Embed Size (px)
Citation preview

CNS Tuberculosis
Guide:Dr.SL Mathur sir
Presented by Dr.Pradeep2/7/20151
Introduction
2/7/20152
Tuberculosis, MTB, or TB (short for tubercle bacillus), in the past also
called phthisis, phthisis pulmonalis, or consumption.
Tuberculosis is the major cause of death worldwide.
Causative agent –mycobacteria tuberculosis.first isolated by Robert Koch in
1882 who received Nobel prize for this discovery
Neutral on gram staining, acid fast to 20% H2SO4
• CNS tuberculosis occurs in upto 10% of those infected and if untreated
carries high mortality.

Classification of neurotuberculosis
2/7/20153
• Intracranial
- Tuberculous meningitis
- Tuberculoma
- Tuberculous abscess
- Tuberculous encephalopathy
- Tuberculous vasculopathy
• Spinal
- Pott’s spine and Pott’s paraplegia
- Tuberculous arachnoiditis
- Spinal tuberculoma
- Spinal meningitis

Pathology
2/7/20154
• T lymphocyte dependent necrotising granulomatous inflammatory response.
• Thick gelatinous exudate.
• Three processes cause most of the neurological deficits:
Hydrocephalous
Adhesive arachnoiditis
Obliterative vasculitis

Tuberculous meningitis (TBM)
2/7/20155
• Commonest form of neurotuberculosis (70 to 80%) .
• TBM is also the commonest form of chronic meningitis.
• Clinical features include h/o vague ill health for 2-8 weeks prior to
development of meningeal irritation.
Contd…

Tuberculous meningitis (TBM) Contd…
2/7/20156
• Signs of Meningeal irritation.
• Cranial nerve palsies (20-30%)
• papilloedema or rarely choroid tubercles, seizures, focal neurological deficits secondary to infarction.
• Visual loss
• Increasing lethargy, confusion, stupor, deep coma, decerebrate or decorticate rigidity.

Investigations
2/7/20157
CBC,ESR,CXR-PA,LFT,RFT
HIV
CSF examination:
CSF Smear examination:
CSF culture on solid media: .
Adjunctive tests : .
Molecular diagnosis :
CT/MRI

Sensitivity & specificity of various
diagnostic tests for TBM
Menzies et al, Ann Int Med. 2007; 146: 340-354.
Diagnostic
test
Sensitivity Specificity
ZN staining 10-20% 100%
LJ Culture 15% (25-80) 100%
BACTEC Culture 55% 100%
ELISA 52.3% 91.6%
TB PCR 56% 98%
TST 73% 56%
QTF-GOLD 76% 98%
ELISPOT 87% 92%
2/7/20158

Test Appearance Pressure WBC/μL Protein mg/dL Glucose mg/dL
Chloride
Normal CSF Clear 90 – 180 mm 0-5lymph. 15-45 50-80 115-130 mEq/L
Acute bacterial meningitis
Turbid Increased 1000 -10000 100 – 500 < 40 Decreased
Viral meningitis
Clear Normal to moderate increase
5-300, rarely >1000
Normal to mild increased
Normal Normal
Tuberculous meningitis
Slightly opaque cobweb formation
Increased/ decreased,
100-600 mixed Initially neutrophillic & later lymphocytic
50-300 Decreased Decreased
Fungal meningitis
Clear Increased 40-400 mixed 50-300 Decreased Decreased
2/7/20159

Staging of TBM
Modified MRC criteria
Grade I: Alert and oriented (GCS 15) without focal
neurological deficit.
Grade II:GCS 14-10 with or without focal neurological
deficit or GCS 15 with focal neurological deficit.
Grade III: GCS less than 10 with or without focal
neurological deficit.

Diagnostic criteria for TBM
2/7/201511
Patients with at least four of the following:
i. History of tuberculosis.
ii. Predominance of lymphoytes in the cerebrospinal fluid.
iii. A duration of illness of more than six days.
iv. A ratio of CSF glucose to plasma glucose of less than 0.5.
v. Altered consciousness
vi. Turbid cerebrospinal fluid.
vii. Focal neurologic signs.
Possible
Patients with one or more of the following:
i. Suspected active pulmonary TB on chest radiography.
ii. AFB found in any specimen other than the CSF.
iii. Clinical evidence of extrapulmonary tuberculosis.
Probable
Acid-fast bacilli seen in the cerebrospinal fluid.Definite
DefinitionClass
Thwaites GE et al. Diagnosis of adult tuberculosis meningitis by use of clinical and laboratory features.
Lancet 2002; 360: 1287-92.

