Embed Size (px)
Citation preview

Kathryn Hassell, MDProfessor of Medicine, Division of
HematologyUniversity of Colorado Denver
New Oral AnticoagulantsWho Gets What for Atrial Fibrillation
and Venous Thromboembolism?

DisclosuresNo financial or commercial conflicts of
interest
No intended off-label discussion

ObjectivesDescribe the basic characteristics of new
oral anticoagulants (OACs) Recognize potential candidates for new
anticoagulants for atrial fibrillation and treatment of venous thrombosis

Outline of PresentationDiscuss the properties of new oral
anticoagulants (new OACs)Compare/contrast with older anticoagulantsMechanisms and reversibility
Review the pivotal trials for atrial fibrillation and venous thromboembolismGlean important and pertinent clinical
lessons
Consider ways to decide who gets what

Anticoagulant Mechanisms of Action
Adapted from Eriksson, Ann Rev Med 62:41, 2011
RivaroxabanApixaban
Dabigatran
Warfarin
Fondaparinux
Heparin LWMH
VII

Another way to look at itHeparin blocks most activated factorsLow molecular weight heparin blocks two
activated factors: Xa and thrombin (IIa)Newer agents block only one factor:
Anti-Xa agentsFondaparinux (Arixtra) s.q. dailyRivaroxaban (Xarelto) p.o. every 24 hrsApixaban (Eliquis) p.o. every 12 hrs
Anti-IIa agentsArgatroban i.v.Bivalirudin i.v,Dabigatran (Pradaxa) p.o. every 12 hrs
Warfarin doesn’t block ANY activated factors

Yet another way to look at it
COOH
COOH
COOH = carboxyl groupsplaced by vitamin KFactors II, VII, IX, X
Protein unfolds withactivation, revealing
COOH, used to adhereto build a clot
Prothombo
tic
sitmulus
Factors circulate folded until they areactivated during a prothrombotic stress

Warfarin: Fewer “Sticky” Factors
No COOH COOH
Prothrombotic stimulus

Heparins/New Oral Anticoagulants: Inhibition of Activated Factors
COOH
Prothrombotic stimulus

New OACs: “Like drinking your LMWH”
LMWHInhibit activated factorsNo vitamin K impactWeight-adjusted doseDependent on renal
clearanceNo medication
interactionsNo monitoring neededIrreversibleInjections (ouch)Very expensive
NEW ORAL AGENTSInhibit activated factorsNo vitamin K impactFixed doseDependent on renal
clearance (not apixaban)Few medication
interactionsNo monitoring needed
(can’t)IrreversibleOral5-10x cheaper than
LMWH

Potential Drug InteractionsDabigatran: affected by pGP inhibitors or
inducersNot excluded from clinical trialsPI notes quinidine contraindicated; use
caution with:strong inhibitors “like verapamil, clarithomycin and
others”strong inducers (rifampin, St. John’s wort) reduced
effect
May be impacted by degree of renal insufficiency

Potential Drug InteractionsRivaroxaban: affected by combined pGP and
CYP3A4Studies excluded subjects on strong inhibitors
(e.g. HIV meds), strong inducers (e.g. rifampin, phenytoin)
Package insert (PI) advises avoiding or increasing rivaroxaban dose if using carbamazepine, phenytoin, rifampin, St. John’s wort
May be impacted by degree of renal insufficiency

Potential Drug InteractionsApixaban: affected by combined pGP and
CYP3A4; per package insert:For patients receiving >2.5 mg twice daily,
decrease dose of by 50% when coadministered with strong dual inhibitors of CYP3A4 and P-gp (e.g., ketoconazole, itraconazole, ritonavir, clarithromycin)
For patients receiving 2.5 mg twice daily, avoid coadministration with strong dual inhibitors
Avoid concomitant use of strong dual inducers of CYP3A4 and P-gp (e.g., rifampin, carbamazepine, phenytoin, St. John’s wort)
May be impacted by degree of renal insufficiency

Potential Drug InteractionspGP + CYP3A inhibitors:
itraconazole, ketoconzole, clarithromycin, azithromycin
cyclosporin, dronedaroneverapamil, diltiazem, dronedaronelopinavir/ritonavir, conivaptanamiodarone, captopril, carvedilol, felodipine,
quinidinepGP inducers:
carbamazepine, phenytoin,rifampin, tipranavir/ritonavir, St. John’s wort
CYP3A inhibitors: voriconazole (strong), cimetidine (weak)

