Embed Size (px)
Citation preview
How do capacity building programmes work in local health systems?
A realist evaluation of a local health system strengthening intervention in Tumkur, India
Prashanth Nuggehalli Srinivas
Private defense UCLFebruary 20, 2015
Promoter: Jean MacqCo-promoter: Bart Criel
Outline
• Part 1: The big picture – Strengthening health systems in India
• Part 2: Local health systems and organisational change
• Part 3: Study setting and intervention
• Part 4: Methodology and study design
• Part 5: Analysis and results
• Part 6: Discussion, relevance and lessons learned
2
Background
Methods
Results & Discussion
The big picture
Strengthening health systems in India
3
Part 1
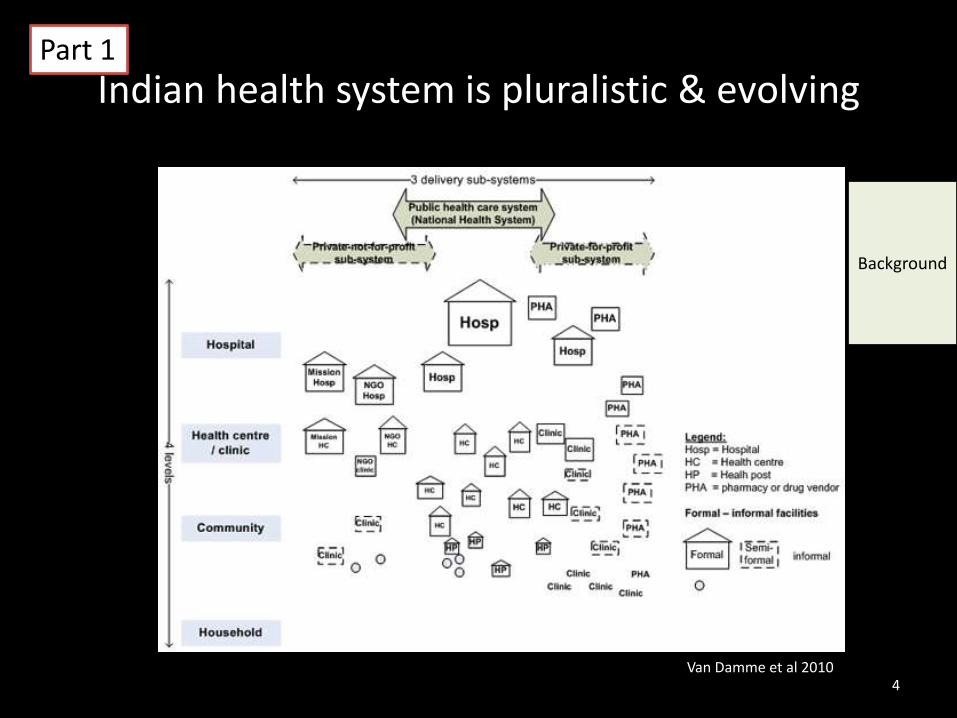
Indian health system is pluralistic & evolving
4Van Damme et al 2010
Part 1
Background
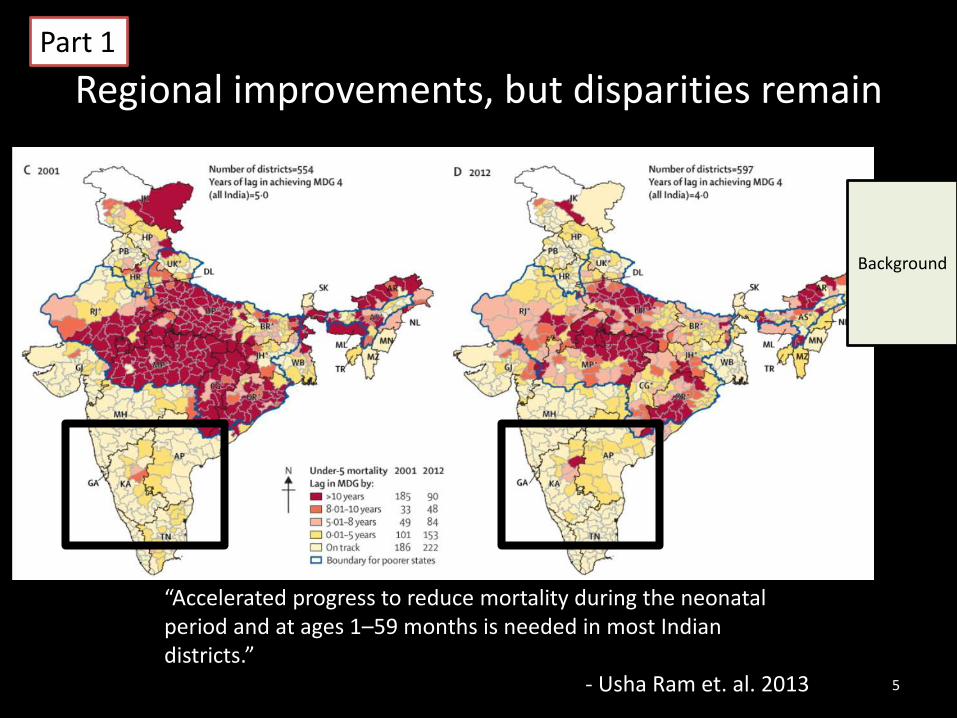
Regional improvements, but disparities remain
5
“Accelerated progress to reduce mortality during the neonatal period and at ages 1–59 months is needed in most Indian districts.”
- Usha Ram et. al. 2013
Part 1
Background
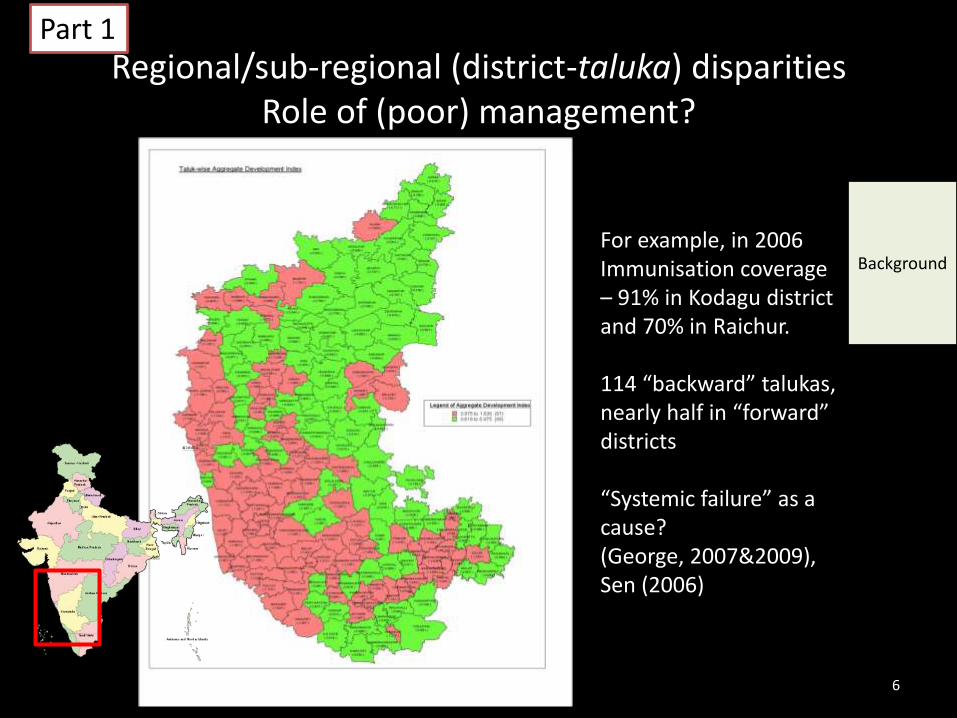
Regional/sub-regional (district-taluka) disparitiesRole of (poor) management?
For example, in 2006Immunisation coverage – 91% in Kodagu district and 70% in Raichur.
