Embed Size (px)
Citation preview
Endovenous or Surgical Treatment of CVI
Professor Alun H DaviesAcademic Section of Vascular Surgery,
Imperial College,Charing Cross & St Mary’s Hospital,
London
Whom is best the:-
CUTTER
FRYER/FREEZER
STICKER
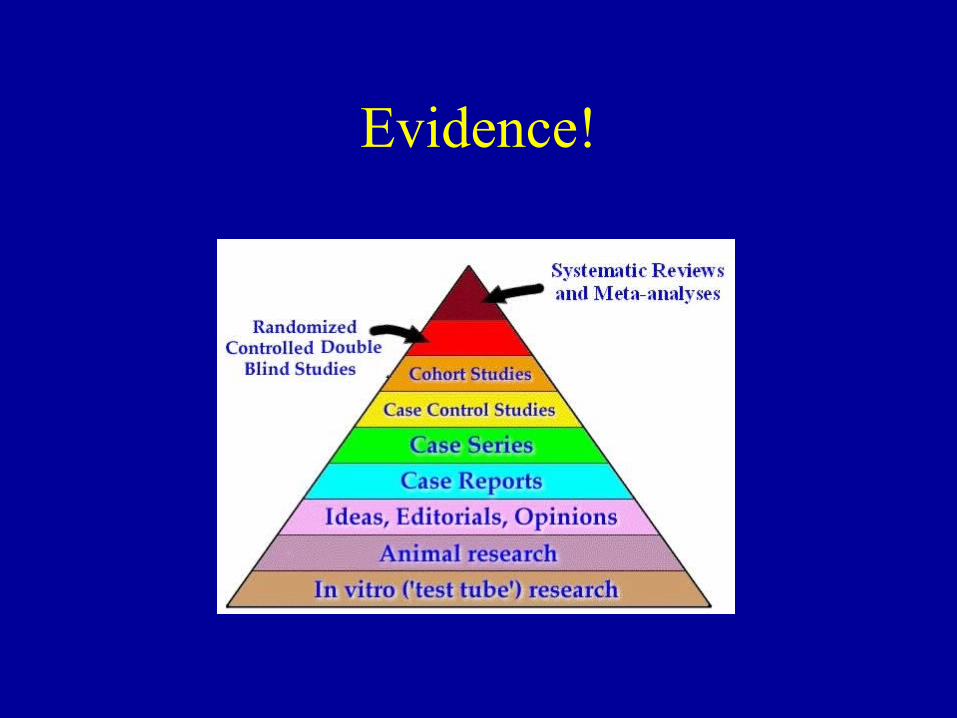
Evidence!
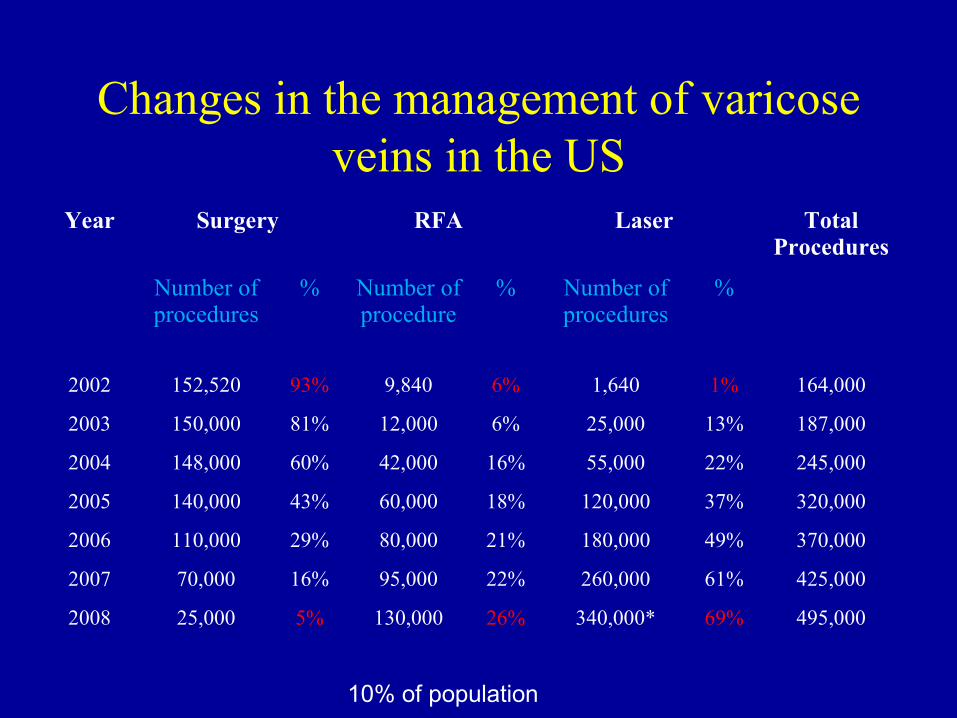
Changes in the management of varicose veins in the US
Year Surgery RFA Laser Total Procedures
Number ofprocedures
% Number of procedure
% Number of procedures
%
2002 152,520 93% 9,840 6% 1,640 1% 164,000
2003 150,000 81% 12,000 6% 25,000 13% 187,000
2004 148,000 60% 42,000 16% 55,000 22% 245,000
2005 140,000 43% 60,000 18% 120,000 37% 320,000
