Embed Size (px)
Citation preview

Easy EMG
Chapter 1 & 2
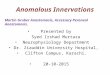
CHAPTER 1: What is EMG?The entire purpose of electrodiagnostic (END) studies is to help figure out whether
there is a problem in the nervous system and if so, where the problem is occurring.
The Most Common END Tests Done Are:
1. Nerve Conduction Studies (NCS)
2. Electromyography (EMG)
• Both NCS and EMG are normally done together.
• Both tests can provide different information.
• NCS provides information on nerves
• EMG provides information on nerves but can indirectly tell us information on the nerves affecting them.
• Remember they are really an extension of Neurological and Musculoskeletal examination
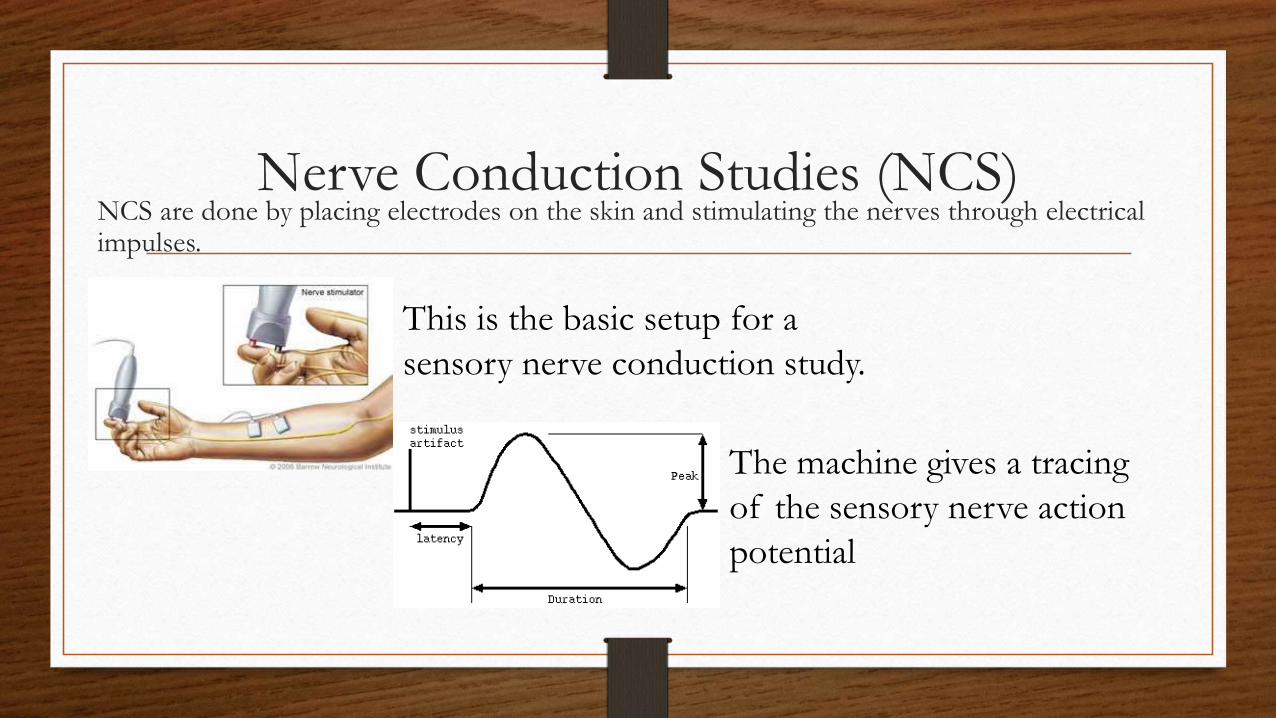
Nerve Conduction Studies (NCS)NCS are done by placing electrodes on the skin and stimulating the nerves through electrical impulses.
This is the basic setup for a
sensory nerve conduction study.
