regenerative procedures.
FIGURE 11. A line drawing showing the initial submarginal incisions(dotted lines) for a modified νvidman flap. τhe incisions increase thelength of the interproximal tissue extensions. Diagonal incisions(Figure 10) may also be used in the modified \rvidman flap design.
Positioned fΙaps are flap procedures where the coronalmargins of the flap are advanced apically, coronally, orlaterally to a ne\Λ/ loοation relative to the site they occu-pied before the procedure. The category includes apicaιlypositioned flaps, coronaΙly positioned flaps, and laterallypositioned flaps. Like repositioned flaps, most positionedflaps heal by repair (ie, a new attachment οonsisting of along junctional epithelium and connective tissue adhesionor attachment).
Apically Positioned Flap (APF). The ΑPF is a full-thick-ness, mucoperiosteaι flap. Like the RF, the APF is a"work-horse" of periodontal surgery. lt is most commonlyused in conjunction with osseous surgery, and it has fewother applications (Figure 12).
Coronally Positioned Flap (CPF). The CPF is a full-thickness mucoperiosteal flap that has almost exclusivelybeen used to restore gingival height and the zone ofattaοhed gingival over isolated areas of gingival reces-sion. Since it is peformed to correct defects in themorphology or position of the dental gingival junction, it isclassified as a mucogingival surgical procedure. Briefly,the surgical principles and wound healing for the CPF aresimilar to those of the APF. Sulοular initial incisions andvertical releasing incisions through the mucogingivaljunction are used to mobilize the flap. CPFs are elevatedfrom bone by blunt dissection and then positionedcoronally to the cementoenamel junction of the affectedtooth. Wound stability at closure, wound contractionduring healing, and local anatomic features will determinethe final amount of root οoverage achieved. ln instanceswhere there is an inadequate band of gingiva in the tissueto be coronally placed, a CPF may be performed in 2stages. ln the first stage, a free autogenous soft tissuegraft is placed to augment the gingiva. Three to sixmonths later, the second stage CPF is pedormed tocoronally position the nevι/ly augmented gingiva.
Laterally Positioned Flap (LPF). The LPF, also knownas Ιhe pedicle flap, is a positioned flap that is performedto correct defects in the morphology, position, or amountof attached gingiva. Positioned and repositioned flapsare, in reality, pediοle flaps. They are all physicallyattached at their apical base by a pediοle of liningmucosa and an intact blood supply (Figure 13).
1.
2.
3.
FIGURE 13. A clinicat photograph showing a partial thickness pedicleflap. τwo parallel reιeasing incisions have been made. The base ofthe pedicle is as wide as flap margin.
ΑBF|GUHES '12Α and B. A. Line drawing showing a marginal internal bevel
incision (dotted line) to the alveolar crest. B. τhe apical position ofgingival margin to the crest of the bone after osteoplasty (dotted line).
What Are the Anatomic LandmarkConsiderations of the Maxilla and MandibleBefore Periodontal Surgery? How Do TheseLandmarks Limit the Use of Relaxinglncisions or Flap Position?
The surgiοal anatomic landmarks of concern in periodon-ta| Surgery may be grouped into four οategories.

CHAPτER 7
They involve:
. Osseous morphology
. Musculotendinous anatomy
ο Vascular anatomy
. Redundant innervation
The osseous landmarks of surgical importance in themaxilla are the maxilΙary sinuses, the maΙar processes ofthe maxillary bone, the pterygoid hamulus, and palataltori (Figure 14).
FIGURE 14. A dried human specimen showing the palatal osseouslandmarks of impοrtance in periodontal surgery. τhey are the ptery-goid hamulus, the palata| torus exostoses, and the greater paΙatineforamen.
The osseous landmarks in the mandible of surgicalimportance are mental and lingual foramina, the mylo-hyoid and the external oblique ridges, the genial tuber-cles, and lingual mandibular tori. The lingual undercut inthe mandibular molar area dictates careful full-thicknessflap reflection to avoid penetration into the sublingualspace and possible injury to the lingual nerve and artery(Figure 15 and Figure 16).
FlGURΕ 15. A dried human specimen showing the mylohyoid ridge and alingual mandibular undercut. τhe linqua| nerve runs close to themylοhyoid ridge and is at risk durinσsurgery distal to mandibularsecond and third molars,
Αlmost a|Ι osseous landmarks have a limiting effect onthe degree of flap reflection, flap positioning, and the useof relaxing incisions. Τhey indireοtly affect the amount ofsurgica| aοcess to teeth and bony defeοts.
FlGURE 16. A dried human specimθn showing the myΙohyoid ridge andlingual mandibular undercut. lt also shows the attachment of thebuccinator muscle.
The musculotendinous landmarks are the attachment ofthe mentalis muscle in the mandible, and the tendon ofthe tensor veli palatini (TVP) muscle in the hamular notchand the attachment of the bucοinator muscle (Figure 17).Surgery in the maxillary tuberosity and the hamular notοhalso increases opportunities of accidental penetration ofthe pterygomandibular space with possible injury to thesuperior constrictor muscle and the medial or lateral pter-ygoid muscles.
The vascular landmarks are the greater palatine arteryand the pterygoid plexus in the maxilΙa and the linguaΙartery and mental artery in the mandible. They are insuch proximity to the marginal periodontium to precludethe pΙacement of relaxing incisions in palatal and mandib-ular flaps. lf absolutely required for access, vertical inci-sions within the gingiva only could satisfy that needwithout risk of vascular injury. Τhe Ιocation of the mentaΙartery rules against verticaΙ and cutbaοk incisions andlateral positioned full or partial thickness flaps in themandibular premolar region (Figure 17). The venouspterygoid plexus in the pterygomandibular space isalways at risk io injury during loοaΙ anesthesia injeοtionsof the posterior superior alveolar nerve.
τ.:, Ξ
',::.1
-:l
::
s*#ffi
FIGURΕ 17. A companion view ot the specimen in Figure 18 showing theattachment of the buccinator buccal to mandibular molars. lt alsoshows the mental ,oramen located between the apices of the premo-lars-

SURGICAL TREATMENT: PRINCIPLES
The innervation landmarks are the lingual nerve, the longbuccal nerve, the inferior aιveolar nerve, and the mentalnerve in the mandible and the nasopalatine nerve and thegreater palatine nerve in the maxilla. Vertical and relaxingincisions in the palate or in mandibular posterior facialflaps increase the opportunity for regional transient orpermanent paraesthesia.
How Are Periodontal Surgery WoundsClosed? What ls the Role of Suturing? WhatSuture Materials Are Best Suited for theClosure Periodontal Wounds?
All periodontal wounds, except for the gingivectomy,require a method of closure that will maintain the reposi-tioning or positioning of flaps during the early phases ofwound healing. Sutures are used to maintain woundclosure and flap position. Other methods of closureinclude tissue tacks and the adhesive, cyanoacrylate.Conceptually, tissue tacks offer an attractive alternativeto sutures, but they have not gained acceptance becauseof the trauma they produce at flap margins and to bone.
Cyanoacrylates have potent hemostatic capabilities, andthey are effective in maintaining postoperative tissueposition. On the downside, they are technique sensitive.They flow easily over tissue before they "set" and aredifficult to contain at νvound edges. Cyanoacrylates havebeen known to 'TloW" between flap margins and bone,which will only abrogate surgical outcomes. lf used care-lessly in the oropharynx, cyanoacrylates could presentrisks to the patient's airway.
Suture materials used in periodontal surgery are eitherresorbable or nonresorbable. They may also be made ofbraided naturaι fibers or nonbraided monofilamentsynthetic fibers. Braided natural fiber sutures (ie, silk andcotton), tend to absorb wiοk and retain bacteria in thewound. Suture tracts through tissue νvilΙ develop clinicalsigns of inflammation within 3-7 days, which necessitatestheir removal at the end of the first postoperative νveek.
Monofilament synthetic fiber sutures will not absorb oralbacteria and may be kept in the wound site for longerperiods of time. They are generally more expensive thannatural fiber sutures.
The choice of suture material should depend primarilyupon the type of surgery being performed and the require-ments for the maintenance of extended wound closureand, secondarily, upon office economics. The cost of thesuture material should not enter into the decision-makingprocess. For example, one absolute prerequisite forregenerative periodontal surgery using guided tissuebarrier membranes is that the wound edges maintainprimary edgeto-edge approximation during the initialweeks of healing. To achieve the objective of optimalwound closure and, at the same time, minimize thebacterial contamination of the wound, more expensivemonofilament nonresorbable sutures are clearly prefer-able over braided sutures.
Sutures should be placed in enough tissue (ie, the baseof interdental papillae) to assure their retention for aslong as intended, and tied with a surgeon's knot. Theyalso should be tied tightly enough to maintain tissue posi-
tion, but, at the same time, not so tightly that they tear/cutthrough the tissue they are intended to stabilize. Suturesthat "pull-out" or untie during healing are of no value tothe surgery. Ties should be planned so that knots will beaccessible for suture removal. Suture removal should notbe a surgical experience for the patient.
What Are the PrincipIes of Periodontal νιroundClosure and Suturing? \Mhat Are lnterrupted,Figure 8, Sling, and Vertical MattressSutures?
AtΙer wound closure and suturing, the surgeon mustmake certain that:
. The wound is clean and the oral cavity has beenirrigated free of debris
. Gentle positive pressure was maintained over thewound for 3-5 minutes immediately after closure tocontrol hemostasis
ο A thin fibrin clot has formed betνveen the flap and theunderlying periosteum or bone
. Wound margins are held in their intended position bysutures and the fibrin clot
o The wound has been covered with a periodontaldressing, if required
o The patient has been given written and verbal instruc-tions for postoperative wound care
ο The patient has been given prescriptions for pain andinfection control
ο The patient has been given an appointment to returnfor postoperative care in 6-8 days
The interrupted circumferential, the figure 8, the sling,and the vertiοal mattress sutures are the most popularsuturing techniques in periodontics. Continuous slingsutures, horizontal mattress sutures, and purse-stringsutures are more difficult to perform and time consuming.As far as surgical outcomes are conοerned, there may belittle advantage to using complex suturing methods in
most periodontal surgical cases.
The interrupted circumferential suture is the "universal"suture in periodontal surgery. While they may be usedin almost all periodontal surgeries, they are most appro-priate for closure of facial and lingual replaced flaps andmodified Widman flaps.
lnterrupted sutures provide the best opportunities forconneοtive tissue contact betM/een f|aps interproximally,and, because of this, they are also preferable to figure 8sutures when closing flaps in edentulous areas (ie, adistal wedge) (Figures 184, B, and C).
The figure I suture is so called because it looks like an"8" lying on its side. lt is used most often to close facialand lingual apically positioned flaps. When tied, the figureI suture aides in the adaptation of the tips of interdentalpapillae to underlying recontoured alveolar bone (Figure18).
68

CHAPτER 7
/s
/,FIGURES 184, B, and C. A, lnterrupted circumferential suture. B. Figure 8
suture. C. Vertical mattress suture. lt is used when it is important toexclude suture material from regenerative periodontal surgery sites.νιrhen tied, lhis suture aids in the adaptation of interdental papilla tothe underlying alveolar bone.
A verticaΙ mattress Suture may be used when it is impor-tant to exclude braided natural suture material fromregenerative periodontal surgery sites. The suture mate-rial is threaded through and over the sudace of each ofthe interdental flap papillae (Figure 18). The interpapillaryvariation of the vertical mattress suture excludes allsuture material from a regenerative site. The mattresssuture is more technique sensitive than the interruptedsuture, and any perforation of the flap will negate itspurpose (Figure 18).
The sling suture is used primarily to suspend/position asingle facial interdental papilla. lt is usually employed incases where a corresponding Ιingual flap may not havebeen raised (ie, a laterally or a coronally positioned flap).The support for the sling suture is derived from either thelingual of the tooth involved or from an ad.iacent tooth.
What ls the Purpose of a PeriodontalDressing? Can Periodontal Surgery BeSuccessful Without Postsurgical PeriodontalDressings?
Periodontal dressings were born out of necessity duringthe era of reseοtive periodontal Surgery when the gingi-vectomy and osseous denudation procedures werepopular. These procedures produced "stormy" postopera-tlve healing. Severe inflammation and pain, hard and softtissue necrosis, and bone resorption were οommon' Theperiod of discomfort was determined by the length of timeneeded for inflammatory ceΙls to remove neοrotic tissue.ln some cases where bone exposure was excessive, thisprocess took 2-3 weeks to complete. To reduce patientcomplainis of postoperative pain, periodontal dressings
of the time were specially formulated to overcome them.Some contained sedative agents. The most popular, andmost effective, of these agents ννas eugenol. Eugenol\Λ/as later found to cause its own tissue injury andnecrosis. Commercially available periodontal dressingscurrently do not contain eugenol.
Today, there are probably two accepted purposes in peri-odontal surgery. They:
. Serve as a barrier to protect the periodontal woundfrom accidental injury during the critical days ofhealing (Figure 19).
. Provide the patient \,vith some degree of comfortduring the acute infΙammation phase of healing andwhile epithelialization of the wound takes place(Figure 20).
F|GURΕ'19. Α clinical photograph of an apically positioned flap posi-tioned at crest with a continuous sling suture. A delicate fibrin clotmediates the initiaι union between the flap and underlying tissuesand tooth structure. A periodontaι dressing was placed to protectthe wound from accidental iniury during the first postoperativeweek.
FlGURE 20. A clinical photograph of a gingivectomy Wound. τhe exposedconnective tissue will be a source of patient discomfort until epithe-lial closure is complete. Periodontal dressings were placed tocontrol patient discomfort during the first and second postoperativeweeks.
Periodontal dressing should not be used to οontrolbleeding. Hemostasis should be achieved before adressing is placed.
%\oΛD'U+
/ o'η
/$CC
t'

SURGICAL TREATMENT: PRINCIPLES
Periodontal dressings have no \η/ell-defined effect on theproοesses of \Λiound heaΙing or on SUrgical outcomes (ie,gains of periodontal attachment or reduction in probingdepths).
How Do Periodontal Wounds Heal? How ArePeriodontal Wounds Classified?The heaΙing of periodontal wounds involves the Sameprocesses that ocοur in all wounds. Epithelium, ordinaryοonnective tissue, cementum and bone, heal according totheir own tissue specific biologic "rules", which have foun-dation in tissue embryogenesis. ln the case of woundhealing, surgical injury creates the environment and stim-ulus for cellular differentiation.
Periodontal wounds are classified according to the envi-ronment for epithelial closure of the wound.
ο Primary νVound healing occurs when mucosal \Ι/oundmargins are edge to edge and the epithelium hasonΙy a short distanοe to migrate to another \Λ/oundmargin of tooth surface before the \η/ound is sealed.Primary wound closure occurs folΙowing the closureof distal wedges and some endodontic access flaps(Figure 21).
FlGUFlΕ 21. A clinical photograph showing primary closure of an endo-dοntic access procedure' τhe wound edge of the flap has beensutured to approximate the wound edge on the attached gingiva.
FΙGURE 22. A clinical photograph showing primary c|osure of a replacedflap covering a periodontal regenerative procedure. τhe tlap marginscontact tooth structure and the tips ot the facial and lingual inter-dental papilιae contact each other interproximally.
FIGURΕ 23. A clinical photograph showing a gingivectomy that will healby secondary wound healing. Epithelial cells must migrate acrossthe exposed connective tissue until they contact the tooth or othermigrating epithelial cells.
. Secondary wound healing occurs \η/hen epithelialcells must migrate several millimeters to close thewound. The gingivectomy is an example of a woundthat heals by secondary \Λ/ound healing (Figures 22and 23).
FIGUΗE 24. A clinical photograph showing tertiary wound healing of anapically positioned flap procedure at the week one postoperativevisil. τhe patient experienced considerable postoperative pain, andnοrmal epithelial migration will be delayed until it is removed byresorption and sequestration,
FIGURE 25. A clinical photograph of the removed bony sequestrum fourweeks after surgery.

cHAPτER 7
o τertiary \Λ,ound healing occurs \ivhen there iS anobstacle to epitheIial migration. Τypically, thisobstacle is necrotic tissue created during the surgery.Epithelial migration and wound closure will bedelayed until the obstacle has been removed(Figures 24 and 25).
What ls the Sequence of Events inPeriodontal Wound Healing? How May ThisSequence Be Interrupted?
Following surgical injury:
. Epithelium. The epithelium is the first tissue torespond to injury. Epithelial cells begin to proliferateat νvound margins at 1-2 days. other epithelial cellsdedifferentiate and migrate onto and across exοori-ated connective tissue until they either contact eachother or they make contact with a tooth. The migra-tion takes place at a rate of 0.5 mm per day. The areato be covered determines duration of migration. Forinstance, it may take 10-14 days to cover a gingivec-tomy wound while a replaced flap may be sealed tothe tooth in 2-4 days. Once the monolayer is formed,proliferation and differentiation of progeny cells intomature epitheΙial cells predominates. ln most perio-dontal wounds, epithelialization and the formation ofa junctional epithelium are complete by the end of thesecond week of healing.
ο Gonnective tissue. ln the repair of ordinary gingivalconnective tissue, fibroblasts begin to proliferate afterday 2 with evidence of collagen synthesis in thewound by day 4. The duration of these activities isdetermined by the amount of tissue that needs to berestored. ln the most uncomplicated periodontalsurgery, restoration of gingival connective tissue wiΙl
be complete in 4-6 weeks.
. Alveolar bone. Τhe healing of alveolar bone ispreceded by a period of reactive bone resorption.Osteoclasts appear in the wound at about day 4 anddisplay peak osteoclastic activity at day 10. Τhe dura-tion and severity of the osteitis depends upon thedegree of injury and necrosis of bone. Osteoblastsbegin to appear and proliferate in the wound duringthe second week, and they display peak osteoblasticactivity by the end of the third week. Deposition ofbone continues into the second month. Bone remod-eling and maturation is a feature of the third postoper-ative month.
. Cementum. Repair of cementum is the "turtle" ofperiodontal wound healing. Not only isοementogenesis delayed in onset; it is also slow toexert its effect on the overall outcome of periodontalhealing. Proliferating cementoblasts appear adjacentto root surfaces at the end of month one and proceed\Λ,ith cementogenesis during the months two andthree. These events are critical to the formation of ane!η, attachment apparatus and some forms of newattaοhment. lt is for this reason that manipuΙation ofthe newly healed dentogingival junction should bedelayed at least until the end of the third postopera-tive month.
ln overview, periodontal wound healing is dominated bynecrosis, inflammation, and resorption in the first week,proliferation, differentiation, and production in the secondthrough the sixth week, with maturation and remodelingfrom the seventh week through the end of the thirdmonth. Figure 26 details the chronology of events in peri-odontal wound healing.
Week One Week Two Week Three Week Four
TΑBLE 1. Sμopsis of Bioξical Eγents in the Heιling of Periodontg! Surgicεl Wounds
Εpithelium
Yasculature
Connectivetissue
Bone
Cementum
Migration ( l)--{overage (7}-Maturation (14)*Ρrοliferation (2p
Junctiοnal epithelium (l4)Angioblasts (2p
Endothelial budding (7)-Yascularity (14)Fibroblasts (2 21)
Fibrogenesis (5
Resoφtion(4#l0)tDeposition (10 / /--------19O)lCementoblasts (12 / /-----<9O)
( ) Postoperative day* Delayed in the healing of free gingival grafts.t Delayed in cases where osseous surgery v,as performed.f Ηealing of the dentogingival junction complete.
The scenario depicted is that οfa hypothetical consιruct based upon scientific data as repοrted in the liιerature. Restorativeprocedures should not be performed until after the third postoperative month.
FlGURE 26. A table showin9 the chronology of epitheιiaι, ordinary connective tissue, bone and cementum wound healing events in periodontal surgery.(Αdapted from Hawley ο and Serio F, "Periodontal ννound heaiing," clark'S cιinical Dentlsιry, Philadelphia, PΑ: JB Lippinοott οo, '1989, 1:'17.)
71
-

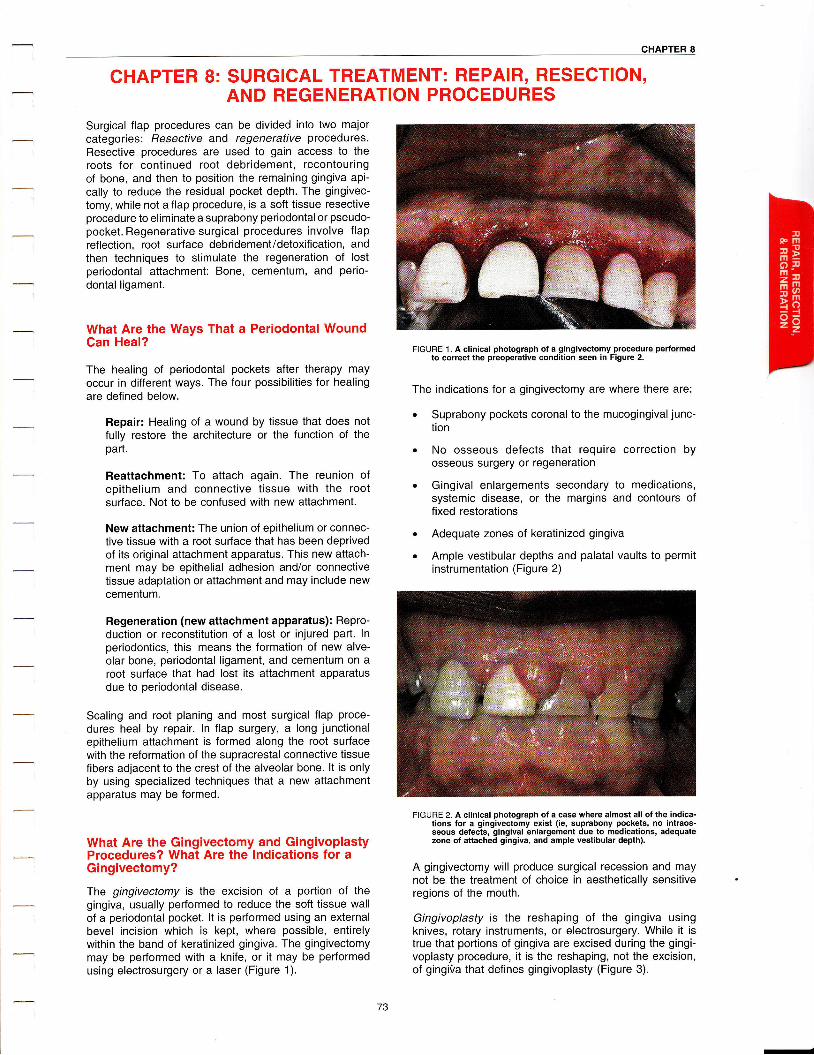
cHAPτER 8
CHAPTER 8: SURGICAL τREATMENT: REPAIR' RESΕcTloN,AND REGENERATION PROCEDURES
Surgical flap proοedures can be divided into two majorcategories: Resectiνe and regeneraflve procedures.Resective procedures are used to gain access to theroots for οontinued root debridement, recontouringof bone, and then to position the remaining gingiva api-οally to reduce the residual pocket depth. Τhe gingivec-tomy, while not a flap procedure, is a soft tissue resectiveprocedure to eliminate a suprabony periodontal or pseudo-pocket. Regenerative surgicaΙ procedures involve flapreflection, root surface debridement/detoxification, andthen techniques to stimulate the regeneration of lostperiodontal attachment: Bone, cementum, and perio-dontal ligament.
What Are the Ways That a Periodontal WoundCan Heal?
The healing of periodontal pockets after therapy mayoοcur in different ways. The four possibiΙities for healingare defined below.
Repair: Healing of a wound by tissue that does notfully restore the architecture or the function of thepart.
Reattachment: To attach again. The reunion ofepithelium and connective tissue \lνith the rootsurface. Not to be confused with new attachment.
Neι,v attachment: The union of epithelium or connec-tive tissue with a root surface that has been deprivedof its original attachment apparatus. This new attach-ment may be epithelial adhesion and/or connectivetissue adaptation or attachment and may inοlude newcementum.
Regeneration (new attachment apparatus): Repro-duοtion or reconstitution of a lost or injured part. lnperiodontiοs, this means the formation of new aΙve-olar bone, periodontal ligament, and cementum on aroot surface that had lost its attachment apparatusdue to periodontal disease.
Scaling and root planing and most surgical flap proce-dures heal by repair. ln flap surgery, a long junctionalepithelium attachment is formed along the root surfacewith the reformation of the supracrestal conneοtive tissuefibers adjacent to the crest of the alveolar bone. lt is onlyby using specialized techniques that a new attaοhmentapparatus may be formed.
What Are the Gingivectomy and GingivoplastyProcedures? What Are the lndications for aGingivectomy?
The gingivectomy is the excision of a portion of thegingiva, usually performed to reduce the soft tissue waΙl
of a periodontal pocket. lt is performed using an externalbevel incision which is kept, where possible, entirelywithin the band of keratinized gingiva. The gingivectomymay be performed with a knife, or it may be performedusing electrosurgery or a laser (Figure 1).
FIGURE 1. A clinical photograph of a gingivectomy procedure performedto correct the preoperative condition seen in Figure 2.
The indications for a gingivectomy are where there are:
. Suprabony pockets coronal to the mucogingival junc-tion
. No osseous defects that require correction byosseous surgery or regeneration
. Gingival enlargements secondary to medications,systemic disease, or the margins and contours offixed restorations
. Αdequate zones of keratinized gingiva
. AmpΙe vestibuΙar depths and palatal vaults to permitinstrumentation (Figure 2)
FlGURE 2. A clinical ρhotograph of a case where almost all of the indica-tions for a gingivectomy exist (ie, suprabony pockets, no intraos-seous defects, gingivaι enlargement due to medications, adequatezone of attached gingiva, and ample vestibular depth).
A gingivectomy will produce surgical recession and maynot be the treatment of choice in aesthetically sensitiveregions of the mouth.
Gingivoplasty is the reshaping of the gingiva usingknives, rotary instruments, or electrosurgery. While it istrue that portions of gingiva are excised during the gingi-voplasty procedure, it is the reshaping, not the excision,of gingiVa that defines gingivoplasty (Figure 3).
-

SURG|CAL TREATMENT: RESECΤ|VE AND REGEΝERAT|VE PROCEDURES
F|GURΕ 3. A clinical photograph of the case in Figure 1 after the gingivec-tomy was embellished by shaving the wound margins with knivesand creating interdental grooves using rotary instruments. Gingivalbulk has been reduced, and the aesthetics of the case have beenimproved.
The gingivectomy and the gingivoplasty should not beperformed in the presence of inadequate inflammatorydisease control.
After satisfying its indications and contraindications, thegingivectomy is classically performed by:
ο Producing bleeding points on the surface of thegingiva corresponding to the pocket depth
o Making a 45' angle externaι bevel incision usingsharp Kirkland or Goldman-Fox gingivectomy knives(Figure 4)
. Beginning the incision on the gingival surface slightlyapical to the bleeding points and ending the initialincision at the point of gingival attachment to thetooth
. Using narrow Orban interproximal knives to extendthe initial incision interproximally and to meet anyopposing initial incision
. Removing the excised collar of gingival tissue n fofo
FIGURE 4. A clinical photograph of an initial gingivectomy incision. lt ismade using a Kirkland knife held at a 45" angle with the tooth begin-ning iust apical to the clinical attachment level and ending at theattachment level.
Gingivoplasty instruments include coarse rotary diamondstones, soft tissue nippers, or gingivectomy knives tosmooth, groove, and contour the wound edges (Figure 5).The procedure is completed using curettes to scale, rootplane, and remove residual tissue tags.
FIGURE 5. A clinical photograph ot a completed gingivectomy showingthe blended Wound margins and vΘrtical interdental grooves madeby gingivoplasty.
Τhe healing of a gingivectomy/gingivoplasty takes placeby secondary wound healing. Beοause of the large areaexposed connective tissue and the fixed rate of epithelialcell migration, re-epithelialization and the formation of anew junctional epithelium may take up to 2 \Λ/eeks tocomplete. Αnother 2-4 weeks may be necessary to re-establish the marginal gingiva and gingival sulcus.
What ls Electrosurgery? Is Electrosurgery aReasonable Alternative to Knives inGingivectomy/Gingivoplasty Procedures?
Εlectrosurgery is the "division of tissues by highfrequency electrical current applied locally with a metalinstrument or needle." ln the process, electrosurgery cutsand cauterizes. Cutting energy in the form of heat isproduced at the needle tip. The amount of injuryproduοed by the heat depends upon:
. How long the electrode maintains static contact vι/ith
tissue
. Ηow current is being applied
. The type of electrode being used
ο The impedance of the tissue
lmpedance is the measure of tissue resistance to thespread of cutting energy. lt is very low in inflamed gingivaltissue, which makes electrosurgery well suited for gingi-vectomy/gingivoplasty procedures. lf the electrode is keptproperly tuned and kept in οonstant motion to limit thelateral spread of heat, soft tissue healing does not appearto be adversely affected by electrosurgery.
lmpedanοe is very high in mineralized tissues, and elec_trosurgery should not be used \Λ/here the needle \,νill
contact bone ortooth structure (ie, periodontal flap proce-dures). Any electrode contact with mineralized tissueswill produce bony necrosis, inflammation, and resorption.Cementum may also be damaged to the extent that it willbe unable to maintain existing gingival attachment.
Hemostasis is usually better with eΙectrosurgery than withsurgery with a blade. Soft tissue reshaping in gingivec-
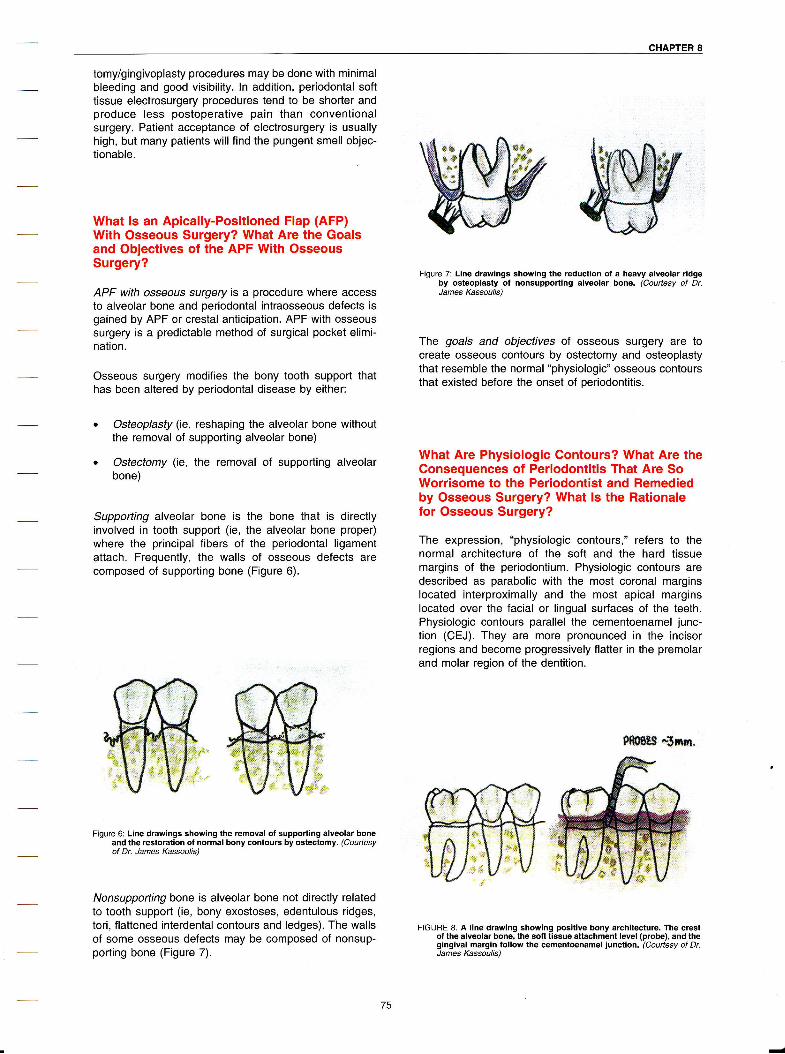
CHAPτER 8
tomy/gingivoplasty procedures may be done with minimalbleeding and good visibility. ln addition, periodontal softtissue electrosurgery procedures tend to be shorter andproduce less postoperative pain than conventionalsurgery. Patient acceptance of electrosurgery is usuallyhigh, but many patients will find the pungent smell objec-tionable.
VVhat Is an Apically-Positioned Flap (AFP)With Osseous Surgery? What Are the Goalsand Obiectives of the APF With OsseousSurgery?
APF with oSSeouS Surgery is a procedure where acοessto alveolar bone and periodontal intraosseous defects isgained by APF or crestal anticipation. APF with osseoussurgery is a predictable method of surgical pocket elimi-nation.
osseous surgery modifies the bony tooth SuppoΙ1 thathas been aΙtered by periodontal disease by either:
ο osteoplasfy (ie, reshaping the alveolar bone withoutthe removal of supporting alveolar bone)
o Ostectomy (ie, the removal of supporting alveolarbone)
Supporting alveolar bone is the bone that is directlyinvolved in tooth support (ie, the alveolar bone proper)νvhere the principal fibers of the periodontal ligamentattaοh. Frequently, the walls of osseous defects arecomposed of supporting bone (Figure 6).
Figure 6: Line drawings showing the removal of supporting alveolar boneand the restoration of normal bony contours by ostectomy. (Couftesyof Dr. James Κassouιis)
Nonsupporting bone is alveolar bone not directιy relatedto tooth support (ie, bony exostoses, edentulous ridges,tori, flattened interdental contours and ledges). The wallsof some osseous defects may be composed of nonsup-porting bone (Figure 7).
Figure 7: Line drawings showing the reduction of a heavy alveolar ridgeby osteoplasty of nonsupporting alveolar bone. (Courtesy of Dr.James Kassoulis)
Ιhe goaΙs and objectives of osseous Surgery are tocreate osseous contours by ostectomy and osteoplastythat resemble the normal "physiologic" osseous contoursthat existed before the onset of periodontitis.
What Are Physiologic Contours? What Are theConsequences of Periodontitis τhat Are SoWorrisome to the Periodontist and Remediedby Osseous Surgery? What ls the Rationalefor Osseous Surgery?
The expression, "physiologic contours," refers to thenormal architecture of the soft and the hard tissuemargins of the periodontium. Physiologic contours aredescribed as parabolic with the most coronal marginslocated interproximally and the most apical marginslocated over the facial or lingual surfaces of the teeth.Physiologic contours parallel the cementoenamel .junc-tion (CEJ). They are more pronounοed in the incisorregions and become progressively flatter in the premolarand molar region of the dentition.
Fffit* €x*l.
FlGURΕ 8. A line drawing showing positive bony architecture. The crestof the alveola. bone, the soft tissue atιachment level (probe), and thegingival margin follow the cementoenamel iυnclion. (cour1esy of Dr.James KassouιiS)
75

sURGlcAL TREATMENT: REsEcTlvE AΝD REGEΝERAτlvE PRocEDURΕS
Positive bony architecture is the term used todescribe the normal "physiologic" relationship of inter-dental and radiοular bone heights. lt is positive bonyarchitecture that the normal bioΙogic width (sulcus,junctional epithelium, and connective tissue attach-ment) and the gingival margin tend to follow in health(Figure 8).
Νegative bony architecture is the term used todesοribe any abnormal, nonphysiologic relationshipof interdental and radicular bone heights. Periodon-titis destroys periodontal attachment and the normalparallelism bet\r/een the crest of bone and the CEJ isΙost. The bony margins and gingival attachmentlevels become irreguΙar and inconsistent \r/here intra-osseous defects are formed. Not all intraosseousdefects should be treated by osseous surgery.
β*θB€$ *ι,ι*.
FΙGURΕ 9. A line drawing showing negative bony architeclure. τhe contours ofthe aiveolar bone and attachment level (probe) do not follow the cemento-enamel iunction. (Courtesy of Dr. James Kassoulis)
. The normal "physiologic" gingival morphology tendsto retain its parabolic gingival margin contours whilebony morphology is changed by periodontitis. Thebulk of gingival tissue is inοapable of adapting to thesharp, inconsistent bony margins of negative archi-tecture (Figure 9).
The degree of discrepancy between ihe persistent posi-tive contours of the gingival margin and the emergingnegative bony contours is measured cliniοally as progres-sively increasing probing depths (Figures 10 and 11).
F|GURE 10. A cΙinical photograph of a periodontitis case before perio-dontal surgery. The gingival margin contours do not reflect the 5-7mm probing depths and negalive bony arοhitecture that exist inter-proximally.
F|GURΕ 11. A cΙinical photograph of the case shown in Figure'10following retlection of a full-thickness apically positioned flap anddebridement of osseous defects. τhe generalized pattern of hori-zontal bone loss and negative bony archilecture was obscured bythe positive contours ot the gingival margin.
The worrisome consequences of periodontitis are thedeepening probing depths that:
. Produce an ecosystem that is conducive to the emer-gence and gro\Λith of periodontaΙ pathogens
. Αre difficult to efficiently and effeοtively clean, scaleand root plane, and maintain nonsurgically
. Αre associated with the persistence and/or re-emer-gence of periodontal pathogens after nonsurgiοal andsurgical debridement, and, as a consequence....
ο Αre associated wiih progressive periodontitis
The rationaΙe for osseous Surgery is based upon thefollowing tenets:
. Deep periodontal pockets are inconsistent with perio-dontal health
ο The basis for the increased ρocket depths is theprogressively increasing discrepancy between theposition of the gingival margin and the leveΙ of perio-dontal attachment (see previous Figures 10 and 11).
ο lf ihe underlying negative bony architeοture is elimi-nated and the positive bony arοhitecture is restored(Figure 12)
F|GURΕ 1 2. A clinical photograph of lhe case shown in Figures 1 0 and 1 1
after positive bony architecture was restored by osseous surgery.

