Embed Size (px)
Citation preview

1

FACIAL NERVE
2

1. Introduction
2. Embryology & Nuclei of origin
3. Course & Relations
4. Branches of facial nerve
5. Functional components
6. Ganglia associated with facial nerve
7. Blood supply
8. Applied Aspect
CONTENTS 3

4

• 7th cranial nerve
• Mixed nerve
• It emerges from the brain stem between the pons and the medulla.
• Function- Conveys taste sensation from anterior 2/3rd of tongue and oral cavity and also , controls the muscles of facial expression.
• Supplies- preganglionic parasympathetic fibres to several head and neck ganglia
5
Sensory root
Motor root

Embryology
The facial nerve is developmentally derived from the hyoid
arch, which is the second branchial arch.
It arises as 2 main divisions- motor and sensory
The motor division of facial nerve is derived from the basal
plate of the embryonic pons
The sensory division originates from the cranial neural
crest
6

Facial nerve course, branching pattern, and anatomical
relationships are established during the first 3 months
of prenatal life
The nerve is not fully developed until about 4 years of
age.
The first identifiable Facial Nerve tissue is seen at the
third week of gestation- facioacoustic
primordium or crest
7

FACIAL NERVE EMBRYOLOGY: 4TH WEEK
By the end of the 4th
week, the facial and
acoustic portions are
more distinct
The facial portion
extends to placode
The acoustic portion
terminates on otocyst
8

FACIAL NERVE EMBRYOLOGY: 5TH WEEK
Early 5th week, the
geniculate
ganglion forms
from distal part of
primordium
It separates into 2 branches: main trunk of facial nerve and chorda tympani
9

FACIAL NERVE EMBRYOLOGY: 6TH WEEK
Near the end of the 5th
week, the facial motor nucleus is recognizable
The motor nuclei of VI and VII cranial nerves initially lie in close proximity.
The internal genuforms as metencephalon, it elongates and CN VI nucleus ascends
10

FACIAL NERVE EMBRYOLOGY: 7TH WEEK
Early 7th week, geniculate ganglion is well-defined and
facial nerve roots are recognizable
The nervus intermedius arises from the ganglion and
passes to brainstem. Motor root fibers pass mainly
caudal to ganglion
11

Proximal branches form in the 6th week, posterior
auricular branch, branch of digastric
Early 8th week temporofacial and cervicofacial divisions
present
Late 8th week, 5 major peripheral subdivisions present
12

NUCLEI OF ORIGIN
13

FUNCTIONAL
COMPONENT
NUCLEI DISTRIBUTION FUNCTION
GVE Superior salivatory
nucleus
(lies in the pons lateral to
the main motor nucleus
of VII )
Submandibular and
sublingual salivary
glands.
Preganglionic
Secretomotor
SVE Motor nucleus of facial
nerve
(lies in lower part of
pons)
Muscles of facial
expression,
stylohyoid, posterior
belly of digastric,
platysma and
stapedius.
Facial expression
SVA Nucleus of tractus
solitarius (lies in
medullla)
Taste buds in the
anterior 2/3rd of
tongue except
vallate papillae.
Taste sensations
GSA Spinal nucleus of Vth
nerve
Part of skin of
external ear.
Exteroceptive
sensation
14

COURSE OF FACIAL
NERVE
15

The course of facial nerve is divided by stylomastoid
foramen into
INTRACRANIAL
INTRAPETROUS PARTEXTRACRANIAL PART
16

The nerve arises in
the pons in brainstem. It
begins as two roots; a
large motor root, and a
small sensory
root (Nervous
intermedius)
The two roots travel
through the internal
acoustic meatus.
17

Within the temporal bone, the
roots leave the internal
acoustic meatus, and enter
into the facial canal (‘Z’
shaped) . The two
roots fuse to form the facial
nerve.
1. The nerve forms
the geniculate ganglion
2. The nerve gives rise to
the greater petrosal
nerve (parasympathetic
fibres to glands), the nerve
to stapedius (motor fibres
to stapedius muscle), and
the chorda
18

The facial nerve then exits the facial canal
(and the cranium) via the stylomastoid
foramen, located just posterior to the styloid
process of the temporal bone
19

After exiting the skull, the
facial nerve turns
superiorly to run just
anterior to the outer ear.
The first extracranial
branch to arise
is the posterior auricular
nerve. It provides motor
innervation to the some of
the muscles around the
ear.
Immediately distal to this,
motor branches are sent to
the posterior belly of the
digastric muscle and to
20

