Embed Size (px)
Citation preview
The Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea
By:
Mazi Ejeckam Chukwuebuka . C.
6th October 2017
Preston Healthcare Consulting

Outline: Understanding Pneumonia
Background, Aetiology, Transmission, Prevention & Treatment
Understanding Diarrhoea Background, Aetiology , Transmission, Prevention & Treatment
GAPP Basic Intervention
GAPPD- Fore runners
Sustainable Development Goal 3
GAPPD - Background
Outline –cont’d 15 High Burden States
GAPPD- PPT Framework
GAPPD- Closing the Gap
GAPPD- Goals, Targets & Indicators
GAPPD – Country Level Actions
GAPPD: Scorecard Indicators
GAPPD- 2016 Assessment Highlights
Nigeria Highlights
Challenges & Opportunities
References
Tolstoy
Harrison
Tubman
Puskas
Pavorroti
Candido
BackgroundPneumonia is a form of acute respiratory infection that affects the lungs, caused by a number of infectious agents – bacteria, viruses and fungi.
Pneumonia is the single largest infectious cause of death, accounting for 16% of all deaths of children under 5 in 2015.
Pneumonia is also a leading infectious cause of death in developed countries. Pneumonia is referred as the ‘’ forgotten killer” because historically it has received little attention despite it’s importance.
Pneumonia is most prevalent in South-Asia and Sub-Saharan Africa, killing more children than those from HIV/AIDs, malaria and measles combined.
Economic cost of pneumonia is estimated at around 109 million USD per year. This includes price of antibiotics and diagnostics of pneumonia management
Pneumonia can be prevented using simple interventions, treated with low-cost, low- medication and care.
Background : NigeriaIn 2010, an estimated 868,000 under five died in Nigeria via Pneumonia. Pneumonia is the second leading cause of death killing more 140,000 children each year.
Nigeria is second only to India in the total number of childhood deaths via Pneumonia.
In 2012, Nigeria introduced the pentavalent vaccine which protects against Hib, Pneumonia and meningitis, along with other four childhood diseases.
Though there are wide gaps, Nigeria has made appreciable gains with regards to immunization coverage across all vaccine schedule. Between 2000-2010,DTP3 coverage more than doubled from 29% to 69% (WHO).
Aetiologic Agents
Bacteria
• Streptococcus Pneumoniae
• Haemophilus Influenza type b(Hib)
Virus
• Respiratory Syncytial Virus
• Inflluenza Virus
• Para-influenza Virus
Fungi
• Coccidioides
• Blastomyces
• Aspergillus
• Cryptococus
• Pneumocystis JiroveciPneumonia
TransmissionThe viruses and bacteria that are found in a child’s nose or throat can infect the lungs if inhaled.
Can also spread via air-borne droplets from cough or sneeze.
Can also be spread or transmitted through blood, especially during and shortly after child birth
Risk FactorsImmuno- compromised children, whose natural defence lines are weakened, are at a higher risk of developing Pneumonia ( Malnutrition or undernourishment especially in infants not exclusively breastfed).
Pre-existing infections, such as symptomatic HIV infections and measles, also increases a child risk of contracting Pneumonia.
Environmental factors : Indoor air pollution caused by cooking and heating with biomass fuel ( wood & dung), Living in crowded homes, etc.
Parental smoking also exposes an infant to the risk of developing Pneumonia.
Prevention Preventing pneumonia in children is an essential component of the strategy to reduce child mortality. Immunization against Hib,pneumococcus, measles and whooping cough (pertussis) is the most effective way to prevent pneumonia.
Adequate nutrition is key to improving children’s natural defences, starting with exclusive breastfeeding for the first 6 months of life. In addition to being effective in preventing pneumonia, it also helps to reduce the length of the illness if a child does become ill.
Addressing environmental factors – provision of clean affordable indoor stoves and encouraging good hygiene in crowded homes.
In children infected with HIV, cotrimoxazole is given daily to reduce risk of contracting pneumonia.

TreatmentAmoxicillin dispersible tablet is the antibiotic of choice for the treatment of pneumonia. Most cases will require oral antibiotics which are prescribed at health centres.
Hospitalization is recommended only for severe cases of pneumonia.
In 2009, WHO & UNICEF released GAPP showing that pneumonia deaths could be reduced by 2/3 if existing interventions could be scaled up to 90 percent of the world children. There are 6 basic strategic intervention to achieve the above target-

6 Basic GAPP Intervention (WHO/UNICEF)
Reducing Indoor Air Pollution
Immunization with vaccines against Hib, Pneumococcus, Measles and Pertusis
Effective Case management and treatment at community level.
Exclusive Breastfeeding for the first 6 months and providing zinc supplementation
Con’td
Preventing Mother-To-Child Transmission of HIV
Promoting Regular Hand Washing
DiarrhoeaDiarrhoea – passage of unusually loose or watery stool at least 3 times in 24 hours. For infants especially, stool consistency/integrity rather than frequency is most important.
Diarrhoea is the second leading cause of death in children <5, accounting for 9% of under five mortality. Globally, there are 1.7 billion cases of childhood diarrhoea every year, resulting in about 525000 mortalities annually.
According to a 2016 UNICEF global WASH fact sheet, 2,200 children die every day as a result of diarrhoea disease in low and middle income countries (LMIC).
Diarrhoea is usually a symptom of the infestation of the intestinal tract which can be caused by a variety of bacteria, viral and parasitic organisms.
Diarrhoea infection is spread through contaminated food or drinking water, or from person-to-person as a result of poor hygiene. 88% of death from diarrhoea are from unsafe drinking water, inadequate availability of water for hygiene and lack of access to sanitation.
There are simple interventions to treat diarrhoea ranging from the provision of safe drinking water, use of improved sanitation and hand washing using soap.