CHAPτER 8
. lf the gingival margins are repositioned to nev/lyreοontoured bone (Figure 'l3)
FIGURE 13. A clinical photograph of the case shown in Figures 10, 11,and 12 With the margins of the flap positioned at the aιveolar cresιusing continuous sling sutures.
. The healed dentogingival junction will closely followthe contours of the recontoured bone
. The new relationship of bone to soft tissue will bestablΘ
. Shallow pockets will ρersist
. Periodontal health will be restored and more easilymaintained
The dominating influences on postsurgical gingival formare:
ο The width of the interproximal space
. The morphology of the embrasure
ο The location of the contact poini with respeοt to thealveolar crest
ln summary, any failure to achieve its goals and objec-tives (ie, create osseous contours by ostectomy and oste-oplasty that resemble the normal "physiologic" osseouscontours) wiΙΙ result in discrepancies bet\Λ/een thegingival margin and the attaοhment leveΙ (ie, periodontalpockets and progressive disease).
How Are Periodontal Osseous DefectsClassified? Which Defects Are the Bestlndicated for APF and Osseous Surgery, andWhich Defects Are Not lndicated for APF andOsseous Surgery?
The pattern of bone loss from periodontitis may be eitherhorizontal (ie, the pattern of interproximal bone loss tendsto parallel the cementoenamel junοtions of adjacent teeth- see previous Figure 11) or vertical (ie, the pattern ofinterproximal bone loss does not parallel the cemento-enamel junction). Horizontal patterns of bone loss areusually generalized (ie, they involve multiple teeth in asegment), and verlical bone loss patterns may be foundaround isolated teeth (Figure 14).
FIGURE 14. A clinical photograph of an isolated vertical intraosseousdefecι. τhese defects frequently go unnoticed without the use ot aperiodontal probe.
Periodontal osseous defects are classified acοording tothe number of bony walls present or remaining at the timeof their surgical exposure. The location of the defect withrespect to the tooth will have a lot to do wiih the numberof waΙls. ln order for a defeοt to have a bony wall, it mustbe intraosseous (ie, partially or compΙetely within alveolarbone).
Periodontal osseous defects may be 0 wall, 1 wall, 2 wall,3 wall, 4 wall, or combination lesions. Common usagetrivial names have been used to describe some defects ineach οlass.
o 0 Wall Defeοts are alveolar dehiscences and fenes-trationstound on the facial or lingual surfaοes of teethwhere the alveolar housing is typically thin or wherethe tooih is abnormally inclined or malpositioned,They are not seen in radiographs. Fenestrations, inthe presence of marginal periodontitis, may οonveftto dehiscences (Figures 15 and 23). Osseoussurgery is not a treatment of choice for 0 wall dehis-cenοeS.
. 1 Wall Defeοts are commonly interproximal oSseoUSdefects where either only the proximal wall is present(a hemiseptum), or a facial or lingual wall is present(a ramp) (Figure l6). Shallow 1 wall defects may bemanaged suοcessfully using osseous surgery.
FIGURE 15. A dried human specimen showing dehiscences over promi-nent roots of mandibular anterior teeth. Partiaι thickness flapsshould be considered when planing surgical access to areas wheredehiscences and fenestralions may be present,
77

sURGlcAL TREAΤMENT: RΕsEcTlvE AND REGENERAτlvE PRocEDUREs
F|GURΕ 16. A dried human specimen showing a 1 wall hemiseptum defecton the mesial of a mandibular molar. τhe wall of the defect is formedby bone attached to the distal of the second premolar.
. 2 Wall Defects \Λ/here the facial and lingual walls arepresent, and bone Ιoss has occurred on the proximalsurfaces of adjacent teeth are very common (an inter-dentaΙ crateη (Figures 17 and 18). 2 wall interprox-imal defects \,vith either a facial or lingual \Λ/all and aproximaΙ walΙ are less common. Shallow 2 walldefects may be managed using osseous surgery.
FIGURE 17. A dried human specimen with shallow 2 wall interdentalcraters between maxillary molars. τypically' craters have a buccal(facial) wall and a lingual wall. Lingual walls are shown.
FIGURE 18. A dried human specimen with the same shallow interdentalcraters between maxillary molars in Figure 16. Buccal (facial) wallsare shown,
'' . ..-....Ξ,:-,|.'',.'',,, ' . ' 1 _ , :. :.;:.-,:.t... :.
F|GURΕ 1 9. A dried human specimen with a 3 wall intrabony detect on themesial ot a mandibular molar. τhe 3 walls are the buccal wall, theproximal (mesial) waΙl, and the lingual wall.
3 Wall Defects occur either interproximally or on thefacial or linguaΙ suι.faces of teeth. lnterproximaΙly, the3 wall defect has a facial, a lingual, and a proximalwall and may be caΙled an intrabony defecr. lntrabonydefects are frequently assoοiated with food impaction(Figure 19). Three waΙl defects may also be found onthe facial and lingual of teeth where there is enoughbone present to support the formation of walls, suchas the lingual or facial of mandibular posterior teethand the palatal of alΙ maxiΙlary teeth. These 3 walldefects are sometimes called wel/s. Periodontalregeneration, not osseous surgery, is the treatment ofchoice for 3 wall defects.
4 Wall Defects are usually present with a facial, amesiaΙ, a lingual, and a distal \Λ/all. Because theysometimes encircle an entire tooth, 4 \Λ/all defectshave been called circumferentiaΙ or moat defects(Figure 20). Osseous surgery is not the treatment ofchoiοe for 4 wall defects.
FIGURE 20. A dried human specimen with a 4 wall well defect on thebuccal of a maxillary second molar. The 4 walls are the distal wall atthe distal buccal line angle, the buccaΙ Wall, the mesial Wall at themesial buccal line angle, and the lingual interproximal wall.
. 1, 2, 3, and 4 Wall Defects are also known as combination defecΙs' They are usually found only interprox-imally, but will be found anywhere there is enoughbone present to form walls in the wake of advanοing
78

cHAPτER 8
periodontitis (see 3 wall defects). A combinationdefeοi will be more complex (more walls) apicallythan coronally (Figure 21). Coronal 1 and 2 waΙlportions of οombination defects are Sometimesmanageable by osseous surgery. The apical portionsof combination defects are usually candidates forperiodontaΙ regeneration.
Decisions over whether or not to use osseous surgery inthe management of periodontal bony defects shoulddepend upon:
ο The number of remaining walls
. Τhe depth of the defect
. The width of the defect
o The proximity of the defect to imρortant anatomicallandmarks
. The amount of bone that will be removed to achievepositive bony architecture
. The predictability of alternate forms of therapy
Segments of the periodontium with generalized horizonialpatterns of bone loss and multiple shallow interproximalosseous defects with less than 3 walΙs are traditionalindications for osseous Surgery. other indiοations forosseous Surgery inοlude:
The management of Grade I and early Grade ll furca-tion invasions (Figures 20 and 23)
The management of bony ledges and interproximalbone flattened by periodontitis (Figure 22)
The management of exostoses and tori (Figure 24)
Root resections or amputations (Figure 25)
Crown lengthening procedures where osseousSurgery will be used to remove enough suρportingbone to support prosthetic treatment ρlans
F|GURE 22. A dried human specimen of a bοny ledge buccal to maxillarymolars. As periodontitis occurs over these teeth, the ledge maybecome the mesiaι, buccal, and distal walls of a 3 Wall or a 4 WaΙΙosseous defect.
FIGURE 23. A dried human specimen showing horizontal bone loss andearly furcation invasions of maxillary molars. Note the fenestrationon the distal buccal root o, the first molar.
FlGURE 24. A clinical photograph showing the surgical expοsure o,palatal torus exostoses. These bony protuberances complicate tlapelevation and positioning of palatal fΙaps and must be removedduring osseous surgery.
4***bε",ffi:'
ffi
FIGURΕ 21. A dried human specimen with a combination defect on amandibular second premolar. τhe defect has 4 walΙs apically(lingual, mesial, buccal, and distal) and 1 Wall cοronally (lingual).
φsΨ9
.::*#
-

SUBGlcAL TREATMENT: REsEcTtvE AΝD REGENERAτlvE PRocEDURES
FlGURΕ 25. A clinical photograph showing the amputation of the distalbuccal root of a maxillary tirst molar. There was a through andthrough furcation invasion from the buccal to the distal. Positivebony architeοture Will be resιored by osseous surgery after rootremoval.
The more \Λ/alls that compose the defeοt (ie, 3 wall inter-proximal intrabony defects and 4 \η/alι moat defects), themore likely the defect is contraindicated for osseoussurgery. Defects that conceivably "will hold watel' offerexcellent opportunities for bone graft containment andperiodontal regeneration procedures (see Figures 14, 19,and 20). Other contraindications for osseous surgeryinclude:
. Operating in the aesthetic zone where cosmetics willbe adverseΙy affected
. Where the removal of supporting bone during ostec-tomy will unduly compromise the attachment of teethin the operative field
. Where the removal of supporting bone during ostec-tomy will unduιy compromise the attachment of teethat the edge of the operative field
o Where a risk of root caries is considered high
. Cases where patients have experienced problemscontro|Ιing root hypersensitivity
How ls Osseous Surgery Performed? Whatlnstruments Are Used in Osseous Surgery?
Αccess to osseous defects for osseous surgery isperformed using an ΑPF. other methods of flap surgeryare Ιess suited because they limit access and do notpermit, in their classic descriptions, the opportunity toelevate apical to the mucogingival junction. The guide-lines for using an APF with osseous surgery are that:
. The APF must be full thickness to provide unre-stricted visibility of osseous defects.
. The incisions must be planned so that an adequateband of keratinized tissue is retained on the flap.
o The "scaΙloped'' incision line conforms to thepresurgical gingival morphology at the site.
o The initiaΙ inοisions follow, or "antiοipate", the finalbony contours.
o Τhe internal bevel incisions thin, or "filet", the internalsudace of the flap enough to permit passive adapta-tion of the flap to the final osseous form.
. Osseous recontouring is performed to eliminateosseous defects and re-establish positive bony archi-tecture (Figures 26 and 27).
FΙGUΗE 26. A clinicaI photοgraph showing the shaΙιow 2 and 3 Wall inter-proximal defects, the buccal ledges, and the flattened interproximalbone that is typically produced by periodontitis.
FIGURΕ 27. A clinical photograph of the segment shown in Figure 26 afterosseous surgery. The 2 and 3 walι defects, the buccal ledges, andthe tlattened interproximal bone have been eliminated. τhe boneover the buccaΙ turcation of the tirst molar has been preserved. Notethe vedical interdental groove.
. Flaps are repositioned apically to the crest of thebone and sutured in place (Figure 28).
FIGURE 28. A clinical photograph o, the flap closure ot the segment ofοsseous surgery shown in Figure 27. τhe facial alveolar οrest wascovered With sofι tissue and secured with continuous sling sutures.Pressure was applied to stabilize the llap during fibrin clot forma-tion.

cHAPτER 8
What ls a Crown Lengthening Procedure?What Will Be the Clinical Outcomes if a CrownLengthening ls Not Performed?
A crown lengthening (CL) is a preprosthetic surgicalprocedure where the principles of osseous surgery arepracticed. lt is "a surgiοaΙ procedure designed to increasethe extent of supragingival tooth structure for restorativeor aesthetic purposes by apically positioning the gingivalmargin, removing supporting bone, or both." ln reality, atypical CL procedure should ideaΙly include osseoussurgery and appropriate apical positioning of the gingivalmargin around all teeth in the surgical segment.
Failure to perform a CL wilΙ produce clinical outοomes ofloss of attachment, reverse bony architecture, andincreased probing depths around the restored teeth. τhejunctional epithelium and the conneοtive tissue attach-ment collectively occupy a reasonably constant biologiczone of gingival attachment to a tooth (Figure 29).
FiGURΕ 29. A photomicrograph oΙ a human tooth and a mildΙy inflamedmarginal periodontium. τhe zone of gingival attachment is locatedbetween the crest of the bone and the histologic base of the sulcusand is occupied by the connective tissue attachment and the iunc-tional epithelium. τhe sulcus itself iS not shown.
Occasionally, the attachment zone will be invaded byrestorative procedures. lf the impingement is notrendered permanent by restoration margins placed in thezone, any injury in the gingival attachment should repairwithout deformity. On the other hand, restoration marginsplaced in the zone could permanently impinge upon theattachment. ln this case, the zone of attachment \λ/ill bere-established apiοal to the restoration margin' usingprocesses not unlike chronic periodontitis. The mostworrisome clinical outcome is the risk to periodontalheaιth that will emerge from the increased probing depthsaround the restored tooth (Figure 30).
FlGυRE 30. A clinical photograph of osseous deformities produced by adental restoration that impinged on the biologic width. τhemorphology of the osseous crest around the first premolar followsthe crown margin contours. τhere were 5 mm probing depths on thedistal of the restored looth.
lssues of plaque control and force control must beaddressed before CL. lt is also essential that sound deci-sions be made vis-a-vis the feasibility of the CL proce-dure and the restorability of the tooth after healing. All CLprocedures result in reduced croνvn to root ratios, and inthe case of teeth that are in secondary occlusal trauma-tism, force control will be complicated even further by aCL. Τooth removal and the fabriοation of a fixed orremovable partial denture or tooth removal or the place-ment of an implant are attractive alternatives to a CLprocedure where aesthetic or periodontal deformities willbe certain outcomes.
CLs may also be accomplished using orthodontics (ie,forced eruption). ln this instance, the tooth that requiresextension for restorative reasons is orthodonticallyextruded, and then the alveolar support that movedocclusally with the tooth is removed by osseous surgery.The major advantage to forced eruption is that supportingbone is not removed from adjaοent teeth. lts disadvan-tage is that the orthodontic process may require \iveeks tomonths before the position of the extruded tooth is stable"
What ls the Biologic ι,vidth and \Mhat Are ltsDimensions? How Does the Biologic \iVidthGuide Decision-Making in the CrownLengthening Procedure?
CL procedures are based on a thorough knowledge ofthe concepts ol the biologic width (BW). Most periodon-tists wiΙl agree that the biologic width includes the fixedbiologic dimension of gingival attachment (ie, the supra-crestal connective tissue attachment of the gingival andthe junctional epithelium). Some authors include thedepth of the healthy sulcus in the biologic width as well(Figure 31).
Ιhe dimension of thedentogingiνal junction (DGJ)' as itisused in periodontics, is based upon the average of

sURGlcAL TREATMENT: REsEcτΙvE AΝD REGENERAτ|VE PRocEDUREs
hundreds of individual measurements. τhe DGJ hasthree elements and average of each is:
. The sulcus = 0.69 mm
. The junctional epithelium = 0.97 mm
. The connective tissue attachment = 1.07 mm
The concept of the BW used here includes only the junc-tional epithelium and the connective tissue attachment.Τhe dimensional sum of the BW is 2.04 mm. The dimen-sional sum of the DGJ is 2.73 mm, or, for all practicalpurposes, 3.00 mm.
d"ιωcτιn*υΕPΓrΜu'$
Sλftλc.'eeΦ\Lco'.')Εeτινε
71ΞS4ιΞFιBEιP'S
FlGURE 3'1. Biologic ν\ridth. Junctional epilheΙium and supracrestal connectivetissue fibers (dentogingival, dentoaΙveolar, circulaf, transseptal) must bemaintained in health.
Concepts of the BW \Λ/ere used aS a decision makingguide to the amount of soft and hard tissue that should beremoved during a CL so that at least 3 mm of toothstructure would remain above the crest of bone. Thatallowed 2 mm above the crΘst of bone for the connectivetissue attachment to the root and the junctional epithe-lium. The remaining 2 mm provided enough tooth struc-ture for the margin of the restoration.
\Λ/ith experience, it became apparent that 3 mm of toothstructure was probably insufficient and at least 5 mm ofsupracrestal tooth structure may be required. The 3 mmtarget was based on average data, and many BWs areeither greater or /ess than the average. τhe range'for thesum of the junctional epitheΙium and the connectivetissue attachment is probably more than twice Ιhe 2.o4mm average dimension.
When it comes to individual patients, averages amonggroups of subjects may not apply. Healthy nonperiodon-titis sites in a given patient usually display uniform BWs,and the radiographic distance bet\Ι/een the cEJ and thecrest of alveolar bone at healthy sites could be used as aguideline for determining the BVι/ for individual patients.The finding that up to 12Υ" ot teeth restored after surgicalCL procedures showed evidence of recession within 6months suggested that clinicians need to expose >3 mmof tooth structure during CLs. lndeed, restoration marginsplaced <1 mm from the alveolar crest tend to producemore gingival bleeding, deeper probing depths, andgreater loss of periodontal attachment than restorationmargins placed >2 mm from the crest.
Hoιv ls the Crown Lengthening Performed? lsthe Position of the Relocated Alveolar CrestStable Over Time?
The components of a CL are:
. The selection of an appropriate οase for CL (Figure32)
FIGURE 32. A clinical photograph of a case selected for crown length-ening. Additional clinicaΙ crown is needed for restoration of thelateral incisors.
. Α full thickness mucoperiosteal flap
. Removal of supporting and nonsupporting bonearound the tooth in question and adjacent teeth in thesurgiοa| field following the principles of osseoussurgery
o Root planing the exposed root up to a millimeter ofthe alveolar οrest
. Αpically positioning the flap margins to the ne\,v levelof the alveolar crest (Figure 33)
FIGURE 33- A clinical photograph of the apically positioned flaps aftercrown lengthening. AdditionaΙ increased length of the clinicalcrowns is apparent.
lnstrumentation (ie, root planing) to the crest of bonefrequently results in additional bone resorption to providespace for a new biologic width. To prevent this un\ivantedand unpΙanned for loss of tooth support and to minimizerecession following CLs, it is suggested that a 1 mm zoneof periodontal attachment fibers be preserved coronal tothe alveolar crest.
82

CHAPτER 8
The properly planned and executed CL that conforms tothe principles of osseous surgery and respects theconcepts of the biologic width will result in stable restora-tion and periodontal tissue relationships (Figure 34).
F|GURE 34. A clinical ρhotograph of the healed and restored case
How Does Osseous Surgery Heal? Does theApplication of Hand and Rotary lnstrumentsto Bone Delay the Healing of an APF WithOsseous Surgery?
ln general, osseous surgery heals according to the basicprinοipΙes of periodontal wound healing. lrregularities anddelays in healing events will depend upon the extent ofosseous manipulation and the duration of the procedure.
The healing of bone following osseous surgery occurs in
two phases.
. Phase one begins aΙ day 4 with the appearance ofosteoclasts in the marro\,v and periodontal ligament. ltreaches a peak during the second week of healingand ends early in the third postoperative week. Theoutcome of this reactive bone resorption is an overallloss of crestal alveolar bone. The amount of resorp-tion will range from several millimeters to somethingless than a millimeter.
. Phase two begins during the second postoperativeweek with the initial deposition of osteoid by osteo-blasts. The measurable events of phase two (ie, therecovery of most of the bone lost in phase one) areοomplete by the end of the third month' Evidence ofbone maturation and remodeling can be seen in
osseous surgery wounds for over 18 months.
Postoperative wound care of ΑPF and osseous surgerywounds should include weekly postoperative visitsthrough the end of the sixth week of healing. Τhe effec-tiveness of plaque control by the patient must be moni-tored closely, and professional supragingivaldebridement should be pedormed weekly. During the firstmonth, the patient should avoid harsh foods, such asshellfish, popcorn, peanuts, and pretzels that mightdisplace the flap from the underlying bone.
PERIoDoNτAL REGENERATIoN
τhe ultimate goal for any dental therapy would be torestore that which has been damaged or destroyed bydisease to its original form. Periodontal regenerativetherapy is the only procedure in dentistry that restoresboth histologically and functionally identiοal tissue to thatwhich has been lost. Significant progress has been madeto ensure predictable results when applied to the appro-priate clinical situations.
ls it Possible to Regenerate Lost AttachmentApparatus on a Previously Diseased RootSurface?
Many studies and case reports have demonstrated newalveolar bone growth in areas of previous periodontaldisease' Clinical or radiographiο evidence of new bonegrowth alone does not indicate \Λ/hether or not the attach-ment apparatus has been regenerated. For many years,the ability to stimulate the formation of new attachmentapparatus on a previously diseased root surface had yetto be ansvι/ered. Τhe regeneration of true new histologicattachment apparatus was shown by Bowers, et al, inseveral studies entitled "Histologic Evaluation of NewAttachment in Humans." ln these studies, the most apicalextent of radicular οalοulus in a periodontal defect wasmarked by making a notch with a 1/4 round bur. Theroots νvere then submerged by being covered with thegingival flap with the osseous defects left unfilΙed ortreated with demineralized freeze-dried bone. After a 6-month healing period, the roots and surrounding hardand soft tissues were surgically removed for histologicanaΙysis. Consistent formation of bone, ne\r/ cementum,and periodontal ligament was shown coronal to the notch.The average amount of new attachment apparatusformed νvas approximately 2 mm, the amount dependingon the treatment utilized.
What CellTypes Are lnvolved in Regenerationof the Periodontium?
Pluripotential progenitor celΙs from the periodontal liga-ment and bone are responsible for regeneration of theattachment apparatus. These cells differentiate into oste-obΙasts, cementoblasts, and fibroblasts to form new peri-odontal tissues. lt has been shown that junctionalepithelial cells and cells from the gingival connectivetissues do not contribute to regeneration. lt is preferablethat these cells be excluded from the healing surgical siteto allow complete regeneration to occur. Regeneration islimited by the ability of these pluripotential cells and thevasculature to proliferate into a defect or furcation area.
What ls Meant by the Terms Osteoconduction,Osteoinduction, and Osteogenesis?
Osteoconduction. The creation of a site suitable forbone growth. The graft material acts as a trellis orscaffold around and through which new bone willform. ln regeneration, this includes the use of variousbone fill materials that act as a trellis or template to

sURGlcAL TREATMΕNT: BEsEcτlvE AND REGΕNΕRAT|VE PROOEDUREs
assist in ne\Λ/ bone formation. Τhe graft material itselfdoes not have any properties that actuaΙly stimulatene\Λ/ bone formation'
Osteoinduction. The direct stimulation of nevιl boneformation. This inductive process may be achievedby a bone-grafting material containing substancessuch as bone morphogenetiο proteins or other growthfactors (platelet-derived gro\,vth factor, insulin-likegrowth factor, transforming growth factor B).
Osteogenesis: The development or formation ofbone, usually by the grafting of bone forming cellsfrom one site to another.
What ls "Bone Fill" in Periodontal Therapy?
Bone fill is the clinical restoration of bone tissue in atreated periodontal defect. Bone fill does not address thepresence or absence of histologic evidence of a newconnective tissue attachment or the formation of a newperiodontal ligament. Clinically, bone fill may be demon-strated as increased bone in a defect on surgical re-entryor radiographic radiopacity in an area that previouslydemonstrated a periodontal defect.
What ls Guided Tissue Regeneration?
Guided tissue regeneration is a procedure that blocks therepopulation of the root surface by long junctional epithe-lium and gingival connective tissue to allow cells from theperiodontal ligament and bone to repopulate the perio-dontal defect. This physical blockade may be aοcom-plished using nonresorbable barriers such as expandedpolytetrafluoroethylene (ePTFE) or resorbablemembranes and barriers such as Type 1 bovine collagen,calcium sulfate, or polylactic acid (Figures 35Α and B).
FlGURΕ 35A. Expanded Polytetrafluoroethylene Membrane (ePτFE).Nonresorbable ePτFE membranes come in several shapes fordifferent anatomic locations. (Couιlesy of Dr. Paul A. Posen)
FlGURE 35B. Expanded Polytetrafluoroethylene Membrane (ePτFE). AnePτFE membrane is in place durin9 a regenerative procedure for thefurcation of the molar. (Courtesy of Dr. Paul A. Rosen)
What Are the lndications for PeriodontalRegeneration Procedures?
Case seiection and proper technique are critical to thesuccess of regenerative therapy. Currently, regenerativeprocedures are applicabΙe and predictable under acertain set of circumstances:
. The patient exhibits exemplary plaque control bothbefore and after regenerative therapy.
o The patient does not smoke.
. There is occlusal stability of the teeth at the regenera-tive site.
. Osseous defects are vertical in nature, with the morewalls of bone remaining increasing the likelihood ofregenerative success (if the osseous defect will hold\Λ/ater, regenerative therapy is a viable treatmentoption). The probabiΙity of success is as follows:three-wall defects > two-wall defects > one-walldefects, and class l furcas > class ll furcas \Λ/ith areasof horizontal bone loss and class lll or class lV furca-tion involvement offering no chance of practicalregenerative success.
What Are the Contraindications forPeriodontal Regeneration Procedures?
There are general and specific contraindications forregenerative therapy. Flap surgery of any kind is contra-indicated in patients who do not exhibit excellent plaqueοontrol. Performing surgery in a plaque-infected dentitionwill result in further attachment loss. Patients with anunstable medical condition are also poor surgical risks. lthas been sho\η/n that smoking results in poorer treatmentoutcomes with both surgical and nonsurgical therapy.Osseous defects must have the appropriate topography(numbers of walls, furcation involvement) and depth forregenerative therapy to be effective.
What Are the Expected Clinical andRadiographic Results from PeriodontalRegeneration Procedures?
Decreased probe depth, increased tooth stability, andclosure of furcations are the expected clinical outcomes
84

CHAPTER 8
of regenerative therapy. Radiographically, there shouldbe evidence of increased bone density (radiopacity) inpreviously detected vertical or furcation defects. Regen-erated defects heal at markedly different rates in differentindividuals. Final radiographic healing may continue up to2 years after the surgical procedure (Figures 36, 37, and38).
FlGUΒE 36A. Badiographic Evidence of Bone Fill. τhis patient had a 10mm defect on the distal of the molar.
FIGURE 368. Radiographic Evidence of Bone Fill. Seven months afterguided tissue regeneration with a DFDBA graft, significant osseoushealing is visible. τhe increase in radiodensity in this area continuedfor another year. clinically, the probing in ιhis area was reduced to 3mm.
FlGURE 37Α- Demineralized Freeze-Dried Bone Allograft (DFDBA) WithouιGτR. Preoperative radiograph shows severe bone loss on the distalof lhe maxillary right second premolar. A vertical defect is alsovisible on the distal of the canine.
FΙGURE 37B. Demineralized Freeze-Dried Bone Allograft (DFDBA) withoutGTR. Afιer flap reflection, the extent of the defects is apparent.
FlGUΒE 37ο. Demineralized Freezθ-Dried Bone Allo9raft (DFDBA) withoutGTR. The defects have been fil|ed wilh rehydrated DFDBA. Εxcessgraft material was removed be{ore flap closure.
FlGURΕ 37D. Demineralized Freeze-Dried Bone Allografι (DFDBA) withoutGτR. one year after surgery, the patient shows exemplary plaquecontrol and optimaι gingival health' Probings on the distal of thesecond premolar decreased trom 10 mm to 4 mm.
85
-

SURGlcAL TREATMENT: REsEcτιvE AND REGΕNΕRAτ|VE PROOEDURES
FIGURE 37E. Demineralized Freeze-Dried Bone Allograft (DFDBA) withoutGTR- τhere is radiographic evidence of substantiaι bone fill on thedistal of the second premolar and the distal of the canine.
F|GURES 38A and B. Guided τissue Regeneratiοn and DFDBA Graft. Aand B' τhis 32_year-old patient had one periodontal defect on themesial of ιhe lateral incisor. (case courtesy of Dr' Paut A' Rosen)
FiGURE 38c. Guided τissue Regeneration and DFDBA oraft. A 2-walldefect was present on the mesiotacial aspect of the lateral incisor.(case courtesy of Dr' Pauι A. Rosen)
FιGURE 38D. Guided Tissue Regeneration and DFDBA Graft. An ePτFEmembrane was placed over a DFDBAgtaf1- (οase courtesy ot Dr. PaulA. Rosen)
FlGURE 38Ε. Guided τissue Regene.ation and DFDBA Graft.Significant bone was regenerated and the tissue returned to astate of health. (Case courtesy of Dr. Paul A. Rosen)
86

CΗAPτER 8
FIGURE 38F. Guided Tissue Regeneration and DFDBA Graft.significant bone was regenerated and the ιissue returned to astate of health. (case couΙtesy of Dr' Pauι A' Rosen)
What Materials May Be Utilized in PeriodontalRegeneration Procedures?
Bone graft materials:
Autograft: Α graft from one part of an individualto another part of that same individual. Autograftsinclude iliac crest marro\Λ/, osseous οoagulum,harvested bone from a healing extraction site,bone swaging, and bone shavings from varioussources.
lliac crest marro!ν grafts have sho\r/n to have thehighest osteogenic potential. Unfortunately, thereis high morbidity with this material as procuringiliac crest marro\η/ is expensive and painful, andthese grafts have been shovvn to cause signifi-cant root resorption over time.
Osseous coagulum is bone that is harvested wiiha slow speed at about 25-30,000 rpm. Τhe boneis then mixed with blood. Bone may be harvestedfrom extraction sites that are 6-12 weeks old.Bone swaging is the creation of a "greenstick"fracture to move bone into a defect without sepa-rating the grafted bone from its base. Bone shav-ings may be collected from exostoses,edentulous ridges, or the lingual bone of themandible.
Allograft: Α graft between genetically dissimilarmembers of the same species. Freeze-driedbone alΙograft and demineraΙized freeze-driedbone allografi (DFDBA) are the two major typesof allografts. DFDBA contributes to bone gro\r/th
by osteoinduction as the bone morphogeneticproteins are exposed by the demineralizationprocess. Properly procured and prepared allo-graft materials are nonantigenic and do nottransfer infeοtious agents to the recipient. Τhese
graft materials should be obtained from licensed,accredited tissue banks that can ensure theseconditions of procurement and preparation(Figures 394 and B).
FlGURE 39Α. Demineralized Freeze-Dried Bone Aιlograft. DFDBA materialas it is received from the tissue bank.
FlGURΕ 39B. Demineralized Freeze-Dried Bone Allo9raft. DFDBA materialin a Dappen dish awaiting rehydration with sterile saline.
Alloplast: Α Synthetic or inert foreign graft. Thereare many alΙoplast graft materials, some resorb-able, and Some nonresorbable. Αmong alloplastmaterials are "bioactive" silica based glasses,nonresorbable hydroxyapatite, calciumcarbonate, and others.
Xenograft: A graft taken from a donor of adifferent species. Various preparations havebeen used over the years. Currently, bovinexenograft materials, and porcine xenograftenameΙ matrix proteins are being used.

sURGlcAL TBEATMENT: REsEcτlvE AND REGENERAτlvE PROOEDUREs
Guided tissue regeneration membranes:
Nonresorbable. Expanded polytetrafluoro-ethylene (ePTFE). The majority of GTR clinicalstudies have been done using this mem-brane. The major disadvantage to any non-resorbable membrane is the need for a secondprocedure to retrieve the membrane severalweeks after the initial surgery.
Resorbable. There are several resorbablemembranes from which to choose. Some areType I collagen based and others are made ofpoΙymers that are metabolized to carbon dioxideand water.
Collagen-based membranes: Type I
coΙlagen
Polymer-based membranes: Polylactic acid
others: Calcium sulfate, pιaster of Paris
Root conditioners:
Citric acid, tetracycline, and EDTΑ (ethylenediamine tetra-acetic acid) are chelating agentsthat have been advocated as root conditioners.These substances remove the smear layer andendotoxin from root surfaces that have beenscaled and root planed, dissolve microscopicpieces of calculus, and expose collagen tufts inthe dentinal surface that can unite with the flapwhen replaced. Tetracycline also has an antimi-crobial effect. The evidence for improved regen-erative results is somewhat equivocal, and theuse of root conditioners is by clinician's prefer-ence at this time.
Growth factors:
Bone morphogenetic proteins (BMP). TheBMPs are proteins found in bone and are respon-sible for the stimulation of bone gro\Λ/th. PureBMPs may be manufactured using recombinantDNA technology.
Platelet-derived gro\Λrth factor (PDGF). PDGFis obtained from thΘ patient's own platelets andmixed with the bone graft material. This is a rela-tively new technology that shows promise inimproving the regenerative result.
Other growth factors. Other factors such asinsulin_Ιike growth factor and transforming growthfactor B are being investigated for use in regener-ative therapy.
What Are the Techniques Used inRegenerative Therapy?
Τhe overarching approach to regenerative therapy is toeliminate or control any negative influences on thehealing of both soft tissue and bone to the greatestdegree possible. The basic technique of successfulregenerative surgical therapy is as follows. There may bevariations due to specific clinical conditions or the prefer-ence of the practitioner.
Gase selection. The patient should have exemplaryplaque control and not smoke. Periodontal osseouslesions to receive regenerative therapy should be 2-or 3-wall vertiοaΙ defects at least 3 mm deep. Molarswith CΙass l and ll furcation involvement are alsoamenabΙe to regenerative therapy.
Plaque control. The better the patient's plaquecontro|, the greater the chanοes of suοcess. Surgeryin a plaque infected dentition leads to additionalattachment loss.
Marginal inflammatory control. lnflammation of thegingival margin must be controlled presurgically tomaximize gingival health for the surgical procedure.FΙap reflection and suturing are more predictablewhen accomplished in healthy marginal tissue andintraoperative bleeding is reduced. Of course, deepinflammation may still be present, necessitating thesurgical procedure in the first place.
Aseptic technique. The chance for infection fromsources other than the patient's mouth must be mini-mized. Aseptic teοhnique includes the use of steriledrapes for the patient and equipment and strictadherenοe to the sterile zone once the operator andassistant don sterile gloves. Sterile water or salinemust be applied when a high-speed handpiece isused for bony recontouring. Tap water is by nomeans sterile.
FIap design and surgica! technique. Flaps must bedesigned and incisions made to maximize the reten-tion of the interdental papillae, minimize trauma to theflap, and allow for coronal positioning of the flap if
desired. Envelope replaced flaps are often used inregenerative therapy. Vertical incisions may be usedas long as there are no anatomic or aesthetic contra-indications to their use.
Debridement" Soft tissue debridement of theosseous defect must be complete. This allows forinspection of the defect itself and exposure of anyresidual radicular calculus that is then removed byscaling and root planing.
Scaling and root planing. All visible and detectablecalculus must be removed as thoroughly as possible.Microscopic calculus may be removed by root condi-tioning.
lntramarrour penetration. lntramarrow penetration isthe creation of small holes with the corticatedosseous walls of a periodontal defect. lt is thoughtthat by penetrating the calcified walls of the osseousdefeοt, cells involved in repopulating the defect maymigrate from the marro\iv spaces more readily.
Root preparation. The use of citric acid, tetracycline,or ethylene diamine tetra-acetic acid (EDTA) todetoxify the root surface, remove the smear Ιayer,decalcify minute pieces of residual calculus, andexpose collagen tufts in the dentinal surface hasbeen advocated.
88

CHAPτER 8
Graft placement. The graft material should beplaced within the confines of the osseous defect toensure maximum success. Graft material placedoutside the defect may contribute to increased bonegrowth, but results are less predictable.
Guided tissue regeneration. The membrane usedshould be pΙaced over the osseous defect, being welladapted to the root surface and extending at least 2mm past the edges of the defect. The membrane maybe resorbable or nonresorbable as described above.The membrane aids in graft containment as well asserving as a barrier to unwanted cell migration andgrowth.
Wound closure. Primary closure should be achievedif at all possibΙe. Bone graft materials, when usedalone, must be completely covered by the flap toensure that the material remains in the osseousdefect. Membranes must be covered to minimizeplaque accumulation on the membrane surfaces andto allow for the dissolution of resorbable membranes.
Flaps are generally closed using vertical mattresssutures and monofilament suture material such asnylon suture.
Wound adaptation. The flaps must be well adaptedto the underlying bone and around the roots of theteeth. The thickness of the blood clot under the flapmust be minimized by placing gentle pressure on theflap for several minutes. Flap/wound stability is crit-ical to regenerative success. A periodontal dressingmay be used to aid in flap stability and wound protec-tion.
Postoperative care. Standard postsurgical instruc-tions apply to regenerative surgical procedures aswell. Pain and swelling must be minimized so ice andthe use of nonsteroidal anti-inflammatory drugs isrecommended. There is some evidence to suggestthat a postoperative course of antibiotics (tetracy-
cline, doxycycline, or penicillin) may be of someadvantage. Smoking is to be strongly discouraged.'The patient should not use mechanical means ofplaque control in the area. An antimicrobialmouthrinse is a useful plaque control adjunct. Thepatient should not use interproximal plaque controlmeasures untiΙ the membrane has been removed oris resorbed. Nonresorbable membranes are removed6-9 \η/eeks after surgery unless evidence of infectionnecessitates earlier removal.
What ls Guided Bone Regeneration?
Guided bone regeneration (GBR) is the application of theprinciples of guided tissue regeneration to enhancing theosseous topography of the edentulous ridge. Bone graftmaterials and barrier membranes may be used to createa space within the bony compartment of the ridge intowhich new bone will form. GBR may be used eitherbefore or in con.iunction with endosseous implant place-ment.
What ls Distraction Osteogenesis?
Distraction osteogenesis is a technique whereby bone issplit, mechanically separated in an incremental fashion,with new bone forming betu/een the separated bonysegments. The underlying biological principle is that ofosseous healing by tension-stress. As the new reparativecallus forms on either bone edge, the bone segments areslowly moved apart placing the callus under tension. Afterthe desired amount of bone length is achieved, thedistraction is halted and the bone allowed to mature.Distraction osteogenesis has applications in cranio-mandibular orthopedics and in remodeling atrophic alve-olar ridges, either to improve contour or provide room forendosseous implant placement.
-

Ξ

CHAPTER 9
GHAPTER 9: SURGIOAL TREATMENT: PERloDoNΤAL PLAsTlcSURGERY
Aesthetics are a primary focus of dental care today. Αspatients live longer and have the means by which tochange their appearanοe, more and more patients aretaking advantage of the recent advances in aesthetictreatments. Aesthetic dentistry is not only related toproper color matching of composite resin or porcelainrestorations but to the entire presentation of the orofacialcomplex. Color and contour of the soft tissues. and thesoft tissue relationship to restorations are importantοomponents of aesthetic dentistry.
What ls Periodontal Plastic Surgery?
Periodontal plastic surgery involves surgical techniquesthat alter the shape of the gingiva or edentulous alveolarridge. These techniques relate to morphological changes,not necessarily functional changes. Traditional muco-gingival procedures are also considered to be periodontalplastic surgical procedures. Functional or supportchanges must be accomplished using either guided boneregeneration or distraction osteogenesis.
What Types of SofVHard Tissue Defects MayBe Treated with Periodontal Plastic SurgeryTechniques?
Periodontal plastic surgery procedures may be used toaugment the zone of attached gingiva, correct isolated oradjacent areas of gingivaΙ recession, correct excessivegingival display (the "gummy smile"), to move or eliminatean aberrant frenum, and to augment the morphoΙogy of aresorbed edentulous ridge prior to the pιacement of afixed prosthesis.
How ls the Patient's Aesthetic PresentationEvaluated?
The patient's aesthetiο presentation includes not just thecharacteristics of the teeth but also the soft tissues(gingival margins and edentulous ridges), lips, andoverall facial appearance.
The evaluation must staft with an analysis of the patient'sdesires and a history of any aesthetic change. ln somecases, the patient has a clear idea of what features are tobe improved. ln other instances, the patient may not beaware of aesthetic problems, or may be self-consciousabout the aesthetic presentation. The patient who hidesor stifΙes a smile when something humorous is said mayhave an unrecognized aesthetic need. lt is important that,\ivhatever the need, the request is reasonable and may beaccompΙished by the praοtitioner. lt may be necessary torefer the patient to a practitioner \r/ith more expertise in
aesthetic approaches to dentistry.
Τhe face is then examined for symmetry of shape andmovement, the relationship of the interpuρillary line to themidsagittal plane, and the proportions of the variousfacial features. The rule of fifths - the breaking up of theface into 5 equal vertical sections - can help in pinpointingdisproportionate features. The overall shape of the faceand contours of the cheeks are important. The visualinclinations of the maxillary anterior teeth, particularly the
frontal visual profile of the canine, should parallel thefrontal visual contour of the cheeks. Recent work by Dr.Stephen Marquardt has attempted to quantify theaesthetically pleasing face using calculations based onThe Golden Proportion. The so-called Phi Mask has beenderived from the Golden Ratio of 1.618:1.0:0.618. Thecloser the faοial features fit the mask, the more pleasingthe faοe is to the eye. Further information may beobtained at W\iv\Λ/.beautyanalysis.com.
The lips are examined in repose and in a full smile. lt isimportant for the patient to produce a spontaneous smilethereby maximizing the extent of the exhibition of theteeth and intraoral soft tissues. A patient with a high lipline will present a Signifiοant challenge particularly if fixedrestorations are planned for the maxillary anterioraesthetic zone (Figure 1). The lateral extent of tooth visi-bility is also determined (Figure 2).
F|GURE 1. τhe High smile Line. This patient's high smile line makes anyperiodontal or restorative therapy a challenge to maintain a pleasingaesthetic presentation.
F|GURE 2. τhe Broad smile. τhis patient shows the mesial of the maxil-lary first molar when she smiles. Metal restorations in the molar areamay not be acceptable to some patients with this broad a smile,
The features of the gingiva should be studied for contoursof the gingival margins, width of keratinized tissue, eΧces-sive gingival display, any inflammation, open embrasures(the dreaded black triangles), recession, discolorations,and edentulous ridge defects in the aesthetic zone.
-

Ξ
SURG|CAL TREATMΕNT: PERloDoNTAL PLASTIC SURGERY
Tooth characteristics and position should be noted. Therelative visual widths of the maxillary central incisor-maxiΙlary lateral incisor and the maxillary οanine shou|dalso approach the Golden Proportion of 1.618:1.0 (lateraiincisoQ: 0.618 (visual width when viewed from the front,not the actual width of the canine (Figure 3). Root prox-imity may be important in developing interdental papilΙaeand proper interproximal restorative οontours (Figure 4)'
F|GURΕ 3. τhe Goιden Proportion. τhe appearance of these teeth isarranged in the Golden Proportion, 1.618:1.0:0.618.
FιGURE 4c- Root Proximity. After aesthetic crown lengthening, moreappropriate crown contours and increased embrasure space werepossible in these provisionaι reslorations.
How ls Gingival Recession Classified?Τhere are t\rio maior classifiοation systems for gingivalrecession.
The SulΙivan and Atkins Classification of recession is adescriptive system first presented in 1968. lt was thoughtat the time that it u/as often not possible to achievecomplete soft tissue coverage for the denuded rootsurface. Τhe classification system described the type ofrecession and expected amount of root coverage utilizingthe free gingival graft procedure. Deep, wide defectswere thought not to be able to be covered, althoughalmost complete coverage was possible with narrowdefects. The four classes of reοession are:
Shallow, narrowDeep, narrowShallow, wideDeep, wide
Miller presented a system of classifying recession basedboth on the apical extent of the recession and the adja-cent interproximal bone height. Τhe system also predictsthe amount of root οoverage possible. With no interprox-imal bone loss, most roots may be covered with new softtissue to the cementoenamel junction.
Miller Classification System (Figure 5):FlGURE 4Α. Root Proximity. τhe contours of the maxillary anteriorcrowns are too straight due to the proximity ot the adjacent roots.There is nοt enough embrasure space tor the interdental papillae'
FIGURE 48. Root Proximity. The surgical appearance of the closeness ofthe roots.
FlGURE 5A. Miller Recession cΙassitication. class lrecession
Class l. Recession coronal to the mucogingival junc-tion with no interproximal bone loss. 100% roolcoverage to the cementoenamel junction is ρossible.