114 “backward” talukas, nearly half in “forward” districts
“Systemic failure” as a cause? (George, 2007&2009), Sen (2006)
6
Part 1
Background
Human resources for health
• Good health workforce –Available & competent
• Improved organisationaloutcomes through ‘good HRM’– Lifelong learning and supportive
(yet firm) supervision
– Competent and responsive managers who are able to manageresources and plan health care services
Part 1
Background
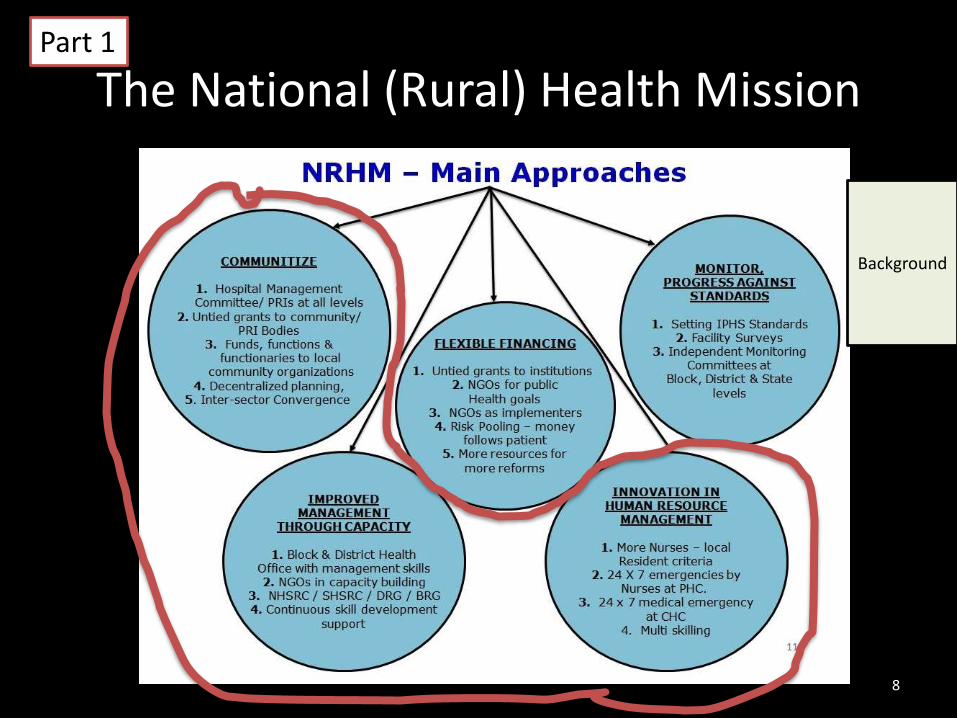
The National (Rural) Health Mission
8
Part 1
Background
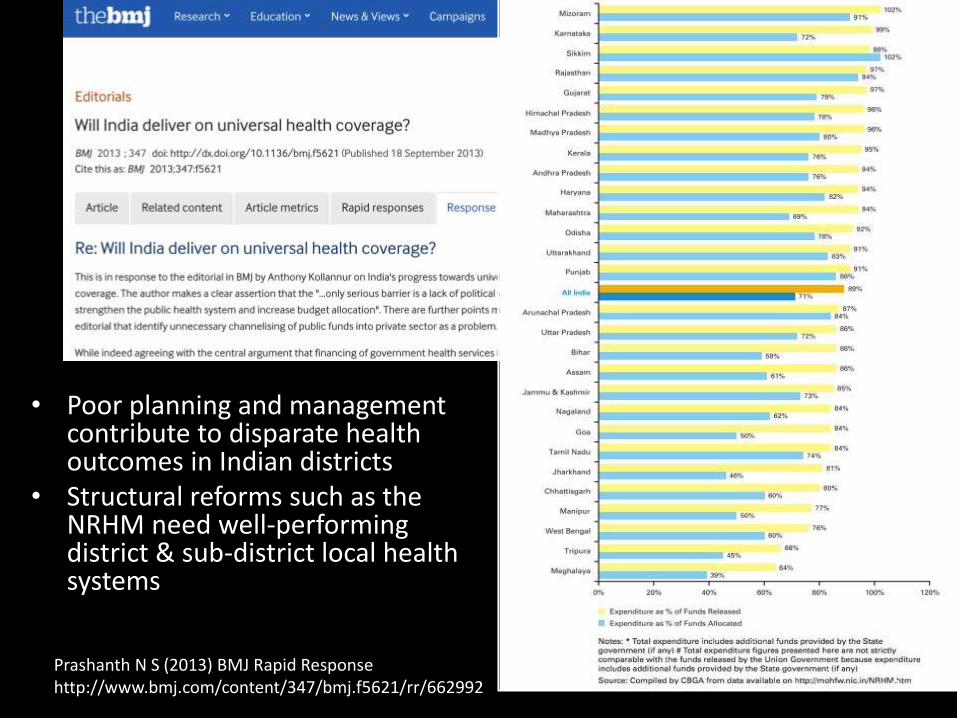
• Poor planning and management contribute to disparate health outcomes in Indian districts
• Structural reforms such as the NRHM need well-performing district & sub-district local health systems
Prashanth N S (2013) BMJ Rapid Responsehttp://www.bmj.com/content/347/bmj.f5621/rr/662992 9
Understanding local health system performance
10
Local health systems
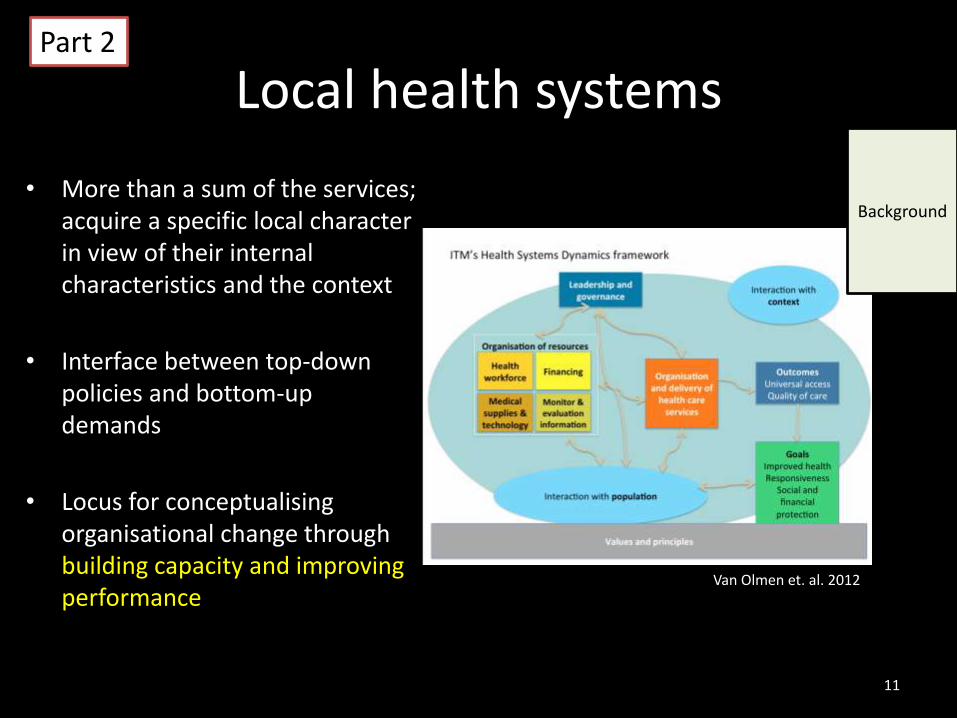
• More than a sum of the services; acquire a specific local character in view of their internal characteristics and the context
• Interface between top-down policies and bottom-up demands
• Locus for conceptualisingorganisational change through building capacity and improving performance
Van Olmen et. al. 2012
11
Part 2
Background
Capacity and performance
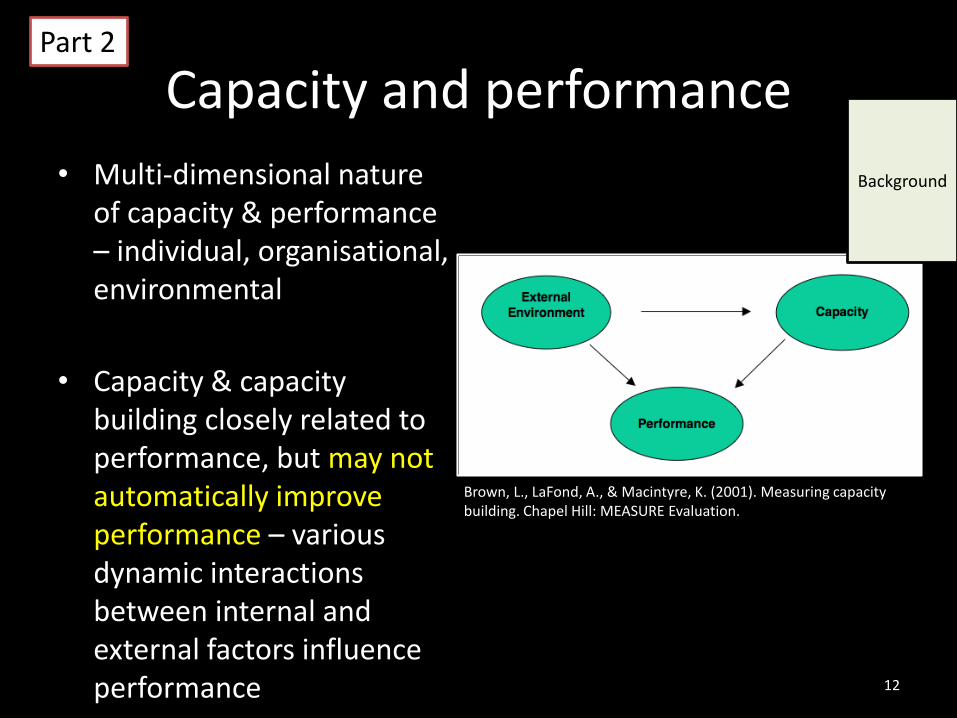
• Multi-dimensional nature of capacity & performance – individual, organisational, environmental
• Capacity & capacity building closely related to performance, but may not automatically improve performance – various dynamic interactions between internal and external factors influence performance 12
Part 2
Background
Brown, L., LaFond, A., & Macintyre, K. (2001). Measuring capacity building. Chapel Hill: MEASURE Evaluation.
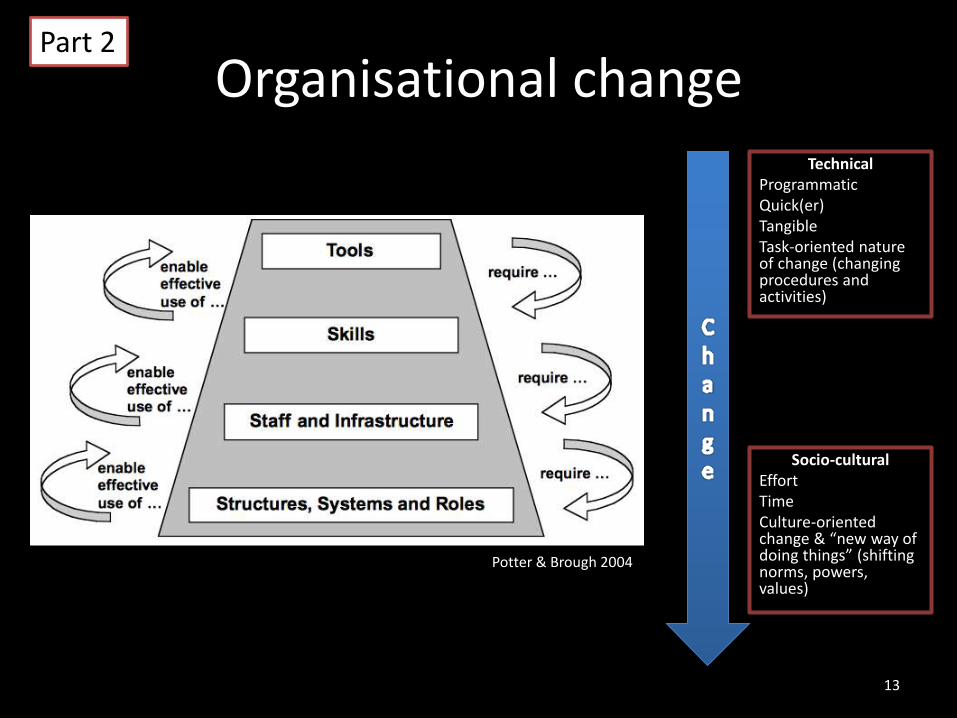
Socio-culturalEffortTimeCulture-oriented change & “new way of doing things” (shifting norms, powers, values)
13
TechnicalProgrammaticQuick(er)TangibleTask-oriented nature of change (changing procedures and activities)
Potter & Brough 2004
Organisational changePart 2
Capacity-building as an HRM intervention
• Implemented with the objective of knowledge or skills transfer through training programmes
• Frequent calls for greater capacity-building in literature and some studies on effectiveness, but:– How do these programmes work at the “systems” level?
– Under what circumstances do these lead to behaviouralchange and improved performance of the organisations?
– What are the contextual elements that promote (or hinder) such change?
14
Part 2
Background
Rationale for the study
• The literature gap – Review of 28 European Commission-funded projects shows need for systemic capacity building & research; and scanty literature on how it works (Potter & Borough 2005)
• The evidence gap – poor evidence for structuring capacity-building interventions (Rowe et al 2005)
• The methodological gap – evaluation of complex HRM interventions
• Timeliness & relevance – National Rural Health Mission
15
Part 2
Background
Asking the how question in healthcare evaluations in India
• Review of health programmeevaluation in India
• Little inter-disciplinarity
• Heavy tilt towards “did programme work” and comparing coverage and effectiveness
• Two case studies – maternity benefit scheme & health insurance for people below poverty line Prashanth, N. S., Marchal, B., & Criel, B. (2013). Evaluating
Healthcare Interventions: Answering the “How” Question. Indian Anthropologist, 43(1), 35–50.