Clinical Presentation & Aetiology
Acute Watery Diarrhoea ( last for several hours or days, includes chorela .
Common aetiologic agents includes V.cholera,
E.coli and Rotavirus.
Acute Bloody Diarrhoea (last for 3-6 weeks, also termed dysentery with mucus and/or blood in
stool. Common aetiologic agent is Shigella bacteria.
Persistent Diarrhoea (last 14 days or longer with or
without blood loss). Commonly affects
malnourished children and those with illnesses
such as AIDs.

Transmission & PreventionTransmission
Diarrhoea disease can spread from person-to-person aggravated by poor personal hygiene.
Food prepared or stored in very unhygienic conditions. Fish and seafood from polluted water may also contribute to the disease.
Unsafe domestic water storage and handling is also a critical risk factors.
Prevention
Access to safe drinking water
Use of improved sanitation
Exclusive breastfeeding for the first 6 months of life
Good personal and food hygiene
Health education about how infections spread
Rotavirus vaccination
TreatmentRehydration – with Oral Rehydration Salt (ORS). Rehydration with intravenous fluids in case of severe dehydration or shock.
Zinc supplement- reduces episode by 25% and associated with a 30% reduction in stool volume.
Nutrient rich food-like breast milk during episode and EBS for the first 6 months of life.
Consulting a health professional in particular for management of persistent diarrhoea.



Treatment Con’td
GAPPD : Ending Two Major Preventable Causes of Child Death – the fore runnersUnited Nations Global Strategy for Women’s and Children’s Health (2010) – calls for a continuum of care approach, aiming to save 16 million lives. With Every Woman Every Child (EWEC), efforts have continued.
Call to Action: Committing to Child Survival- A promise Renewed (2012) – Global community to reduce child mortality to 20 or fewer deaths per 1000 live births by 2035
Global Vaccine Action Plan (GVAP, 2012)-strategy for preventing childhood diseases through vaccination.
United Nations Sustainable Energy for All Initiative – a public –private commitment to universal access to modern energy services by 2030
United Nations Commission on Life Saving Commodities (2012)– recommendations to strengthen access to and use of saving commodities including treatment for diarrhoea and pneumonia
