Embed Size (px)
Citation preview
Dr. Francis Nwachukwu Ukwuije
Snr. Health Economist Healthcare Financing Equity & Investment,
HSS, DHPR&S FMOH
06 February, 2017
Federal Ministry of Health
Where is Nigeria on Universal Health Coverage (UHC)?
World Health Assembly (WHA) Resolution 2005: urged countries to develop their health financing systems to: Ensure all people have access
to needed key promotive, preventive, curative and rehabilitative health services of good quality at an affordable cost without the risk of financial hardship linked to paying for care.
Definition of Universal Health Coverage (UHC)
3
4
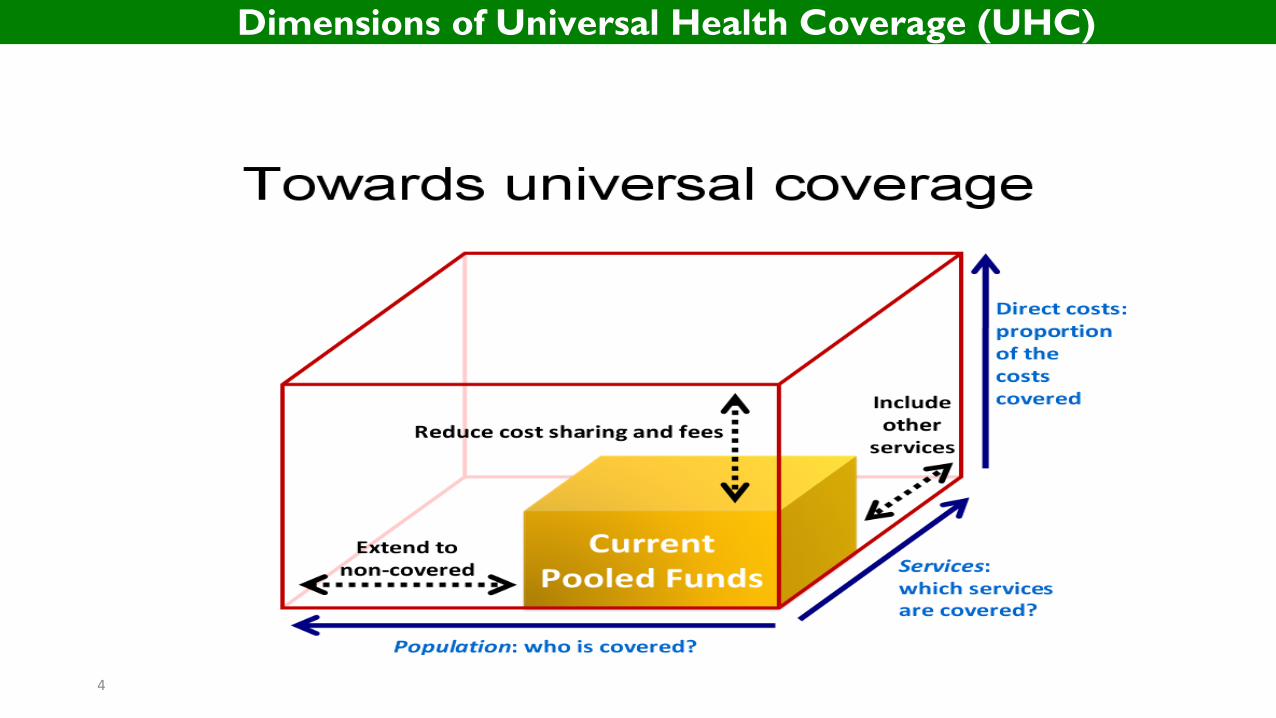
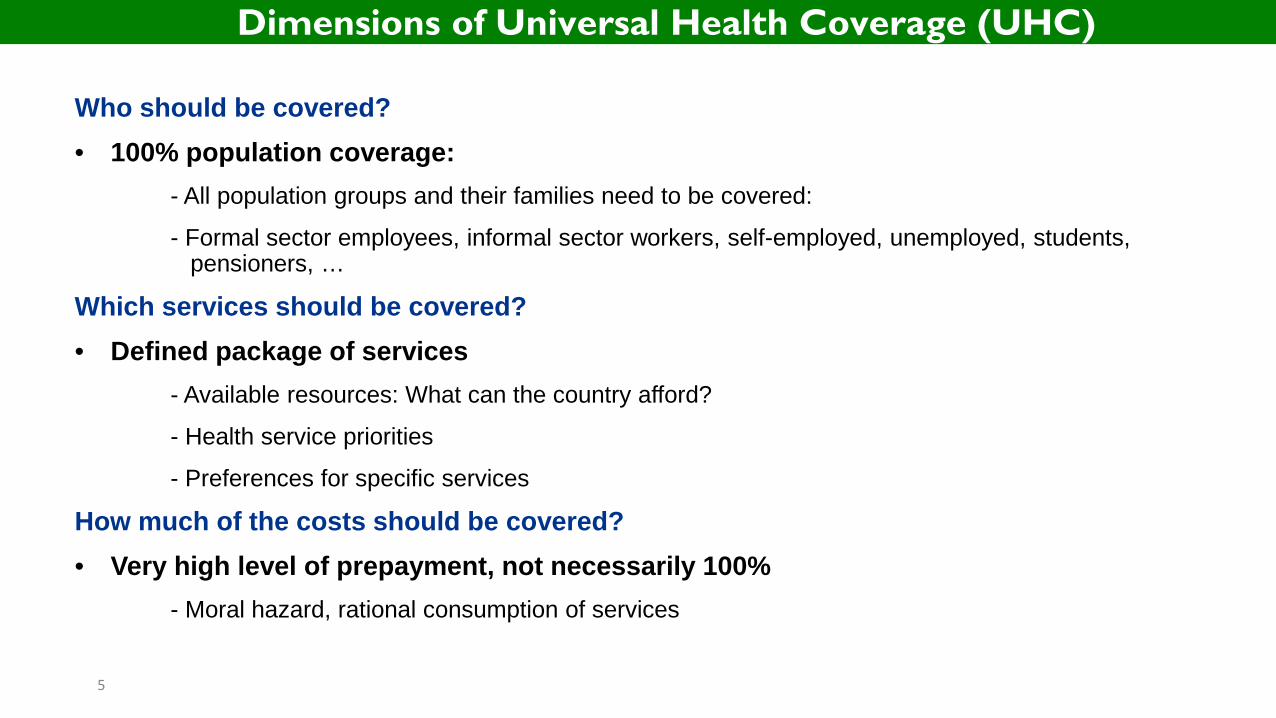
Dimensions of Universal Health Coverage (UHC)
5
Who should be covered? • 100% population coverage: - All population groups and their families need to be covered:
- Formal sector employees, informal sector workers, self-employed, unemployed, students, pensioners, …
Which services should be covered? • Defined package of services - Available resources: What can the country afford?
- Health service priorities
- Preferences for specific services
How much of the costs should be covered? • Very high level of prepayment, not necessarily 100% - Moral hazard, rational consumption of services
Dimensions of Universal Health Coverage (UHC)
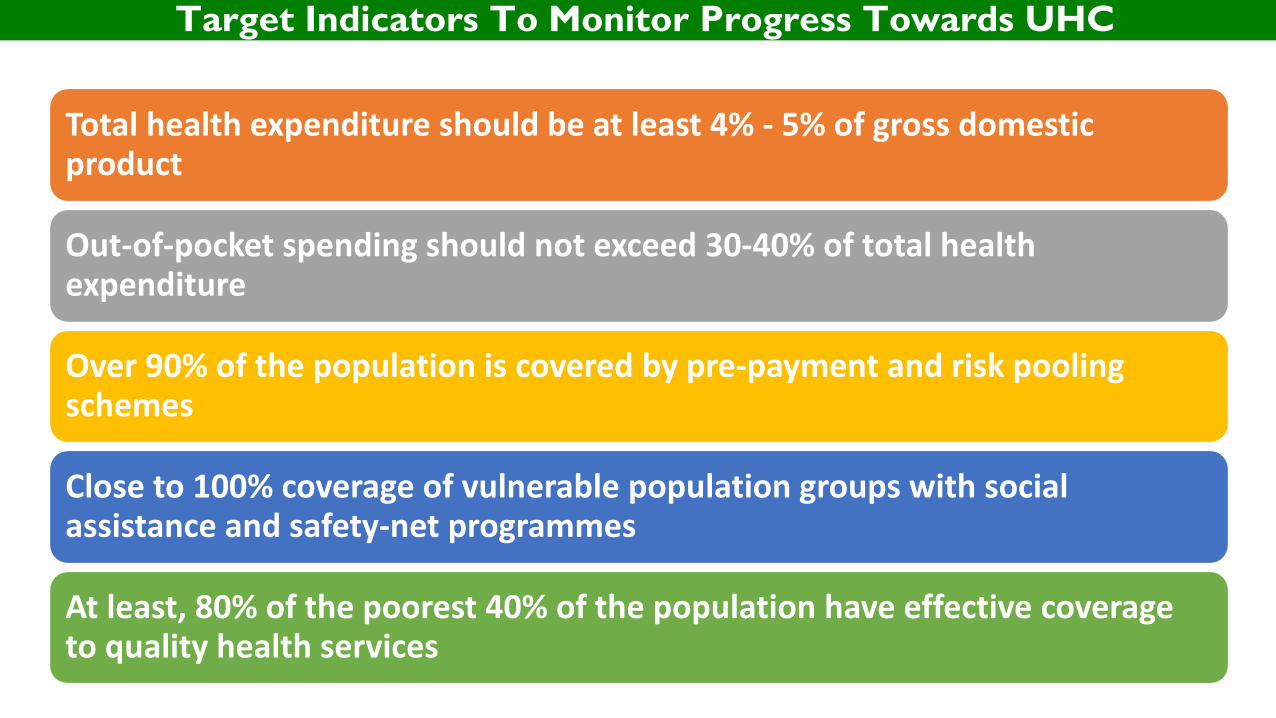
Total health expenditure should be at least 4% - 5% of gross domestic product
Out-of-pocket spending should not exceed 30-40% of total health expenditure
Over 90% of the population is covered by pre-payment and risk pooling schemes