2006 110,000 29% 80,000 21% 180,000 49% 370,000
2007 70,000 16% 95,000 22% 260,000 61% 425,000
2008 25,000 5% 130,000 26% 340,000* 69% 495,000
10% of population
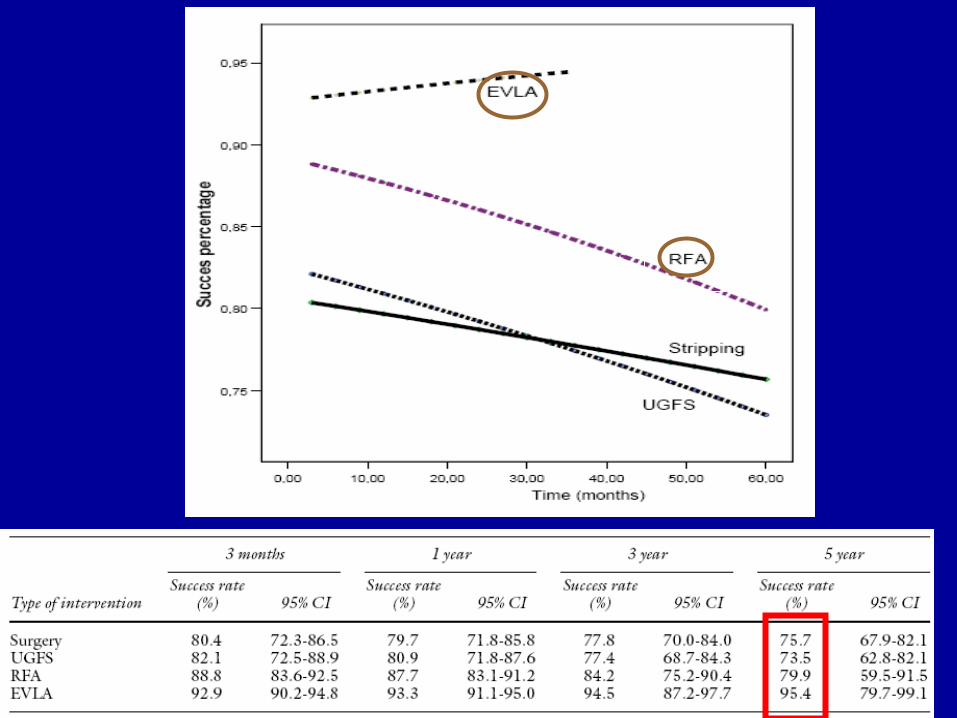
Results
Systematic Review
• Ablation in 87.9-100%
• Re-treatment 1.8-3%
• DVT 1 in 1289 patients 0.08%
• Poor long-term follow up
Mundy et al, 2005
n=1289
Non-occlusive uncertainties
• Stripping operation requires demonstration of sapheno-femoral junction and disconnection
• Endovenous procedures – Occlusion rate of 88-100% after EVLT1
– Open sapheno-femoral junction after RFO in 88%2
– Recanalisation rates of 12%3 ( EVLT) to 25% at 3 years4 (RFO)