cHAPτER 9
FIGURE 58. Miller Recession Classitication. Class ll recession
Class ll. Recession apical to the mucogingival junc-tion with no adjacent interproximal bone loss. 100%root coverage to the CEJ is possible.
FlGURΕ 5c. Miιler Recession classification. class lll recession
Class lll. Recession apicaΙ to the mucogingival junc-tion \r/ith mild to moderate adjacent interproximalbone loss. Some root coverage is possible, based onthe level of the interproximal bone.
FlGURΕ 5D. MiΙler Recession classification. class lv recession
Class lV. Severe recession with accompanyingsevere bone loss. No root coverage can be expected.
How Are Alveolar Ridge Defects Classified?
Αβproximately 95Y" of maxillary anterior edentulousridges exhibit resorption to some degree. lt is often achallenge to fabricate an aesthetically pleasing restora-tion in the face of this ridge deformity. ln addition, onceteeth are removed, ridge contours are generaΙly smoothwith root eminences obΙiterated. GingivaΙ margins andinterdentaΙ papilla are also absent when pontics are fabri-cated. li then becomes difficult to provide a pontic thatappears to be emerging from the soft tissue rather thansitting on the ridge. Ridge defects may be classified asfollows:
Seibert Classification (Figure 6).
F|GURE 6Α. seibert classification of Bidge Defects. class l facio-palataldefect
Class l. Bucco-IinguaΙ defect-ridge height is intact butthere is a concavity on the facial surface of the ridge.May be best treated with a submucosal connectivetissue graft
*.1::j+ :##r,_i;.*?:::+.; i:. 'i:::iΞffi;ii:: .
.: :i 1.*.
FΙGURE 6B. seibert classirication ot Ridge Defects. Predominantlyvertical defect
cΙass ll. Αpicoronal defect. Ridge height is lost by thefacial ridge contour is intact. This is the last commonridge defect.
-

Ξ
sURGlcAL TREATMENT: PERloDoNτAL PLAsτlc SURGERY
F|GURE 6ο. seibert classification of Ridge Defects. combination defΦt
class l]l. Combination of a class l and οlass ll defect'This may be treated wth a single procedure or mayrequire multiple procedures depending on theseverity of the initial defect.
What ls Excessive Gingival Display?Excessive gingival display, also referred to as alteredpassive eruption, delayed passive eruption, or the"gummy smile," is a condition where a significant amountof gingiva is visible in the maxillary aesthetic zone whenan individual smiles (Figure 7). This may occur when thegingival margin has not migrated to the vicinity of thecementoenamel junction (CEJ) after eruption of the tooth(altered passive eruption) or be related to skeletal anom-alies.
F|GURE 7. Altered Passive Eruption. τhe gingival margins on the maxil-lary central incisors are 5 mm coronal to the cementΦnamel iunc-tion in this 27 year old patient.
Excessive gingival display may be caused by:
. Failure of the gingiva to migrate apically along thecrown of thΘ tooth after active tooth eruption iscompleted.
o Facial crestal alveolar bone located adiacent to theCEJ thereby preventing apical migration of thegingiva.
. Vertical maxillary excess \Λ/here the gingival margin isat the proper location but the maxilla is enlarged inthe superioιinferior dimension'
. Upper lip incompetence where the upper lip does notcover the teeth or gingiva.
How ls Altered (Delayed) Passive EruptionClassified? What Corrective Procedures AreApplicable to Each Classification?
Type 1. There is excessive gingiva present. ln Type1A, the gingival margin is coronal to the cemento-enamel junction (CEJ) and the tip of the probe canpenetrate to the CEJ. The crest of the alveolar boneis apical to the CEJ. This may be corrected using agingivectomy procedure. ln Type 1B, Ιhere is exces-sive gingiva but the probe cannot penetrate to theCEJ. ln this case, the crest of the alveoΙar bone onthe facial of the tooth is most likely at the level of theCEJ. This must be οorreοted with an apically posi-tioned flap, perhaps with local gingivectomy and withostectomy/osteoplasty as neοessary to create 1-2mm of exposed root structure for the biologic width.
Type 2. The width of the gingiva is in the normalrange. ln Type 2A, the crest of the alveolar bone is 1-2 mm apical to the CEJ. ln Type 2B' Ιhe crest of thebone is at the Ievel of the CEJ. ln either case, anapically positioned flap with or without osseousrecontouring is indicated. Τhere is not enough gingivapresent to allow for a gingivectomy.
lf a gingivectomy is performed in either Type 18 or28, the tissue will grow back in a matter of monthsand the procedure will be for naught. Skeletal abnor-malities (verticaΙ maxillary excess) cannot becorrected by periodontal surgical procedures.
What Types of Procedures Are Available inPeriodontal Plastic Surgical Therapy?
There are various approaches to periodontal plasticsurgery techniques. Grafts may be autogenous, allograft,alloplast, or xenograft in nature. Ridges may beaugmented \Λ/ith οonnective tissue only, or with bone orbone substitutes with or without connective tissuegrafting. The foοus of this chapter will be on the use ofautogenous connective tissue harvested from the palateto achieve the desired aesthetic result. Details of eachsurgical procedure may be found in standard periodonticstexts or surgical atlases listed in the Reference Section.
Free ginglval graft (Figure 8)
Lateral pedicle graft (flap) (Figure 9)
Submucosal connective tissue graft (Figure 10)
lnterpositional connective tissue graft
Onlay connective tissue graft (Figure 11)
Double papillae connective tissue graft (Figure 12)
Ovate pontic seat preparation (Figure 13)
CoronalΙy-positioned flap
Allograft (Αllodermo) use for root coverage or ridgeaugmentation
Gingivectomy (Figure 14)
Aesthetic crown lengthening (Figure 15)
Frenectomy (Figure 16)

cHAPτER 9
What Materials Are Available for PeriodontalPlastic Surgical Procedures?
There are a variety of materials available for periodontalplastic surgery proοedures.
. Αutogenous gingiva, connective tissue and/or bone
ο Allograft connectiνe tissue substitutes (Allodermo) orbone grafting materials
o Xenograft bone fill materials
. Membranes used in guided tissue regeneration havebeen used to increase the zone of attached gingivaand for guided bone regeneration
What Are the Aesthetic Problems andPotential Solutions Most Often Encounteredin Aesthetic Periodontal Therapy?
Surgical Problems and Treatment Options
What ls a Free Gingival Graft?
A free gingival graft (Figure 8) is the grafting of a piece ofgingiva that has been οompletely detached from thedonor area to the recipient site. \Λ/hile originally intendedto increase the zone of attached gingiva, the free gingivalgraft may provide root coverage in the appropriate situa-tion. Difficulty in getting complete root coverage lies in thefact that an avascular graft is placed over a root surfacealso devoid of a blood supply. For the first 30 hours, thefree gingival graft survives by plasmatic circulation, theoozing of nutrients from the cut blood vessels of therecipient site into the graft. At day 2 the blood supplybegins to re-establish itself and continues to reorganizefor the next 28 days. Creeping attaοhment, the coronalmigration of the free gingival margin after a free gingivalgraft, may ocοur when there is coronal interproximal boneand the original dentogingival junction and free gingival
margin are removed when the reοipient site for the graft isprepared (Figures BE, F, and G). This procedure is usedto increase the zone of attached gingiva with thepossibiιity of gaining root οoverage as well.
F|GURE 8A. Free Gingival Graft. τhis patient has no keratinized tissue onthe facial surfaces of the mandibular central incisors.
F|GURΕ 8B. Free Gingival Graft. τhe graft recipient site is prepared usingsplit thickness dissection.
FIGURE 8C. Free Gingival Graft. The graft was haruested from the palateand plaοed at the recipient site.
Problem Solution(s)Gingival recΘSsion and/or
Inadequate zone of attached gingivaFree gingival gratt (Figure 8)
Submucosal connective tissue graft (Figure10)
Lateral ρedicle graft (Figure 9)
AllodermΘ graft
Continuous connective tissue gratt
coronally positioned Ιlaρ
lnadequate zone of attached gingivawithout recession
Free gingival graft (Figure 8)
AllodermΘ graft
Prevention of ridge resorption Socket preservation procedures
RetΘniion of natural teeth or roots
Resorption of the edentulous ridge SUbmuοosal connective tissue gratt (Figure10)
Onlay connective tissue graft (Figure 1 1)
Particulate bone graft
Guided bone regeneration
Distraction osteogenesis
Submucosaι connective t Ssue graft (Figure10)
Combination Drocedures (Fioure 1 7)
Abetranl
Excessiγe gingival display
Altered passive eruption
Gingiveοtomy (FigUre 14)
Aesthetic crown lengthening (Figure 15)
ot'hοοnathie sllrnοru
-

Ξ
sURGlcAL TREATMENT: PEΒloDoΝτAL PLAsτlc sURGERY
F|GURΕ 8D. Free Gingival Graft. Finaι heaιing. The zone of attachedgingiva was increased and 2 mm of root coverage was accomplishedon the right central incisor.
F|GURE 8Ε. Free Gingival Graft. Preoperative view of a free gingival graftsite.
FlGURE 8G. Free Gingival Graft. τhe root of the right central incisor waseventually covered with gingiva due to creeping attachment.
What ls a Lateral Pedicle Graft?Α lateral pedicle graft (Figure 9) iS the transposition ofgingiva from one site to an adjacent area of recession orminimal attached gingiva while leaving the bΙood supplyof the donor connected at the base of the graft. lncreasedroot οoverage compared to a free gingival graft may beexpected. Τhe donor site must have a sufficient amountof gingiva to be moved. lt is possible to get a slightamount of recession at the donor site. This technique isused to obtain root coverage and increase the zone ofattached gingiva.
FiGURE 9Α. Lateral Pedicle Fιap. Tttis patient had severe reοession onboth the maxiιlary and mandibuΙar canines.
FlGURΕ 98. Lateral Pedicle Flap. τhe lateral pedicle graft in pιace on themandibular left canine- τhe denuded area by the donor site wilI healby granulation and maturalion.
FlGURE 8F. Free Gingival Graft. τhree weeks after the graft was placed.
96

CHAPTER 9
FIGURE 9C. Lateral Pedicle Flap. Complete root coverage was obtained.
What ls a Submucosal Connective TissueGraft?
Α submucosal connective tissue graft (Figure 10) is onewhere connective tissue devoid of surJace epithelium iseither compΙetely or partialΙy submerged under a par1ial
thiοkness flap or ρlaced in a prepared pouch. This graftmay be used to augment a deficient ridge, usually aSeibert Class I or Class Ill defect. The submucosalconnective tissue graft may also be used to cover adenuded tooth root.
FlGURΕ 1 0Α. submucosal connective Tissue Graft. τhis patient presentswith a Seibert Class I ridge defect.
FIGURE 10B. submucosal connective Tissue Graft. τhe 4 mm depth otthe defect strained this procedure to the limit due to the inelasιicityof the gingiva.
F|GURE 10c. submucosal connective Tissue Graft. τhe graft is in place.Notice the smalΙ vertical lear in the pouch. τhis healed withoutcomplication.
F|GURE 1 0D. submucosal connective τissue Graft. The facial contour ofthe ridge was completely restored with one graft procedure.
FlGURE 10E. submucosal connecιive τissue Graft' τhis patientpresented with a Class I ridge defect and recession on the maxillaryleft lateral incisor.
97
-

Ξ
sURGΙcAL TREATMENT: PERloDoNτAL PLAsτlc sURGERY
FlGURΕ 10F. submueosaΙ connective τissue Graft. τWo submucosalgrafts are in place, one to correct the ridge defect and ιhe second tocover the root.
FIGURE 10G. Submucοsal connective τissue Graft. Final healing showsaccomplishment οf both goals. τhe maxilιary left central incisor isan ovate pontic.
What ls an lnterpositional Connective TissueGraft?
Τhis procedure is simiΙar to the submuοosal connectiveiissue graft when used for an edentuΙous ridge. With theinterpositional graft, the donor tissue is usually quite thickSo that the reοipient site may not be comp|etely closed.The donor tissue is placed between the facial tissue andalveolar bone, \i'fith the coronal aspect of the graftexposed. This technique is used to increase the heightand width of an edentulous ridge.
What ls an Onlay Connective Tissue Graft?
The onlay connective tissue graft (Figure 11) is essen-tially a large free gingival graft. The donor tissue iscompletely severed from its blood supply and plaοed onthe edentulous ridge that has been denuded of its epithe-lium. This graft may be used for Seibert Class ll ridgedefects to increase ridge height and for Class lll defects.li may also be used to improve the facial contours of anedentulous ridge. When ρlaced, it is imperative that theonlay connective tissue graft has intimate contact with ableeding recipient site surface.
F|GURE 1 1 A. onlay connective τissue Graft. This patient lost significantridge dimension after exlraction of the maxillary anterior teeth. Sheinsisted on not have any type of removable appliance.
FlGURE 11B. onΙay connective Tissue Graft. τhe recipient site isprepared by epithelial denudation to receive the 9raft.
98
FlGURE 11c. onlay connective τissue Gratt. τhe onlay 9raft washarvested from the palate and placed with intimate adaptation to therecipient site.

CHAPτER 9
FlGURΕ 11D. onlay οonnective τissue Graft. The final fixed prosthesiswas placed using ovate pontics.
What Is a Double Papilla Connective TissueGraft?
The doubΙe papilla connective tissue graft (Figure '|2) isbasically a double papilla graft wiih donor conneciivetissue placed beneath the released tissue. This techniquemay be used to increase the blood supply over themidsection of an exposed tooth root.
FlGURE 12A. Double Papilla connective Tissue Graft. τhis patient hadιrauma to the facial 9ingiva subsequent to an endodontic perfora-tion.
FlGUFlΕ '12ο. Double Papilla connective τissue Graft. τhe final result Wasacceptable ιo ιhe patient.
What ls an Ovate Pontic?
The ovate, or egg shaped pontic, is used as the preferredpontic design once an edentulous ridge has beenaugmented. The tissue surface of the pontic is completeΙyconvex and has passive but intimate contact with theproperly prepared ridge. The advantages of the ovatepontic are that a gingival margin and interdental papillamay be sculpted from the restored ridge, giving the ponticthe appearance of a natural tooth as it emerges from thesoft tissue. The convex tissue surface of the pontic maybe easily οleaned with dental floss, dental tape, or yarn.
The ovate pontic seat is prepared (Figure 13) by anes-thetizing the patient in the vestibule, taking care not todistend the shape of the ridge. A large coarse diamond isused to prepare the ovate pontic seat. This area shouldbe about 1.5 to 2.0 mm deep vvith development ofgingival margins and interdental papillae. The pontiοshould have intimate but passive contact with the under-lying ridge surfaοe. The advantage of using connectivetissue for ridge augmentation is that there is a sufficientthickness of tissue to develop the pontic seat. There mustbe approximately 2 mm of soft tissue covering bone orgrafted bone substitute in heaΙth. When a conneοtivetissue graft is utilized, there is sufficient room to deveΙopthis site without worry of involving the underlying bone.
FiGURE 1 3Α. ovate Pontic seat Preparation. Pretreatment view showingan attempt at gingival colored porcelain.
FlGURE 12B. Double Papilla connective τissue Graft' τhe connectivetissue graft is ρlaced under the lifted interdental ρapilla.
99
-

Ξ
sUΒGlcAL TΒEATMENT: PEBloDONTAL PLASτ|c sURGERY
FlGURE 138. ovate Pontic seat Preparation. An examplθ of the coarseround diamond used to prepare the depression and define thegingival margins and interdental papilla.
F|GURΕ 13c. ovate Pontic seat Preparation- τhe pontic seat preparedand ready for the provisional restoration.
What ls a Coronally Positioned Flap?
A οoronally positioned flap is, as the name suggests, thecoronal placement of an elevated flap. Τhis proceduremay be used to cover an area of recession or to cover aconnective tissue graft that has been placed on a rootsuιJace. There must be interproximaΙ bone of sufficientheight to support this flap in its new coronal position. Theextent of οoronal posiiioning may be limited by the depthof the vestibule, as this depth will be shallower with thisprocedure.
What ls a Gingivectomy?
A gingivectomy (Figure 14) is the surgical removal ofexcess gingiva down to the base of the sulcus. Τhis isaοcomplished using an external bevel incision. Τheremust be a sufficient amount of attaοhed gingivaremaining after the procedure for this technique to beused. A gingiveοtomy is the procedure of choice withType 1A excessive gingival display. Gingivoplastyreshapes the gingival contours without removing any ofthe soft tissue pocket wall.
F|GURE 14A. Gingivectomy for Excessive Gingival Display. τhis patientpresented with Type 1A altered passive eruption.
FIGUΗE 148. Gingivectomy for Excessive Gingival Display. A gingivec-tomy Was pertormed because there was sufΙicient gingiva and thecΕJ was reached preoperatively.
FlGURΕ 1 3D' ovate Pontic seat Preparation. τhe provisional restorationwith ovate pontic for the patient shown in Α.
100

cΗAPTER 9
F|GURE 14ο. Gingivectomy for Excessive Gingival Display. Final healingafter ιhe palient received composite veneers on the maxillary inci-sors.
What ls Aesthetic Crown Lengthening?Aesthetic cro\η/n |engthening (Figure 15) is an apicallypositioned flap with or without osseous recontouring(resective surgery) to improve the aesthetic presentation.ln many cases, routine resective surgery to treat perio-dontitis will detract from a pleasing appearance in theaesthetic zone. With excessive gingival display, this typeof procedure may be of great benefit to the patient.
FlGURE 15Α. Aesthetic crown Lengthening for Excessive GingivalDisplay. τhis 25 year old lemale presented With τype 2B alleredpassive eruptiοn.
FlGURE 15c. Aesthetic crown Lengthening for Εxcessive GingivalDisplay. Bone is removed to aΙΙow room for ιhe biologic width and tobe able to apically position lhe gingival flap.
FIGURE 15D. Αesthetic crown Lengthening for Excessive GingivalDisplay. τhe flap is placed With the gingival margins at the cΕJ ofeach tooth.
FlGUΒΕ 15E' Aesthetic crown Lengthening ,or Excessive GingivalDisplay. The compΙete contours of the crowns of the teeth are nowvisible-
FΙGURE 15B. Aesthetic crown Lengιhening ,or Εxcessive GingivalDisplay. After flap reflection, the crestal bone is seen aι the cEJ.
101
-
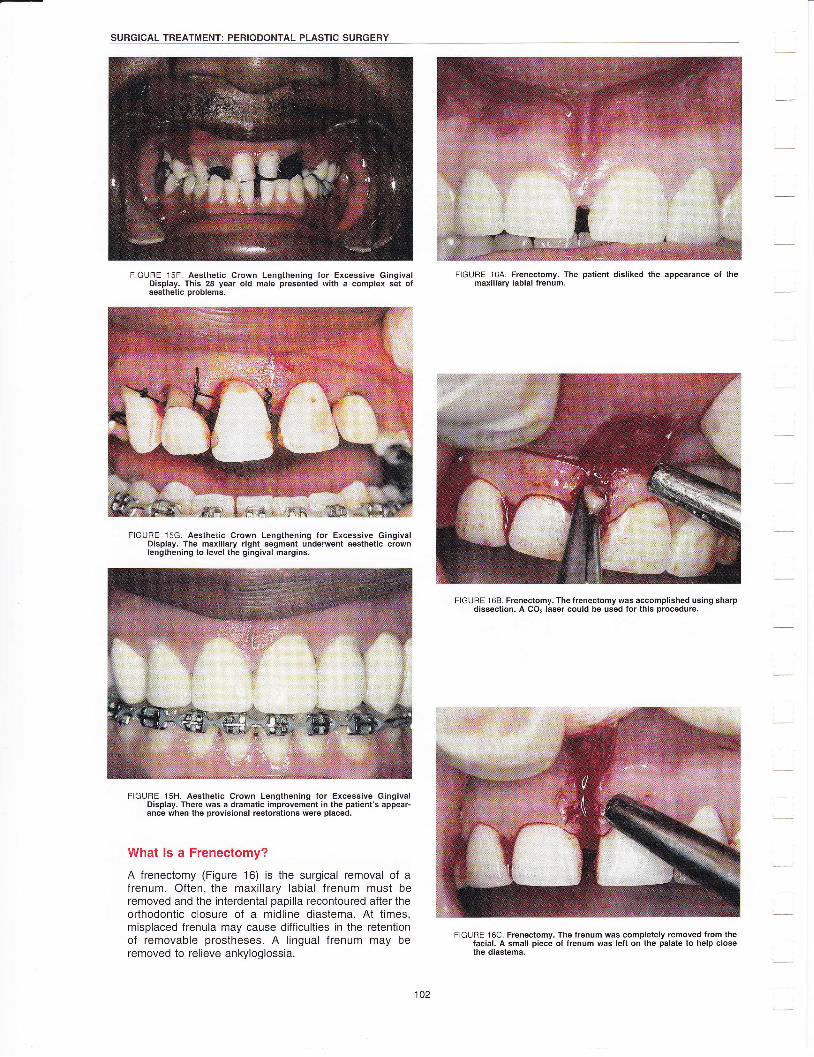
sURGlcAL TREATMENT: PEΒloDONτAL PLAsTΙc sURGERγ
FlGURE 15F. Aesthetiο crown Lengthening for Excessive GingivalDisplay. τhis 28 year old male presented With a complex set ofaesthetic probΙems.
FlGURΕ '15G. Aestheiic οrown Lengthening for Εxcessive GingivalDisplay. The maxillary right segmenl underwent aesthetic crownlengthening to level the gingival margins.
FlGURE '15Η. Aesthetic crown Lengιhening tor Excessive GingivalDisplay. There was a dramatic improvemeηt in the patient's appear-ance when the provisional restorations were placed.
What ls a Frenectomy?
Α freneοtomy (Figure 16) is the Surgical removal of afrenum. Often, the maxillary labial frenum must beremoved and the interdentaΙ papilla recontoured after theorthodontic closure of a midline diastema. Αt times,misplaced frenula may cause diffiοulties in the retentionof removable prostheses. Α lingual frenum may beremoved to relieve ankyΙogΙossia.
F|GURE 16A. Frenectomy. τhe patient disliked the appearance of themaxiΙlary labial frenum.
FlGU RE 1 6B. Frenectomy. τhe frenectomy was accomplished using sharpdisseclion. A CO2 laser could be used for this procedure.
F|GURE '16ο. Frenectomy. τhe frenum was completely removed from thefacial. A small piece of frenum was left on the palate to help closethe diastema.
102

CHAPTER 9
FlGURE 1 6D. Frenectomy. τhe diastema Was closed With composite resin.Orthodontic therapy was not an option in this case.
What ls a Socket (Ridge) Preservation?
Socket preservation, better described as ridge preserva-tion, iS the maintenanοe of the dimensions of the alveolarridge after the removal of a tooth. This is particularlyimportant in the aesthetic zone where ridge resorptionshould be minimized. Socket preservation may beaccomplished by keeping the facial plate of bone intactand placing a bone fill material in the socket. There maybe some sΙight resorption even with these measures.Shallow Seibert ridge defects are much easier to rectifythan deep ridge concavities.
Ηow ls the Patient Treatment Planned forAesthetic Periodontal Therapy?
Treatment of the aesthetic patient usually requires amultidisciplinary approach. ln many cases, the perio-dontal plastic surgical procedures are done in conjunctionwith, or in advance of, restorative dentistry. ln situationswhere excessive gingival display, recession, or a lack ofattached gingiva is ihe problem, the periodontal plasticsurgery procedures may stand alone.
ln compΙex cases, the patient must be advised that theaddition of aesthetic surgery to the treatment plan willincrease the effort, expense, and time for treatmentcompΙetion. The patient should also be reminded fromtime to time, that alΙ of the bother will be weΙl worth it inthe final outcome. As with other plastic surgical proce-dures, the desired result may not be obtained or bepossible with one approach. Combination procedures(Figure 17) may be necessary to achieve complete reso-Ιution of the aesthetic challenge.
F|GURES 17A and B. combination τherapy. This patient has resectiveperiodontal surgery after the placement of the crowns in the maxiFlary arch.
F|GURΕ 17c' combination Therapy. τhe right centraι incisor wasremoved and a submucosal connective ιissue graft placed.

SURG|CAL TREATMEΝT: PERloDONTAL PLAST|C SURGERY
FlGURΕ '17D. combination Therapy. An onlay grafι was the second stageprocedure performed.
F|GURE 17E. combination Therapy. τhe ovate pontic seats WereprΘpared.
FIGURE 17F. Combination Therapy. Four years after the completion oftherapy the aesthetic zone remained stable.

CHAPτER 10
OΗAPTER 10: PERIODONTAL EMERGENOIESPeriodontal emergencies are a part of the everyday prac-tice of dentistry. The clinician must be able to assess theemergent condition rapidly and accurately in order toprovide relief for the patient. Effective management ofperiodontal emergencies aids in both the patient's phys-iοal and psychological well-being and may contribute topersonal satisfaction for the treating clinician.
Clinical manifestations and general treatment regimenswill be presented in this chapter. Detailed informationabout therapeutic agents may be found in Chapter 6.
νvhat Are the Common PeriodontalEmergencies?
o Acuteherpeticgingivostomatitis
o Necrotizing ulcerativegingivitis
. Periodontal abscess
ο Pericoronitis
o Differentiation of the endodontic from periodontalabscess and the combined endodontic-periodontalabscess (lesion)
How ls the Diagnosis of the EmergencyCondition Determined?
One of the most difficult yet rewarding challenges indentistry is arriving at an accurate diagnosis andrendering appropriate treatment for the emergencypatient. Τhis patient presents with an acute prob|em andis seeking immediate relief. At this time, all dental proce-dures should be focused on identifying and rectifying theproblem at hand. Proper treatment of the emergency mayprovide the practitioner with a lifelong patient.
A diagnosis may be determined by first obtaining acomplete history of the problem from the patient andcompleting a targeted clinical and radiographic examina-tion. Questioning the patient regarding the signs andsymptoms of the problem may lead to the diagnosis.
ο ls the problem acute or chronic?
ls there pain?
ls the pain sharp, dull, or throbbing? (Periodontalpain is usually dull or throbbing.)
ls the pain intermittent or chronic?
Does anything in particular cause the pain (cold,sweets)?
Did the pain awaken the patient from a soundsleep? (A yes ansνver, the problem is usually endo-dontic in nature.)
ls the pain relieved/made worse by cold? (Painrelieved by cold, think endodontics.)
Does heat make the pain worse? (Yes, think endo-dontics.)
Does the tooth in question feel longer (now bitingon that tooth first)? (Yes, think endodontics.)
ls the tooth sensitive to biting or percussion?
ls the tooth mobile?
Has there been any swelling? (Localized by gingivalmargin, generally periodontal; more diffuse or cellu-lites, generally endodontic in nature.)
lf so, when, what kind (indurated or fluctuant),where, and for how long?
Has there been any drainage from the swelling orbad taste?
ls there a fistula present? Can the fistula be tracedradiographically with a piece of gutta percha?
Are there any ulcers or other oral lesions present?How long have they been present?
Does the patient feel sick or fatigued?
ls the patient febrile?
Ηas this happened before?
ls it getting worse?
What are the radiographic findings?
ls the pulp vital?
What is the periodontal probing pattern? (lsolateddeep probings, probably endodontic; broad probingpattern more likely a periodontal problem.)
Are there any systemic problems (ie, diabetesmellitus Type 1 or Tyρe 2' smoking)?
Has the patient been eating popcorn or nuts? (lfyes, possibly a periodontal abscess due to foodimpaction.)
once the ans\Λ/ers to these questions have been obtained,the diagnosis is often evident. Occasionally, there is stillsome question and further tests, such as a biopsy of somesuspicious tissue, may be in order.
What Are the Signs and Symptoms of a Gingival/Periodontal Abscess?
A gingival abscess is a supeι'ficial, painful, rapidly expandingpurulent inflammatory lesion found in the supedicial gingivaltissues. A periodontal abscess (Figure t) is localized purulentinfΙammation deeper in the periodontal tissues. Both lesionsmay be marked by pain, fluctuant swelling, and collection ofpurulence. The pain generally does not awaken the patientfrom a sound sleep. The periodontal abscess may have rapiddestruction of alveolar bone. Teeth may be sensitive topercussion, mobile, and may have extruded or shifted posi-tion in the alveolar housing. A gingival abscess may occur ina patient who has no chronic periodontal disease. The mostΙikely cause is the lodging of a foreign object or other irritant,usually food (popcorn hull, etc)' in the gingival tissues. Αperiodontal abscess may be οaused by the entrapment of aforeign object, loose calculus after scaling and root planing,or by superficial healing of the gingival tissues \Λ/ith activeinfection deeper in the pocket.
105
-
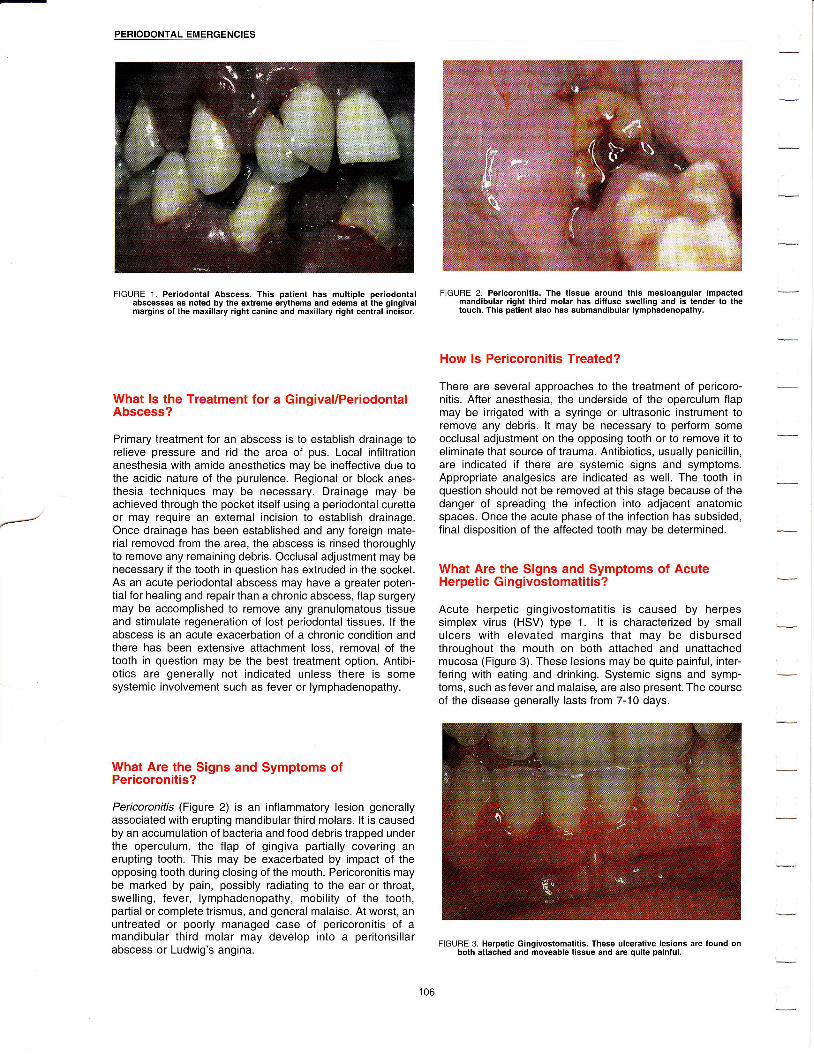
Ξ
PΕRloDoNτAL EMERGENclEs
FlGURE 1. Periodontal Abscess. τhis patient has multiple periodontalabscesses as noted by the extreme erythema and edema at the gingivalmargins of the maxillary right canine and maxiΙlary right central incisor.
What ls the Treatment for a Gingival/PeriodontalAbscess?
Primary treatment for an abscess is to establish drainage torelieve pressure and rid the area of pus' Local infiΙtrationanesthesia with amide anesthetics may be ineffective due tothe acidic nature of the purulence. Regional or block anes-thesia techniques may be neοessary. Drainage may beachieved through the pocket itself using a periodontal curetteor may require an external incision to establish drainage.Once drainage has been established and any foreign mate-rial removed from the area, the absοess is rinsed thoroughlyto remove any remaining debris. occlusaΙ adjustment may benecessary if the tooth in question has extruded in the socket.As an acute periodontal absοess may have a greater poten-tial for healing and repair than a chronic abscess, flap surgerymay be accomplished to remove any granulomatous tissueand stimulate regeneration of lost periodontal tissues. lf theabscess is an acute exacerbation of a chronic condition andthere has been extensive attachment loss, removal of thetooth in question may be the best treatment option. Antibi-otics are generally not indicated unless there is somesystemic involvement such as fever or lymphadenopathy.
What Are the Signs and Symptoms ofPericoronitis?
Pericoronitis (Figure 2) is an infΙammatory Ιesion generallyassociated \Ιvith erupting mandibular third molars. lt is causedby an accumulation of bacteria and food debris trapped underthe operculum, the flap of gingiva partially covering anerupting tooth. This may be exacerbated by impact of theopposing tooth during closing of the mouth. Pericoronitis maybe marked by pain, possibly radiating to the ear or throat,swelling, fever, lymphadenopathy, mobility of the tooth,partial or complete trismus, and general malaise. Αt worst, anuntreated or poorly managed case of pericoronitis of amandibular third molar may develop into a peritonsillarabscess or Ludwig's angina.
FιGURE 2. Pericoronitis. τhe tissue around this mesioanguιar impactedmandibular right third molar has diffuse sweιling and iS tender to thetouch. τhis patient also has submandibular ιymphadenopathy.
How ls Pericoronitis Treated?
There are several approaches to the treatment of pericoro-nitis. After anesthesia, the underside of the operculum flapmay be irrigated with a syringe or ultrasonic instrument toremove any debris. lt may be neοessary to perform someoοcΙusal adjustment on the opposing tooth or to remove it toeliminate that source of trauma. Antibiotics, usually penicillin,are indicated if there are systemic signs and symptoms.Αppropriate analgesics are indicated aS vι/ell. The tooth inquestion should not be removed at this stage because of thedanger of spreading the infection into adjacent anatomicspaοes. once the acute phase of the infection has subsided,final disposition of the affected tooth may be determined.
What Are the Signs and Symptoms of AcuteΗerpetic Gingivostomatitis?
Acute herpetic gingivostomatitis is caused by herpessimplex virus (HSV) type 1. lt is characterized by smallulcers with elevated margins that may be disbursedthroughout the mouth on both attached and unattachedmucosa (Figure 3). These lesions may be quite painful, inter-fering with eating and drinking. Systemic signs and symp-toms, such as fever and malaise, are also present. The courseof the disease generalΙy lasts from 7-10 days.
FlGURE 3. Herpetic Gingivostomatitis. τhese uιcerative lesions are found onboth attached and moveable tissue and are quite painful.