Close to 100% coverage of vulnerable population groups with social assistance and safety-net programmes
At least, 80% of the poorest 40% of the population have effective coverage to quality health services
Target Indicators To Monitor Progress Towards UHC
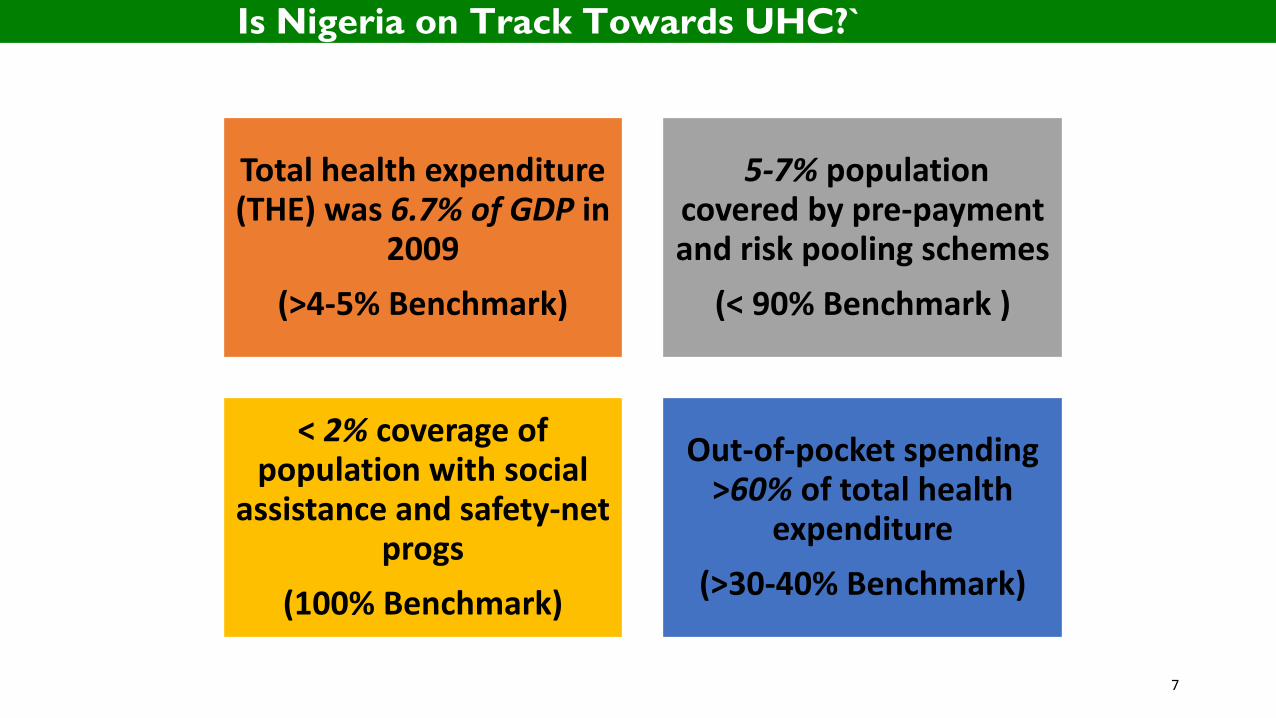
Total health expenditure (THE) was 6.7% of GDP in
2009 (>4-5% Benchmark)
5-7% population covered by pre-payment and risk pooling schemes
(< 90% Benchmark )
< 2% coverage of population with social
assistance and safety-net progs
(100% Benchmark)
Out-of-pocket spending >60% of total health
expenditure (>30-40% Benchmark)
7
Is Nigeria on Track Towards UHC?`
Tunisia
Kenya
Tanzania
Cote d'Ivoire
Ghana
South Africa
EthiopiaSenegal
Rwanda
Uganda
Georgia
Sri LankaVietnam
Nigeria
LOW INCOMELOWERMIDDLEINCOME
UPPERMIDDLEINCOME HIGH INCOME1
520
4060
100
Share
of TH
E (%)
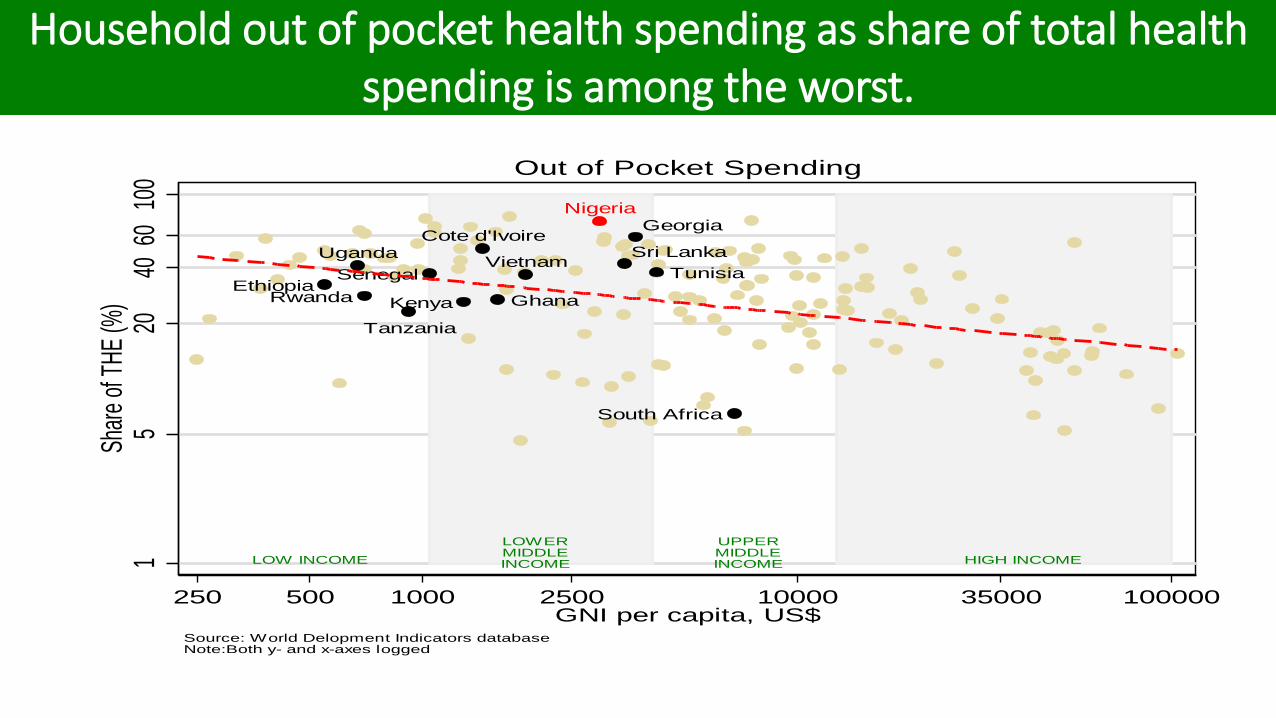
250 500 1000 2500 10000 35000 100000GNI per capita, US$
Source: World Delopment Indicators databaseNote:Both y- and x-axes logged
Out of Pocket Spending
Household out of pocket health spending as share of total health spending is among the worst.
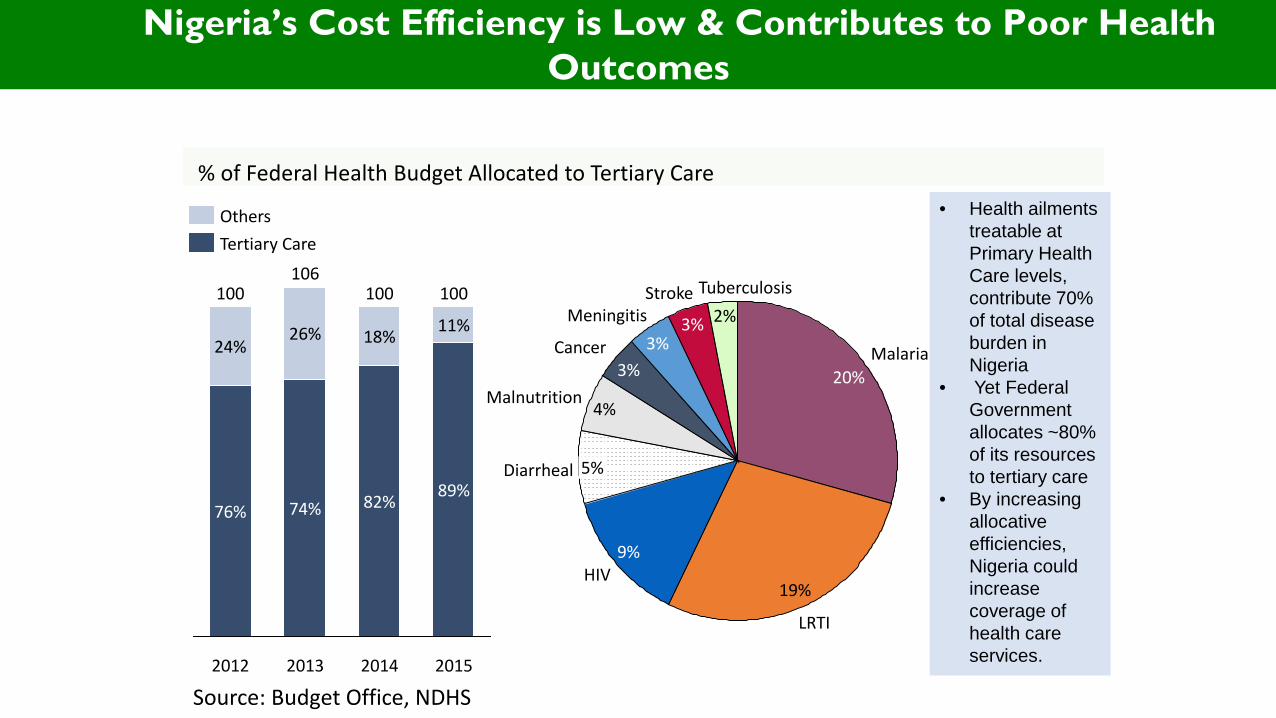
2015
100
89%
11%
2014
100
82%
18%
2013
106
74%
26% 24%
76%
2012
100
% of Federal Health Budget Allocated to Tertiary Care
Others Tertiary Care
• Health ailments treatable at Primary Health Care levels, contribute 70% of total disease burden in Nigeria
• Yet Federal Government allocates ~80% of its resources to tertiary care
• By increasing allocative efficiencies, Nigeria could increase coverage of health care services.