1 Proebstle et al. 2003,20062 Pichot et al. 20043 Merchant et al. 20024 Nicolini et al.2005
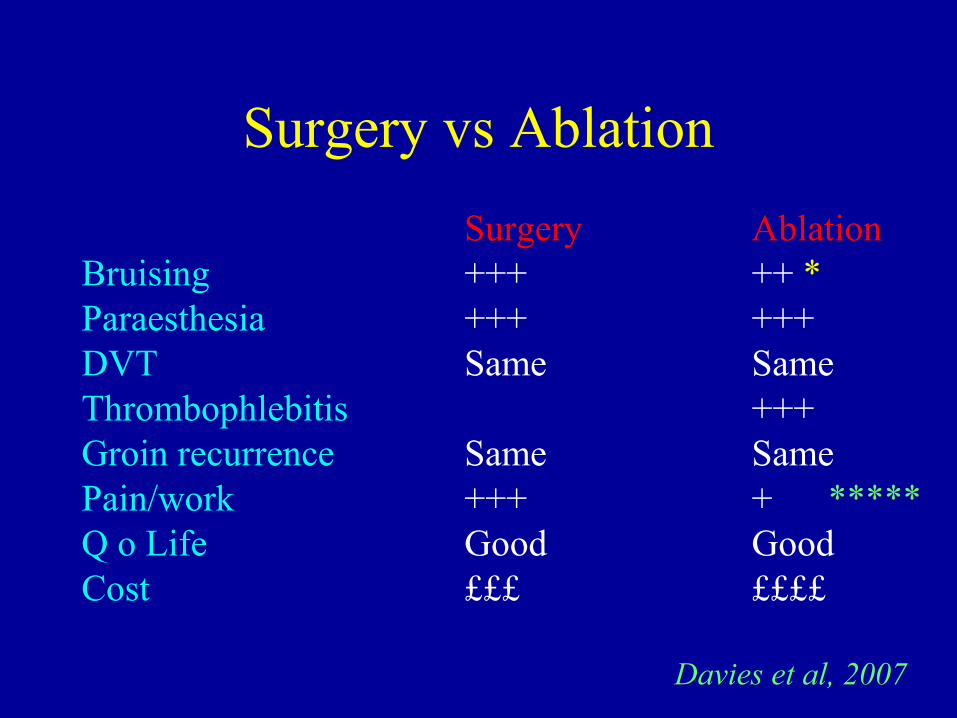
Surgery vs Ablation
Surgery AblationBruising +++ ++ *Paraesthesia +++ +++DVT Same SameThrombophlebitis +++Groin recurrence Same SamePain/work +++ + *****Q o Life Good GoodCost £££ ££££
Davies et al, 2007
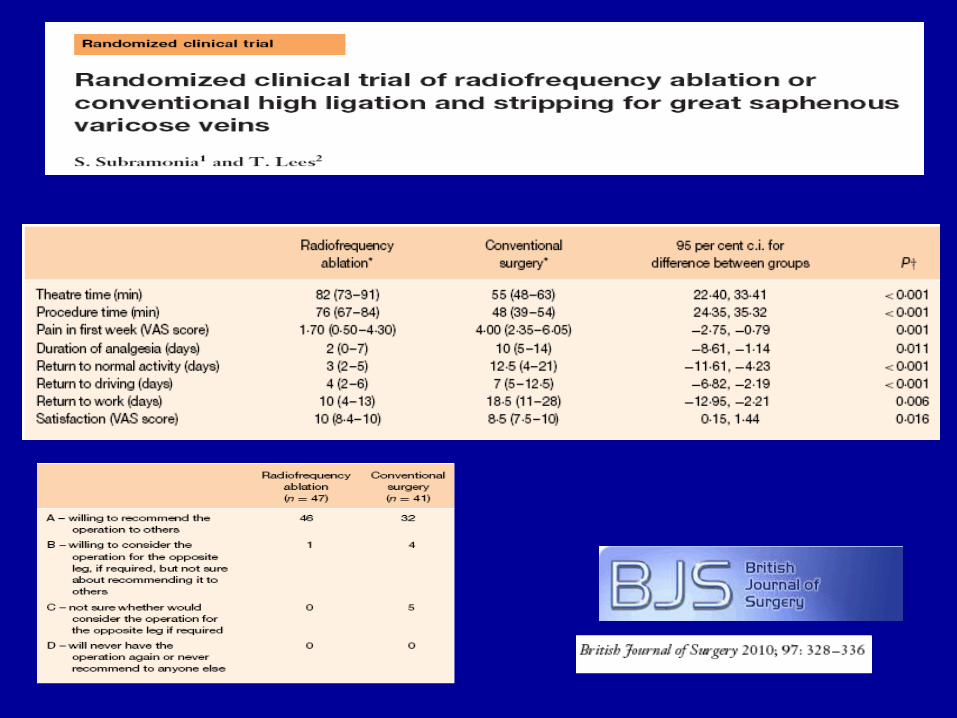

2010
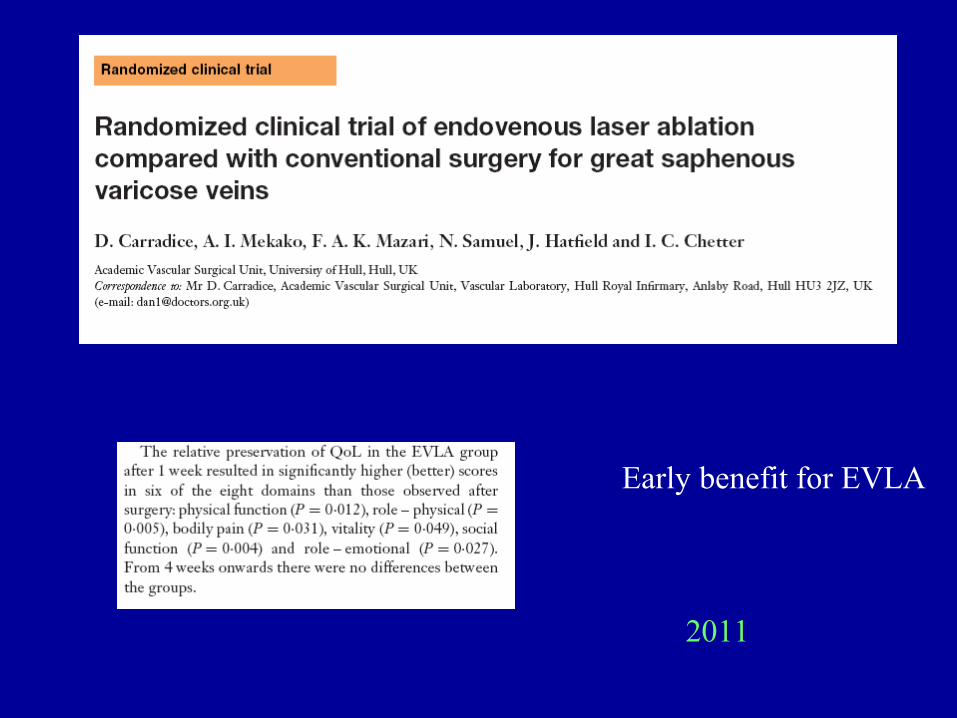
Early benefit for EVLA
2011
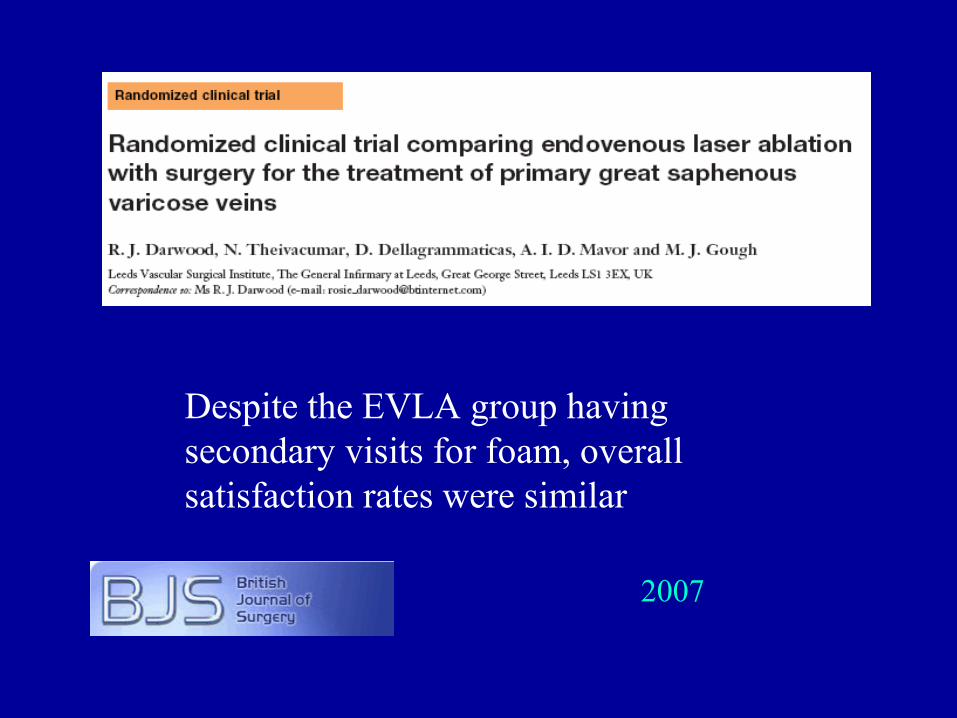
Despite the EVLA group having secondary visits for foam, overall satisfaction rates were similar
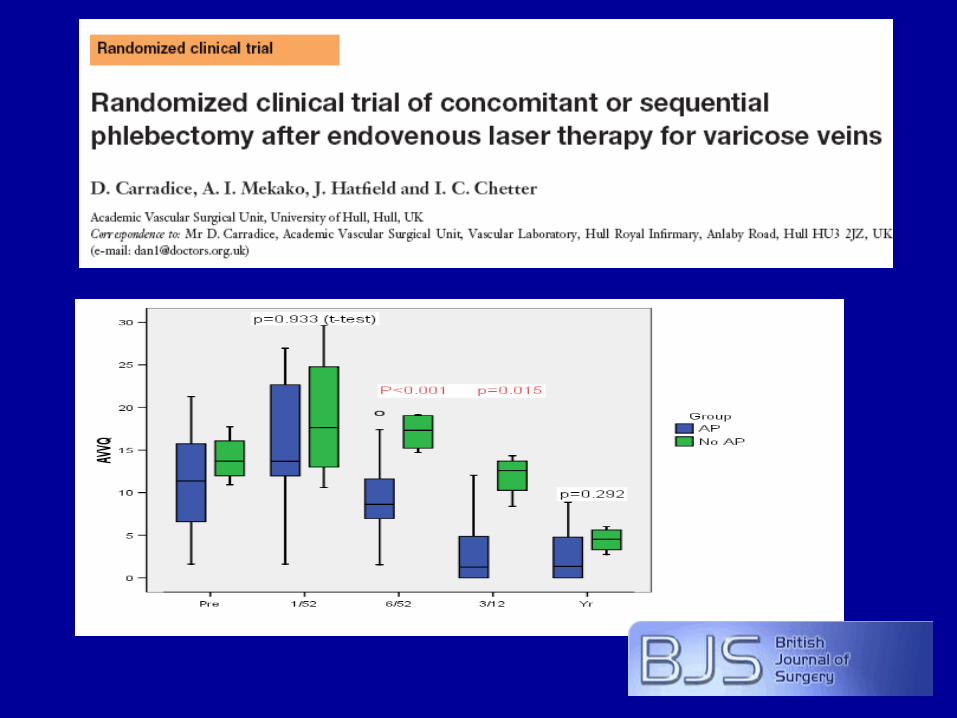
2007
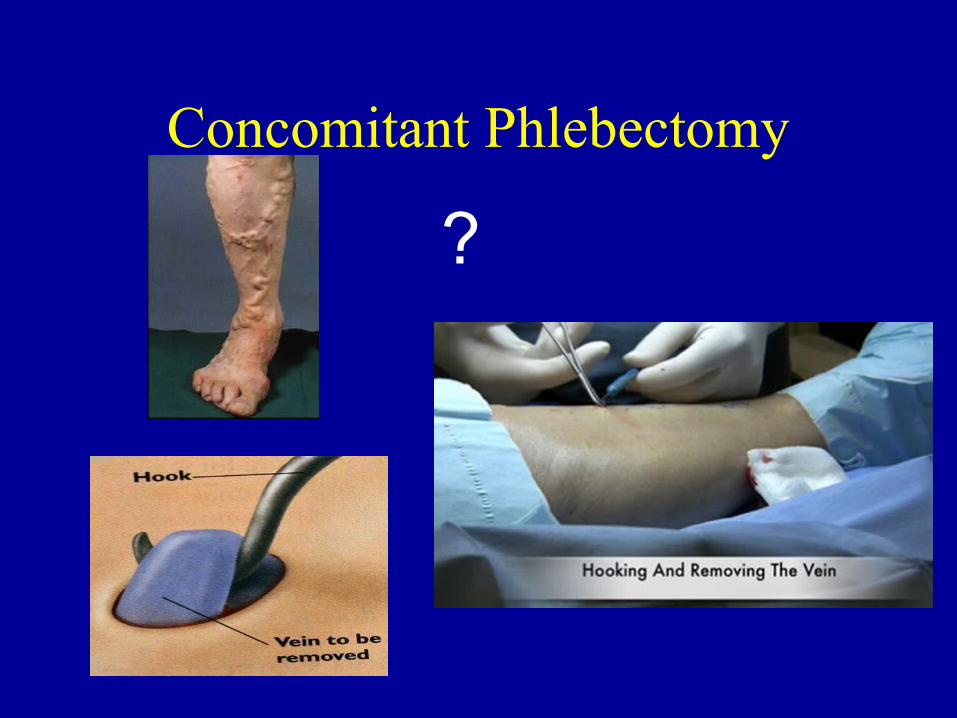
Concomitant Phlebectomy
?
Laser vs Radiofrequency
?
