Embed Size (px)
Citation preview

The Best Medical Treatment of Venous Insufficiency in 2013
Dr. Fatih İslamoğluDepartment of Cardiovascular Surgery, Department of Cardiovascular Surgery,
Ege University Medical Ege University Medical FacultyFaculty,, Izmir, TurkeyIzmir, Turkey

Epidemiology of Chronic Venous Disorders
Age 35-40 yo - M % 7-35 - F % 20-60Age > 60 yo; - M % 15-55 - F % 40-78
Framingham Study
Management of chronic venous disorders of lowew limps: Guidelines according to scientific evidence Nicolaides et. al. İnt.Ang.Vol:27 2008

Etiological and Anatomical Aspects of Chronic Venous Disorders
• Primary etiology; 77.4 %• DVT prevalance ; 25 %
• Superficial system disease; 88.7 %• Reflux ; 97.5 %
• Reflux combined with obstruction ; 11 %

Socioeconomic Aspects
• Estimations of the overall annual costs of CVD vary
from 600 to 900 million € (US$720 million-1 billion) in Western European countries
• 2.5 billion € (US$3 billion) in the USA.
• 1-3 % of total health care budget .• In France, 41% of total expenditure for CVD is for
drugs.
1-McGuckin M. et al. Validation of venous leg ulcer guidelines in the United States and United Kingdom AmJ Surg 2002; 183 2-Levy E. et al.(Management of venous leg ulcer by French physicians, diversity and related costs. A prospective medicoeconomic observational study), j Mal Vasc 1994;19

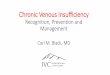
ManagementStory
Clinical examination
Duplex scanning
DVT Venous reflux Normal
Treatment Sclerotherapy
Operation Medical Treatment
Ligation Stripping, Ablations Sclerotherapy

Management Options According to CEAP
C A: S, D, P P: R, O, O+R Management
C0-2 S S R Medical TreatmentSclerotharpy
Surgery
Mild C3 SD O Medical Treatment
Severe C3 SD (above inguinal level)
O Medical TreatmentAngioplasty-stent
C 4-6D (above inguinal level)
O Medical TreatmentAngioplasty-stent
C 6 active or
repeating venous ulcer
D R+O Medical TreatmentCerrahi
Management of chronic venous disorders of lowew limps: Guidelines according to scientific evidence
Nicolaides et. al. İnt.Ang.Vol:27 2008

MEDICAL THERAPEUTIC METHODS
• Venoactive drugs
• Compression therapy
• Adaptation of lifestyle

The care of patients with varicose veins and associated chronic venous diseases: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum
Gloviczki P, Comerota AJ, Dalsing MC, Eklof BG, Gillespie DL, Gloviczki ML, Lohr JM, McLafferty RB, Meissner MH, Murad MH, Padberg FT, Pappas PJ, Passman MA, Raffetto JD, Vasquez MA, Wakefield TW; Society for Vascular Surgery; American Venous Forum.
J Vasc Surg. 2011 May;53(5 Suppl):2S-48S. doi: 10.1016/j.jvs.2011.01.079.
Guidelines for the management of varicose veins.Gloviczki P, Gloviczki ML. Phelobology 2012 Mar;27 Suppl 1:2-9. doi:
10.1258/phleb.2012.012S28.

Guideline No. 8. Medical treatment We suggest venoactive drugs (diosmin, hesperidin, rutosides, sulodexide, micronized purified flavonoid fraction, or horse chestnut seed extract [aescin]) for patients with pain and swelling due to chronic venous disease, in countries where these drugs are available.. We suggest using pentoxifylline or micronized purified flavonoid fraction, if available, in combination with compression, to accelerate healing of venous ulcers..
Guideline No. 9. Compression treatment
We suggest compression therapy using moderate pressure (20 to 30 mm Hg) for patients with symptomatic varicose veinsWe recommend against compression therapy as the primary treatment of symptomatic varicose veins in patients who are candidates for saphenous vein ablationWe recommend compression as the primary therapeutic modality for healingvenous ulcers. . We recommend compression as an adjuvant treatment to superficial vein ablation for the prevention of ulcer recurrence.
2 B8.1
8.22 B
9.12 C
9.2 1 B
9.3
9.4
1
1 A
B
Grade ofRecommend.
Level ofevidence