United Nations Commission on Information & Accountability – improved monitoring of programmes to protect women and children’s health.
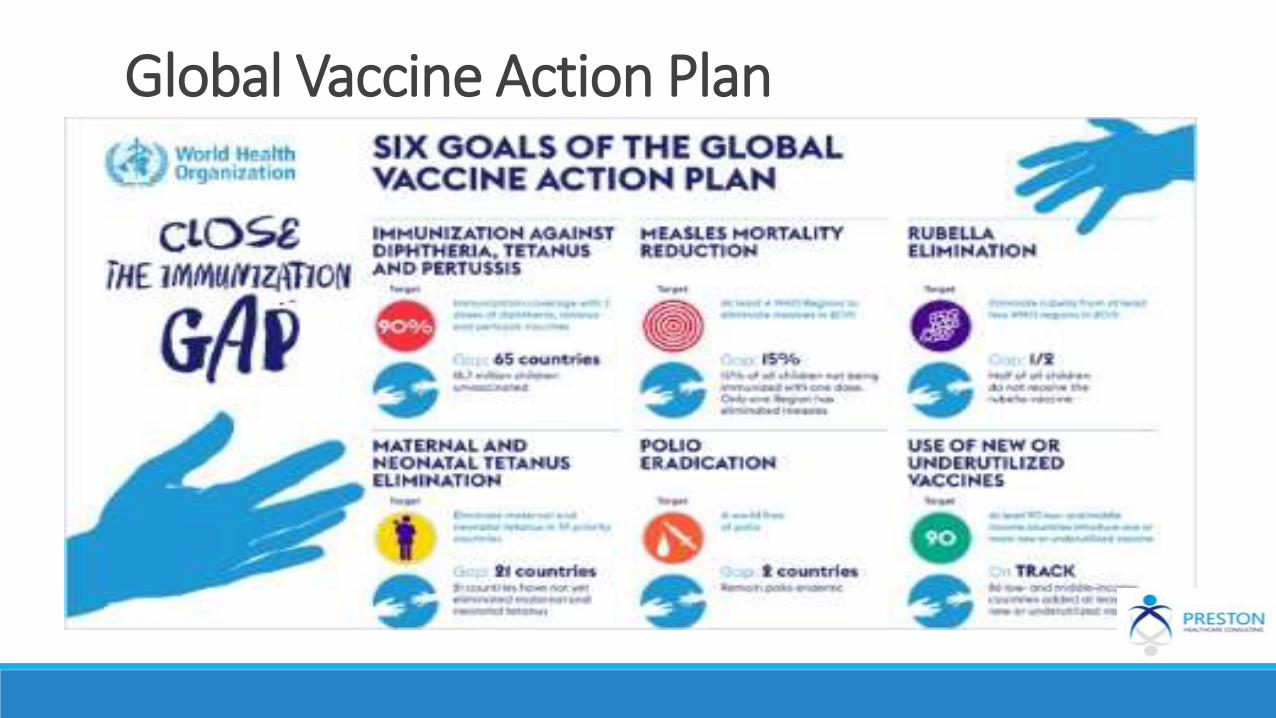
Global Vaccine Action Plan
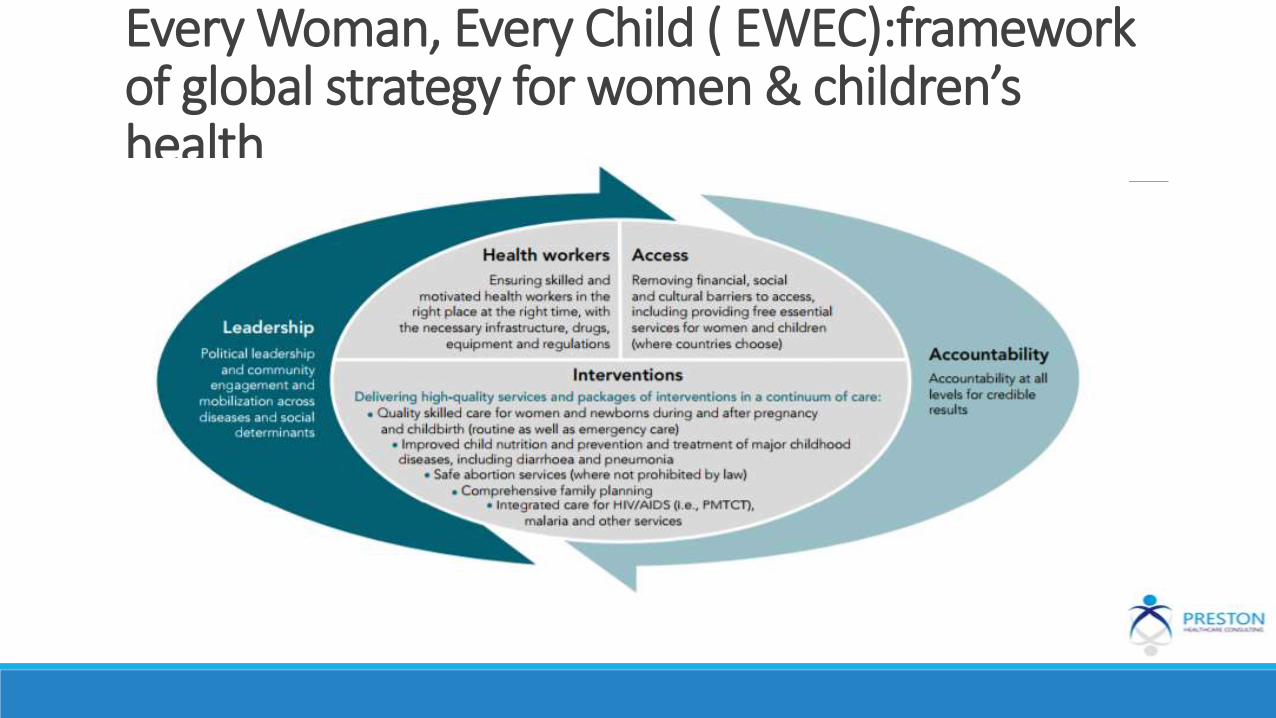
Every Woman, Every Child ( EWEC):framework of global strategy for women & children’s health

Sustainable Development Goal
Goal 3: Ensure Healthy Lives and Promote Wellbeing for All in All Ages
Target 3.2: Reducing Death in Children under 5 years of age to at least as low as 25 per 1000 live births.

Integrated Global Action Plan for Prevention of Pneumonia & Diarrhoea (GAPPD) - Background
In 2009, W.H.O,UNICEF and partners published 2 separate strategies for control of pneumonia and diarrhoea-GlobalAction Plan for Prevention and Control of Pneumonia (GAPPD) and a Diarrhoea Disease Prevention and Control Strategy-Diarrhoea: Why Children are still dying and what can be done.
Since these strategies were launched, it’s been recognised that (1) Pneumonia & Diarrhoea are most effectively addressed in a coordinated manner(2) Share same determinants as well as same control strategies and delivery system ( 3) Both are caused by multiple pathogen and no single intervention will manage either problem (4) Many countries are already addressing these diseases jointly through inter-sectoral working group, integrating protection, prevention and treatment.
GAPPD, an integrated 2013 plan from W.H.O and UNICEF representing the first-ever simultaneous plan to address childhood Pneumonia & Diarrhoea. Target is set for 2013 – 2025-2030.
Designed to inform national program and policies, providing a cohesive framework to PROTECT children, PREVENTdisease and TREAT children who do become sick using proven interventions that have already contributed to reductions in child death.
Country level performances are assessed via a GAPPD intervention scorecard developed by IVAC (John Hopkins Bloomberg School of public health) across 10 key GAPPD indicators using available coverage data.
The GAPPD scorecard assessment specifically focuses on the 15 most burdened states – Nine of which are in Africa & 6 in the Asian pacific both in 2014 and2016 –carries 72% of the global burden of pneumonia/diarrhoea child death even though they are home to only 55% of the world > 5 population.