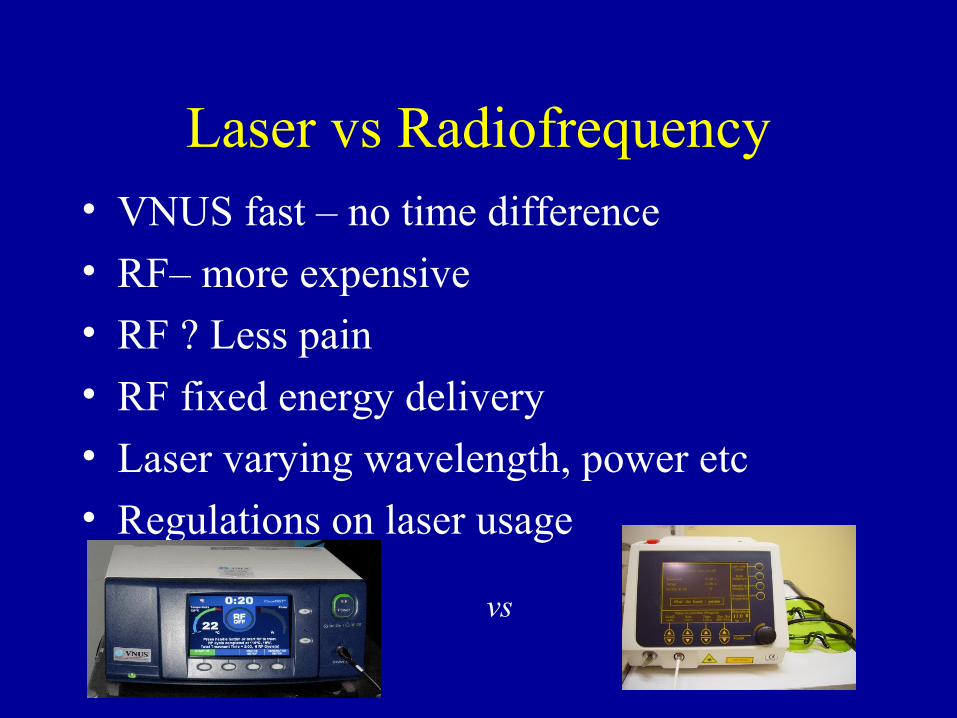
Laser vs Radiofrequency• VNUS fast – no time difference
• RF– more expensive
• RF ? Less pain
• RF fixed energy delivery
• Laser varying wavelength, power etc
• Regulations on laser usage
vs
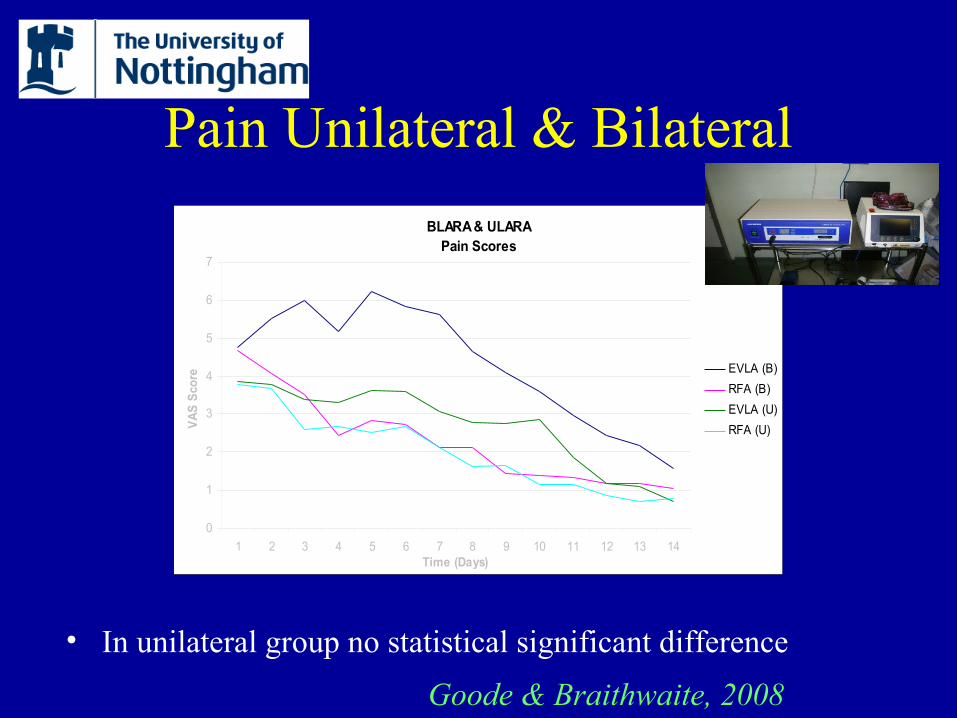
Pain Unilateral & Bilateral
BLARA & ULARA Pain Scores
0
1
2
3
4
5
6
7
1 2 3 4 5 6 7 8 9 10 11 12 13 14Time (Days)
VA
S S
core
EVLA (B)
RFA (B)
EVLA (U)
RFA (U)
• In unilateral group no statistical significant difference
Goode & Braithwaite, 2008
RECOVERY Trial – Conclusions
• 100% Vein occlusion in both RF and laser groups
• Procedure times were similar between RF and laser
• Compared to laser, RF treatment with ClosureFAST produced significantly
– Less pain p < 0.0001
– Less tenderness p = 0.008
– Less bruising p < 0.0001
– Fewer adverse events p = 0.021
VALVV trial early outcomes
• RFA less painful than EVLA
• Patients took significantly more analgesia following EVLA
• Both groups experienced similar improvements in QOL and VCSS at
6 weeks
• No difference in complications
VALVV trial 6 month outcomes
• No difference observed between clinical and QoL outcomes at 6 months between RFA and EVLA
• Poor correlation between duplex findings and functional outcomes
• More treatment failure in the RFA group at 6 months compared to EVLA (ns)
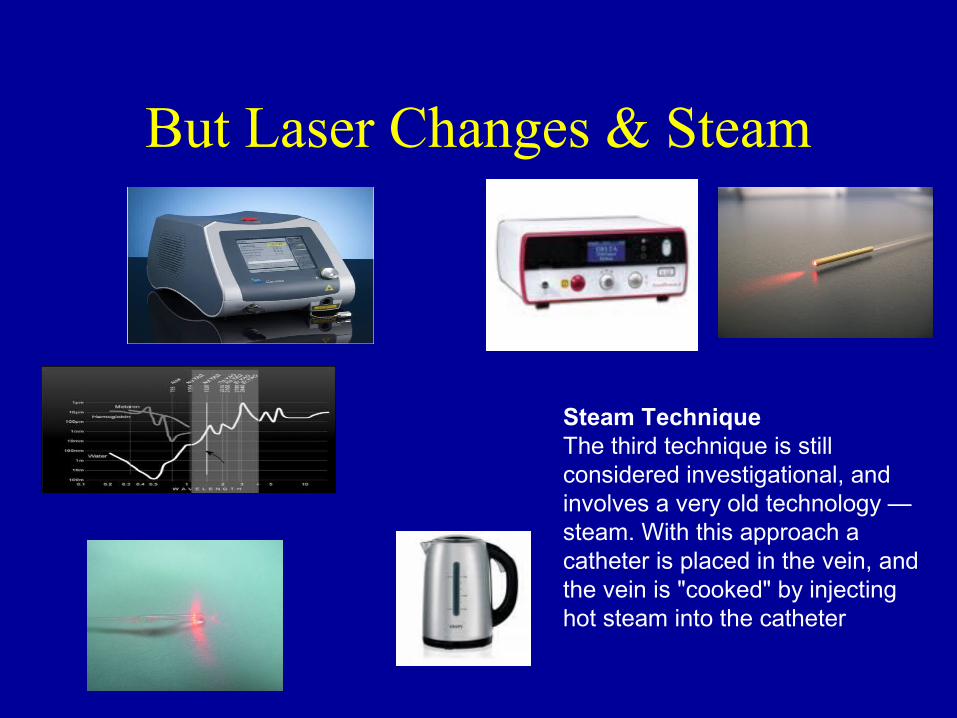
But Laser Changes & Steam
Steam TechniqueThe third technique is still considered investigational, and involves a very old technology — steam. With this approach a catheter is placed in the vein, and the vein is "cooked" by injecting hot steam into the catheter
2010
86% of patients were satisfied or very satisfied with their treatment.