Classification of the main venoactive drugs• Benzopyrones - Alpha benzopyrones
• Coumarin - Gamma benzopyrones
• Diosmin • Micronized purified flavonoid fraction (MPFF) • Rutin and rutosides• 0-(b-hydroxyethyl)-rutosides (troxerutin, HR)
• Saponins• Escin• Ruscus extract
• Other plant extracts • Anthocyan Proanthocyanidins (oligomers), Extracts of Ginkgo,
heptaminol and troxerutin, Total triterpene fraction• Synthetic products
– Calcium dobesilate– Benzaron– Naftazone

Mode of Action of Venoactive DrugsEffect on Venous Tone
Effect on capillary Leakage
Lymphatic Network
Anti-inflammatory effect
Micronized purified flavanoid fractions (MPFF)
Increases venous tone by prolonging noradrenergic activity
Reduces capillary hyperpermeability by inhibition of leukocyte adhesion
Increases lymphatic flow and number of lymphatics
Reduces release of inflammatory mediators by inhibiting adhesions of leukocytes
Rutin and Rutosides
Increases venous tone by bhlocking the inactivation of noradrenalin
Reduces capillary hyperpermeability
_ Inhibits free radical generation
Coumarin and rutin Increase of venous flow Beneficial effects on the microcirculation
Increases high-protein edema proteolysis and lymphatic flow
_
Escin Increases venous wall tone
Decreases capillary filtration
_ Free radical scavenging anti-elastase and anti-hyaluronidase properties,
Ruscus extract Increases venous tone by venous α1 adrenergic receptors
Antipermeability effect _ _
Proantocyanidines _ Reduces hyperpermeability
_ Free radical scavenging effect
Gingko biloba _ _ _ _
Calcium dobesilate Increases venous tone Increases capillary resistance by mitigating reactive O2 species and histamine effect
Improves lymphatic drainage
Anti-oxidant and angioprotective effects, enhances nitric oxide synthetase activity
Naftazone _ Same Same Same ?

The Effects of Venoactive Drugs on Symptoms
Positıve results on the following indications
Recommendation Trials and Meta-analyses
Micronized purified flavanoid fractions (MPFF)
Pains, cramps, heaviness, sensation of swelling, edema
Grade A Coleridge-Smith etal. 2005
Hydroxethyl-rutosides
Itching, edema Grade A Unkauf et al. 1996Krenendo et al. 1993Grossman 1997
Coumarin and rutin (troxerutin)
_ Grade C Vanscheidt, et al, 2002
Escin Pain, edema Grade B Diehm et al, 1996Pittler and Ernst, 2006Siebert et al, 2002
Ruscus extract Pain, edema Grade B Boyle et al. 2003.
Proantocyanidines Pain Grade C Kiesswetter et al. 2000
Gingko biloba _ Grade C _
Calcium dobesilate Cramps, restless legs, sensation of swelling, edema
Grade A Labs et al. 2004Ciapponi et al. 2004
Naftazone _ Grade C Vayssairat et al, 1997

Indication VAD Recommendation Level of evidence
code
Relief of symptoms associated with CVDIn patients with C0s andC6s and withCVD related oedema
MPFF Strong Moderate 1B
Nonmicronized Flavanoid
Moderate Poor 2C
Oxerutin Moderate High 2A
Ca Dobesilate Moderate High 2A
Escin Moderate Moderate 2B
Ruscus Ext Moderate Moderate 2B
Gingko Biloba Weak Poor 2C
Venous ulcer healing
MPFF Strong Moderate 1B
Updated recommendations foUpdated recommendations forr VADs VADs

Drug: Drug: CalciuCalciumm dobesilate dobesilate
Symptoms: Cramps, restless Symptoms: Cramps, restless legs, sensation of swelling, legs, sensation of swelling, edemaedema
Number of RCT: 4Number of RCT: 4
Meta-analyses: 2Meta-analyses: 2
Grade of recommendation: 2AGrade of recommendation: 2A
Venoactive drugs: EfficacyVenoactive drugs: Efficacy

Drug: Drug: MPFF MPFF
Symptoms: Pain, cramps, heaviness, Symptoms: Pain, cramps, heaviness, sensation of swelling, trophic changes sensation of swelling, trophic changes and ulcerationand ulceration
Number of RCT: 5Number of RCT: 5
Meta-analyses: 1Meta-analyses: 1
Grade of recommendation: 1BGrade of recommendation: 1B
Venoactive drugs: EfficacyVenoactive drugs: Efficacy