New Oral Anticoagulants:Measurement ≠ MonitoringCommon assays (aPTT, prothombin time)
insensitive and inconsistently affectedINR is a lab parameter created ONLY for
warfarinOther measures may better reflect drugs
Ecarin clotting time (ECT): dabigatranChromogenic factor Xa actvity level (as done
for people with a lupus anticoagulant): rivaroxaban, apixaban
Even if drug effect can be measured, not the same as what results correlated with outcomes in the studies

New Oral Anticoagulants: Effect on INRDabigatran: therapeutic concentration (NOT
clinical outcomes) correlates with INR range of 1.3-1.7
Stangier, Clin Pharmacokinet 47:285, 2008

New Oral Anticoagulants: Effect on Protime ItselfRivaroxaban: therapeutic concentrations
(NOT clinical outcomes) associated with PT 13-23 seconds
Kubitza D, et al. Clin Pharmacol Ther 2005;78:412-421

New Oral Anticoagulants: Effect on aPTTDabigatran: therapeutic concentrations (NOT
clinical outcomes) associated with aPTT 45-55 seconds
Eriksson BI, et al. J Thromb Haemost 2004;2:1573-1580.Liesenfeld L-H, et al. Br J Clin Pharmacol 2006;62:527-537.

New Oral Anticoagulants: Effect on Coagulation AssaysRivaroxaban, Apixaban: “anti-Xa”, so how
about an anti-Xa (“heparin”) assay?Relatively linear, with some scatterExpected range unknown, no clinical
correlations
Barrett Thromb Haemost 104:1263, 2010

New Oral Anticoagulants:Pharmacological Properties
Attribute Dabigatran Etexilate Rivaroxaban Apixaban
Absorption 6.5%Better in acidic environment
(tartaric acid added)Sl delayed high-fat
diet
66-80%Slightly delayed
by food
66%Not affected by
food
Tmax 1.25-3 h 0.5-4 h 0.5-3 hHalf-Life 7-17 h 3.2-11 h 8-15 hMetabolism
Converted to active drug by esterases in plasma or liver
Metabolized by CYP3A4 (18%) and CYP212
(14%)
Metabolized by CYP3A4,1A
1/2
Elimination 80% renal 66% renal 30% renalReversibility
?Factor VIIa concMay be dialyzed
?aPCC conc ?aPCC concGiorgi. Expert Opin Pharmacother 12:567, 2011

Renal ClearanceWarfarin: not impacted by renal functionDabigatran, rivaroxaban: GFR ≥ 60
ml/min bestMean GFR in studies 60-100 ml/min
Very few subjects had lower GFRWill not detect drug accumulation – no
monitoring Apixaban: only 25% cleared really
Likely to be better tolerated with lower GFRSubgroups defined in pivotal trial for
reduced dose (2.5 mg bid instead of 5 mg bid)≥80 yrs, Cr ≥1.5, wt ≤60 kg
Bauersachs, Thromb Res 129:107, 2012

Drug Clearance in the ElderlyDabigatran (150 mg bid dosing)
Healthy elderly (≥ 75 yrs): up to 2x ↑ exposure after 6 dys
Risk of major bleeding higher in subjects ≥ 75 yrsDoubled risk if >80 yrs and CrCl 50-80 ml/min
Recommended dose of 75 mg bid based on modeling
Rivaroxaban (20 mg/day dosing)Healthy elderly (>75 yrs): ↑ AUC but not max
levelSimilar safety & efficacy in subjects >75 yrsNo differences with mild-moderate renal
impairment15 mg/day (instead of 20) used for CrCl 30-49 ml/min
Bauersachs, Thromb Res 129:107, 2012

Principles Regarding BleedingAnticoagulation doesn’t cause bleeding
Bleeding occurs when a vessel rupturesAnticoagulation doesn’t weaken vesselsMost people who bleed to death aren’t on
anticoagulation
Risk of major bleeding, including intracranial, does not correlate with history of falls
Donze, Am J Med 125:773, 2012
Outcome PlaceboApixaban
2.5 mg po bid
Apixaban 5.0 mg po
bidBleeding 22 (2.7%) 27 (3.5%) 35 (4.3%) Major 4 (0.5%) 2 (0.2%) 1 (0.1%)