Management
Therapy:
Isoniazid – 5mg/kgd
Rifampicin – 10mg/kg/d
Pyrazinamide – 30mg/kg/d
Ethambutol – 15-25 mg/kg/d
Pyridoxine – 50mg/day
Ofloxacin-200mg BD
Dexamethasone for 8 weeks.
2/7/201512

Tuberculous brain abscess
2/7/201513

Tuberculous encephalopathy
2/7/201514
• Seen in infants and children.
• Characterized by convulsions, stupor and coma with signs of
meningeal irritation or focal neurological deficit.

Tuberculoma
2/7/201515

Spinal Tuberculosis
2/7/201516
Potts spine

Spinal form of tuberculous meningitis
2/7/201517
• May result from rupture of Rich foci in the spinal arachnoid space.
• The acute form presents with fever, headache, and root pains
accompanied by myelopathy.
• The chronic form presents with spinal cord compression.

WHO Recommended TB treatment
regimen
Drug regimens
Initial phase- first 2-3 months
During the initial phase, there is rapid killing of TB bacilli
Three or more drugs are used in combination
Infectious patients become non-infectious within about 2
weeks and symptoms usually improve
Continuation phase- additional 4-6 months
• Fewer drugs are necessary (usually 2), but longer time
• These drugs eliminate the remaining bacilli
Directly Observed Treatment Strategy (DOTS)
DOTS is a strategy for TB control which aims to detect 70 percent of
active TB cases and to successfully treat 85 percent of them2/7/201518
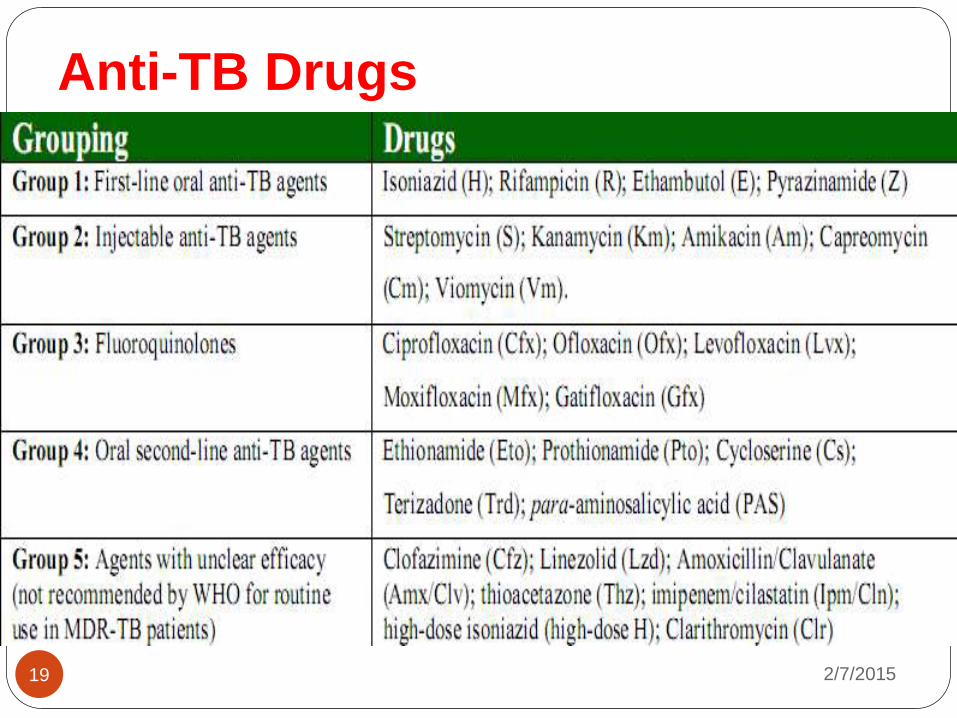
Anti-TB Drugs
2/7/201519

2/7/201520

Antiretroviral Therapy for Individuals with
Tuberculosis Co infection
WHO guidelines:Recommendation for public health approach -2010
revision.
ART should be started in all TB patients, including drug-resistant TB,
irrespective of the CD4 count
AKT should be initiated first, followed by ART as soon as possible within the
first 8 weeks of treatment.
HIV-positive TB patients with profound immunosuppression (CD4 <50)
should receive ART immediately within the first 2 weeks of AKT .
2/7/201521

Adjunctive steroid therapy
2/7/201522
• The rationale behind the use of steroids includes the reduction of
inflammation within the subarachnoid space.
• The largest RCT in TBM recommends dexamethasone treatment in
patient with TBM for 8 weeks.
Thwaites GE et al. N Engl J Med 2004; 351: 1741-51;
Lancet Neurol 2007; 6: 280-6.

Role of surgery in CNS tuberculosis
2/7/201523
• Hydrocephalus
• Tuberculous cerebral abscess
• vertebral tuberculosis with paraparesis are all indications for
neurosurgical referral .

2/7/201524