Patients undergoing treatment for primary veins were more likely to be satisfied than those undergoing treatment for recurrent varicose veins (92% vs 75% respectively p=0.027 Fishers exact test)
85% of patients would be prepared to undergo the same treatment again if necessary 2010

Patient preference for local or general anaesthesia during laser ablation
• Single centre study, 290 patients undergoing EVLA of saphenous veins with concomitant avulsion of varicosities
• Following informed consent patients chose either general (GA) or local anaesthesia (LA) with tumescence
• 56% chose LA, 44% chose GA
• Patients undergoing unilateral treatment were more likely to prefer LA than those undergoing bilateral intervention (63% vs 36%, p<0.01)
• 24% of those who chose LA said they would prefer GA if they required a second treatment, mostly due to anxiety and pain. ie 57% prefer GA
• Sridar P et al. International Angiology, August 2009. 28; 4, suppl 1 pp 6.

Sclerotherapy and foam sclerotherapy for varicose veins.
• RCTs limited
• Foam better than liquid• 3% polidocanol foam is no more effective than 1%• optimum ratio of gas to liquid is 4:1
• carbon dioxide foam reduces the systemic complications
• The relative advantages or disadvantages of this treatment in the longer term have yet to be published.
Coleridge Smith 2009
• Filtering• Occluding junction• CO2• Leg elevation before• Leg elevation after• Immobilization after the procedure
2011 BUT – volume / time interval
Darvall et al, 2009
Changes in health-related quality of life after ultrasound-guided foam sclerotherapy for great and small saphenous varicose veins
Medium-term results of ultrasound-guided foam sclerotherapy for small saphenous varicose