Anticoagulants and BleedingRisk of major bleeding 0.7-1.2%/yearWarfarin: the most reversible form of oral
anticoagulationFresh frozen plasma – immediate repletion of
factors, temporary effectVitamin K p.o. or i.v. – production of
functional factors within 6-12 hrsNew agents: active anticoagulation (e.g.
binds activated factors) – no benefit with FFP/Vit KNo proven way to reverse anticoagulationTwice-daily (e.g. dabigatran or apixaban)
may be preferred with shorter effective half-life

With excessive anticoagulation, can use vitamin K to drop INRs:
Guidelines (and experience) advise AGAINST subcutaneous vitamin K for patients on oral anticoagulation
Vitamin K and Warfarin
INR Drop By Time Interval1 mg i.v. 4-5 6-8 hrs1 mg s.q. 2-4 24-48 hrs2.5-5 mg p.o. 4-5 12-24 hrs

Reversal of New OACsFIX THE HOLE that’s bleedingDecrease quantity of drug
Activated charcoal if thought to still be in stomach
Dabigatran may be dialyzedBypass the drug effect
Prothrombin complex (PCC), factor VIIa concentrates anecdotally successful
Recent study suggested aPCC may work best for anti-Xa (rivaroxaban) but not anti-thrombin (dabigatran)
No increased risk of mortality or morbidity (even in >75 y.o.) related to bleeding with new agents
DeLoughery, Am J Hem 86:586, 2011 Eerenberg, Circulation 124:1508, 2011Sardar, J Am Geriat Soc 62:857, 2014

New OACs: Interruption of TherapyDabigatran (per package insert)
If CrCl>50 ml/min, hold 1-2 daysIf CrCl<50 ml/min, hold 3-4 daysEcarin clotting time may be a marker of
activityaPTT “approximates” activity (??), INR unreliable
Rivaroxaban (per package insert)Hold for at least 24 hours
Apixaban (per package insert)Hold for at least 24 hours, 48 for
interventions with higher bleeding risk

New OACs: Interruption of TherapyBridging with LMWH?? Per package
insert:Dabigatran: interruption has been
associated with risk of stroke and thrombotic events“consider administration of other anticoagulant”
Rivaroxaban: events occurred when moving from the drug back to warfarin during clinical trials“consider administration of other anticoagulant”
Apixaban: bridging not recommendedSimilar half-life to LMWH, no clear
theoretical reasons to bridge

New OACs: Switching DrugsOn warfarin, going to a new OAC
Hold warfarin for ~2-3 daysRemember, the lower the daily warfarin
dose, the longer it takes to clear the systemIf in doubt, check an INR before starting the
new OACStart new drug once INR is at/below
desired range (e.g. <2, <2.5, <3)Remember, new OACs fully therapeutic
within 2-3 hours

New OACs: Switching DrugsOn a new OAC, going to warfarin
New drugs affect INR, so need to hold for 24-48 hours before it can be used to measure warfarinMay see some effect even at very low drug
concentrationsIf worried about thrombotic risk, start LMWH
in place of new drug while making the transition
Discontinue LMWH once INR >2.0 (or into desired range) for 24 hours

New OACs and AdherenceOnset of activity within 2-3 hours
Rapid return to therapeutic benefitLoss of activity within 12-24 hours
Missed doses may really be “missed” – no lingering effect as is true with warfarin
Once-daily may be easier to rememberCannot assess drug levels: drug failure
or failure to take the drug?PT/INR, aPTT insensitiveNo data regarding anti-Xa levels
(rivaroxaban, apixaban)

New OACs: Different than Warfarin
WARFARINProduction of
dysfunctional factorsChanges the body
Effect through vitamin KMultiple medication
interactionsDose adjustedCan/must be
monitoredCan be used in renal
failureReversible
NEW ORAL AGENTSInhibition of activated
factorsNo effect unless factors
active
No vitamin K (diet) impact
Few medication interactions
Fixed doseNo monitoring (can’t)Dependent on renal
clearance (not apixaban)
Irreversible

