Embed Size (px)
Citation preview

بسم ال الرحمن الرحيم“ ال الذين آمنوا منكم والذين أوتوا العلم درجاتيرفع”
صدق ال العظيم
قال رسول ال صلى اله عليه وسلم:قال رسول ال صلى اله عليه وسلم:
”من سلك طريقا يلتمس فيه علما سهل ال له طريقا إلى ”من سلك طريقا يلتمس فيه علما سهل ال له طريقا إلى الجنة وإن الملكئكة لتضع أجنحتها لطالب العلم رضا بما الجنة وإن الملكئكة لتضع أجنحتها لطالب العلم رضا بما يصنع وإن العالم يستغفر له من فى السماوات ومن فى يصنع وإن العالم يستغفر له من فى السماوات ومن فى الرض حتى الحيتان فى الماء وفضل العالم على العابد الرض حتى الحيتان فى الماء وفضل العالم على العابد
كفضل القمر على ساكئر الكواكب وإن العلماء ورثة البنبياء“كفضل القمر على ساكئر الكواكب وإن العلماء ورثة البنبياء“
صدق رسول ال صدق رسول ال
بسم ال الرحمن الرحيمبسم ال الرحمن الرحيم““يرفع ال الذين آمنوا منكم والذين أوتوا العلم درجاتيرفع ال الذين آمنوا منكم والذين أوتوا العلم درجات””
صدق ال العظيمصدق ال العظيم

The largest abdominal organ, occupies The largest abdominal organ, occupies most of the right upper abdomen. most of the right upper abdomen. Sonography of the liver is most frequently Sonography of the liver is most frequently performed for evaluation of suspected performed for evaluation of suspected focal or diffuse abnormalities. focal or diffuse abnormalities. With the increasing availability of color With the increasing availability of color Doppler ultrasound, sonography plays an Doppler ultrasound, sonography plays an important role in the evaluation of hepatic important role in the evaluation of hepatic vascular abnormalities. vascular abnormalities.
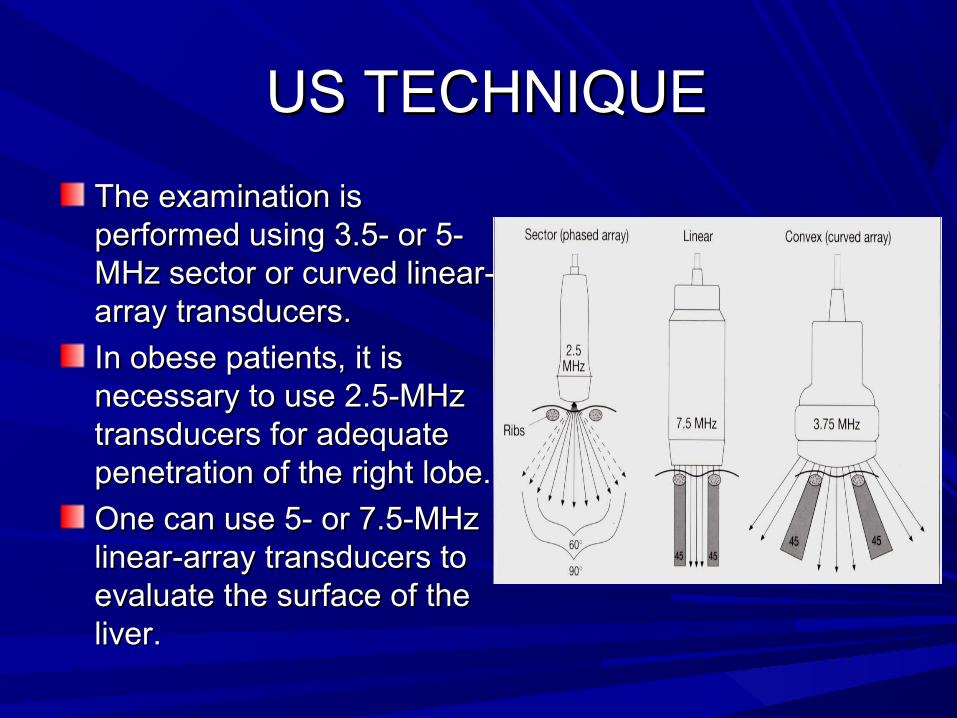
US TECHNIQUEUS TECHNIQUE
The examination is The examination is performed using 3.5- or 5-performed using 3.5- or 5-MHz sector or curved linear-MHz sector or curved linear-array transducers. array transducers.
In obese patients, it is In obese patients, it is necessary to use 2.5-MHz necessary to use 2.5-MHz transducers for adequate transducers for adequate penetration of the right lobe. penetration of the right lobe.
One can use 5- or 7.5-MHz One can use 5- or 7.5-MHz linear-array transducers to linear-array transducers to evaluate the surface of the evaluate the surface of the liver. liver.

US TECHNIQUEUS TECHNIQUE
The initial The initial examination is examination is performed with the performed with the patient in the supine patient in the supine position.position.

US TECHNIQUEUS TECHNIQUE
Followed by examination in the left posterior Followed by examination in the left posterior oblique position, which is specially useful for oblique position, which is specially useful for evaluation of the deeper posterior portions of the evaluation of the deeper posterior portions of the right lobe. right lobe. Most of the liver is accessible by subcostal Most of the liver is accessible by subcostal scanning. scanning. Cranial portions of the liver, especially the Cranial portions of the liver, especially the subdiaphragmatic portions of the right lobe, may subdiaphragmatic portions of the right lobe, may be difficult to evaluate and are better seen by be difficult to evaluate and are better seen by intercostal scanning with sector transducers. intercostal scanning with sector transducers.

Duplex Doppler and color Doppler Duplex Doppler and color Doppler sonographysonography
can enable the clinician to differentiate can enable the clinician to differentiate blood vessels from bile ducts blood vessels from bile ducts
to document vascular occlusions or to document vascular occlusions or thrombosis, collateral vessels.thrombosis, collateral vessels.
Flow within hepatic lesions.Flow within hepatic lesions.

THE NORMAL LIVERTHE NORMAL LIVER
An ultrasound estimate of liver size can be made An ultrasound estimate of liver size can be made based on the craniocaudal extent of the right based on the craniocaudal extent of the right lobe and anteroposterior extent of the left lobe. lobe and anteroposterior extent of the left lobe. When measured in the midclavicular line the When measured in the midclavicular line the right lobe normally measures up to 13 cm and is right lobe normally measures up to 13 cm and is considered enlarged if more than 15 cm. considered enlarged if more than 15 cm. The left lobe does not normally exceed 6 cm The left lobe does not normally exceed 6 cm measured anteroposteriorly in the midline. measured anteroposteriorly in the midline. Accurate positioning of the probe is important as Accurate positioning of the probe is important as the right lobe may measure more than 15 cm in the right lobe may measure more than 15 cm in length when measured more laterally.length when measured more laterally.

Echo-patternEcho-patternThe normal liver has a The normal liver has a characteristic characteristic parenchymal echo parenchymal echo texture, more echogenic texture, more echogenic than the renal than the renal parenchymaparenchyma
The portal vein lumen is The portal vein lumen is also anechoic, but it has also anechoic, but it has echogenic walls owing to echogenic walls owing to surrounding connective surrounding connective tissue in the portal tracts. tissue in the portal tracts.

Echo-patternEcho-pattern Within this background, Within this background, hepatic veins are visible hepatic veins are visible as anechoic structures as anechoic structures draining superiorly draining superiorly towards the IVC. towards the IVC. Normal bile ducts may be Normal bile ducts may be visible extending into the visible extending into the left and right lobe with the left and right lobe with the portal veins, measuring portal veins, measuring up to 40% of the adjacent up to 40% of the adjacent portal vein diameter. portal vein diameter. Intrahepatic arterial Intrahepatic arterial branches are generally branches are generally not visible without colour not visible without colour Doppler Doppler

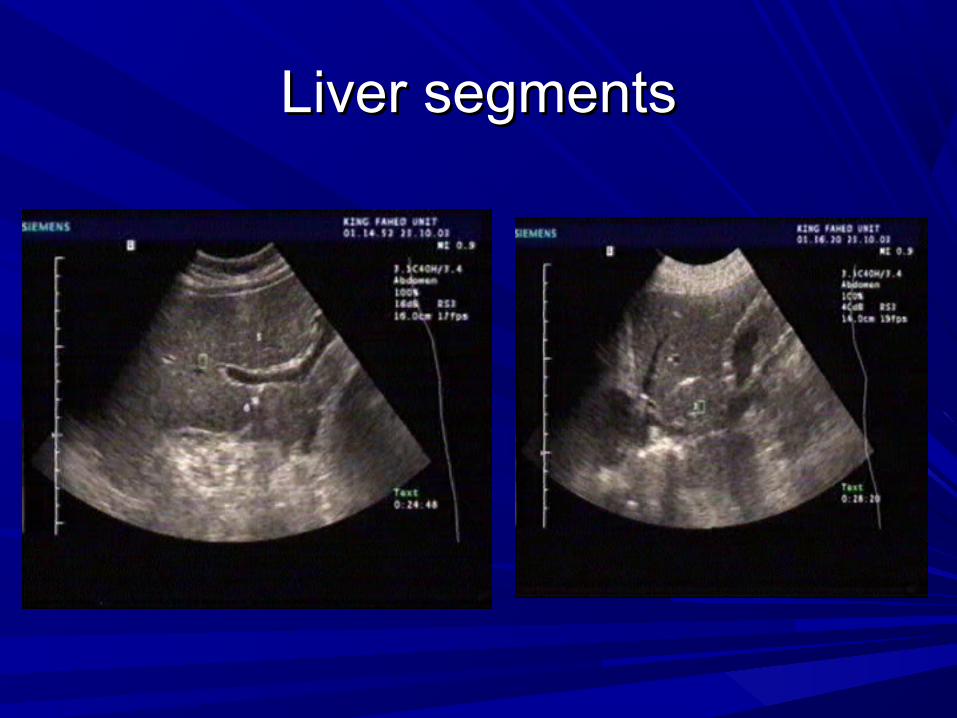
Liver segmentsLiver segments
The left and right lobes The left and right lobes are separated by a plane are separated by a plane through the middle through the middle hepatic vein and the hepatic vein and the gallbladder bed and are gallbladder bed and are roughly equal in size. roughly equal in size.
The right lobe is further The right lobe is further divided into anterior and divided into anterior and posterior sectors by the posterior sectors by the right hepatic vein. right hepatic vein.
Liver segmentsLiver segments