16
Part 2
Study setting and intervention
17
18
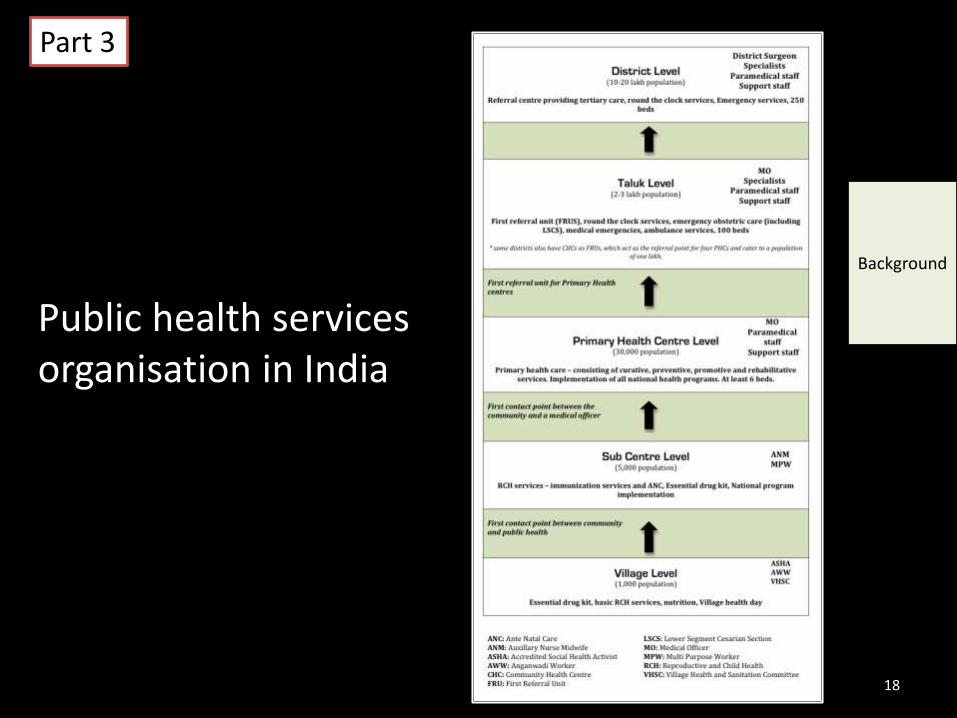
Public health services organisation in India
Part 3
Background
19
Part 3
Background
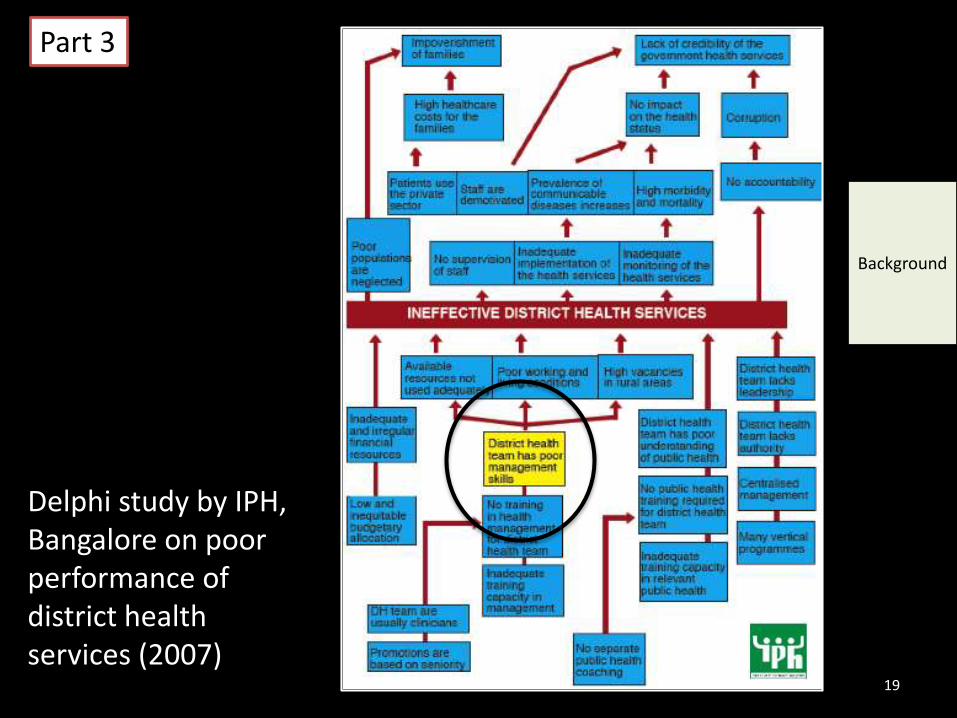
Delphi study by IPH, Bangalore on poor performance of district health services (2007)
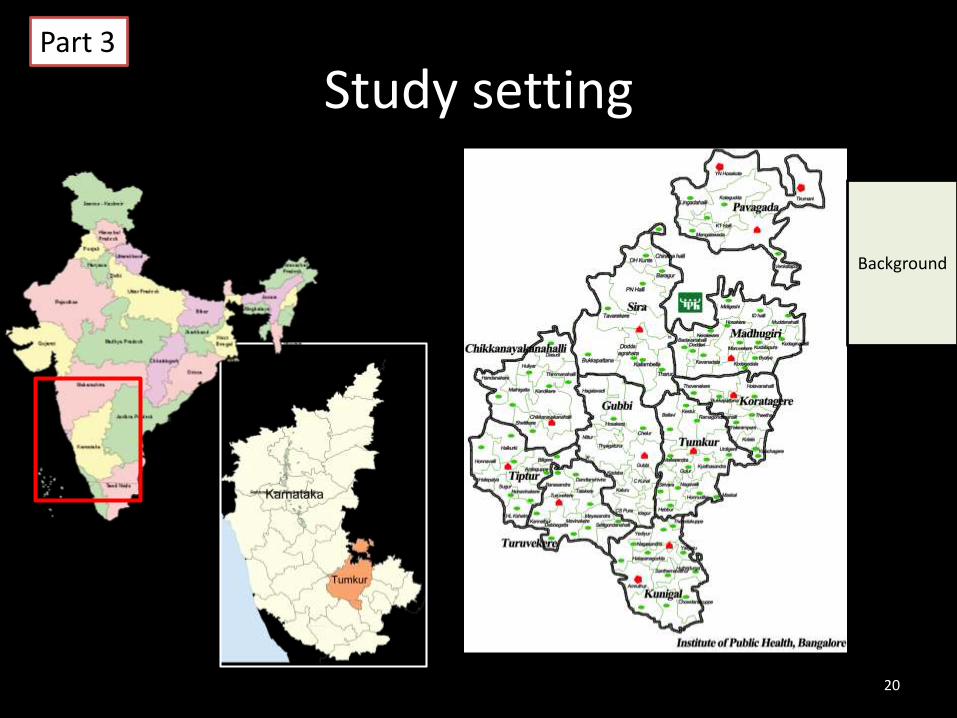
Study setting
20
Part 3
Background
21
22
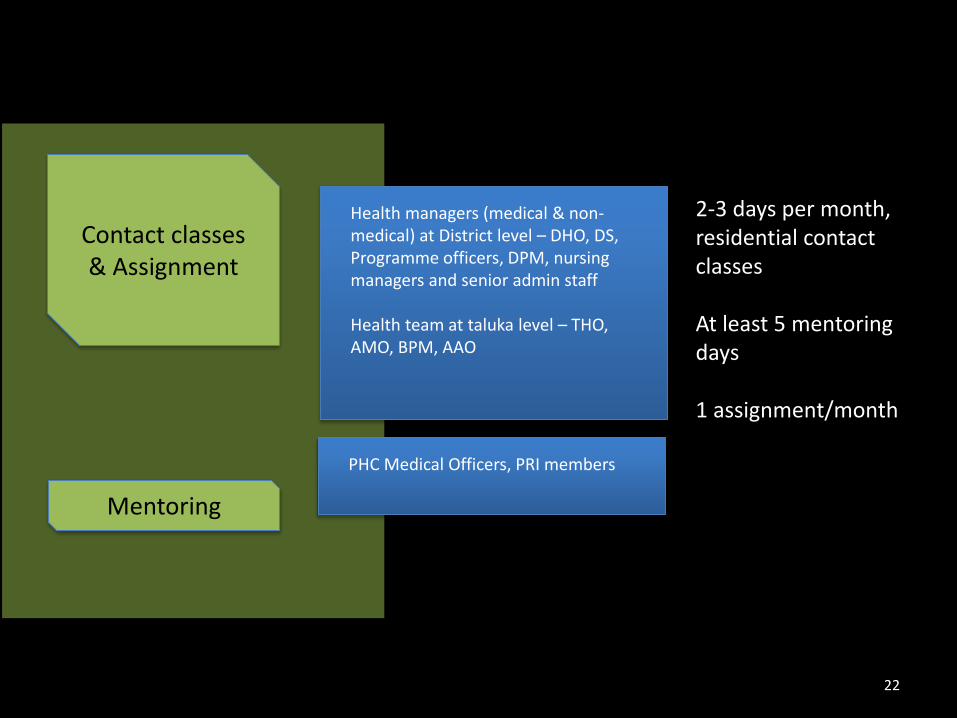
Mentoring
Contact classes & Assignment
Health managers (medical & non-medical) at District level – DHO, DS, Programme officers, DPM, nursing managers and senior admin staff
Health team at taluka level – THO, AMO, BPM, AAO
PHC Medical Officers, PRI members
2-3 days per month, residential contact classes
At least 5 mentoring days
1 assignment/month
Methodology and study design
23
Methodological considerations
• Programme theory and assumptions were not explicitly formulated
• From effectiveness to mechanisms of change in organisations
• Mixed methods study
24
Part 4
Methods
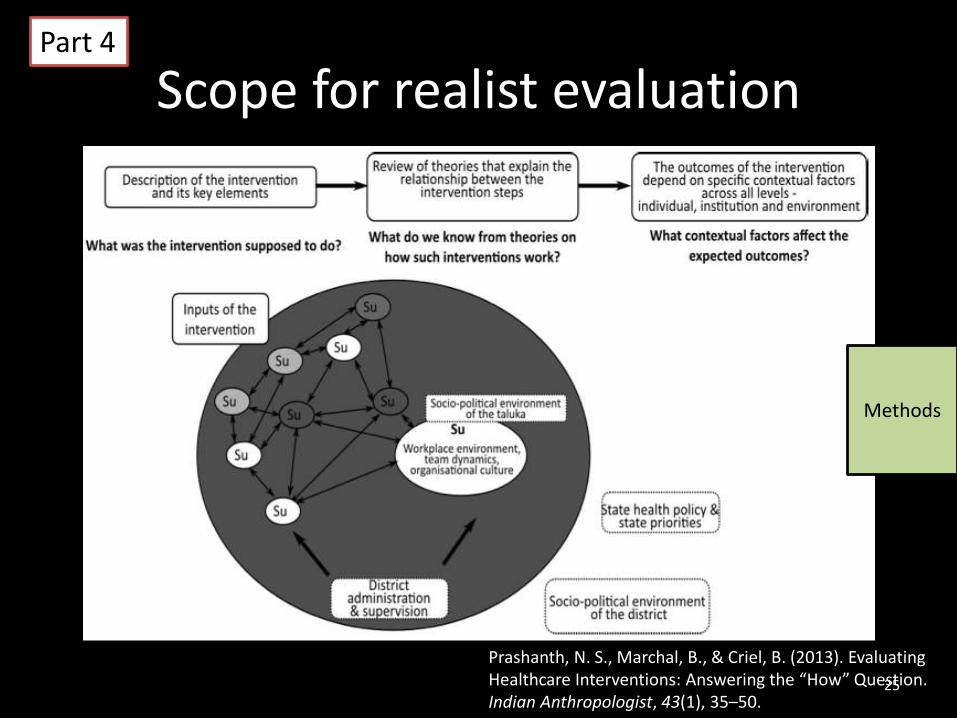
Scope for realist evaluation
Prashanth, N. S., Marchal, B., & Criel, B. (2013). Evaluating Healthcare Interventions: Answering the “How” Question. Indian Anthropologist, 43(1), 35–50.