Drug: Drug: Hydroxyethyl rutosidesHydroxyethyl rutosides
Symptoms: Itching, edemaSymptoms: Itching, edema
Number of RCT: 11Number of RCT: 11
Meta-analyses: 4Meta-analyses: 4
Grade of recommendation: 2Grade of recommendation: 2AA
Venoactive drugs: EfficacyVenoactive drugs: Efficacy

Drug: Drug: Ruscus extract(Cyclo-3R)Ruscus extract(Cyclo-3R)
Symptoms: EdemaSymptoms: Edema
Number of RCT: 2Number of RCT: 2
Meta-analyses: 1Meta-analyses: 1
Healing of ulcers: RCT 1Healing of ulcers: RCT 1
Grade of recommendation 2BGrade of recommendation 2B
Venoactive drugs: EfficacyVenoactive drugs: Efficacy

Mode of Action of Venoactive Drugs
1- Effects on Macrocirculation Most VADs increase the venous tone by a
mechanism related to noradrenaline pathway. Especially. MPFF and hydroxyethylruosides have more affinity to venous wall.
Last studies show that CVD is closely related to primary insufficiency of venous valves origined from inflammation.
MPFF: Potential anti-inflammatory effect on an animal model of acute venous HT. The protective effect on venous valves in CVD..

2-Effects on MicrocirculationCapillary resistance:: To increase capillary resistance
and to decrease capillary filtration. Especially MPFF enhanced inhibition of
adhesion of leukocytes on capillariees by micronisation..
Lymphatic drainageCoumarin and rutin edema lysis effect by proteolysis.MPFF: increase both lymphatic flow and lymphatic
channelsCa dobesilate: increases lymphatic drainage.

Protection against inflammation: The attenuation of inflammatory response by free radical scavenging, anti-elastase and anti-hyaluranidase properties of VADs (rutosides, escin, ruscus extracts, proanthocyanidines, Ca dobesilate, MPFF).
Hemorrheological disorders: Inflammation increased fibrinogen, plasma volume contraction, increased blood viscosity accumulation of huge red cell aggregates around the venules, reduced blood flow and poor O2 delivery lipodermatosklerosis.
Decrease in viscosity: MPFF, Ca dobesilate,
Increase in red cell velocity: MPFF

Efficacy on edema of Venous OriginThe confirmed efficacy by meta analyses: MPFF, Ca
debosilate, rutosides, escin, proanthocyanidine and coumarin rutin..
Pharmacological Treatment of Leg UlcersOnly MPFF: This efficacy was confirmed in 2005 by a
meta-analysis of 5 trials using MPFF as an adjunct to standard treatment in 723 patients of stage 6 of the CEAP classification.

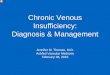
Leukocyte-Endothelium Interaction:The cause of venous inflammation and
following damage
Leukocyte-endothel interactionLeukocyte

At the level of microcirculation: Hyperpressure at the capillary level induces capillary leakage allowing the accumulation of fluids, protein, and red blood cells in the interstitial space, forming edema. Red blood cell degradation products and protein extravasations are the initial inflammatory signals that result in leukocyte migration into the interstitial space..
Leukocyte Endothelium Capillaryadhesion changes hyperpressure
Inflammation
Plasma leakage
Adhesion molecules
Free radicals
Proteolytic enzymes
Red blood cell
Leukocyte
Venous hypertension is transmitted to the microcirculation causing an inflammatory state and damage to capillaries. This leads to complications
ranging from edema to open leg ulceration.
1 - Nicolaides AN. Angiology. 2003;54:533-544. 2 - Adapted from Bergan J et al. Microcirculation. 2000;7:S23-S28. 3 - Boisseau MR. Angéiologie. 2000;52:71-77.

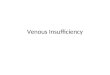
Leukocytes and changes in Leukocytes and changes in venous valvesvenous valves

Venous inflammation is the first step in
progression of early-term leg symptoms1
1 - Boisseau MR. Medicographia. 2006;28:128-136.
Inflammatory mediators released after the
leukocyte/endothelium interaction may
stimulate nociceptors in the venous wall,
causing venous pain and leg symptoms.

New England Journal of Medicine:The importance of early treatment of CVD1
1 - Bergan JJ, et al. N Engl J Med. 2006;355:488-498.
1-“Early treatment aimed at
preventing venous hypertension,
reflux, and inflammation could
alleviate symptoms of chronic
venous disease and reduce the risk
of ulcers.”
2-“Treatment to inhibit inflammation
may offer the greatest opportunity to
prevent disease–related
complications.”
• Among the medical therapy options, especially MPFF has a confirmed protective effect on mıcrocirculation against the ambulatory venous hypertension.
• MPFF attenuates the leukocyte/endothelium interaction by inhibiting and/or reducing the release of endothelial intercellüler adhesion molecule I, vasculary cell adhesion molecule and some other leukocyte adhesion molecules.

