Embed Size (px)
Citation preview
OCULAR PHARMACOLOGY II
AntiglaucomaMydriatic & cycloplegic
Ocular toxicity of systemic & ocular medications -DR. T.
KurinjhiAsst.Prof.
Ophthalmology
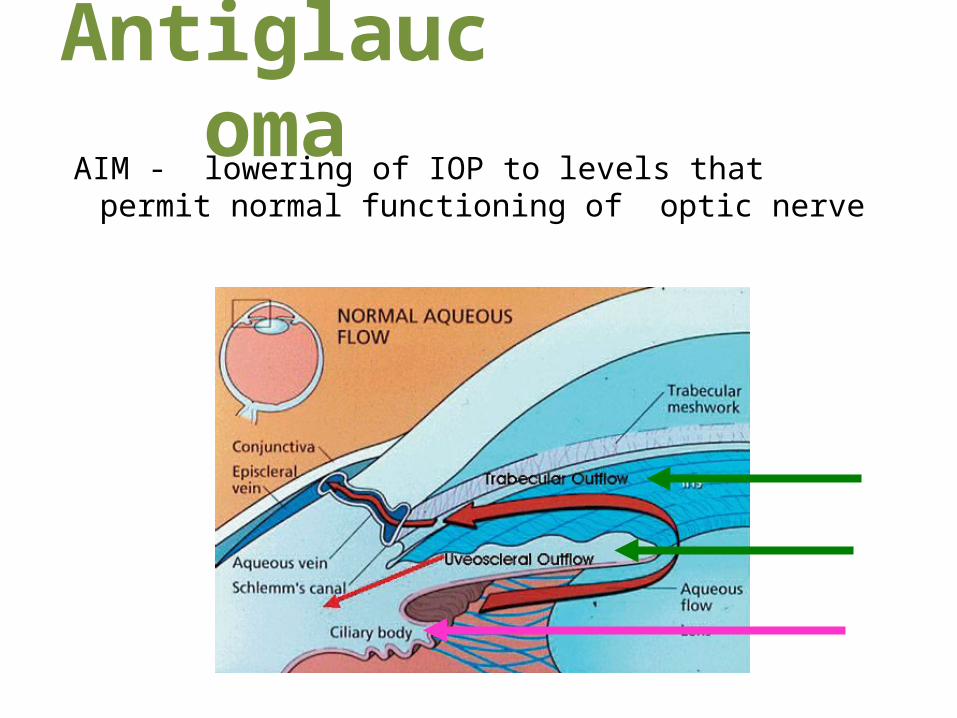
AntiglaucomaAIM - lowering of IOP to levels that permit
normal functioning of optic nerve
PARASYMPATHOMIMETICS
Pilocarpine (2% - 4%) 6-8 hrly, ocuserts
MOA: contraction of longtitudinal fibres of ciliary muscle : pull on scleral spur & widen TBM spaces.
pull peripheral iris away from angle structures
Miosis, brow ache, accomodative spasm
SYMPATHOMIMETICS
Non selective - epinephrine(1%), dipivefrine(0.1%)MOA: increase rate of aqueous outflowStinging, reactive hyperemia, adrenochrome
deposits, CME
Selective – α1& α2 : apraclonidine (0.25%-1%) α2 : brimonidine (0.15%-0.2%)MOA: Decrease aqueous production, increase
uveoscleral outflow, increase optic nerve head perfusion
Ocular allergy, conjunctival blanching

ADRENERGIC ANTAGONISTS(ß blockers)
Non selective – timolol (0.25%-0.5%), levobunolol (0.25%-0.5%)
MOA: reduce rate of aqueous production.Tachyphylaxis, dry eye, bradycardia, bronchial
spasm
Selective – (ß1) betaxolol (0.25%-0.5%)MOA: reduce rate of aqueous production increase perfusion of optic nerve headStinging sensation, local anesthesia
PROSTAGLANDIN ANALOGUES
Latanoprost (0.005%) OD, unoprostone(0.12%), bimatoprost(0.03%), travoprost (0.004%).
MOA: increase uveoscleral outflow
Conjunctival hyperemia, SPK, iris pigmentation
CARBONIC ANHYDRASE INHIBITOR
Acetazolamide (oral-1gm/day), dorzolamide (topical 2%) brinzolamide (topical 1%)
MOA: reduces aqueous production
Altered taste, paresthesia, loss of appetite, depression, metabolic acidosis.
HYPEROSMOTIC AGENTS
Mannitol (5%-25%,1%-2% intravenous), glycerol (1-1.5 gm/Kg BD/TDS oral)
MOA: lower IOP by reducing vitreous volume
Not suitable for diabetics, uncontrolled hypertensives, pul.odema, cardiac/renal failure.