25
Part 4
Methods
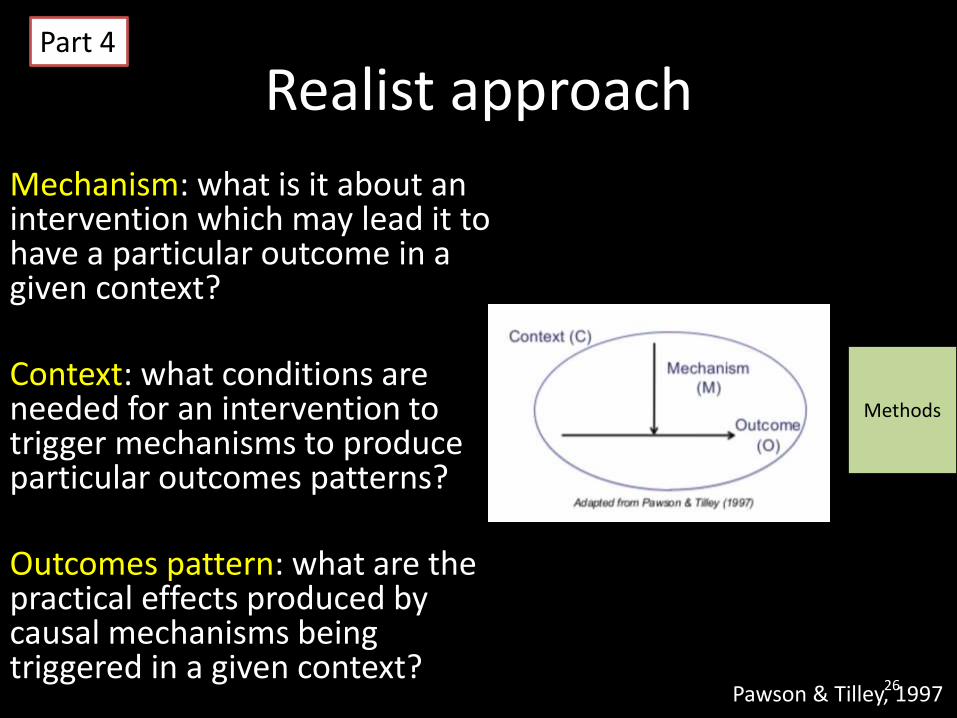
Realist approach
Mechanism: what is it about an intervention which may lead it to have a particular outcome in a given context?
Context: what conditions are needed for an intervention to trigger mechanisms to produce particular outcomes patterns?
Outcomes pattern: what are the practical effects produced by causal mechanisms being triggered in a given context?
Pawson & Tilley, 199726
Part 4
Methods
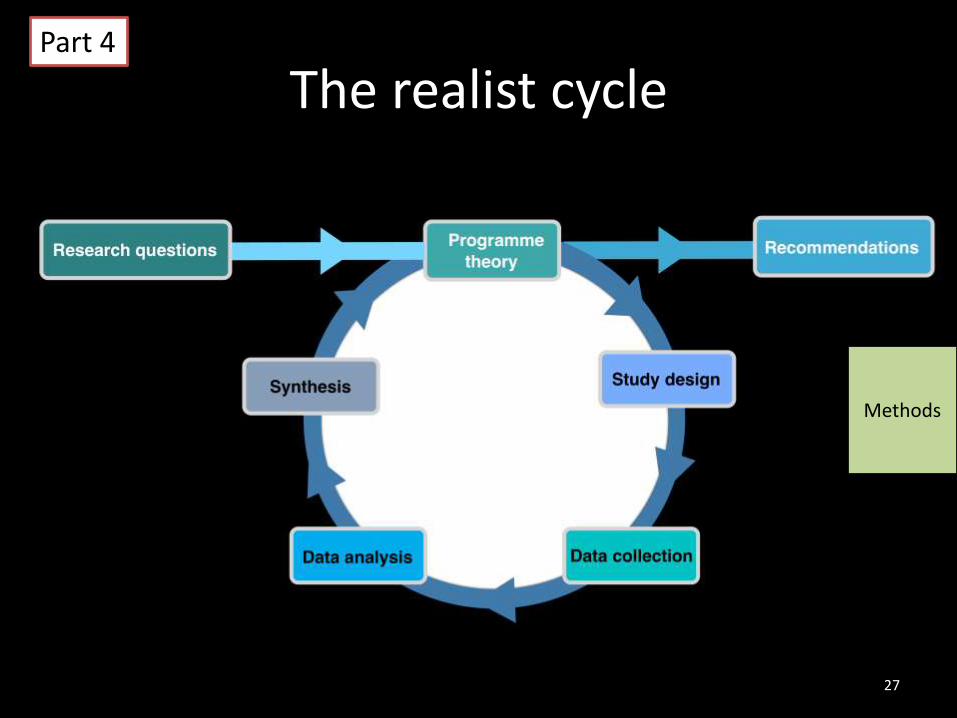
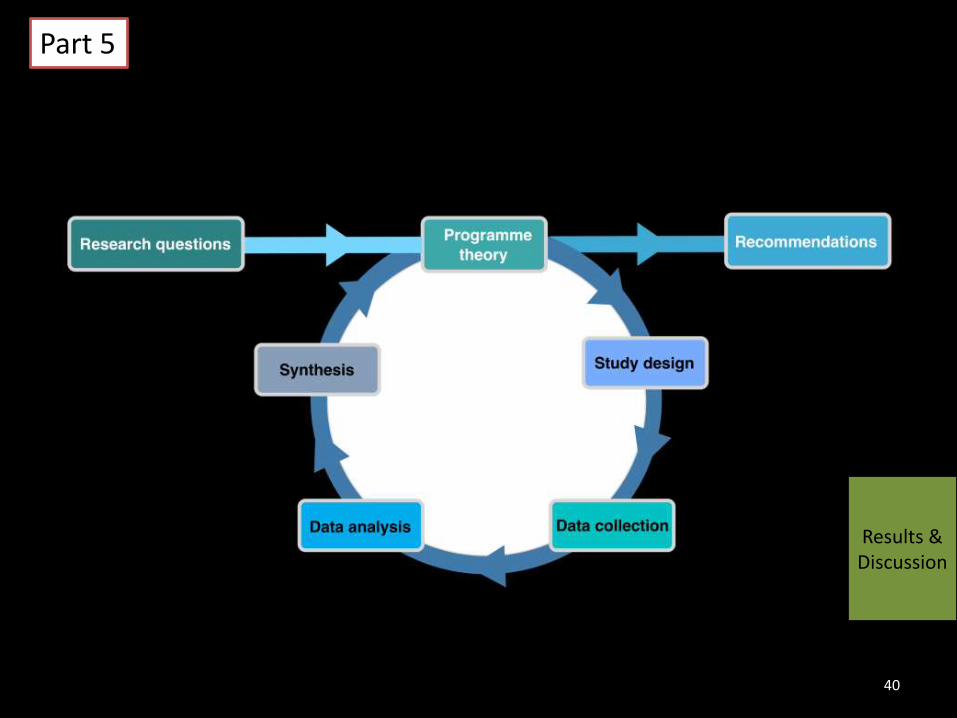
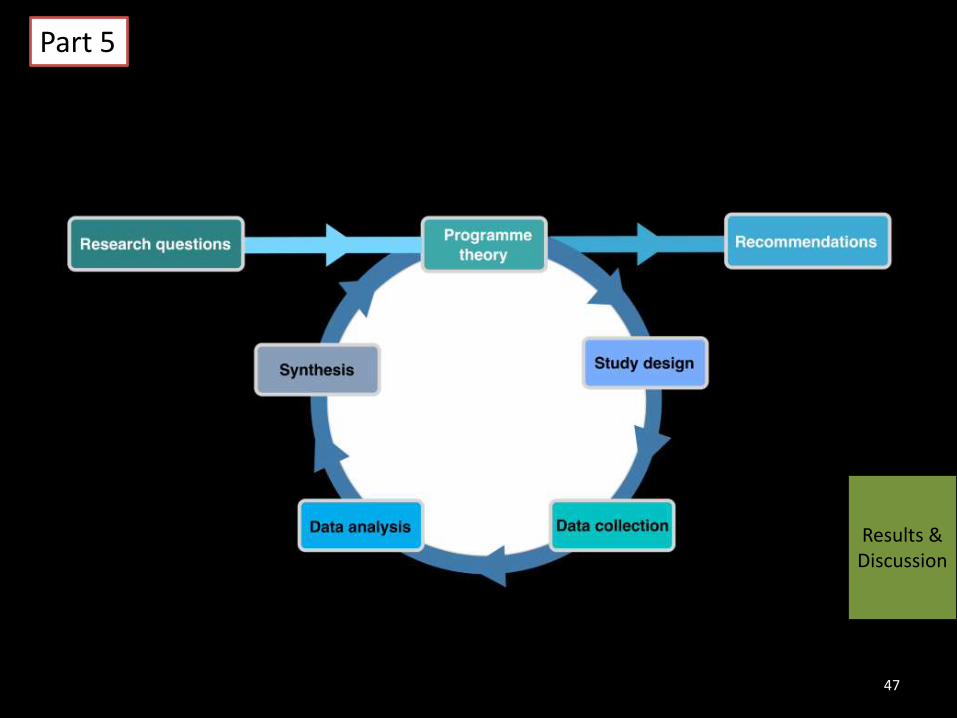
The realist cycle
27
Part 4
Methods
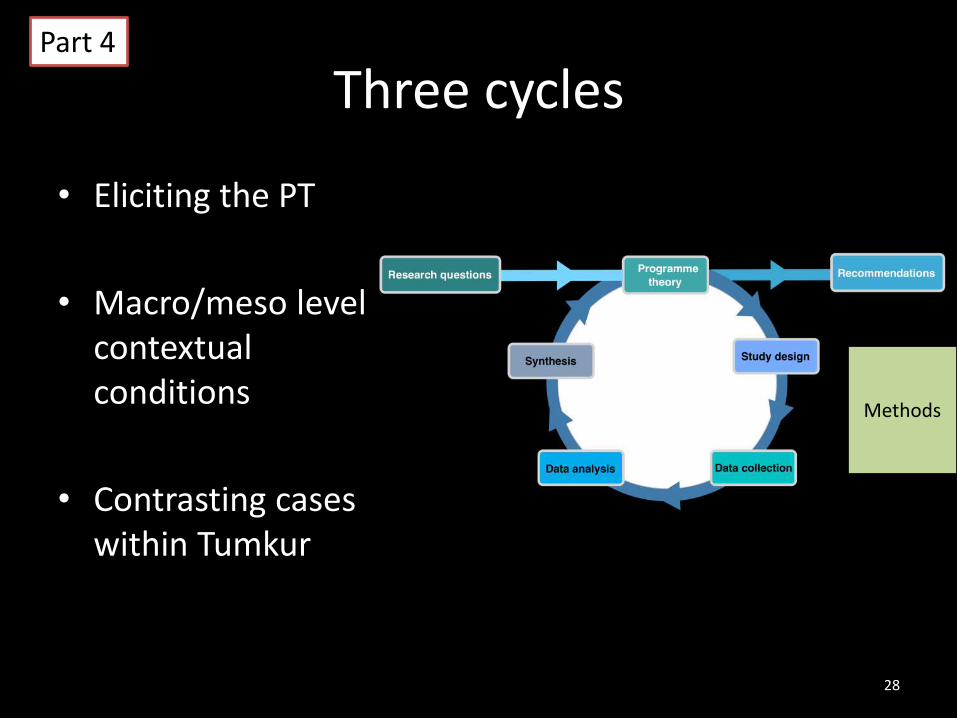
Three cycles
• Eliciting the PT
• Macro/meso level contextual conditions
• Contrasting cases within Tumkur
28
Part 4
Methods
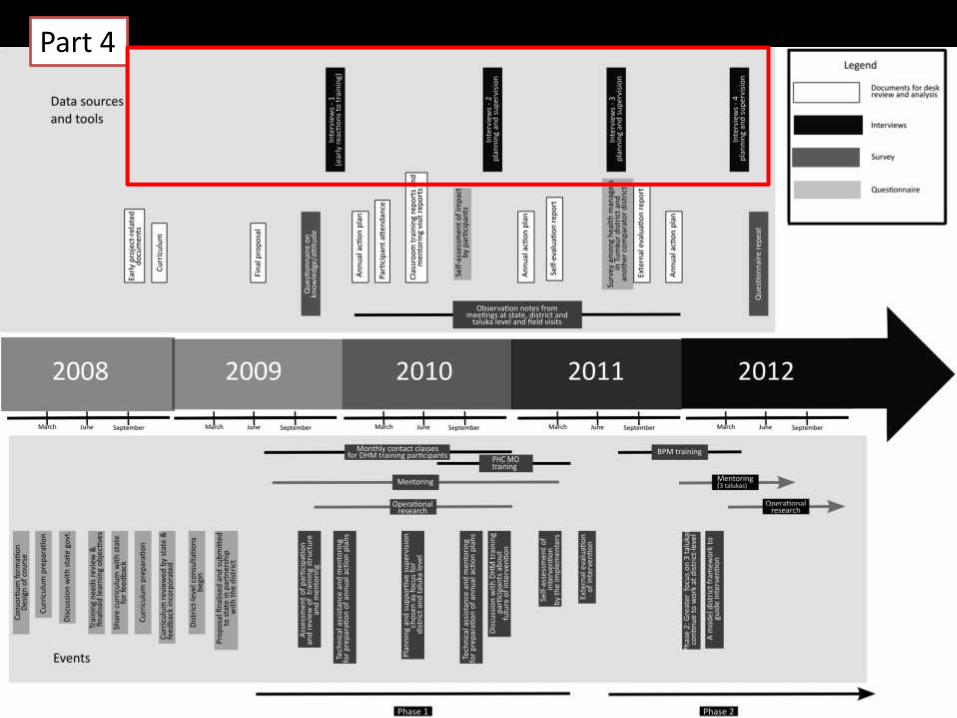
Data collection
• Field notes of observations during classroom teaching, mentoring visits, district and talukareview meetings and supervision visits
• Interview with participants (7+7+8), supervisors (2), state-level bureaucrats (2) and implementers (2) in three episodes: early intervention, mid and post
• Secondary data: annual plans, district-planning guidelines from state and central government, programme documents of the NRHM
29
Part 4
Methods
Survey
– Attitude towards decentralised planning and training programmes
– Organisational commitment (Mayer & Allen)
– Self-efficacy (Bandura)
– Supervision (Oldham & Cummings as adapted from Michigan OA package)