Liver capsuleLiver capsule
The liver is surrounded by The liver is surrounded by Glisson's capsule, which Glisson's capsule, which is a thin layer of is a thin layer of connective tissue. connective tissue. The thin liver capsule is The thin liver capsule is usually not visible usually not visible sonographically.sonographically. When the liver is When the liver is surrounded by ascites surrounded by ascites and the ultrasound beam and the ultrasound beam is perpendicular to the is perpendicular to the liver surface, a linear liver surface, a linear echo is frequently seen echo is frequently seen along the liver surface along the liver surface
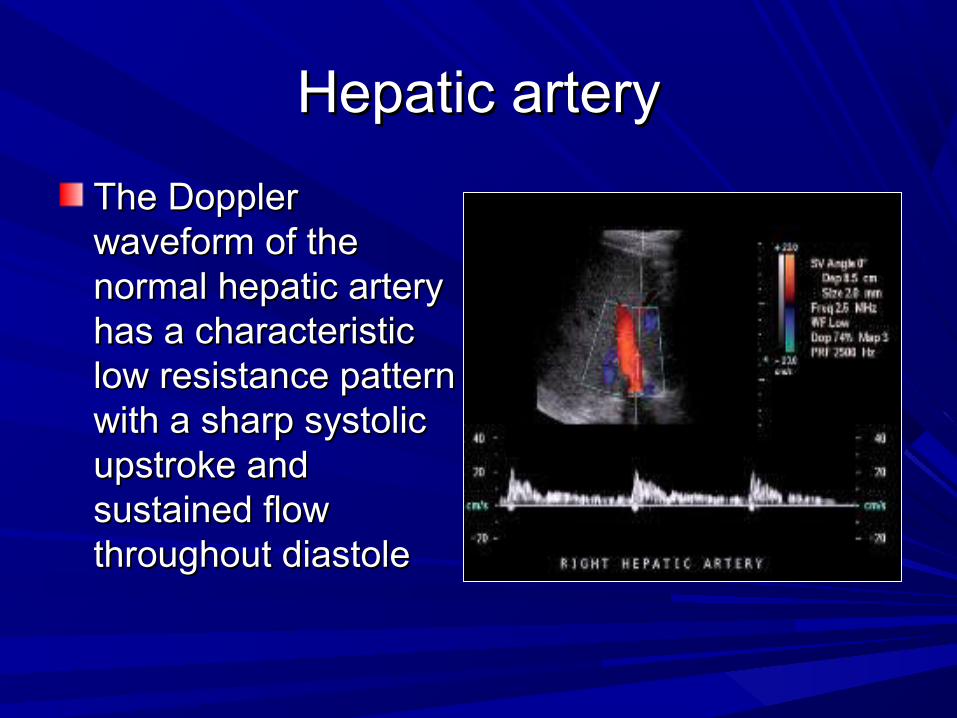
Hepatic arteryHepatic artery
The Doppler The Doppler waveform of the waveform of the normal hepatic artery normal hepatic artery has a characteristic has a characteristic low resistance pattern low resistance pattern with a sharp systolic with a sharp systolic upstroke and upstroke and sustained flow sustained flow throughout diastole throughout diastole

Hepatic veinHepatic vein
have a characteristic have a characteristic biphasic or triphasic biphasic or triphasic waveform showing waveform showing hepatofugal flow hepatofugal flow during most of the during most of the cardiac cycle but cardiac cycle but transient hepatopetal transient hepatopetal flow during atrial flow during atrial systole corresponding systole corresponding with the venous 'a' with the venous 'a' wave wave

Portal veinPortal veinPortal flow remains Portal flow remains antegrade throughout the antegrade throughout the normal cardiac and normal cardiac and respiratory cycle slight respiratory cycle slight cyclical variation cyclical variation The main portal vein The main portal vein ascends in the porta hepatis ascends in the porta hepatis , where it divides into right , where it divides into right and left branches. The right and left branches. The right portal vein divides into portal vein divides into anterior and posterior anterior and posterior branches branches Main portal vein is less than Main portal vein is less than 13 mm in diameter 13 mm in diameter examined in the left examined in the left posterior oblique position posterior oblique position

Diffuse pathology: Fatty liverDiffuse pathology: Fatty liver NUTRITIONAL Obesity Intestinal NUTRITIONAL Obesity Intestinal bypass Parenteral nutrition bypass Parenteral nutrition METABOLIC METABOLIC Diabetes mellitus Glycogen storage Diabetes mellitus Glycogen storage disease Hyperlipidaemias DRUG disease Hyperlipidaemias DRUG RELATED Alcohol Corticosteroids RELATED Alcohol Corticosteroids Cytotoxic agentsCytotoxic agentsIDIOPATHICIDIOPATHICALCOHOLMETABOLIC HaemochroALCOHOLMETABOLIC Haemochromatosis Wilsons disease Alpha-1-matosis Wilsons disease Alpha-1-antitrypsin deficiency CHOLESTASISantitrypsin deficiency CHOLESTASISPrimary and Secondary biliary Primary and Secondary biliary cirrhosiscirrhosisIMPAIRED VENOUS OUTFLOW IMPAIRED VENOUS OUTFLOW Budd-Chiari syndrome Veno-Budd-Chiari syndrome Veno-occlusive disease Chronic cardiac occlusive disease Chronic cardiac failure failure DRUGS Methotrexate MethotrexateDRUGS Methotrexate MethotrexateCRYPTOGENICCRYPTOGENIC

Focal fatty infiltrationFocal fatty infiltration
usually affects large usually affects large areas of the liver with a areas of the liver with a geographical or wedge-geographical or wedge-shaped outline and a shaped outline and a subcapsular distribution. subcapsular distribution. Areas of focal fatty Areas of focal fatty infiltration commonly infiltration commonly interdigitate with areas of interdigitate with areas of normal hepatic normal hepatic parenchyma. parenchyma. Normal vessels may be Normal vessels may be seen coursing through seen coursing through these areas indicating these areas indicating preservation of hepatic preservation of hepatic architecture. architecture.

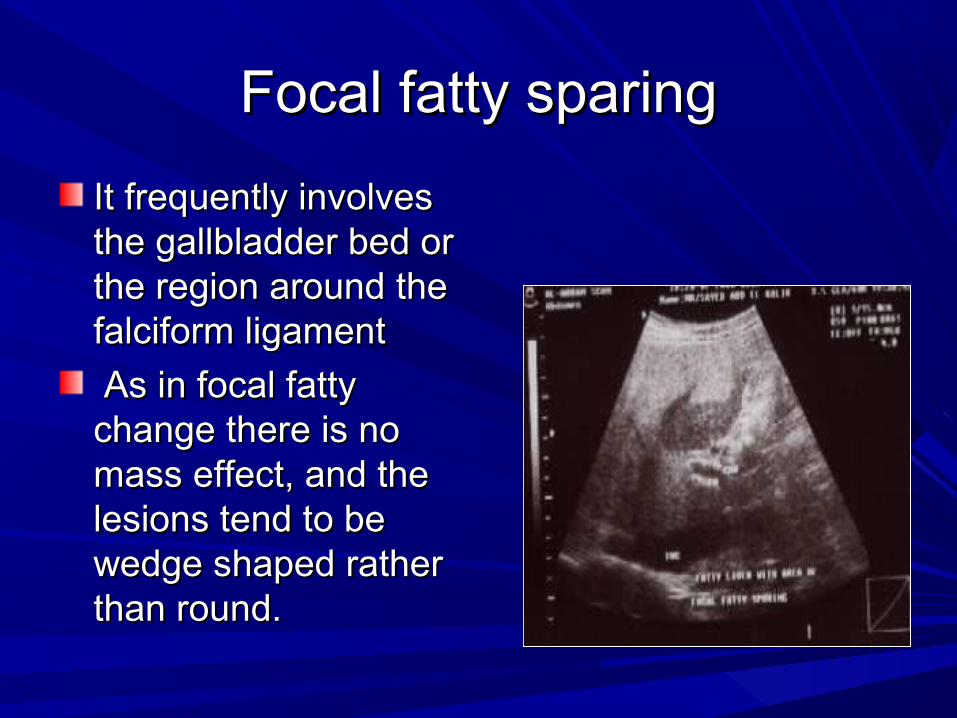
Focal fatty sparingFocal fatty sparing
It frequently involves It frequently involves the gallbladder bed or the gallbladder bed or the region around the the region around the falciform ligamentfalciform ligament
As in focal fatty As in focal fatty change there is no change there is no mass effect, and the mass effect, and the lesions tend to be lesions tend to be wedge shaped rather wedge shaped rather than round. than round.