The machine gives a tracing
of the sensory nerve action
potential
Process of the NCS
• To study motor nerves, electrodes are placed over a muscle that receives its
innervation from the nerves you want to test (stimulate).
• The electrical response of the muscle is then recorded and you can
determine both how fast and how well the nerve responded.
• This can determine whether the problem stems from a nerve or muscle.
NCS are broken down into TWO categories:
1) Motor Nerve Conduction Testing
2) Sensory Nerve Conduction Testing
• NCS can be performed on any accessible nerve including peripheral nerves and
cranial nerves.
Basic Findings are generally two-fold:
1) How fast is the impulse traveling?
2) What does the electrical representation of the nerve stimulation (Action potential
morphology) look like on the screen?

Nerve Conduction Study Terms
• Action Potential: this is the waveform you see on the screen.
• Latency: Time interval between the onset of a stimulus and the onset of action potential
• Conduction Velocity: How fast the fastest part of the impulse travels (sensory or motor conduction velocity)
• Amplitude: the maximal height of the action potential
• Antidromically: Physiologically opposite direction an impulse travels on a certain nerve.
• Orthodromically: Physiologically normal direction an impulse travels on a certain nerve.
• F-Wave: a compound muscle action potential evoked by antidromically stimulating a motor nerve from a muscle using an electrical stimulus.
• H-Reflex (Hoffman Reflex): a compound muscle action potential evoked by orthodromically stimulating sensory fibers, synapsing at the spinal level and returning orthodromically via motor fibers
Electromyography (EMG)
Electromyography (EMG) is the process by which an examiner puts a needle
into a particular muscle and studies the electrical activity of that muscle
• Electrical activity comes from the muscle itself- no shocks are used to
stimulate the muscle.
• Does not actually test nerves, however, does test nerves indirectly by testing
the muscles.
EMG vs NCS
1. You use a needle and put it into the muscle for EMG rather than
electrodes that are placed on the skin for NCS.
2. You don’t use any electrical shocks in EMG; rather you look at the intrinsic
electrical activity of the muscle.
3. You get direct information about the muscles in EMG and indirect
information about the nerves that supply the muscles you test
END of Chapter 1
CHAPTER 2: Why Do Electrodiagnostic
Studies?
Electrodiagnostic testing is an important method for physicians to distinguish between many nerve and muscle disorders.
• They represent a part of the diagnostic puzzle
• They are sometimes essential in establishing a particular diagnosis and sometimes they are not useful at all.
In a practical sense, you can consider electrodiagnostic testing in any of the following
circumstances, when a patient is complaining of or has:
1. numbness
2. tingling (parenthesis)
3. pain
4. weakness
5. a limp
6. Muscle atrophy
7. Depressed deep tendon reflexes
8. fatigue
However, the list of signs and symptoms do not automatically lead to electrodiagnostic
testing.
• These tests are an extension of the history and physical examination.
• They are useful in establishing the correct diagnosis, whether someone should have
surgery and prognostic reasons to follow the course of recovery (or deterioration)
from an injury.
Electrodiagnostic studies are useful to:
1) Establish the correct diagnosis.
2) Localize the lesion.
3) Determine treatment even if the diagnosis is already known.
4) Provide information about the prognosis.
The Skilled and Compassionate
Electrodiagnostician
It is important for you to be both technically skilled and able to put the patient at ease:
1. Avoid keeping the patient waiting, as that will increase his or her anxiety.
2. Before you start, explain to the patient what you are going to do.
3. Explain that these tests will be useful in determining the diagnosis.
4. Reassure the patient you will stop the test anytime they request you to.
5. Start with the area of greatest interest- especially if you suspect that the patient
won’t tolerate the entire study.
6. Although not typically used, analgesic or sedating medication can be given.
7. In most instances, it is best not to show patients the needle as many people
associate more pain with a longer needle, when a larger diameter needle would
actually cause more discomfort.