– Respondents (Tumkur and a comparator district): 65+27
30
Part 4
Methods
31
Part 4

Eliciting the programme theory (PT)
• Described the process of refining PT– Understanding the
intervention (IPT)– Review of literature to
identify mechanisms reported
– Identify relevant contextual factors
– Refine PT– Formulate change scenarios
(C-M-O)
32
Part 4
Methods
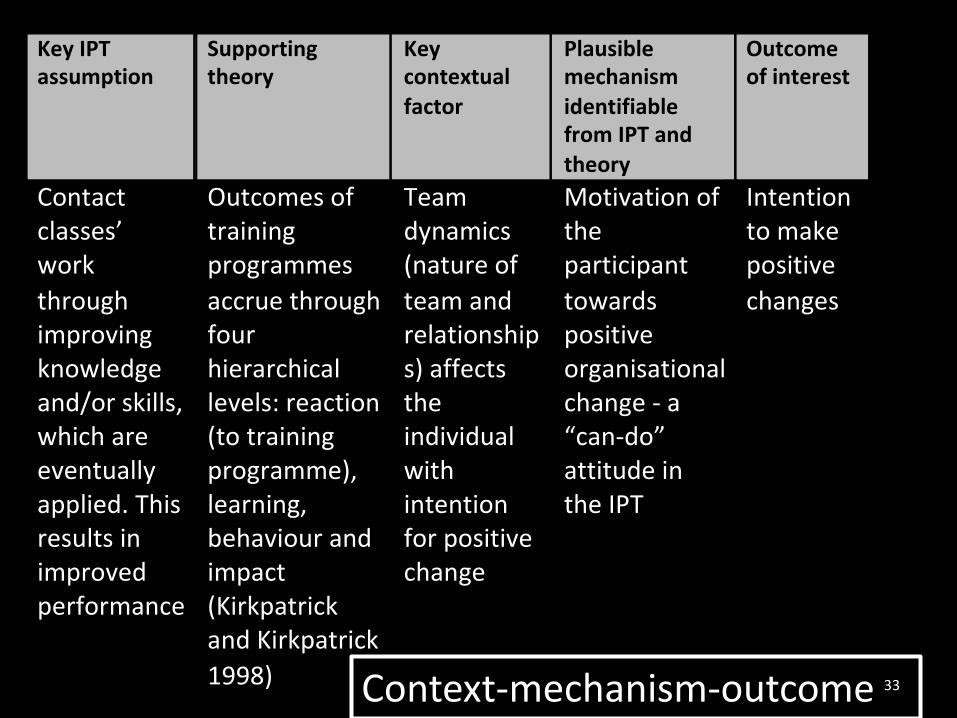
KeyIPTassumption
Supportingtheory
Keycontextual
factor
Plausiblemechanism
identifiablefromIPTand
theory
Outcomeofinterest
Contactclasses’work
throughimprovingknowledgeand/orskills,whichareeventuallyapplied.Thisresultsinimprovedperformance
Outcomesoftrainingprogrammes
accruethroughfourhierarchicallevels:reaction(totrainingprogramme),learning,behaviourandimpact(KirkpatrickandKirkpatrick
1998)
Teamdynamics(natureof
teamandrelationships)affectstheindividualwithintentionforpositivechange
Motivationoftheparticipant
towardspositiveorganisationalchange-a“can-do”attitudeintheIPT
Intentiontomakepositive
changes
Context-mechanism-outcome 33
KeyIPTassumption
Supportingtheory
Keycontextualfactor
Plausiblemechanism
identifiablefromIPT
andtheory
Outcomeofinterest
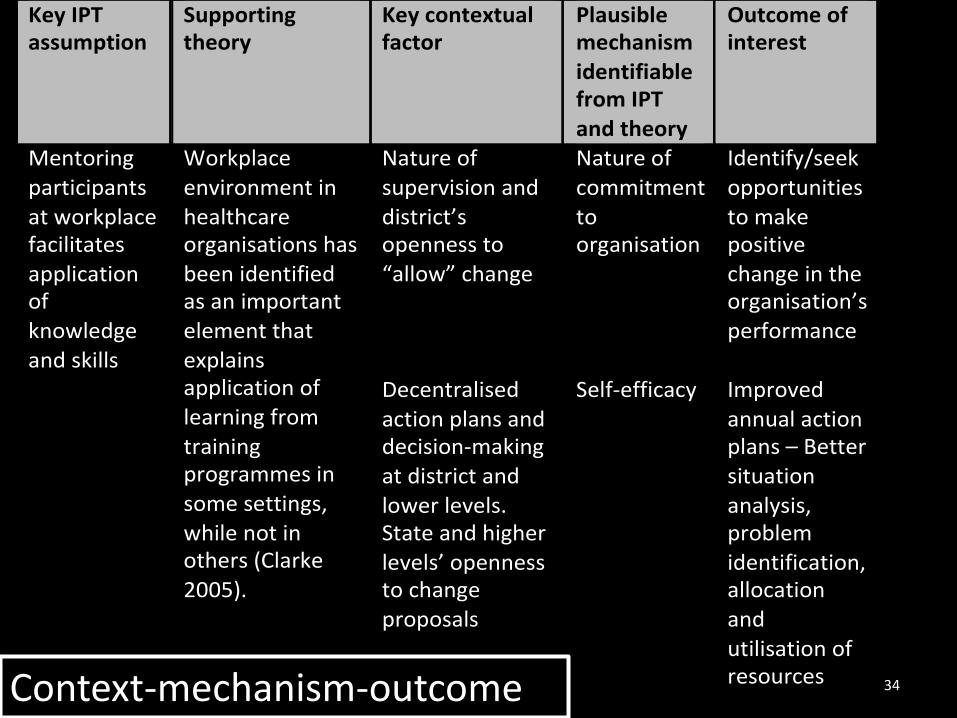
Mentoring
participants
atworkplacefacilitates
applicationof
knowledge
andskills
Workplace
environmentin
healthcareorganisationshas
beenidentifiedasanimportant
elementthat
explainsapplicationoflearningfrom
trainingprogrammesin
somesettings,
whilenotinothers(Clarke
2005).