Findings in early cirrhosisFindings in early cirrhosis
Subtle surface Subtle surface nodularity of the liver, nodularity of the liver, especially in alcoholic especially in alcoholic cirrhosis, which is cirrhosis, which is typically micronodular typically micronodular in its early stages. in its early stages. ( 7.5 MHz probe )( 7.5 MHz probe )Alteration in the Alteration in the Doppler waveform of Doppler waveform of the hepatic veins, with the hepatic veins, with loss of normal flow loss of normal flow reversal reversal


Advanced cirrhosisAdvanced cirrhosisReduced liver size with Reduced liver size with caudate enlargement: a caudate enlargement: a caudate to right lobe caudate to right lobe transverse diameter ratio transverse diameter ratio of 0.65 is said to be of 0.65 is said to be highly specific and highly specific and moderately sensitive in moderately sensitive in the diagnosis of cirrhosis the diagnosis of cirrhosis 2· A coarse liver texture 2· A coarse liver texture with a mild increase in with a mild increase in echogenicity.echogenicity.3· Nodularity of the liver 3· Nodularity of the liver surfacesurface

Extrahepatic findingsExtrahepatic findings1· Splenomegaly (spleen > 13 cm).1· Splenomegaly (spleen > 13 cm).2· Portal vein enlargement > 13 mm.2· Portal vein enlargement > 13 mm.3· Splenic vein enlargement > 10 mm.3· Splenic vein enlargement > 10 mm.4· Loss of respiratory variation in the diameter of the 4· Loss of respiratory variation in the diameter of the portal and splenic veins.portal and splenic veins.5· Reduced or even reversed main portal vein velocity. 5· Reduced or even reversed main portal vein velocity. The main portal vein may be thrombosed or demonstrate The main portal vein may be thrombosed or demonstrate cavernous transformationcavernous transformation6· Portosystemic shunts via the short gastric, left gastric 6· Portosystemic shunts via the short gastric, left gastric and lienorenal veins. These are more easily detected and lienorenal veins. These are more easily detected with the aid of colour Dopplerwith the aid of colour Doppler7. A patent paraumbilical vein with hepatofugal venous 7. A patent paraumbilical vein with hepatofugal venous flow) .8· flow) .8· Ascites - this results from a combination of portal Ascites - this results from a combination of portal hypertension and hypoalbuminemia.Ascites makes hypertension and hypoalbuminemia.Ascites makes surface nodularity of the liver more easily visible.surface nodularity of the liver more easily visible.

Extrahepatic findingsExtrahepatic findings

Budd-Chiari syndromeBudd-Chiari syndrome
ultrasound there is ultrasound there is usually evidence of usually evidence of caudate and/or left lobe caudate and/or left lobe hypertrophy and hypertrophy and sometimes a sometimes a heterogeneous echo heterogeneous echo texture. texture. Ascites may be present. Ascites may be present. The hepatic veins appear The hepatic veins appear abnormal and may be abnormal and may be thrombosed, small and thrombosed, small and irregular in calibre, or not irregular in calibre, or not visualised visualised

Budd-Chiari syndromeBudd-Chiari syndrome
Colour and duplex Doppler Colour and duplex Doppler analysis may demonstrate analysis may demonstrate abnormalities specific to Budd-abnormalities specific to Budd-Chiari syndrome, including Chiari syndrome, including hepatic vein to hepatic vein hepatic vein to hepatic vein collateralscollaterals. The normal triphasic hepatic . The normal triphasic hepatic venous waveform is usually venous waveform is usually lost due to decreased liver lost due to decreased liver compliance or obstruction compliance or obstruction between the hepatic vein and between the hepatic vein and right atrium . right atrium . The sonographic changes of The sonographic changes of portal hypertension are often portal hypertension are often present. present.

HepatitisHepatitismost often produces an most often produces an enlarged liver with normal enlarged liver with normal echogenicity. echogenicity. A generalized reduction in A generalized reduction in echogenicity is occasionally echogenicity is occasionally seen reflecting increased seen reflecting increased tissue fluid and inflammatory tissue fluid and inflammatory cell infiltration . This results in cell infiltration . This results in a dark liver with relatively a dark liver with relatively bright portal tracts. bright portal tracts. Marked thickening of the Marked thickening of the gallbladder wall is frequently gallbladder wall is frequently present. present. Serial measurement of liver Serial measurement of liver size is useful in fulminant size is useful in fulminant hepatitis as a rapidly shrinking hepatitis as a rapidly shrinking liver carries a poor prognosis liver carries a poor prognosis

Diffuse MetastasisDiffuse Metastasis
The presence of a large The presence of a large number of small focal number of small focal lesions may produce the lesions may produce the appearance of diffuse appearance of diffuse disease with a coarse disease with a coarse liver texture liver texture The presence of The presence of hepatomegaly and the hepatomegaly and the absence of other signs of absence of other signs of chronic liver disease help chronic liver disease help to distinguish these cases to distinguish these cases from cirrhosis. from cirrhosis. A similar appearance A similar appearance may be produced by may be produced by multifocal hepatocellular multifocal hepatocellular carcinoma. carcinoma.

Granulomatous diseasesGranulomatous diseasesTuberculosisTuberculosis
Miliary lesions : multiple echogenic foci or even Miliary lesions : multiple echogenic foci or even a diffusely echogenic liver . a diffusely echogenic liver .
Larger confluent granulomata present as echo Larger confluent granulomata present as echo poor or echogenic lesions one to two poor or echogenic lesions one to two centimetres in diameter. centimetres in diameter.
Healed granulomata may calcify. Healed granulomata may calcify.

SarcoidosisSarcoidosis
Hepatic involvement is Hepatic involvement is common in sarcoidosis. common in sarcoidosis.
Hepatomegaly, Hepatomegaly, sometimes with an sometimes with an increase in echogenicity, increase in echogenicity, which may be diffuse or which may be diffuse or inhomogeneous, causing inhomogeneous, causing a coarse liver texture. a coarse liver texture.
The coarse texture is The coarse texture is associated with nodularity associated with nodularity of the liver surfaceof the liver surface

Focal liver pathologyFocal liver pathology Simple cyst Simple cyst
is the commonest cystic liver lesion is the commonest cystic liver lesion encountered encountered They usually arise from They usually arise from developmental abnormalities of the developmental abnormalities of the bile ducts but do not communicate bile ducts but do not communicate with the biliary tree. with the biliary tree. They range from 1 mm in size to 10 They range from 1 mm in size to 10 cm or even larger, and are cm or even larger, and are frequently multiple. frequently multiple. Their characteristics are the same Their characteristics are the same as those of simple cysts elsewhere as those of simple cysts elsewhere – thin walls , anechoic contents – thin walls , anechoic contents and posterior acoustic and posterior acoustic enhancement . Occasional thin enhancement . Occasional thin septa may be present.septa may be present.

HaemangiomaHaemangioma
Hemangioma is the Hemangioma is the commonest benign commonest benign liver tumour liver tumour . . The typical ultrasound The typical ultrasound findings are a solitary, findings are a solitary, round or ovoid, uniformly round or ovoid, uniformly hyperechoic lesion, which hyperechoic lesion, which usually lies in a usually lies in a subcapsular location in subcapsular location in the right lobe . The lesion the right lobe . The lesion usually measures less usually measures less than 4 cm in diameter but than 4 cm in diameter but larger lesions may occur larger lesions may occur

HaemangiomaHaemangiomaThe high echogenicity is due to The high echogenicity is due to multiple reflections from the multiple reflections from the walls of the tiny vascular walls of the tiny vascular spaces found throughout the spaces found throughout the lesion. lesion. However, because the However, because the vascular spaces contain blood, vascular spaces contain blood, there is good through there is good through transmission with larger transmission with larger lesions demonstrating lesions demonstrating posterior acoustic posterior acoustic enhancementenhancement
There is no evidence of There is no evidence of flow on colour Doppler flow on colour Doppler imaging as blood flow imaging as blood flow within hemangiomas is within hemangiomas is too slow to detect too slow to detect

Atypical haemangiomaAtypical haemangioma
Approximately 20 % of Approximately 20 % of hemangiomas have an hemangiomas have an atypical ultrasound atypical ultrasound appearance. appearance. They are completely They are completely anechoic, most of these anechoic, most of these have a partial or complete have a partial or complete echogenic rim and a echogenic rim and a hypoechoic centre. These hypoechoic centre. These changes result from changes result from thrombosis, fibrosis or thrombosis, fibrosis or myxomatous myxomatous degeneration within the degeneration within the hemangioma hemangioma

Liver abscessLiver abscess
An abscess is usually An abscess is usually visible as a round, fluid visible as a round, fluid filled structure, filled structure, sometimes with a sometimes with a thickened wall.thickened wall. Its contents are variably Its contents are variably echogenic and may even echogenic and may even be more echogenic than be more echogenic than surrounding liver, but surrounding liver, but posterior acoustic posterior acoustic enhancement is usually enhancement is usually present indicating its fluid present indicating its fluid nature nature

HydatidHydatid
The classical ultrasound The classical ultrasound appearance is of one or appearance is of one or more cysts with slightly more cysts with slightly thickened echogenic thickened echogenic walls containing a walls containing a combination of dependent combination of dependent debris, termed hydatid debris, termed hydatid sand, daughter cysts and sand, daughter cysts and membranes. However, membranes. However, the hydatid initially the hydatid initially develops as a unilocular develops as a unilocular lesion and may mimic a lesion and may mimic a simple cystsimple cyst

HydatidHydatid The wall becomes thicker and more The wall becomes thicker and more echogenic as the host fibrous echogenic as the host fibrous reaction increases. Eventually it reaction increases. Eventually it calcifies. Complete dense calcifies. Complete dense calcification usually signifies a dying calcification usually signifies a dying or dead cyst.or dead cyst.2. Daughter cysts appear as slight 2. Daughter cysts appear as slight focal wall thickenings, focal wall thickenings, 3. Debris is shed into the parent cyst 3. Debris is shed into the parent cyst and daughter cysts. This debris is and daughter cysts. This debris is composed of scolices,. Together composed of scolices,. Together with infolding and fragmentation of with infolding and fragmentation of the germinal membrane, this results the germinal membrane, this results in a parent cyst full of echogenic in a parent cyst full of echogenic material, which surrounds multiple material, which surrounds multiple fluid filled daughter cysts, giving rise fluid filled daughter cysts, giving rise to the spoke wheel appearance of a to the spoke wheel appearance of a mature hydatidmature hydatid

Amoebic liver abscessAmoebic liver abscessusually found anteriorly in the usually found anteriorly in the right lobe of the liver, possibly right lobe of the liver, possibly because the right lobe receives because the right lobe receives most of the colonic portal most of the colonic portal drainage. drainage. appears as a well-defined cyst, appears as a well-defined cyst, with no visible wall, containing with no visible wall, containing homogeneous low-level echoes, homogeneous low-level echoes, which represent the debris of which represent the debris of lysed liver cells. Posterior lysed liver cells. Posterior acoustic enhancement is usually acoustic enhancement is usually seen , seen , 3 and 17 cm in size . 14% are 3 and 17 cm in size . 14% are multiple. 1% present as diffuse multiple. 1% present as diffuse microabscesses microabscesses Direct extension from liver to lung Direct extension from liver to lung may occur through the right may occur through the right hemidiaphragm. hemidiaphragm.

