Embed Size (px)
Citation preview

Gateway to Home A community based convalescent care program
Gregory Marr, Manager Long Term Care, Assisted Living, and Short Stay Programs

Disclosure Statement
• None to declare

The Team
• Carly Chuby – physiotherapist
• Crystal Magnant – clinical practice lead
• Kim Forrest – occupational therapist
• Maria Love – nursing unit assistant
• Roy Pei – rehab assistant
• Sandra Harker – social worker
• Various nursing care staff


Gateway to Home
• Short term reactivation and recuperation
• “Do with” rather than “Do for”
• Promote optimal independence in the community
See: Ministry of Health, HCC Policy Manual, Chapter 6, section A




Study Context
End of 2014: Northern Health Board Strategy • Convalescent Care: 1 of 6 initiatives
Did we achieve the intended results?

Measure Result Standard Deviation
Number of Clients 50 NA
Male 12 NA
Female 38 NA
Average Age 81.8 years 12.8 years
Average Length of Stay 37 days (5.3 weeks) 20.4 days (2.9 weeks)
Connected with Primary Care Home
(and interprofessional team where
available)
100% NA
Discharge summaries sent/received 100% NA
Total Bed Days Utilized* 1673 (92%) NA
Table 1. Summary of the Gateway to Home Program as of March 31st, 2016
NOTE: Two additional beds were opened during high overcapacity times at UHNBC (September and December
2015). The total bed capacity was adjusted by +60 days to compensate.

0
1
2
3
4
5
6
7
8
9
10
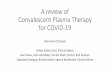
# Individuals
Week Ending
NOTE: Two additional beds were opened during high overcapacity times at UHNBC (September and December 2015)
Figure 1. Number of unique individuals in a Gateway to Home bed during the week
Target

NOTE. 75% of persons who returned to the hospital were deemed palliative
Post Discharge Destination Number of People (%)
Home 33 (75%)
Acute Care 7 (16%)
Deceased 3 (7%)
Long Term Care 1 (2%)
Table 2. Client destination post Gateway to Home participation

Cohort Comparison
28 Day Readmission p = 0.07
ALC-p Designation p = 0.16

• The physical layout of the floor
• Participants are encouraged to be up and doing
• Regular and interval maintenance programming by the Rehab Assistant
• Targeted practice and development of ADLs
• Home visits
Key Success Factors

Key Success Factors continued…
• Collaboration and communication with client/families
• Holistic discharge planning
• Same day turnarounds
• Matching communication (e.g. discharge summaries)

1. Dissemination of results and action planning with staff
2. Completion of a Gateway to Home Operational Playbook
3. Disseminate the findings with Northern Health leadership and
stakeholders
4. Explore opportunity for increased capacity
What’s Next?