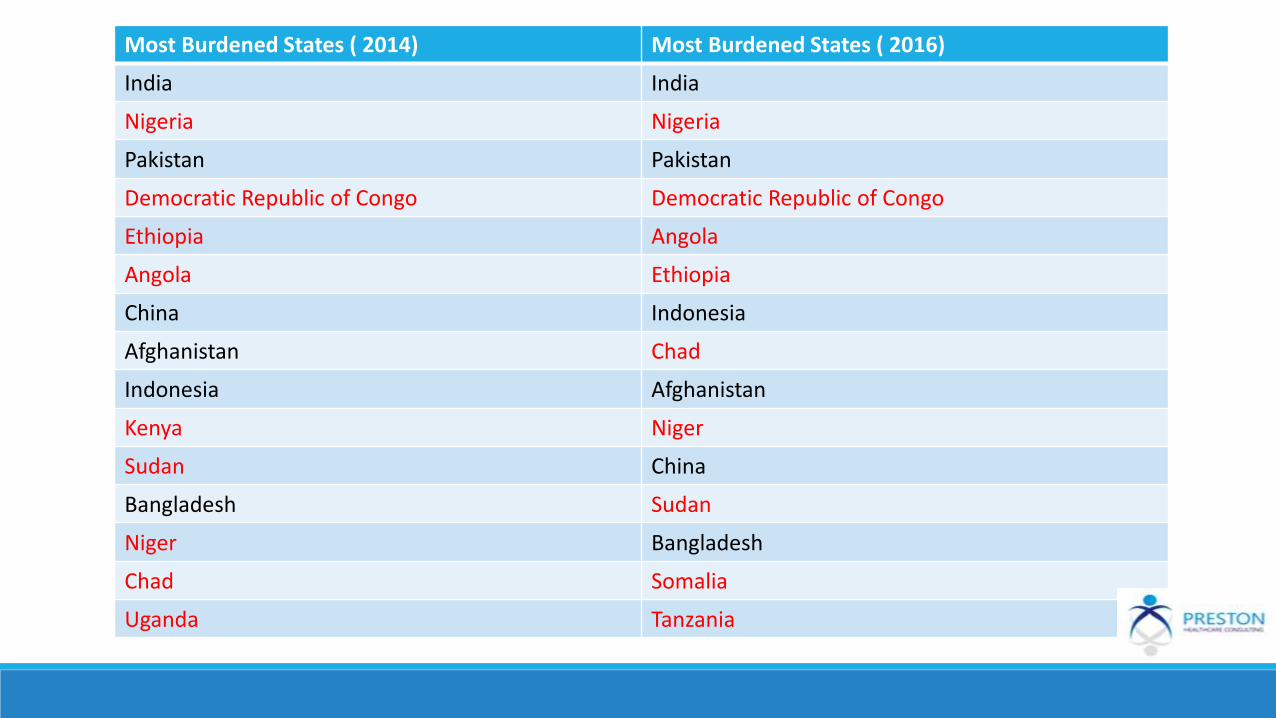
Most Burdened States ( 2014) Most Burdened States ( 2016)
India India
Nigeria Nigeria
Pakistan Pakistan
Democratic Republic of Congo Democratic Republic of Congo
Ethiopia Angola
Angola Ethiopia
China Indonesia
Afghanistan Chad
Indonesia Afghanistan
Kenya Niger
Sudan China
Bangladesh Sudan
Niger Bangladesh
Chad Somalia
Uganda Tanzania