HepatomaHepatoma
can be classified into can be classified into unifocal, multifocal unifocal, multifocal and diffuse infiltrating and diffuse infiltrating forms.forms.
Hepatomas less than Hepatomas less than 3 cm in diameter are 3 cm in diameter are usually homogenous usually homogenous hypoechoic or hypoechoic or hyperechoic lesions.hyperechoic lesions.

HepatomaHepatoma
As they increase in size, As they increase in size, haemorrhage, necrosis and haemorrhage, necrosis and cystic degeneration cause cystic degeneration cause hepatomas to become hepatomas to become echogenic and heterogeneous. echogenic and heterogeneous. Eighty percent of small Eighty percent of small hepatomas demonstrate hepatomas demonstrate arterial and/or venous flow on arterial and/or venous flow on Doppler ultrasound Doppler ultrasound distinguishing them from distinguishing them from hyperplastic nodules. hyperplastic nodules. Hepatomas larger than 5 cm in Hepatomas larger than 5 cm in diameter frequently diameter frequently demonstrate high velocity demonstrate high velocity blood flow due to arterioportal blood flow due to arterioportal shunting shunting

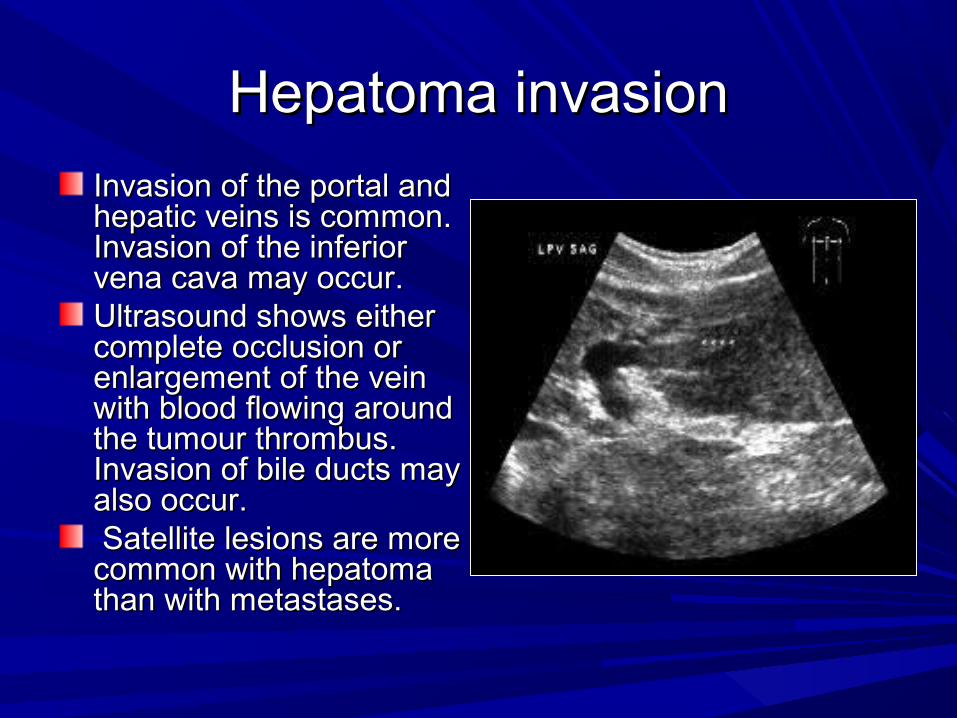
Hepatoma invasionHepatoma invasion
Invasion of the portal and Invasion of the portal and hepatic veins is common. hepatic veins is common. Invasion of the inferior Invasion of the inferior vena cava may occur. vena cava may occur. Ultrasound shows either Ultrasound shows either complete occlusion or complete occlusion or enlargement of the vein enlargement of the vein with blood flowing around with blood flowing around the tumour thrombus. the tumour thrombus. Invasion of bile ducts may Invasion of bile ducts may also occur.also occur. Satellite lesions are more Satellite lesions are more common with hepatoma common with hepatoma than with metastases. than with metastases.

Ultrasound of liver metastasesUltrasound of liver metastases can have a bewildering variety of appearances. Patterns do exist between can have a bewildering variety of appearances. Patterns do exist between ultrasound appearance and likely primary, which is sometimes helpful in ultrasound appearance and likely primary, which is sometimes helpful in directing search for unknown primary, as well as helping distinguish directing search for unknown primary, as well as helping distinguish between benign lesions and metastatic disease form a particular primary. between benign lesions and metastatic disease form a particular primary.
hypoechoic: most common ~ 65%hypoechoic: most common ~ 65% lung cancerlung cancer breast cancerbreast cancer pancreatic adenocarcinomapancreatic adenocarcinoma lymphomalymphoma
hyperechoichyperechoic colorectal carcinoma (CRC)colorectal carcinoma (CRC) renal cell carcinoma (RCC)renal cell carcinoma (RCC) choriocarcinomachoriocarcinoma Kaposi sarcomaKaposi sarcoma neuroendocrine tumours neuroendocrine tumours carcinoidcarcinoid pancreatic islet cell tumourspancreatic islet cell tumours

peripheral halo : a hypoechoic halo peripheral halo : a hypoechoic halo is a concerning featureis a concerning feature
– common in manycommon in many– lung cancerlung cancer
calcifiedcalcified– mucinous adenocarcinomamucinous adenocarcinoma
gastrointestinal gastrointestinal
ovarian mucinous ovarian mucinous adenocarcinomaadenocarcinoma
cysticcystic– squamous cell carcinomasquamous cell carcinoma– ovarian cancerovarian cancer– pancreatic adenocarcinomapancreatic adenocarcinoma– colorectal carcinoma (CRC)colorectal carcinoma (CRC)
poorly defined (infiltrative)poorly defined (infiltrative)– melanomamelanoma– breast cancerbreast cancer– lung cancerlung cancer

Focal metastasesFocal metastases
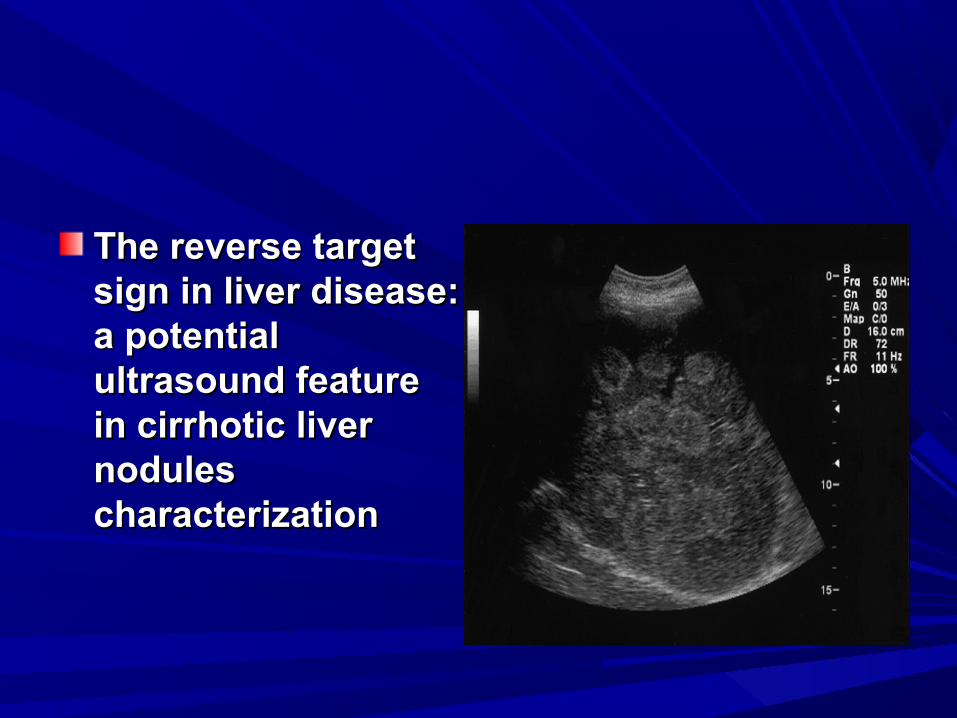
The reverse target The reverse target sign in liver disease: sign in liver disease: a potential a potential ultrasound feature ultrasound feature in cirrhotic liver in cirrhotic liver nodules nodules characterizationcharacterization

Figure 5c. US appearance of FNH. (a) Sagittal US scan shows FNH that is slightly hypoechoic relative to the surrounding liver tissue (arrows) and causes slight distortion of the outer liver
contour.
Hussain S M et al. Radiographics 2004;24:3-17
©2004 by Radiological Society of North America

HaematomaHaematomaappears as an echogenic appears as an echogenic region within the liver. As region within the liver. As it becomes liquefied over it becomes liquefied over subsequent days it forms subsequent days it forms an anechoic collection an anechoic collection with posterior with posterior enhancement and enhancement and irregular walls. irregular walls. It will usually progress to It will usually progress to complete resolution over complete resolution over weeks to months but may weeks to months but may leave a residual scar or a leave a residual scar or a fluid collection with the fluid collection with the appearance of a simple appearance of a simple cyst cyst