8. Assure the patient you will minimize the length of the exam, doing what is
absolutely necessary to obtain required information.
9. Keep the room warm. Two purposes:
a) The patient will most likely be dressed in a gown and therefore is prone to being cold.
b) The results of your electrodiagnostic test may be affected if the patient’s extremity is cold.
Special Precautions
There are a number of clinical situations that deserve special mention
• These are cases where the electrodiagnostic studies can be safely done, as long as the physician takes measures to ensure the safety of the patient and the accuracy of the test.
Morbid Obesity: Overweight; it may be difficult (or impossible) to localize specific muscles.
Thin Individuals: important not to insert the needle too far as it can injure other tissues.
Bleeding Disorders: a patient with a known bleeding disorder or those who are on Anticoagulant medications should be assessed on an individual basis and the risk/ benefit of the test evaluated.
Blood Precautions: practice safe needle stick procedures.
Contraindications:
• For EMG: Patient with severe bleeding disorders or whose anticoagulation therapy is
out of control.
• For NCS: Patient with cardiac defibrillators implanted.
Complications:
• Infection: bleeding and accidently penetrating into some other part.
Controversy:
• May cause some discomfort (pain)
• Relatively expensive test to perform
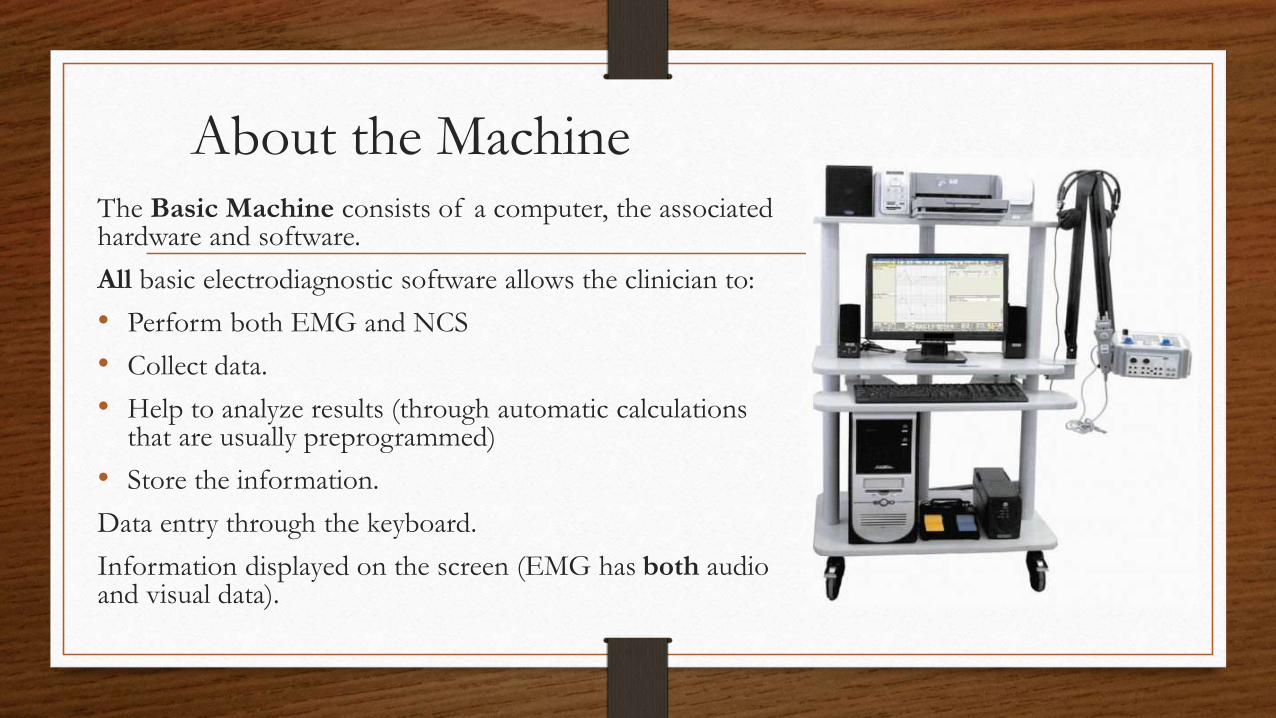
About the MachineThe Basic Machine consists of a computer, the associated hardware and software.