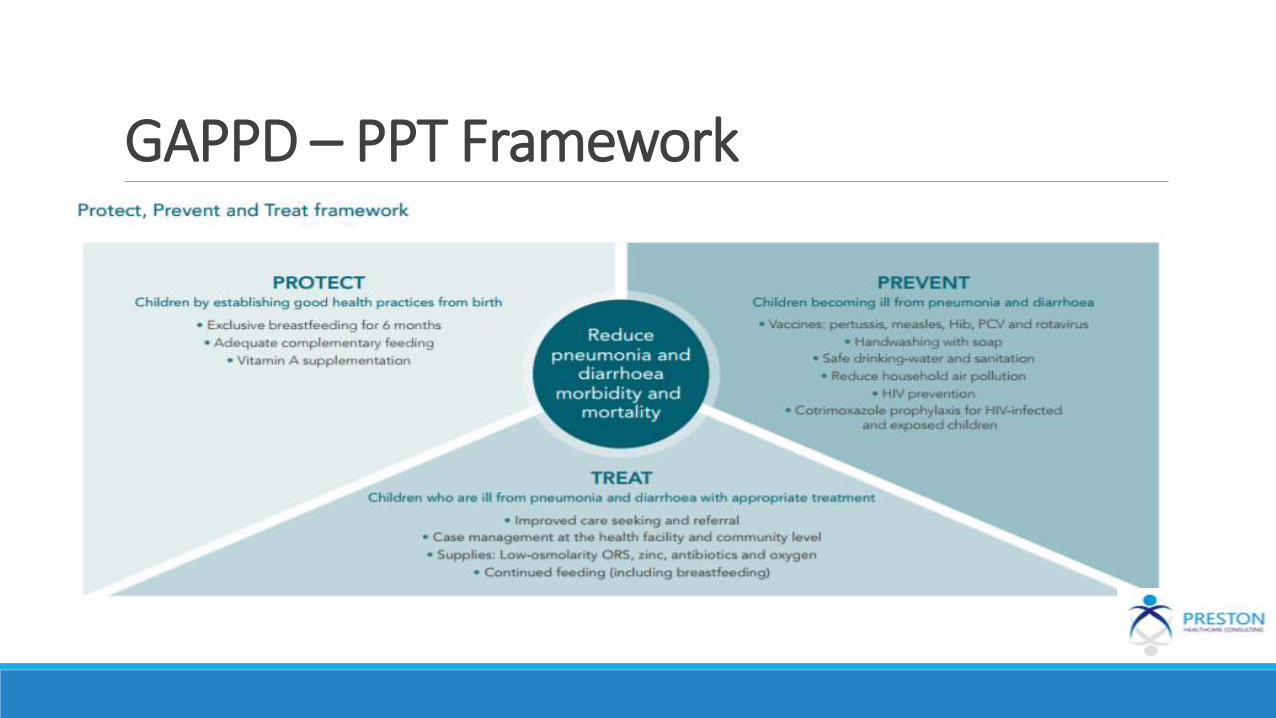
GAPPD – PPT Framework
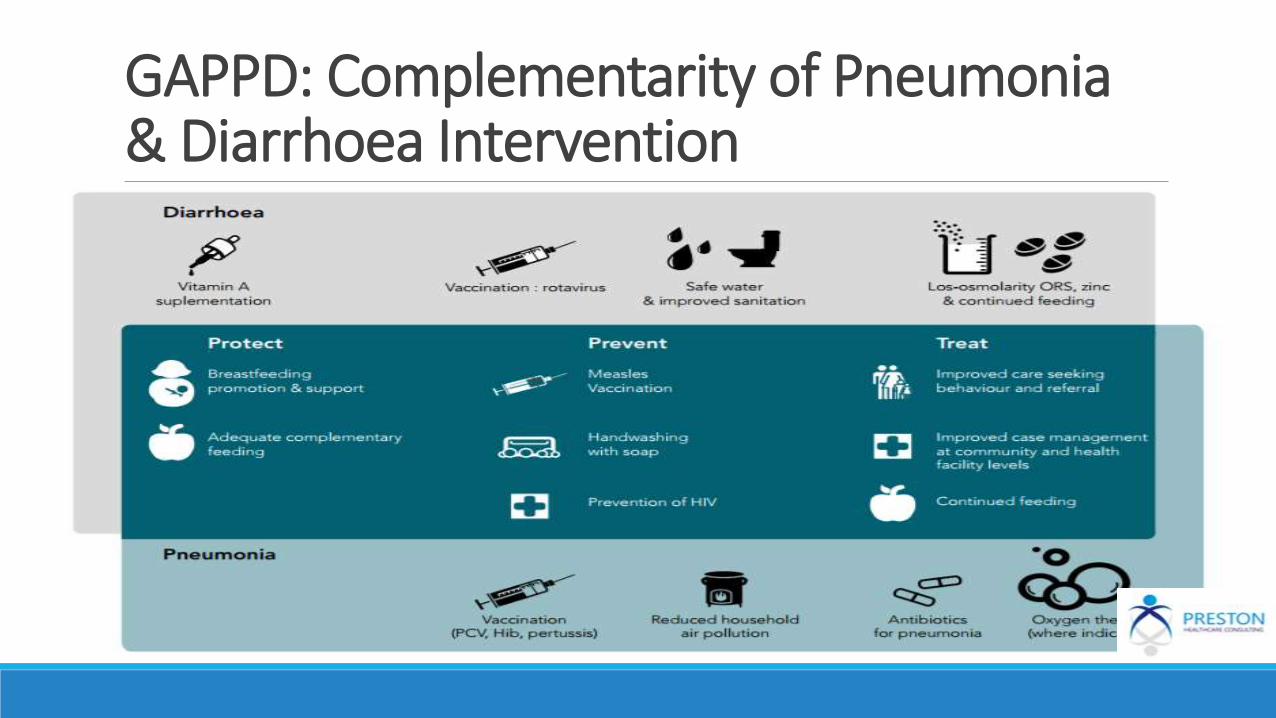
GAPPD: Complementarity of Pneumonia & Diarrhoea Intervention
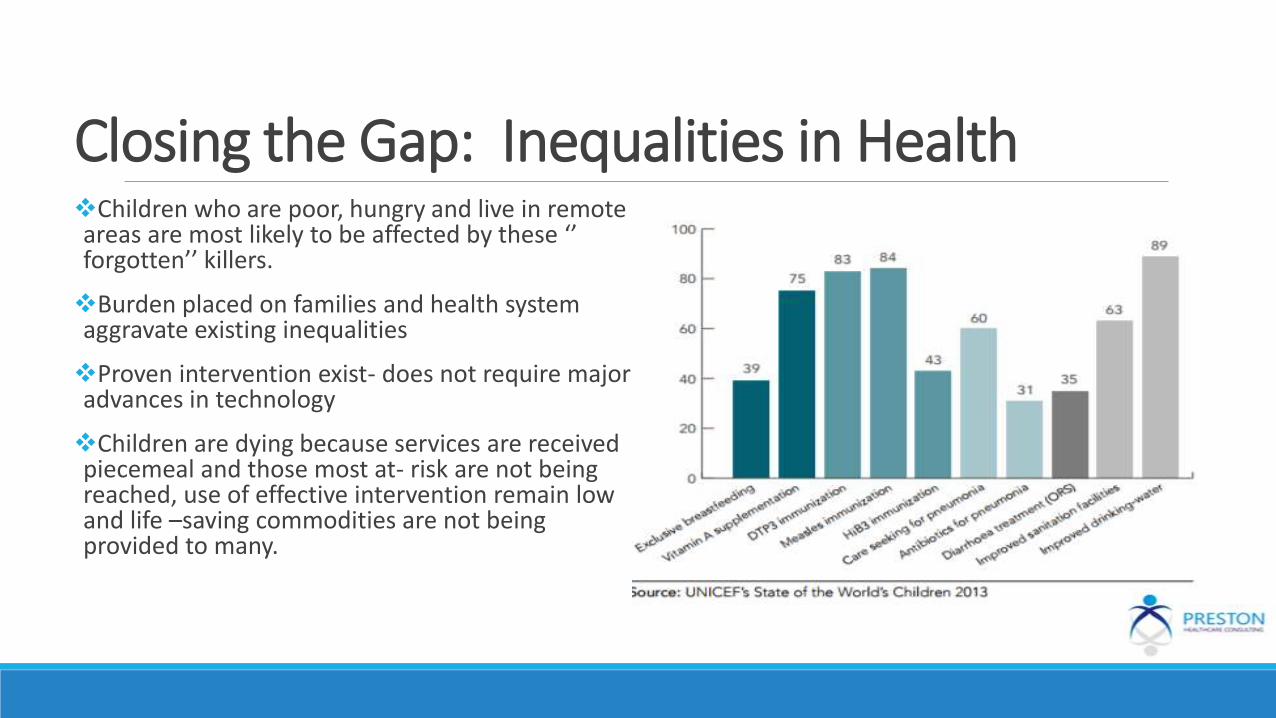
Closing the Gap: Inequalities in HealthChildren who are poor, hungry and live in remote areas are most likely to be affected by these ‘’ forgotten’’ killers.