CHAPτER 10
What ls the Treatment for Acute HerpeticGingivostomatitis?
Τhere is a two-pronged approach to the treatment of acuteherpetic Aingivostomatitis. First, antiviral agents, such asacyclovir, may be used topically and/or systemically to controlthe infection. ln addition, palliative therapy to relieve painmust be initiated to allow the patient to eat and drink. Dehy-dration is a threat, particularly in infants and small children.Once the acute phase of the disease has passed, about onethird of these patients will have recurrent herpes infections.These recurrent infections may be managed with the antiviralmedications. There is some evidence to suggest that theamino acid, lysine, may play a role in prevention or attenua-tion of herpetic outbreaks by disrupting viral replication.
\Mhat Are the Signs and Symptoms of NecrotizingUlcerative Gingivitis (NUG)?
The patient with NUG presents for treatment because of pain.This disease is characterized by gingival and oral pain thatmay be severe, fetid oris (bad breath), necrosis of thegingival papilla that appear to be punched out, pseudomem-brane formation at the tips of the papillae, and spontaneousgingival bleeding (Figure 4). Systemic signs and symptomsinclude fever, lymphadenopathy on the affected side, loss ofappetite, and malaise. Stress, fatigue, smoking, poor oralhygiene, and an impaired immune system may all contributeto the development of NUG. NUG must be differentiated fromacute gingivitis, primary herpetic gingivostomatitis, thevesiculobullous diseases, leukemia, and the secondary stageof syphilis.
FlGURE 4. Necrotizing υΙcerative Gingivitis. τhis patient presents withextremely painful gingiva, foul smelling breath, spontaneous gingivalbleeding, and necrosis of the interdental papilιa. The patient was alsofebrile and had sUbmandibuιar ιymphadenopathy.
What ls the Treatment for Necrotizing UlcerativeGingivitis?
Necrotizing ulcerative gingivitis is treated in a stepwisefashion to control the baοterial infection, manage the acutesymptoms, and eliminate the predisposing factors. At the firstvisit, as much debris, plaque, and calculus should beremoved as gently as possible, either with hand or poweredinstrumentation. The patient should be instructed in plaqueοontrol using a neνv toothbrush. Chemotherapeuticmouthrinses (chlorhexidine, phenoliο compounds) may be
helpful although could be uncomfoι1able at first due to theiralcohol content. Αntibiotics, such as penicillin, are indicated ifthere is systemic involvement. Patients should refrain fromsmoking until the acute phase subsides although this mayincrease the patient's stress. Α bland diet should be recom-mended along with drinking plenty of Water. τhe patientshould return 24 hours after the first appointment to continuethe debridement of the area and to polish the teeth. Thepatient should return for a third visit one to t\Λ/o days later. Bythis time, the acute phase should have subsided. lf signs andsymptoms persist, other systemic diseases must be ruledout. Send for a medical evaluation if necessary.
Hoι,v ls an Endodontic Abscess/LesionDifferentiated From a Periodontal Abscess/Lesion?
Endodontic and periodontal emergencies are sometimes diffi-cult to distinguish. The patient presents with pain that issometimes severe. Other signs and symptoms may be vaguemaking a rapid diagnosis of the problem difficult. lt is impor-tant to arrive at the correct diagnosis as the sequence oftreatment is different for each type of lesion. ln general, thereare several patterns that help the practitioner differentiatebetween these t\ι/o lesions.
Pain. Both lesions may cause pain. The pain of an endo-dontic lesion may be sharp, have an intermittent naturewith each succeeding bout of pain being more intense, beof more rapid onset, and awaken the patient from asound sleep. The pain of a periodontal abscess is gener-ally more diffuse and can be described as a "throbbing"type of pain. Periodontal pain, except in the case of NUG,generally does not awaken the patient from a soundsleep. Teeth in both instances may be sensitive topercussion.
Probing depths. An endodontic abscess may drainthrough the gingival sulcus. ln general, probe depths willbe shallow until the drainage area is reached upon whichthere wilΙ be a sudden deepening of the pocket. ln othercases, the abscess may create a fistula somewhere inthe soft tissue. Using a size 30 gutta percha cone placedinto the fistula and then exposing a radiograph will oftenlead directly to the pathologiο tooth apex. Periodontallesions generally have a wider area of deep pockets.Although it is possible to have a narroνν, deep pocket,such as a pocket associated with a cervical enamelprojection of a mandibular first molar, this is less commonthan with an endodontic lesion.
Pulp vitality. This may be problematic in multirootedteeth. The pulp tissue in one canal may be necrotic withvital tissue elsewhere in the root canal system.
Endo-perio problems may be classified as primary pulpaldisease, primary pulpal disease with secondary periodontaldisease, primary periodontal disease, primary periodontaldisease with secondary pulpal disease, or combined pulpaland periodontal disease. Pulpal disease can contribute to theinitiation or progression of periodontal disease by communi-cation through lateraΙ οanals, dentinal tubules, the apicalforamen, tooth οraοks or fractures, and periodontal diseasemay contribute to pulpal disease through the same pathways.
107
-

Ξ
PERloDoNτAL EMERGΕNclEs
How Are Endodontic-Periodontal ProblemsTreated?
ln an emergency situation, it is important to address theproblem that is causing pain and/or swelling for the patient. lna chronic situation, if the determination has been made thatthe lesion is primarily of pulpal origin but there is some perio-
dontal involvement, the pulp is treated first and then theperiodontal condition is re-evaluated 2-3 months after thecompletion of endodontic therapy. At that tame, any residualperiodontal defect may be treated. ln the presence of both achronic endodontic and periodontal lesion, both lesions mustbe treated in order to achieve comριete healing.
'
l
108

CHAPτER 11
CHAPTER 11: CONSIDERATIONS lN IMPLANT DENTISTRYThe placement and restoration of endosseous dentalimplants has become a predictable part of dental treatment.While many patients have had missing teeth, or even anentire dentition restored with implant supported dentistry,implant dentistry is not a panacea. lt is important toremember that most implant patients are dental failures andthat the clinician should identify the causes of the patient'stooth loss. ιf a patient lost teeth due to periodontal disease, it
is probable that there will be plaque-induced peri-implantdisease if the etiology cannot be οontrolled. lmplantsupported prosthesΘs may also be jeopardized by inappro-priate occΙusa| forces that are directed onto the restorationsor the implants themselves. Proper maintenance is as impor-tant as the proper placement and restoration of implants.
What Are the Biomechanics of Modern lmplants?Although there are many varieties of implants available, mostimplants are either threaded Screνv or press-fit endosseousroot-form implants (Figure 1). lmplants are made of titaniumor titanium alloy with a highly polished collar at the top orcoronal end of the implant fixture. The surface of the implanthas been roughened to increase the surface area of contactbet\iveen the implant and the bone. The implant surfaοe maybe blasted or coated with a titanium plasma spray or hydroxy-apatite.
F|GUΒΕ 1. Root-form endosseous implants usually have a threaded screwdesign (left) or a ρress-fit design (right). τhe implant is placed in aprepared osteotomy site of a slightly smaller diameter that the diameter ofthe implant.
The coronal aspect of all implants has a highly polished collartrom 1-4 mm wide. This collar may be kept relatively plaque-free with the appropriate home care devices and titanium-friendly instruments. lmplants should never be cleaned withmetaltipped ultrasonic deviοes.
There is a permucosal attachment of the gingiva to the coΙlarof the implant. Histologically, the gingiva attaches to theimplant collar by a hemidesmosomal attachment from thejunctional epithe|ium celΙs. This is the only soft tissue attach-ment that protects the underlying bone. Connective tissuefibers cannot insert into the body of the implant. As such, thissoft tissue attachment is more fragile and may be moresusοeptible to trauma' once this attachment is compromised,the bone-implant interface may be reached. Connectivetissue fibers adjacent to the implant suface are orientedparallel to the implant surface.
Current thinking suggests that there should be a band ofattached gingiva surrounding the implant collar. This densertissue can better protect the fragile permucosal epithelial
attachment than thinner alveolar mucosa can. lt is preferablethat this keratinized tissue be present either before implantplacement or uncovering.
What Are the Clinical and Radiographic Signs ofa HΘalthy and AiIing or FaiIing lmplant?
Muοh as \r/ith a tooth with a healthy periodontium, a healthyimplant will be surrounded by gingiva that is firm and pinkwith no evidence of erythema, edema, or suppuration. Radio-graphically, bone will approximate the implant surface fromthe area of the most coronal thread to the apex of the implantfixture (Figures 2A and B). The implant will be nonmoveablewhen gently pushed upon with tvvo instruments.
F|GURE 2A. τhese radiographs show the appearance of impΙants in healthybone. τhreaded Screw type implant.
FIGURΕ 28. These radiographs show the appearance of implants in healthybone. Press-fit type implant, Note the dense bone extending to thecoronal aspect of each implant.
-

coΝslDERAτloNs lΝ lMPLANT DENτ|SτRY
lmplants may be jeopardized from two directions. Plaque-induced inflammation caused by the same bacteria thatcause chronic periodontitis may be responsible for the initia-tion and progression of peri-implantitis. τhiS process beginsaround the implant collar. As long as the implant is still stable,this type of problem may be treated using surgicalapproaches similar to those used to treat periodontitis. A retro-grade implantitis may be caused by microfracture of bonesurrounding the implant due to an overload of occlusal forceson the implant. This problem may be manifest by a radiolu-cency at the apeΧ of the implant. This is an irreversibleprocess.
An ailing or failing implant may exhibit any number of signs ofinflammation. Ιncreased probing depth in the peri-impΙantsulcus, soft tissue erythema, or suppuration either from thesulcus or a draining fistula οan denote an ailing implantfixture. Bone loss will occur around the body of the implant.Any mobility of the fixture in the osseous housing is definedas a failing implant that must be removed. Radiographicsigns of an ailing implant include bone Ιoss at the collar, aninοrease in the number of threads no longer in bone, or aradiolucency at the apex of the implant (Figure 3A and B).
FlGURE 3Α. Radiographic and cιinical appearance of two ailing impιants. τhereare radiolucencies around the body of each of these implants.
FιGURE 3B. Badiographic and clinical appearance of two ailing implants. υponflap reflection, the extent of the bone destruction can be seen. τheseimplants were rescued using regenerative techniques similar to thoseused around natural teeth.
What ls the Protoοol for Implant Maintenance?
The sulcus around an implant must be examined with aplastic periodontal probe (Figure 4) as a metal probe maymar the implant surface. Gentle probing forοe must be usedin order not to completely penetrate the junctional epithelium.ln the presence of inflammation, the probe tip may approxi-mate the surface of the bone. Some authors suggest that animpΙant sulοus should not be probed unless there is someevidenοe of pathology. Unfortunately, inοreased probingdepth and bleeding upon gentle probing, the t\Λ/o mostobvious clinical signs of inflammation and destruction, cannotbe ascertained without probing.
F|GURE 4. τhis is an example of a plastic probe that may be used around animplant. Gentle probing force must be used to avoid complete penetrationof the permucosal seal.
The maintenance appointment for implant patients is in manyways similar to that for other dental patients with somenotable exceptions. only plastiο, graphite, or titanium instru-ments should be used on implant surfaces (Figure 5). Stan-dard stainless steel scalers and curettes will scratch theimplant surface. Although the metal tips of ultrasonic scaΙerswill damage the implant surface, the use of a sonic scaler\,νith plastic inserts is safe. An ultrasonic scaler may be usedon the surface of an ailing or failing implant during a surgicalrescue procedure in order to help detoxify the implantsurface.
FiGURE 5. τhese instruments are examples of plastic curettes that should beused when cleaning ιhe implant collars. steel-tipped instruments shouldnever be used for implant cleaning.

CHAPTER 11
Several protocols have been developed for the implant main-tenance appointment. All protocols have essentially the samecomponents.
Clinical and Radiographic Examination
Remove superstructure (if possible): Removal of ascrew-retained prosthesis will facilitate cleaning.Removal of the restoration will also allow the clinicianto differentiate between a loose restoration and aloose implant.
EvaΙuate tissue for tone, coΙor, consistency, size, andtexture.
Check for mobility: Α mobile implant is a failedimplant.
Probe implant sulcus depth: This should be done witha plastic periodontal probe and gentle force.
Evaluate plaque for quantity and location.
Evaluate calculus for quantity and location.
Radiograph implant area: There may be bone loss tothe first thread during the first year. Αfter this, boneloss shouΙd be negligible from year to year.
Record cliniοal and radiographic findings.
lmplant Maintenance Treatment Procedures
. Home care instructions emphasizing missed plaque:Have the ρatient demonstrate these new procedures.Behavioral modification may be necessary if thepatient is reverting to poor habits that caused toothloss in the first place. Powered toothbrushes maybe more effective than manual brushes in workingaround implants (Figure 6). An end-tufted brush mayalso be used for hard to reach areas (Figure 7).
FIGURE 6. Powered toothbrushes may be used for effective home care aroundimplants. τhere are many designs of powered brushes avai|able. lt isimportant to ensure that the head of the brush can contact the implantsurfaεe'
:ri::::,],:r:::t,t.. ..:.. t:.., : :::..:!::.: :: _:a]] .::'--a 1 :,.τjl:a'ι:a a||.1...a :.
FIGURE 7. An end-tuft brush can be used to clean hard-to-reach areas forimplant and superstruoture maintenance.
Specially designed floss provides effective yet safe plaqueremoval from implant surfaces (Figure 8). lnterproximalbrushes with nylon coated wires, soft foam inserts, orbrushes without a wire core οan also be used (Figure 9).Chlorhexidine gluconate may be used adjunctively toοontroΙ plaque.
FlGURE 8. γιride-diameter floss is an important component of implant mainte-nance.
FIGURE 9. lnterproximal devices may be used to remove plaque and to deliverantimicrobial agents to the interproximaι sufaces of implants duringhome care procedures.
-

coNs|DERAτtoNs lN |MPLANτ DENTISτRY
. Remove supra- and subgingival plaque from the ο Clean any remaining natural teethimplant surface: Plastic, graphite or titanium curettes ^--:__ ^_i ^^^^i+λ,i+ι, ^^A..^lmay be used. ' caries and sensitivity control
ο Remove supragingival plaque and stain: Use a ' Establish recaΙl interval
rubber οup and fine paste. Beware of heat buildup'as Proper maintenance is the key to implant surviνal. While thethe titanium implant will conduct heat to the inte- prinlipμs ire the same as with natural teeth, care must be ;
grated osseous surface' taken to use instruments that are both effective and safe for
. Clean superstructure the implant surface'
112

;
APPENDIX TABLΕ oF coNτENTS
Medical Considerations in the Periodontal Patient " 114
Calcium Channel Blockers and Gingival Hyperplasia . '. . . .. " 115
Dental Drug lnteractions: Update on Drug Combinations Requiring Special Considerations ........... 116
occupational Exposure to Bιoodborne Pathogens (Universal Precautions). . . . ' 121
Predominant Cultivable Microorganisms of the Oral Cavity ' " 124
Reference Values for Adults '. " " 125
DentifriceProducts " "128
Oral Rinse Products. ... " " 133
PrescriptionWriting " '134
Abbreviations Commonly Used in Medical Orders .. ' '.. " ' 1U
SafeWritingPractices. .......'.136
lnsurance Coding for the Periodontal Patient
r Selected Readings - General. "' " " 141
SelectedReadings-Specific. " " ""142
:
1

Ξ
AΡPEΝDlx
MEDICAL CONSIDERATIONS IN THE PERIODONTAL PATIENT
American Society of Anesthesiologists (ASA)Physical Status Classification System
The Αmerican Society of Anesthesiologists has developed apatient classification system to categorize surgery patientsbased on their medical condition. General precautions arepresented based on these medical findings.
ASA Class l: Class I patients are normal, healthynonsmokers who are not under the care of a physicianand do not take prescribed medications. Medical consul-tations are not required before surgery and there is noneed to modify the surgical plan because of medicalconcerns.
ASA Class ll: Class ll patients have mild systemicdΙsease, are Class l patients νvith some dental anxiety'and are generally older than Class I patients. Controlledsystemic diseases include diabetes, seizure disorders, orhypertension. Pregnant patients are also categorized asClass ll. Such patients have medical conditions thateither require alterations in patient management duringsurgery (eg, SBE antibiotic prophylaxis is necessary), orthey may have lifestyle conditions that potentially couldaffect the outcome of periodontaΙ surgery (eg' smoking,stress, or alcohol consumption). A consultation with thepatient's physician is recommended with Class llpatients.
ASA Class lll: Class lll patients require a medicalconsultation and recommendations from a physicianbefore any periodontal surgery. Patients in this categoryhave serious, potentially life-threatening medical condi-tions (eg, poorly controlled diabetes, epilepsy, hyperten-sion, ischemic heart disease, or a recent myocardialinfarction). Their physiοal activity is limited, but patientsare not completely incapacitated. Elective surgical proce-dures may not be in the best interest of these patients.Commonly, health considerations in Class lll patientsrequire that the procedure be modified (eg, shorter dura-tion, no vasoconstrictors in the local anesthetic, or stressmanagement).
ASA Class lV: Class lV patients have major, life-threat-ening health conditions (eg, severe cardiovasculardisease, uncontrolled diabetes or hypertension, unstableangina pectoris, or unstable seizure disorders). Theirphysical activity is extremely limited. Any elective perio-dontal surgery is contraindicated and emergency surgeryshould only be performed in a hospital environmentwhere medical life support systems are readily available.
ASA Class V: Class V patients are moribund and are notsurgical candidates. These patients are hospitalized andusually in the end-stages of disease. Any periodontalprocedures rendered to Class V patients should belimited to procedures to οontrol infection and relieve pain.

CALCIUM CHANNEL BLOCKERS AND GINGIVAL HYPERPLASIA
Druq FDA Aooroval Cases Cited in LiteiatureAmlodioine (NorvascΘ) 1 992 3BeDridil (Vascοr@) 1 993 0
Diltiazem (cardizemΘ, DiιacorΦ) 1 982 >20
Felodioine (PlendilΘ) 1 992lsradioine (DvnacircΦ) 1 991
Nicardiοine (cardene@) 1989 0Nifedioine (Adalat@. ProcardiaΘ) 1942 >120
Nimodipine (NιmotopΘ) r989 0
Nisoldipine (Sulaρ) I 99s ο
l.linincl fBavnress@\ 1
VeraoamΙl (calan@. lSootinΘ, verelan@) 1 982 7lNot yet approved for use in the United States.
SOME GENERAL OBSERVATIONS OF CCB-INDUCED GH
Calcium channel blockers (CCBs) are νveΙl known to cause control subjects Were inοluded. lt νvas found that 6.3% ofgingival enlargement. ln the early 199Os, it was thought that subjects taking nifedipine \Λ/ere seen to have significant over-
tniJctass of drugs caused a true hyperplasia of the gingiva. gro\Mth, which was significantly greater than the overgrowth
Current thinking is that the term "hyperplasia" is inappropriate seen with the other two drug groups or the control group. The
since the drug-induced effect results in an increase in extra- prevalence of gingival overgrou/th induced by amlodipine or
cellular tissue volume rather than an increase in the number diltiazem νvas not significantly different compared to the
of οells.l Most of the reported cases of CCB-induced gingival c9n]19] sΨue Τhis study concluded that the prevalence of
enlargement have involved patients >50 years of age"taiing significant gingival overgrowth related to CCBs was low'
ccBs for postmyocardiat infarction syndrome, "ngin"
;rir, l'jil iil".t were 3 times as likelv as females to develop
essential hypertension, and Raynaud's syndrome. iiii"αipi"J significant overgro\Λ/th'
(Procardia@) is associated with the highest "'TP9Ι :] ln a second study by Jorgensen,g a large group of patients
reported cases in the literature, followed by diltiazem irκinδirloαipinqwasstrδiedinordertodeterminetheprev-(Cardizemo).2 Depending on the CCB in question, gingival ,δnJ" ot, what he called, ,,gingival hyperplasia,,. out oi lsoenlargement has appeared any time betνveen 1-24 months dentate patients who volunteered to undergo a screeningafter daily dosing. Discontinuance of the CCB usually results examinaiion, mild hyperplasia was found in 5 patients (9.3%).in compιete disappearance or marked regression of symp- This was significantiy less than rates reported for patientstoms, with symptoms reappearing upon remedication. The taking nifedipine and not significantly different from ratestime required after drug discontinuance for marked regres- reported in control groups of cardiac patients not takingsion of enlargement has been 1 week. Complete disappear- CCBs. Jorgensen concluded that amlodipine, at a dose of 5ance of all symptoms usually takes 2 months. lf gingivectomy mg daily, did not induce gingival hyperplasia.is peι{ormed and the drug retained or resumed, the gingivalenlargement can recur. Only when the CCB is discontinued There have been reports of verapamil-induced gingival
or a switch to a non-CCB occurs, will the gingivectomy enlargement in the literature with at least 7 cases listed in the
usually be successful. one study of Nishikawa "t
ai. snoreδ review by this author.2 The prevaΙence of verapamil-induced
that if nifedipine could not be discontinued, gingivaΙ enlarge- enlargement, however' has not been investigated.
ment did not recur after gingivectomy when extensive plaquecontrol \ivas carried out. lf the CCB is changed to anotherclass of cardiovascular drug, the enlargement will probably Footnotesregress and disappear. A switch to another CCB, however,will probably result in οontinued gingival enlargement. For 1. Desai P and Silver J_G, "Drug-lnduοed Gingival Enlargements," J can Dent ASSΦ,
example, Giustiniani et al,a reportei disappearance of symp- 199Θ' 64(4):263-8'
toms within 15 days after discontinuance of verapamil, with 2. !νynn FlL, "Update on calcium channel Blocker-lnduced Gingival Ηyperplasia,''
recurrence of symptoms after resumption with diltiazem. One Gen Dent' 1995' 43(3\:218'20' 222'
case report described a nonsurgical management of a patient 3. Nishikawa s, Τada H, Hamasaki A, et al, ,.Nifedipine-lnduced Gingival Hypetrpresenting with nifedipine-induced gingival overgrowth.' plasia: Α clinical and ιn Vitro sιυdy,'' J Periodonfol, 1991, 62(1):30-5.
Establishment and maintenance of a considerably improvedstandard of plaque control led to οomplete resolution of the ' u'BτHilbfiλ::,l"iι"J',l.i?,''''?'f,"!b!;il'o,ξ'Τ,'!?,$,'r;?Ιt'Φ'"'ic Gingivitis
overgro\ivth without recurrence, even though the medicationdosgwas inοreased. The reader is referred to the review of 5 οianttr
lJ,;"i+i""',:i,!,:;';3χ:i'ir:i::l'rxr};{.iow1h:.Remission Following
1 99 t6 for descriptive clinical and histological f indings of CCB-induced gingival enlargement. Α more recent review has 6.\Λ/ynn.RL,'calciumchannel BlockersandGingival Hyperplasia,''GenDent,1991,
been author2ed by Silverstein et al, and published in 1997.7 3e(4):240-3'
τνvo reports described the prevalence of amlodipine(Norvasc@)-induced gingival overgro\Λ/th. The study by EΙlis etal,8 examined a sample of patients taking 1 of 3 CCBs whowere drawn from a community-based population in north-eastern England. out of 911 patients, 442ν'tere taking nifedi-pine, 181 amlodipine, and 186 diltiazem. ln addition, 102
7. Silverstein LH, Garnick JJ, Szikman M, et al, "Medication-lnduced GingivalEnlargement: A Clinical Review," Gen Dent, 1997, 45(4):371 -6.
8. Ellis Js, Seymour RA, Steele JG, et al, "Prevalenοe oΙ Gingival overgroMhlnduced by Calcium Channel Blockers: A Community-Based Study," J Periodontol, 1999, 70(1):63-7.
9. Jorgensen MG, "Prevalence of Amlodipine-Related Gingival Hyperplasia, J Perιodontol, 1997, 68(7):676-8.
Ξ

APPENDIX
DENTAL DRUG INTERACTIONS: UPDATE ON DRUG COMBINATIONSREQUIRING SPECTAL CONSIDERATIONS
This update disοussion includes 16 drug interaction mono-graphs describing clinically important drug combinationsrequiring special considerations in dental praοtice. Theactions which have resulted from these combinations rangefrom life-threatening adverse effects to attenuation of thetherapeutic effects of the interacting drug. The monographsare organized acοording to the four major groups of drugsused in dentistry: Antibiotics, nonsteroidal anti-inflammatorydrugs (including aspirin), epinephrine (vasoconstrictors), andnarcotic analgesics. Αn additional monograph on Valiumoand alcohol is included.
ANτIBloTlcs _ oRAL coNTRAcEPTIvEs
Description of the lnteraction
Case reports suggest that antibiotics used in dentistry canreduce the effectiveness of oral contraceptives resulting inbreakthrough ovulation and unplanned pregnancies.
Mechanism
Εstrogens, which are components of oral contraceptives, areactivated in the intestine by bacteria and reabsorbed into theblood stream as active compounds to inhibit ovulation. Αntibi-otics reduce the bacteria population in the intestine, whichmay result in less activated estrogen available to inhibitovulation.
Background Reports
Tetracyclines: one report described a \Λ/oman on anestrogen-type oral contraceptive who became pregnant aftera S-day course of tetracycline.1 Αlso, several cases of unin-tended pregnancy and menstrual irregularities have beenreported following concurrent use of tetracyclines and oralcontraceptives.2'3
Penicillins: Ampicillin has been shoνvn to reduce estrogenlevels in νvomen not taking oral contraceptives and there arereports of unplanned pregnancies in women taking ampicillinwith oral contraceptives.a's Concomitant use of penicillin withestrogen-containing oral οontraceptives decreased the effi-cacy of the contraceptive and increased the incidence ofbreakthrough bleeding.6,7 Since amoxicillin is closely relatedto other penicillins, it may also interact with oral contracep-tives.
Cephalosporins: Cephalexin (Keflexo) has been reported tointeract with oral contraceptives resulting in an unplannedpregnancy.s
Erythromycins: Unlike ampicillin and tetracyclines, erythro-mycins have been implicated in only a few cases of oralcontraceptive failure over the last 15 years and it is question-able whether erythromycin was the cause of those reportedfailures.
Management
lf antibiotics are prescribed to oral contraceptive users, it issuggested that the patients be advised to use additionalmethods of birth control during both 7- to 1O-day dosing, andthe two-dose prophylaxis regimens. Any additional method ofbirth control should be continued through the remaining oralcontraceptive cycle.
1. Bacon JF and Shenfield GM, "Pregnancy Αttributable to lnteraction BetweenTetracycline and oral contraceptiνes,'' Br Med J,1980' 280(6210):293.
2- orme ML, 'τhe cliniοal Pharmacology of oral contraceptive stθroids," Br Jcιin PharmacoΙ, 1982' 14'.31.
3. Back DJ, Grimmer SF, orme ML, et aι, "Evaluation of οommittee on safety ofMedicines Yellow card Reρorts on oral contraceptive-Drug lnteraοtions\,νith Αnticonvulsants and Antibiotics,'' Br J clin Pharmacol' 1988'25(5):527-32.
4. Trybuchowski H, "Effect ot Αmpicillin on the Urinary output of steroidalHormones in Pregnant and Nonpregnant ννomen,'' clin chim Acta, 1973'45:9-18.
5. Αldercreutz H, Martin F, Lehtinen τ, et al, "Effect of Amρicillin Administration onPlasma conjugated and Unconjugated Εstrogen and ProgesteroneLevels in Pregnancy,'' Am J obstet Gynecoι,1977,128(3\|266'71.
6. Proudfit c\Λ/, "concurrent oraI contraceptive and Antibiotic τherapy''' JAMA'1981, 246t2076.
7. True RJ, "lnteractions Between Antibiotics and oral contraceptives," J/MΑ,1982, 247(1O)t14Oa.
8. Bainton R, "lnteraction Between Antibiotic τherapy and contraceρtive Medica-lion,'' olal Surg oraι Med oraΙ Pathol, 1986, 61(5):453-5.
TETRACYCLINES - ANTACIDS (ContainingDivalent or τrivaIent Ions)
Description of the lnteraction
Concomitant therapy with a tetracycline and an antacidcontaining aluminum, calcium, or magnesium can reduceSerum concentration and the efficacy of the tetraοycline.
Mechanism
Aluminum, calcium, and magnesium ions can combine withthe tetracycline molecule in the gastrointestinal tract to form alarger ionized molecule unable to be absorbed into the bloodstream.
Background
τhe interaction between tetracyclines and antacidscontaining aluminum, calcium, and magnesium is well docu-mented. Foods and dairy products containing calcium \Λ/ill
also impair the absorption of tetracyclines. Some reportssuggest that doxycycline and minocycline are minimallyaffected by antacids and dairy products.l'2
Management
Tetracyclines should be given as far apart as possible fromantacids and dairy products.1. \Λ/elling PG, Koch PΑ, Lau cc' et al, "Bioavailability of Tetracycline and Doxy-
cycline in Fasted and NonΙasted subjects,'' Antimicrob AgentschΘmothe r, 1 97 7' 1 1 (3):462-9.
2. 'Anti-lnfective Drug lnteractions," Drug ιnteractions and υpdates, Hansten PDand Horn JR, eds, Malvern, PA: Lea and Febiger.
TETRACYCLINE - PENICILLIN
Description of the lnteraction
Simultaneous tetracycline-penicillin therapy may impair theefficacy of penicillin.
Mechanism
Penicillin kills bacteria by inhibiting cell wall synthesis. Tetra-cycline inhibits protein synthesis in bacteria and this actionhas been sho\Λ/n to antagonize the cell \ΙvaΙl inhibiting theeffect of penicillin.
Background
Most of the manufacturers' product information containswarnings against using tetracyclines and penicillins together.
116
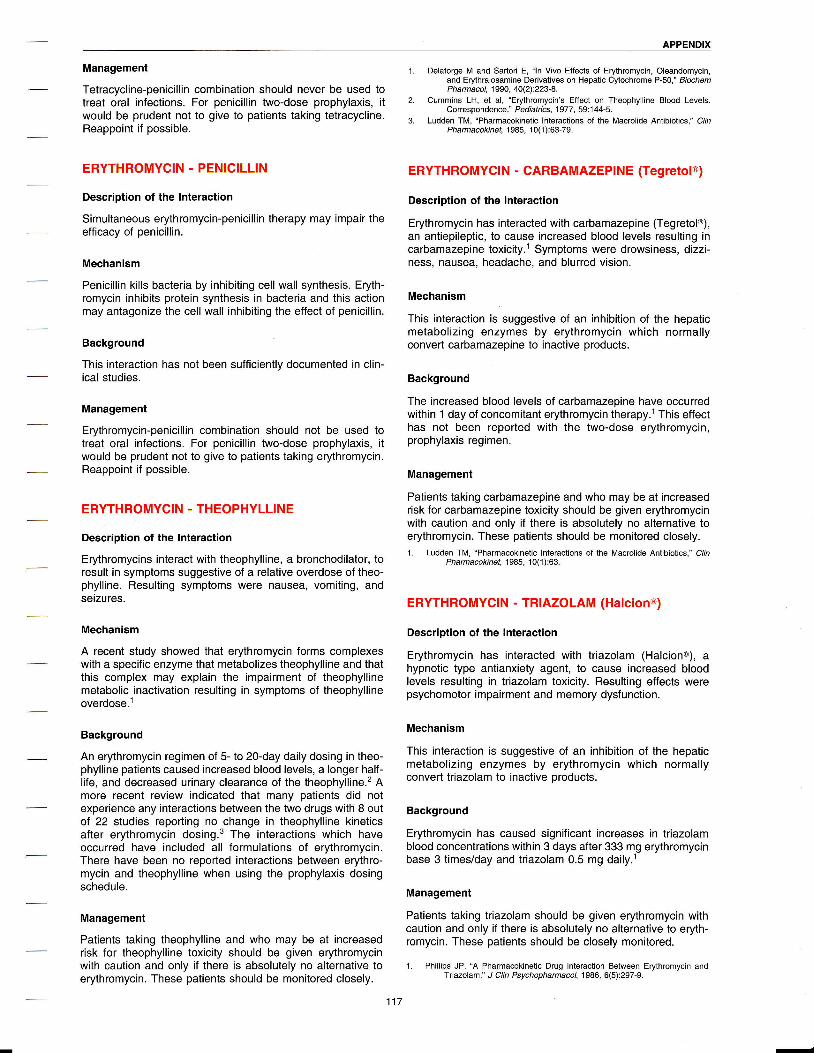
APPENDIX
Management
Tetracycline-penicilΙin combination should never be used totreat oral infections. For penicillin t\η/o-dose prophylaxis' itwould be prudent not to give to patients taking tetracycline.Reappoint if possibΙe.
ΕRYTHRoMYCIN - PENIcILLIN
Description of the lnteraction
Simultaneous erythromycin-penicillin therapy may impair theefficacy of penicillin.
Mechanism
Penicillin kills bacteria by inhibiting cell wall synthesis. Eryth-romycin inhibits protein synthesis in bacteria and this actionmay antagonize the cell wall inhibiting the effect of penicillin.
Background
τhis interaction has not been sufficiently documented in clin-ical studies.
Management
Erythromycin-penicillin combination should not be used totreat oral infeοtions. For penicillin two-dose prophylaxis, it
would be prudent not to give to patients taking erythromycin.Reappoint if possible.
ERYτHRoMYCIN - τHEoPΗYLL|NE
Description of the lnteraction
Erythromycins interact ιΛ/ith theophylline' a bronchodilator, toresult in symptoms suggestive of a relative overdose of theo-phylline. Resulting symptoms \ivere nausea, vomiting, andseizures.
Mechanism
A recent study showed that erythromycin forms οomplexeswith a specific enzyme that metabolizes theophylline and thatthis complex may explain the impairment of theophylΙinemetabolic inactivation resulting in symptoms of theophyllineoverdose.l
Background
An erythromycin regimen of 5- to 20-day daily dosing in theo-phylline patients caused increased blood leveΙs, a longer half-life, and decreased urinary clearance of the theophylline.2 Amore reοent review indicated that many patients did notexperience any interactions betνveen the t\Λ/o drugs with 8 outof 22 studies reporting no change in theophylΙine kineticsafter erythromycin dosing.3 The interactions which haveoccurred have included all formulations of erythromycin.There have been no reported interactions between erythro-mycin and theophylline when using the prophylaxis dosingschedule.
Management
Patients taking theophylline and who may be at increasedrisk for theophylline toxicity should be given erythromycinνvith caution and on|y if there is absolutely no alternative toerythromycin. τhese patients should be monitored closely.
1. Delaforge M and Sartori Ε, "ln Vivo Effects oΙ Erythromycin, oleandomycin,and EΦhralosamine Deriνatives on Hepatic ομochrome P-50,'' BiochemPhamacol, 1990, 40(2):223-8.
cummins LH, et al, "ΕMhromycin's Effect on τheophylIine Bιood Levels.Correspondence," Pediatrics, 1977, 59i1 44-5.
Ludden TM, "Pharmacokinetic lnteractions of the Macrolide Antibiotics," C/nPharmacokιnet' 1 985' 10(1 ):63-79.
ERYTΗROMYOIN - OARBAMAZEPINE (TegretoIo)
Description of the lnteraction
Erythromycin has interacted with carbamazepine (Tegretolo),an antiepileptic, to cause increased blood Ιevels resulting incarbamazepine toxicity.l Symptoms were drowsiness, dizzi-ness, nausea, headache, and blurred vision.
Mechanism
Τhis interaction is suggestive of an inhibition of the hepaticmetaboΙizing enzymes by erythromycin which normallyconvert carbamazepine to inactive products.
Background
The increased blood levels of carbamazepine have occurredwithin 1 day of concomitant erythromycin therapy.l This effecthas not been reported with the t\Λ,o-dose erythromycin,prophylaxis regimen.
Management
Patients taking carbamazepine and who may be at increasedrisk for carbamazepine toxicity should be given erythromycinwith caution and only if there is absolutely no alternative toerythromycin. These patients should be monitored closely.1. Ludden TM, "Pharmacokinetic lnteractions oΙ the Macrolide Antibiotics," c/ln
Phamacokinet, 1985, 10(1):63.
ERYTHROMYOIN - TRIAZOLAM (Ηalciono)
Description of the lnteraοtion
Erythromycin has interacted with triazolam (Halciono), ahypnotic type antianxiety agent, to cause increased bloodlevels resulting in triazolam toxicity. Resulting effects werepsychomotor impairment and memory dysfunction.
Mechanism
This interaction is suggestive of an inhibition of the hepaticmetabolizing enzymes by erythromycin which normallyconvert triazolam to inactive products.
Background
Erythromycin has caused significant increases in triazolamblood concentrations within 3 days after 333 mg erythromycinbase 3 times/day and triazolam 0.5 mg daily.l
Management
Patients taking triazolam should be given erythromycin withcaution and only if there is absolutely no alternative to eryth-romycin. These patients should be closely monitored.
1. Philιips JP, 'Α Pharmacokinetic Drug lnteraction Between Erythromycin andτriazolam," J cιin Psychopharmacol, 1986, 6(5):297-9-
2.
117
Ξ

APPEΝDlx
IBUPROFEN (Motrino, Advil@, Nuprino) - ORALANτIOOAGULANTS (Coumarins)
Description of the lnteraction
Bleeding may ocοur when ibuprofen is administered topatients taking coumarin-type anticoaguΙants.
Mechanism
lnhibition of prostaglandins by ibuprofen results in decreasedplatelet aggregation and interference with blood clotting,resuΙting in an enhancement of the anticoagulant effect ofcoumarins.
Background
Product information on ibuprofen in the 1995 edition of thePhysicians' Desk Reference (PDR) states that Motrinoinhibits platelet aggregation, but the effeοt is quantitativelyless and of shorter duration than aspirin. lt goes on to statethat bleeding has been reported when Motrino \Λ/as adminis-tered to patients on coumarin-type anticoagulants and theclinician should use caution in these circumstances. Addi-tional product information on naproxen, diflunisal, and flurbi-profen is listed in the same edition of the PDR. lt advisescaution when using naproxen with coumarins since interac-tions have been seen with other NSAIDS of this class; itstates that diflunisal, when given with warfarin, resulted inprolongation of prothrombin time; and it states that seriousclinical bleeding has been reported in patients taking flurbi-profen together \Λ/ith coumarins. Product information forwarfarin (Coumadino) in the 1995 PDR states that ibuprofen,naproxen, and diflunisal may be responsible for increasedprothrombin time response of the ιλ,arfarin. Flurbiprofen wasnot mentioned.
Management
It is suggested that ibuprofen (Motrino, Advilo, Nuprino) andother dental NSAIDS such as naproxen (Naprosyno),naproxen sodium (Anaproxo, Aleveo), diflunisal (Dolobido),flurbiprofen (ANSAιDΘ), and ketorolac (Τoradolo oral), beused νvith caution (if at all) in patients taking coumarin-typeanticoagulants. Use of other analgesics is preferred.
IBUPROFEN (Motrino, Advi]@, Nuprino) - LlτHIUM
Description of the ]nteΙaction
Concurrent administration of ibuprofen with lithium producessymptoms of lithium toxicity including nausea, vomiting,slurred speech, and mental confusion.
Mechanism
Prostaglandins stimulate renal lithium tubular secretion.NSAIDS inhibit prostaglandin-induced renal secretion oflithium, which increases lithium plasma levels and producessymptoms of lithium toxicity.
Background
Lithium is used for the treatment of acute mania and toprevent recurrent episodes of bipolar (manic-depressive)
illness. The therapeutic lithium plasma concentration isextremely narrovv (0.8-1.2 mEq/L) and drugs that causelithium plasma levels to go outside this narrow therapeutiοrange will result in lithium toxicity. Of the four NSAIDS used indentistry (ibuprofen, naproxen, diflunisal, and flurbiprofen)the former t\ivo have been well documented to interact \ivith
lithium. ln 1980, Ragheb et al, reported that a patient taking2400 mg ibuprofen daily experienced nausea and drowsinesswhile stabilized on lithium.1 τhe lithium plasma leveΙincreased from 0.8-1.0 mEq/L. Subsequently, in a study of 11
healthy volunteers, Kristoff et al, observed that 400 mg ofibuprofen 4 times/day combined with 450 mg of lithiumοarbonate every '12 hours, increased lithium plasma levelswithin several days.2 Decreased ability to concentrate, light-headedness, and fatigue resulted from this interaction.
Ragheb reported that concomitant administration of lithiumand ibuprofen (1.8 g/day) in nine patients with bipolar- orschizoid-type disorders resulted in significant increases(average 34%) in lithium plasma concentrations as well asdecreases in lithium clearance.3 lndividual variations wereobserved, with increases in lithium levels ranging from 12/oto 66% within 6 days of concomitant administration ofibuprofen. ln this study, tremors occurred in three patients asa result of this interaction. Ragheb reported that patientsolder than 50 years νvere more susceptible to lithium toxicity.The 1993 edition of the Physician's Desk Reference (PDR)(in the monograph for Motrino) warns that concomitant use ofibuprofen and lithium citrate or carbonate may elevate lithiumplasma leveΙs and reduce renal lithium clearance.
ln a 1986 study by Ragheb and Powell, concomitant adminis-tration of naproxen and lithium resulted in individual varia-tions in plasma lithium Ιevels (from increases of 0% to 42"λ.aln that study, lithium renal clearance decreased in patientswho were taking daily doses of lithium (900 mg) andnaproxen (750 mg) for 6 days. The monograph for Naprosynoin the 1993 PDR cautions that conοomitant use of naproxenand lithium could increase lithium plasma concentrations.
lnteractions bet\Λ/een difIunisal (DoΙobido1 and lithium, andflurbiprofen (AnsaidΘ) and lithium have not been reported.Nor is any potential interaction between these tνvo NSAIDSand lithium mentioned in the PDR, lnterestingly, aspirin hasbeen shown to affect plasma lithium levels in healthysubjects.s Lack of documentation about diflunisal and flurbi-profen does not mean these agents are safe to use inconjunction with lithium. NSA|Ds should be used \Λ/ith cautionby dental patients who are taking lithium. Substitution ofNSAIDS with acetaminophen preparations may be warranted.
Management
Extreme caution is necessary in administering NSAIDS tolithium patients; use of analgesics other than NSAIDS ispreferred.
1. Ragheb M, Ban τA, Buchanan D, et ai, "lnteraction of lndomethacin andlbuprofen \Λ/ith Lithium in Manic Patients Under a Steady-State LithiumLeνel,'' J cιin Psychiatry, 1980, 41(1 1):397-8.
2_ Kristofi cA, Hayes PE, Barr \Λ/H, et al, "Effect of lbuprofen on Lithium Plasmaand Red Blood ceΙl concentrations,'' clin Pharm,1986' 5(1):51-5.
3. Ragheb M,'lbuρrofen can lncrease serum Lithium Level in Lithium-τreatedPatients," J C/n Psychiatry, 1 987, 48(4):161 -3.
4. Ragheb M and Powell AL' "Lithium lnteraction \Λ/ith sulindac and Naproxen,'' Jcιin Psychophamacol,'1986, 6(3):1 50-4.
5. Reimann l\Λ/, Diener U, and Frolich Jc, "lndomethacin But Not Αspirinlncreases Plasma Lithium lon Levels," Arch Gen Psychiatry, 1983,40(3):283-6.

