Embed Size (px)
Citation preview

Management of Endoleaks after EVAR
Michel Makaroun MDCo-Director UPMC Heart and Vascular Institute
Professor and Chief, Division of Vascular Surgery University of Pittsburgh School of Medicine

Disclosures
Consultant:
WL Gore, Cordis, Medtronic
Research Grants:
WL Gore, Cook, CordisMedtronic, Boston Scientific, Abbott
Bolton, Lombard, Trivascular

Type IAttachment leak
Type IIBranch flow
Type IIIDefect in graft ormodular disconnection
Type IVFabric porosity
The Different Types of Endoleaks

There is almost uniform consensus about
Type I and III Endoleaks
They are serious and associated with a significant risk of rupture!
Should be treated whenever feasible:
either with
Endovascular Salvage or Open Conversion

6 Ruptures All from Type I or Type III

TYPE I + III
J Vasc Surg 2002;35:461-73

Type I Endoleaks

World Review of Ruptures after EVAR55% (129/235) of All Ruptures
are due to Type I endoleaks 38 of the ruptures in the first 30 days

Intrasac Pressure Measurements
Before Exclusion
Mean Pressure: 75 mmHg
After EVAR with Type I
Mean Pressure: 111 mmHgBefore Implantation Type I endoleak

Earliest EVAR Tube Experience
Parodi first 50 patients (1995)
5 Type I endoleaks (10%) : 3 proximal 2 distal
4 died by 8 months, one from Rupture @2 months
20% Mortality from Rupture 1st year !

Earliest EVAR Bifurcated Experience
Chuter first 41 patients (1996)
9 Type I endoleaks (22%)
2 Type I died within 3 days from rupture
22% Mortality from Rupture!

Early Experience proved Type I Endoleaks to be serious. ALL Type I Endoleaks have since been treated when feasible
at original procedure or when discovered!!
1. Incidence has decreased significantly2. Very few type I endoleaks are monitored conservatively
Small endoleaks missed at completion angiography Endoleaks difficult to manage by endovascular means
in sick patients with limited life expectancy

Endovascular Rx of Type I Endoleaks Extensions with Stent Grafts
High pressure balloons Increase Radial Force by Palmaz Stents
Endostapling
Extension Simple and effective but can be limited by
1. Renals close to the proximal end2. Essential internal iliac artery
In those situationsCoiling of the track may work
Or Coverage of the Renals with chimneys
Rarely Open Conversion is required
Higher Mortality and morbidity

Procedural Type I Endoleak Treated by Ballooning
Pre deployment Type I Endoleak Ballooning No more endoleak

Procedural Type I Endoleak Treated by Extension
Pre deployment Type I Endoleak Extension No more endoleak

Procedural Type I Endoleak Treated with Palmaz
Type I Endoleak Palmaz Stent No Endoleak

Procedural Type I Endoleak Treated by Endostaples
Courtesy of Jim Joye DO

Late Type I Endoleaks
Can be due to Migration
Aneurysmal degeneration of neck
Enlargement of Iliac arteries
Angulation

Treated with New Endograft inside first one
Endovascular Rx of Proximal Type I Endoleakafter Proximal Migration

Endovascular Rx of Distal Type I from Iliac Degeneration
7 years post Ancure:
Distal Type I Endoleak
Right Limb
Endoleak
Excluder 14.5 x 7cm Extension
No moreEndoleaks
Treated by Extension

Endovascular Rx of Proximal Type I Endoleakafter Proximal Migration
3 years post AneuRx:
Migration and Proximal Type I
No More Endoleaks
Treated by Extension and Palmaz Stent

Endovascular Rx of Proximal Type I Endoleakafter Proximal Migration
Treated by Extension and Left renal stent
Type I
Old Type II coiled
NO Type I
No RoomTo extend

Endovascular Rx of Proximal Type I Endoleakwith renal coverage and chimneys
Aneurysm neck wall
Poor deployment and Type I Treated with suprarenal Extension and 2 chimneys
FailedExtension
Palmaz
Staples

Coiling of Distal Type I
6 months post Tube Ancure
Distal Type I
Graft
Endoleak
Coils1 Month Post Coiling 5.8 cm

Coiling of Distal Type I1 year post coiling 4.6 cm 2 years post coiling 3.4 cm
5 year post coiling 2.8 cm4 year post coiling 2.8 cm

Type I
Open Conversion
Does not always require complete ExplantationOperative Mortality: 5-10%
High Morbididty
Conversion To Open Repair

Type III Endoleaks

Fabric Tear and Type III Endoleak
Fabric Tear from Wall stent in Ancure Rx with Excluder Limb6 years after Implantation

Limb Disconnection and Type III endoleak
Rt Limb Disconnection in a Lifepath Rx with Excluder Limb 6 years after Implantation

How about Type II Endoleaks?
The opinions here are much more divided !