Source: Budget Office, NDHS
3%
2% Tuberculosis
Meningitis 3%
4%
Cancer
Malnutrition
3%
Stroke
Diarrheal 5%
Malaria 20%
LRTI
19%
9% HIV
Nigeria’s Cost Efficiency is Low & Contributes to Poor Health Outcomes
10
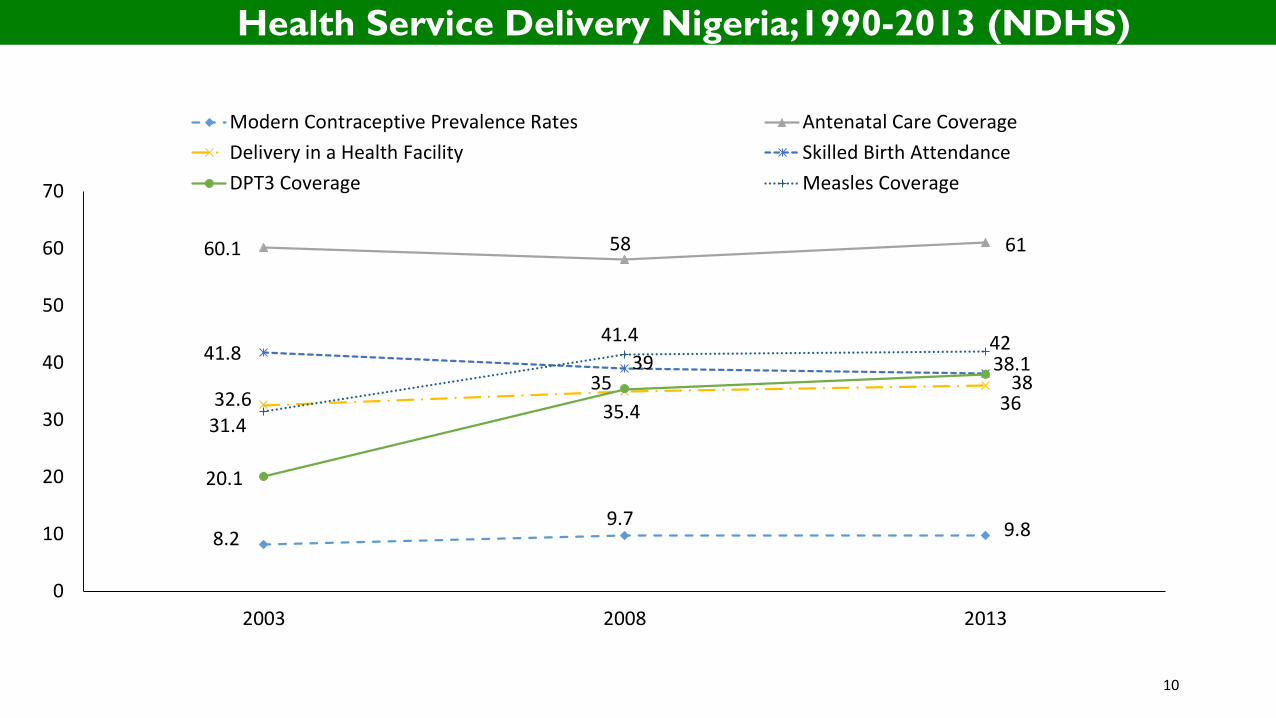
8.2 9.7 9.8
60.1 58 61
32.6 35
36
41.8 39 38.1
20.1
35.4 38
31.4
41.4 42
0
10
20
30
40
50
60
70
2003 2008 2013
Modern Contraceptive Prevalence Rates Antenatal Care CoverageDelivery in a Health Facility Skilled Birth AttendanceDPT3 Coverage Measles Coverage
Health Service Delivery Nigeria;1990-2013 (NDHS)
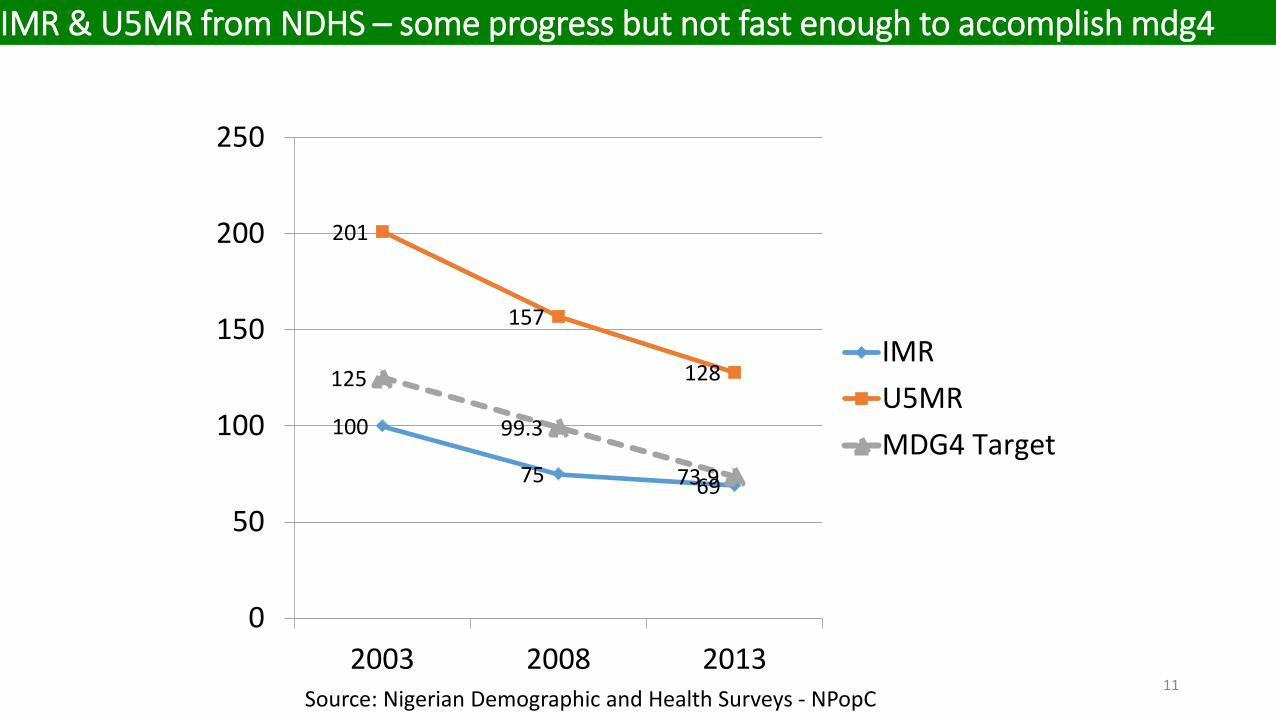
100
75 69
201
157
128 125
99.3
73.9
0
50
100
150
200
250
2003 2008 2013
IMRU5MRMDG4 Target
11 Source: Nigerian Demographic and Health Surveys - NPopC
IMR & U5MR from NDHS – some progress but not fast enough to accomplish mdg4
12
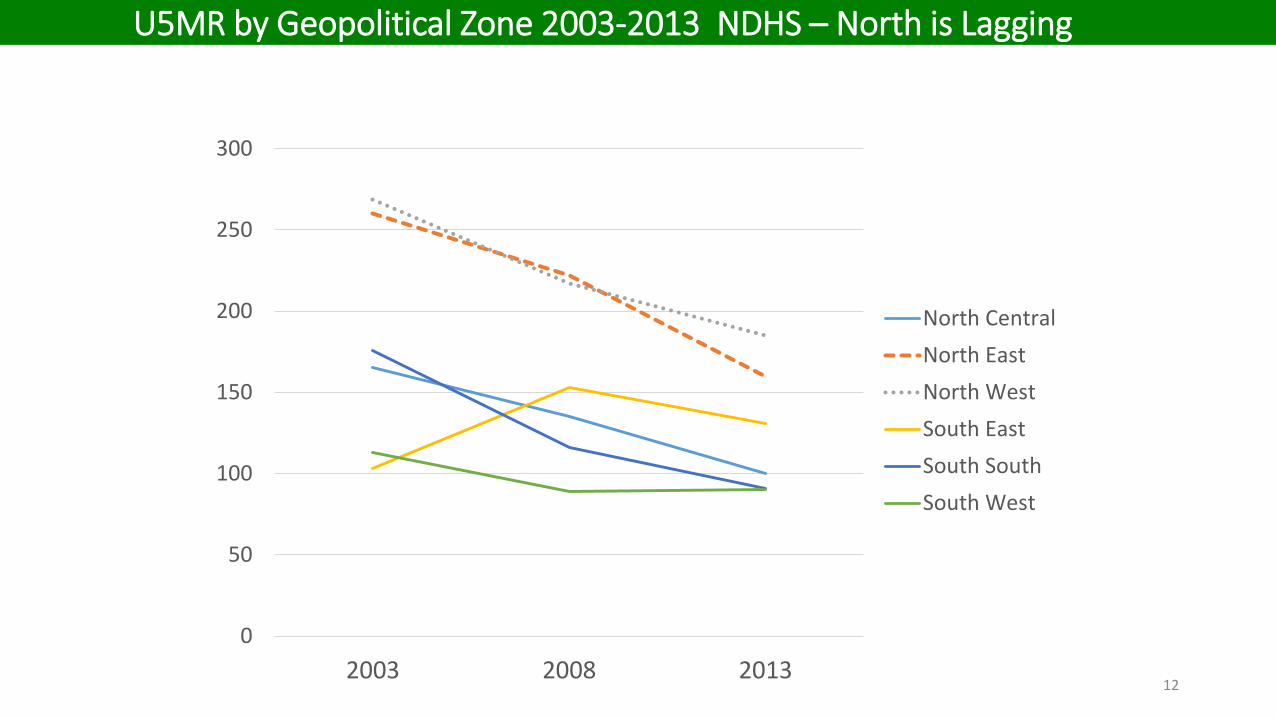
0
50
100
150
200
250
300
2003 2008 2013
North CentralNorth EastNorth WestSouth EastSouth SouthSouth West
U5MR by Geopolitical Zone 2003-2013 NDHS – North is Lagging
13
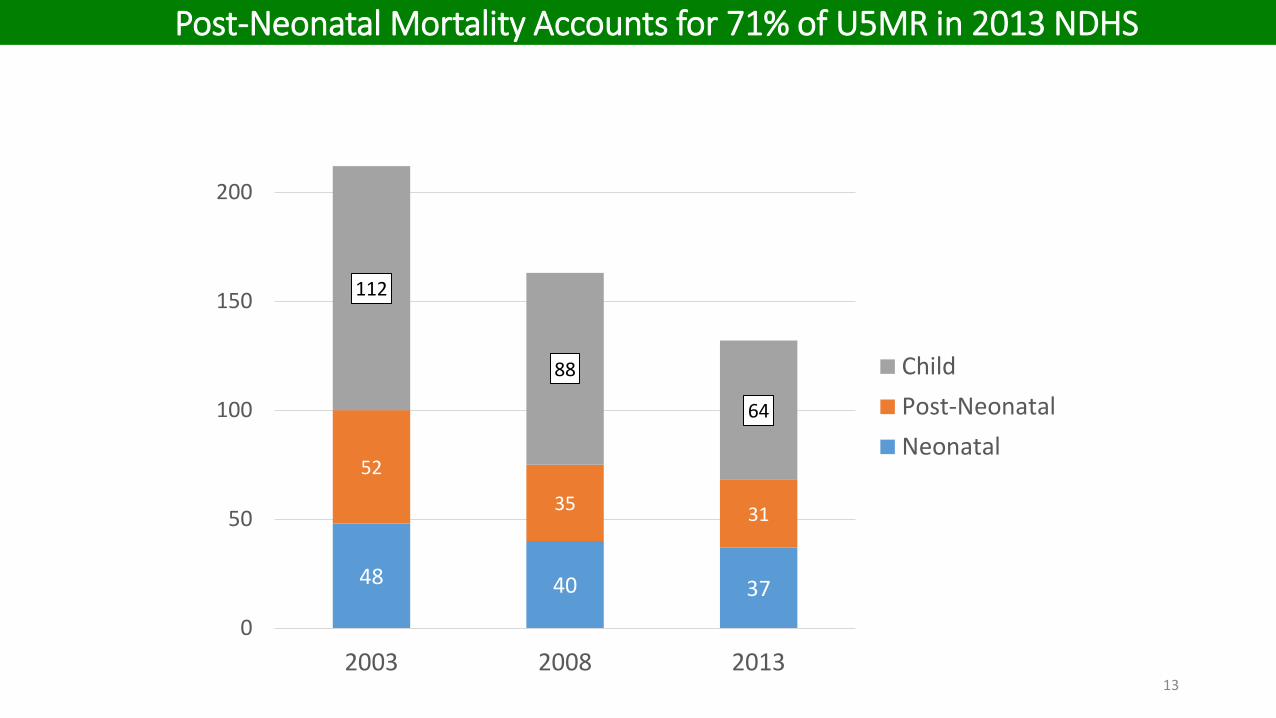
48 40 37
52
35 31
112
88
64
0
50
100
150
200
2003 2008 2013
ChildPost-NeonatalNeonatal
Post-Neonatal Mortality Accounts for 71% of U5MR in 2013 NDHS
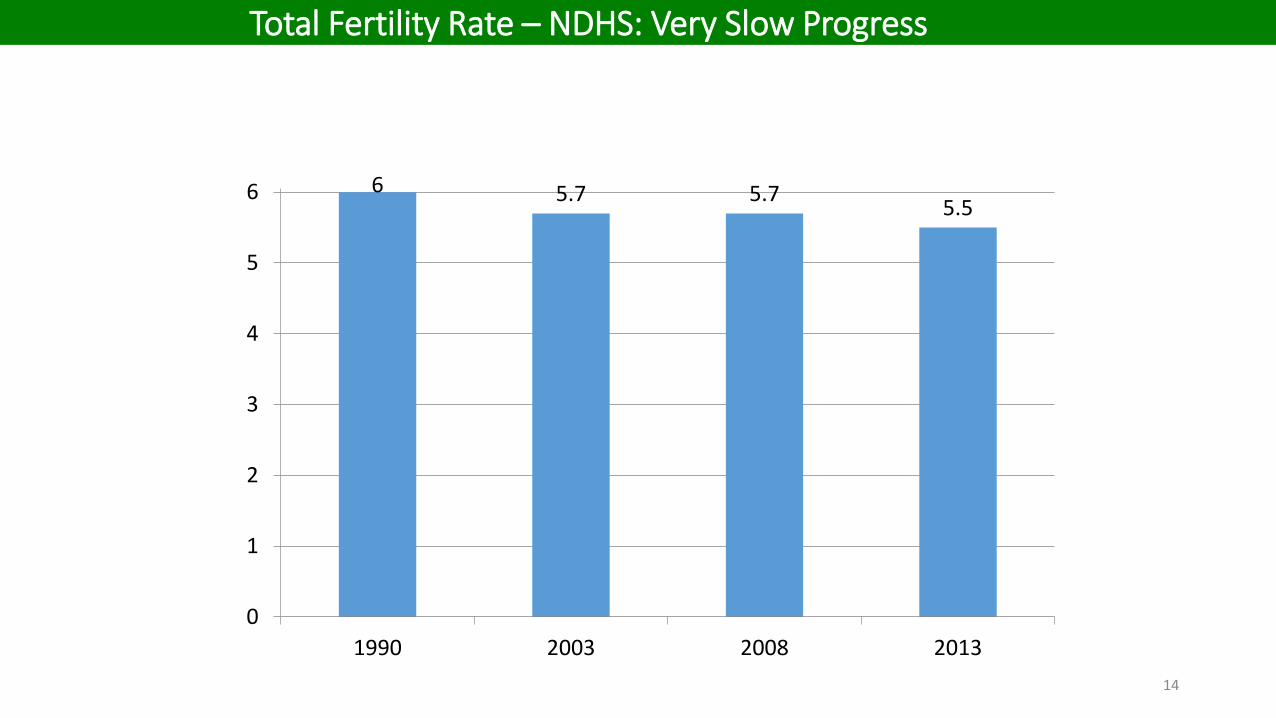
6 5.7 5.7 5.5
0
1
2
3
4
5
6
1990 2003 2008 201314
Total Fertility Rate – NDHS: Very Slow Progress
15
0
1
2
3
4
5
6
7
8
2003 2008 2013
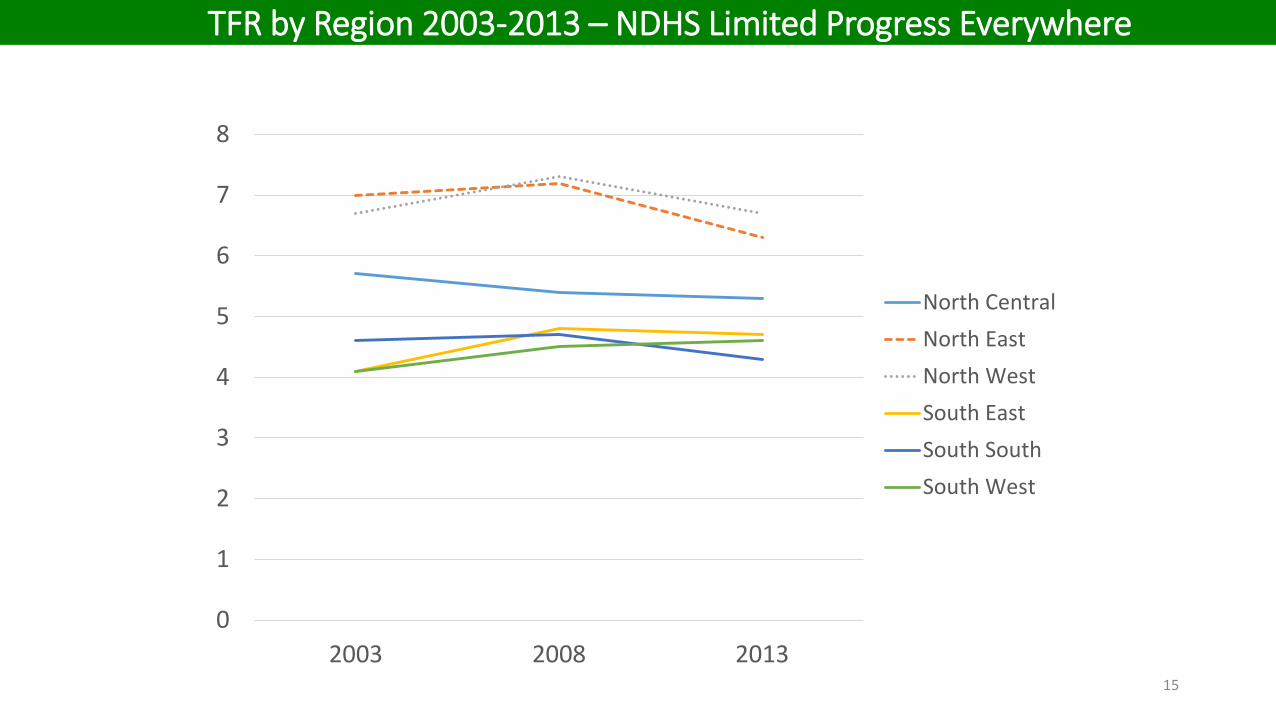
North CentralNorth EastNorth WestSouth EastSouth SouthSouth West
TFR by Region 2003-2013 – NDHS Limited Progress Everywhere
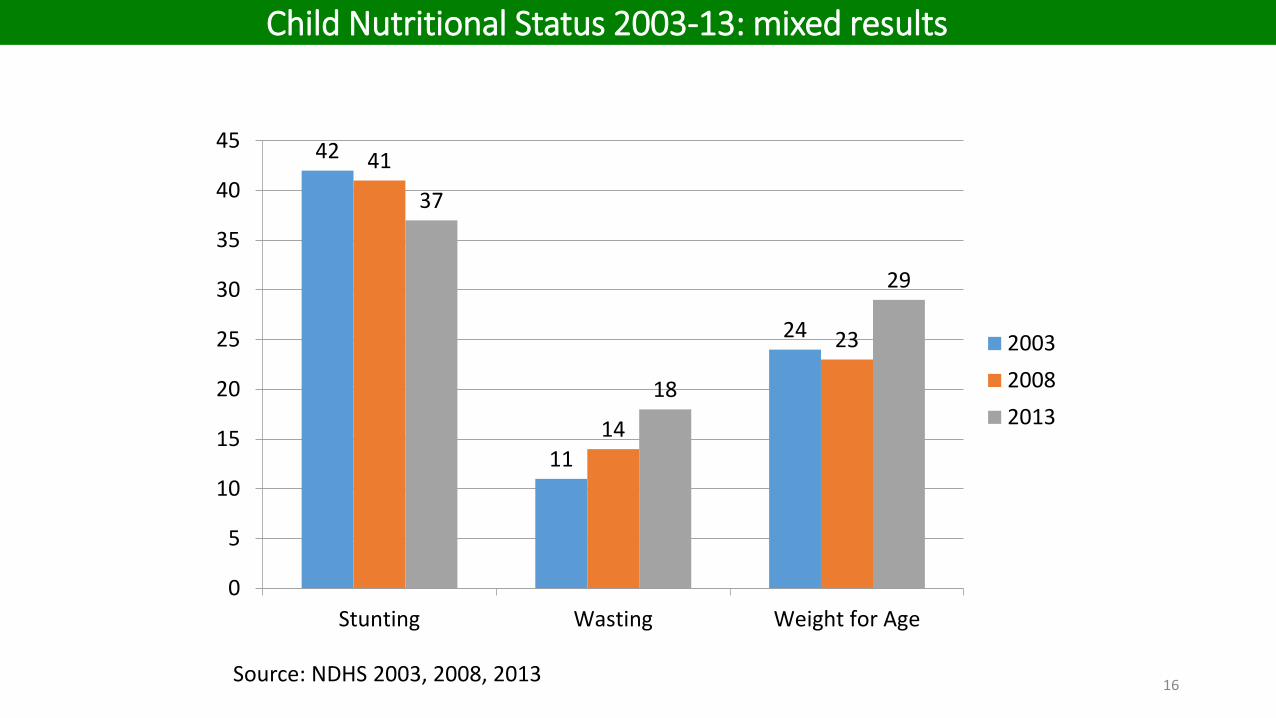
42
11
24
41
14
23
37
18
29
0
5
10
15
20
25
30
35
40
45
Stunting Wasting Weight for Age
200320082013
Source: NDHS 2003, 2008, 2013 16
Child Nutritional Status 2003-13: mixed results
17
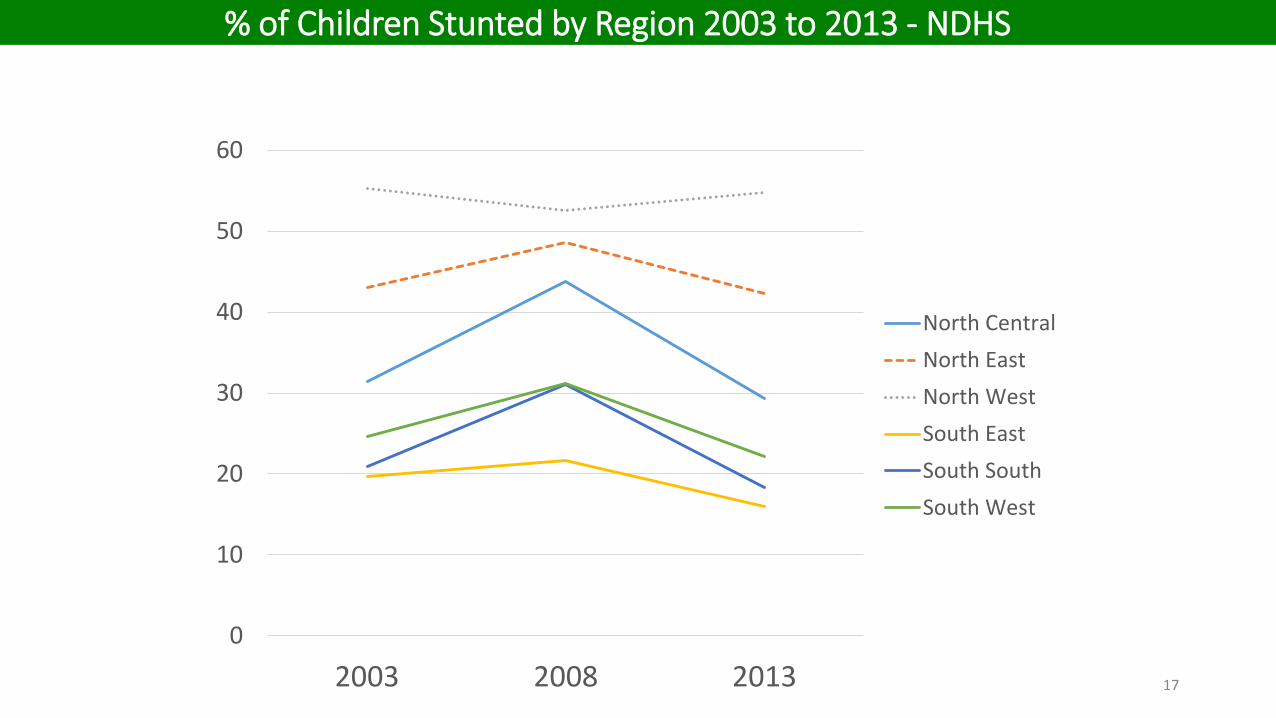
0
10