Mydriatic & cycloplegic
SYMPATHOMIMETICSDilate pupilPhenylephrine (5%-10%)
ANTICHOLINERGICS / PARASYMPATHOLYTICS
Dilate pupil, impair accomodationAtropine (1%), homatropine (2%),
cyclopentolate(1%), tropicamide (0.5%)
Fundus examinationTo measure objective refractive error
of the eyeHeadaches, latent hypermetropiaSuspected malingering or hysteriaPharmacologic occlusion therapy in
amblyopia
• Narrow anterior chamber angle – ACG
• Toxicity : fever, skin rash, rapid and irregular pulse, dry mouth and nose, and delirium
• Systemic toxicity - death, from an idiosyncratic response.
Ocular toxicity of systemic &
ocular medications
Corticosteroids Long-term use produces:• posterior subcapsular cataracts, (especially in
asthmatics, renal-transplant recipients and with rheumatic arthritis)
• increased IOP (steroid-induced glaucoma)• exacerbation of bacterial and viral infections• scleral melting
NSAIDs• corneal complications: melting
perforation

AmiodaroneCardiac arrhythmia drugWhorl shaped pigment deposits in corneal
epithelium – cornea
verticillata Deposits are dosage related and reversible
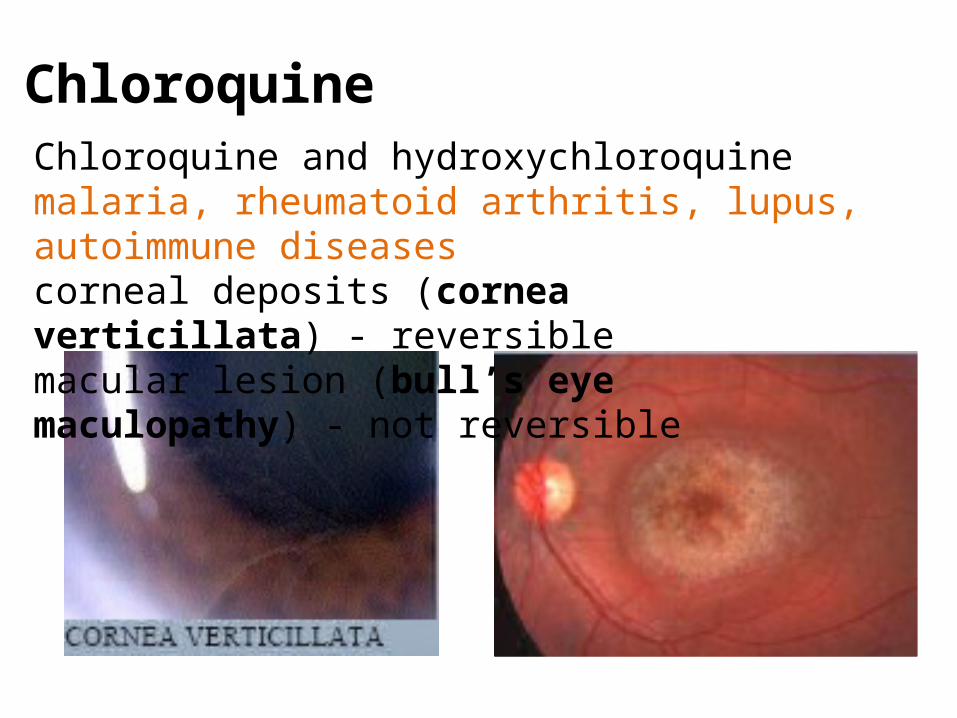
ChloroquineChloroquine and hydroxychloroquinemalaria, rheumatoid arthritis, lupus, autoimmune diseasescorneal deposits (cornea verticillata) - reversible macular lesion (bull’s eye maculopathy) - not reversible