Burden placed on families and health system aggravate existing inequalities
Proven intervention exist- does not require major advances in technology
Children are dying because services are received piecemeal and those most at- risk are not being reached, use of effective intervention remain low and life –saving commodities are not being provided to many.
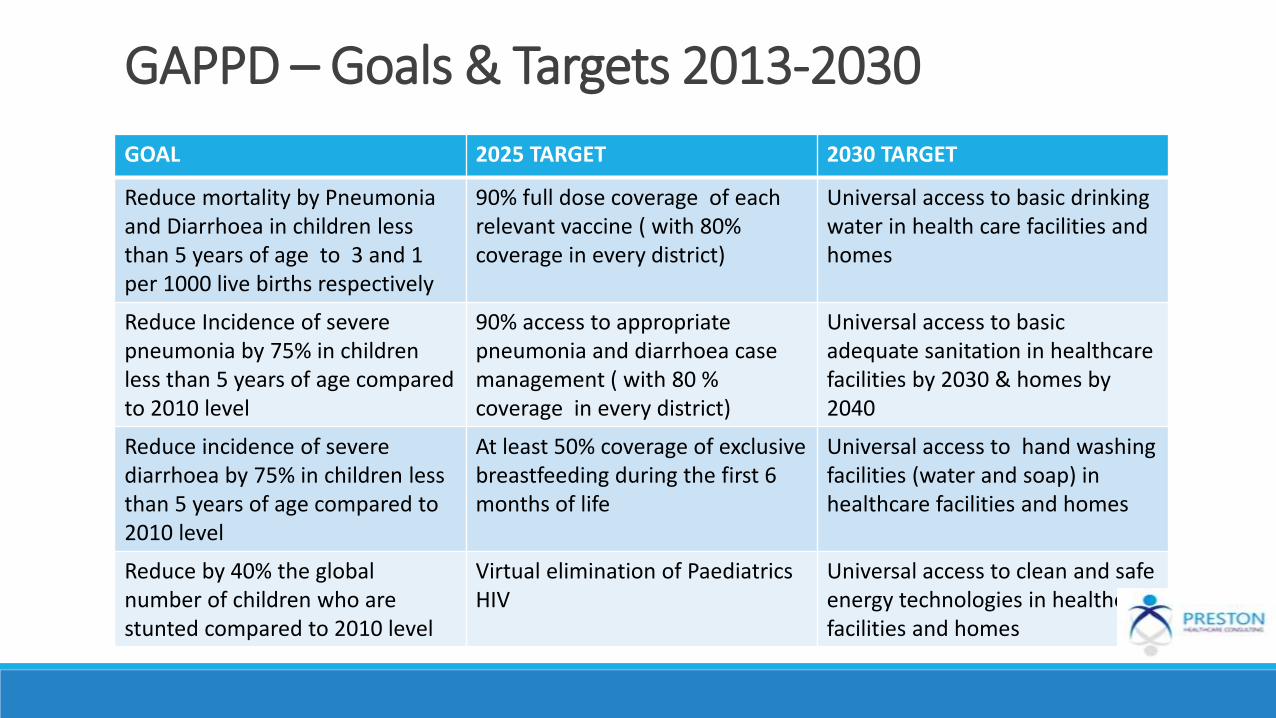
GAPPD – Goals & Targets 2013-2030
GOAL 2025 TARGET 2030 TARGET
Reduce mortality by Pneumonia and Diarrhoea in children less than 5 years of age to 3 and 1 per 1000 live births respectively
90% full dose coverage of each relevant vaccine ( with 80% coverage in every district)
Universal access to basic drinking water in health care facilities and homes
Reduce Incidence of severe pneumonia by 75% in children less than 5 years of age compared to 2010 level
90% access to appropriate pneumonia and diarrhoea case management ( with 80 % coverage in every district)
Universal access to basic adequate sanitation in healthcare facilities by 2030 & homes by 2040
Reduce incidence of severe diarrhoea by 75% in children less than 5 years of age compared to 2010 level
At least 50% coverage of exclusive breastfeeding during the first 6 months of life