Hepatic adenomaHepatic adenoma
is usually a solitary well-circumscribed is usually a solitary well-circumscribed lesion, measuring up to 15 cm in size. Like lesion, measuring up to 15 cm in size. Like FNH it is usually slightly hyperechoic or FNH it is usually slightly hyperechoic or hypoechoic but may become hypoechoic but may become heterogeneous as a result of heterogeneous as a result of haemorrhage or necrosis haemorrhage or necrosis


Biliary systemBiliary system

GBGB
Ultrasound remains the primary imaging Ultrasound remains the primary imaging modality in the evaluation of the modality in the evaluation of the gallbladder and bile ducts. gallbladder and bile ducts.
The most common indications include The most common indications include suspected gallstones, cholecystitis, and suspected gallstones, cholecystitis, and biliary obstruction biliary obstruction
GB techniqueGB technique
The examination is usually performed using The examination is usually performed using 3.5- to 5-MHz transducer.3.5- to 5-MHz transducer. Routine examination includes scanning Routine examination includes scanning subcostally in supine and left posterior oblique subcostally in supine and left posterior oblique positions. positions. Scanning may be performed intercostally, if Scanning may be performed intercostally, if there is shadowing from bowel gas. there is shadowing from bowel gas. Additionally, examination in either the erect or Additionally, examination in either the erect or prone position . The prone view is useful for prone position . The prone view is useful for demonstrating the mobility of the stones, for demonstrating the mobility of the stones, for avoiding reverberation artifacts in anteriorly avoiding reverberation artifacts in anteriorly placed gallbladders placed gallbladders

Prone positionProne position

GB anatomyGB anatomy
on the transverse view the on the transverse view the gallbladder is located gallbladder is located posterior to or partly within posterior to or partly within the main lobar fissure, the main lobar fissure, between the right lobe and between the right lobe and the medial segment of the the medial segment of the left lobe left lobe On the longitudinal view, the On the longitudinal view, the linear hyperechoic main linear hyperechoic main lobar fissure can be seen lobar fissure can be seen between the gallbladder between the gallbladder caudally and the right portal caudally and the right portal vein cranially in many vein cranially in many persons (nearly 70%) persons (nearly 70%)

Sonographic anatomy of the gall bladderSonographic anatomy of the gall bladder
Sonographically, the Sonographically, the gallbladder is an gallbladder is an anechoic, fluid-filled, anechoic, fluid-filled, pear-shaped or pear-shaped or ellipsoid structure, ellipsoid structure, widest at the fundus widest at the fundus and narrowest at the and narrowest at the neck. neck.


Size: If it's transverse diameter exceeds 5 cm, the gall bladder is likely to be hydropic.If its diameter is less than 2 cm despite adequate fasting, the gall bladder is likely to be abnormally contracted.
Gall bladder wall : A pencil thin echogenic line that is less than 3 mm thick.
Sonographic anatomy of the gal l Sonographic anatomy of the gal l bladderbladder

The shape of the gallbladderThe shape of the gallbladdercan vary because of its folds. The folds are caused by can vary because of its folds. The folds are caused by infolding of the gallbladder wall and do not represent true infolding of the gallbladder wall and do not represent true septations within the gallbladder. septations within the gallbladder. The most common fold (the junctional fold) is seen at the The most common fold (the junctional fold) is seen at the junction of the neck and the body of the gallbladder.junction of the neck and the body of the gallbladder. Less commonly, folds can occur in the mid-body or Less commonly, folds can occur in the mid-body or distal body of the gallbladder, and multiple folds can give distal body of the gallbladder, and multiple folds can give the gallbladder a sigmoid (S) shape .the gallbladder a sigmoid (S) shape . A "phrygian cap" deformity is caused by folding of the A "phrygian cap" deformity is caused by folding of the fundus over the body of the gallbladder and is seen in fundus over the body of the gallbladder and is seen in approximately 4% of healthy persons A phrygian cap approximately 4% of healthy persons A phrygian cap deformity results when a mucosal fold partially deformity results when a mucosal fold partially subdivides the lumen of the gallbladder. Occasionally, subdivides the lumen of the gallbladder. Occasionally, prominent folds may cause acoustic shadowing. prominent folds may cause acoustic shadowing. When only a part of the fold is visualized, it may mimic a When only a part of the fold is visualized, it may mimic a polyp or a stone polyp or a stone

Shapes of GBShapes of GB

Detection of cholelithiasis is the primary role Detection of cholelithiasis is the primary role of gall bladder sonography, showing of gall bladder sonography, showing posterior acoustic shadowing and mobility posterior acoustic shadowing and mobility
of the stoneof the stone..

Wall echo shadow triadWall echo shadow triad

Thickened wallThickened wall

Pericholecystic f luidPericholecystic f luid

Role of color Doppler Role of color Doppler sonographysonography

Complications of acute Complications of acute cholecystit ischolecystit is
Mucocele of GB

Emphysematous cholecystitisEmphysematous cholecystitis

GB polypsGB polyps

GB massGB mass


Choledocal cystCholedocal cyst

Caroli diseaseCaroli disease
is a nonobstructive dilatation of the is a nonobstructive dilatation of the intrahepatic bile ducts. This is a rare intrahepatic bile ducts. This is a rare congenital disorder that classically causes congenital disorder that classically causes saccular ductal dilatation, which usually is saccular ductal dilatation, which usually is segmental. Caroli disease is associated segmental. Caroli disease is associated with recurrent bacterial cholangitis and with recurrent bacterial cholangitis and stone formation.stone formation.

Caroli diseaseCaroli diseaseUltrasonography is widely Ultrasonography is widely available, and it often is available, and it often is used first in the diagnosis used first in the diagnosis of any process involving of any process involving the liver; therefore, it is the liver; therefore, it is commonly performed commonly performed early in the workup of early in the workup of patients with Caroli patients with Caroli disease. disease. Demonstration of the Demonstration of the continuity of the cystic continuity of the cystic lesions with the bile ducts lesions with the bile ducts is paramount in is paramount in diagnosis. diagnosis.

CaroliCaroli


The spleenThe spleen
The spleen normally lies in the left upper The spleen normally lies in the left upper quadrant of the abdomen between the 9th quadrant of the abdomen between the 9th and 11th ribs. and 11th ribs.
It is the largest lymphoid gland in the body It is the largest lymphoid gland in the body with a mean weight of 150 -180 grams. with a mean weight of 150 -180 grams.
The long axis of the spleen is normally The long axis of the spleen is normally less than 13 cms some departments use less than 13 cms some departments use 12 cms as their maximum length 12 cms as their maximum length

TechniqueTechnique
The spleen is initially examined The spleen is initially examined with the patient lying supine, with the patient lying supine, the transducer being placed the transducer being placed between the ribs in or near the between the ribs in or near the mid axillary line to produce mid axillary line to produce coronal and transverse images. coronal and transverse images. Scanning is performed Scanning is performed throughout quiet respiration. A throughout quiet respiration. A deep inspiration often produces deep inspiration often produces poor images by extending the poor images by extending the pulmonary sulcus. pulmonary sulcus. Visualisation of the normal Visualisation of the normal sized spleen may be improved sized spleen may be improved by the patient lying in the right by the patient lying in the right lateral decubitus position lateral decubitus position

The spleenThe spleen

EchopatternEchopattern
The normal splenic parenchyma displays The normal splenic parenchyma displays a homogeneous pattern, which consists in a homogeneous pattern, which consists in the main of low-level echoes. the main of low-level echoes. The splenic hilum, unlike the splenic The splenic hilum, unlike the splenic substance, returns higher-level echoes. substance, returns higher-level echoes. The normal splenic tissue is generally of The normal splenic tissue is generally of slightly lower reflectivity than hepatic slightly lower reflectivity than hepatic tissue, however, it may occasionally be tissue, however, it may occasionally be more reflective in normal subjects. more reflective in normal subjects.

Accessory spleenAccessory spleen
The incidence of an accessory The incidence of an accessory spleen, or splenunculus, is spleen, or splenunculus, is approximately 10 % on autopsy approximately 10 % on autopsy studies, but they may be too small studies, but they may be too small to be identified on ultrasound .to be identified on ultrasound . They are almost always single, They are almost always single, but occasionally two or more may but occasionally two or more may be present. be present. They are smooth rounded nodules They are smooth rounded nodules 1-2 cms in diameter situated at or 1-2 cms in diameter situated at or near the splenic hilum .near the splenic hilum .Diagnosis is made from their Diagnosis is made from their position and texture. Hypertrophy position and texture. Hypertrophy of an accessory spleen in post of an accessory spleen in post splenectomy patients is a well-splenectomy patients is a well-recorded observation recorded observation