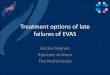
The Majority of Endoleaks are Type II
0
20
40
60
80
100
None Type I Type II Type III Type IV TypeIndet
% s
ub
ject
s ev
alu
ated
12 Mos
24 Mos
36 Mos
48 Mos
60 Mos
Excluder Regulatory Trial: 5 year Chart

12 MosType II Total % Type II Total % Type II Total %
Talent 10 159 6.2%* 1 118 0.80% 0 113 0.00%Lifepath 4 57 7.00%Excluder 13 86 15.10% 8 55 14.50% 5 36 13.90%Zenith 19 124 15.30% 3 43 7.00%AneuRx 34 327 10.40% 29 210 13.80% 13 92 14.10%Ancure 27 295 9.20% 15 213 7.00% 2 121 1.60%Total 107 1048 10.20% 56 639 8.80% 20 362 5.50%
24 Mos 36 Mos
Occurs with all Grafts in 14% (10-20%) of patients Prevalence decreases to 5-10% between 1-3 years
Sheehan MK, Makaroun MS et al J Vasc Surg 2006;43:657-61
Incidence Similar for ALL Endografts

Diagnosis of Type II Endoleaks
CT and Duplex agree in many cases on Endoleak.
Source of Endoleak ???

Diagnosis of Type II Endoleaks

Source can be difficult to determine Some endoleaks are very complex
90 x 91 mm AAA
MB Nov 2003
MB Dec 2003
Type I Endoleak ??
Or is it IMA Type II ??
CT Diagnosis of Type II Endoleaks

SMA Injection
Large Patent IMA
Type II IMA Endoleak

MB February 2004
5 Fr Glide cath
RenegadeMicrocath
Transcend .014 wire

1. WHEN TO TREAT?
The answer has changed steadily over the years gradually favoring a more conservative approach
The current recommendation: Rx confirmed Type II Endoleaks ONLY when
associated with AAA sac Enlargement !
Also eliminates many unnecessary re-interventions

Evidence suggests that Type II endoleaks have a relatively Benign Natural History !
0
10
20
30
40
50
60
70
80
90
OP D/C 3m 6m 12m 24m 36m
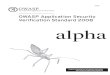
Excluded
Endoleaks
No Interventions until 6 Months
2/3 resolve spontaneouslyby 6 months
Makaroun et al Eur J Vasc Endovasc Surg 1999;18:185-90
UPMC 1999

Spontaneous resolution can occur Late
Year 1. May 2003
Type II Endoleak
Year 2. May 2004
Type II Endoleak
Year 3. May 2005
No Endoleak
Late Spontaneous Resolution (3 Years)

PersistentType II Endoleak
Lumbars
September 2006
+ AAA can shrink despite Type II Endoleak
September 200553 x 55 mm
September 200643 x 45 mm
10 mm Decrease

486 Patients with 90 Type II Endoleaks (18.5%) 61% sealed spontaneously in 6 months Only 6% experienced enlargement > 5mm
J Vasc Surg 2004;39:306-13

965 Patients with 154 Type II Endoleaks (16%) 75% seal spontaneously in 5 years (KM analysis) Only 8.4% experienced enlargement > 5mm
J Vasc Surg 2006;44:453-59

So Should we Ignore Type II Endoleaks?
Probably not!

Review of 270 Aneurysm Ruptures after EVAR Endoleaks the cause of rupture in 160 patients
Type I or III in 114 Patients Type II in 23 Patients
Eur J Vasc Endovasc Surg 2009;37:15-22

Type II Endoleaks Usually run a benign course
But can rarely result in rupture
Should ONLY be treated when associated with AAA enlargement!
Caveat: Increasing Sac Size is an unproven surrogate for the potential of future rupture but quite likely

2. How to do it?
There is no consensus as to the best way to treat Type II Endoleaks, as they can be very different
from each other and can be very complex to treat.

Approaches to Type II Endoleaks
Observation
Laparoscopic clipping of branches
Open Surgical Conversion
Partial or Complete
Endovascular Approaches !!