Universal access to hand washing facilities (water and soap) in healthcare facilities and homes
Reduce by 40% the global number of children who are stunted compared to 2010 level
Virtual elimination of PaediatricsHIV
Universal access to clean and safeenergy technologies in healthcare facilities and homes
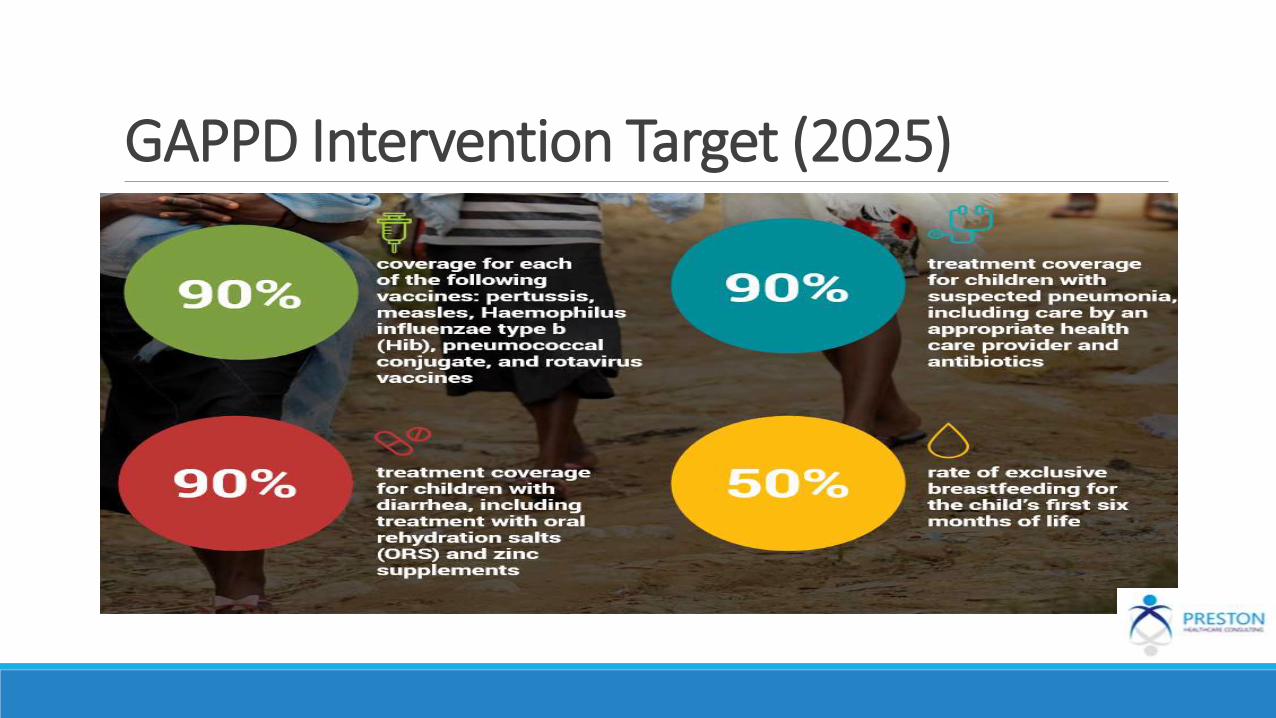
GAPPD Intervention Target (2025)
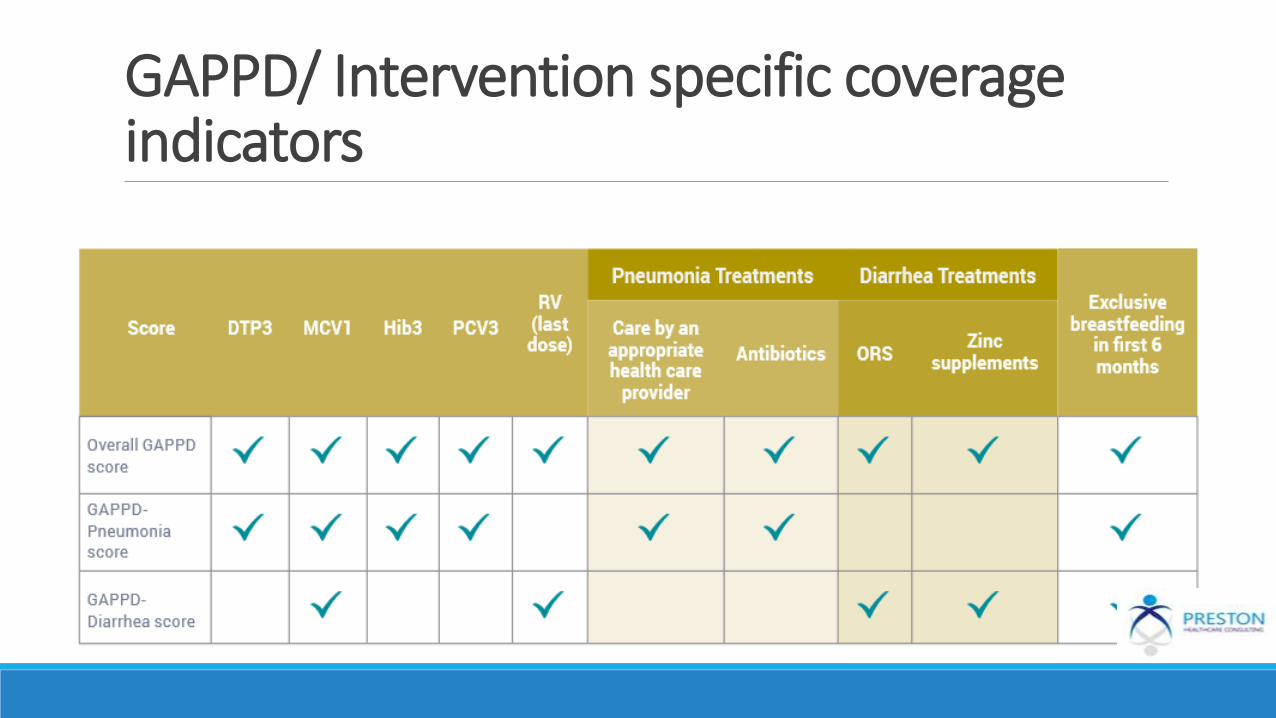
GAPPD/ Intervention specific coverage indicators

GAPPD: Actions at Country LevelDevelop a clear country-level strategy and work plan, with key responsibilities assigned
Coordinate implementation of interventions
Generate political will and prioritize interventions
Designate a national working group for pneumonia and diarrhoea prevention and control or review membership of an appropriate existing group
Develop/update a situation analysis for pneumonia & diarrhoea
Mobilize resources
Identify areas of harmonization and collaboration between programmes and sectors, including the private sector, academia and civil society
Apply lessons from other integrated disease prevention and control efforts
Use data to identify groups at greater risk or missed by services and develop targeted approaches to reach them and develop a set of common indicators for tracking progress.