Natureof
supervisionand
district’sopennessto
“allow”change
Natureof
commitment
toorganisation
Identify/seek
opportunities
tomakepositive
changeintheorganisation’s
performance
Decentralised
actionplansanddecision-making
atdistrictand
lowerlevels.Stateandhigher
levels’opennesstochange
proposals
Self-efficacy Improved
annualactionplans–Better
situation
analysis,problem
identification,allocation
and
utilisationofresources
34Context-mechanism-outcome
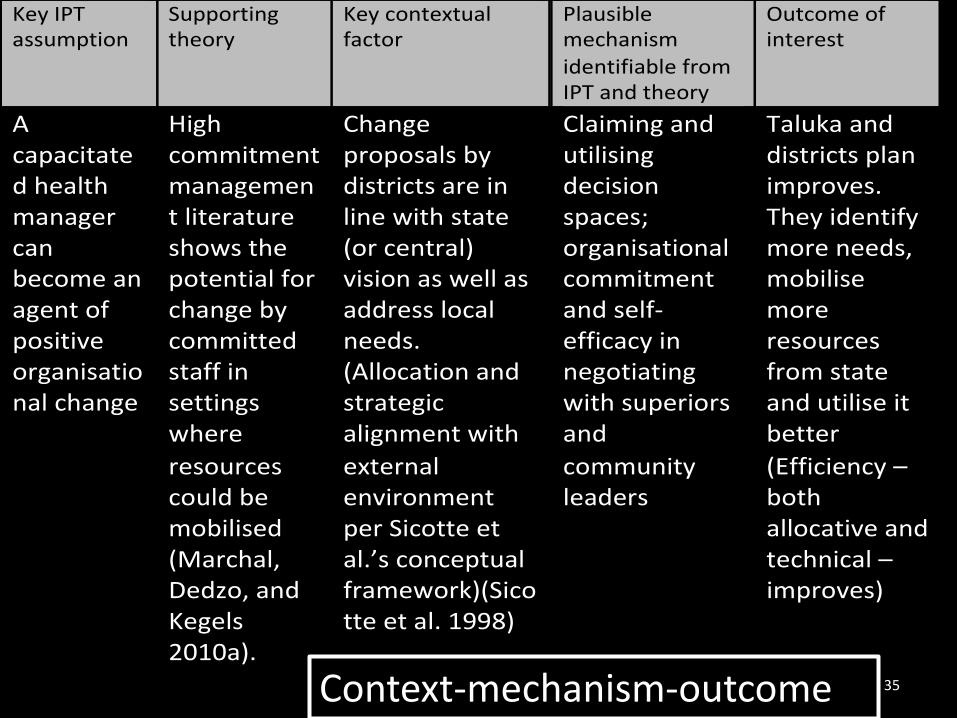
KeyIPTassumption
Supportingtheory
Keycontextualfactor
Plausiblemechanism
identifiablefromIPTandtheory
Outcomeofinterest
Acapacitatedhealthmanagercanbecomeanagentofpositiveorganisationalchange
Highcommitmentmanagementliteratureshowsthepotentialforchangebycommittedstaffinsettingswhere
resourcescouldbemobilised(Marchal,Dedzo,andKegels2010a).
Changeproposalsbydistrictsareinlinewithstate(orcentral)visionaswellasaddresslocalneeds.(Allocationandstrategicalignmentwith
externalenvironmentperSicotteetal.’sconceptualframework)(Sicotteetal.1998)
Claimingandutilisingdecisionspaces;organisationalcommitmentandself-efficacyinnegotiatingwithsuperiorsand
communityleaders
Talukaanddistrictsplanimproves.Theyidentifymoreneeds,mobilisemoreresourcesfromstateandutiliseitbetter
(Efficiency–bothallocativeandtechnical–improves)
35Context-mechanism-outcome
Analysis and results
36
Elicited PT - 1
Contact classes could work through commitment and efficacy of health managers who bear an intention to make positive change by providing them resources in the form of knowledge and/or skills; they are likely to apply these knowledge and skills in talukas where local team environment supports such change and the change agenda aligns with the local PRI and district/state expectations
37
Results & Discussion
Part 5
Mentored participants are more likely to seek opportunities to improve their local health systems to make positive change in the organisation’s performance wherever there is no hindrance (or there is an alignment) to such moves either from above or from the PRI/community structures
Elicited PT - 2
38
Results & Discussion
Part 5
Local health systems could be improved in decentralising health systems if teams have the ability to negotiate with various actors about their change proposals and if they claim decision-spaces for preparation and implementation of action plans and local decision-making at district and lower levels; if the capacity building programme could work at multiple levels to ensure better alignments between opposing elements across various actors and levels in the health system.