20
30
40
50
60
2003 2008 2013
North CentralNorth EastNorth WestSouth EastSouth SouthSouth West
% of Children Stunted by Region 2003 to 2013 - NDHS
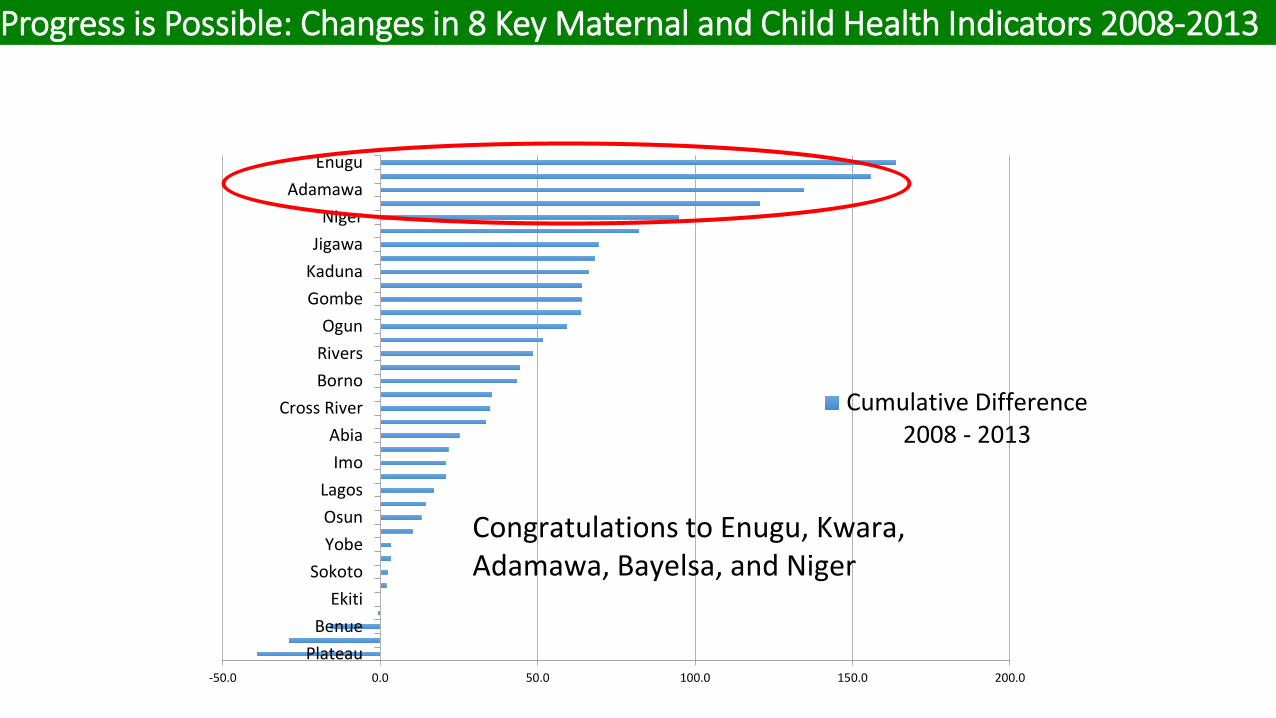
-50.0 0.0 50.0 100.0 150.0 200.0
PlateauBenue
EkitiSokoto
YobeOsunLagos
ImoAbia
Cross RiverBornoRiversOgun
GombeKadunaJigawa
NigerAdamawa
Enugu
Cumulative Difference2008 - 2013
Congratulations to Enugu, Kwara, Adamawa, Bayelsa, and Niger
Progress is Possible: Changes in 8 Key Maternal and Child Health Indicators 2008-2013
19
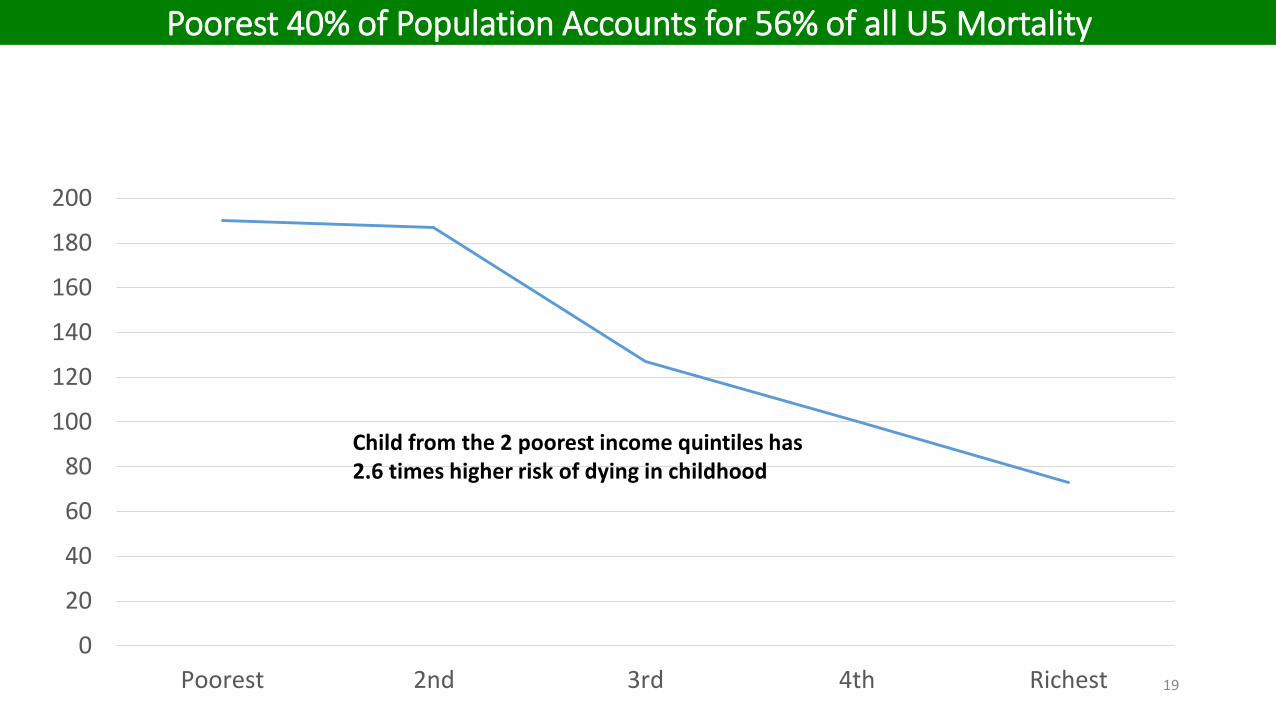
0
20
40
60
80
100
120
140
160
180
200
Poorest 2nd 3rd 4th Richest
Child from the 2 poorest income quintiles has 2.6 times higher risk of dying in childhood
Poorest 40% of Population Accounts for 56% of all U5 Mortality
20
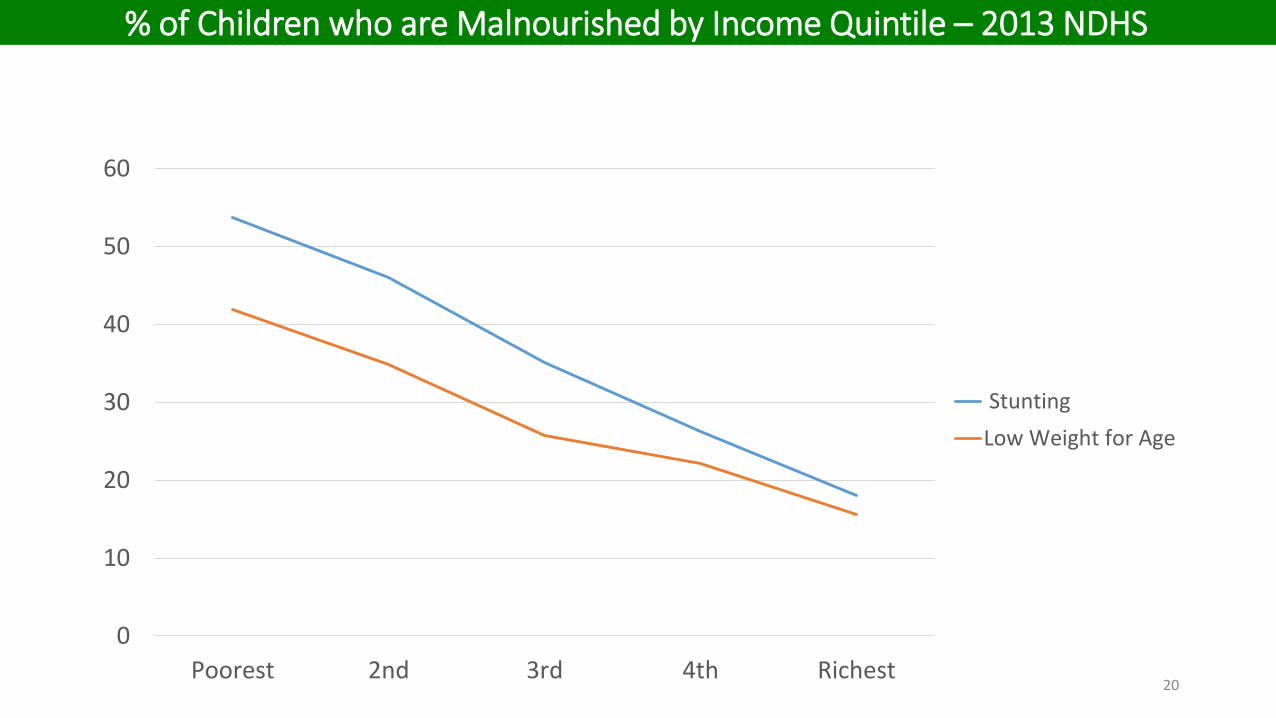
0
10
20
30
40
50
60
Poorest 2nd 3rd 4th Richest
StuntingLow Weight for Age
% of Children who are Malnourished by Income Quintile – 2013 NDHS
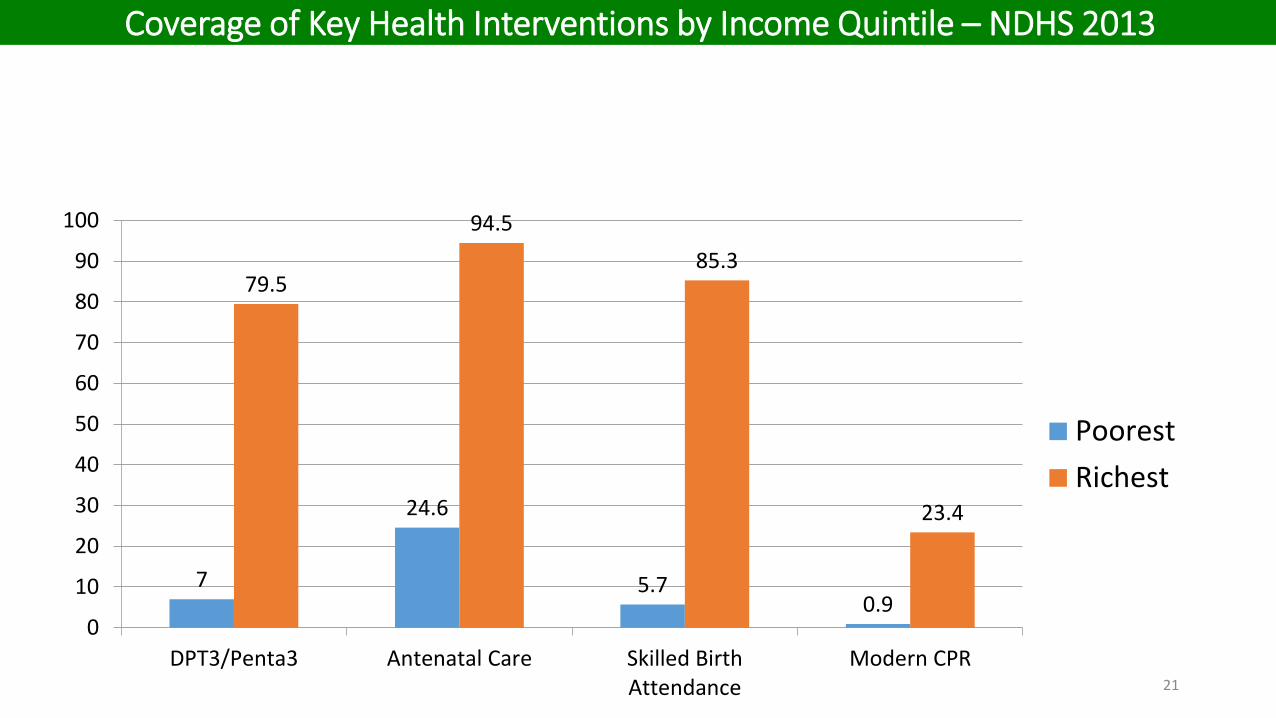
7
24.6
5.7 0.9
79.5
94.5 85.3
23.4
0
10
20
30
40
50
60
70
80
90
100
DPT3/Penta3 Antenatal Care Skilled BirthAttendance
Modern CPR
PoorestRichest
21
Coverage of Key Health Interventions by Income Quintile – NDHS 2013
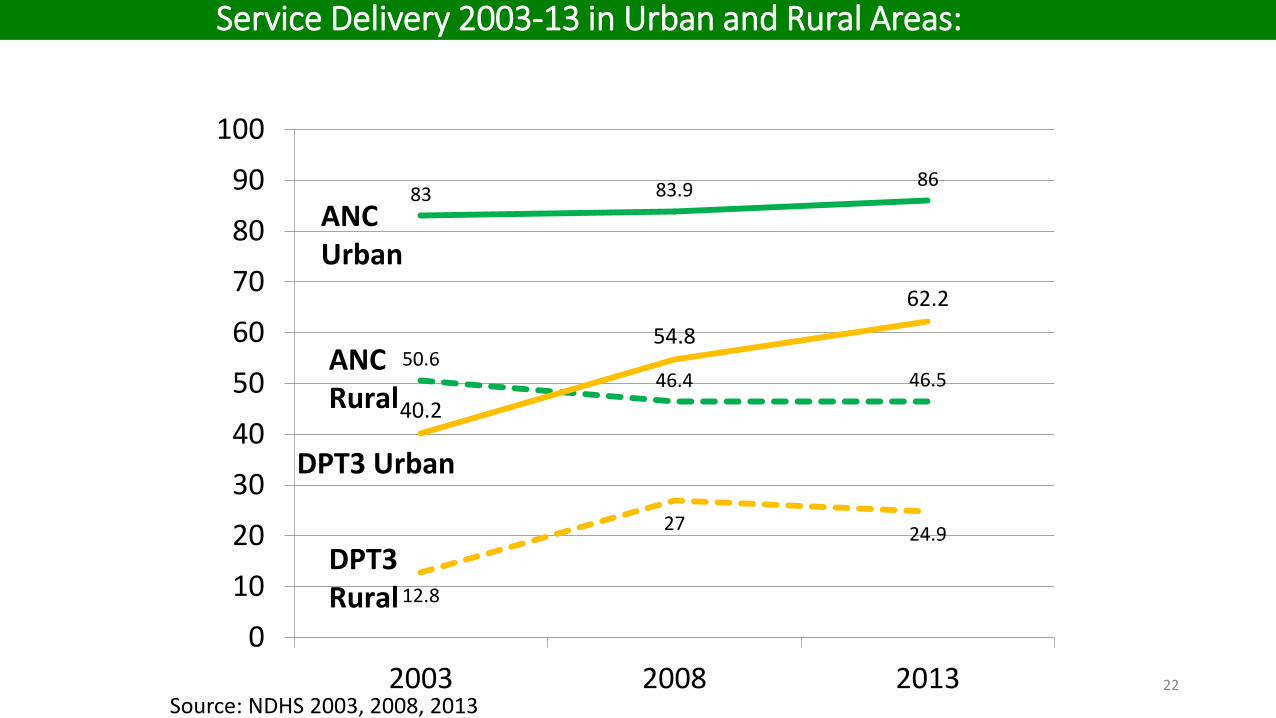
83 83.9 86
50.6 46.4 46.5
12.8
27 24.9
40.2
54.8 62.2
0
10
20
30
40
50
60
70
80
90
100
2003 2008 2013
ANC Rural
DPT3 Rural
DPT3 Urban
ANC Urban
Source: NDHS 2003, 2008, 2013 22
Service Delivery 2003-13 in Urban and Rural Areas:

23
Need for Clear & Strong Government Leadership &
Commitment
24
Presidential Declaration on UHC;
March 10, 2014
I. Financial access II. Physical access III. Quality of services
Key Outputs from Presidential Summit on UHC: March 10, 2014
Governments at all tiers should declare that the achievement of Universal Health Coverage in Nigeria is a priority goal