Darvall et al, 2010
Recovery after ultrasound-guided foam sclerotherapy compared with conventional surgery for varicose veins
Darvall et al, 2009
Surgery vs UGFS: an RCT
• 29 surgery and 27 by UGFS
• 180 days after treatment, ocllusion in 78% of the surgery group, compared with 90% in the foam sclerotherapy group
• UGFS effective
Figueiredo et al, 2009
Is foam safe?
• 9 case reports (11 patients)
6 CVAs 1 TIA
• 17 series (8888 patients)
1 CVA 1 TIA
Sarvananthan, et al 2011
2011
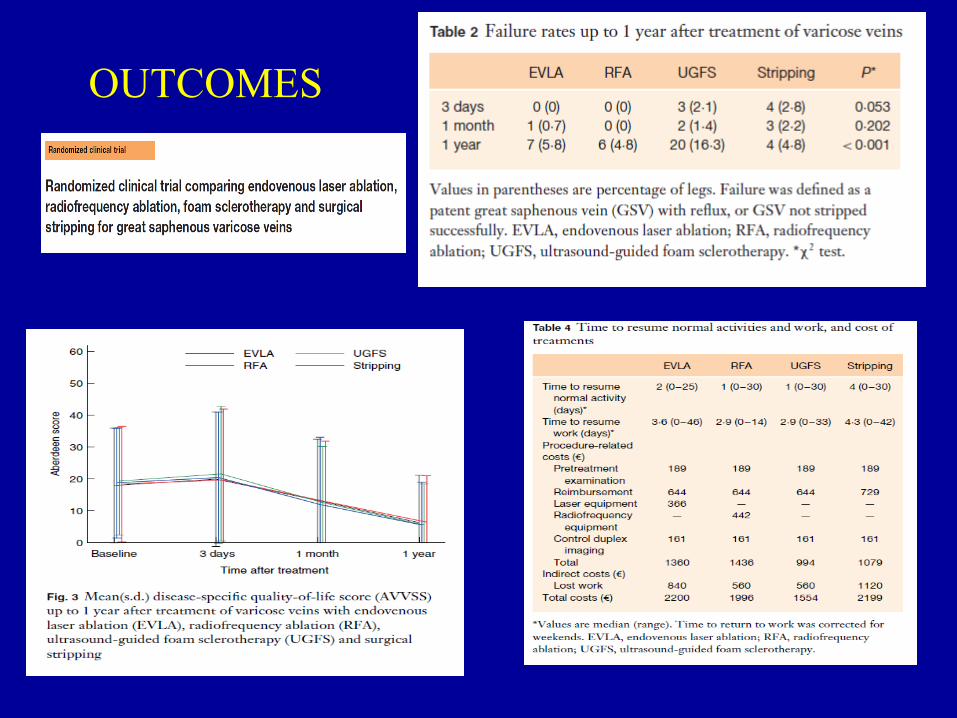
OUTCOMES
Clarivein
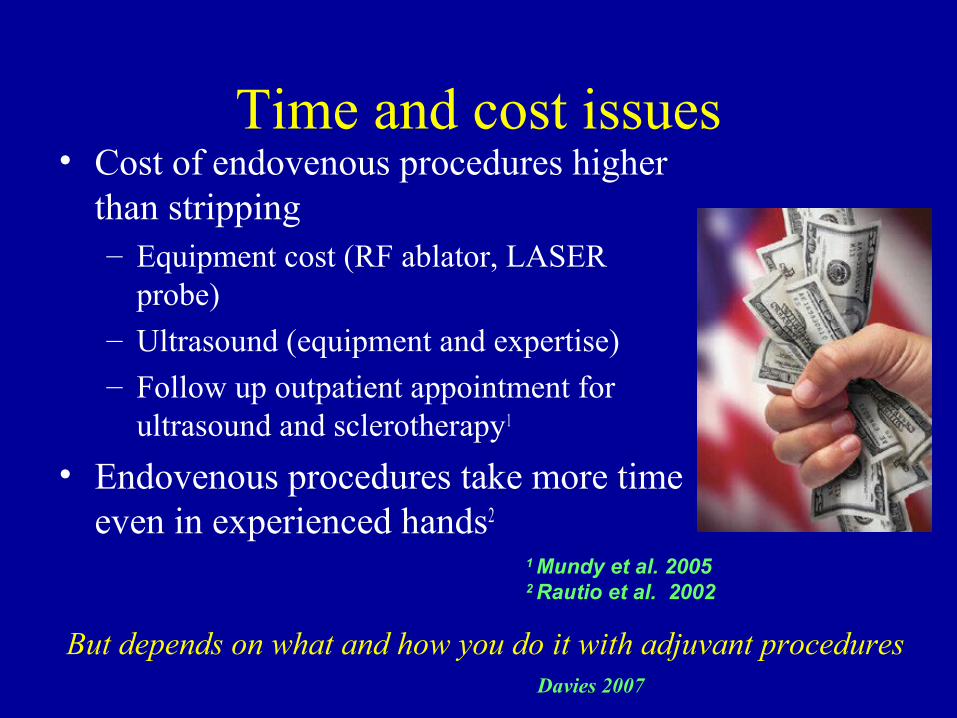
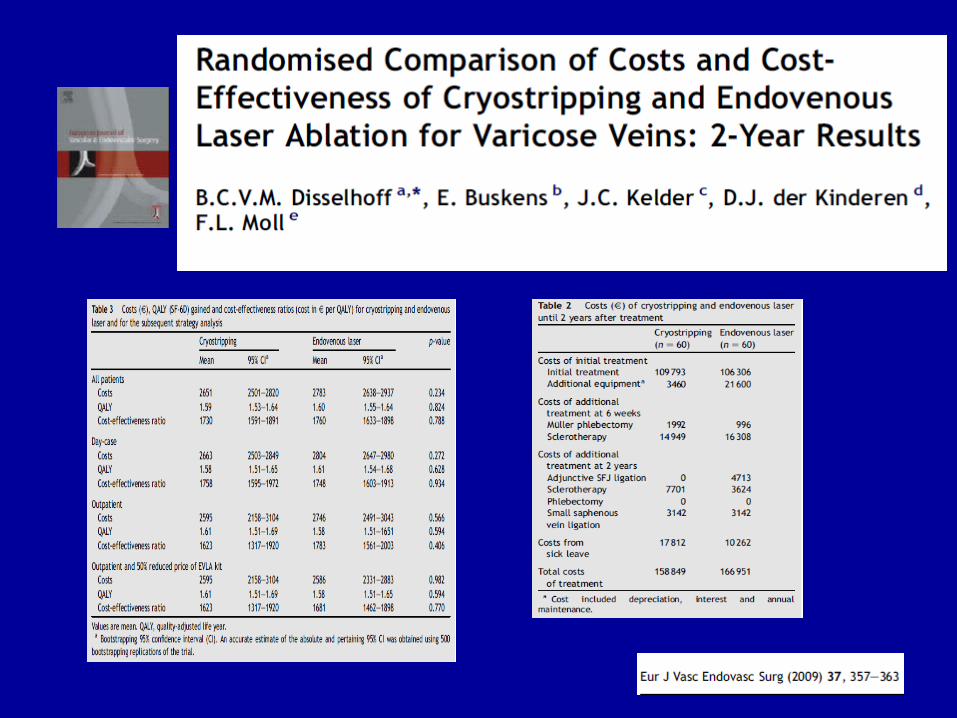
Time and cost issues• Cost of endovenous procedures higher
than stripping– Equipment cost (RF ablator, LASER
probe)– Ultrasound (equipment and expertise)– Follow up outpatient appointment for
ultrasound and sclerotherapy1
• Endovenous procedures take more time even in experienced hands2
1 Mundy et al. 20052 Rautio et al. 2002
But depends on what and how you do it with adjuvant proceduresDavies 2007
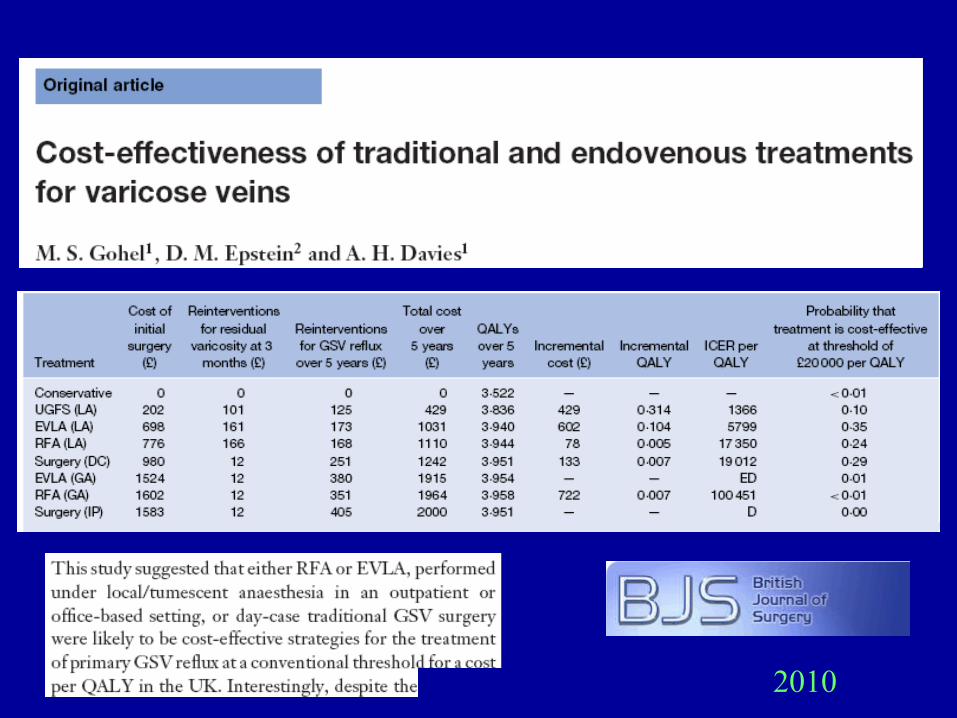
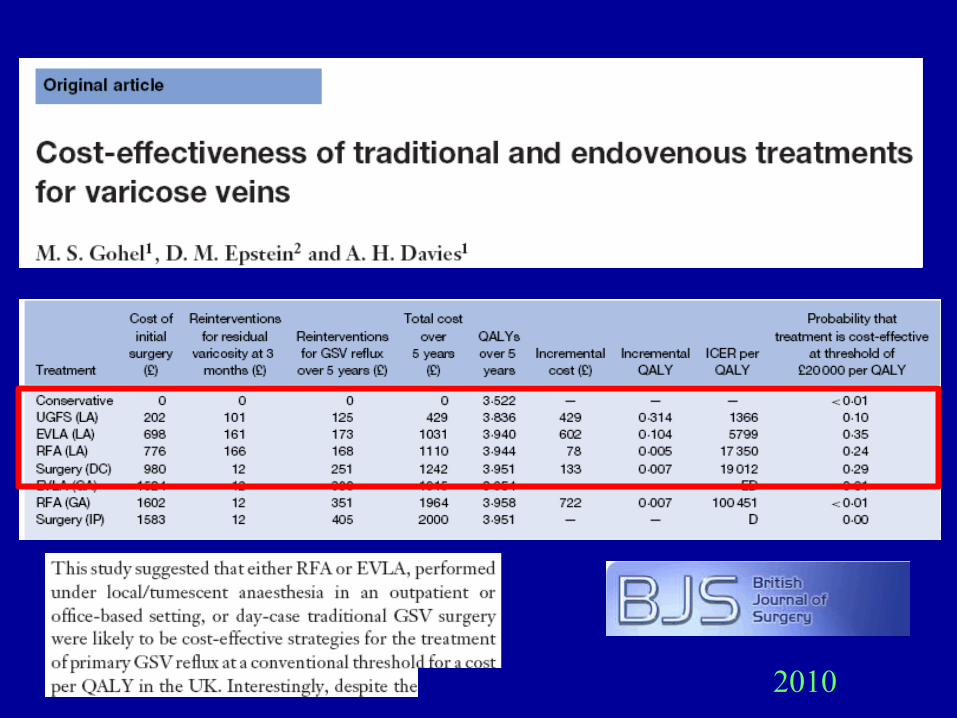
2010
2010
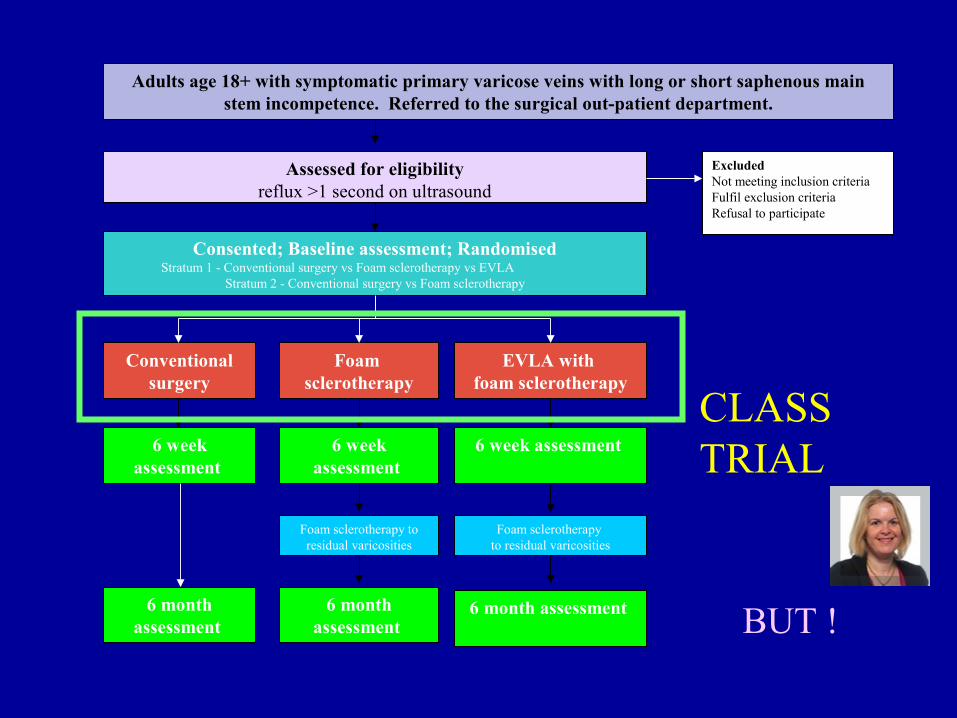
Excluded Not meeting inclusion criteriaFulfil exclusion criteriaRefusal to participate
Assessed for eligibilityreflux >1 second on ultrasound
Consented; Baseline assessment; RandomisedStratum 1 - Conventional surgery vs Foam sclerotherapy vs EVLA
Stratum 2 - Conventional surgery vs Foam sclerotherapy
Foam sclerotherapy
Adults age 18+ with symptomatic primary varicose veins with long or short saphenous main stem incompetence. Referred to the surgical out-patient department.