New Oral Anticoagulants (OACs)
IndicationDabigatran Etexilate (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Atrial fibrillation
150 mg bid 20 mg/dy 5 mg bid
↓ renal fctn (GFR)
CrCl 15-30: 75 mg bid
CrCl 15-30: 15 mg/dy
2.5 mg bid
Acute VTE 5-10 days of LMWH, then 150 mg bid
15 mg bid x 21 days, then 20 mg/day
10 mg bid x 7 days, then 5 mg bidFDA
ApprovedWittkowsky, J Thromb Thrombolysis 29:182, 2010; Giorgi, Expert Opin Pharmacother 12:567, 2011; DeLoughery, Am J Hem 86:586, 2011

Statistical vs. Clinically Relevant (?) Pause for Perspective
Stroke ICH0
1
2
3
4
5
New Drug Old Drug
Stroke ICH0
20
40
60
80
100
New Drug Old Drug
p<.05 p<.05

New OACs: Atrial FibrillationComparator: warfarin
Consider time in therapeutic range (TTR)Usual thrombotic outcomes (%/year): non-
inferiority design Composite of stroke, systemic embolism
Usual hemorrhagic outcomes:Major bleedingClinically relevant, non-major bleeding
Typical duration of study: 2 yearsEXCLUDES valvular disease/artificial heart
valves

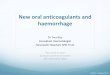
Dabigatran vs. Warfarin for A Fib: RE-LY
Stroke / Em-
bolism
Death Major Bleeding
ICH012345
1.11
3.64
2.71
0.3
1.69
4.133.36
0.7400000000000
02
Dabigatran 150 mg bid
Perc
enta
ge/Y
ear
Subjects: 18,113 Mean age: 71 yrs Mean CHADS: 2.1 Mean CrCl: NR % ASA use: 39%Dosing: Dabigatran: 110 mg bid or 150 mg bid Warfarin: INR 2-3Primary Outcome: Stroke/systemic embolism Warfarin TTR: 64%
- Side effect of dyspepsia in 11.8% vs. 5.8% GI bleeding 1.5% vs. 0.9% (p<.001)- CrCl>30 ml/min to be on study- No differences noted in patients on amiodarone, H2-receptor antagnoists, proton pump inhibitors
*+
+p<.001*p<.05
Connolly, NEJM 361:1139, 2009

Rivaroxaban vs. Warfarin for A Fib: ROCKET-AF
0
2
42.1
4.53.6
0.5
2.4
4.63.4
0.7000000000000
01
Rivaroxaban Warfarin
Perc
enta
ge/Y
earSubjects: 14,264
Median age: 73 yrs Mean CHADS: 3.47 Median CrCl: 67 ml/min % on ASA: 35%Dosing: Rivaroxaban: 20 mg q dy Warfarin: INR 2-3Primary Outcome: Stroke/systemic embolismWarfarin TTR: 55%
-Use of CYP3A4 or P-glycoprotein inhibitors prohibited-As treated safety population 1.7% vs. 2.2% favoring rivaroxaban (p=.02)-No difference across INR ranges
*p=.02*
Patel, NEJM 365:883, 2011

Apixaban vs. Warfarin for A Fib:ARISTOTLE
Throm-bosis
Death Major Bleeding
ICH012345
1.27
3.52
2.18
0.33
1.6
3.943.09
0.8
Apixaban Warfarin
Perc
enta
ge/Y
ear
-Excluded creat >2.5 mg/dl, CrCl<25 ml/min-Interaction between bleeding and -diabetes: apixaban=warfarin if DM -renal function: apixaban better than warfarin with severe renal failure
+p=.01
+*
*p<.001*
Subjects: 18,206 Median age: 70 yrs Mean CHADS: 2.3 CrCl <50 ml/min: 16% % on ASA: 31%Dosing: Apixaban: 5 mg bid or 2.5 mg bid (renal/age) Warfarin: INR 2-3Primary Outcome: Stroke/systemic embolismWarfarin TTR: 66%
Granger, NEJM 365:981, 2011

Meta-Analysis of New Agents for A FibThree RCTs including 44, 563 subjects
RE-LY (Dabigatran)ROCKET AF (Rivaroxaban)ARISTOTLE (Apixaban)
As compared to warfarin:
Miller, Am J Cardiol, amjcard.2012.03.049
Stroke, Systemic
Embolism0.78
(0.67-0.92)Major
Bleeding0.88
(0.71-1.09)
Vascular Mortality
0.87(0.77-0.98) ICH 0.49
(0.36-0.66)
All-Cause Mortality
0.88(0.82-0.95) GI Bleeding 1.25
(0.91-1.72)