All basic electrodiagnostic software allows the clinician to:
• Perform both EMG and NCS
• Collect data.
• Help to analyze results (through automatic calculations that are usually preprogrammed)
• Store the information.
Data entry through the keyboard.
Information displayed on the screen (EMG has both audio and visual data).
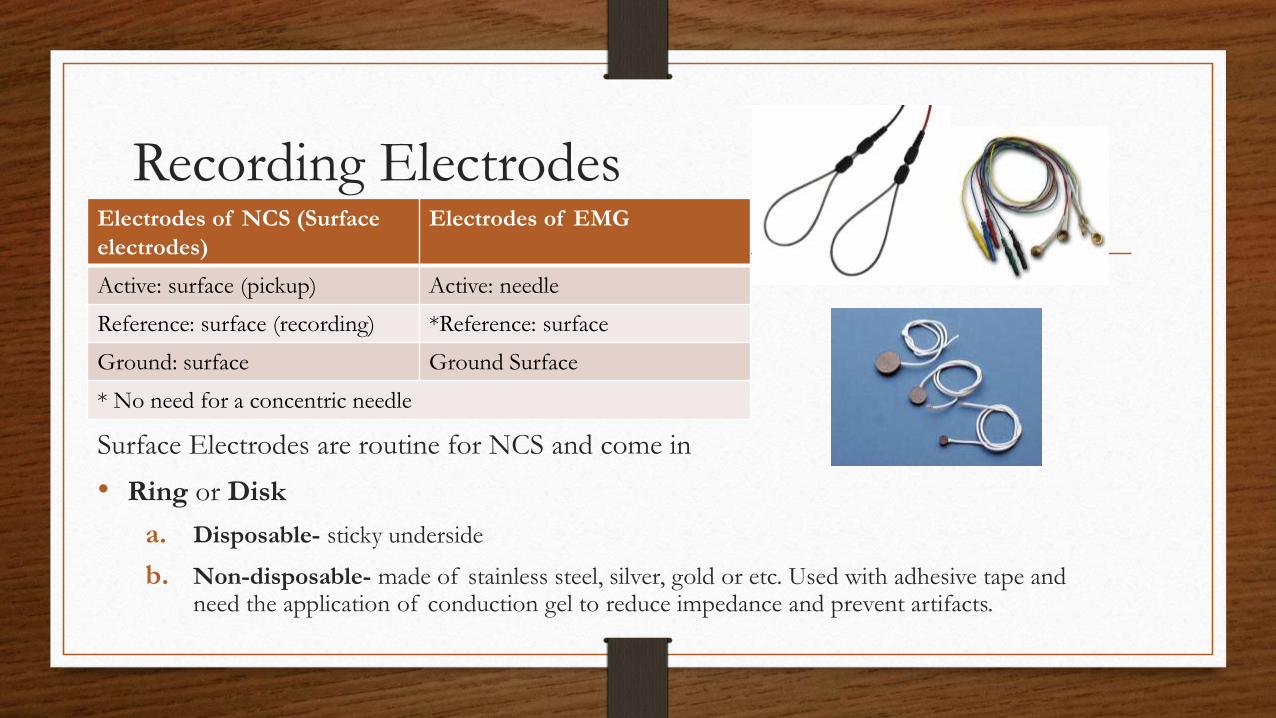
Recording Electrodes
Surface Electrodes are routine for NCS and come in
• Ring or Disk
a. Disposable- sticky underside
b. Non-disposable- made of stainless steel, silver, gold or etc. Used with adhesive tape and need the application of conduction gel to reduce impedance and prevent artifacts.