APPENDIX
ASPIRIN - ORAL ANTICOAGULANTS (Coumarins)
Description of the lnteraction
Aspirin increases the risk of bleeding in patients taking oralanticoagulants.
Mechanism
Small doses of aspirin inhibit platelet function. Larger doses(>3 g/day) elicit a hypoprothrombinemic effect. Aspirin mayalso displace oral anticoagulants from plasma protein-bindingsites. These actions of aspirin alΙ contribute to increase therisk of bleeding in patients taking oral anticoagulants.
Background
There is much documentation in the literature confirming thisinteraction. One study using over 500 patients showed thatexοessive bleeding \,vas about 3 times more common withwarfarin (Coumadino) plus aspirin (500 mg/day) than withwarfarin alone.1 Αnother study showed enhanced hypopro-thrombinemia in warfarin patients during the first few days ofaspirin therapy (1 glday).2 There are other reports describingbleeding episodes due to concurrent therapy with aspirin andoral anticoagulants.3'a
Management
Patients receiving oral anticoagulants should avoid aspirinand aspirin-containing products.
1. chesebro JH, Fuster v, Elveback LR, et al, "Τrial of combined WarfarinTherapy Plus Dipyridamole or Aspirin τherapy in Prosthetic Heart ValveReplacement: Danger of Aspirin compared ννith Dipyridamole," Αm Jcardioι, 1 983' 51 (9):1 537-41.
2. Donaldson DR, Sreeharan N, crow MJ, et al, "Assessment of the lnteraοtion ofWarfarin \Λ/ith Αspirin and Dipyridamole," τhromb Haemost, 1982,47(1):77.
3. Starr KJ and Petrie JC, "Drug lnteractions in Patients on Long-Term OralΑnticoagulant and Antihypertensive Αdrenergic Neuron-Blocking Drugs,"Br Med J,1972, 4(833):133-5.
4. Udall JA, "Drug lnterference \Λ/ith Warfarin τherapy,'' cιin Med' 1970' 77:20.
ASPIRIN - PROBENECID (Benemido)
Description of the lnteraction
Aspirin inhibits the uricosuric action of probenecid.
Mechanism
Unknown
Background
The inhibition of probenecid-induced uricosuria by aspirin isdose-dependent. Doses of aspirin of 1 g or less do notappear to affect probenecid uricosuria. Larger doses,however, appear to considerably inhibit uricosuria.Conversely, probenecid appears to inhibit uricosuria followinglarge doses of aspirin. Aspirin does not interfere with theactions of probenecid to inhibit the renal elimination of peni-cillins.
Management
It appears prudent to use a nonsalicylate-type analgesic (ie,
acetaminophen or NSAID) in patients receiving probenecidas a uricosuriο agent (treatment of gouty arthritis).
EPlNEPHRINE (Vasoconstrictor) - τRIcYcLlcANτIDEPREssANTs
Description of the lnteraction
Use of epinephrine as a vasoconstrictor in local anestheticin.lections may cause a hypertensive interaction in patientstaking tricyclic antidepressants.
Mechanism
Τricyclic antidepressants cause increases of norepinephrinein synaptic areas in the centra! nervous system andperiphery. Epinephrine may add to the effects of norepineph-rine resulting in vasoconstriction and transient hypertension.
Background
There is adequate information in the literature to confirm ahypertensive interaοtion between epinephrine, norepineph-rine, and levonordefrin with TCΑs. An l'V' infusion ofepinephrine to healthy subjects reοeiving imipramine resultedin two- to fourfold increases in the pressor response toepinephrine.l,2 Also cardiac dysrhythmias M/ere reported.Αlthough these effeοts \Λ/ere seen with l.V. infusions, thesereports suggested that caution should certainly be exercisedif epinephrine is administered by other routes. l.V. infusionsof norepinephrine to healthy subjects receiving imipramineresulted in a four- to eightfold increase in the pressorresponse to norepinephrine,l'2 and a later study showed atwofold increase in pressor response to norepinephrine.3other tricyclics were associated \Λ/ith a threefold increase inpressor response to norepinephrine.4 This increased pressorresponse was probably due to tricyclic antidepressant-induced inhibition of norepinephrine reuptake. Similar effectshave been reported with levonordefrin.s
Management
The use of epinephrine in patients taking tricyclic type antide-pressants is potentially dangerous. Use minimum amounts ofvasoconstrictor νvith caution in patients on tricyclic antide-pressants.
1. Boakes AJ, Laurence DR, Teoh PC, et al, "lnteractions Between Sympathomi-metic Amines and Αntidepressant Agents in Μan,'' Br Med J' 1973'1 (849):31 1 -5.
2. Svedmyr N, "The lnfΙuenοe of a τricyclic Antidepressive Agent (Protriptyline) onSome of thΘ circulatory Effects of Noradrenaline and Αdrenaline in Man,"ιlfe sc,, 1968' 7(1):77-84.
3. Larochelle P, Hamθt P, and Enjalbert M, "Response to Tyramine and Norepi-nephrine Αfter lmipramine and τrazodone,'' cιin Pharmacoι τher,1979,26(1\:24-30.
4. Mitchell JR, cavanaugh JH, Arias L, et al, "Guanethidine and ReIated Αgents.lll. Antagonism by Drugs μ/hich lnhibit the Norepinephrine PUmp in Man,''J cιin ιnvest, 1970, 49(8):1596-604.
5. Jastak JT and Yagiela JΑ,'γasoconstrictors and Local Αnesthesia: Α Reviewand Rationale tor υSe,'' J Am Dent Assoc,1983, 107(4):623-30.
EPINEPHRINE (Vasoconstrictor) - MONOAMINEoxIDASE INHIB!τoRs
Description of the lnteraction
Use of epinephrine as a vasoconstriοtor in local anestheticinjections may cause a hypertensive interaction in patientstaking monoamine oxidase inhibitors.
Mechanism
Drugs which inhibit monoamine oxidase cause increases inthe concentration of endogenous norepinephrine, serotonin,and dopamine in storage sites throughout the central nervoussystem. Epinephrine may add to the effects of norepinephrineresulting in vasoconstriction and transient hypertension.
-
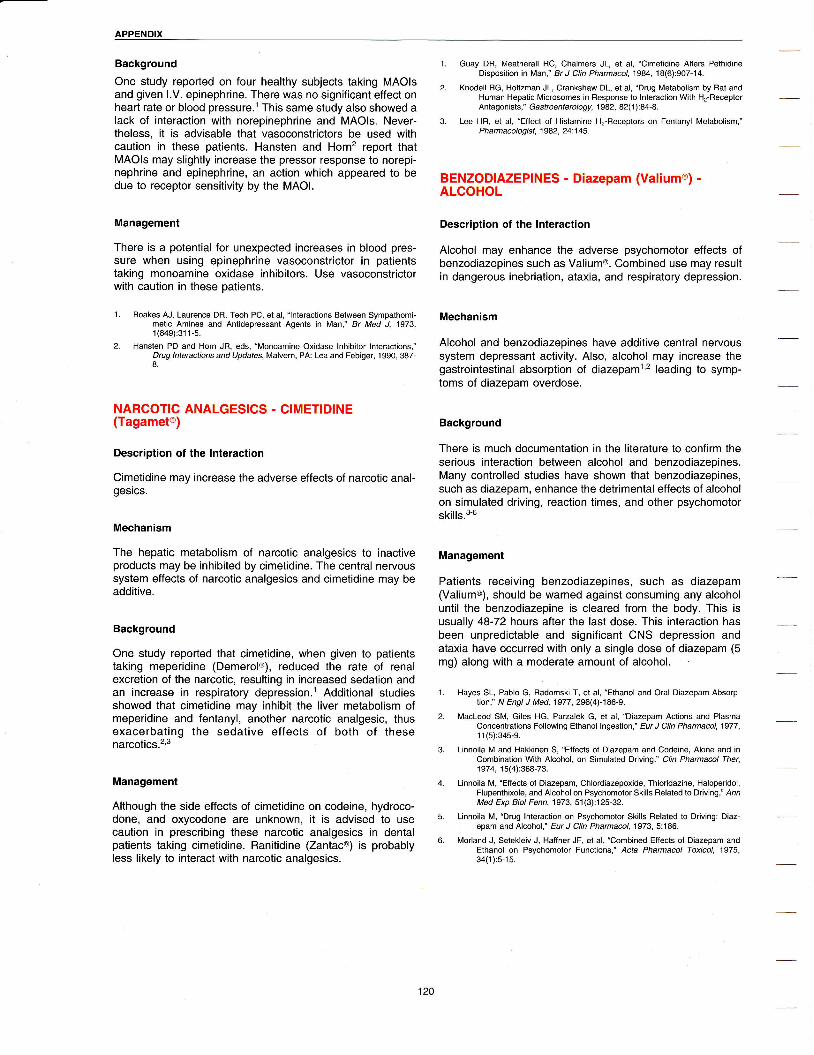
APPENDIX
Background
One study reported on four healthy subjects taking MAOIsand given l.V. epinephrine. There \Λ,as no significant effect onheart rate or blood pressure.1 τhis same Study also Sho\Λ/ed alack of interaction with norepinephrine and MAOls. Never-theless, it is advisable that vasoconstrictors be used withcaution in these patients. Hansten and Horn2 report thatMΑols may slightly increase the pressor response to norepi-nephrine and epinephrine, an action \Ιvhich appeared to bedue to receptor sensitivity by the MAOI.
Management
There is a potential for unexpected increases in blood pres-sure when using epinephrine vasoconstrictor in patientstaking monoamine oxidase inhibitors. Use vasoconstrictorwith caution in these patients.
1. Boakes ΑJ, Laurence DR, Teoh Pc, et al, "lnteraοtions Between symρathomi-metic Amines and Αntidepressant Agents in Μan,'' Br Med J, 1973'1 (849):31 1 -5.
2. Ηansten PD and Ηorn JFi, eds, "Monoamine oxidase lnhibitor lnteractions,"Drug lnteractions and υpdates, Malvern, PA: Lea and Febiger, 1 990, 387-8.
NARcoTIc ANALGEslcS - cIMETIDINΕ(Tagameto)
Description of the lnteraction
Cimetidine may increase the adverse effects of narcotic anal-gesics.
Mechanism
The hepatic metabolism of narcotic analgesics to inactiveproducts may be inhibited by cimetidine. The central nervoussystem effects of narcotic analgesics and cimetidine may beadditive.
Background
One study reported that cimetidine, when given to patientstaking meperidine (Demerol@), reduced the rate of renalexcretion of the narcotic, resulting in increased sedation andan increase in respiratory depression.l Additional studiessho\Λ,ed that cimetidine may inhibit the liver metabolism ofmeperidine and fentanyl, another narοotic analgesic, thusexacerbating the sedative effects of both of thesenarcotics.2'3
Management
Αlthough the side effects of cimetidine on codeine, hydroco-done, and oxycodone are unkno\Λ,n, it iS advised to usecaution in prescribing these narcotic analgesics in dentalpatients taking cimetidine. Ranitidine (Zantaco) is probablyless likely to interact with narcotic analgesics.
1. Guay DR, Meatherall Rο, chalmers JL, et al, "cimetidine Αlters PethidineDisposition in Μan,'' Br J clin Pharmacol, 1984, 18(6):907-14.
2. Knodell RG, Holtzman JL, Crankshaw DL, et al, "Drug Metabolism by Rat andHuman Hepatic Microsomes jn Responsθ to lnteraοtion \Λ/ith H2-ReοeptorAntagonists," Gastroenterology, 1982, 82(1):84-8.
3. Lee HR, et al, "Effect of Histamine H2-Fleceρtors on Fentanyl Metabolism,"P h arm acologist, 1982, 24:1 45 -
BΕNzoDlAzEPlNEs _ Diazepam (VaIiumo1 -ALCOHOL
Description of the lnteraction
Αlcohol may enhance the adverse psychomotor effects ofbenzodiazepines such as Valium@. Combined use may resultin dangerous inebriation, ataxia, and respiratory depression.
Mechanism
Αlcohol and benzodiazepines have additive central nervoussystem depressant activity. AΙso, alοohol may inοrease thegastrointestinal absorption of diazepaml,2 leading to symp-toms of diazepam overdose.
Background
There is much documentation in the literature to confirm theserious interaction bet\Λ/een alcohol and benzodiazepines.Many controlled studies have shown that benzodiazepines,suοh as diazepam, enhance the detrimental effects of alcoholon simulated driving, reaction times, and other psychomotorskills.3-6
Management
Patients receiving benzodiazepines, such as diazepam(ValiumΘ), should be warned against consuming any alcoholuntil the benzodiazepine is cleared from the body. This isusually 48-72 hours after the last dose. This interaction hasbeen unpredictable and significant CNS depression andataxia have occurred with only a single dose of diazepam (5mg) along with a moderate amount of alcohol.
1. Hayes SL, Pablo G, Radomski Τ, et al, "Εthanol and oral Diazepam Absorp-lion," N Εngι J Med,1977, 296(4)-186-9.
2. Macleod sM, Giles HG, Parzalek G, et al, "Diazeρam Actions and Plasmaconcenιrations Following Ethanol lngestion," Εur J cιin Phamacoι,1977,1 1 (5):345-9.
3. Linnoila M and Hakkinen s, "Effects of Diazepam and οodeine, Alone and incombination \Λ/ith Alcohol, on Simulated Driνing,'' clin Pharmacol τher,1974,15(4):368-73.
4. Linnoila M, "Εffects of Diuepam, chlordiαepoxide, Thioriduine, Haloperidol,Fluρenthixole, and Alcohol on Psychomotor SkillS Related to Driνing,'' AnnMed Εxp Bioι Fenn' 1973, 51(3):125-32.
5. Linnoila M, "Drug lnteraction on Psychomotor Skills Fielated to Driving: Diaz-epam and Alcohol,'' Εur J cιιn Pharmacoι,1973, 5:186.
6. Morland J, setekleiv J, Haffner JF, et al, "οombined Εffects of Diazepam andEthanol on Psychomotor Funοtions,'' Acta Pharmacoι τoxicoι, 1975'34(1 ):5-1 5.

APPENDIX
OCCUPATIONAL EXPOSURE TO BLOODBORNE PATHOGENS(uNrvERsAL PRECAUTIONS)
ovERvIEι'v AND REGULAτoRYCONSIDERATIONS
Every healthοare employee, from nurse to housekeeper, hassome (albeit small) risk of exposure to HIV and other viralagents such as hepatitis B and Jakob-Creutzfeldt agent. Theincidence of ΗlV-1 transmission associated \ivith a percuta-neous exposure to blood from an HIV-1 infected patient isapproximately o.3"λ per exposure.1 ln 1989, it was estimatedthat 12,000 United States healthcare workers acquired hepa-titis B annually.2 An understanding of the appropriate proce-dures, responsibilities, and risks inherent in the collectionand handling of patient specimens is necessary for safe prac-tice and is required by Occupational Safety and HealthAdministration (OSHA) regulations.
The occupational Safety and Health Αdministrationpublished its "Final Rule on Occupational Exposure to Blood-borne Pathogens" in the Federal Register on December 6,1991. OSHA has chosen to follow the Center for DiseaseControl (CDC) definition of universal precautions. The FinalRule provides full legal forοe to universal preοautions andrequires employers and employees to treat blood and certainbody fluids as if they were infectious. The Final Rulemandates that hea|thcare workers must avoid parenteraιcontact and must avoid splattering blood or other potentiallyinfectious material on their skin, hair, eyes, mouth, mucousmembranes, or on their personal οlothing. Hazard abatementstrategies must be used to protect the workers. Such planstypically include, but are not limited to, the following:
. safe handling of sharp items ("sharps") and disposal ofsuch into puncture-resistant containers
. gloves required for employees handling items soiled withblood or equipment contaminated by blood or other bodyfluids
o provisions of protective οlothing when more extensivecontact with blood or body fluids may be anticipated (eg,surgery, autopsy, or deliveries)
. resuscitation equipment to reduce necessity for mouth tomouth resuscitation
ο restriction of HlV- or hepatitis B-exposed employees tononinvasive procedures
oSHΑ has specifically defined the following terms: occupa-tional exposure means reasonably anticipated skin, eyemucous membrane, or parenteral contact with blood or otherpotentially infectious materials that may result from theperformance of an employee's duties. Other potentiallyinfectious materials are human body fluids includingsemen, vaginal seοretions, cerebrospinal fluid, synovial fluid'pleural fluid, pericardial fluid, peritoneal fluid, amniotic fluid,saliva in dental procedures, and body fluids that are visiblycontaminated with blood, and all body fluids in situationswhere it is difficult or impossible to differentiate between bodyfluids; any unfixed tissue or organ (other than intact skin)from a human (living or dead); and HIV-containing cell ortissue cultures, organ cultures, and HIV- or HBV-containingculture medium or other solutions, and blood, organs, orother tissues from experimental animals infected with HIV orΗBV. Αn exposure incident involves specific eye, mouth,other mucous membrane, nonintact skin, or parenteralcontact with blood or other potentially infectious materialsthat results from the performance of an employee's duties.3 ltis important to understand that some exposures may gounrecognized despite the strictest precautions.
A written Exposure Control Plan is required. Εmployers mustprovide copies of the plan to employees and to OSHA upon
request. CompΙiance with oSHΑ rules may be accomplishedby the following methods.
ο Universal precautions (UPs) means that all humanblood and certain body fluids are treated as if known tobe infectious for ΗlV, HBV, and other bloodborne patho-gens. UPs do not apply to feces, nasal secretions, saliva,sputum, s\iveat, tears, urine, or vomitus unless theycontain visible blood.
. Engineering controls (ECs) are physical devices whichreduce or remove hazards from the workplace by elimi-nating or minimizing hazards or by isolating the νvorkerfrom exposure. Engineering control deviοes includesharps disposal containers, self-resheathing syringes,etc.
o Work practice controls (ιlvPCs) are practices andprocedures that reduce the likelihood of exposure tohazards by altering the way in which a task is performed.Specific examples are the prohibition of two-handedrecapping of needles, prohibition of storing food along-side potentially contaminated material, discouragementof pipetting fluids by mouth, encouraging handwashingafter removal of gloves, safe handling of contaminatedsharps, and appropriate use of sharps containers.
. Personal protective equipment (PPE) is specializedclothing or equipment worn to provide protection fromoccupational exposure. PPE includes gloves, gowns,laboratory coats (the type and characteristics will dependupon the task and degree of exposure anticipated), faceshields or masks, and eye protection. Surgical caps orhoods and/or shoe covers or boots are required ininstances in which gross contamination can reasonablybe anticipated (eg, autopsies, orthopedic surgery). lf PPEis penetrated by blood or any contaminated material, theitem must be removed immediately or as soon asfeasible. The employer must provide and launder ordispose of all PPE at no cost to the employee. Glovesmust be worn when there is a reasonable anticipation ofhand contact with potentially infectious material, includinga patient's mucous membranes or nonintact skin. Dispos-able gloves must be changed as soon as possible afterthey become torn or punctured. Hands must be washedafter gloves are removed. OSHA has revised the PPEstandards, effective July 5, 1994, to include the require-ment that thΘ employer ceι1ify in writing that it hasconducted a hazard assessment of the workplace todetermine whether hazards are present that will necessi-tate the use of PPE. Also, verification that the employeehas received and understood the PPE training isrequired.a
Housekeeping protocols: oSΗΑ requires that alΙ bins,cans, and similar receptacles, intended for reuse which havea reasonabΙe likelihood for becoming contaminated, beinspected and decontaminated immediately or as soon asfeasible upon visible contamination and on a regularly sched-uled basis. Broken glass that may be contaminated must notbe picked up directly with the hands. Mechanical means (eg,brush, dust pan, tongs, or forceps) must be used. Brokenglass must be plaοed in a proper sharps container.
Employers are responsible for teaching appropriate clean-upprocedures for the work area and personal protective equip-ment. A 1:10 dilution of household bleach is a popular andeffective disinfectant. lt is prudent for employers to maintainsignatures or initials of employees who have been properlyeducated. lf one does not have written proof of education of
-

APPENDIX
occUPAτIoNAL ExPosURE τo BLooDBoRNE PAτHOGENS (UNIVERSAL PRECAUTIONS) (Continued)
universal precautions teaching, then by OSHA standards,such education never happened.
Pre-exposure and postexposure protocols: oSHΑ's FinalRule includes the provision that employees, who are exposedto contamination, be offered the hepatitis B vaccine at no costto the employee. Employees may decline; however, a decli-nation form must be signed.. τhe empΙoyee must be offeredfree vaccine if he/she changes his/her mind. Vaccination toprevent the transmission of hepatitis B in the healthοaresetting is widely regarded as sound practice.s ln the event ofexposure, a confidential medical evaluation and follow-upmust be offered at no cost to the employee. Follow-up mustinclude collection and testing of blood from the source indi-vidual for HBV and HlV if permitted by state Ιaw if a bloodsample is available. lf a postexposure specimen must bespecially drawn, the individual's consent is usually required.Some states may not require consent for testing of patientblood after accidental exposure. One must refer to state and/or local guidelines for proper guidance.
The employee follow-up must also include appropriatepostexposure prophylaxis, counseling, and evaluation ofreported illnesses. The employee has the right to declinebaseline blood collection and/or testing. lf the employee givesconsent for the collection but not the testing, the sample mustbe preserved for 90 days in the event that the employeechanges his/her mind \η/ithin that time. Confidentiality relatedto blood testing must be ensured. The employer does nothave the right to know the results of the testing of eitherthe source individual or the exposed employee.
MANAGEMENT OF OCCUPATIONAL EXPOSURETo Htv lΝ THE \,lvoRKPLAcE6.l . Likelihood of transmission of HIV-1 from occupational
exposure is O.2o/" per parenteral exposure (eg, needle-stick) to blood from HIV infected patients.
2. Factors that increase risk for occupationaΙ transmissioninclude advanced stages of ΗlV in source patient, hol|owbore needle puncture, a poor state of health,or inexperi-ence of the healthcare worker (HCW).
3. lmmediate actions an exposed healthcare worker shouldtake include aggressive first aid at the puncture site (eg,scrubbing site \λ/ith povidone-iodine solution for 10minutes) or at mucus membrane site (eg, saline irrigationof eye for 15 minutes). Then immediate reporting to thehospital's occupational medical service. The authors indi-cate that there is no direct evidence for the efficacy oftheir recommendations. Other institutions suggestrigorous scrubbing \ivith soap.
4. After first aid is initiated, the healthcare worker shouldreport exposure to a supervisor and to the institution'soccupational medical service for evaluation.
5. Occupational medicine should perform a thorough inves-tigation including identifying the HIV and hepatitis Bstatus of the source, type of exposure, volume of inoc-ulum, timing of exposure, extent of injury, appropriate-ness of first aid, as well as psyοhologicaΙ status of thehealthcare worker. ΗlV serologies should be performedon the healthcare worker. HIV risk counseling shouldbegin at this point.
6. All parenteral exposures should be treated equally untilthey can be evaluated by the occupational medicineservice, who wilΙ then determine the actual risk of expo-sure. Follow_up οounseling sessions may be necessary.
7. Although the data are not clear, antiviral prophylaxis maybe offered to healthcare workers who are parenterally ormucous membrane exposed. lf used, antiretroviral
prophylaxis should be initiated within 1-2 hours aftΘrexposure.
8. Counseling regarding risk of exposure, antiviral prophy-laxis, plans for follow-up, exposure prevention, sexualactivity, and providing emotional support and response toconcerns are necessary to support the exposed health-care worker. Follow-up should consist of periodic sero-logic evaluation and blood chemistries and counts ifantiretroviral prophylaxis is initiated. Additional informa-tion should be provided to healthcare workers who arepregnant or planning to become pregnant.
HAzARDoUs coMMUNIcAτloNCommuniοation regarding the dangers of bloodborne infec-tions through the use of labels, signs, information, andeducation is required. Storage locations (eg, refrigerators andfreezers, \Λ/aste containers) that are used to store, dispose of,transport, or ship blood or other potentially infectious mate-rials require labels. The label background must be red orbright orange with the biohazard design and the wordbiohazard in a contrasting color. The Ιabel must be part of thecontainer or affixed to the container by permanent means.
Eduοation provided by a qualified and knowledgeableinstructor is mandated. The sessions for employees mustinclude:
. accessible copies of the regulation
. general epidemiology of bloodborne diseasesο modes of bloodborne pathogen transmission. an explanation of the exposure control plan and a means
to obtain copies of the written plan. an explanation of the tasks and activities that may involve
exposure. the use of exposure prevention methods and their limita-
tions (eg, engineering controls, work practices, personalprotective equipment)
. information on the types, proper use, location, removal,handling, decontamination, and disposal of personalprotective equipment)
. an explanation of the basis for selection of personalproteοtive equipment
ο information on the HBV vaccine, including information onits effiοacy, safety, and method of administration and thebenefits of being vaccinated (ie, the employee mustunderstand that the vaccine and vaccination will beoffered free of charge)
. information on the appropriate actions to take andpersons to contaοt in an emergency involving exposure toblood or other potentially infectious materials
. an explanation of the procedure to follow if an exposureincident occurs, including the method of reporting theincident
. information on the postexposure evaΙuation and follow-upthat the employer is required to provide for the employeefollowing an exposure incident
. an explanation of the signs, labels, and color coding
. an interactive question-and-answer period
RECORD KEEPING
The OSHA Final Rule requires that the employer maintainboth education and medical records. The medical recordsmust be kept confidential and be maintained for the durationof employment plus 30 years. They must contain a copy ofthe employee's HBV vaccination status and postexposureincident information. Education records must be maintainedfor 3 years from the date the program was given.
APPEΝDlx
OSHA has the authority to conduct inspections ι/vithoutnotice. Penalties for cited violation may be assessed asfollows.
Serious violations. ln this situation, there is asubstantial probability of death or serious physicalharm, and the employer kneνv, or should have known,of the hazard. A violation of this type carries amandatory penalty of up to $7000 for each violation.
Other-than-serious violations. The violation is unlikelyto result in death or serious physical harm. Τhis type ofviolation carries a discretionary penalty of up to $7000 foreach violation.
Willful violations. These are violations committed know-ingly or intentionally by the employer and have penaltiesof up to $70,000 per violation with a minimum of $5000per violation. lf an employee dies as a result of a wiΙlfulviolation, the responsible party, if convicted, may receivea personal fine of up to $250,000 and/or a 6-month iailterm. Α corporation may be fined $500,000.
Large fines frequently follow visits to laboratories, physicians'offices, and healthcare facilities by OSHA Compliance Safetyand Health Offices (CSHOS). Regulations are vigorouslyenforced. Α working knowledge of the final rule and imple-mentation of appropriate policies and practices is imperativefor all those involved in the collection and analysis of medicalspecimens.
Effectiveness of universal precautions in averting exposure topotentially infectious materials has been documented.TCompliance with appropriate rules, procedures, and policies,including reporting exposure incidents, is a matter of personalprofessionalism and prudent self-preservation.
Footnotes
1. Henderson DK, Fahey BJ, Willy M, et al, "Risk Ιor occupational τransmission ofHuman lmmunodeficiency Virus Tyρe 1 (HlV-1) Associated \Λ/ith cliniοal Expo-sures. A Prospective ΕValuation," Ann ιntern Med' 1990' 113(10):740-6.
2. Niu MT and Margolis Ηs, "Moving lnto a New Era of Government Regulation:Provisions Ιor Heρatitis B Vaccine in the Workplace, cιin Lab Manage Rev,1 989, 3:336-40.
3. Bruning LM, τhe Bloodborne Pathogens Final Rule - Understanding the Regula-Ιion,'' AoRN Journaι' 1993' 57(2':439-40-
4. "Rules and Regulations," Federal Register,1994, 59(66):16360-3.
5. sοhaffner W, Gardner P, and Gross PΑ, "Hepatitis B lmmunization strategies:Εxρanding the Target," Ann ιntern Med, 1993, 1 18(4):308-9.
6. Fahey BJ, Beekmann SE, Schmitt JM, el al' "Managing occupalional Exρosuresto HιV-1 in the Healthcare ννorkplace," ιnfect control HoSp Εpidemioι' 1993'14(7):405-12.
7. \Λ/ong ES, stoιka JL, chinchil|i VM' et aι, iAre Universal Precautions Etfective inReducing the Number of Occupational Exposures Among Healthcareννorkers?'' JAMA' 199'l' 265(9):1 123-8.
References
Buehler J\Λ/ and Ward JW, 'Α New Definition for AlDs Surueillance,'' Ann ιntern Med'1993, 1 18(5):390-2-
Brown Jμ/ and Blackwell H, "complying \Λ/ith the NeW oSHA Regs, Part '1: TeachingYour Staff About BiosaΙety," MLo' 1992' 24(4)24-8. Part 2: "saΙety ProtocolsNo Lab can lgnore," '1992, 24(5'|27-9. Part 3: "οompiling Employee safetyRecords τhat \Λ/ill Satisfy oSHA," 1992, 24(6):45-8.
Department of Labor, occupationaI safety and HΘalth Administration, "occupationalExposure to Bioodborne Pathogens; Final Rule (29 CFR Part 1910.1030),'' Federaι Register' December 6, 'l99'1, 64004-182.
Gold J\Λ/, "Hlv-1 lnfection: Diagnosis and Management," Med clin North Am, 1992,76(1 ):1 -18.
"Hepatitis B Virus: A comprehensive Strategy for Eliminating τransmission in lheUnited states τhrough Universal childhood Vaccination," Recommendations ofthe lmmunization Practices Advisory committee (Ac'P)' MMWR Morb MoιtaιwkΙy Rep' 1991' 40(RR-13):1-25.
"Mortality Attributable to HlV lnfection/ΑlDs - United sΙates'', MMWH Morb Mor1aιWkly Rep, 1991, 40(3):41-4.
National Committee for Clinical Laboratory Standards, "Protection of Laboratory\Λ/orkers From lnfectious Disease Transmitted by Blood' Body Fluids, andTissue,'' NccLS Document M29-T, Villanova, PΑ: NCCLS' 1989' 9(1).
"ΝosocomiaI Transmission of Hepatitis B Virus Αssociated \Λ/ith a sρring-LoadedFingerstick Device - california," MMWR Morb Mortaι wkιy Eeρ' 1990,39(35):610-3.
Polish LB, Shapiro CN, Bauer F, et al, "Nosocomial Transmission of Hepatitis B VirusAssociated With the Use oΙ a spring-Loaded Fingerstick Deνice,'' N Εngl JMed, 1 992, 326(1 1 t:721 -5.
"Recommendations for Preventing τransmission of Human lmmunodeficiency Virusand Hepatitis B virus to Patienιs During Exposure-Prone lnvasive Procedures,"MMWR Morb Mortal wkιy Reρ' 1991, 40(RR-8):1-9.
"Update: Acquired lmmunodefiοiency Syndrome - United Sιates," MMWR MorbMofial wkly Reρ, 1992' 41 (26):463-8.
"Update: τransmission of ΗlV lnfection During an lnvasive Dental Procedure -Florida,'' MMWR Morb Mortal wkιy Reρ' 1991' 40(2)j21-7' 33."Update: Universal Precautions Ιor Prevention oΙ Transmission of Human lmmuno-
deficiency virus, Hepatitis B Virus, and other Bloodborne Pathogens in Ηealth-care settings,'' MMWR Morb Moltaι wkly Rep' '1988' 37(24):377-82' 387-8'
123

PREDOMINANT CULTIVABLE MICROORGANISMSOF THE ORAL CAVITY
τvDe P]edominant Genus or FemiιvAerobic or Facultative
Gram'positive cocci Streptocφcus spS. mutaλs
3:."iδ*i'"S. salivarius
Gram_positive rods Lactobaci!ιus sρCorynebacteium sp
Gram-negative cocci Moraxella sρGram-negative rωs Εnterobacteiaceae sρ
AnaerobicGram-positive cocci PeptostreptococcusspGram-positive rods Actinomyces sρ
Eubacterium SρLactobaciιιus spLeptotrbhia sρ
Gram-negative cocci veiιlonelιa SρGram-negative rods Actinobaciιιus sρ
FusobacterΙum sρPrevoteιιa sρPorphyromonas spBacteroides spcempyιobacter sρ
spirochetes τreρonemasρFungi candidasρ
124

APPEΝDlx
REFERENCE VALUES FOR ADULTS
Automated chemistry (cHEMlsτRY A)Values Remarks
SERUM PLASMAAοetone
Albumin
Alcohol, ethyl
AldolaseAmmonia
AmylaseBilirubin, direct
Bilirubin, total
Calcium
Calcium, ionized
chloridΘ
Cholesterol, total
HDL cholesterol
LDL cholesterol
co,οreatine kinase (cK) isoenzymes
CK.BBCK-MB (cardiac)
CK-MM (musle)
cκ-MB levels must be both >47o and
Creatine phosphokinase (CPK)
οreatinine
Ferritin
Folate
GGτ (gamma-glutamyltEnsρeρtidase)
male
female
GLDHGlucose (2-h postprandial)
Glucosθ, fasting
Glucose, nonfasting (2-h postprandial)
Hemoglobin 41"
Hemoglobin, plasma free
Hemoglobin, total glyΦsylated (Hb A1)
lron
lron binding capacity, total (τlBc)Lactic acid
Lactate dehydrogenase (LDH)
Lactate dehydrogΘnase (LDH) isoenzymes
LDt
LD,LD"
LDn
LDu
10 lU/L to meet diagnostic critΘria for CK-MB positive result Φnsistent with myocardial injury
8-150 rU/L
ο.5-1.4 mαdL13-300 nσmL3.6-20 ng/dl
1 1-63 rU/L
8-35 rU/L
To be determined
Up to 140 mσdl60-110 mσdl60-140 mσdlI<2.5 mΦ10ο mL
4γ"-8"/.
65-150 mcg/dL
250-420 mcgldL0.7-2.1 mΕq/L
56-194 rU/L
20%-340/"
29oλ-41o/"
150/"-250/"
10/"-120/"
10/"-150/"
Specimen to be placed on ice as soon asωllected
Fasted blood required _ normal γalue atfectedby dietary habiιsτhis reference range is tor a general adultρopUlationFasted blood rθquired _ normal νaιue atfectedby dietary habits
LDLo calculated by Friewald formula... whiοhhas certain inaccuracies and is invalid at triglevels >3o0 mσdl
specimen to be kept on iΦ and sent to lab assoon as ρossible
Negative
3.2_5 ΦdLNegative
1.2-7.6lυlL20-70 mcg/dl
30-1 10 units,/L
0-0.3 mΦdL0.1-1.2 mg/dL
8.6-10.3 mΦdl2.24-2.46 mΕqlL95-108 mEq/L
Ξ22o mΦdL
40-60 mσdl
65-170 mσdl
23-30 mEq/L
oγ"
oγ"-3'9o/"
960/-10οo/o
Flipρed LD]/LD, ratios (>1 may be consistent with myocardial iniury) particular|y when considered in combination with a reΦnt cK-MB positive result
Lipase
Magnesium
Osmolality
Phosphatase, alkaline
adults 25-60 y
adults 61 y or older
infancy-adolescence
Phosρhate, inorganic
Potassium
Prealbumin
Protein, total
SGoτ (Asτ)
SGPT (ΑLτ) (10-35)
Sodium
τransfeπnτri9lycerides
Urea nitrogen (BUN)
Uric acid
malefemale
lncreased by slight hemoιysis
lncreased by slight hemolysis
23-208 units/L
1.6-2.5 mσdl289-308 mosm/kg
33-131 lU/L
5'1-153 tU/L
Values range up to 3-5 times higher thanadults
2.8-4'2 mΦdL3.5-5.2 mEq/L
>15 mΦdl6.5-7.9 ΦdL<35 tU/L (20-48)
<35 tU/L
134-149 mΕΦL>200 mΦdl45-155 mg/dl7-2O mg/dL
2.0-8.0 mσdl2.O-7.5 mgldL
125
Fasted blood required
-
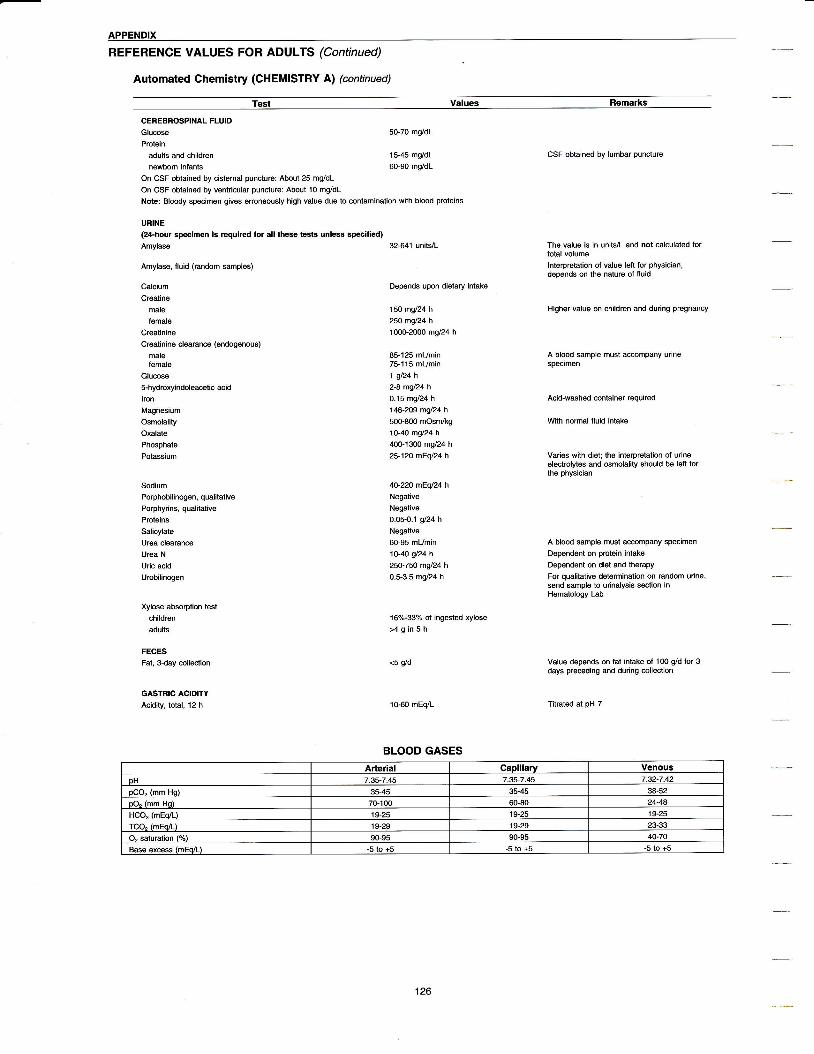
APPENDIX
REFERENOE vALUEs FoR ADULτS (Continued)
Automated chemistry (cHEMlsτRY A) (continued)
τest Values Remarks
CEREBROSPINAL FLUIDGlucoseProlein
adults and children
newborn infants
on csF obtained by cisternai puncture: Aboυt 25 mg/dL
on οsF obtained by ventricular puncture: Αbout 10 mg/dlNote: Bloody specimen gives erroneously high value due to contamination with blood proteins
URINE
50-70 mg/dl
15-45 mσdl60-90 mg/dl
(24-hour spΦimen is rΘquired for all thes tests υnless spΦified)Amylase
Αmylase, fluid (random 9mples)
οalciUm
Creatine
male
lemaleCreatinine
Creatinine clearance (endogenous)
malefemale
Glucose5-hydroxyindoleacetic aοid
lpnMagnesiυm
Osmolality
Oxalate
Phosρhate
Potassium
Sodium
Poφhobilinφen, qualitative
Porphyrins, qualitative
Proteins
Salicylate
υrea clearance
Urea N
Uric acid
Urobilinogen
Xylos absorption test
children
adults
FECESFat, 3-day coι|ection
GAsTRlc AclDlτYAcidity, total, 12 h
32-64'l unittL
Depends upon dietary intake
150 mσ24 h
25O mgl24 h
10ο0-2000 mg/24 h
85-125 ml/min75-115 mumin1 gl24 h
2-a mgl24hO-15 mgl24 h
146-209 mgl24 h
500-800 mosπ/kg1O-4O mgl24 h
400-1300 mg/24 h
25-120 mΕql24h
4o-22o mΕq24hNegative
Negative
0.05-0-1 g/24 h
Negative
6ο-95 mumin1o-4O gl24 h
25o-75O mgl24 h
0.5-3.5 mg/24 h
16%-33o/" of ingested xylose
>4gin5h
<5 αd
10-60 mEΦL
CSF obtained by lumbar puncture
The value is in units/l and not Φlculated fortoιal volume
lnterρretalion of value |ett for physician,deρends on the nature of fluid
Higher value on children and during pregnancy
A blood Sample must aΦmpany urinespecimen
Acid-washed container required
νvith normal fluid intake
Varies with diet; the interpretation of urineelectrolytes and osmolality should be left forthe physician
Α blood sample must accompany specimen
Dependent on protein intake
Dependent on diet and therapy
For qualitative deteminalion on random urine,send samρle to urinalysis section inHematology Lab
value depends on fat intake of 100 Φd lor 3days preceding and during Φllectιon
Titrated at pH 7
BLOOD GASESArterial CaDillaru Venous
oΗ 7.35-7.45 7.35-7,45 7.32-7.42
oCO" (mm Ho) 35-45 35-,ι5 38-52
oO" (mm HoΙ 70100 5ο-8o 24-48
HCO" (mEo/L) 19-25 19-25 19-25
τco" 1mEo/L) 19-29 19-29
O" saturation (o/") 90-95 90-95 40-70
Base exοess (mΕo/L) -5 to i5 -5 to +5 -5 to +5
126