EVLA with foam sclerotherapy
Conventional surgery
6 week assessment
Foam sclerotherapy to residual varicosities
Foam sclerotherapy to residual varicosities
6 week assessment
6 week assessment
6 month assessment
6 month assessment
6 month assessment
CLASS TRIAL
BUT !
Quality of life
• Major improvement following truncal intervention.Smith et al, 1999,2002
Mackenzie et al,2002
Rasmussen et al 2007,2010
Shepherd et al, 2010

Treatment options
Surgery
Sclerotherapy
Laser
Radiofrequency
http://www.rsm.ac.uk/academ/downloads/venous_referral_guidelines_jan11.pdf
The Care of Patients with Varicose Veins and Associated Chronic Venous Diseases
The Department of Health has asked NICE:
To produce a clinical guideline on
‘the management of varicose veins’
Publication date 2013
Twenty nine RCT’s (32 articles) on radiofrequency ablation(RFA), endovenous laser ablation (EVLA) and chemical ablation (CA) have been identified
Conventional open Surgery (OS) vs RFA (n = 7)
Conventional open Surgery (OS) vs EVLA (n = 10)
Conventional open Surgery (OS) vs CA (n = 6)
EVLA vs. RFA (n = 5)
OS vs. Thermal vs. Chemical ablation (n =1)
Summation Data from M Perrin and Bo Eklof
Summary results on OS versus RFA
- Almost all RCT’s conclude that after radiofrequency ablation there was less postoperative pain, faster recovery and earlier return to work and normal activities, as well as higher patient satisfaction.
- The longest follow-up is 3 years and there is nodifference in terms of clinical result between classical surgery and radiofrequency ablation.
Summary results on OS versus EVLA
- All RCT’s except two used 980 nm bare tipped fibers.Observation time was < 1 year in 7 studies and >1 year in 4 studies. Quality of safety and early efficacy was high with no real difference between the groups.
- After two years no significant difference was found in clinical or DUS recurrence, clinical severity or QOL.
No Difference!!
Surgery
Sclerotherapy
Laser
Radiofrequency
=
Other studies
n=404 80% Primary success with EVLT Myers et al,2006
n=145 31% Recurrent/residual veinSharif et al,2006
n=150 82% vein occlusion with RF Welch et al,2006
n=145 22% re-canalization after RFA plus SFJ ligationSalles-Cunha et al,2006
Systematic Review:- Complications
• Ecchymosis 23-100%
• Paraesthesia 1-36.5%
• Induration 55-100%
• Phlebitis 1.6-12%Mundy et al, 2005
n=1289
Medium-term results of ultrasound-guided foam sclerotherapy for small saphenous varicose veins
UGFS was an effective treatment for SSV, in 92 legs with abolition of reflux in 91% and 93% of visible varicose veins, and improvement in HRQL for at least 12 months.
Darvall et al, 2009
Changes in health-related quality of life after ultrasound-guided foam sclerotherapy for great
and small saphenous varicose veins.
• n= 296 66% C2-3
• Improvement in SF12 and AVVQ
Darvall et al, 2010
Recovery after ultrasound-guided foam sclerotherapy compared with conventional
surgery for varicose veins.