Starting-point for achieving UHC
• Commitment by all tiers of government to ensure every Nigerian has financial access to health services through mandatory health insurance and other financial risk protection mechanisms
• Fast-track the amendment of the NHIS Act to ensure that all employers in formal, informal and organized private sector cover their employees with mandatory health insurance
Recommended Actions for improving financial access for UHC (1)
• Establish a Universal Health Coverage (UHC) fund with innovative funding sources – general tax revenue with budget line for UHC, Sin tax (alcohol, tobacco), air-ticket levy, percentage of VAT, GSM contributions, etc.
• Governments (Federal and states) should ring-fence the UHC fund for ensuring compulsory coverage for the poor and vulnerable groups including, pregnant women, children, those physically challenged, etc.
Recommended Actions for improving financial access (2)
• Governments at all levels should increase their budgetary allocations to health to reach the “Abuja Declaration”
• Establish mechanisms to ensure all government workers pay the 1.75% salary contributions for the Formal Sector Social Health Insurance Programme of the National Health Insurance Scheme.
Recommended Actions for improving financial access (3)
• Governments at all levels should ensure the presence of at least one functional primary health care centre per ward and one general hospital per LGA that can deliver the minimum defined benefit package.
• All states should reactivate their Central Medical Stores to conform to a minimum standard for the supply chain management of health products
• Governments at all levels should ensure that their health facilities have the availability of the minimum standards (numbers and skill sets) defined for human resources for health at each level