Electrodes of NCS (Surface
electrodes)
Electrodes of EMG
Active: surface (pickup) Active: needle
Reference: surface (recording) *Reference: surface
Ground: surface Ground Surface
* No need for a concentric needle
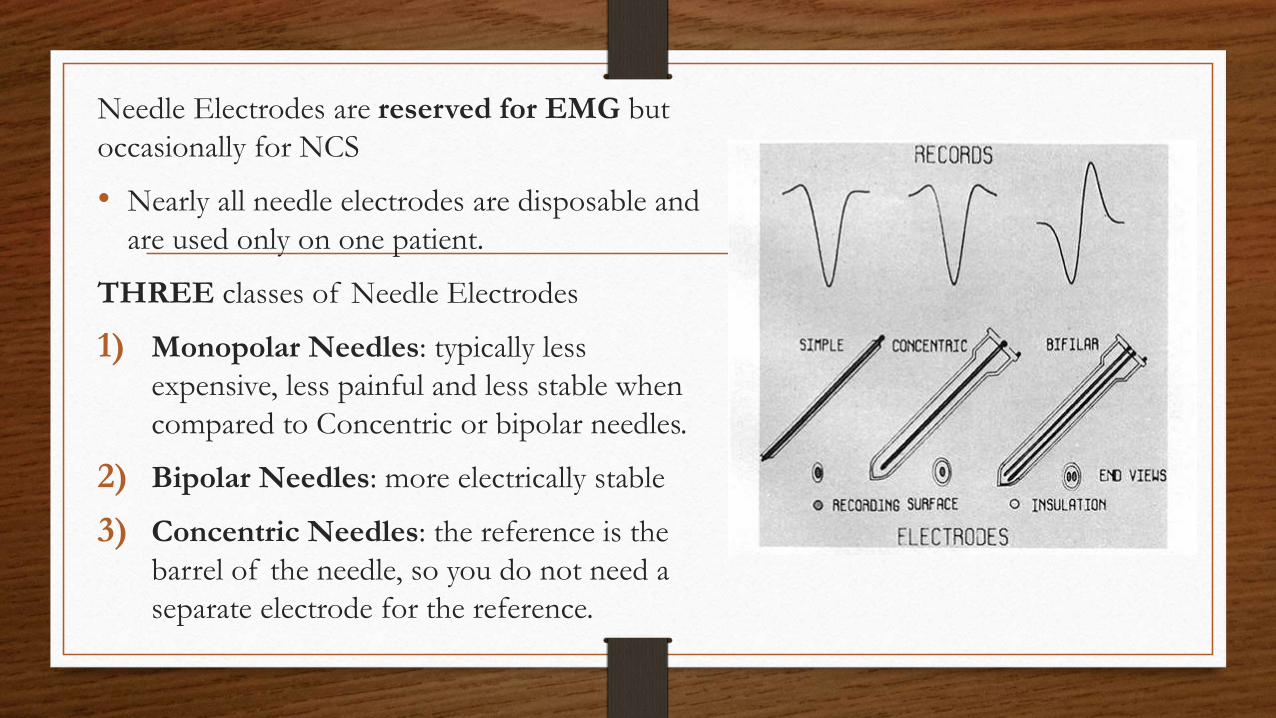
Needle Electrodes are reserved for EMG but
occasionally for NCS
• Nearly all needle electrodes are disposable and
are used only on one patient.
THREE classes of Needle Electrodes
1) Monopolar Needles: typically less
expensive, less painful and less stable when
compared to Concentric or bipolar needles.
2) Bipolar Needles: more electrically stable
3) Concentric Needles: the reference is the
barrel of the needle, so you do not need a
separate electrode for the reference.
Amplifiers
Amplifiers magnify the signal so that it can be displayed.