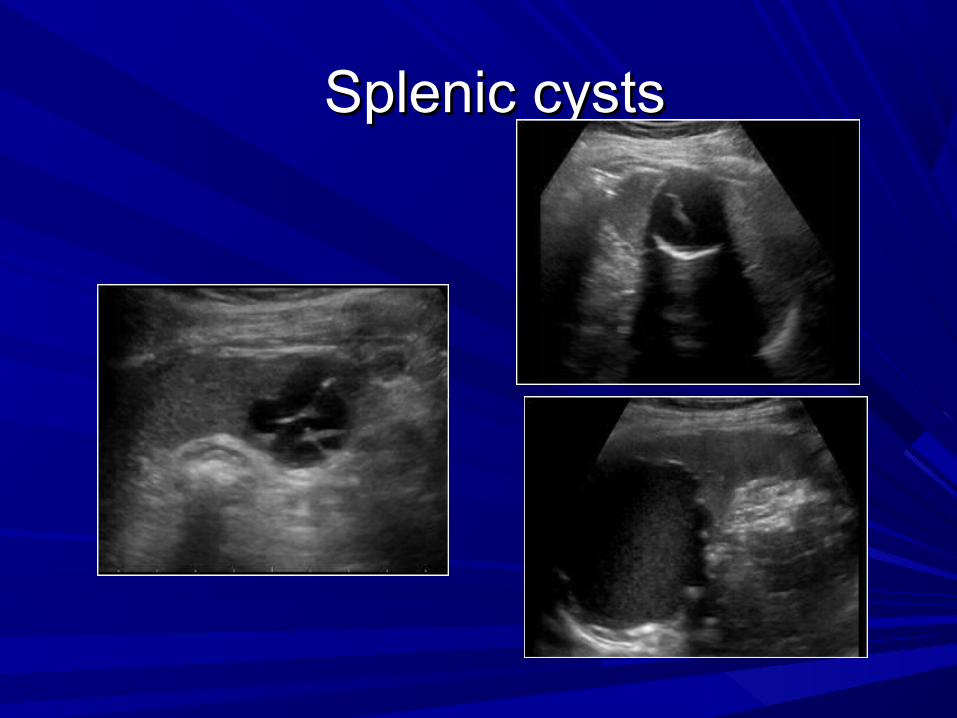
Splenic cystsSplenic cysts

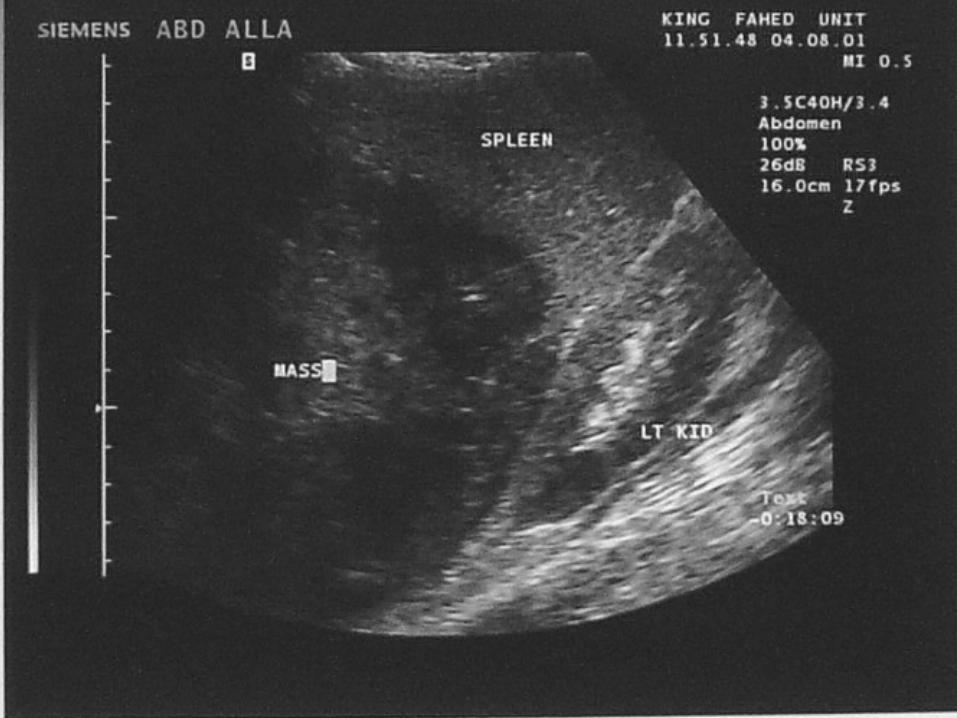
Splenic metastasisSplenic metastasis

PancreasPancreasTransverse scans utilize the left lobe of the liver Transverse scans utilize the left lobe of the liver as much as possible as a window into the as much as possible as a window into the pancreatic bed, Sagittal scanning begins in the pancreatic bed, Sagittal scanning begins in the midline, identifying the great vessels and midline, identifying the great vessels and proceeds to the right until the right kidney is proceeds to the right until the right kidney is seen and left to the splenic hilum seen and left to the splenic hilum In both scan planes steady, firm pressure In both scan planes steady, firm pressure gradually applied will frequently eliminate gradually applied will frequently eliminate interposed bowel gas and allow pancreatic interposed bowel gas and allow pancreatic imaging imaging Additionally, having the patient drink 250 -500 cc Additionally, having the patient drink 250 -500 cc of water may replace stomach gas and provide a of water may replace stomach gas and provide a window into the pancreas window into the pancreas


Pancreatic sizePancreatic size
Normal AP measurements of the head, neck, body and Normal AP measurements of the head, neck, body and tail to be in the range of 3.5 cm, 2.0 cm, 2.5 cm and 2.5 tail to be in the range of 3.5 cm, 2.0 cm, 2.5 cm and 2.5 cm, respectively. cm, respectively. In actual practice, focal enlargement or localized change In actual practice, focal enlargement or localized change in texture carries much more significance than an in texture carries much more significance than an aberrant measurement aberrant measurement

EchopatternEchopattern
The texture of the pancreas varies with age. In the infant The texture of the pancreas varies with age. In the infant and young child the gland may be hypoechoic as and young child the gland may be hypoechoic as compared with the normal liver. This is attributed to the compared with the normal liver. This is attributed to the preponderance of glandular tissue and relative paucity of preponderance of glandular tissue and relative paucity of both fat and fibrous elements both fat and fibrous elements

Pancreatic ductPancreatic duct
The pancreatic duct may be seen as a single echogenic The pancreatic duct may be seen as a single echogenic line within the gland; line within the gland; occasionally the duct contains sufficient fluid to appear occasionally the duct contains sufficient fluid to appear tubular with both echogenic walls imaged. This is still tubular with both echogenic walls imaged. This is still considered normal so long as the internal diameter of the considered normal so long as the internal diameter of the duct does not exceed 2-2.5 mm duct does not exceed 2-2.5 mm

acute pancreatitisacute pancreatitisThe classic sonographic The classic sonographic findings diffuse findings diffuse enlargement of the gland enlargement of the gland with a generalized with a generalized decrease in its decrease in its echogenicity. echogenicity. Hypoechoic focal Hypoechoic focal enlargement of the enlargement of the pancreas is also possible pancreas is also possible in acute inflammation; in acute inflammation; this is generally confined this is generally confined to the head, and focal to the head, and focal enlargement confined to enlargement confined to the tail would be unusual the tail would be unusual in pancreatitis and much in pancreatitis and much more worrisome for more worrisome for neoplasm neoplasm
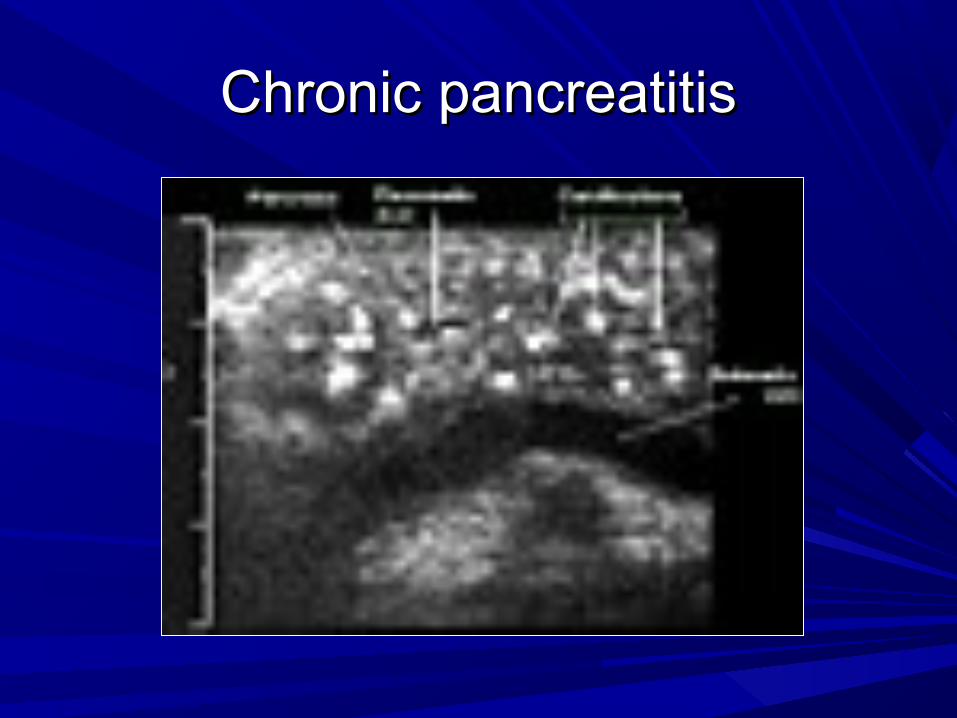
Chronic pancreatitisChronic pancreatitis


AortaAorta
The patient is initially The patient is initially scanned in the supine scanned in the supine position during quiet position during quiet respiration. respiration. Transverse scans are Transverse scans are used to localise and used to localise and follow the course of the follow the course of the great vessels within the great vessels within the abdomen. The aorta can abdomen. The aorta can be traced from the be traced from the diaphragm to the diaphragm to the bifurcation in most bifurcation in most patients. patients. Longitudinal scans are Longitudinal scans are then used to demonstrate then used to demonstrate the long axis of the the long axis of the vessels vessels

AortaAorta
The aorta measures The aorta measures approximately 2.5 cm approximately 2.5 cm in diameter at the in diameter at the level of the crura and level of the crura and it tapers to a mean it tapers to a mean diameter of 1.5 cm at diameter of 1.5 cm at the bifurcation the bifurcation

Aortic thrombosisAortic thrombosis

Saccular Aortic aneuryzmSaccular Aortic aneuryzm

Thrombosed aneuryzmThrombosed aneuryzm

Lymph NodesLymph Nodes To search for lymphadenopathy To search for lymphadenopathy
Identify the associated vessels and trace their Identify the associated vessels and trace their abdominal courses looking for para-vascular abdominal courses looking for para-vascular echo poor masses. Enlarged nodes may be echo poor masses. Enlarged nodes may be found at the porta hepatis, renal hila, splenic found at the porta hepatis, renal hila, splenic hilum and in the mesentery as well as around hilum and in the mesentery as well as around the coeliac axis and along the pancreas. the coeliac axis and along the pancreas. The commonest sites are in the para-aortic and The commonest sites are in the para-aortic and retro-aortic areas, the iliac chains and retro-aortic areas, the iliac chains and retrocrurally. retrocrurally. Normal nodes measure up to 1 cm in diameter Normal nodes measure up to 1 cm in diameter except in the retrocrural area where over 0.6 cm except in the retrocrural area where over 0.6 cm is considered abnormal is considered abnormal