ACCP 2012 Guidelines for A FibCHADS2 score
One point each for:- CHF- Hypertension- Age ≥75- Diabetes mellitus- Stroke/TIA history (2 pts)
Score Therapy
0 Nothing or ASA 75-325 mg
≥1
Oral anticoagulant (OAC)
or ASA+clopidogrel (if not OAC candidate)
If OAC: favor dabigatran over warfarinRivaroxaban or apixaban instead of warfarin?
You, Chest 141(Suppl):e531S, 2012

New OACs: Treatment of VTEUsual comparator: LMWH→ warfarin
Warfarin goal INR 2-3; remember TTRUsual outcomes:
Recurrent VTEBleeding
Usual duration of therapy3-6 monthsExtension studies (compared to placebo
or warfarin) for up to 2 years

Dabigatran vs. Warfarin for VTE: RE-COVER
Prim
ary O
utco
me
All-Cau
se Dea
th
Major B
leed
+ Cl
in Rel
Bleed
0
4
8
2.40.5 1.6
5.6
2.10.6000000000000
01 1.9
8.8Dabigatran Warfarin
Perc
enta
ge
Subjects: 2564 Mean age: 55 yrs Isolated PE: 21% History of VTE: 25% Weight: 85 (38-175) kg Est CrCl: 105 ml/minDosing: Dabigatran 150 mg bid Warfarin INR 2-3Primary Outcome: VTE/related deathWarfarin TTR: 60%
Treated for a mean of 3 days with standard therapy before randomizationMore dyspepsia with dabigatran (2.9 vs. 0.6, p<0.001)2% were cancer patients
*p=.002*
NEJM 361:2342, 2009

Subjects: 3445 Mean age: 55 yrs Isolated PE: 0.6% History of VTE: 19% Thrombophilia: 7% Weight>100 kg: 14% CrCl<50 ml/min: 7.5%Dosing: Rivaroxabn: 15 mg bid x 3 wks, then 20 mg/day LMWH+Warfarin INR 2-3Primary Outcome: VTEWarfarin TTR: 58%
Rivaroxaban vs. Warfarin for VTE:EINSTEIN –DVT
Thro
mbosis
Death
Major B
leedin
g
All Blee
ding
02468
10
2.1 2.20.8
8.1
3 2.91.2
8.1
Rivaroxaban Warfarin
Perc
enta
ge
-Excluded -CrCl <30 ml/min -strong CYP3A4 inhibitors (e.g. HIV meds) or inducers (e.g. carbamazepin, dilantin)
*p<.001non-inferior
*
NEJM 363:2499, 2010

Rivaroxaban vs. Warfarin for VTE:EINSTEIN-PE
Thro
mbosis
Death
Major B
leedin
g
All Blee
ding
02468
1012
2.1 2.41.1
10.3
1.8 2.1 2.2
11.4Rivaroxaban Warfarin
Perc
enta
ge
-Excluded -CrCl <30 ml/min -strong CYP3A4 inhbiitors (e.g. HIV meds) or inducers (e.g. carbamazepine, dilatin)
*p<.003^*non-inferiority
*
NEJM 366:1278, 2012
^
Subjects: 4817 Mean age: 57 yrs Unprovoked: 64% History of VTE: 19% Thrombophilia: 5% Weight>100 kg: 14% CrCl<50 ml/min: 8%Dosing: Rivaroxabn: 15 mg bid x 3 wks, then 20 mg/day LMWH+Warfarin INR 2-3Primary Outcome: VTEWarfarin TTR: 62.7%

Apixaban vs. Warfarin for VTE:AMPLIFYSubjects: 5395 Mean age: 57 yrs Unprovoked: 90% History of VTE: 16% Thrombophilia: 2.5% Weight>100 kg: 19% CrCl<50 ml/min: 6%Dosing: Apixaban: 10 mg bid x 7 dys, then 5 mg bid LMWH+Warfarin INR 2-3Primary Outcome: VTEWarfarin TTR: 61%
Thrombosis Death Major Bleeding
All Bleeding02468
1012
2.3 1.50.6000000000000
01
4.32.7 1.9 1.8
9.8
Apixaban Warfarin
Perc
enta
ge
*p<.003^*non-inferiority
^^
*
-Excluded -CrCl <25 ml/min or serum Cr >2.5 mg/dl -potent CYP3A4 inhibitors-Cancer: 2.6%
NEJM 369:799, 2013