Elicited PT - 3
39
Results & Discussion
Part 5
40
Results & Discussion
Part 5
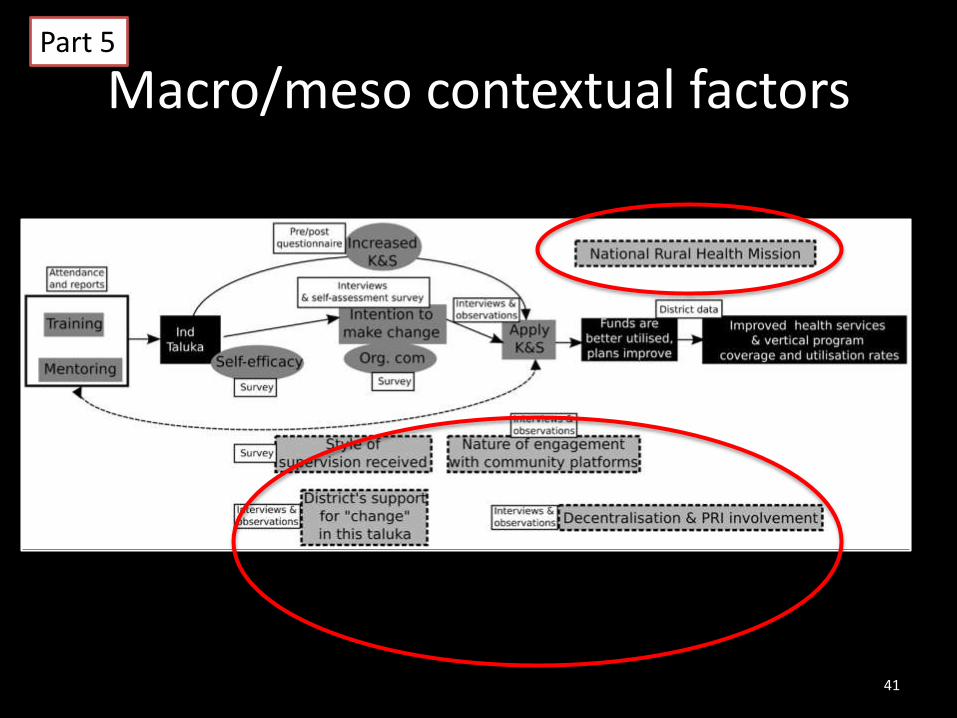
Macro/meso contextual factors
41
Part 5
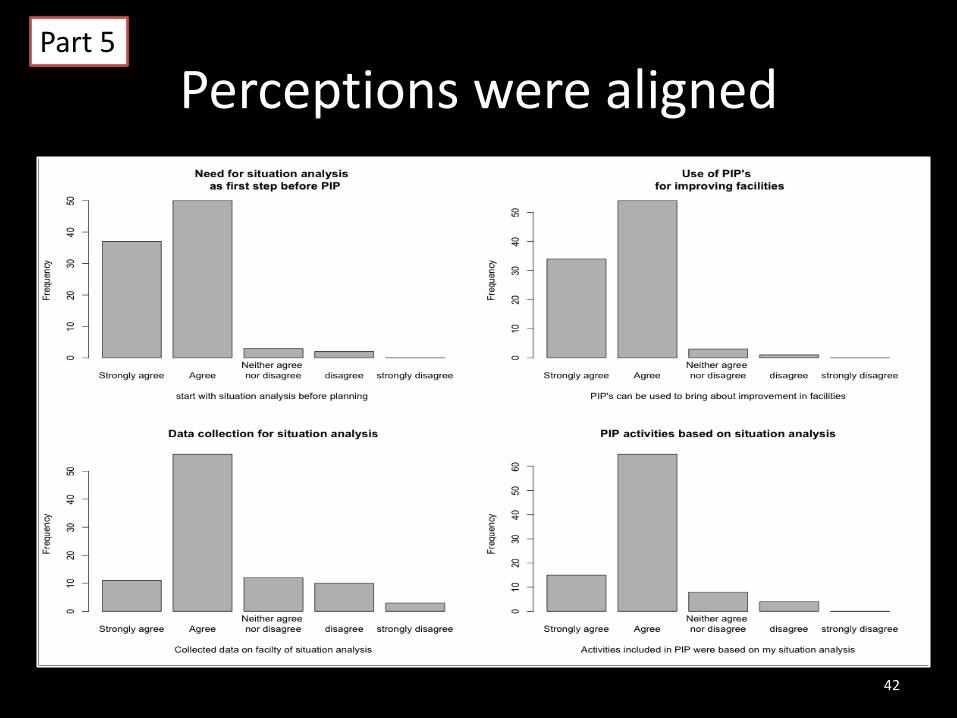
Perceptions were aligned
42
Part 5
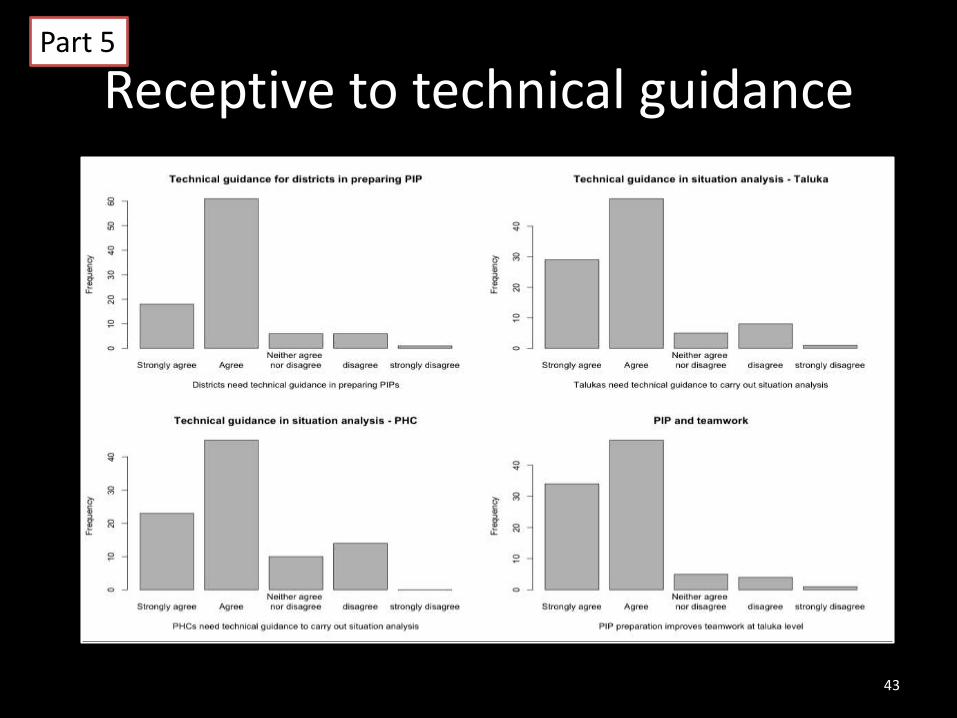
Receptive to technical guidance
43
Part 5
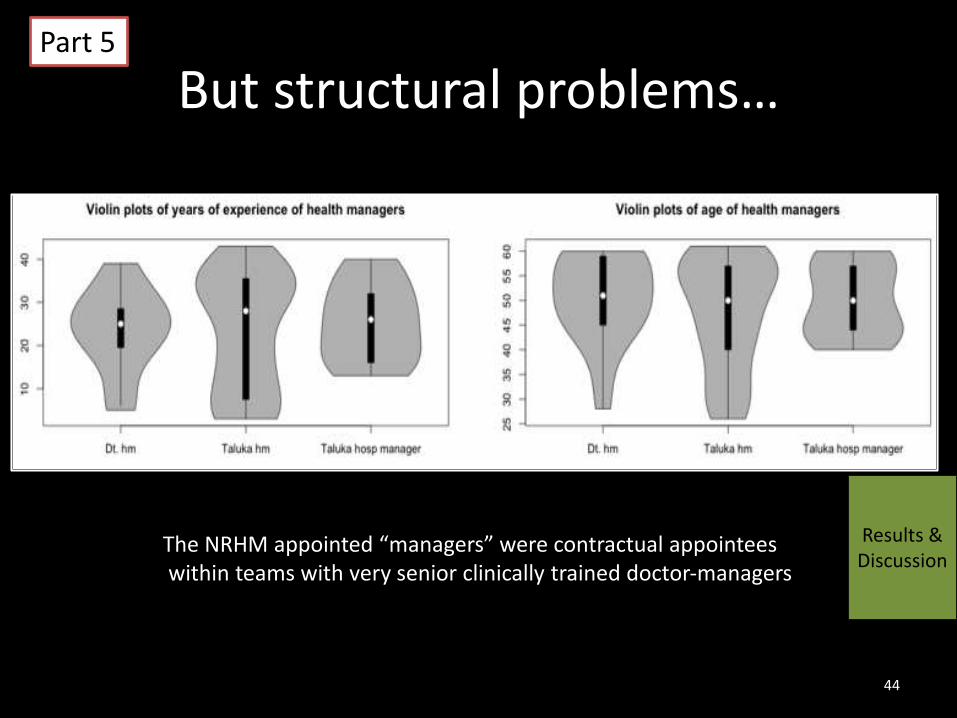
But structural problems…
44
The NRHM appointed “managers” were contractual appointeeswithin teams with very senior clinically trained doctor-managers
Results & Discussion
Part 5
“What is the use of putting my time into the PIP, if they will change it anyway at the state (level)?”
a district level health manager
“They seemed to make more noise than usual”
a senior state-level official
45
“At village level they do not really know much planning. They are actually not bothered about plans and all.”
a taluka health manager
“What do they know? After all, many of them are uneducated? What is the need for them to oversee our decisions?”
a taluka health manager
“BPMs should provide data as and when required and prepare good reports. They are too young and cannot understand the health department’s work.”
a taluka health manager
Part 5
Perceptions across the health bureaucracy
46
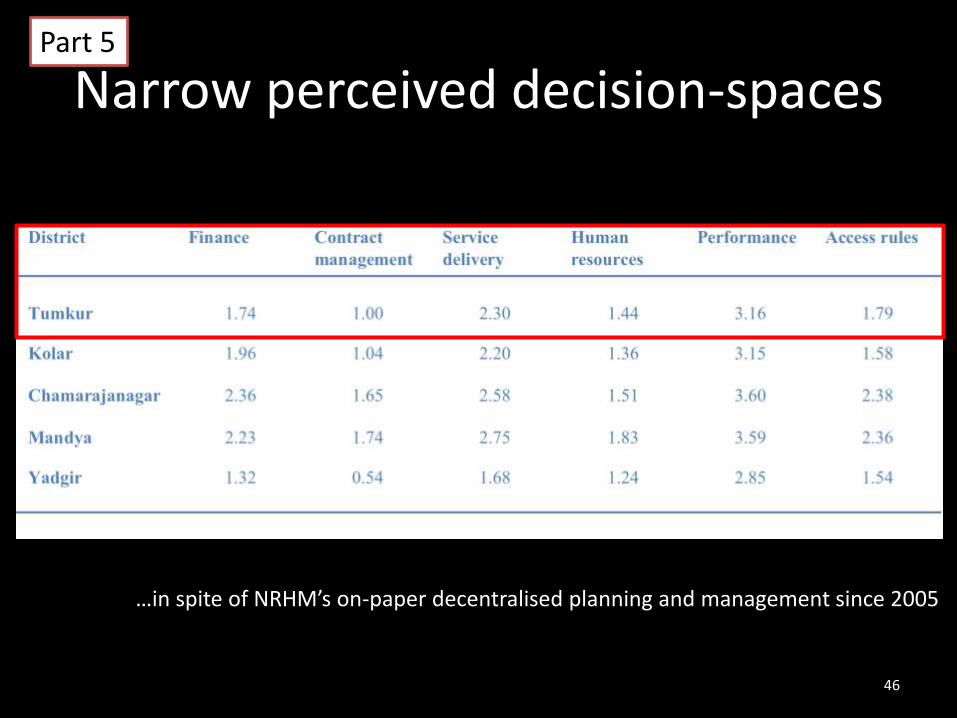
Narrow perceived decision-spaces
…in spite of NRHM’s on-paper decentralised planning and management since 2005
Part 5
47
Results & Discussion
Part 5
Case analysis
The hypothetical CMO frames offer a context-sensitive, theory-informed lens to analyse the intervention
– In purposively chosen talukas with and without a positive outcome (relate-able to the intervention), what were the differing contexts?
– What were the differences in the nature of commitment of the individuals in these contrasting talukas?
– ..…
48
Results & Discussion
Part 5
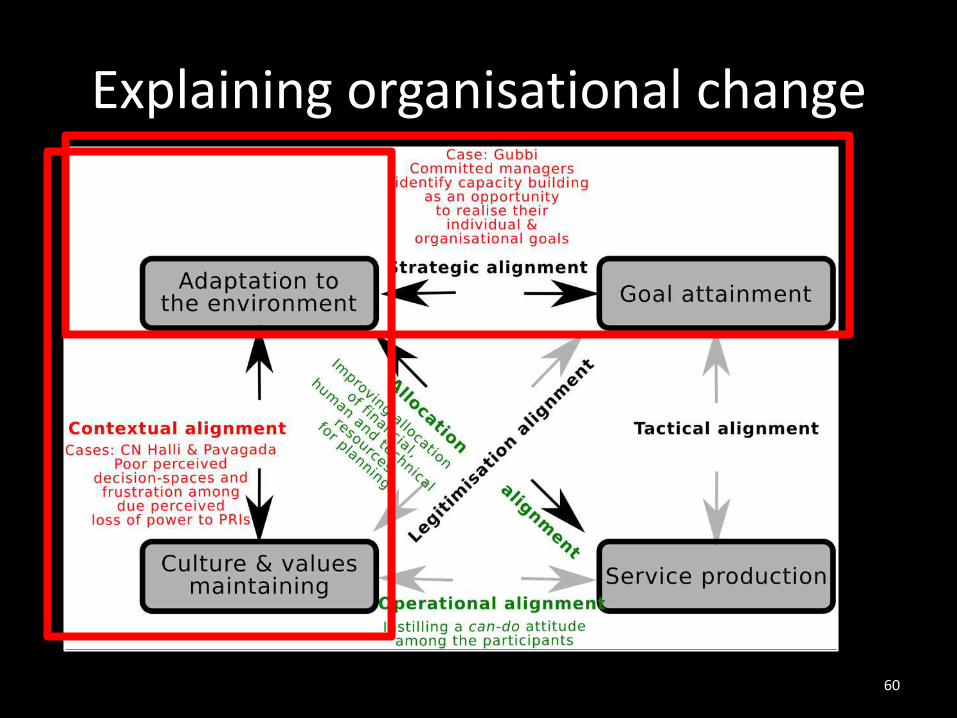
Explaining organisational change
• Identified case studies based on diversity of context and/or outcome after scanning context, mechanism and outcome elements
• Confronted the reformulated PT and first round of CMO-based change scenarios to these cases
49
Results & Discussion
Part 5
Case selection
• a mix of individual, organisational and contextual factors
– intervention exposure
– socio-economic development index of taluka
– mentoring interest & supervision received
– stability of team
– proxy measures of outcomes logically related to improvements in the talukas.