Recommended Actions for improving physical access
• Training institutions should ensure that there is competency-based training of all health professionals. around priority health needs
• The government should address mal-distribution of health workers through policies and incentives around retention
Recommended Actions for improving physical access
• Governments at all levels should conduct a health system needs assessment for improvement of quality of services
• Governments should strengthen existing systems for supervision and monitoring of quality of healthcare provision and institutionalize monitoring and evaluation of health system in Nigeria
• Governments should explore the use of an Independent Health Quality System for issues relating to quality in health services
Recommended Actions for improving quality of health services
• Strengthen existing consumer protection agencies including SERVICOM and every hospital should have its own SERVICOM desk
• Governments should establish a Clinical Governance body or bodies to protect both providers and consumers at all levels
• Governments at all levels should improve healthcare infrastructure and equipment (including maintenance strategy).
Recommended Actions for improving quality of health services
• Affordability is important but may not be enough
• Target the poor, but keep an eye on the non-poor
• Benefits should be closely linked to target populations' needs
• Highly focused interventions can be a useful initial step toward UHC
(Giedion et al, 2013)
In implementing UHC interventions
• Strive for more health for money (improved efficiency in use of available funds)
• Advocacy to decision makers and all Nigerians to understand and be fully involved in interventions to achieve UHC
• UHC will save millions of lives in Nigeria
In implementing UHC interventions