New OACs: Treatment of VTERecurrent thrombosis: equal to warfarinBleeding: maybe less than warfarinPopulation included some
ThrombophiliasWt >100kg
Relatively few with renal insufficiencyException is apixaban, which is minimally
renally cleared

Management of VTE: ACCP 2012Acute Management: active anticoagulation
Subcutaneous LMWH
Intravenous or subcutaneous UFH
Fondaparinux
Rivaroxaban?, Apixaban?
Kearon, Chest 141:e419S, 2012

Management of VTE: ACCP 2012Transition to chronic phase of anticoagulation
Initiation of VKA (warfarin) on first day (if not using rivaroxaban or apixaban?)
Continue LMWH/UFH until INR stable and ≥ 2.0 for at least 24 hours
Treatment with LMWH/UFH for at least 5 days
Switch to dabigatran?Kearon, Chest 141:e419S, 2012

Cost Effectiveness Drug costs ~AWP (not the same as
copay/coverage)Warfarin: $0.22-0.25/dayEnoxaparin (prophylaxis): $30-40/day Enoxaparin (treatment): $50-100/dayNew Agents: $4-$8/day
Cost-effectiveness of therapy depends on CHADS score for dabigatran in atrial fibrillationCHADS score 0: ASACHADS score 1-2: warfarin, if INR stable
(TTR>57%) and low bleeding riskCHADS score ≥3: dabigatran, unless INR very
stable (TTR>75%)Shah, Circulation 123:2562, 2011

In patients with DVT or PE, and cancer, per ACCP:LMWH over VKA
CLOT study
If not treated with LMWH, ACCP recommends VKA over rivaroxaban or dabigatran (“too few patients”)
Other Scenarios: Cancer
Lee, NEJM 349:146, 2003
Kearon, Chest 141:e419S, 2012

Other Scenarios: Antiphospholipid Antibody SyndromeRAPS Study (Cohn, UK)
Rivaroxaban vs. warfarin for 3 monthsStudy characteristics:
Population: thrombotic APS ± SLE, single episode VTE
Endpoint: endogenous thrombin potential at 4 months
If successful, will endorse clinical use (!)No plans for clinical outcomes studyHowever, we routinely use LMWH if
concerned about warfarin and this was never studied, eitherRemember, new OACs act like LMWH

Agent Selection – Who Gets What?New OACs Instead of LMWH
Basically similar properties – irreversible, unmonitored - except new agents require:Better (e.g. >60 ml/min) renal function, probablyAwareness of potentially interacting medsAbility to take p.o. medication
Arguably, new agents are at least as efficacious and safe, easier to administer and cheaper

New OACs Instead of WarfarinNormal renal function; low risk for rapid
progression to renal insufficiencyLow bleeding risk: unlikely to need reversalPatients with unstable INRs: new agents likely
cost-effective in addition to safety/efficacy advantage
Adherence: missed dose will be missed!However, immediate return to adequate anticoagulation
once dosing resumed…Drug monitoring not “needed” to assess
adherence, interpret clinical eventsNot on potentially interacting drugs
Agent Selection – Who Get’s What?

Agent Selection – Who Gets What?Warfarin Instead of New Anticoagulants:
Renal insufficiency (GFR<60? <30?), ESRDHigh bleeding risk: most easily reversedPatients with stable INR: most cost-effectiveDifficulty with adherence: least harm with
missed doseHistory of multiple events (bleeding or clotting)
Can measure INR to assess degree of anticoagulation relative to event (INR too high or too low)
On medications that may interact with new anticoagulants, especially those that inhibit drug clearance and in patient with fluctuating mild-moderate renal insufficiency

New Anticoagulants Instead of WarfarinNormal renal function, low risk for rapid
progression to renal insufficiencyLow bleeding risk: unlikely to need reversalPatients with unstable INRs: new agents likely
cost-effective in addition to safety/efficacy advantage
Adherence: missed dose will be missed!However, immediate return to adequate anticoagulation
once dosing resumed…Drug monitoring not “needed” to assess
adherence, interpret clinical eventsNot on potentially interacting drugs
Agent Selection – Who Get’s What?