To search for lymphadenopathyTo search for lymphadenopathy

Role Of Ultrasound In The Role Of Ultrasound In The Assessment Of gutAssessment Of gut

Four histologic layers of the gutFour histologic layers of the gut
MucosaMucosa :consists of an epithelial lining :consists of an epithelial lining ,loose connective tissue or lamina propria, ,loose connective tissue or lamina propria, and muscularis mucosaand muscularis mucosa
Submucosa Submucosa
Muscularis propriaMuscularis propria with inner circular with inner circular and outer longitudinal fibersand outer longitudinal fibers
Serosa or adventitiaSerosa or adventitia




Normal stomach ultrasoundNormal stomach ultrasound

Thick stomach wallThick stomach wall

Ultrasound of a stomach filled with Ultrasound of a stomach filled with waterwater

Gut wall pathologyGut wall pathology
Diffuse Diffuse
Focal Focal

Inflammatory bowel diseaseInflammatory bowel disease


FocalFocal
IntraluminalIntraluminal . .
Exophytic componentExophytic component..
UlcerationUlceration..




The appendix is seen as The appendix is seen as a blind ended, tubular a blind ended, tubular structure with a laminated structure with a laminated wall wall
arises from the base of arises from the base of the caecum in the the caecum in the longitudinal plane and as longitudinal plane and as a target in the transverse a target in the transverse plane. plane.
It should be aperistaltic It should be aperistaltic and non compressible and non compressible

Graded Graded compression compression describes the use of describes the use of uniform pressure on uniform pressure on the region of the region of interest. interest. Compression should Compression should be applied in a be applied in a graded manner to graded manner to avoid pain.avoid pain.

Sonographic criteriaSonographic criteriaof acute appendicitisof acute appendicitis
Tenderness on probingTenderness on probing
Thickened wall(>6mm)Thickened wall(>6mm)
Presence of peri-appendiceal fluidPresence of peri-appendiceal fluid
Distended appendixDistended appendix
The presence of an appendicolithThe presence of an appendicolith
Increased vascularity Increased vascularity

acute appendicitisacute appendicitis

KidneysKidneys

KidneysKidneys
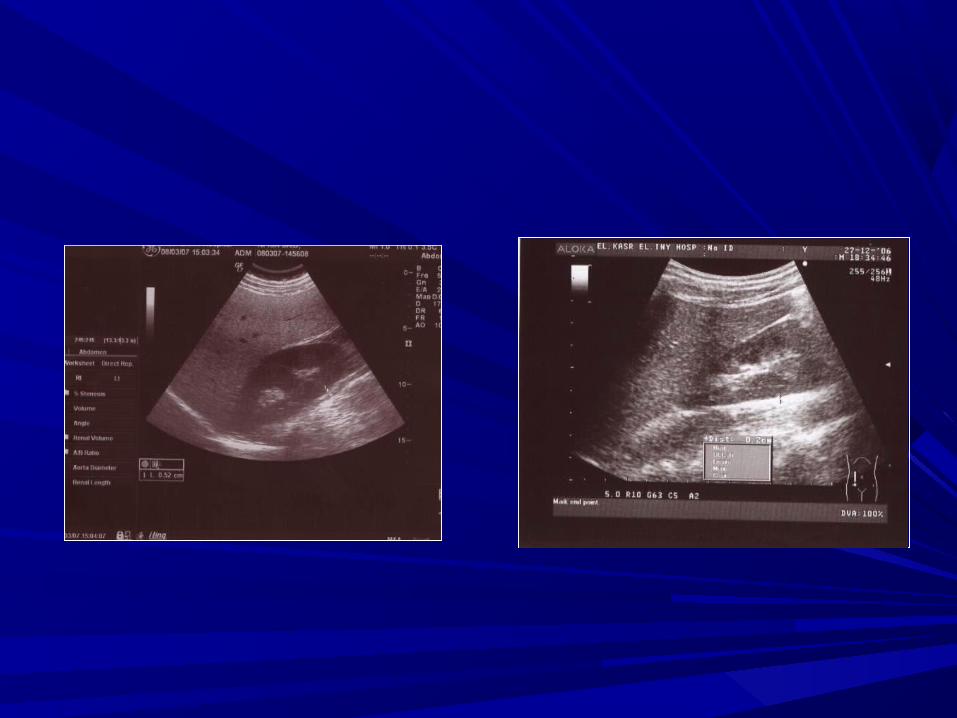

Medical renal diseaseMedical renal disease

Grade IGrade I

Grade II nephropathyGrade II nephropathy

Grade IIIGrade III
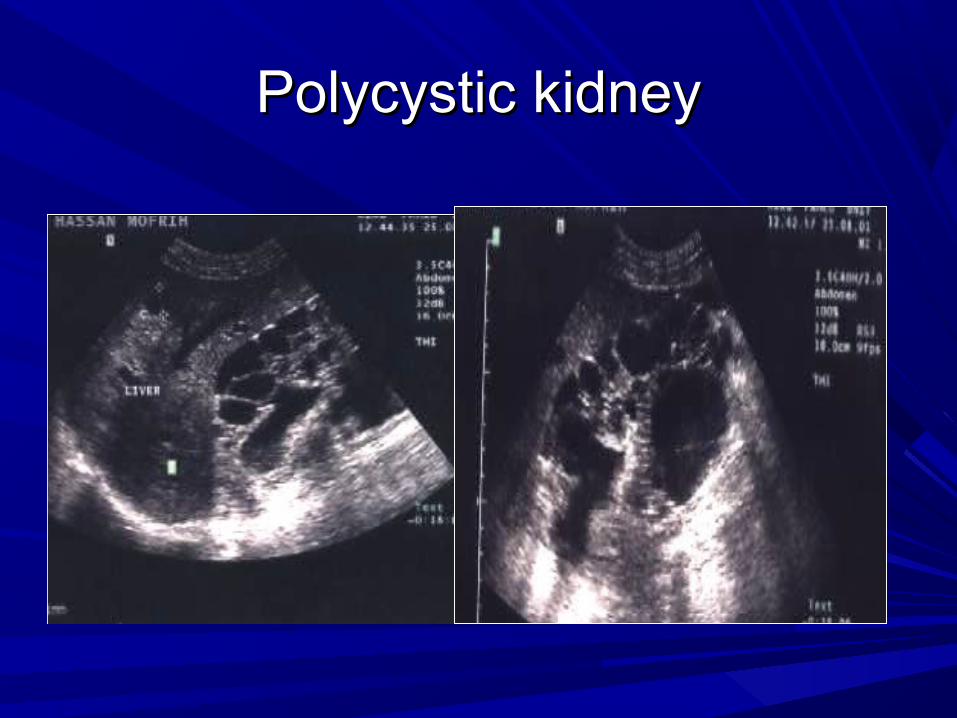
Polycystic kidneyPolycystic kidney
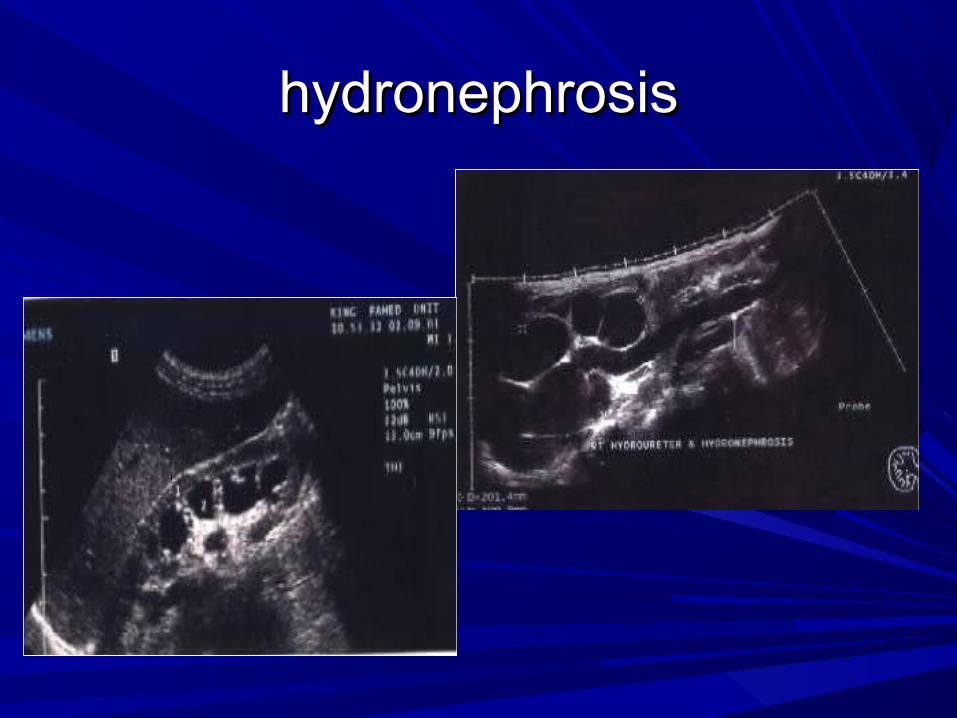
hydronephrosishydronephrosis