UGFS 332 (84.9 per cent) of 391
Surgery 53 (56 per cent) of 94
UGFS was associated with less pain and analgesia requirement, time off work and quicker return to driving
Darvall et al, 2009
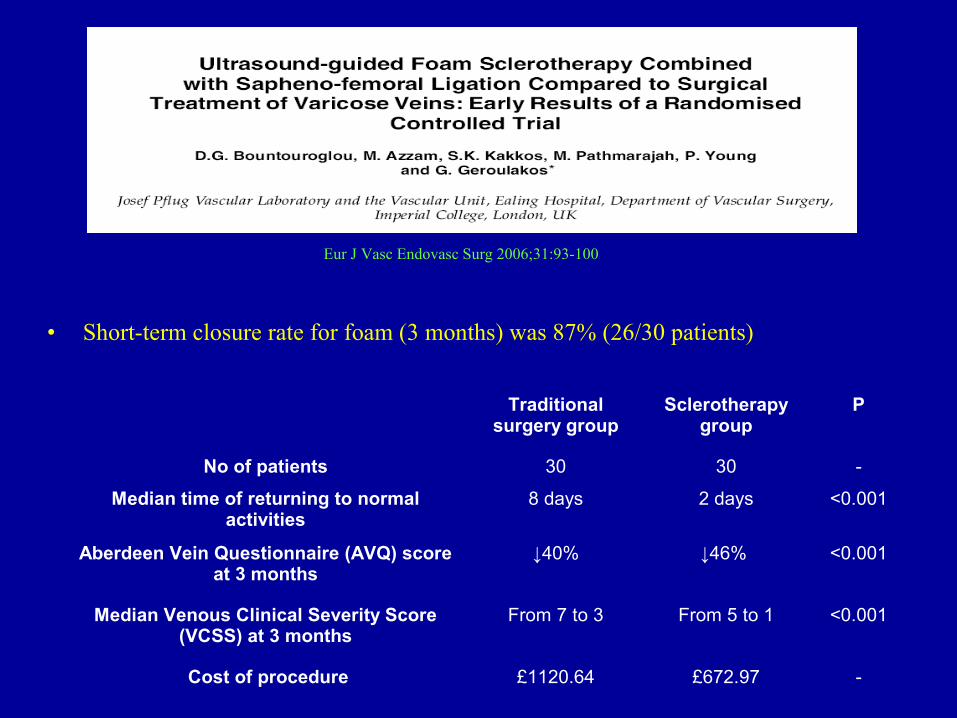
• Short-term closure rate for foam (3 months) was 87% (26/30 patients)
Traditional surgery group
Sclerotherapy group
P
No of patients 30 30 -
Median time of returning to normal activities
8 days 2 days <0.001
Aberdeen Vein Questionnaire (AVQ) score at 3 months
↓40% ↓46% <0.001
Median Venous Clinical Severity Score (VCSS) at 3 months
From 7 to 3 From 5 to 1 <0.001
Cost of procedure £1120.64 £672.97 -
Foam sclerotherapy and crosectomy
Eur J Vasc Endovasc Surg 2006;31:93-100
Conventional open Surgery (OS) versus Endovenous laser ablation EVLA # RCT’s 10, articles 11
Theivacumar NS. Neovascularization and recurrence 2 years after treatment for sapheno-femoral and great saphenous reflux : a comparison of surgery and endovenous laser. Eur J Vasc Endovasc Surg 2009;38:203-207
Christenson JT. Prospective randomized trial comparing endovenous laser ablation and surgery for treatment of primary great saphenous varicose veins with a 2 year follow-up. J Vasc Surg 2010;52:1234-41
Rassmussen LH. Randomized trial comparing endovenous laser ablation with stripping of the great saphenous vein : clinical outcome and recurrence after 2 years. Eur J Vasc Endovasc Surg 2010;39:630-5
Pronk P. Randomised Controlled Trial Comparing Sapheno-Femoral Ligation and Stripping of the Great Saphenous Vein with Endovenous Laser Ablation (980 nm) Using Local Tumescent Anaesthesia: One Year Results. Eur J Vasc Endovasc Surg 2010;40:649-656
Rass K. Comparable Effectiveness of Endovenous Laser Ablation and High Ligation With Stripping of
the Great Saphenous Vein Arch Dermatol online september19,.2011 doi:10.1001/archdermatol.2011.27
Conventional open Surgery (OS) versus
Radiofrequency ablation (RFA) # 7 RCT’s, 9 articles Rautio T. Endovenous obliteration versus conventional stripping operating in the treatment of primary varicose veins : a randomized controlled trial with comparison of the costs. J Vasc Surg 2002;35:958-65
Lurie F. Prospective randomized study of endovenous radiofrequency Obliteration (Closure procedure) vs ligation and stripping in a selected patient population (EVOLVES Study) J Vasc Surg 2003;38:207-14
Lurie F. Prospective randomized study of endovenous radiofrequency obliteration (Closure) versus ligation and vein stripping (EVOLVeS) Two-year follow-up. Eur J Vasc Endovasc Surg 2005;29:67-73
Perala J. Radiofrequency endovenous obliteration vs stripping of the long saphenous vein in themanagement of primary varicose veins:3-year outcome of a randomized study. Ann Vasc Surg2005;19:1-4
Hinchliffe RJ. A prospective randomized controlled trial of VNUS Closure versus surgery for thetreatment of recurrent long saphenous varicose veins. Eur J Vasc Endovasc Surg 2006;31:212-8
Kianifard B. Radiofrequency ablation (VNUS Closure) does not cause neo-vascularisation at the groin at one year : results of a case controlled study.Surgeon 2006;4:71-74
Stötter L. Comparative outcomes of radiofrequency endoluminal ablation, invagination stripping and cryostripping in the treatment of great saphenous vein. Phlebology 2006;21:60-4
Subramonia S. Radiofrequency ablation versus conventional surgery for varicose veins-a comparison of treatment costs in a randomized trials. Eur J Vasc Endovasc Surg 2009;39:104-11
Elkaffas KH. Great saphenous vein radiofrequency ablation versus standard stripping in the management of primary varicose veins- a randomized clinical trial. Angiology 2010;62:49-54
Conventional open Surgery (OS) versus Endovenous laser ablation EVLA # RCT’s 10, articles 11
de Medeiros CAF. Comparison of endovenous treatment with an 810 nm laser versus conventional stripping of the great saphenous vein in patients with primary varicose veins. Dermatol Surg.2005;31:1685-94
Vuylstecke M. Endovenous laser obliteration for the treatment of primary varicose veins. Phlebology 2006;21:80-87
Ying L. A random, comparative study on endovenous laser therapy and saphenous veins stripping for the treatment of great saphenous vein incompetence. Zhonghua-Yi-Xue-Za-Zhi 2007;87(43):3043-3046.
Rassmussen LH. Randomized trial comparing endovenous laser ablation of the great saphenous vein with ligation and stripping in patients with varicose veins : short-term results J Vasc Surg 2007;46:30815
Darwood RJ. Randomized Clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous veins. Br J Sug 2008;95:294-301
Kalteis M. High ligation combined with stripping and endovenous laser ablation of the great saphenous vein: Early results of a randomized controlled study. J Vasc Surg 2008;47:822-9
Conventional Open Surgery (OS) versus Chemical Ablation (CA) # 6
Bountouroglou DG. Ultrasound-guided foam sclerotherapy combined with sapheno-femoral ligation compared to surgical treatment of varicose veins: early results of a randomised controlled trial.Eur J Vasc Endovasc Surg. 2006;31:93-100
Wright D. Varisolve® polidocanol microfoam compared with surgery or sclerotherapy in the management of varicose veins in the presence of trunk vein incompetence: European randomized controlled trial. Phlebology 2006;21:180-90.
Abela R. Reverse foam sclerotherapy of the great saphenous vein with sapheno-femoral ligation compared to standardand invagination stripping: a prospective clinical series. Eur J Vasc Endovasc Surg. 2008;36:485-90
Figueiredo M. Results of surgical treatment compared with ultrasound guided foam sclerotherapy inpatients with varicose veins: a prospective randomised study. Eur J Vasc Endovasc Surg 2009;38:758-63
Liu X. Ultrasound-guided foam sclerotherayof the great saphenous vein with-saphenofemoral junction ligation compared to standard stripping: a prospective clinical study. InternationalAngiology 2011;30:321
Kalodiki E. Long Term Results of a Randomized Controlled Trial on Ultrasound Guided Foam Sclerotherapy Combined with sapheno-femoral Ligation versus standard Surgery for Varicose Veins. JVS 2011;accepted for publication
EVLA versus RFA # 5
Almeida JI. Radiofrequency Endovenous Closure FAST versus Laser Ablation for the Treatment of
Great Saphenous Reflux : A Multicenter, Single-blinded, Randomized Study (RECOVERY Study).
J Vasc Interv Radiol 2009;20:752-759
Shepherd AC. Randomized clinical trial of VNUS Closure FAST radiofrequency ablation versus laser
for varicose veins. Br J Surg 2010;97;810-8
Gale SS. A randomized, controlled trial of endovenous thermal ablation using the 810-nm wavelength
laser and the ClosurePLUS radiofrequency ablation methods for superficial venous insufficiency of
the great saphenous vein. J Vasc Surg 2010;52:645-50
Goode SD. Laser and Radiofrequency ablation Sudy : a randomized Study comparing
Radiofrequency Ablation and Endovenous Laser Ablation ( 810 nm). Eur J Vasc Endovasc Surg
2010;40:246-53
Nordon IM. EVVERT comparing laser and radiofrequency: An update on endovenous treatment
options. In Greenhalgh R, editor. BIBA publishing, UK. 2011:381-388





