Track execution and progress
Develop/update a costed plan for accelerated action
Take and/or assign accountability for action
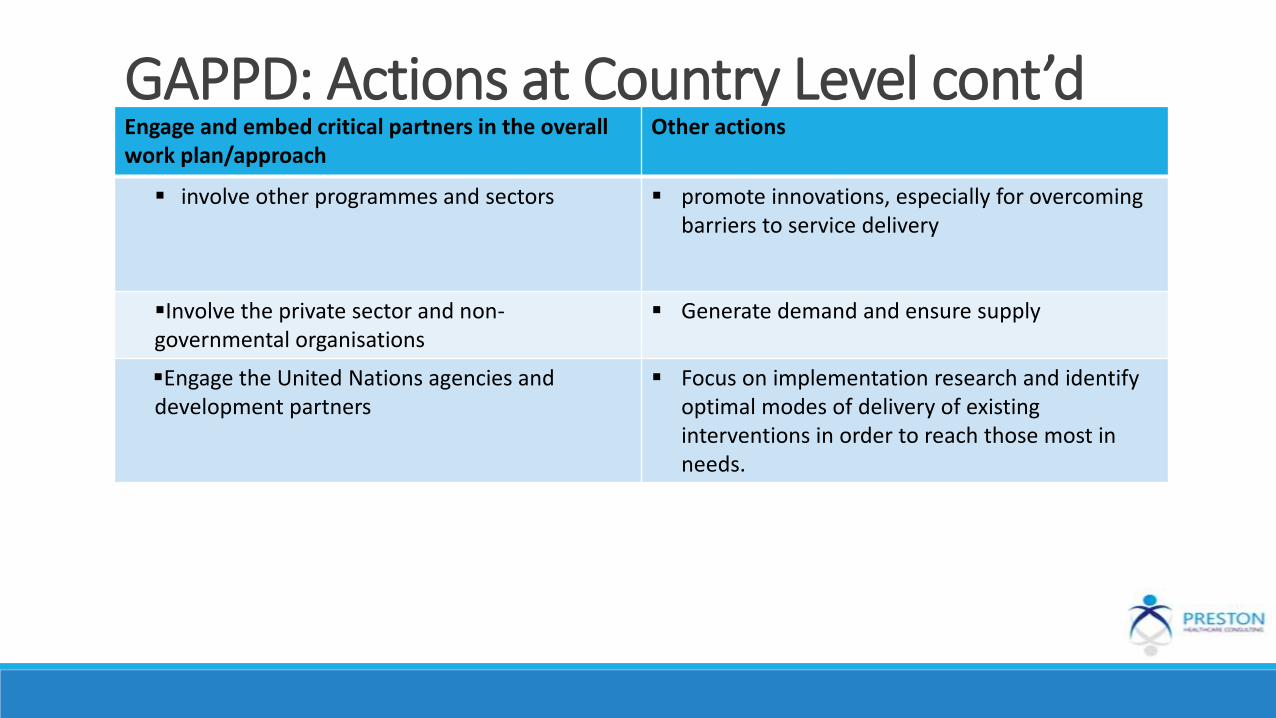
GAPPD: Actions at Country Level cont’dEngage and embed critical partners in the overall work plan/approach
Other actions
involve other programmes and sectors promote innovations, especially for overcoming barriers to service delivery
Involve the private sector and non-governmental organisations
Generate demand and ensure supply
Engage the United Nations agencies and development partners
Focus on implementation research and identify optimal modes of delivery of existing interventions in order to reach those most in needs.
10 GAPPD Intervention Scorecard IndicatorsCoverage rates for third dose of pertussis vaccine
Coverage rates for Measles containing vaccine(MCV)
Coverage rates for third dose of Hib vaccine
Coverage rates for third dose of Pneumococcal vaccine
Coverage rate for last dose of rotavirus vaccine
Access to appropriate healthcare provider
Antibiotic treatment for children with suspected Pneumonia
Treatment with Oral Rehydration Salt(ORT)
Zinc supplements for children with diarrhoea
Exclusive breastfeeding for a child in the first six months of life
GAPPD – 2016 Assessment Scorecard HighlightsOverall GAPPD scores varied widely from as low as 20% ( Somalia) to 74% (Tanzania)
The median score among the 15 high burden states was 48% - a point above the 2015 median score of 47%
None of the 15 high burden states met the 86% target for overall GAPPD assessment score.
5 countries met atleast 50% -(minimal threshold target ) – Afghanistan, Sudan,Bangladesh,Ethiopia and Tanzania
Countries with the highest under 5 pneumonia and diarrhoea deaths ( India, Pakistan, Nigeria & DRC) have overall GAPPD score less than 50%
Ethiopia & Tanzania ( countries with the highest overall GAPPD score) are using all five vaccines preventive against pneumonia & diarrhoea and are achieving relatively coverage with each vaccine
Nigeria - Highlights
Compared to 2015, Nigeria only made a moderate +3% increase in 2016.
In the 2014 report, GAPPD state level data ranges from 2% ( Sokoto & Kebbi) to 49% in EkitiState. 7 states had below 10%
Geographic patterns in GAPPD scores by states shows that southern states with higher scores having lower under 5 mortalities when compared to northern states with low GAPPD scores ( a pattern also noticed in India).
Urban – Rural disparities also existed in vaccine coverage ( 37% and 31%) for pentavelent and measles respectively. This was also observed with regards to treatment although the differences were relatively smaller .
Challenges & Opportunities

ReferencesGAPPD: Pneumonia and Diarrhoea Progress Report (2014), IVAC/ John Hopkins Bloomberg School of Public Health
GAPPD: Pneumonia and Diarrhoea Progress Report (2016), IVAC/ John Hopkins Bloomberg School of Public Health
Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025 – the Integrated Global Action Plan for Pneumonia & Diarrhoea
Nigeria: Diarrhoea Diseases – World Health Ranking, May 2014
Fight Pneumonia – Final Report of Small Grant Program In Nigeria, 2011
‘’ Intervention to Prevent Pneumonia exist – the challenge is delivering them to children who need them. Overcoming these hurdles will save the lives of millions of children’’
Orin Levine, PhD (Executive Director, International Vaccine Access Centre)