50
Results & Discussion
Part 5
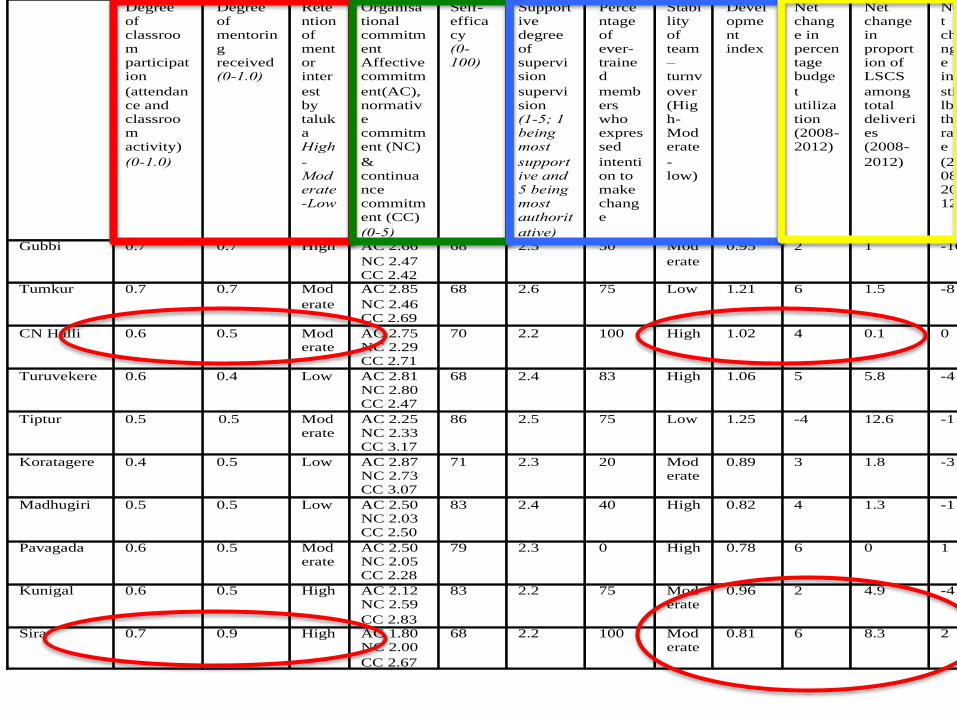
Degree of classroom participation
(attendance and classroom activity)
(0-1.0)
Degree of mentoring received (0-1.0)
Retention of mentor inter
est by taluka High
-Moderate-Low
Organisational commitment Affective commitm
ent(AC), normative commitment (NC)
& continuance commitment (CC)
(0-5)
Self-efficacy (0-100)
Supportive degree of supervision
supervision (1-5; 1 being most
supportive and 5 being most authorit
ative)
Percentage of ever-trained
members who expressed
intention to make change
Stability of team – turnv
over (High-Moderate
-low)
Development index
Net change in percentage budge
t utilization (2008-2012)
Net change in proportion of LSCS
among total deliveries (2008-
2012)
Net change in
stillbirth rate
(2008-2012)
Gubbi 0.7 0.7 High AC 2.66
NC 2.47 CC 2.42
68 2.5 50 Mod
erate
0.95 2 1 -16
Tumkur 0.7 0.7 Mod
erate
AC 2.85
NC 2.46 CC 2.69
68 2.6 75 Low 1.21 6 1.5 -8
CN Halli 0.6 0.5 Moderate
AC 2.75 NC 2.29 CC 2.71
70 2.2 100 High 1.02 4 0.1 0
Turuvekere 0.6 0.4 Low AC 2.81 NC 2.80 CC 2.47
68 2.4 83 High 1.06 5 5.8 -4
Tiptur 0.5 0.5 Moderate
AC 2.25 NC 2.33 CC 3.17
86 2.5 75 Low 1.25 -4 12.6 -1
Koratagere 0.4 0.5 Low AC 2.87 NC 2.73 CC 3.07
71 2.3 20 Moderate
0.89 3 1.8 -3
Madhugiri 0.5 0.5 Low AC 2.50 NC 2.03 CC 2.50
83 2.4 40 High 0.82 4 1.3 -1
Pavagada 0.6 0.5 Moderate
AC 2.50 NC 2.05 CC 2.28
79 2.3 0 High 0.78 6 0 1
Kunigal 0.6 0.5 High AC 2.12 NC 2.59
CC 2.83
83 2.2 75 Moderate
0.96 2 4.9 -4
Sira 0.7 0.9 High AC 1.80 NC 2.00
CC 2.67
68 2.2 100 Moderate
0.81 6 8.3 2
51
Committed and mentored teams with low-moderate intention to make change
“In my taluka for example, I think we can make big change. It is not that everybody in my taluka want to make changes. Only one-third of them are motivated to make changes. And that is enough. I think I can make a lot of improvement by motivating these people.”
- a Gubbi taluka helath manager
“More resources mean more opportunities to make change. If they slowly give more and more power to us at taluka level, we can make many more improvements. Right now, very little is possible at taluka level. “
- another taluka health manager from Gubbi (g2)
52
Results & Discussion
Part 5
Committed health management teams could utilise new opportunities for organisational improvement presented by decentralising health systems wherever their change agenda aligns with the expectations of higher levels of the bureaucracy.
53
What PIP? What decentralisation? I sent so many requirements for staff and proposals for improvement. Only thing I got is more work, less staff and zero solutions. On one hand, I have to answer the local ZP members’ complaints and on the other hand, I have to just keep implementing plans and schemes coming from above. Nothing can be done without more staff.
- a health manager from CN Halli (cnh1)
We felt that we have to do it. So many mothers were just being referred to Tumkur. The delivery load is high and for several months, we had only one obstetrician, but somehow we managed. I know how the pressure is at the distict hospital, so having LSCS facility at Sira decreases the burden at the district hospital. It’s not easy, but somehow it is happening.
- a Sira health manager (s1)
“Nothing much can be done without giving powers at taluka level and PHCs. I cannot even appoint a Group D staff. Where is decentralisation in this?”- a PHC staff from CN Halli taluka
Tapping commitment for organisational change could be frustrating in low-resource local health systems where health managers working in poorly resourced talukas, in spite of their improved management capacities and intentions to make change, could get frustrated by the lack of facilitating action from above.
Poorly resourced teams with varying commitment levels/types & high intention for change
Discussion, relevance and lessons learned
54
Results & DiscussionResults & Discussion
Part 6
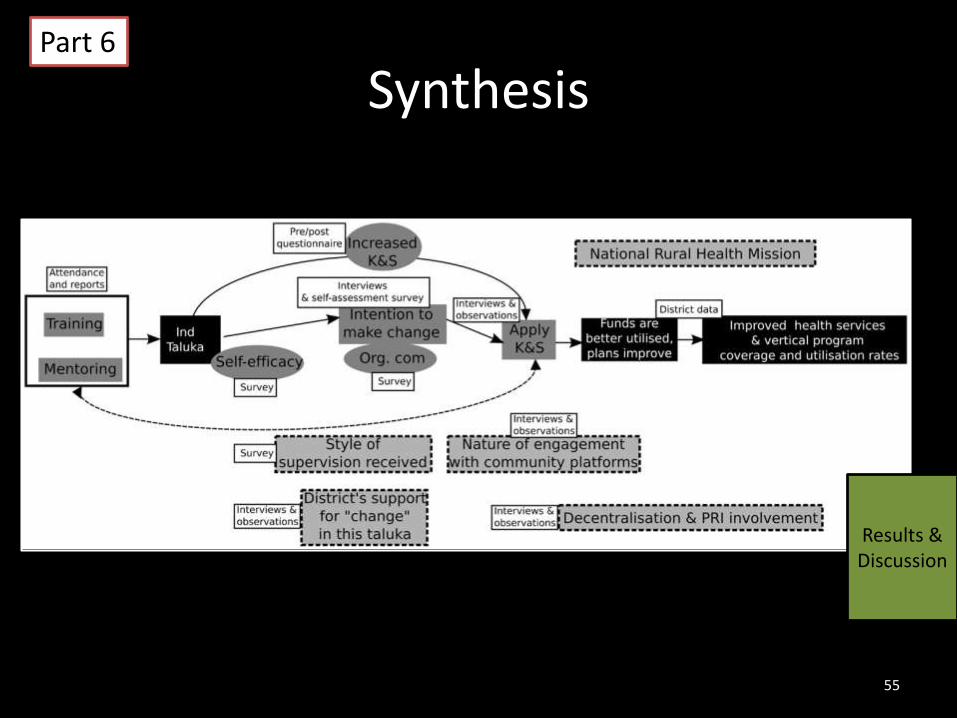
Synthesis
55
Results & Discussion
Part 6
Lessons learned – capacity building• Capacity building programmes seek to influence health
manager decisions and choices: capacity to manage alignments matter, not only determinants
• Pushing public health service organisations towards change in decentralising health organisations: need to engage with multiple levels in the bureaucracy
• Capacity building strategies need to invest more in local goal-setting and negotiation and coping skills of health managers, and not entirely focus on knowledge/skill transfer
• Capacity building programmes could seek to become the context for change through facilitating a desire for change(or harness pre-existing feeling of unhappiness with the current status) 56
Results & Discussion
Part 6
• Application of insights from organisational sciences and social sciences in health systems strengthening
• Using PT refinement and realist evaluation as an operational tool for implementation
• Need for more case diversity and further iterationscould improve the final refined theory
Lessons learned - methods
57
Results & Discussion
Part 6
Relevance• Building a human resources
management strategy for improved district health system functioning in Karnataka
• Improving the design of existing state and district level capacity building efforts
• Teaching material for teaching organisational change approaches within health servcies and for teaching theory-driven and realist approaches for evaluating healthcare interentions
58
Results & Discussion
Part 6
Thank you
59
Explaining organisational change
60
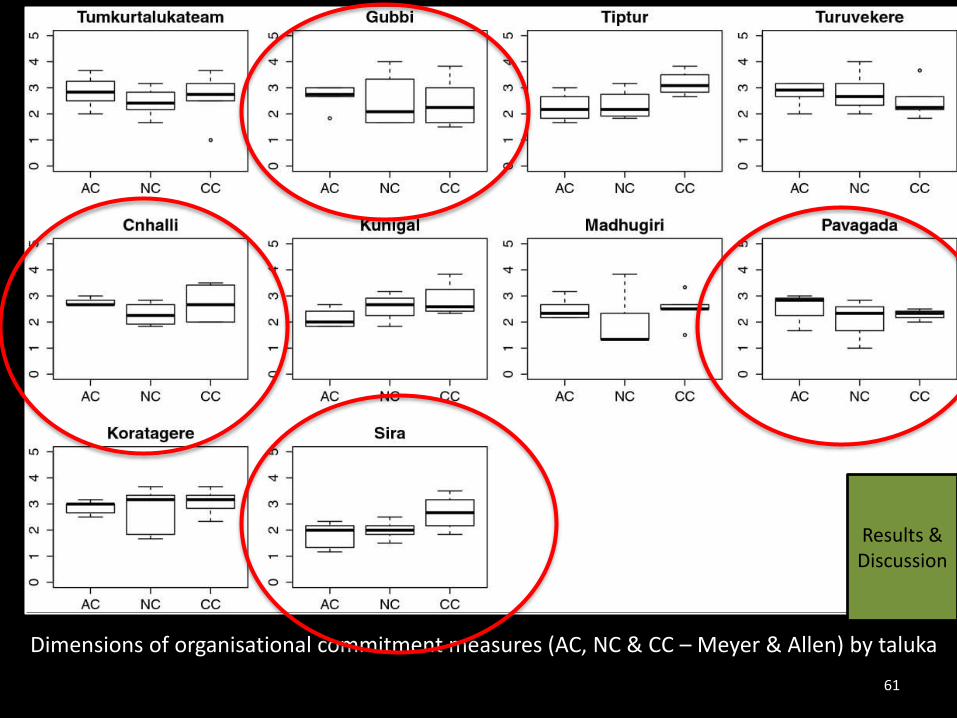
Dimensions of organisational commitment measures (AC, NC & CC – Meyer & Allen) by taluka
61
Results & Discussion