Embed Size (px)
Citation preview

XV. ULUSAL VASKULERCERRAHI KONGRESI
Mr. Paul Bachoo
Consultant Vascular Surgeon
Aberdeen
Scotland


WHY REPOSITIONABLE ?


Proximal aortic neck diameter> 28mm
Length <15mm
11-15mm
<10mm
• Angle >60
• Reverse taper / bulging neck
• Thrombus lining
• Calcification
Neck 10mm
Angle 94
Aberdeen case

Stent graft
attributes
ACCURATE
DEPLOYMENT

Aberdeen: 3mensio Vascular Tera-recon


Trans renal Infra renal
Top downBottom up
Repositionable

Device Manufacturer Stent Graft Delivery Special feature
Talent Medtronic Nitinol Woven Polyester
Integratedsheath
Pararenal bare stent
Zenith Flex Cook Stainless steel
WovenPolyester
Integrated sheath
Uncovered stent, suprarenal fixation
Powerlink Endologix Cobalt chromium
ePTFE Integrated sheath
Sits on bifurcation

Device Manufacturer Stent Graft Delivery Special feature
Anaconda Vascutek Nitinol WovenPolyester
Integrated sheath
RepositionableMagnetic guidance
Aorfix Lombard Nitinol WovenPolyester
Integrated sheath
Crumple zone
Endurant Medtronic Nitinol Woven Polester
Integrated sheath
Pararenal bare stent,suprarenal hooks


Endoframes Endobags

Infrarenal
hooks
NitinolePTFE
RepositionableTop down
Infra renal



Deploy the trunk to the contra gate. This allows distal
perfusion and prevents wind sock effect

Repositioning is not mandatory

Point of no return

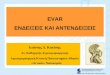
Step 3: deploying the ispi legDeploying the ipsi-lateral leg

However if repositioning is required

Constraining the trunk will disengage the anchoring
pins and allow re-positioning of the device

After repositioning




Deploy Trunk
Attempt Cannulation
Remove
Constraining
Mechanism
Deploy ipsi
Balloon Trunk-ipsi
Reposition
Reposition
Happy
With
Position?
Success?
NoYes
Yes
No
Deploy Contra

Confidence
Take on challenging aortic neck anatomy Angulated long Angulated short Straight short
Train future endovascular surgeons Introduce surgeons experienced in open AAA surgeons to EVAR Allow experienced endovascular surgeons to take on challenging
anatomy

Short straight neck
Courtesy of Professor Eric Vorhoeven



C3 ADDRESSES THE INABILITY OF BEING ABLE TO RELIABLY PREDICT THE EXACT LANDING SITE OF A GRAFT WITHIN A CURVED SEGMENT




Site
Number Site Name
Procedure Date
Range
C3 Deployment
System
203 Klinikum Nürnberg Süd 08/10 - 10/11 40(24.2%)
209 University of Cologne University Clinics 09/10 - 09/11 17(10.3%)
215 Klinikum der Universität Regensburg 08/10 - 08/11 12(7.3%)
218 University of Heidelberg 03/11 – 8/11 8(4.8%)
263 Hospital Clinic I Provincial de Barcelona 09/10 – 6/11 5(3.0%)
264 Orebro University Hopsital 9/10 – 6/11 16(9.5%)
278 Aberdeen Royal Infirmary 9/10 – 10/11 32(19.0%)
279 Cambridge University Hospitals NHS Trust 09/10 - 09/11 13(7.9%)
280 Royal Liverpool University Hospital 09/10 – 10/11 16(9.7%)
283 Weißeritztal Kliniken GmbH 08/10 - 05/11 9(9.5%)
Total Subjects Enrolled 08/10 - 10/11 168