Preamplifiers attenuate the biological signal before it gets to the amplifier in
order to:
1. Make sure that the filters have sufficient signal voltage to work with.
2. To make sure that the level of signal voltage is much higher than that of
system noise.
Preamplifiers Filters Amplifier

Differential Amplifiers are used in electrodiagnostic studies because of it Common
Mode Rejection Feature.
• Common Mode Rejection (CMR) rejects unwanted signals from the electrodes being
compared that are similar. (i.e. 60 Hz Signal)
• Differential Amplifiers take the electrical impulses from the active electrode and
amplifies them.
• Takes impulses from the reference electrode, inverts them, and amplifies them.
• Combines these two potentials.
• Cancels out any common noise to both electrodes (i.e. 60 Hz artifact present in both electrodes
are cancelled out).
• Differences, however, will be amplified.
CMR ratio is how well an amplifier eliminates similar types of noise
Filters
Filters are used to faithfully reproduce the signal you want while trying to exclude both
High and Low Frequency electrical noise.
• Every signal in both NCS and EMG passes through both a low frequency filter
before being displayed.
• It is important to understand that there is always a trade off when you use filters (the
signal will be altered to some degree)
Type of Filter Other Name Description
Low Frequency
Filter
High Pass Filters out low frequency signals that if present cause a
wandering baseline.
High Frequency
Filter
Low Pass Filters out high frequency signals that if present can cause a
“noisy” baseline especially on sensory studies.
Display System
Display systems for electrodiagnostic
studies are either via a video screen or
paper
Cathode Ray tube is the standard
display, which uses a controlled
electron beam (cathode ray) to excite
phosphorus on the screen that
presents a visual display.

Two Settings on the Display Screen
1. Sweep Speed: the horizontal axis; represents how long an action potential can
last; milliseconds (ms or msec)
2. Sensitivity (gain): Vertical axis; represents response amplitude; Millivolts (mV)
for Motor Studies or microvolts (µV) for Sensory Studies
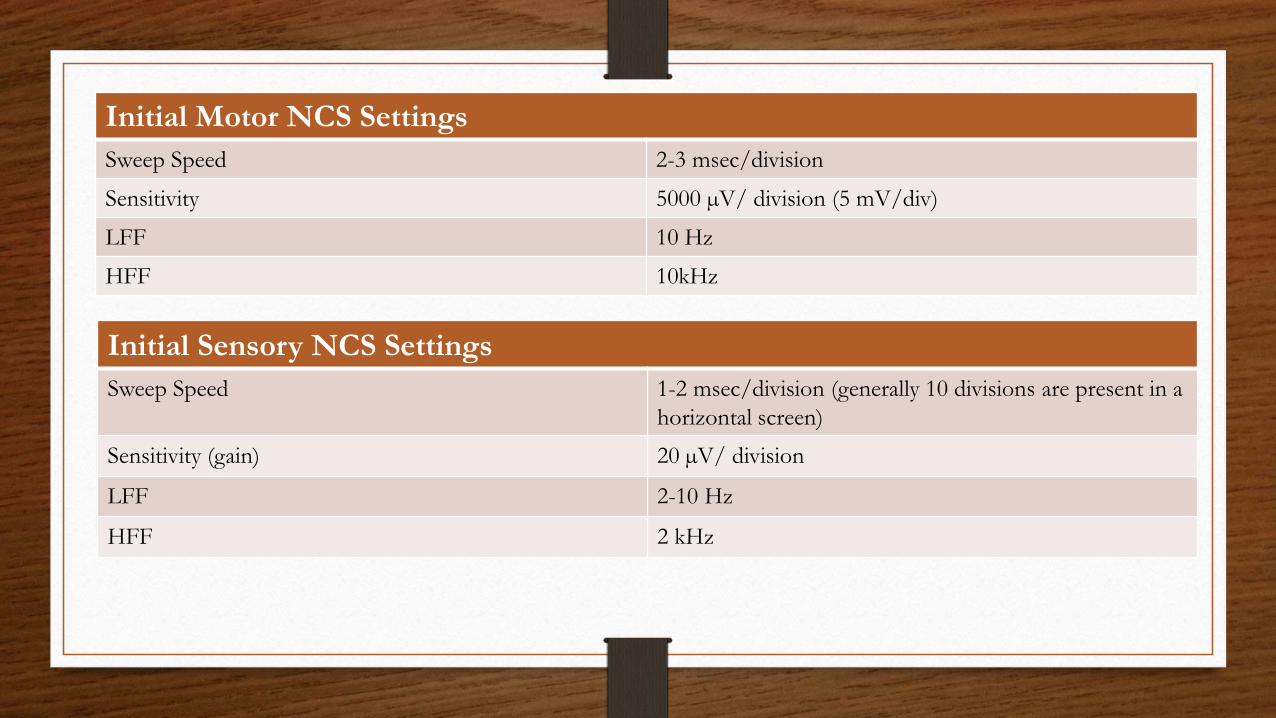
Initial Motor NCS Settings
Sweep Speed 2-3 msec/division
Sensitivity 5000 µV/ division (5 mV/div)
LFF 10 Hz
HFF 10kHz
Initial Sensory NCS Settings
Sweep Speed 1-2 msec/division (generally 10 divisions are present in a
horizontal screen)
Sensitivity (gain) 20 µV/ division
LFF 2-10 Hz
HFF 2 kHz

Artifacts and Technical Factors
Physiological Factors (Patient- related)
• Stimulus Artifact is an electrically recorded response that is elicited directly from the stimulator.