Diphenylhydantoin
Antiepileptic
Dose-related cerebellar-vestibular effects (e.g.,nystagmus, diplopia)
Complex forms of nystagmus and ophthalmoplegia
All reversible effects
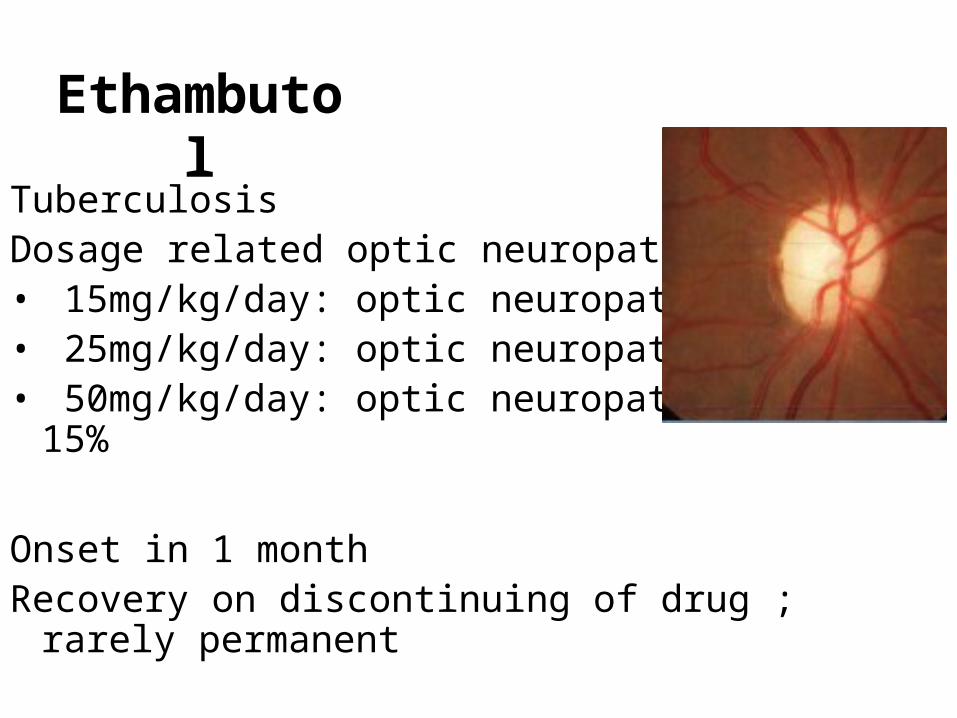
Ethambutol
TuberculosisDosage related optic neuropathy• 15mg/kg/day: optic neuropathy in 1%• 25mg/kg/day: optic neuropathy in 5%• 50mg/kg/day: optic neuropathy in 15%
Onset in 1 monthRecovery on discontinuing of drug ;
rarely permanent
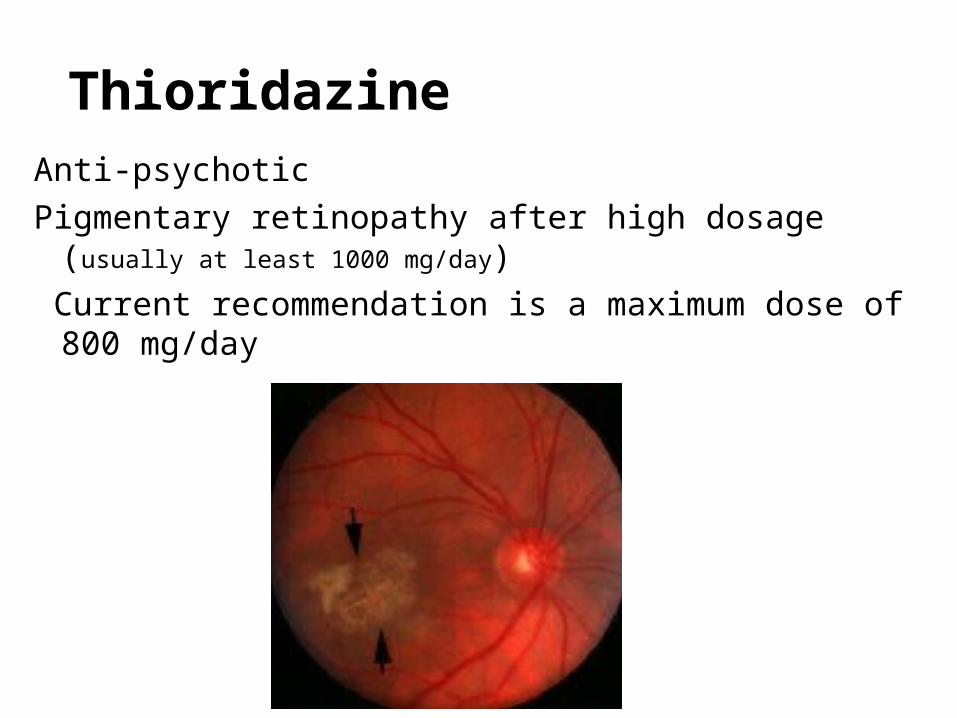
ThioridazineAnti-psychoticPigmentary retinopathy after high dosage (usually at least
1000 mg/day) Current recommendation is a maximum dose of 800
mg/day

Thank You
Anti-inflamatory
CorticosteroidsNSAIDSMast-cell stabilizers, Antihistamines,Antifibrotics
Corticosteroids – systemic, topical - drops, ointment, subconjunctival injections, subtenon’s injection, intravitreal injections /
implants.uveitispost ocular surgical procedures ocular inflammation in traumaoptic neuritis systemic immune diseases with severe
ocular inflammationsPrednisolone; dexamethasone; fluromethalone;
loteprednol

NSAIDS – systemic, topical -drops, ointment
anterior segment inflamation, prophylaxis of CMEReduces intraoperative miosispostoperative inflammation allergic conjunctivitis
Indomethacin, Flurbiprofen, Ketorolac, Diclofenac, Nepafenac and Bromfenac





