• The healing effect of MPFF is most evident in patients with leg ulcers.
• The patients who were treated with MPFF and compression combination showed 32% better healing rate than the patients who were treated topical care and compression alone during 6-month follow-up.

Other Drugs Having Effect on Venous System
• Pentoxifilline: Reduces leukocyte adhesion and erythrocyte aggregation, and a mild fibrinolytic action. Although it is relatively well tolerated, its value for treating leg ulcers remain debatable until new data become available.
• Stanozolol: Stanozolol (stanazol), an anabolic steroid, stimulates blood fibrinolysis and has been evaluated with several randomized trials for the treatment of the more advanced skin changes associated with lipodermatosclerosis. and it possibly faster ulcer healing rates.
• Prostoglandins E: Augments blood flow in the capillaries, increases fibrinolytic activity, reduces platelet and leukocyte aggregation and adhesion to endothelium. A significant improvement in the status of leg ulcers with intra-venous systemic application. (No recommendation can be made)
• Topical prostacyclin-Iloprost: Local application to the ulcer edge and surrounding skin. No clear benefit.
VAD Adverse Events• Safety of VADs is in general good and well
tolerated,
• Hepatotoxicity: Coumarin and benzarone,
• Gastrointestinal and autonomic adverse events, 5%,
• Usage in pregnancy: Some VADs have been used without any problem during 2. and 3. trimester of pregnancy, but there are no long-term series documenting this.
• Caution is recommended during breast feeding also.

INDICATIONS FOR VADs• Symptomatic CVD: Heavy legs, pain, resless legs, night
cramps, itching, numbness. If there is no symptom recurrence; max. 3-month usage. Combined usage of VADs is not appropriate.
• Anti-edema effecti: A clear effect proved by double-blind studies
• Lymphedema, MPFF, Coumarine and rutin, Ca dobesilate• Venous ulcer treatment: MPFF,• Additive effect in combination with sclerotherapy, surgery
and compression.• Compression + VAD > compression,• Compression necessary but contra-indicated (arterial
insufficiency, neuropathies),• Topical treatment: VADs + heparinoids (anti-inflammatory
effect + analgesic effect by inactivating histamine and anti-thrombotic effect),
• Prevention of venous hypertension and inflammation, protection of venous valves; MPFF

Compression Therapy
• Bandages– Short strech bandages– Four layer bandages– Hard-stiff bandages (Unna Bout)
• Compression stockings• İntermittant pneumotic compression devices

Effects of Compression Therapy
• Reduces edema• Reduces venous volume• Increases venous flow• Reduces venous reflux• Improves venous pump• Increases lymphatic flow

Recommendations for Compression Stockings
Indication Grade of recommendation and evidence
A (10-14 mmHg) C0S, C1S B
I (15-21 mmHg ) C2SC2S (cerrahi sonrası)C2S (skleroterapi sonrası)
BBC
II (23-32 mmHg) C3 C4DVT sonrası
BA
III (34-46 mmHg) C5 C6 A
CEN pressure gradings

Compression Bandaging
• There is no proved superiority in comparison of different bandaging styles (i.e, circular, figure of eight or spiral).
• Only, the superiority of multi-layer (four layer) bandaging was shown in treatment of active venous ulcers.

Intermittant pneumatic compression devices
• Shortens the healing time in treatment of active venous ulcers. (recommendation and evidence level B)
Caution in arterial insufficiency: Can not be used if the patient has ABI<0,4, or can be used after revascularization
Should not be used in dermatitis origined from synthetic materials used for compression.

Adaptation of lifestyle
There is no evidence-based recommendation about their efficacy.
• Walking exercises• Avoiding from long-time stand up position• Avoiding from obesity• Leg elevation and bed rest• Avoiding from heat, hot water

Ineffective adjuncts to ulcer care• Hyperbaric oxygen —• Electromagnetic therapy — . • Therapeutic ultrasound —
• Medical management of lower extremity chronic venous disease Literature review current through: Sep 2013.

Conclusion
• The combination of medical treatment with compression provides considerably superior healing results and better life quality than the compression alone.
• Medical treatment has a considerable efficacy in almost every stages of CVD by both alleviating the symptoms and preventing the progression of symptoms as well as complications.