36
OPPORTUNITIES

37
THE NHAct 2014: VEHICLE FOR ACHIEVING UHC
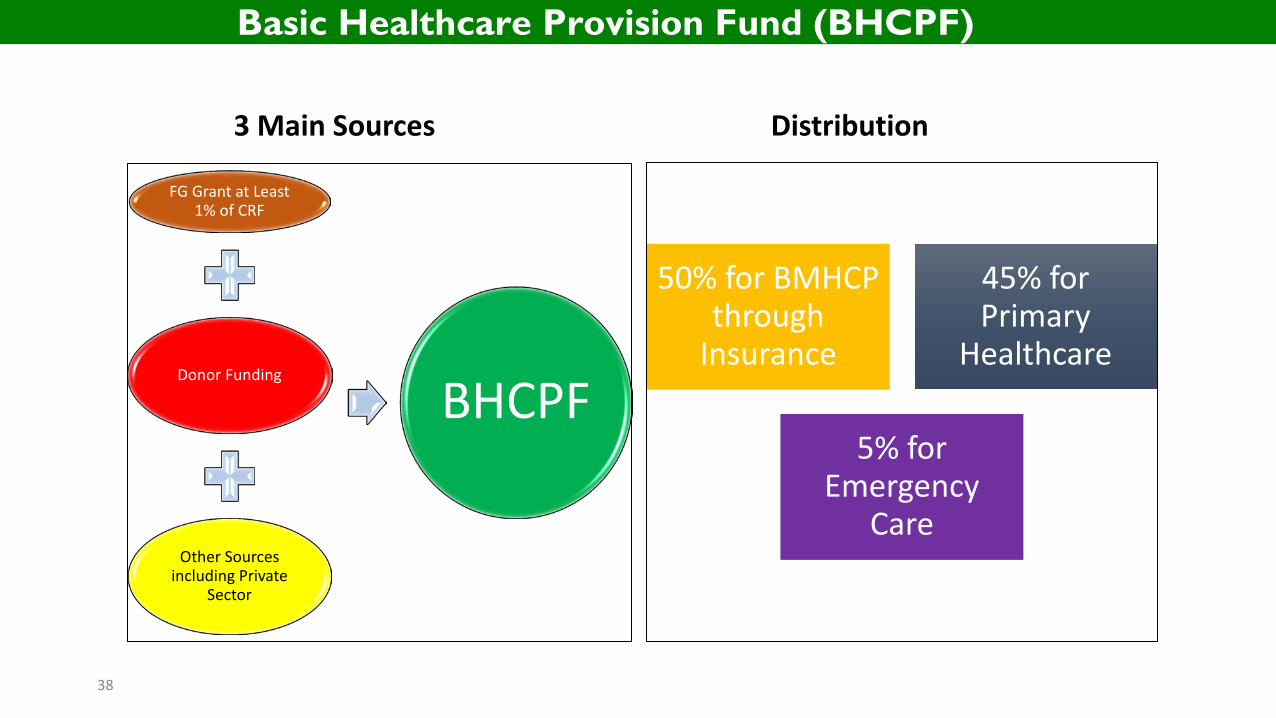
3 Main Sources
FG Grant at Least 1% of CRF
Donor Funding
Other Sources including Private
Sector
BHCPF
Distribution
50% for BMHCP through
Insurance
45% for Primary
Healthcare
5% for Emergency
Care
38
Basic Healthcare Provision Fund (BHCPF)

1. Investment Case 2. Healthcare financing strategy 3. Joint financing for investment case
The Global Financing Facility (GFF)
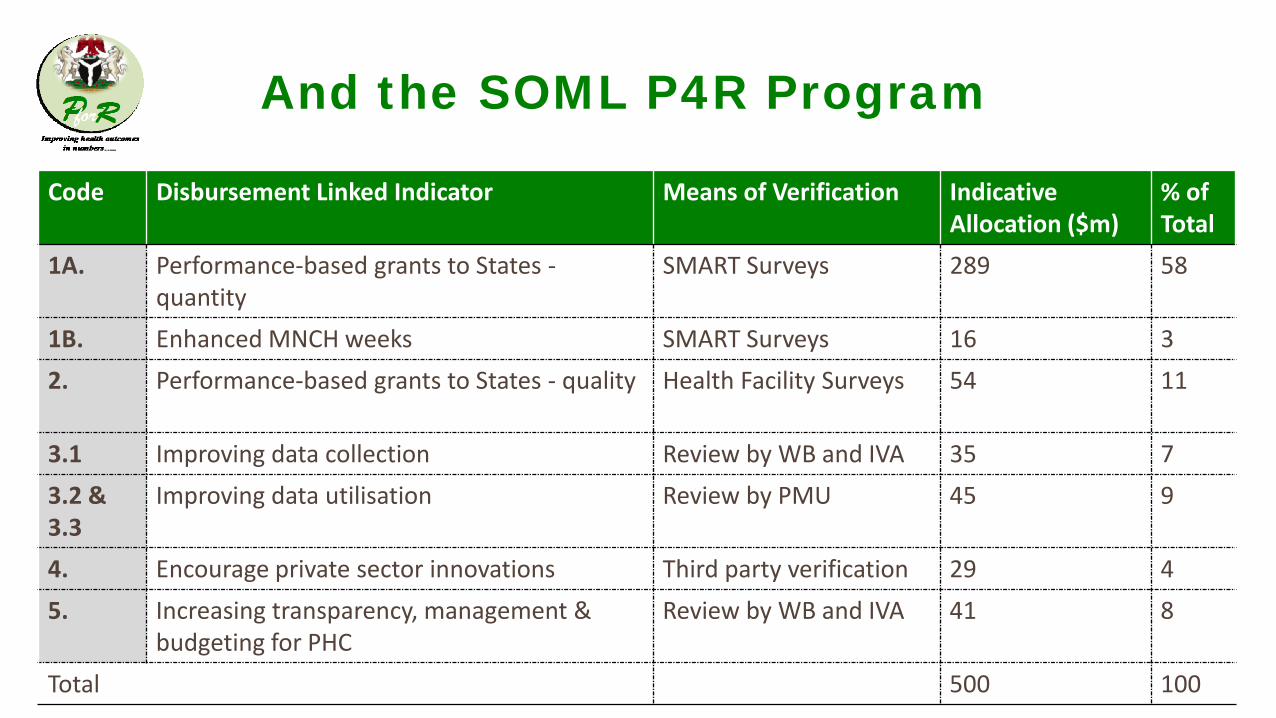
And the SOML P4R Program
Code Disbursement Linked Indicator Means of Verification Indicative Allocation ($m)
% of Total
1A. Performance-based grants to States - quantity
SMART Surveys 289 58
1B. Enhanced MNCH weeks SMART Surveys 16 3 2. Performance-based grants to States - quality
Health Facility Surveys 54 11
3.1 Improving data collection Review by WB and IVA 35 7 3.2 & 3.3
Improving data utilisation Review by PMU 45 9
4. Encourage private sector innovations Third party verification 29 4 5. Increasing transparency, management &
budgeting for PHC Review by WB and IVA 41 8
Total 500 100

• Achieve Universal Health Coverage by ensuring 1 functional PHC per ward in Nigeria
UNIVERSAL
HEALTH
COVERAGE
Responsiveness
Greater
Equity
Improved Health
Outcomes
Financial protection
Efficient, accountable
and transparent
system
Increased job
Reduction in poverty
Greater productivity
• Significant resources are required to achieve the goal.
• Government thus needs to determine a financially sustainable mode of financing
• To achieve UHC, Nigeria will scale up the inputs required for efficient service delivery
• 10, 000 PHC facilities will be revitalised over the next 2 years.
• 100m Nigerians will have access to qualitative health care
The PHC revitalisation program will serve as the basis for achieving Universal Health Coverage