APPENDIX
Segs = segmented neutrophils
Bands = band neutroρhilS
HEMATOLOGY
Complete Blood Count
Lymphs = lymphocytes
Monos = monocytes
Erythrocyte Sedimentation Rates and Reticulocμe countsSedimentation rate, \Λrestergren
Sedimentation rate, \Λrintrobe
Reticulocyte count
Children 0-20 mm/hour
Adult male 0-15 mm/hour
Adult female 0-20 mm/hour
οhiΙdren 0-13 mm/hour
Adult ma|e ο-10 mm/hour
Adult female 0-15 mm/hour
Newborns 27.-67"
1-6 mo o"/"-2'8γ"
Αdults 0.5%-1.5%
Age Hgb(q/dL)
Hclιo/^1
RBCamill/mm3) RD\iV
0-3 d 15.0-20.0 45-61 4.0-5.9 <18
1-2 wk 12.5-18.5 39-57
1-6 mo 10.0-13.0 29-42 3.1-4.3 <16.5
7 moΙo2ν 10.5-13.0 33-38 3.7-4.9 <16
l1 5-13 ο 34-39 3.9-5.0 <15
5-8 v 11 5-145 35-42 4.ο-4.9
'13-18 v 12.O-15.2 36-47 4.5-5.1 <14.5
Adult male 13.5-16.5 41 -50 < ι4.5
Adult female 12 o-'15 ο 36-44 4.0-4.9 <14.5
Age MCV(fLt
MCH MCHCιo/^\
Pltsx 103/mms)
0-3 d ο5-1 29-37 250-450
1-2 wk A6-1 1ο 2Β-36 28-38 25ο-450
1-6 mo 74-96 25-35 30-36 300-700
7 mo'ιo 2 ν 70-84 23-30 31-37 250-600
2-5 75-47 24-30 31-37 250-550
5-8 v 77-95 25-33 31-37 250-550
13-18 r 7A-96 25-35 31-37 150-450
Adult male aο-'1οο 26-34 31-37 150-450
Adult female aο-1οο 26-34 31-37 15ο-450
WBC and Diff
Age γιrBc(x 103/mm3) Segs Bands Lymphs Monos
0-3 d 9_0-35.0 32-62 10-18 19-29 5-7
1-2 wk 5.0-2ο.0 14-34 6- 36-45 6-10
1-6 mo 6.0-17.5 1 3-33 4^12 41-71 4-7
7 moΙo2ν 6_0-17.0 1 5-35 5. 45-76
2-5 ν 5.5-15.5 23-45 5-1 1 35-65
5-8 v 5.0-14.5 32-54 2A-44 3-6
13-18 v 4.5-13.0 34-64 5-1 1 25-45 3-6
Adults 4.5-1 1.0 35-66 5- 24-44 J-O
AgΘ Eosinophils Basophils Atypicall νmnhξ
No. ofNRBCs
0-3 d o-2 o-1 0-8 n-t
1-2 wk o-2 ο_1 ο-8 0'1-6 mo 0-3 ο_1 ο-8 ο
7moιo2 ο-3 o-1 0-θ ο
2_5 ν 0-3 0-1 ο-8 0
5_8 ν ο-3 ο-1 ο-8 0
13-18 v ο-3 ο-1 ο-8 ο
Adults ο-3 0-1 0-8 ο
127

APPENDIX
DENTIFRICE PRODUCTS
Brand Name Abrasive τherapeuticlnqredient lnqredient
FoamingAgent
Aim@ Baking soda Gel Ηydrated silica, Sodium bicarbonate sodium monofluorophosphate 0.7ol. sodium lauryl sulfate(fIuoride ο.14%)
Other lngredients: Sorbitol and related polyols, water, glycerin, SD alcohol 388, flavor, cellulose gum, sodium saccharin, blue #1,#
Aim@ Extra Strength Gel Ηydrated silica Sodium monofluorophosphate '1.2ol. Sodium lauryl sulfate
Other tngredients: Sorbitol, water, PEG-32, SD alcohol 388, flavor, cellulose gum, sodium saccharin, sodium benzoate, blue #1,#10
AimΘ Regular Strength Hydrated silica sodium monofluoroρhosphate 0.8% sodium lauryl sulfate(ΙtUoride ο.'14%)
αher lngredients: Sorbitol and other related ρolyols, Water, glycerin, sD alcohol 38B, flavor, cellulose gum, sodium saccharin, blue#1 vellow#10
Aim@ τartar control Gel Hydrated silica sodium monotluorophosphate 0.8% sodium lauryl sulfate(lluoride 0.14%)
αher lngredients: sorbitol and reIated polyols, water, glycerin, zinc citrate trihydrate, sD alcohol 38B, flavor, cellulose gum, sodiumblυe #1. vellow #'lο
AquafreshΘ Baking soda Toothpaste calcium carbonate, hydrated silica, sodium sodium monotluoroρhosρhate sodium lauryl suIfatebicarbonate
other lngredients: calcium carrageenan' cellυlose gum, coloE, flavor, glycerin' PEG-8, sodium benzoate, sodiUm saΦharin, sorbitol,titanium dioxde. water
AquafreshΘ Extra Fresh Toothpaste* Ηydrated silica, οalcium carbonate sodium monofluorophosphate sodium lauryl sulfate
Other lngredients: Sorbitol, water, glycerin, PEG-8, titanium dioxide, cellulose gum, flavor, sodium saccharin, sodium benzoate,calciυm carraoeenan. colors
AquafreshΘ for Kids τoothpaste* Hydrated silica, caicium carbonate sodium monofΙuorophosphate Sodium lauryl sulfate
other lngredients: Sorbitol, Water, glycerin, PEG_8, titanium dioxide, cellulose 9Um, flavor, sodium Saοcharin, calcium carrageenan,sodium benzoate. colors
Aquafresh@ Gum Care Toothpaste Hydrated silica, calcium carbonate Sodium monofluorophosphate Sodium lauryl sulfate
other lngredients: calcium carrageenan, cellUlose gum, colors, flavor, PEG-8, sodium benzoate, sodium Saωharin, sorbitol, titaniumwater
AqualreshΘsensitiveτoothpaste Hydratedsilica Potassium nitrate, sodium fluoride Sodium lauryl sulfate
Other lnqredients: Colors, flavor. qlvcerin, sodium
AquafreshΘ Tartar control τoothpaste* Hydrated silica Sodium fluoride sodium |auryl su|Ιate
other ιngredients: τetrapotassium pyrophosphate, tetrasodium pyrophosphate, sorbitol, glycerin, PEG-8, flavor, xanthan gum, sodiumsaccharin. sodium benzoate. colors.
AquafreshΘ Triple Protection τoothpaste* Hydrated silica, Φlcium carbonate sodium monofιuorophosphate Sodium lauryl sulfate
Other lngredients: PEG-8, sorbitol, cellulose gum, sodium benzoate, titanium dioxide, calcium carrageenan, flavor, sodium saccharin,coloE. water
Aquafresh@ \rνhjtening Gel or Toothpaste HydΙated silica sodium lluoride sodium lauryl sulfate
Other lngredients: Colors, flavor, glycerin, PEG-8, sodium benzoate, sodium hydroxide, sodium saccharin, sodium tripolyphosphate,
BioteneΘ Antibacterial Dry Mouth Hydrated silica, calcium pyrophosphate Lactoperoxidase, glucose oxidase,τoothpaste lysozyme, sodiυm monofluorophosphate
(o.76γ")
other lngredients: sorbitol, glyοerin, xylitol, isoceteth-2o, cellulose gum, flavor, sodium benzoaie, beta-d-glucose, potassium
close-UpΘ Baking soda Toothpaste (mint) Hydrated siliοa, sodium bicarbonate Sodium monofluorophosphate 0.79% Sodium lauryl suIfate(fluoride 0.15%)
other lngredients: sorbitol and related ρolyols, water, glycerin, SD alcohol 38B, flavor, cellulose gum, sodium saccharin, sodiumbenzoate, red #33' red #4ο, titanium dioxide
close-Up@ οlassic Red Gel Hydrated silica sodium monofluorophosphate 0.8% sodium lauryl sulfate(lluoride 0.14%)
other lngredients: sorbitol and related polyols, water, g|yοerin, SD alcohol 38B, flavor, cellulose gum, sodium saccharin, sodium
close_Up@ cool Mint Gel Ηydrated silica sodium monofluorophosρhate 0.79% sodium lauryl sulfate(fluoride 0.15%)
other |ngredients: Sorbitol, water, glycerin, sD alcohol 38B, flavor, cellulose gum, sodium saωharin, po|ysorbate 20, blue #1, mica,red #33 titanium dioxide
close-UpΘ original Red ιΛ/hitening Hydrated siιiοa Sodium monofluorophosphate 0.8% sodium lauryl sulfateτoothpaste (Ιluoride 0.14%)
αher lngredients: sorbitoi and related poIyols, water, glycerin, sD alcohol 38B, flavor, celluiose gum, sodium saccharin, sodiumchloride. red iP30 lake. titanium dioxide. blue #1
close-Up@ τartar control Gel (mint) Hydrated silica sodium monof|uorophosphate 0.79% sodium lauryl sulfate(fluoride 0.15%)
αher lngredients: Sorbitol and related ρolyols, water, glycerin, zinο citrate trihydrate, sD alcohol 38B, flavor, cellulose gum, sodiumsaΦharin. red #33. red #4o. caffeine frΦ
close_Uρ@ Tartar contml \Λrhitening Ηydrated silica Sodium monofluorophosphate ο.8% sodium lauryl sulfateToothpaste (Ιluoride 0.14ol")
αher lngredients: SoIbitol and related ρolypols, water, glycerin, sD alcohol 38B, Ιlavor, zinc citrate trihydrate, cellulose gum, sodiumtitanium dioxide. blue #1. vellow #10
οolgateΘ Baking soda & Peroxide τartar Hydrated silica, sodium bicarbonate Sodium monofluorophosphate 0.76% sodium lauryl sulfatecontroΙ Toothpaste'
othe. lngredients: Glycerin, propylene glycol, water, pentasodium triphosρhate, tetrasodium pyroρhosρhate, titanium dioxide, Ιlavor,sodium hvdroxide. calcium Deroxide, sodium saccharin, carraqeenan, cellulose qum, FD&C blue #1, D&C yellow #10
colgate@ Baking soda & Peroxide Ηydrated Silica, sodium bicarbonate, Sodium monofluorophosphate 0.76% Sodium lauryl sulfate\Λrhitening τωthpaste* aluminum oxide
other lngredients: GlyΦrin, polypylene glycol, water, penιasodium triphosphate, tetrasodium pyrophosphate, titanium dioxide, tlavor,
sodium hvdroxide. calcium oeroxide. sodium saccharin. carraoeenan, cellulose qum, dietetically sucrose free
colgateΘ Baking Soda Tarlar control Gel Hydrated silica, sodium bicarbonate Sodium tluoride 0.243% Sodium lauryl sulfateor τoothρaste
other lngredients: Glycerin, tetrasodium ρyrophosphate, PVM/MA coρolymer, cellulose gum, flavor, sodium saccharin, sodiumhvdroxide. titanium dioxide (paste). FD&c blue #'1, D&ο ve|low #10 (οeI), dieteticaιly sucros free
Hydrated siliοa Sodium fluoride 0-243ol" SodΙUm lauryl sulfate
other lngredients: sorbitol, water, PEG-12, flavor, tetrasodium ρyrophosphate, cellulose gum, sodium Saοcharin, mica, titaniumοolgateΘ Junior Gel-
dioxide, colorants,
128

APPΕNDlx
Toothpaste
Brand Name Abrasive τherapeuιiclnοredient lnq]edient
FoamingAqent
colgateΘ PlatinumτM \Λrhitening Toothpaste- Silica, aluminum oxide sωium monof|uorophosρhate SωiUm lauryl sulfate
αher lngrcdients: \Λrater, hydrated silica, Sorbiιol, glycerin, PEG-12, tetrapotassium pyrophosρhate, PVM/MA copolymer, flavor,sodium hγdrcxide, sodium saΦharin, titanium dioxide
colgate@ PlatinumτM \Λrhitening with Baking Sodium bicarbonate, aluminum oΧide sωium monofluorophosρhate 0.76% sωium lauryl sullateSoda Toothρaste*
other lngrcdients: \Λrater, glycerin, PEG-12, tetrapotassium pyroρhosphate, PVM/MA copolymer, flavor, sodium hydroxide, sodiumsacοharin, titanium dioxide, celluΙose gum
colgateΘ sensitive Maximum Strength Ηydrated silica, sodium bicarbonate Potassium nitrate 57o, stannous fΙuoride Sodium lauryl sulfateo.45γ"
Other lngaedients: Glycerin and/or sorbitol, water, PEG-40 castor oil, PEG-12, poloxamer 407, sodium citrate, flavor, titanium dioxide,sοdium hydroxide, cellu|ose gum, xanthan gum, sodium saccharin, stannous chloride, citric aοid, tetEsodium pyrophosρhate, FD&cBlue No. 1
colgate@ τartar οontrol Micro cleansing Hydrated si|ica sodium fIuoride 0.243% Sodium lauryl suIlateGel or Toothpaste*
other lngredienιs: \rνater, sorbitol, glycerin, PEG-12, tetrasodium pyroρhosphate, PVλ/VMA copolymer, cellulose gum, flavor, Sodiumhvdroxide. titaniυm dioxide. Sodium saccharin. οarraoeenan, dieteticallv sucros
'@colgateΘ Tartar control Plus ννhitening HydEted silica, aluminum oxide sodium monofluoroρhosphate 0.76% sodium lauryl sulfate
other lngredients: \tr/ater, sorbitol, glycerin, pentasodium triphosphate, tetrasodiUm pyrophosphate, PVλ4/MA copolymer, cellυloseoum. flavor. sodium hvdroxide. titanium dioxide. sodium saccharin. οaΙraoeenan
colgateΘ Toothpaste- Dicalcium phosphate dihydrate sodium monofluorophosphate 0.76% sodium lauryl sullate
other lnoredients: Glvcerin. cellulose oum. tetrasodiUm oγroohosohate' sodium saccharin, flavor, dieteticallv sucroΦ frΦColgate Total@ Toothpaste Hydrated silica Sodium fluoride 0.243ol., triclosan 0.3% Sodium lauryl sulfate
oιher lngredients: \Ι/ater, glycerin, sorbitol, PVM/MΑ copolymer, cel|ulose gum, flavor, sodium hydΦxide, propylene glycol,sodium saccharin. titanium dioxide
colgate τotalΘ Fresh stripe τoothρaste Hydrated Silica Sodium fluoride 0.243ol", triclosan 0.3% Sodium lauryl sulfate
Other lngredients: Water, glycerin, sorbitol, PVM/MA copolymer, cellulose gum, flavor, sodium hydrcxide, propylene glycol,carraoeenan. sodium saΦharin. mica' titanium dioxide, FD&c bΙue #1, D&c vellow #10
colgateΘ ιryinterfresh Gel- Hydrated Silica sodium fluoride 0.243% sodium lauryl sulfate
other |ngredients: sorbitol, Water, PEG-12, llaνor, tetrasodium pyrophosphate, cellulose gum, sodium Saccharin, FD&c blue #1,sucrose free
crest@ Baking Soda τartar Protection Gel Hydrated silica, sodium bicarbonate Sodium fluoride 0.243%or τoothpaste (mint)-
Sodium lauryl sulfate
other lngredients: \Λ/ater, glycerin, sorbitol, tetrasodium pyrophosphate, PEG-6, fΙavor, celιulose gum, sodium saΦharin, titaniumdioxide (paste), FD&ο blue #'1 (gel), disodium ρyrophosphate, tetrapotassium pyrophosρhate, carbomer 956, xanthan gum, FD&c
#5
crestΦ cavity Proteοtion with Baking soda Hydrated siΙiΦ, sodium bicarbonate Sodium fluoride 0.243ol"Gel or Toothpaste (mint)*
Other lngredients: Sorbitol, water, glycerin, sodium carbonate, flavor, cellulose gum, sodium saccharin, titanium dioxide (paste),
Sodium lauryl sulfate
FD&C blue #1
creslo οavity Protection Gel (cool mint)* Hydrated silica Sodium fluoride 0.243%
other ιngredients: Sorbitol, water, trisodium phosphate, flavor, Sodium phosphate, xanthan gum, sodium Saccharin, carbomer 956,
Sodium lauryl sultate
FD&C blue #1,
crest@ οavity Protection ToothpastΘ" (icy Hydrated silicamint or regular)
Sodium f luoride 0.24Ι}y"
αhe. lngrcdients: Sorbitol, Water, glycerin (mint), trisodium phosρhate, llavor, sodiυm phosphate, cellulose gum (mint), Xanthan gum(reqular), sodium saccharin, carbomer 956, titanium dioxide, FD&C blue #1. carbomer 9404
Sodium lauryl sulfate
crest@ Extra \Λrhiιening Gel or τoothpaste Hydrated siiica Sodium fluoride 0.15ol. Sodium lauryl sulfate, poloxamer 407
αher lngrcdients: Sorbitol, water, glycerin, tetrasodium pyrophosphate, sodium οarbonate, carboxymethylcellulose sodium, titaniumdiοxi.|e carnaltba wax sodium saωharin. flavor. FD&c blue #1. FD&c vellow #5. PEG-6. sodium bicarbonatet
crest@ ror Kids cavity Protection GeΙ Hydrated silica Sodium fluoride 0.243% Sωium lauryl sulfate
other lngredients: sorbitol, Water, trisodium phosρhate, sodium ρhosρhate, xanthan gum, llavor, sodium saΦharin, carbomer 956,miΦ, titanium dioxide, FD&c blue #1
οrestΘ Gum care Gel or τoothpaste Hydrated silica Stannous fluoride 0.4547o sodium laUryI sullate
Other lngredients: Sorbitol, water, stannous chloride, titanium dioxide (paste), flavor, sodium hydroxide, sodium saccharin, sodiumcarraqeenan, FD&C blue #1 (qel), sodium qluconate, hydroxyethylcellulose
οrestΘ Multicare Gel or τoothρaste (cool Hydrated silica, Sodium bicarbonate Sodiυm fiuoride 0.243ol" sodium lauryl sulfatemint, fresh mint)
oιher lngredients: τetrasodium pyrophosphate, xyιitol, water, glyοerin, PEG-6, poloxamer 407, sodium carbonate, f|avor, celluloseoum. xanthan οUm- sodium saΦharin. titanium dioxide. FD&ο blue #1. FD&c ve|low #5 (cool mint)
crestΘsensitivityProtectionToothpaste* HydratedSilica(mild mint)
Potassium nitrate 5olo, sodium rluoride Sodium lauryl sultateo.150/"
other lngredients: Water, 9lycerin, sorbitol, trisodium phosphate, celIulose gum, flavor, xanthan gum, sodium saΦharin, titaniumdioxide. dve free
crest@ τartar Protection Gel* (fresh mint,smooth mint)
sodium fluoride ο.243% Sodium lauryl sulfate
other lngredients: ν1,/ater, sorbitol, glyοerin, tetrapotassium pyrophosphate, PEG-6' disodium pyrophosphate, tetrasodiumovroohosohate. flavor. xanthan oum. Sodium saωharin. carbomer 956. FD&c blue #1 ' FD&c γellow #5 (Smooth mint)
crestΘ τartar Protection Toothpasιe- silica sodium fluoride 0.243% sodium Ιauryl sulfate(original flavo0
other ιngredients: ι/vater, sorbitol, glycerin, tetrapotassium pyrophosphate, PEG-6, disodium ρyrophosphate, tetrasodiumovroohosohate. flavor. xanthan αum. sodium saωharin' carbomΘr 956, titanium dioxide, FD&c blue #1
Dr. τichenor's Toothpaste Hydrated siliοa Sodium fluoride Sodium lauryl sulfate
other lngredients: \Λrater, glycerin, sorbitol, insoluble Sodium metaphosphate, peppermint oil, cellulose gum, sodium saccharin,sodium ohosDhate. titanium dioxide.
EnamelonΘAll-Familyτoothpaste HydratedsiIica Sodium fluoride (fluoride 0.14%) Sodium lauryl sufateotheΙ lngredients: \Λrater, glycerin, sorbitoI, monoammonium phosphate, calcium sulfate, xanlhan gum, llavor, PEG-60 hydrogenaιedcastor oil, sodium Saοcharin, ammonium οhloride, celIUlose gum, titaniUm dioxide, magnesium chloride, methylparaben, propylparaben,FD&c bιue #1
First Teeth.u Baby Gel Lactoperoxidase 0.7 units/g, lactoferrin, Sodium lauryl Sulfaιeglucose oxidase
αher lnαredients: \Λrater.
F|uoride FoamτM"+ lngredients: Fluoride 1.2396 (from sodium fluoride and hydrogen fluoride), Water, phosρhoric acid, poloxamer, sodium saccharin, flavor
gluten free
129
-

APPENDIX
DENτIFRICE PRoDUcTs (Continued)
Brand Name Abrasivelngredient
Τherapeuticlngredient
FoamingAgent
GleemΘ τoothρaste Hydrated silica sodium f luoridΘ 0.243"/" sodium lauryl sυlfate
other lngredienιs: Sorbitol, water, trisodium phosphate, rlavors, sodium phosphate, xanthan gum, sodium saοcharin, caΦomer 956,titaniυm dioxide. dve free
Listerine@ Gel or Toothρaste Hydrated siliοa(cool mint)
Sodium monofluorophosphate Sodium lauryl sulfate
Other lngredients: \ivater, sorbitol, glycerin, flavors, cellulose gum, sodium saccharin, phosphoric acid, FD&C blue #1, D&C yellow#10. sodium DhosDhate. benzoic acid. titanium dioxide (oaste). xanthan
ListerineΦ τartar control Gei or Toothpaste Hydrated silica(cool mint)
Sodium fluoride Sodium lauryl sulfate
other lngredients: ι/vater, sorbitol, glycerin, PEG-32, flavor, cellUlose gum, sodium saccharin, tetrapotassium pyrophosphate, FD&c#1. D&C vellow #10. titanium dioxide
Mentadent@ Advanced \Λ,/hitening Gel or Ηydrated silica, sodium bicarbonate Sodium fluoride 0.15%Toothρaste
sodium lauryl sulfate, hydrogen ρeroxide
other lngredients: Zinο citrate trihydrate, Water, SorbitoI, glyοerin, poloxamer 4o7' PΕG-32' SD alcohol 38B, flaνor, cellulose gum,
MentadentΘ Gum care Gel or Toothpaste Hydrated silica, sodium bicarbonate sodium fluoride 0.24% (fluoride 0.15%) sodiυm lauryl Sulfate, hydrogen peroxide
other lngredients: Zinc citrate trihydrate (1.8old, Water, sorbitol, glycerin, poloxamer 4ο7, PEG-32' SD alcohol 38B, f|avor, cel|ulose
Νrentadent@ τartar control Gel or Hydrated Silica, sodium bicaΦonate sodiυm lluoride 0.24% Sodium lauryl sulfate, hydrogen peroxideτoothpaste
αher lngredients: \Λrater, sorbitol, glycerin, poloxamer 407, PEG-32, zinc citrate, sD alcohol 38B, flavor, cellulose gum, sodium#1
MentadentΘ with Baking soda & Peroxide Hydrated silica, sodium bicarbonate Sodium fluoride o.24oλ (Ιlυoride 0j5ok' sodium lauryl sulfate, hydrogen peroxideGel or τoothpaste-
other lngredients: ννater, sorbitol, glycerin, poloxamer 407, PΕG-32, sD alcohol 38B, flavor, cellUlose gum, sodiUm saccharin,ohosohοric acid blιre #1 titanil]m diοxide
ιjly First colgate@ Gel* Hydrated silica Sodium fluoride 0.243ol" sodium lauryl sulfate
other lngredients: \Λrater, sorbitoI, PEG-12, flavor, tetrasodium pyrophosphate, cellulose gum, sodium saΦharin, FD&c red #40, D&cred f33- dieteticallv sucrose free
Natural \ΛrhiteΘ Toothpaste Hydrated silica Sodium fluoride Sodium lauryl sullateother lnαredients: solbitoi water οlvcerin sodiιlm ben7οate titaniιlm.|iοxide Ιlavοr cellι]lοsρ ο|lm die-te-ticallv sucrosο lrΦ
Νatural \rνhite@ Baking soda τoothpaste calcium carbonate Sodium monofluorophosphate sodium lauryl sulfateother lnσredients: sorbitol. Water olvcerin. sodiιrm bicarbonatef carraοeenan natι]ral flavοr dieteticellv sucrose rrΦ
Natural ννhiteΘ Fights Plaque Toothρaste Hydrated silica Sodium fluoride sodium lauryl Sulfateother Ιnoredients: sorbitοl Water οlvcelin sodium ben7oale titaniι]m dioxide flavοr celhrlοse οιlm diοtEticrlrv sucrose free
Natural WhiteΦ sensitive TΦthρaste Hydrated silica Sodium monofluorophosphate, potassium Sodium lauryl sulfatenitrate
other lngredients: Sorbitol, Water, glyοerin, flavor, FD&c red #40, sodium benzoate, titanium dioxide, sodium saccharin, dieteticallysucrose free
Natural \Ι/hite@ Tartar contro| τoothpaste HydΙated silica Sodium flυοride Sodium lauryl sulfate
oιher lngredients: sorbitol, Water, g|ycerin, Xanthan gum, tetrapotassium pyrophosphate, titanium dioxide, celluIose gum, flavor,sodium benzoate. FD&c blue #1. D&c vellow #10. dietΘtica|lv sucrosΘ ffee
Natural ιΛ/hiteΘ with Peroxide Ge| Hydrogen peroxide
Other lngredients: Vvater, glycerin, flavor, dipotassium phosphate, sodium saccharin, phosphoric acid, poloxamer, dieteticallysucrose f@
oEjelΘ Baby Tooth & Gum cleanser Gelother lngredients: Poloxamer 407 (2%), simethicone (0.12%), Microdent, carboxymethylοe||ulose, sodium, citric acid, flavor, g|ycerin,
sodium saccharin. sorbitο|. fluoride frΦorajelΘ Gold sensitive Teeth Ge| for Adults Hydrated silica Potassium nitrate 5%, sodium Sodium lauryl sultate
monof luorophosphate 0.2%
other lnoredients: FD&c blue #1. flavor. olvcerin. sodiυm laurovl sarcΦinate. sodium
Pearl DropsΘ Toothpolish Paste Hydrated silica, calcium pyrophosρhate, sodium monofluoroρhosphate Sodium lauryl sulfatedicalcium phosphate, aluminum hydroxide
other lngredients: \,νater, Sorbitol, glycerin, PEG-12, flavor, ceIlulose gum, trisodium ρhosphate, SodiUm ρhosρhate, sodiumsaωharjn. dieιeticallv sucrose frΦ. dve free
Pearl DropsΘ τoothpo|ish Gel Hydrated silica sodium monofluorophosphate Sodium laury] sulΙate
Other lngredients: Sorbitol, water, glycerin, PEG-12, flavor, cellulose gum, sodium saccharin, FD&C blue #1, FD&C yellow #10,sucrose free
Pearl Droρs@ \Λ/hitening Extra strength Hydrated silica, calcium pyrophosphate, Sodium monofluorophosphate sodium Ιauryl sulfatePaste diοalcium ρhosphate
other lngredients: ιΛ,/ater, sorbitol. glycerin, PEG-12, flavor, cellulose gum, trisodium phosphate, sodium phosphate, sodiumsaccharin, titanium dioxide. dieteticallv sucrose fe. dve free
Pearl DropsΘ \Λrhitening Gel(icy cool mint)
Hydrated silica sodium monoflυorophosρhate sodium lauryl sulfate
other lngredients: sorbitol, Water, glycerin, PEG-12, flavor, οellulose gum, Sodium Saccharin, FD&c blue #'1, FD&ο yellow #10,
PepsodentΘ Baking soda Toothpaste Hydrated Silica sodium monoΙluorophosphate 0.8% sodium lauryl sulfate(fluoride (0.14%)
Other Ingredients: Sorbitol, water, sodium bicarbonatet, PEG-32, SD alcohol 388, flavor, cellulose gum, sodium saccharin, titanium
Pepsodent@ Original Toothpaste Hydrated silica Sodium monofluorophosphate 0.8% Sodium lauryl sulfate(fluoride 0.14%)
other lngrcdients: Sorbitol and related polyols, water, glycerin, sD alcohol 38B, flavor, cellulose gum, sodium saccharin, titaniυm
Peρsodent@ Tartar control Toothpaste Hydrated silica sωium monotluorophosρhate 0.8% Sodium lauryl sulfate(fluoride 0.14%)
Other lngredients: Sorbitol and related polyols, water, glycerin, SD alcohol 388, zinc citrate trihydrate, flavor, cellulose gum, sodium'l vcllow #1
Pete & Pamπ Gel (premeasured strips) Hydrated Silica Sodiummonofluorophosphateο.76% sodiumlaurylSarcosinateother |ngredients: sorbitol, Water, glycerin, xanthan gum, polysorbate 2ο, sodium benzoate, pluronic P84, FD&c blue #1, FD&c red#33 FD&c νellow #5 flavοr xvlilol
130

APPENDIX
Brand Name Abrasive τherapeuticlnαredient lnqredient
FoamingAEent
Promise@ τoothρaste Dicalcium phosρhate Potassium nitrate, sodiυm Sodium lauryl sulfatemonofluorophosphate
other lngrcdients: \Λ/ater, hydroxyethylcellulose, flavor, sodiυm saccharin, methy|paraben, propylparaben, D&c yelιow #10, FD&cbιue #1 ' οlrοerin. sorbitol. silicon dioxide. dieteticallv sucrose frΦ
Reach Act Adult Antιcavity τreatment ιngredients: sodium fluoride 0.05%, cetylpyridinium chloride, D&ο red #33 (cinnamon), EDTΑ calcium disodium, FD&c yellow #5,
Liquid (cinnamon, mint)+ flavor, glycerin, monobasic sodium phosphale, dibasic Sodium phosphate, poloxamer 407, ρolysorbate 80 (cinnamon), polysorbate 20(mint), propylene glycol, sodium benzoate, sodium saccharin, water, FD&C green rPJ (mint), menthol (mint), methyl salicylate (mint),
Dotassium sorbate (mint). aιcohol frΦReach Act for KidS*+ lngrΘdients: Sodium fluoride 0.05%, οeιy|pyridinium chloride, D&c red #33, EDτA calcium disodium, flavor, glyΦrin, monobasic
sodium phosρhate, dibasic sodium phosphate, poloxamer 407, polysorbate 80, propylene glycol, sodium benzoate, sodium saccharin,water, alcohol free
Rembrandι@ Age_Detying Adult τoothpaste Dicalcium orthophosρhate, Soft silica sodium monofluorophosphate (fluoride(original or mint) 0.15%)
αher lngredients: τrihydroxy proρane, ρerhydrol urea, aluminum oxide, acetylated ρectins, sodium ciιrate' iridiυm' papain, carboxyΙ
Mouthwasht flavor. cocamidooroprl betaine, citric aοid, sodium benzoate, sodium saccharin, sodium hvdroxide, alcohol freRembrandtΘ Daily \Λ/hitening Gel Silica Sodium monof|uoroρhosphate (fluoride carbamide peroxide, sodium lauryl sullate
ο.15%)
Other lnoredients: Glvcerin, sodium citrate, carbopol, triethanolamine, flavor
Rembrandt@ \Λ/hitening Baking Soda Sodium bicarbonate, silica Sodium monofluorophosphate (fluoride sodium lauryl sulfateτoothpaste 0.15%)
αher lngrcdients: Glycerin, sorbito|, aiumina, waler, sodium citrate, sodium carrageenan, papain, flavor, sodium hydroxide, FD&c
Rembrandt@ Whitening canker sore Dicalοium phosphate, silica Sodium monofluorophosphate (fluoridePrevention τoothpaste 0.15%)
αher lnqredients: ν\rater, οlycerin, Xylitol, sodium citrate, natural flavors, Sodium carrageenan, papain, citric acid, dye free
Rembrandt@ ιΛrhiιening Natural Toothpaste Dicalcium phosphate, silica Sodium monofluorophosphate
other lnqredients: \Λrater, glycerin, xylitol, Sodium citrate, natural flavors, Sodium carrageenan, papain, citriο acid, dye free
RembrandtΘ \Λ/hitening sensitive Dicalοium phosρhate dihydrate Potassium nitrate 5%, sodium Sodium lauryl Sulfateτoothpaste monofluoroρhosphate 0.76%
αher lngredients: Glycerin, sorbitol, Water, alumina, paρain, sodium citrate, flavor, carlcoxymethylοel!ulose Sodium, sodium saccharin,methylparaben, FD&C red #40, citric acid
Rembrandt@ \,vhiιening Toothpaste Dicalcium phosphate dihydrate sodium monofluorophosphate 0.76% sodium lauryl sulfate(mint or original)
other lngredients: Glycerin, sorbitol, water, alumina, sodium citrate, flavor, sodium οarrageenan, papain, sodium saccharin,methylparaben, citric acid, FD&c blue #1, FD&ο yellow #5
ReveΙationΘ τoothpowder Calcium carbonate
other lngredientε: Methyl salicylate, menthol, dye freevegetable soap ρowder
SensodyneΘ Baking soda τoothpaste Sodium biοarbonate, silica Potassium nitrate, sodium fluoride Sodium lauryl sulfate
other lngredients: νγater, glycerin, flavor, hydroxyethylcellulose, titanium dioxide, sodium saccharin, dietetically sιcrose frΦ, dyefree
Sensodyne@ cool Gel Silica Potassium nitrate, sodium fluoride sodium meιhyl cocoyl taurate
Other lngredients: \i/ater, sorbitol, glycerin, sodium carboxymethylcellulose, flavor, sodium saccharin, FD&C blue #1, trisodiumohosohaιe. dieteticallv sucrose frΦ
SensodyneΘ Extra \Λ/hitening Toothpaste Silica Potassium nitrate, sodium sodium lauryl Sulfatemonofluoroρhosphate
other lngredients: νγater, flaνor,glycerin, PEG-12, PEG-75, sodium carbonate, sodium sacοharin, titanium dioxide, calcium peroxide,
SensodyneΘ Toothpaste'(fresh mint)
Dicalcium phosphate Potassium nitrate, sodiummonofluorophosphate
Sodium lauryl sulfate
other lngredients: \Λ/ater, glycerin, sorbitol, hydroxmethylcellulose, flavor, Sodium saccharin, methylρa.aben, proρylparaben, D&ο#10. FD&C blue #'1, silicon dioxide, dieteticallv sucrose tree
sensodyneΘ Toothpaste (origina|) Silica Potassium nitrate, sodium fluoride sodium methvl cocovΙ taurate
other lngredients: \Λ/ater, glycerin, Sorbitol, ceιlulose 9um, titanium dioxide, sodium Saccharin, flavor, D&c red #28, trisodium
slimeι@ Gel" Hydrated silica Sodium fluoride 0.15%
other lngredients: sorbitol, Water, glycerin, PEG-32' flavor, ethyl alcohol, ρropylene glycol' glyceryl triacetate, οellulose gum, sodiumsaccharin, sodium benzoate, FD&C blue #1
τhermodent Toothpaste Diatomaceous earth, silica Strontium chloride hexahydrate Sodium methyl cocoyl taurate
other lnοredients: sorbitol. olvcerin. titanium dioxide, quar qUm, PEG-40 stearate, hγdroxvethγlcellulose. flavor, preseryative' Water
τom'sΘ Νatural Baking Soda With Propo|is calcium carbonate, sodium biοarbonate sodium lauryl sulfate& Myrrh Toothρaste
other lnσredients: G|vcerin, Water. carraoeenan, peρρermint oil, mvrrh, ρropolis, fluoride frΦτom'sΘ Natural Baking Soda, οalcium, and calοium carbonate, sodium bicarbonate Sodium monofluorophosphate Sodium lauryl sulfateFluoride Τoothpaste
τom'sΘ Νatura| calcium and Fluoride ca|cium carbonate sodium monofluorophosphate sodium lauryl sullateτoothpaste*
other lngredienιs: Glycerin; Water; carrageenan; xylitol (sρearmint); cinnamon, fennel oil, or Spearmint; peppermint oil (cinnamon,
τom's@ Natural calcium and Fluoride calcium carbonate, hydrated silica sodium monofluorophosphate Sodium lauryl sulfateτoothpaste
otheΙ lnqredients: Glycerin, Water' carraqeenan, xylitol, natural winterqreen oil
Tom'sΘ Natural for children with calcium caΙcium carbonate, hydrated silica Sodium monofluorophosphate Sodium lauryl sulfateand Fluoride τoothpaste
Other lnqredients: Glvcerin, fruit extracts, carraqeenan, water
Tom'sΘ Natural With Propolis and lνΙyrrh calcium carbonate Sodium lauryl sulfateτoothpaste
t-. "'".
raki"*"* *"*τoothpasιe
Other lngredients; Glycerin, water, propylene glycol, cellulose gum, flavor, sodium saccharin, titanium dioxide, sodium hydroxide,οalcium peroxide, carrageenan, dietetically sucrose free
131
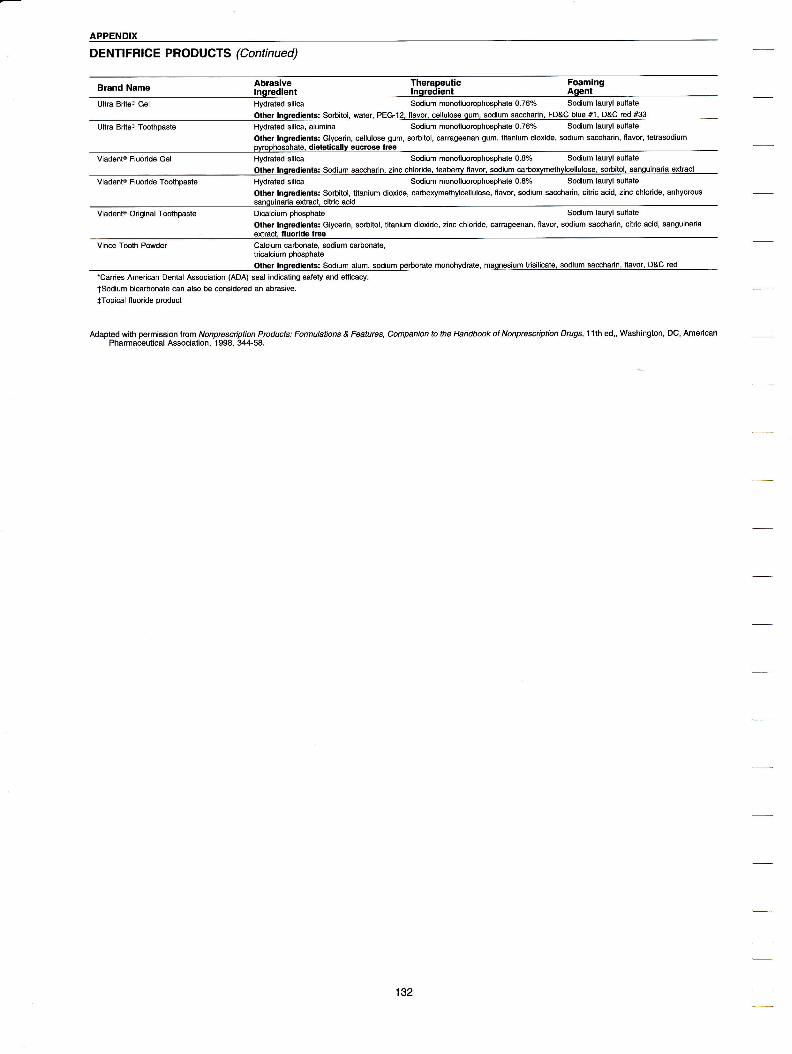
APPENDIX
DENτlFRlcE PRoDυcτs (Continued)
Brand Name Abrasive Therapeuticlnαredient lnqredient
FoamingAqent
Ultra BriteΘ Gel Hydrated silica sodium monofluorophosphate ο.76% sodium lauryl sulfate
αher lnqredients: sorbilol. water, PEG-12, ,lavor, celluiose qum, sodium saccharin, FD&c blue #1, D&c red #33
Ultra BriteΘ τoothpaste Hydrated silica, alumina sodium monolluorophosphate ο.76% sodium lauryl sulfate
othΘr lngredients: Glycerin, ce|lulose gum, sorbitol, carrageenan gum, titanium dioxide, sodium saωharin, flavor, tetrasodiumsuc]ose frΦ
viadentΘ Fluoride Gel Hydrated silica Sodium monofluorophosphate ο.8% sodium lauryl sulfate
other lnoredients: sodium saωharin. zinc οh|oride, teaberry flaγor, sodium οarboxvmethylcellulose, sorbitol, sanguinaria extract
viadentΘ FIuoride TΦthpaste Hydrated silica sodium monofluorophosphate 0.8ol. sodium lauryl sulfate
Other lngredients: Sorbitol, titanium dioxide, carboxymethylcellulose, flavor, sodium saccharin, citric acid, zinc chloride, anhydrous
viadentΘ original Toothpaste Dicalcium phosphate Sodium lauryl sulfate
αher lngredients: Glycerin, sorbitol, titanium dioxide, zinc chloride, carrageenan, flavor, sodium saccharin, citric acid, sanguinariaextract,
VinΦ Tooth Powder οalcium Φrbonate, sodium carbonate,tricalcium ρhosρhateother lnqredients: sodium alum, sodium oerborate monohvdrate, maοnesium trisilicate, sodium saccharin, flavor, D&c red
*carries American Dental Association (ADA) seal indiΦting safety and etficacy.
tsodium bicarbonate can also be Φnsidered an abrasiνe.
+τopical fluoride product
Adapted with ρermission from Λ/onprescriρtion Products: Formutations & Features' companion to the Handbωk of Nonprescriρtion Drugs,1 1th ed,, \Λ/ashington, Dc, AmericanPharmaceutical Association, 1998, 344-58.
132