HydronephrosisHydronephrosis
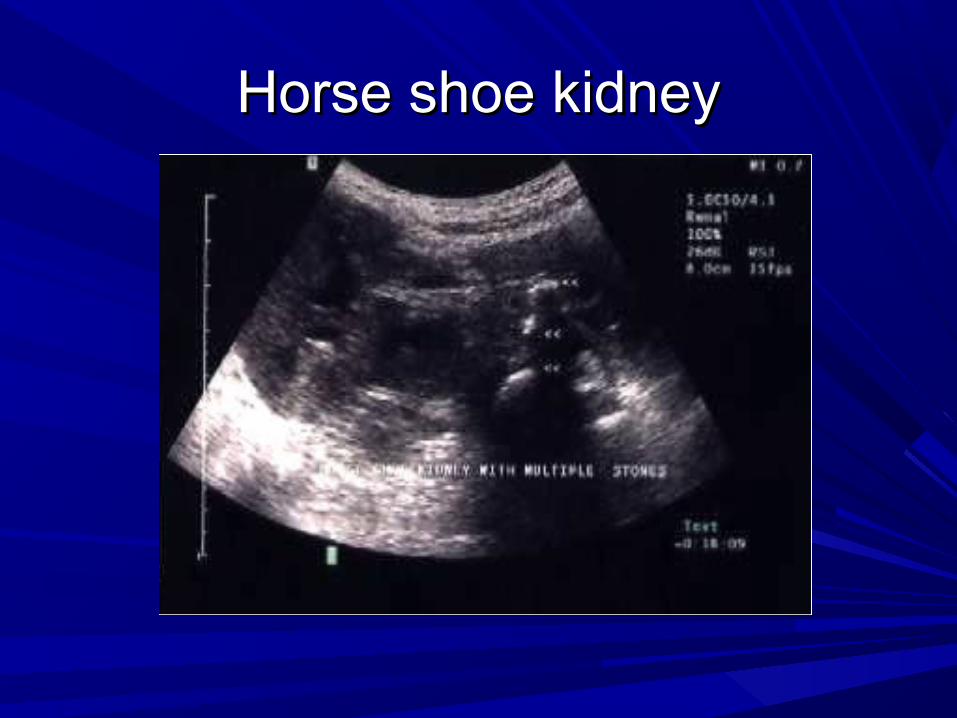
Horse shoe kidneyHorse shoe kidney

Renal stones& massRenal stones& mass


AdrenalsAdrenals
Adrenal Adrenal hemorrhagehemorrhage
Spontaneous Spontaneous Traumatic Traumatic

Adrenal cystAdrenal cyst

Adrenal massAdrenal mass

Adrenal massAdrenal mass

Adrenal cortical caAdrenal cortical ca

Adrenal lymphomaAdrenal lymphoma
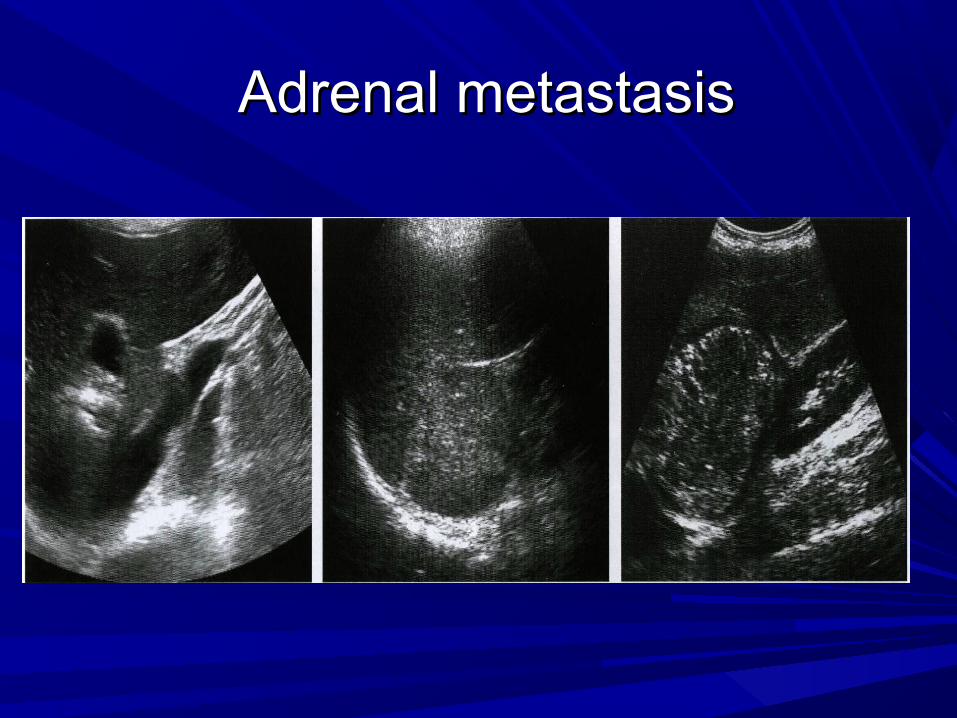
Adrenal metastasisAdrenal metastasis

Urinary bladderUrinary bladder
The most common use for bladder ultrasound is The most common use for bladder ultrasound is the assessment of residual bladder volume in the assessment of residual bladder volume in patients with outflow obstruction. patients with outflow obstruction. Ultrasound may also be used to look for bladder Ultrasound may also be used to look for bladder tumors in cases of hematuria or high-risk tumors in cases of hematuria or high-risk patients, but is inferior to cystoscopy for the patients, but is inferior to cystoscopy for the detection of tumors and inferior to CT or MRI for detection of tumors and inferior to CT or MRI for staging. staging. Other abnormalities such as bladder diverticulae Other abnormalities such as bladder diverticulae are usually incidental findings are usually incidental findings

Causes of a small, shrunken Causes of a small, shrunken bladderbladder
Partial cystectomyPartial cystectomy
Chronic cystitisChronic cystitis TuberculosisTuberculosis SchistosomiasisSchistosomiasis Postvaricella cystitisPostvaricella cystitis
RadiationRadiation
PostchemotherapyPostchemotherapy
Interstitial cystitisInterstitial cystitis
Eosinophilic cystitisEosinophilic cystitis
Neurogenic bladderNeurogenic bladder
Repeated fulgurationRepeated fulguration
(Reduced functional capacity)(Reduced functional capacity)

Causes of a large bladder Causes of a large bladder volumevolume
CongenitalCongenital
Prolonged bladder Prolonged bladder outflow obstructionoutflow obstruction
Neurogenic bladderNeurogenic bladder
Infrequent voidingInfrequent voiding

Causes of pear-shaped bladderCauses of pear-shaped bladderLarge psoas musclesLarge psoas muscles
Pelvic lymphadenopathyPelvic lymphadenopathy
Pelvic lipomatosisPelvic lipomatosis
Pelvic hematomaPelvic hematoma
RareRare
Retroperitoneal fibrosisRetroperitoneal fibrosis
Bilateral lymphocelesBilateral lymphoceles
Bilateral pelvic abscessesBilateral pelvic abscesses
Bilateral urinomasBilateral urinomas
Bilateral iliac artery Bilateral iliac artery aneurysmsaneurysms
Bilateral renal transplantsBilateral renal transplants

The thickness of the bladderThe thickness of the bladder vary according to its distension. In vary according to its distension. In a normal bladder, the wall a normal bladder, the wall decreases in thickness until it is decreases in thickness until it is half full (200–250 mL), half full (200–250 mL),
The range of thickness is 3–5 mm, The range of thickness is 3–5 mm, but with a full bladder it should be but with a full bladder it should be smooth and measure <3 mm. smooth and measure <3 mm.
Chronic diffuse thickening of the Chronic diffuse thickening of the bladder is most commonly due to bladder is most commonly due to muscular hypertrophy ,a muscular hypertrophy ,a compensatory phenomenon compensatory phenomenon secondary to significant outflow secondary to significant outflow obstruction (e.g., due to obstruction (e.g., due to prostatomegaly or urethral prostatomegaly or urethral stricture) or with a neurogenic stricture) or with a neurogenic bladder.bladder.

Residual urineResidual urine

THE URETERSTHE URETERS
The upper ureters are demonstrated on oblique The upper ureters are demonstrated on oblique longitudinal scans as fine structures continuous longitudinal scans as fine structures continuous with the renal pelves. with the renal pelves. The lower ureters may be demonstrated through The lower ureters may be demonstrated through the full bladder, while the mid ureters are the full bladder, while the mid ureters are normally only seen if very dilated. normally only seen if very dilated. The only information usually obtained from an The only information usually obtained from an ultrasound examination about the ureters ultrasound examination about the ureters themselves is the presence and level of themselves is the presence and level of dilatation. Periureteral pathology causing dilatation. Periureteral pathology causing obstruction such as retroperitoneal fibrosis or obstruction such as retroperitoneal fibrosis or invasive prostatic cancer may also be invasive prostatic cancer may also be demonstrated.demonstrated.

Lower ureterLower ureter

ProstateProstate


US guided InterventionUS guided Intervention
FINE NEEDLE BIOPSYFINE NEEDLE BIOPSY
COARSE NEEDLE BIOPSYCOARSE NEEDLE BIOPSY
NEPHROPYELOSTOMYFLUID NEPHROPYELOSTOMYFLUID
COLLECTIONS: ABSCESSES, ASCITES, COLLECTIONS: ABSCESSES, ASCITES, PLEURAL EFFUSIONS AND PERICARDIAL PLEURAL EFFUSIONS AND PERICARDIAL EFFUSIONSEFFUSIONS
CYST THERAPYCYST THERAPY
TUMOR THERAPYTUMOR THERAPY SPECIAL PROCEDURESSPECIAL PROCEDURES
TIPS IndicationsTIPS Indications

Ultrasound guided biopsyUltrasound guided biopsy

Drainage proceduresDrainage procedures
FLUID COLLECTIONS: ABSCESSES, ASCITES, FLUID COLLECTIONS: ABSCESSES, ASCITES, PLEURAL EFFUSIONS AND PERICARDIAL PLEURAL EFFUSIONS AND PERICARDIAL
EFFUSIONSEFFUSIONS

THANK YOU