And Health As an Investment that yields huge returns to the
National Economy
42
review policy to ensure efficient and effective management of our health system with focus on
prevention
Ensure that no Nigerian will have any reason to go outside the country for medical treatment
Guarantee financial sustainability to the health sector and minimum basic healthcare for all
Review occupational health laws and immediately commence enforcement of the provisions to reduce hazards in the work place
Partner with state Governments and development partners to ensure all round implementation of our primary health plans by expanding access to
health insurance for rural communities
43
The President’s Pledge for Health
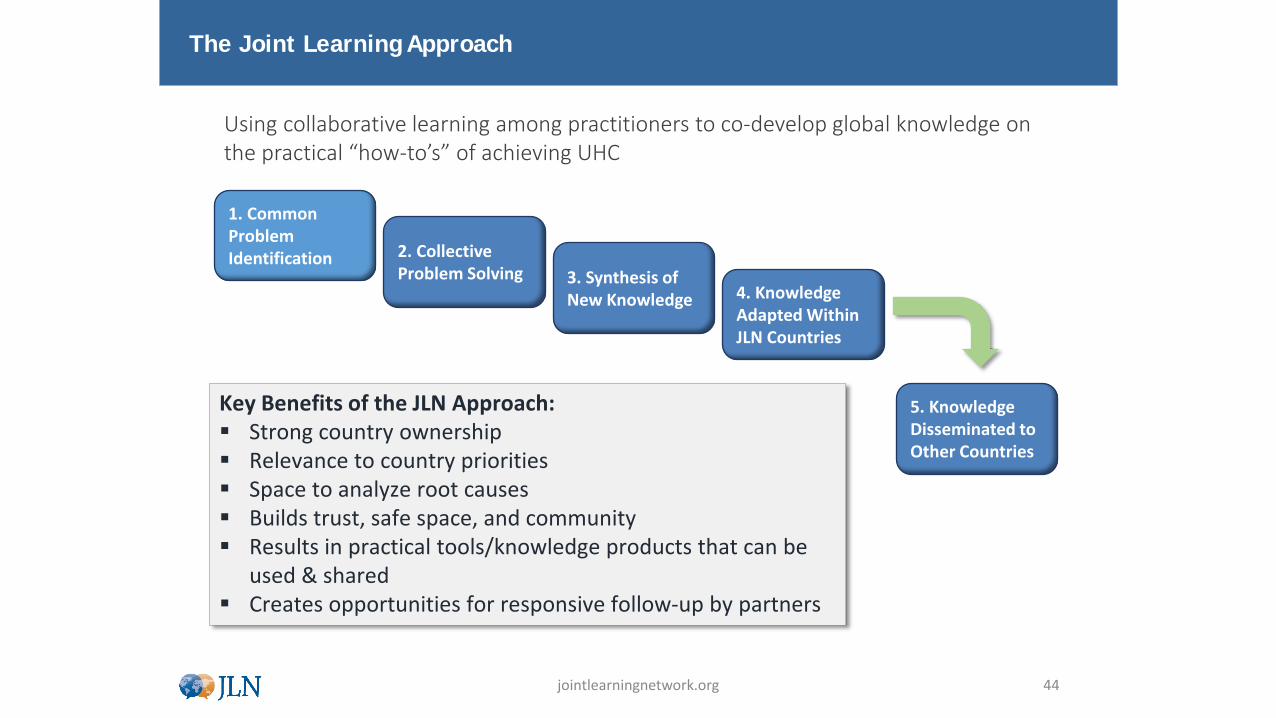
The Joint Learning Approach
1. Common Problem Identification 2. Collective
Problem Solving 3. Synthesis of New Knowledge 4. Knowledge
Adapted Within JLN Countries
5. Knowledge Disseminated to Other Countries
Key Benefits of the JLN Approach: Strong country ownership Relevance to country priorities Space to analyze root causes Builds trust, safe space, and community Results in practical tools/knowledge products that can be
used & shared Creates opportunities for responsive follow-up by partners
jointlearningnetwork.org 44
Using collaborative learning among practitioners to co-develop global knowledge on the practical “how-to’s” of achieving UHC
How Do I Support My State Achieve UHC?

Thank You
46


![Universal Health Coverage UHC in Global Health · Universal Health Coverage [ UHC ] in Global Health Ariel Pablos-Méndez, MD, MPH ... Voice and Accountability matters more ! UHC](https://img.pdfslide.net/doc/110x75/5f0f7c537e708231d4446621/universal-health-coverage-uhc-in-global-health-universal-health-coverage-uhc-.jpg)

