APPENDIX
ORAL RINSE PRODUCTSBrand Name Antiseptic Other lngredientsAstring-o-SolΘ Liquid SD alcohol 388 75.6%, methyl Water, myrrh extract, zinc chloride, citric acid
salicvιateBetadineΘ Mouthwash/Gargle Alcohol 8.8% Povidone-iodine 0.5%, glycerin, sodium
saccharin, flavor
Bioteneo Mouthwash Lysozyme (6 mg), lactoferrin (6mg) glucose oxidase (4000units)
Water, xylitol, hydrogenated Starch, propylθneglycol, hydroxyethylcellulose, aloe vera, naturaΙpeppermint, ρoloxamer 407, calcium lactate, zincgluconate, sodium benzoate, benzoic acid
Cepacolo Mouthwash/Gargle Alcohol 14%, cetylpyridiniumchloride 0.05%
EDTA disodium, color, flavor, glycerin,polysorbate 80, saccharin, sodium biphosphate,sodium phosphate, νvater, gluten free,dieteticallv sucrose free
cepacolΘ Mouthwash/Gargle(mint)
Alcohol 1 4.5%, cΘtylpyridinιumchloride 0.5%
Color, flavor, glucono delta-lactone, glycerin,poloxamer 407, sodium saccharin, sodiumgluconate, \Λ/ater, gluten free, dieteticallysucrose free
Dr. Tichenor'so Antiseptic Liquid SDA alcohol 38B 7oΥo Oil of peppermint, extract of arnica, \ivater, dyefree. qluten free
ListerineΘ- Liquid Alcohol 26.9%, eucalyptol0.092%, thymol 0.064%,methyl saliοylate 0.06%,menthol O.O42"/"
Benzoic acid, poloxamer 407, caramel, water,sodium benzoate
ListerineΘ- Lιquid(freshburst, cool mint)
Alcohol 21 .6%, eucalyptol0.092γ", thymol 0.064%'methyl salicylate 0.06%,menthol o.o42"λ
Water, sorbitol solution, poloxamer 4O7, benzoicacid, flavor, sodium saccharin, sodium citrate,citric acid, FD&C green #3, D&C yellow #10(freshburst)
MentadentΘ Mouthwash(οoo| mint, fresh mint)
Alcohol 10% νvater, Sorbitol, sodium bicarbonate, hydrogenperoxide, poloxamer 407, sodium lauryl sulfate,flavor, polysorbate 20, methyl salicylate (coolmint), sodium sacοharin, phosphoric acid, blue#1 , yellow #5 (cool mint)
Plaxo Advanced Formula(mint sensation)
Alcohol 8.7% Water, sorbitol solution, tetrasodiumpyrophosphate, benzoic acid, tlavor, poloxamer407, sodium benzoate, sodium lauryl sulfate,sodium saccharin, xanthan gum, FD&C blue #1
Plax@ Advanced Formula(original, SoftMlNT)
Alcohol 8.7% Sodium lauryl sulfate, water, sorbitol solution,sodium benzoate, tetrasodium pyrophosphate,benzoic acid, poloxamer 407, sodium saccharin,ftavor (SoftMlNτ), xanthan gum (SoftMlNT),flavor enhancer (SoftMlNT), FD&C blue #1(SoftMlNT), FD&C yellow #5 (SoftMlNT)
S.T. 37Θ Solution Hexylresorcinol 0.1% Glycerin, propylene glycol, citric acid, EDTAdisodium. sodium bisulfite. sodium citrate
Scopeo Baking Soda SD alcohol 38F 9.9olo,cetylpyridinium chloride,domiphen bromide
Sorbitol, sodium bicarbonate, sodium saccharin,flavor
Scopeo(cool peppermint)
SD alcohol 38F 14%,cetylpyridinium chloride,domiphen bromide
Purified water, glycerin, poloxamer 407, sodiumsaccharin, sodium benzoate, N-ethylmethylcarboxamide, benzoic acid, FD&Cblue #1, flavor
TargonΘ Smokers' Mouthwash(clean taste)
SDA alcohol 388 15.6% Water, glycerin, polyoxyl 40 hydrogenated casteroil, sodium lauryl sulfate, dibasic sodiumphosphate, benzoic aοid, sodium saccharin,caramel powder, dietetically sucrose free
TargonΘ Smokers' Mouthwash(original)
SDA alcohol 388 16% Water, sodium saccharin, sodium benzoate,glycerin, sodium lauryl sulfate, FD&C green #3,FD&C yellow #5, polyoxyl 40 hydrogenatedcastor oil, dietetically sucrose free
Tom's of Maineo Natural Mouthwash(cinnamon, original)
Menthol ν1/ater, glyοerin, aloe vera juice' witch hazel,poloxamer 335, spearmint oil, ascorbic acid,alcoho! free
Viadent@ Oral Rinse Alcohol 10% Sanguinaria extract, gιycerin, polysorbate 80,flavor, sodium saccharin, poloxamer 237, citricacid, zinc chloride 0.2%
-carries American Dental Αssociation (ADA) seal indicating safety and efficacy.Note: sD alcohol refers to "sρecially denatured" alcohol.
Αdapted with permission from Nonprescription Products: Formulations & Features, companion to the Handbook of Nonprescriρtion Drugs,11th ed, Washington, Dc, AmericanPharmaceutical Association,'1 998, 341-2.
133

APPENDIX
PREScRIPτIoN \MRITING
Doctor's NameAddress
Phone Number
Patient's Name/Date
Patient's Address/Age
RxDrug Name/Dosage Size
Disp: Number of tablets, caρsules, ounces to be dispensed (roman numerals added aS precaution for abused drugs)
Sig: Direction on how drug is to be taken
Doctor's signature
State license number
DEΑ number (if required)
PRESCRIPTTON REQUIREMENTS1. Date
2. Full name and address of patient
3. Name and address of prescriber
4. Signature of prescriber
lf Class ll drug, Drug Enforcement Agency (DEA) number necessary.
lf Class ll and Class lll narcotic, a triplicate prescription form (in the state of california) is necessary and it must be handνvritten by the prescriber.
ABBREVIATIONS COMMONLY USED tN MEDICAL ORDERS
Abb.eviation From Meanino
each ear
134
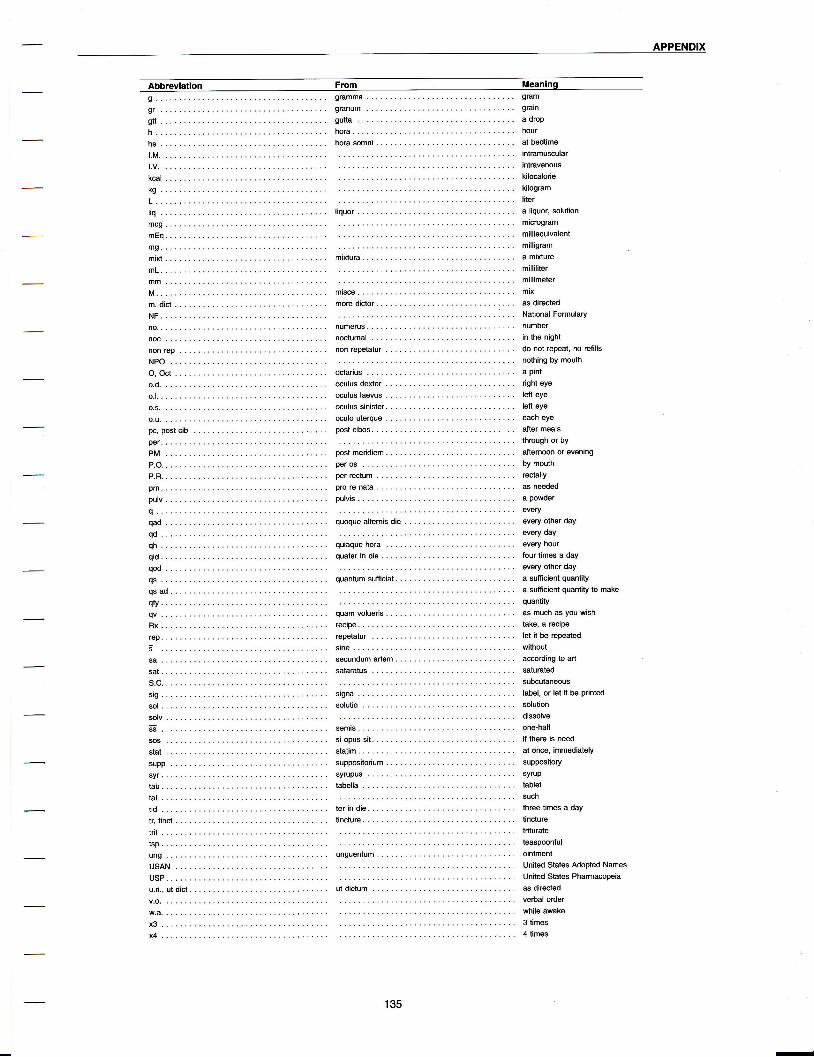
APPENDlX
Abbreviation Faom Meaninq
h.hs
t.M
t.v
ung
USANUSP.
intramusularintravenous
kcal..... " kilocalorie
kg ... . .. .. ... . kilogram
L....... ...... liter
liq...... ...... liquor aliquor,solution
mcg..... ...... microgram
mEq..... ...... milliequivalent
mg...... ...... milligram
mixt..... ...... mixtura. ........ amixture
mL " " milliliter
mm..... ...... millimeter
NF...... ...... NationalFormulary
no....... ..... numerus. ...... number
noc..... ..... nocturnal ...... inthenight
nonrep.. ..... nonrepetatur. .. donotreρeat,norefiιlsNPOO, Octo.d.
o.l. . .
o.s.
oculuslaevus .... lefteye
oculussinister. ... lefιeye
o.u...,.. ....,. oculouteηue.. eacheyepc,postcib .... postcibos. ...... aftermeals
ρer...... ..... throughorby
PM..... ....,. postmeridiem. ... atternoonorevening
P.O...... ...... peros ........ bymouth
P.R...... ...... perrectum ...... rectally
ρrn.....' ...... prorenata... ... asneeded
ρulv,.... ...... pulvis .. aρowder
q .. . .. . . ... ... every
qad..... ...... quoquealternisdie
qd......qh...... ...-.. quiaquehora
qs...... ..... quantumsutficiat.
qsad....
quam volueris
recipe......reρetatur . . .
si opus sit.statim....suppositorium
syrupus . .
tabella . . .
every other day
θvery day
every hour
four times a day
every other day
a sutticient quantity
a sutticient quantity to make
quantity
as much as you wish
take, a reciρe
let it be repeated
without
aΦrding to art
saturated
subcutaneous
label, or let it be printed
solution
dissolve
one-half
if there is need
at once, immediately
supρository
syrup
tablet
such
three times a day
tincture
triturate
teaspΦnfuIointment
United States Adopted Names
United States PharmacopΘia
as directed
stne.....sΦundumarlem....
tid...... ...... terindielr.ιinct... ...... tincture.
u.d..utdict. ..... utdictum
135
-

APPENDIX
SAFE WRITING PRACTICESHealth professionals and their support personnel τ. o.D. is not a safe abbreviation for once daily,frequently produce handwritten copies of information as it is properly interpreted as meaning ,,right
they see in print; therefore, such information is eye" and has οaused liquid medications suchsubjected to even greater possibilities for error or misin- as saturated solution of potassium iodide andterpretation on the part of others. Thus, particular care Lugol's solution to be administered incorrectly.must be given to how drug names and strengths are There is no safe abbreviation for once daily. ltexpressed when creating written healthcare documents. must be written out in full.
Τhe following are a few examples of safe writing rules 8' Do not USe chemical names such as 6-
suggested oy tne lnstitute for Safe Medication Prac- mercaptopurine or 6-thioguaninΘ, as sixfold
tices, lnc.* overdoses have been given when these werenot recognized as chemical names. The proper
1. There should be a space between a number and names of these drugs are mercaptopurine orits units as it is easier to read. Τhere should be thioguanine.no periods after the abbreviations mg or mL' g. Do not abbreviate drug names (sFc, 6Mp, 5-
correct ]ncorrect ASA, MTX, HcτΖ' cPz' PBz' etc) as they are'10 mg 10mg misinterpreted and cause error.100 mg 100ms
10. Do not use the apothecary system or symbols.
2. Never place a decimal and a zero after a whole 11. Do not abbreviate microgram as μg; insteadnumber (2 mg is correct and 2.0 mg is use mcg as there is less likelihood of
incorrect). lf the decimal point is not seen misinterpretation'
because it falls on a line or because individuals 12. When writing an outpatient prescription, write aare working from copies where the decimal complete prescription. A complete prescriptionpoint is not seen, this causes a tenfold can prevent the prescriber, the pharmacist,
overdose. and/or the patient from making a mistake andcan eliminate the need for further clarification.
3. Just the opposite is true for numbers less than The legible prescriptions should contain:
one. Always place a zero before a naked a. patient's full namedecimal (0'5 mL is correct' '5 mL is incorrect)'
b. for pediatric or geriatric patients: their age (or
4. Never abbreviate the word unit. The weight where applicable)handwritten U or u, looks like a 0 (zero), and c. drug name, dosage form and strength; if amay cause a tenfold overdose error to be drug is neγv or rarely prescribed, print thismade. information
5. lU is not a safe abbreviation for international d. number or amount to be dispensed
units. The handwritten lU looks like lV. Write e. complete instructions for the patient,out international units or use int. units. including the purpose of the medication
6. e.D. is not a safe abbreviation for once daily, f. when there are recognized contraindications
as when the Q is followed by a sloppy dot, it for a prescribed drug, indicate to the
looks like QlD which means four times daiΙv. pharmacist that you are aware of this fact (ie,when prescribing a potassium salt for apatient receiving an ACE inhibitor, write "Kserum leveling being monitored")
*From "Safe Writing" by Davis NM, PharmD and cohen MR, MS, Lecturers and consultants for Safe Medication Practices, 1143 \Ιr'right Drive,Huntington Valley, PA 19006. Phone: (215) 947-7566-
136

APPENDlX
INSURANCE coDING FoR THE PERIoDoNTAL PAτIENT
Dealing with insurance is one of the most perplexing and sometimes frustrating aspects of clinical practice.While the patient's insurance plan is, in actuality, an agreement between the patient and his employer, manypatients lose sight of this fact. Often, patients feel that the dentist has some say in the breadth and depth ofthe patient's coverage. Limitations in coverage due to eligibility; waiting periods; deductibles; copayments;yearly benefit maximums; calculation of the usual, customary, and reasonable (UCR) fee base; least expen-sive alternative treatment (LEAT); least expensive, professionally acceptable alternative treatment (LΕPAAT),and preexisting conditions may all play a role in the patient's ultimate coverage. lt is important for thepractitioner and office staff to understand the true nature of this relationship and be ready to assist patients in
understanding this as well. At no time should a practitioner knowingly falsify any insurance claim or use aninappropriate code in order to gain additional benefits for the patient. This may lead to a charge of insurancefraud against the practitioner, not the patient.
Sometimes patients will only agree to treatment that is covered by insurance. While this is their right, it is thepractitioner's obligation to treat the patient, not the patient's insurance plan. A comprehensive treatment planwith sound alternatives covering the patient's dental needs must be presented to the patient with the patientdetermining the course of action. Obtaining a predetermination of dental benefits from the insurance carriermay be of some help to the patient in making treatment decisions. lnsurance carriers often request copies ofperiodontal charting and radiographs in order to make payment or predetermination decisions. Maintaining arecord of what supporting documentation an insurance plan requires when a claim or predeterminationrequest is sent in may expedite payment or a response.
INSURANCE CODES OF PERIODONTAL IMPORTANCE
Adapted and used with permission from lhe Code on Dental Procedures and NomencΙature (CDT-3) availablefrom the Αmerican Dental Association and Current Procedural Terminology for Periodontics and lnsuranceReporting Manual available from the American Academy of Periodontology. Commentary following each codeis of a general nature. lt is incumbent upon each clinician and/or office personnel to be apprised of detailsrelated to specific insurance plans.
CLINICAL ORAL EVALUATION
D0120
D0140
D0150
Periodic oral examination: Completed on a patient of record at a specified interval. Additional diagnostic proceduresare reported separately.Limited oral evaluation - problem focused: Used when a patient has been referred for a specific problem orpresents with an emergency, trauma, infection, or other unusual circumstance.Comprehensive oral evaluation: This includes medical and dental histories, hard and soft tissue examinations,caries exam, periodontal charting, occlusal analysis, and oral cancer screening.
RADIOGRAPHS/DIAGNOSTIC IMAGING
D0210
D0220D0230D0240D0250D0260D0270D0272D0274
lntraoral - complete series (including bitewings): Vertical bitewings preferred for a patient \ivith periodontal disease(author's note)lntraoral: Periapical first filmlntraoral: Periapical each additional filmIntraoral: Occlusal filmExtraoral: First filmExtraoral: Each additional filmBitewing: Single filmBitewings: 2 filmsBitewings: 4 films
τEsτS AND LABoRAToRY ExAMINAτloNs
D0415 Bacteriologic studies for detΘrmination of pathologic agents: May include culture and sensitivity, DNA probeanalysis, and tests for susceptibility to periodonta| disease. Microbial testing may be payable under thΘ patient'smedical coverage.Pulp vitality testsDiagnostic casts
D0460DO470
137
-

APPENDIX
INSURANCE coDING FoR TΗE PERIODONTAL PATIENT (Continued)
PREvΕNTlvE
D1 110 Prophylaxis - adult: lncludes scaling and polishing of supragingival areas. This code may also be used if tνvo visitsare necessary for the completion of the prophy|axis due to thθ heaviness of the tooth accumulated materials. A shodnarrative should accompany the second submission detailing the reason for the extra time needed to complete theprocedure.
D1 120 Prophylaxis - childD12O4 Topical application of fluoride (prophylaxis not included) - adultD'l205 Topical application of fluoride (including prophylaxis) - adultD'l310 Nutritional counseling for control of dental diseaseD1320 τobacco counseling for the control and prevention of oral diseasΘD1330 Oral hygiene instructions
ENDODONTICS
D3450 Root amputation - per root: Τhis procedure leaves the cro\Λ/n of the tooth intact.D3920 Hemisection (including any root removal), not including root canal therapy: This entails the separation of the
crown of the tooth. May or may not retain all of the tooth sections
SURGICAL SERVICES-*See appropriate sections in the manual for procedure indications and descriptions.
SURGIcAL sERvlcEs (INcLUDING USUAL PosτoPERAτlvE cARE)
D4210 Gingivectomy or gingivoplasty - per quadrantD4211 Gingivectomy or gingivopiasty - per toothD4220 Gingival curettage, surgicaΙ - per quadrant, by report: This is a detinitive surgical procedure requiring a short
narrative explanation for the rationale for use. code D4341 should not be reported with D4220. τhis procedure is notthought to be any more beneficial than scaling and root planing in the treatment of periodontitis so it may not bebenefited.
D424O Gingival flap procedure, including root planing - per quadrant: This code may be used as the flap entry for a -regenerative procedure (combined with D4263, D4264, and/or D4266 or D4267).
D4245 Apically positioned flapD4249 Clinica! crourn lengthening - hard tissue: Used to increase the clinical crown and is performed in a healthy
environment. This may require submission of a radiograph and a short narrative.D4260 Osseous surgery (including flap entry and closure) - per quadrant: Performed in the presence of periodontal
disease to treat osseous defects. This procedure may require documentation including charting and possiblyradiographs of the area.
D4263 Bone replacement graft - first site in quadrant: Does not include flap access or cΙosure. Can be applied toautogenous, allograft, and alloplast materials.
D4264 Bone replacement graft - each additional site in quadrantD4266 Guided tissue regeneration - resorbable barrier, per site: Does not include flap access or closure.D4267 Guided tissue regeneration - nonresorbable barrier, per site (includes membrane removal)D4268 Surgical revision procedure, per tooth: Used to refine the results of the previousΙy described procedures.D4270 Pedicle soft tissue graft procedureD4271 Free soft tissue graft procedure (including donor site surgery): one code and fee should be used for one or t\Λ/o
adiacent teeth. Documentation should include the amount of recession, amount of remaining gingiva, influence of thefrenum (if applicable), and thΘ presence of inflammation.
D4273 Subepithelial connective tissue graft procedure (includes donor site surgery): This procedure should be codedfor each tooth that receives a graft.
D4274 Distal or proximal wedge procedure (when not performed in conjunction urith surgical procedures in the sameanatomic area)
NONSURGICAL PERIODONTAL SERVICE
D4320 Provisional splinting - intracoronal: lnterim stabilization for mobile teeth. ldentify the teeth involved and the natureof the spιint.
D4321 Provisional splinting - extracoronalD4341 Periodontal scaling and root planing, per quadrant: Used as a therapeutic, not prophylactic procedure. Usually,
only one or t\,,vo quadrants may be submitted on the same day of serviοe. Under special circumstances (ie, medicalconsiderations), this benefit may be extended to cover three or four quadrants treated at one visit. Many plans ask forcurrent periodontal charting, and possibly radiographs for an estimate of benefits to be completed.
D4355 Full mouth debridement to enable comprehensive periodontal evaluation and diagnosis: τhis procedure may beused to remove plaque and calculus in order to complete the periodontal examination. This procedure should not beinterpreted as comprehensive therapy.
138

APPENDTX
D4381 Localized delivery of chemotherapeutic agents via a controlled release vehicle into diseased crevicular tissue,per tooth, by report: This procedure does not replace conventional or surgical therapy required for debridement,resective procedures, or regenerative therapy. Τhis code is used for any of the locally delivered agents'
OTHER PERIODONTAL SERVICES
D491o Periodontal maintenance procedures (fol]ouring active therapy): lncludes a reviΘ\λ/ of the medical history' plaquecontrol evaluation, scaling, and polishing. Τhis is done after the completion of active therapy and is not synonymouswith prophylaxis. There may be a 3-month waiting period after the completion of active therapy for some plans beforelhis benefit \,vill take effect.
D4920 Unscheduled dressing change (by someone other than treating dentist)D4999 Unspecified periodontal procedure, by report
IMPLANτ sERvlcEs
D6010 Surgical placement of implant body: Endosteal implant: lncludes second stage surgery and placement of healingcap.
D6020 Abutment placement or substitution: Endosteal implantD6080 lmplant maintenance procedures, including removal of prosthesis, cleansing of prosthesis and abutments,
and reinsertion of prosthesis: lncludes prophylaxis of implant system.D6o9o Repair implant suppoπed prosthesis, by reportD6095 Repair implant abutment, by reportD6100 lmplant removal, by reportD6199 Unspecified implant procedure, by report
OTHER SURGICAL SERVICES
D7280 Surgical exposure of impacted or unerupted tooth for orthodontic reasons (including orthodonticattachments)
D7281 Surgical exposure of impacted or unerupted tooth to aid eruptionD7285 Biopsy of oral tissue: Hard, (bone, tooth)D7286 Biopsy of oral tissue: Soft (all others)D7291 Transseptal fiberotomy, by reportD732O Alveoloplasty, not in coniunction urith extractions, per quadrantD734O Vestibuloplasty: Ridgeextension (secondaryepithelialization)
SURGICAL INCISION
D7510 lncision and drainage of abscess: lntraoral soft tissueD7520 lncision and drainage of abscess: Εxtraoral Soft lissueD7530 Removal of foreign body, skin' or subcutaneous alveoιar tissueD754O Removal of reaction producing foreign bodies, musculoskeletal systemD7550 Sequestrectomy for osteomyelitis
oτHER REPAIR PRoCEDUREs
D7960 Frenulectomy (freneοtomy or frenotomy): Separate procedureD7970 Excislon of hyperplastic tissue: Per archD7971 Excision of pericoronal gingiva
MISCELLANEOUS SERVICES
D91 10 Palliative (emergency) treatment of dental pain - minor procedure: Reported on a per visit basis for emergencylreatment of dental pain.
D9230 Analgesia, anxiolysis, inhalation of nitrous oxideD9248 Nonintravenous conscious sedationD9310 Consultation (diagnostic service provided by dentist or physician other than practitioner providing treatment)D9410 House/extended care facility callD9910 AppΙicationofdesensitizingmedicamentD991 1 Application of desensitizing resin for cervical and/or root surface, per toothD9920 Behavior management, by report
139

APPENDIX
INSURANCE coDlNG FoR THE PERIODONTAL PATIΕNT (Continued)
D9930 Treatment of complications (postsurgical) - unusual circumstances, by reportD9940 Occlusal guard, by reportD9951 Occlusal adiustment: LimitedD9952 Occlusal adiustment: CompleteD9971 odontoplasty 1-2 teeth; includes rΘmoval of enamel proiectionD9999 Unspecified adiunctive procedure, by report
**NOTE:
Related procedures may be grouped together lvith the benefit being limited to the most inclusive procedure. Thismay be true for the various steps involved in osseous surgery (incisions, flap, cleanout, scaling, ostectomy/osteoplasty, flap apposition, and suturing). Any regenerative procedures done in conjunction with this (guidedtissue regeneration, bone replacement graft) would be considered additional procedures to the flap operationitseif, even when performed in the same area at the same time.
There are a number of procedures where it would be inappropriate to repoft both services on the same treatmentdate. Among those combinations that should not be reported together are:
D4341 and D4220 on the same day
D4355 and D0150 on the same day. The patient should be allowed to heal and the gingival edema toresolve before completing the periodontal examination. This will allow for more accurate probe measure-ments.
D4381 and D4341 Ιor the same teeth on the same day of Service. While the tooth to receive the locallydelivered antibiotic may be scaled before placement of the medication, definitive scaling should have beencompleted at a previous appointment.
D4249 and D4260 for the same teeth on the same day of service. The clinical crown Ιengthening isperformed in a healthy environment and the osseous Surgery peι'formed where disease has been present.
Τhe American Αcademy of Periodontology has published a checklist for filing dental δlaims:
1. ls the form typed or printed legibly so that third party personnel can read and process the informationprovided?
2. Are the "patient" and "dentist" sections completed accurately and completely, including employee identifica-tion numbers, dates of birth, and information on the spouse for coordination of benefits?
3. Has the diagnosis been noted on the claim form? (Use the AAP disease classification found in Chapler 4 onpage 31.)
4. Have all procedures been identified by ADA codes and properly related to dates of services and fees?5. Have the treatment areas and/or missing teeth been identified on the tooth chart?6. Ηave "by report'' procedures and unusual services been noted in Section 61 on the claim form or described in
more detail on a separate sheet?7. Has notation been made regarding specialty status, if any?8. Has the patient signed and dated the claim form, or has a valid authorization/assignment form been signed by
the patient and has this been noted in the appropriate places as "signature on file?"9. Has the insured person signed the form in the appropriate space in order for benefits to be paid directly to the
dentist if so desired (assignment of benefits)?10. Has notation been made regarding prior (financial) agreement with the patient?11. Has the form been signed and dated by the dentist?12. Has a copy been filed in the office records?
Much of the paperwork involved with submitting insurance information has been eliminated by the use ofelectronic filing. ln this way, the dental office may submit a paperless claim as soon as it is generated by the officebusiness software program to a clearinghouse for checking for completeness and then forwarded to the appro-priate carrier. This decreases the busywork involved and often leads to more rapid return of a predeterminationdecision and payout by the 3rd party carrier.
SELEcτED READINGS
Code on Dental Procedures and Nomenclature, CDT-3, Chicago, lL: American Dental Association, 1999.
Current Procedural TerminoΙogy for Periodontics and lnsurance Reporting Manual, CΛΙcago, lL: Ameriοan Academy of Periodontology, 20ο0
140
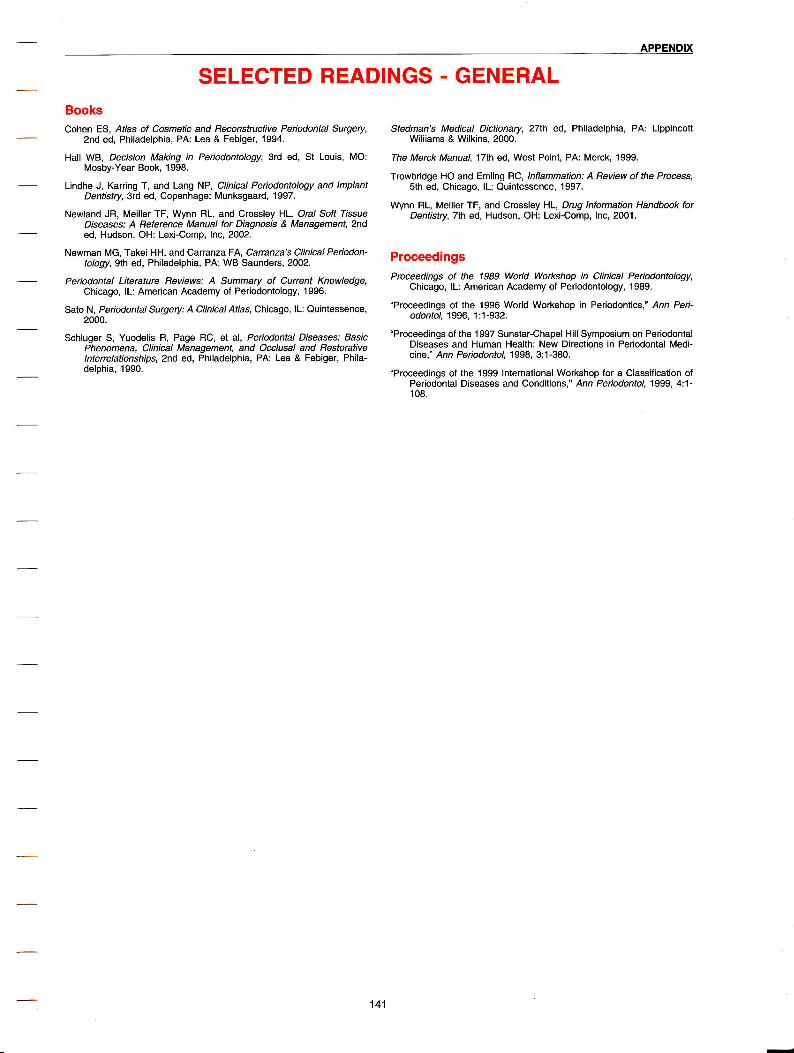
APPENDTX
SELECTED READINGS - GENERALBooksCohen ES, Atlas of Cosmetic and Reconstructive Peiodontal Surgery,
2nd ed, Philadelphia, PA: Lea & Febiger, 1994.
Hall WB, Decision Making in Periodontology, 3rd ed, St Louis, MO:Mosby-Year Book, 1998.
Lindhe J, Karring T, and Lang NP' Clinical PeriodontoΙogy and ImplantDentistry, 3rd ed, Copenhage: Munksgaard, 1997.
Ne\Λ/land JR, Meiller TF, Wynn RL, and crossley HL' oral Soft TissueDiseases: A Reference ManuaΙ for Diagnosis & Management,2nded, Hudson, OH: Lexi-Comp, lnc,2OO2-
Ne\Λrman MG, τakei HΗ, and CarranzaFA, carranza'S Clinical Periodon-tology,glh ed, Philadelρhia, PA: WB Saunders' 2002'
Periodontal Literature Reviews: A Summary of Current ΚnowΙedge,Chicago, lL: American Academy of Periodontology, 1996.
Sato N, Perlodontal Surgery: A Clinical Atlas, Chicago, lL: Quintessence,2000.
Schluger S, Yuodelis R, Page RC, et al, Periodontal Diseases: BasicPhenomena, Clinical Management, and Occlusal and BestorativeιnterreΙationships, 2nd ed, Phi|adeιphia, PA: Lea & Febiger, Phila-delphia, 1990.
Stedman's Medical Dictionary, 27th ed, Philadelphia, PA: LippincoltWiliiams & Wilkins, 2000.
The Merck Manual, 17th ed, West Point, PA: Merck, 1999.
τroνvbridge Ho and Emling Rc, lnfιammation: A Beview of the Process,sth ed, Chicago, lL; Quintessence, 1997.
Wynn RL, Meiller TF, and Crossley HL' Drug ιnformation Handbook forDentistry, Tth ed, Hudson, OH: Lexi-Comp, lnc, 2001.
ProceedingsProceedings of the 1989 World Workshop in Clinical Periodontology,
Chicago, lL: American Academy of Periodontoιogy, 1989.
"Proοeedings of the 1996 World Workshop in Periodontics," Ann Peri-odontoΙ' 1 996' 1 :1 -932.
"Proceedings of the 1 997 Sunstar-Chapel Hill Symposium on PeriodontalDiseases and Human Health: Neι,v Directions in Periodontaι Medi-cine," Ann Periodontol, 1998, 3:1-380.
"Proceedings of the 1999 lnternational Workshop for a Classification ofPeriodontal Diseases and Conditions," Ann Periodontol 1999, 4:1-1 08.
141

APPENDIX
SELECTED READINGS . SPECIFICCHAPTER 1: Problem-Based PeriodontalDiagnosis and Disease ManagementArmitage G, "DevelopmΘnt oJ a Classification System 1or Periodontal
Diseases and Conditions," Ann Periodontol, 1 999, 4(1 ):1 -6.
Dorlands's ΙtΙustrated Medicat Dictionary,23'd ed, Philadelphia, PA: WBSaunders Co., 1957.
Goodson JM, τanner Αc, Haffajee ΑD, "Pafterns of Progression andRegression of Αdvanced Destructive Periodontal Disease,'' J c/,nP e ridonto Ι, 1 9a2' 9 :47 2-81'
Haffajee AD, socransky Ss, and Goοdson JM, "comparison of DifferentData Analysis Ιor Detecting Changes in Attachment Leνel,'' J clinPeiodontoΙ, 1 983, 1 0:298_31 0.
Kornman K, Ne\,vman MG, Alvarado R, et al, "Clinical and MicrobiologicPatterns of Adults With Periodontitis," J Periodontol 1991, 62:634-42.
Neν\,man MG, "lmproved clinical Deοision Making Using the Εvidence-Based Approach," Ann Peiodontol 1996, 1(1):i-ix.
Socransky Ss, Haffajee ΑD, Goodson JM, et al, "New Concepts ofDestructive Periodontal Disease," J Clin Peridontol, 1984, 11:21-32.
The American Academy of Periodontology, Preceedings of the WorldWorkshop in Clinical Periodontics, Chicago, lL: American Academyof Periodontology, 1989.
The American Academy of Periodontology' τhe Parameters of care,Chicago, lL: American Academy of Periodontology, 2OO1.
CHAPτER 2: Anatomy, HistoIogy, and PhysioIogyof the PeriodontiumBartold PM, Walsh LJ, and Narayanan AS, "Molecular and Cell Biology of
the Gingiva," PeridontoΙ 2000, 2ooo' 24i2a-55'
Beertsen W, Mcoulloch CA, and Sodek J, '"fhe Periodontal Ligament: AUnique, Multifunctional connectiνe τissue," Periodontol 2000' 1997'13:2O-4O.
Berkovitz BK, Moxham BJ, and Neγvman HN, Ihe Periodontal Ligamentin HeaΙth and Disease,2nd ed, St Louis' Mo: Mosby-\Λ/olfe' 1995.
Bosshardt DD and Selvig KA, "Dental cementum: Τhe Dynamic Tissuecovering of the Root," Periodontol 2000,1997, 13:41-75.
Cho Ml and Garant PR, "Development and General Structure of thePeriodontium," Peiodontol 2000, 20OO, 24(1):9-27 -
Gargiulo AW, Wentz FM, and Orban B, "Dimensions and Relations of theDentogingival Junction in Humans," J Periodontol, 1961, 32:261-7.
Hassell τM' '"Γissues and cells of the Periodontium,'' PeriodontoΙ 2000'1993,3:9-38.
Mariotti A, '"fhe Extracellular Matrix of the Periodontium: Dynamic andlnteraοtive τissues," Periodontol 2000, 1993' 3:39-63.
Nuki K and Hock J, '"Τhe organization of the Gingival vasculature," JPeriodontal Res, 1 974, 9(5):305-1 3.
Saffar JL, Lasfargues JJ, and Cherruau M, "Alveolar Bone and the Alve-olar Prοcess: The Socket That ls Never Stable,'' Periodontol 2000'1997, 13:76-90.
schroeder ΗE and Listgarten MA, '"The Gingival Tissues: The Architec-ture o{ Periodontal Protection," Periodontol 2000,1997, 13:91-120.
sodek J and McKee MD, "Molecular and Cell Bio|ogy of Αlveolar Bone,''Periodontoι 2oo0' 24(1 ):99-1 26.
stern lB, "current concepts of the Dentogingival Junction: τhe Epithelialand connective τissue Attachements tb the Tooth," J Peiodontol,1981, s2(9):465-76.
τen cate AR' oraι HistoΙow: Deνelopment, Structure, and Fυnction /A.R. τen Cate,41h ed, St Louis, Mo: Mosby, 1994.
OHAPτER 3: EtioIogy and cIassification of thePeriodontat DiseasesAldred MJ and Bartold PM, "Genetic Disorders of the Gingivae and
Periodontium," Periodontoι 20oo' 1998' 18:7-20.
Armitage Gc, "Development oΙ a Classification System for PeriodontalDiseases and Conditions," Ann Periodontol, 1 999, 4(1 ):1 -6.
Blieden τM, '"[ooth-Related lssues," Αnn Peiodontol, 1999, 4(1):91-7.
Brunsvold MA and Lane JJ, '"The Prevalence of Overhanging DentalRestorations and Their Relationship to Periodontal Disease," J C/rnP e riodontoΙ' 1 99o' 17 (2):67 -7 2'
Carnevale G, Sterrantino s, and DiFebo G' "Soft and Hard τissueHealing Follo\Λ/ing Tooth Preparation to the Alveolar crest," /nt JPeriodontics Restorative Denf,'l 983, 3(6):36-53.
Caton J, "Periodontal Diagnosis and Diagnostic Aids," Proceedings of the1989 World workshop in ClinicaΙ Peiodontics, chicago, lL: Amer-ican Academy of Periodontology, 1989, l-1-32.
chandler JA and Brudvik Js' "clinical Evaιuation of Patients Eight toNine Years After Placement of Removable Partial Dentures," J Pros-thet Dent, 1984, 51 (6):736-43.
Darueau RR, Tanner A, and Page RC, "The Microbial Challenge in Perio-dontitis," Periodontol 2000, 1997, 1 4:12-32.
Flemmig τF, "Periodontitis,'' Ann Periodontol, 1999' 4(1):32-8.
Friedman RB, Gunsolley J, Gentry A, et al, "Periodontal status of ΗlV-Seropositive and AIDS Patients," J Periodontol, 1991, 62(10):623-7.
Ηaber J and Kent RL, "cigarette Smoking in a Periodontal Practice," JPeriodontaι, 1 992, 63(2):1 00-6.
Ηaffajee A, Socransky s, Smith C, et al' "Microbial Risk lndicators forPeriodontal Attachment Loss," J Periodontal Res, 1991 , 26:292-6.
Hallmon WW, "occlusal Trauma: Effect and lmpaοt on the Periodon-tiυm,'' Ann Periodontol, 1999, 4(1):102-8.
Holmstrup P, "Nonplaque-lnduced Gingival Lesions," Ann Periodontol,1 999, 4(1 ):2ο-31 .
Holmstrup P and Westergaard J, "HlV lnfeοtion and PeriodontalDisease," Periodontoι 2o0o' 1998, 18:37-46.
"1999 lnternational Workshop {or a Classification of Periodontal Diseasesand conditions. Papers. oak Brook, lllinois, oοtober 3o-November2,1999,' Ann PeriodontoΙ, 1999' 4(1):i' 1-112.
Kay Η, "criteria for Restorative contours in the Altered Periodontal Envi-ronment,'' ιnt J Peiodontics Rest Dent,1984, 5(3):42-63.
Kinane DF, "Periodontitis Modified by Systemic Factors," Ann Peri-od ontoι, 1 999, 4(1 ):54 -64.
Kornman K, Crane A, Wang HY, et al, '"Γhe lnterleukin-1 Genotype As aSeverity Factor in Adult Periodontal Disease," J cΙin Periodontoι,1997 , 24(1)i72-7.
Lalla E, Lamster lB, Drury S, et al, "Hyperglycemia, Glycoxidation andReceptor for Αdvanced Glycalion Endproducts: Potential Mecha-nisms Underlying Diabetic Complications, lncluding Diabetes-Asso-ciated Periodontitls,'' Periodontoι 2oo0' 2oo0' 23:5o-62.
Listgarlen MA, "Structure of the Microbial Flora Associated With Perio-dontal Health and Disease in Man. Α Light and Electron MicroscopicStudy," J Periodontol, 1976, 47(1):1-18.
Loe H, Theilade E, and Jensen S, "Experimenlal Gingivitis in Man," JP e riodontol, 1 965, 36:1 77 -87.
Mariotti A, "Dental Plaque-lnduced Gingival Diseases," Ann Periodontol,1999,4(1):7-19.
Mealey B, PeiodontaΙ Medicine, Rose L, Genco R, cohen DW, et al,eds, Hamilton, Ontario, Canada: BC Decker lnc, 2000, Chapter I,121-5ο.
Meng ΗX, "Periodontal Αbscess,'' Ann Periodontoι, 1 999, 4(1 ):79-83.
Meng HX, "Periodontiο-Endodontic Lesions,'' Ann Periodonιo1 1999'4(1 ):84-90.
Νovak MJ, "Necrotizing Ulcerative Periodontitis"' Ann Periodontol, 1999,4(1):74-8.
αomo-corgel J and Steinberg B, "Periodontal Management and theFemale Patient," Periodontal Medicine, Rose L, Genco R, CohenDW, et al, eds, Hamilton, Ontario, Canada: BC Decker lnc, 2000,chaρter 9, 151-66.
142