C3 Device
N (C3) / N (ABD) =168(%)
%Male 85 / 87
Age (yrs)
Mean (Std Dev) 73.7 / 74 (7.7)
Median 75.0
Range (51.0-90.0)
Patient demographics & surgical risk factors
ASA Classification NYHA Classification
Number Responding 162 Number Responding 161
I 3 / (1.9) I 28(18.0)
II 52(32.1 / 10) II 89(55.3)
III 100(61.7 / 70) III 29(18.0)
IV 7(4.3 / 10) IV 0(0.0)
V 0(0.0) No Cardiac Disease 14(8.7)

N=161(%)
Aortic Pathology
Abdominal aortic aneurysm 157(97.5 / 100)
Common iliac aneurysm 3(1.9)
Abdominal aortic aneurysm rupture 1(0.6)
Reason for Treatment
Primary Procedure for Endovascular Treatment 155(96.3 / 100)
Reintervention of an Open Surgical Procedure 3(1.9)
Reintervention of a Prior Endovascular Procedure 2(1.2)

Aneurysm Diameter (mm)
n 155
Mean (Std Dev) 58.4(60)
Median 56.0
Range (35.0,95.0)
Proximal Neck Length (cm)
n 154
Mean (Std Dev) 2.9 (2.1)
Median 2.5
Range (0.3,21.0)
Infrarenal Neck Angle
n 147
Mean (Std Dev) 27.7(24.4)
Median 22.0
Range (0.0,100.0)
Case Planning
Information
Neck Length < 1.5 cm 13(8.1%)
Neck Angulation ≥ 60 15(9.3%)
Significant Calcification at
Landing Zones
28(17.4%)
Significant Thrombus at
Landing Zones
18(11.2%)

Anesthesia Method n (%)
General 149 (92.5 / 100)
Regional 11(6.8)
Local 0
Procedure Survival 161(100 / 100)
Procedure Time (skin-to-skin)
Mean (Std Dev) 126.7(65.4 / 70)
Median 110.0
Range (60.0,477.0)
Hospital Stay (Days)
Mean (Std Dev) 6.6(8.1 / 3)
Median 5.0
Range (1.0,93.0)

Number of Enrolled Subjects n=168(%)
Number of Cases Requiring Trunk Repositioning 91/8(57)
Reasons for Repositioning
Positioning Closer to Renal Arteries 67 / 7(42)
Contralateral Gate Positioning 27(17)
Other 16(10)

Number of cases requiring repositioning n=95
Number of Repositions per Case
1 61 (7)
2 24(1)
3 5
4 1
Missing 4

Number of Enrolled Subjects 168 (%)
95% CI1
Device Deployed Where Planned 150(93 / 100) (88.2%,96.1%)
Deployed ≥5mm from intended location 4(2.5%) (1.0%,6.2%)

Number of Enrolled Subjects n=168 (%)
Subjects with Aortic Extender(s) Implanted 8 / 2 (5.0)
Subjects with unplanned Aortic Extender(s) 7 (4.3)
Reasons for Unplanned Extender Use
Increase Seal 1 (0.6)
Extend Landing Zone 1 (0.6)
Type I Endoleak 5 (3.1)

Number of Enrolled Subjects n=168 (%)
Any In-Hospital Serious Event 4 / 0 (2.4)
Iliac artery occlusion 2 (1.2)
Device Dislocation 1 (0.6)
Renal haemorrhage 1 (0.6)
Surgical mortality = 0
30 day mortality = 0
Death reported at day 35 due to renal sepsis from dialysis
Death reported at day 173 due to subdural hematoma

Why repositionable ?

Controlled delivery Controlled and precise adjustments in a vertical plane Controlled orientation of contra-lateral limb in a horizontal
plane Controlled proximal landing at preferred site avoiding
calcium plaques / thrombus/preserving accessory renals Controlled proximal landing within a angled neck Controlled and safe training Controlled constraint and disengagement of hooks Controlled use of aortic cuffs / expenses

If not the first time certainly by the third repositioning you will achieve your intended proximal landing site









![Best power point evar! [autosaved]](https://img.pdfslide.net/doc/110x75/548bdd07b479592b788b460b/best-power-point-evar-autosaved.jpg)