Endovascular Rx of Type II Endoleaks
Multiple Branch Vessels involved IMA Multiple sets of Lumbars Other branches Large Nidus
Diagnosis is usually suspected by Duplex or CT but has to be confirmed at angiography!
Principle of Endo RX
Obliterate the feeding vessels and if possible the nidus
Three Different Approaches Trans-Arterial catheterization:
More technically demanding but potentially more effective
Translumbar puncture Transcaval direct access
Rx Nidus. Difficult to get vessels
Occluding Agents Glue Onyx Thrombin Coils

Onyx and Glue are liquid agents that help fill nidus but very expensive and complicate FU
ONYX
18 m later size increased from 9 to 14 cmand presented with a leaking AAA

Onyx and Glue are liquid agents that help fill nidus but very expensive and complicate FU
Type III Disconnection
Type IBEndoleak
UnrecognizedType IIEndoleak
Poorly coiled

2. How I do itTechnical Notes
Trans-arterial Coaxial System Micro-catheters Coils
Can deliver very long coils if needed (Interlocks) Use Saline flush for short ones instead of coil pushers Make sure it is occluded
Proximal lumbars (L1-L3) near impossible to reach

Int Iliac coils
6 Fr Sheath in Internal Iliac5 Fr angled Catheter
Microcatheter

Lumbar EndoleakCoils at origin of Lumbar

Lumbar Endoleak Coils in LumbarOne month later
Treatment of Type II Endoleaks

Coiling of Type II IMA Endoleak
IMA endoleak treated by coiling

Type II Endoleaks Can be Complex: Case AH
June 07: Lumbar Type II endoleak
Microcatheter Access
Lumbars CoiledNo endoleak

AH Oct 07: Endoleak still present/ AAA larger
Oct 07
PersistentEndoleak
MoreFeeders
RenegadeMicroCatheter Access to AAA Sac
Complex Endoleak
Nidus and Branches Coiled
Some endoleaks are complex and
require multiple interventions

Trans-Arterial Access Not Always AvailableOW March 2012
PersistentEndoleak
67x70 mm
Type II EndoleakNo Transarterial Access Right
No Transarterial Access left

Trans-Lumbar Approach Reasonable AlternativeOW March 2012
Patient prone Shiba needle/ .018 wire Puncture endoleak Exchange for Stiff wire 6 Fr 30 cm sheath Catheter Eliminate Nidus

Trans-Lumbar Approach Reasonable AlternativeOW March 2012
6 Fr Sheath5 Fr angled Catheter
Microcatheter

Trans-Caval Approach Useful in Some Patients
Patient Supine Trans-Caval approach
with a Rosch-Uchida catheter
Angiogram Direct embolization of
Nidus and branches Removal of catheter
and completion cavogram

3. Does it Work?
A qualified YES! Of course conversions (both partial and complete) do
work but associated morbidity is high
Endovascular interventions are tedious and will work in most, if operator is experienced and persistent

3. Does it Work?Unfortunately, Very little long term data exists!
It is easy to make claims of effectiveness since:
a) Many interventions were carried too early when most endoleaks would have resolved spontaneously
b) Many techniques obstruct future imagingc) No clear endpoint of effectiveness: Size of AAA

UPMC experience 1995- 2003 All Trans-Arterial coiling
Endoleaks only treated if persistent > 6 months Success: No leaks and stable or shrinking AAA sac
FU: Mean 18 months
J Vasc Surg 2004;40:430-4

Results of Coiling
28 patients Follow-up 1-60mos Clinical Success (82%)
15/19 (79%) Type II 8/9 (89%) Type I
Procedural Morbidity 0% Procedural Mortality 0%

Type II Endoleaks: Results of Coiling
19 patients 21 attempts
2 patients required more than one intervention
Can be very complex 15 successful
1 IMA 7 pure lumbar 7 combined

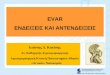
3 Lumbar CoilsTwo years laterTwo interventions laterCoils Not Occlusive
MultipleCoils addedTill Occlusion

Several sources coexist in some complex cases
Type IILumbar
1 Year Year 2
Type IDistal
Year 3
Type IIIMA

Endovascular techniques can be used safely and
effectively to Treat Endoleaks after EVAR Type I and Type III should almost always be treated
when discovered Treatment of Type II should be reserved to patients
with sac enlargement Open Conversions may be necessary but carry a
higher morbidity and mortality
Summary