APPENDIX
Pack AR, Coxhead LJ, and McDona|d BW, "Periodontal Management oΙOverhanging Margins in Posterior Amalgam Restorations and Perio-dontal consequences," J clin Periodontoι, 1990, 17(13):145-52'
Papapanou PN, "Periodontal Diseases: Epidemiology," Ann Periodontol,1996,1(1):1-36.
Pini Prato GP, "Mucogingival Deformities," Ann Periodontol 1999,4(1 ):98-1 01 .
Preber H and Bergstrom J, "EΙfect of cigarette Smoking on PeriodontalHealing Following Surgical τherapy,'' J cιin Periodonfol 1990'17(5)t324-8.
Preber H and Bergstrom J,'"τhe Effect of Nonsurgical τherapy on Perio-dontal Pockets in Smokers and Nonsmokers," J CIin Periodontol,1 986, 1 3(4):31 9-23.
RamS T, ''Γhreshold Values," oMTS Newsletter' 1993' 2(2). oral Microbi-ology Testing Service, Medical College of Pennsylvania.
Rees TD, "Drugs and Oral Disorders," Periodontol 2000, 1998, 18:21-36.
Rees T, "Periodontal Management ol the Patient With Diabetes Mellitus,"Periotontol 2000, 2O0O, 23(1):63-72.
Rowland RW, "Necrotizing Ulcerative Gingivitis," Ann Periodontoι, 1999,4(1 ):65-73.
Scully C and Laskaris G, "Mucocutaneous Disorders," Periodontol 2000,1998,18:81-94.
Ten cate AR, oraΙ Histology: Deveιopment, Structure, and Function /A.R. Ten Cate,4h ed, St Louis, MO: Mosby, 1994.
Theilade Ε, \,γright WH, Jensen SB, et al, "Experimental Gingivitis inMan. ll. A Longitudinal Clinical and Bacteriological lnvestigation," JPeriodontal Fes, 1966, 1:1-13.
Tonetti MS and Mombelli A, "Early-onset Periodontitis," Ann PeriodontoΙ'1 999, 4(1 ):39-53.
zambon JJ, Grossi SG, Maοhtei EΕ, et al, "Cigarette Smoking lncreasesthe Risk of Subgingival lnfection Vyith Periodontal Pathogens," JPeriodontol, 1 996, 67(10 Suppl):1050-4.
Zambon JJ, "Periodontal Diseases: Microbial Factors," Ann Periodontol,1 996, 1 (1 ):879-925.
CHAPTER 4: Clinical Assessment, Diagnosis, andTreatment PlanningAeppli DM, Boen JR, and Bandt CL, "Measuring and lnterpreting
lncreases in Probing Depth and Attachment LoSs," J Periodontoι,1 985, s6(5):262-4.
American Academy of Periodontology. The Parameters of Care,Chicago, lL: Αmerican Aοademy of Periodontology, 2001.
American Academy of Periodontology. chemicaι Agents for Control ofPlaque and Gingivfflb, Chicago, lL: Αmerican Αcademy of Periodon-tology,1994.
Armitage Gc, "Development of a Classification System for PeriodontaΙDiseases and Conditions," Ann Periodontol, 1999, 4(1):1-5.
Armitage Gc, "οlinical EvaΙuation of Periodontal Diseases," Periodontol2000, 1995, 7:39-53.
Atassi F, Nel,vman ΗN, and Bulman JS, "Probe Tine Diameter andProbing Depth,'' J cιin PerΙodontoΙ' 1992, 19(5):301-4.
Beck JD, Koch GG, Zambon JJ, et al, "Evaluation of Oral Bacteria asRiSk lndicators for Periodontitis in older Adults"' J Periodontoι,1 992, 63(2):93-9.
Greenstein G, Polson A, lker H, et al, "AssociaΙions Betνveen crestalLamina Dura and Periodontal status," J Periodontoι' 1981
'52(7):362-6.
Jeffcoat MK, Wang lC, and Reddy MS, "Radiographic Diagnosis in Perio-dontiοS,'' Periodontol 2000, 1995, 7:54-68.
Kennedy JE, Bird WC, Palcanis KG, et al, "A Longitudinal Evaιuation ofvarying Widths of Attached Gingiva,'' J CΙin Periodonιol 1985,12(8)i667-75.
Kornman K and Wilson T, '"τhe Presumptive Diagnosis and Diagnosti-cally Driven Therapy," Fundamentals in PerΙodontics, Chicago, lL:Quintessence Publishing Company lnc, 1996, Chapter 16, 293-317.
Lamster lB and Grbic JΤ, "Diagnosis of Periodontal Disease Based onAnalysis of the Host Response," Periodontol 2000,1995, 7:83-99.
Lindhe J, Socransky SS, Nyman S, et al, "Critical Probing Depths inPeriodontal τherapy," J CΙin PeriodontoΙ' 1982, 9(4):323-6.
Listgarten MA, "Periodontal Probing: What Does lt Mean?" J Clin Peri-odontoι, 1980, 7(3):1 65-76.
Listgarten MA, Mao R, and Robinson PJ, "Periodontal Probing and theRelationship oΙ the Probe Tip to Periodontal τissues,'' J Periodontol,1 976, 47(9):51 1 -3.
McGuire MK, "Prognosis versus Actuaι outcome: A Long-Term Surveyof 100 τreated Periodontal Patients Under Maintenance Care,'' JPeriodontoι, 1991, 62(1 ):51-8.
McGuire MK and Nunn ME, "Prognosis Versus Actual outcome. ll' ΤheEffectiveness of clinical Parameters in Developing an AοcurateDiagnosis," J PeriodontoΙ, 1996, 67(7):658-65'
McGuire MK and Nunn ME, "Prognosis Versus Αctual outcome. lll. τheEffectiveness o{ Clinical Parameters in Accurately Predicting ToothSurvival," J Periodontol, 1 996, 67(7):666-74.
Papapanou PΝ and Tonetti MS, "Diagnosis and Epidemiology of Perio-dontal Osseous Lesions," Periodontol 2000, 20OO, 22(1):8-21.
Perlitsh M, "Periodontal Risk Assessment, Diagnosis and TreatmentPlanning," Dent CΙin North Am, 1980' 24(2):177-93.
Pihlstrom BL, "Periodontal Risk Αssessment, Diagnosis and τreatmentPlanning," Periodontol 2000, 2001, 25i37 -58.
Scannapieco FΑ, "Position Paper of the American Academy of Periodon-tology: Periodontal Disease As a Potential Risk Factor for SystemicDisease," J Periodontol, 1998, 69(7):841-50.
νvang HL, Burgett FG, shyr Y, et al, '"τhe lnfluence of Molar Furcalionlnvolvement and Mobility on Future clinicaΙ Periodontal AttachmentLoss,'' J PeiodontoΙ, 1 994, 65(1 ):25-9.
Wilson T and Kornman K, "τhe Healthy Patient,'' Fundamentals in Perio-don0bs, Chicago, lL: Quintessence Publishing Company ιnc, 1996,Chapter 15, 285-91.
Zambon JJ and Haraszthy Vl, "The Laboratory Diagnosis of Periodontallnfections," Periodontol 2000, 1 995, 7:69-82.
Zinman E, "Dental and Legal Considerations in Periodontal Therapy,"Periodontol 2000, 2001 , 25:114-3O.
CHAPTER 5: Prevention of Disease andMaintenance of Health
Αddy M and Moran JM, "Evaluation of oral Hygiene Products: Science lsΤrue; Don't Be Misled by the Facts"' PeriodontoΙ 2000,1997' 15:40_51.
Bass CC, "Αn Effective Method of Personal oral Hygiene. Parlll''' J LAState Med Soc, 1954, 1 06:1 00-12.
Becker W, Becker BE, and Berg LE, "PeriodontaΙ τreatment WithoutMaintenance. A Retrospective Study in 44 Patients," J Periodontol,1 984, 55(9):505-9.
Becker \,γ, Berg LE' and Becker BE, "Τhe Long-Teιm Evaluation o{Periodontal Treatment and Maintenance in 95 Patients," ιnt J PerΙo-dontics Restorative Dent, 1984, 4(2)i55-7 1.
Becker W, Berg LE, and Becker BE, "Untreated Periodontal Disease: ΑLon gitudinal Study," J P e ri od ontol, 1 97 9, 50 (5):234-44.
Ciancio SG, "Chemical Agents: Plaque Control, Calculus Reduction andτrealment of Dentinal Hypersensitivity,'' Periodontol 2000' 1995'8:75-86.
cummins D, "Vehicles: Ho\Λ/ to Deliver the Goods," Periodontol 2000,1997,15:84-99.
Drisko CH and Lewis LH, "Ultrasoniο lnstrumentation and AntimicrobialAgents in Supportive Periodontal Treatment and Retreatment ofRecurrent or Refractory Periodontitis,'' PeriodontoΙ 2000' 1996'1 2:90-1 1 5.
Forward GC, James AH, Barnett P, et al, "Gum Health Product Formula-tions: νvhat ls in Them and Why?" Periodontol 2000, 1997' 15:32_9.
BeckerW,BergL,andBeckerBE,.Long-τermEvaluationof Periodontal Cancro LP and Fischman SL,'"τhe Expected Effect on oral Health of
Treatmeni and Maintenance in 9-5 Palients,'' ιnt J peio-αoniiΞs ffi;"'ΞLx'ι:a:Ψ:l
Through Mechanical Removal"' PeriodontaΙ
HestoratΙve Dent, 1984, aQ):54-7 1.
143

APPENDIX
SELECTED READINGS - SPECIFIC (Continued)
Glicksman MA, "Referral of the Periodontal Patient to the Periodontist,"PeriodontaΙ 2000' 2oo1 ' 25:.110-3.
Hirschfeld L and Wasserman B, "A Long-Term Survey of Tooth Loss in600 τreaιed Periodontal Patients,'' J Periodontal, 1978' 49(5):225-J/.
Lang NP, Joss Α, and Tonetti MS, "Monitoring Disease DuringSupportive Periodontal τreatment by Bleeding on Probing," Per|odontol 2000, t996, 12:44-8.
Nyman S, Lindhe J, and Rosling B, "Periodontal Surgery in Plaque-lnfected Dentitions,'' J cΙin Periodontol' 1977' 4(4):240-9-
Scannapieco FA, "Monitoring the Efficacy of Plaque Control Methods,"PeriodontoΙ 2000' 1995' 8i24-41.
\r'r'ade WG and Slayne MA, "Controlling Plaque by Disrupting the Processof Plaque Formation,'' Periodontoι 2000, 1997, 15:25-31 .
Wilson TG Jr, "A τypical Supportive Periodontal Trea1ment Visit forPatients With Periodontal Disease," Periodontoι 2o0o, 1996' 12:24-8.
\ruilson τG Jr, "compliance and lts Role in Periodontal Theraρy,'' Perio-dontal 2000,'1 996, 1 2:16-23.
Wi|son τG Jr, "Supportive Periodontal Treatment Ιntroduction - Defini-tion, Extent of Need, Therapeutic Objectives, Frequency and Effi-cacy,'' Periodontoι 2oo0' 1996' 12:11-5'
νViιson τG Jr and Kornman Ks, "Rereatment for Patients \Λ/ith lnflamma-tory Periodontal Disease," Periodontol 2000, 1996, 119-21.
\Λ/ilson TG Jr, Glove ME, Schoen J, et al, "Compliance With Maintenanceτherapy in a Private Periodontal Practice,'' J PeriodontoΙ, 1984,55:468-73.
OHAPτER 6: NonsurgicaI Treatment: ScaIing andRoot Planing, Occlusal Therapy, AntibioticTherapyBadersten A, Nilveus R, and Egelberg J' "EfΙect of Nonsurgical Perio-
dontal Therapy. ll. Severely Advanced Periodontitis," J CΙin Peri-odontoι, 1984, 1 1 (1 ):63_76-
Bhaskar S and orban B, "Experimental occlusal τrauma," J PeriodontoΙ,1955,26i270-84.
Breininger DR, O'Leary TJ, and Blumenshine RV, "Comparative Effec-tiveness of Ultrasonic and Hand Scaling for the Removal of Subgin-givaΙ Plaque and calculus," J Periodontol,1987' 58(1):9-18.
Burgett FG, Ramfjord SP, Nissle RR, et al, "Randomized Trial ofoοclusal Adjustment in the τreatment of Periodontitis Patienls," JClin PeriodontoΙ' 1992' 19(6):381 -7.
Cercek JF, Kiger RR, Garrett S, et al, "Relative Effects of Plaque Controland lnstrumentation on the clinical Parameters of Ηuman Perio-dontal Disease," J clin Periodontol 1983, 10(1):46-56.
Ericsson I and Lindhe J, "Effect of Longstanding Jiggling on ExperimentalMarginal Periodontitis in the Beagle Dog," J Clin Periodontol, 1982,9(6):497-503.
Gher MΕ, "NonsurgicaI Pocket Τherapy: Dental occlusion,'' Ann Peri-odontol, 1996, 1 (1 ):567-80.
Glickman l' "lnflammation and τrauma From occlusion, co-destructiveFactors in Chronic Periodontal Disease," J Periodontol, 1963, 34:5-10.
G|ickman l and smulo\Λ, J, "Effect of Excessive occlusal Forces Upon thePathway of Gingival lnfιammation in Humans," J Periodontol, 1965,36:141-7.
Gιossary of Periodontal Terms, 4Ιh ed, Chicago, lL: American Αcademyof Periodontology, 2001.
Greenstein G, "Nonsurgical Periodontal τherapy in 2000: A LiteratureRevie\λ/,'' J Am Dent Assoc,2000' 131(11):1580-92.
Hallmon W\,ν, "occlusal τrauma: Effect and lmpact on the Periodon-liυm,'' Ann Periodontoι, 1999, 4(1):102-7.
Lindhe J and Svangerg G, "lnfluence of Trauma From Occlusion onProgression of Experimental Periodontitis in the Beagle Dog,'' J CΙinPeridontol, 197 4, 1 (1):3-1 4.
Lindhe J, Socransky SS' Nyman s, et al, "οritical Probing Depths inPeriodontal Therapy," J cΙin PeriodontoΙ, 1982' 9(4):323-6.
Mosques T, Listgarten MA, and Phillips RW, "The Effect of Scaling andRoot Planing on the composition of Human subgingival λ/ΙicrobialFlor a,'' J Periodontaι Res, 1 980, 1 5(2):1 44-51.
Nield-Gehrig JS and Houseman GA, Fundamentals of Periodontal lnstru-mentation, 3'o ed, Baltimore, MD: Williams & Wilkins, 1996.
Polson AM, "Trauma and Progression of Marginal Periodonlitis inSquirrel Monkeys. ll. Co-destructive Faclors of Periodontitis andMechanically-Produced lnjury," J Periodontal Res, 1 97 4, 9: 1 08-1 3.
Polson ΑM, Kantor MΕ, and Zander HA, "Periodonlal Repair AfterReduction in lnflammation,'' J PeriodontaΙ Res, 1979, 14(6):520-5.
Polson AM, Meitner sW, and zander HA, "τrauma and Progression ofMarginal Periodontitis in Squiπel Monkeys. lv. Reversibiιity of BoneLoSs Due to τrauma Alone and Τrauma Superimposed on Periodon-1itis," J Periodontal Res, 1976, 1 1(5):290-8.
Ramfjord SP and Ash MM Jr, "Significance of Occlusion in the Etiologyand Treatment of Early, Moderale, and Advanced Periodontitis," JPeriodontol, 1 981 , 52(9):51 1 -7.
Rosenberg E, Grossberg D, and Hammond B, '"The Effect of Scaling,Root Planing, and Curettage on Cultivable Microflora AssociatedWith Periodontal Disease," ιnt J Periodontics Restorative Dent,1 989, 9:23-33.
Svanberg GK, King GJ, and Gibbs CH, "Occlusal Considerations inPeriodontology," Periodontol 2000, 1 995' 9:1 ο6-1 7.
Wang HL, Burgett FG, shyr Y' et al, ''Γhe lnfluence of Molar Furcationlnvolvement and Mobility on Future Attachment Loss," J Periodontol,1 994, 65(1 ):2s-9.
Wilkinson RF and Maybury JE, "Scanning Electron Microscopy of theRoot Surface Follo\iving lnstrumentation," J Periodontol, 1973,44(9):559-63.
Wylam JM, Mealey BL, Mills MP, et al, "τhe clinical Effectiveness ofOpen Versus Closed Scaling and Root Planing on Multi-rootedτeeth," J Periodontol' 1993' 64(11):1023-8.
zaρpaυ, Smith B, Simona C, et al, "Root Substance Removal by Scalingand Root Planing," J Periodontol, 1991,62(12)i75O-4.
CHAPTER 7: Surgical Treatment: PrinciplesBarrington EP, "An Overvie\r/ of Periodontal Surgical Procedures," J Peri-
odontol, 1981 , 52(9):51 8-28.
cattermole AΕ and Wade AB, "A comparison of the Scalloped andLinear lncisions as Used in the Reverse BeveΙ τechnique'" J CΙinPeriodontol, 1 978, 5(1 ):41-9.
Clarke MA and Bueltman KW, "Anatomical Considerations in PeriodontalSurgery," J PeiodontoΙ, 197 1' 42(1o\:610-25.
Dahlberg \Λ/Η, "lncisions and Suturing: Some Basic consideralionsAbout Each in Periodontal Flap Surgery," Dent cΙin Nofth Am, 1969,1 3(1 ):1 49-59.
Gιossary of Periodontal Terms, 4|h ed, chicago, |L: Ameriοan Αcademyof Periodontology, 2001.
Hawley CE and serio FG, "PeriodontaΙ Wound Healing'', clark'S cΙinicaΙDentistry, Philadelphia, PA: J B Lippincott Co, 1989, Vol 3, Chapter14, 1-17.
Levin MP, "Periodonιal Suture Materials and Surgical Dressings," Denιclin Noιth Αm, 1980, 24(4):767-81'
Malamed s, "Physical and Psyοhological Evaluation," Sedation: A Guideto Patient Management, 3d ed, St Louis, MO: Mosby-Yearbook, lnc,'1994, Chapter 5, 32-62.
Mormann W and Ciancio SG, "Blood Supply of Human Gingiva FollowingPeriodontal Surgery: A Fluorescein Angiograρhic Study,'' J Per:-odontoι, 1977' 48(1 1 ):681 -92.
Pippin DJ, "Fate of Pocket Epitheliυm in an Apically Positioned Flap'" Jcιin Periodontoι, 1990, 17(6):385-91.
Ramfjord sP and Nissle RR, "The Modified Widman Flaρ,'' J Periodontol,1974, 45(8):601-7.
Silverstein L, "Suture Materials, Suturing Techniques, Surgical KnotTechniques," PrincipΙes of Dental Suturing: τhe comρΙete Guide toSurgical cΙosυre. Montage Media corporation, 2002, chapters 2, 4,5i 12-17, 24-33, 34-69.
144

APPENDIX
Wilderman M, "Exρosure of Bone ιn Periodontal Surgery," Dent cιinNorth Am, 1964, 8:23-36.
Wilderman MN, Pennel BM, King K, et al, "Ηistiogenesis of RepairFollowing Osseous Surgery," J Peiodontol, 1 970, 41 (1 0):551 -65.
CHAPTER 8: Surgical Treatment: Repair,Resection, RegenerationBarrington EP, "An Overview of Periodontal Surgical Procedures," J Peri-
odontoι, 1981 , 52(9):51 8-28.
Bowers GM, Chadroff B, Carnevale R, et al, "Histologic Evaluation ofNeνv Attachment Αpparatus Formation in Humans. Par1 ll.'' J Peri-odontol, 1 989, 60(1 2):675-82.
Bowers GM, Granet M, Stevens M, et al, "Histologic Evaluation of Neu/Attachment in Humans. A Preliminary Reporl," J Periodontol, 1985,56(7):381 -96.
Bragger U, Lauchenaur D, and Lang N, "Surgical Lengthening of theClinical Crown,'' J cΙin PeriodontoΙ, 1992, '19(1):58-63.
Brunsvold MΑ and Mellonig JT, "Bone GraftS and Periodontal Regenera-ιion,'' PeriodontoΙ 2000' 1993' 1 (1):80-91 .
Buser D, Dula K, Hess D, et al, "Localized Ridge Augmentation \r'r'ith
Αutografts and Barrier Membranes," Periodontol 2000' 1999'1 9:1 51 -63.
Carnevale G, Sterrantino S, and DiFebo G, "Soft and Hard TissueWound Healing Following τooth Preparation to the Alveolar crest,''lnt J Peiodontics Restorative Dent, 1983,3(6):36-53.
Catοn JG and Greenstein G, "Factors Related to Periodontal Regenera-Iion,'' Periodontoι 2oo0' 1993' 1(1):9-15.
Cochran DL and Wozney JM, "Bioιogical Mediators for PeriodontalRegeneration," Periodontol 2000, 1999, 19:40-58.
Cortellini P and Tonetti MS, "Focus on lntrabony Defects: Guided TissueRegeneration," P e iodonto ι 2000' 2ooo' 22(1):1 04-32'
Floοken J, "Electrosurgical Management of Soft Tissues and RestorativeDentistry,'' Dent cιin North Am' 19ao' 24i247-69.
Friedman N, "Periodontal osseous Surgery," J Periodontoι' 1955'26:257-69.
Gargiulo A, \Λ/entz F, and orban B, "Dimensions of Relations of theDentogingiνal Junction in Humans," J Periodontoι, 1966' 32i261-7'
Garrett S, "Periodonlal Regeneration Around Natural Teeth," Ann Peri-odontol, 1996, 1 (1 );621 -66.
Greenstein G and Caton JG, "Biodegradable Barriers and Guided TissueRegeneration," Periodontol 2000, 1 993, 1 (1 ):36-45.
lngber JS, Rose LL, and Coslet JG,'τhe "Biologic Width'- A concept inPeriodontiοS and Restorative Dentistry," Alpha omegan' 1977'70(3):62-5.
Karfing τ and cortellini P, "Regenerative Therapy: Furcation Defects,"Periodontoι 2000, 1999, 19:1 15-37.
Karring Τ, Lindhe J, and cortellini P' "Regenerative Periodonta|Therapy," CΙinicaΙ Periodontoιogy and Ιmptant Dentistry, 3rd ed,Copenhagen, Denmark: Munksgaard lnternational Publishers, lnc,1997,597-646.
Karring Τ, Nyman S, Gottloνv J, et al, "Development ol the Biologica|concept of Guided τissue Regeneration - Animal and Humanstudies,'' Periodontoι 2000, 1 993' 1 (1 ):26-35.
Krejci R, Kalkνvarf K, and Krause-Hohenstein U, "Electrosurgery - ABiologic Approach," J Clin Periodontol, 1987, 14(10):557-63.
Lindhe J and Nyman S, "τhe Εffect of Plaque control and SurgicalPocket Elimination on the Establishment and Maintenance of Perio-dontal Health. A Longitudinal Study of Periodontal Therapy in Casesof Advanced Disease," J Clin Peiodontol, 1975,2(2\:67-9.
Machtei EE and Ben-Yehouda Α, '"Τhe Effect of Postsurgical Flap Place-ment on Probing Depth and Αttachment Level: A 2-Year Longitu-dinal Study," J Periodontol, 1994, 65(9):855-8.
MacNeil RL and Somerman MJ, "Development and Regeneration o{ thePeriodontium: Parallels and contrasts,'' PeriodontoΙ 2000, 1999'19:8-20.
McOΙain PK and schallhorn RG, "Focus on Furcation Defeοts - Guidedτissue Regeneration in Combination With Bone Grafting,'' Per'-odontol 2000, 2OOO, 22(1):190-212-
Mormann νv and Ciancio SG, "Blood suρply of Ηuman Gingiva FollowingPeriodonlal Surgery: A Fluorescein Αngiographic Stυdy,'' J Peri-odontoΙ, 1977 , 48(1 1 ):681 -92.
Nasr HF, Aichelmann-Reidy ME, and Yukna RA, "Bone and Bone Substi-lυtes,'' PeriodontoΙ 2000' 1999, 19:74-86.
Nevins M and Skurow ΗM, '"The lntracrevicular Restorative Margin, theBiologic Width, and the Maintenance of the Gingival Margin," /nΙ JPeiodontics Restorative Dent, 1984, 4(3):30-49.
ochsenbein C, "A Primer for osseous Surgery'', Ιnt J PeriodonticsRestorative Denι 1 986, 6(1 ):8-47'
ochsenbein c and Bohannan H, "Τhe Palatal Approach to osseousSurgery. ll. Clinical Application," J Periodontol, 1964, 35:54-68.
oιsen cτ, Ammons WF, and van BelΙe G, "A Longitudinal StudyComparing Apicalty Repositioned Flaps With and Without OsseousSurgery," lnt J Peiodontics Restorative Denξ 1985, 54(4):10-33.
Polson AM, ed, Peiodontaι Regeneration: current Status and Directions,Chicago, lL: Quintessence Books, 1994.
Ramfjord SP, Εngler Wo, and Hiniker JJ, "A Radioautographic Study o,Healing Fo|lowing Simple Gingivectomy. ll. The connective τissue,"J Periodontoι, 1 966, 37(3):1 79-89.
Rosen PS, Reynolds MA, and Bowers GM, "Τhe Τreatment of lntrabonyDefects With Bone Grafts," PeriodontoΙ 2000, 2000, 22(1):88-103.
Samchukov ML, cope JB, cherkashin AM, eds, CraniofaciaΙ DistractionOsteogenesis,St Louis, MO: Mosby-Yearbook, 2001.
Sanz M and Giovannoli JL, "Focus on Furcation Defects: Guided TissueRegeneration," PeriodontoΙ 2000, 2000, 22(1):169-89.
Schallhorn RG, "Postoρeralive Problems Associated \Λ/ith lliaο Trans-plants," J Periodontol, 1 972, 43(1):3-9.
Schallhorn RG and McClain PK, "Combined Osseous CompositeGrafting, Root Conditioning, and Guided Tissue Regeneration," lnt JPeriodontics Restorative Dent, 1988, 8(4):9-31.
Schluger S, "osseous Resection - A Basiο Principle in PeriodontalSurgery," oral Surg oral Med oral PathoΙ, 1949' 2|316-25.
τatakis DN, Promsudthi A, and Wikesjo UM, "Deviοes for PeriodontalRegeneration," Periodontoι 20oo, 1 999' 1 9:59-73.
Wagenberg BD, Εskoνv RN, and Langer B, "Exposing Adequate ToothStruοture
'or Restorative Dentistry," ιnt J Periodontics Restorative
Denf, 1989, 9(5):322-31.
Wilderman M, "Exposure of Bone in Periodontal Surgery," Dent CIinNofth Am, 1 964, 8:23-36.
Wilderman MN, Pennel BM, King K, et al, "Histogenesis of RepairFolloιΛ/ing osseous Surgery," J Periodontol, 1970, 41(10):551-65.
Wood DL, Hoag PM, Donnenfeld OW, et al, 'Alveolar Cresl ReductionFollo\,ving Full and Partial Thickness Flaps,'' J Periodontoι, 1972'43(3):141-4.
OΗAPτER 9: SurgicaI Treatment: PeriodontalPlastic SurgeryΑllen EP and Miller PD Jr, "coronal Positioning of Existing Gingiva:
Short-τerm Results in the τreatment of Shallow Marginal τissueReοession,'' J Periodontol,'| 989' 60(6):31 6-9.
Bouchard P, Malet J, and Borghetti A, "Decision-Making in Aesthetics:Root coverage Revisited," Periodontoι 2000,2001 ' 27:97-120'
Camargo PM, Melnick PR, and Kenney EB, '"Τhe USe of Free GingivalGrafts for Aesthetic Purposes," Periodontol 2000, 2OO1 , 27:72-96.
cohen ES, AtIaS of Cosmetic and Reconstrυctive Periodontaι Surgery,2nd ed, Philadelphia, PA: Lea & Febiger, 1994.
coslet JG, vanarsdaΙl R, and Weisgold A, "Diagnosis and classifiοationof Delayed Passive Eruption of the Dentogingival Junction in theAdulls,'' AΙρha omegan' 1977 ' 7o(3)i24-8'
Garber DA and Salama MA, '"τhe Aesthetic Smile: Diagnosis and Treat-ment," Periodontol 2000, 1996, 1 1 :18-28.
Haeri ΑR and Serio FG, "Mucogingival surgical Procedures: Α Review ofthe Literature," Quintessence /nξ 1999, 30(7):475-83.
Haπis RJ, "Double Pedicle Flap - Predictability and Αesthetics Usingconnective τissue''' PeriodontoΙ 2000' 1996' 1 1 :39-48.
145

APPENDIX
SELEOTED RΕADINGS _ sPEclFlc (Continued)
Jorgensen MG and Noνvzari H,'Aesthetic cro\,νn Lengthening,'' Peri- ννennstrom JL, "Mucogingival τherapy," Ann Periodontoι 1996,odontol 2000, 2OO1, 27:45-58. 1 (1 ):671 -701 .
Kois Jc, "τhe Restorative-Periodontal Interface: Biological Parameters," \Λ/ennstrom J and Pini Prato GP, "Mucogingival Τherapy," cιinicaΙ Perio-Peiodontol 2000' t996' 11:29-38
'".,AE:?{tr:"EξHι";ιEift.'"];'J'[1}:',ffi:1sT"g.1s::Langer B and calagna L, *Γhe subepithelial connective Tissue Graft,"
Prosthet Dent, 1 98ο, 44(4):363-7.
Langer B and Langer L, "subepithelial Conneclive Tissue Graft Tech- CHAPTER 10: Periodontal EmergenCieSnique for Root Coverage," J Periodontol,1985, 56(12):715-20.
Dumsha Tc and Gutmann JL, CΙinician's Εndodontic Handbook,Miller PD, "Periodontal Plastic Surgical Techniques for Regeneration," Hudson, OH: Lexi-Comp, lnc, 2OOO.
Peiodontal Regeneration: Current Status and Directions, PolsonAM, ed' Chicago, lL: Quinlessence Books, 1994,53-70. Holmslrup P, ,,Νonplaque_lnduced Gingival Lesions,,, Ann Periodontoι,
Miller PD Jr, "Root coverage Using the Free soft τissue Autograft1999,4(1):20-9.
FollowingCitricAcidApplication.|ll'Asuccessful andPredictable MengHX,,,Periodontal Αbscess,,,AnnPeriodontoΙ,1999,4(1):79-83.Procedure in Areas of Deep-Wide Recession," ιnt J PeriodonticsRestorative Denl 1985' 5(2):14'37' Meng HX, "Perιodontic-Endodonic Lesions,'' Ann Periodonfol 1999,
Miller PD Jr and Αι|en EP,'"rhe Development of Periodontal Plastic 4(1):84-9-
Surgery"', Periodontal 2oo0' 1996' 1 1 :7-17' Ne\Λ,land JR, Meiller TF, Wynn RL, et al, orat Soft Tissue Diseases: A
Pini Prato GP, clauser c, τonetti MS, et al, "Guided Τissue Regenera- 1?!9',:!:: Manual for Diagnosis and Management' 2"d ed' Hudson'
tion in Gingivat Recessions," periodontot 2000,1996, 11;;9:#. oH: Lexi-comp' lnc' 2001'
sato N, Periodonta! Surgery: A cιinΙcat Attas, chicago lL: Quintessence Rowland^RW, "Necrotizing Ulcerative Gingivitis," Ann Periodontoι'
Publishing company, iooo. 4(1):65-73'
Seibert JS, 'Reconstruction of Deformed, Partially Edentulous Ridges,
H]}YJy'::Η:}?"Z?i};ΙΕ!'1!";#itr::xiij,%?and Wound cHAPTER 11: Considerations in tmplant Dentistry
seibert JS and Lindhe J, "Esthetics in Periodontal Theraρy,'' Ctinicat Donley τG and Gillette WB, "Titanium Endosseous lmplant-soft τissuePeriodontoΙogy and Ιmplant Dentistry,3,d ed, Lindehe j,'karring τ, lnterface: A Literature Review,'' J PeriodontoΙ, 1991' 62(2):153-60.
and Lang NP, eds, Copenhagen, Denmark: Munksgaard lnterna-tional Publishers,1gg7,674-81. Lang NP, Wetzel AC, Stich H, et al, "Histologic Probe Penetration in
Healthy and lnflamed Peri-implant Tissues,'' cΙin oral lmplants Res,Seibert JS and Salama H, 'Αlveolar Ridge Preservation and Reconstruc- 1994, 5(4):191-201 .
tion,'' Periodontoι 2000' 1996' 11:69_84.Meffert RM, "Maintenance of Dental lmplants"' contemporary Ιmplant
Serio FG and strassler HΕ, "Perio_esthetic Troubleshooting: Solutions for Dentistry,2nd ed' Misch CE ed, St Louis, Mo: Mosby-Yearbook, lnc,the Unexpected,'' J Εsthet Dent,1997, 9(6):317_26. 1 999, 647-61 .
Sullivan HC and Αtkins JH, "Free Autogenous Gingival Grafts: l. Princi- Wilson TG Jr, "A Typical Maintenance visit for Patients With Dentalples of Successful Grafting," Periodontics, 1 968, 6(3):1 21 -9. |mplants," Periodontoι 2000, 1996' 12:29.
146

Att 6 Dental-lelated TiilesNoιηl Aυailahle 0n a $ingle GD!
A convenient tool for accessing all of ourdentistry-related titles. A single CD-ROMcontains the following:. Drug lnformation Handbook for Dentistry. Dental office Medical Εmergencies. Natural Τherapeutics Pocket Guide. Clinicians Endodontic Handbook. oralSoft Γlssue Diseases. Manualof Clinical Periodontics
Handheld ]Ieυice SoΙtιυareNow you can have Lexi-Comp's dental drug informationfor your Palm. OS or Pocket PC device
Dεπτnl Lεxi,Dπυqs*Drug lnformation Handbook for Denιlsf/'y database
0NtlNE - Αcοess from your internet browser!
lntera*oE| | '}*.g"l
"J l .qΦηtl
DΙug lnleracιions I Drug ldentification I Patienι Education Leaflets
30-Day Free Trial ) vwvw.lexi.com
Φffitrffi
FIip Charts
1{0ψAγailable!
A Patient Guide to Dental lmplants and
A Patient Guide to Root Ganal Therapy
An idealtoolto educate your patients
81/2" x 1 1 " colorJul tabbed flip chart explaining each of the steps involved
ψPdιi.nι cιide ιo Rοοι cdndl Tbσdn

l
D]ug Informa$οnHandhoolι fοrDefiistryThe most complete andconcise drug reference forall dental professionalsCOMPREHENSIVE:Covers over 6,980 dental &medical drugs!Each monograph gives localanesth etic/vasoconstrictorprecautions, effects on dentaltreatment, and drug interactions.It includes sections on medically-
compromised patients and management of patients \ivith
specific oral conditions (with sample prescriptions) including:oral pain, oraUbacterial infections, periodontal disease, etc.
EASY-TO-USE:This book is alphabetically organized like a dictionary andfully cross-referenced by page number. There are 7 uniquetabbed sections, and Therapeutic Category and Αlphabeticallndices.
Oral soΙlιTisueIliseasesA Reference Manualfor Ιliagnosis &Management
Designed for alldental professionalsThis pictorial reference isvisually-cued with over160 high quality colorphotos. lt is designed toassist in the diagnosis andmanagement of oral soft
tissue diseases. The easy to use sections include thediagnosis proοess: obtaining a history examining the patient'establishing a differential diagnosis, selecting appropriatediagnostic tests, interpreting the resuιts, etc. The sectionscover the following topics: White Lesions; Red Lesions;Blistering-sloughing Lesions; Ulcerated Lesions; PigmentedLesions; Papillary Lesions; Soft Tissue Swelling (each lesionis illustrated with a color representative photograph); DrugSection (specific medications for treatment); and a SpecialTopics section.
Glinician'sEnd0dοnticHandhο0lιDesigned for all dentists with21 endodontic topics everydentist can use.
Designed for all general practicedentists, this is a quick referenceaddressing current endodontics. lthas a easy-to-use format and
alphabetical index. lncludes latest techniques, procedures,and materials including: root canaΙ therapy: why's and whynots; a guide to diagnosis and treatment of endodonticemergencies; facts and rationale behind treatingendodonticaΙly-involved teeth; straight{orward dental traumamanagement information; pulpal histology, access openings,bleaching, resorption, radiology, restoration, andperiodontal/endodontic complications. Also includes aFrequently Αsked Questions (FAQ) section and "ClinicalNote" sections throughout.
ffiffixwwl(Φ
(Φ
Denhl OfiiοeMedicalEmergenGiθsDesigned specificallyfor general dentistsduring times ofemergency. A tabbedpaging system allowsfor quick access tospecific crisis events.Created with urgency inmind, it is spiral boundand drilled with a hole in
the upper left corner for hanging purposes. The easy to usesections include: Basiο Action Plan for Stabilization; Αllergic /Drug Reactions; Loss of Consciousness / RespiratoryDistress / Chest Pain; Altered Sensation / Changes in Affect;Management of Aοute Bleeding; office Preparedness /Procedures and Protocols; Automated External Def ibrillator(AED); and Oxygen Delivery
New soon t0 be
fu:finamia:Ι
Lεx.CoιηB lιιcwww.lexi.com
For more information orto order call:
1 -800-837-5394
released!titles
in the Dental Practice +F
2

Manual 0Ι Glinical Periοdontics
) Uisually_cued with oυer 220 high quality color photos
) Organized by basic principles
) Presented in a "Question & Answer" format
) Recοmmendations for treatment, inοluding sampletreatment plans
12 Ghapters Tabbed for Easy Access:
o PROBLΕM-BASΕD PER|ODONTAL D|AGNOS|S
Θ ANATοMY HISΤοLοGY AND PHYSIοLοGY
Θ ETIοLoGY AND DISEASΕ cLASSlFlcATloN
Θ ΑSSESSMENI DIAGNoSIS, AND TRΕATMENT PLANNlNG
Θ PREVΕNTιON AND MA|NTΕΝANCE
Θ NοNSURGIcAL TREATMΕNT
Θ SURG]OAL TRΕAΤMENΤ: PRlNClPLES
Θ REPAIR, RΕSECTION, AND REGENERATION
Θ PERIoDοNTAL PLASTIc SURGERY
@ PERIODONΤAL EMERGENcIES lmΘ IMPLΑNΤ cOΝSIDERAΤIΟNS v
Lεxl,Coιηη lπc@ APPENDIX. u,urw.texi.com
- Medical Considerations
- Oral Health Products
- Prescription Writing
- lnsurance Coding
- Selected Readings
Category: Dentistry, Periodontics, Dental Hyσiene
Providing unique publishing serviοes
to the healthcare industry
TSBN * 1_ΞΞE5Ξθ_θΞ-Ξ
'||uΙ[Ι[Jilffi[ι]|| ffiilfiffii



![Clinical Cases in · Series: Clinical cases (Ames, Iowa) [DNLM: 1. Periodontal Diseases–therapy–Case Reports. 2. Periodontics–methods–Case Reports. WU 240] 617.6'32--dc23](https://img.pdfslide.net/doc/110x75/5f84edf5754ed16bc7248a59/clinical-cases-in-series-clinical-cases-ames-iowa-dnlm-1-periodontal-diseasesatherapyacase.jpg)