• Occurs in all NCS, however, it only becomes a problem when the trailing edge of the recorded artifact overlaps with the potential being recorded.
• Make sure the ground is between is the recording and stimulating electrodes to minimize stimulus artifact.
Technical Factors (technically related)
• Filters: faithfully reproduce the signal you want while trying to exclude both high and low frequencies.
• Electrode Placement: proper electrode placement is a critical part of performing accurate electrodiagnostic studies.
Stimulation
Supramaximal Stimulation: all measurements made in NCS are done with the assumption that the strength of the stimulus is high enough to depolarize every axon in the nerve.
• If Supramaximal stimulation is not achieved at the Distal Site, then you might mistakenly interpret this recording as signifying axonal loss due to low amplitude.
• If Supramaximal stimulation is not achieved at the Proximal Site, this might appear to be a conduction block.
• Conduction block is the failure of an Action Potential to be conducted past a particular point where as conduction is possible below the point of the block.

With Respect to Evoked Potentials the stimulus can be graded as:
• Subthreshold: when the stimulus is less than the threshold.
• Threshold: when the stimulus is sufficient to produce a detectable response.
• Submaximal: is stimuli below the maximal intensity.
• Maximal: is the stimulus intensity after which a further increase in the stimulus intensity causes no increase in the amplitude.
• Supramaximal: is intensity approximately 20% more than maximal, and used for Nerve Conduction Studies.
For NCS, too much stimulation may cause co-stimulation of adjacent nerves or may stimulate nerves farther from the site
The goal is to reach Supramaximal stimulation without applying so much stimulation that adjacent nerve are also stimulated.
Measurements
The machine will do most of the calculations for you
• However, you still need to measure the distance between stimulation sites and the recording electrode of a patient’s limb when determining conduction velocity.
Make sure the measurements are done accurately.
• The main problem is if the patient’s limb is moved in different positions, which changes the distance you are measuring. (Commonly occurs in ulnar nerve studies.)
Remember to follow the course of the nerve, rather than measuring the shortest distance between the stimulating and recording electrodes.
Sweep Speed & Sensitivity
Both the sweep-speed and sensitivity can affect you NCS results.
• As the sensitivity is increased, the onset latency will decrease
• Record all latency measurement with the same sensitivity and sweep speed.
END of Chapter 2