The main trunk of the
nerve (motor root of the facial
nerve), continues anteriorly and
inferiorly into the parotid gland.
Within the parotid gland, the nerve
terminates by splitting into five
branches:
1. Temporal branch
2. Zygomatic branch
3. Buccal branch
4. Marginal mandibular branch
5. Cervical branch
These branches are responsible for
innervating the muscles of facial
21

Branches
Branches of communication
Branches of distribution

TE
RM
INA
L B
RA
NC
HE
S
EX
TR
AC
RA
NIA
L
INT
RA
CR
AN
IAL1.Greater
petrosalnerve
2.Nerve to stapedius
3.Chorda tympani
1.Posterior auricular nerve
2.Digastric nerve
3.Stylohyoid nerve
1.Temporal
2.Zygomatic
3.Buccal
4.Marginal mandibular
5.Cervical
BRANCHES OF DISTRIBUTION 23

I- WITHIN THE FACIAL CANAL:
1- Nerve to stapedius: supplies the stapedius muscle.
2- Greater superficial petrosal nerve (GSPN) : arises
from the geniculate ganglion.
3- Chorda tympani nerve:
It arises from the facial nerve 6 mm above the stylomastoid
foramen and runs upwards to perforate the posterior bony
wall of the tympanic cavity.
24

It then passes forwards on the medial surface of
the tympanic membrane
It comes out of the tympanic cavity through the
petrotympanic fissure to the infratemporal
fossa where it joins the lingual nerve.
Through the lingual nerve, it supplies both the
submandibular and sublingual salivary glands
by secretomotor fibres and taste fibers from the
anterior 2/3 of the tongue
25

II- AT THE EXIT FROM THE STYLOMASTOID
FORAMEN
1- Posterior auricular nerve:
to the auricularis posterior and occipitalis muscle.
2- Digastric branch:
to the posterior belly of digastric muscle
3- Stylohyoid branch:
to the stylohyoid muscle
26

III- TERMINAL
BRANCHES
27

28

29
Elevates upper lip
Smile
Snoring
THE BUCCAL BRANCH SUPPLIES:

30
Moves skin
of forehead
Flare nostrils
closes the
mouth, puckers
the lips
chewing
smile

Internal acoustic meatus Vestibulocochlear nerve
Geniculate ganglion A. Greater petrosal nerve
B. Lesser petrosal nerve
C. External petrosal nerve
Facial canal Vagus nerve
Stylomastoid foramen IX & X cranial nerve
Greater auricular nerve
Auriculotemporal nerve
Behind ear Lesser occipital
Face V nerve
Neck Transverse cutaneous nerve
Branches of Communication 31

GANGLIA ASSOCIATED WITH
THE FACIAL NERVE 32

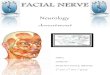
GENICULATE GANGLION
• Derived from Latin GENU = "KNEE“
• L-shaped collection of fibers and sensory neurons of
the facial nerve located in the facial canal of the head.
• Receives fibers from the motor, sensory, and
parasympathetic components of the facial nerve
33

Innervates
Lacrimal glands
Submandibular glands
Sublingual glands
Tongue
Palate
Pharynx
External auditory meatus
Stapedius
Posterior belly of the
digastric muscle
Stylohyoid muscle
Muscles of facial
expression.
34

SUBMANDIBULAR GANGLION
Small and fusiform in shape.
Situated above the deep portion of the
submandibular gland, on the hyoglossus
muscle, near the posterior border of the
mylohyoid muscle.
The ganglion 'hangs' by two nerve
filaments from the lower border of the
lingual nerve one anterior and one
posterior.
Through the posterior of these it receives
a branch from the chorda tympani nerve
which runs in the sheath of the lingual
nerve.
35

PTERYGOPALATINE GANGLION
The Pterygopalatine ganglion
(meckel's ganglion, nasal
ganglion or sphenopalatine
ganglion) - parasympathetic
ganglion found in the
pterygopalatine fossa.
It's largely innervated by
the greater petrosal nerve
(a branch of the facial nerve);
and its axons project to the
lacrimal glands and nasal
mucosa
36

FACIAL NERVE BLOOD SUPPLY
The facial nerve gets it’s blood supply from
1. Anterior inferior cerebellar artery – at the
cerebellopontine angle
2. Labyrinthine artery (branch of anterior inferior cerebellar
artery) – within internal acoustic meatus
3. Superficial petrosal artery (branch of middle meningeal
artery) – geniculate ganglion and nearby parts
37

4. Stylomastoid artery (branch of posterior
auricular artery) – mastoid segment
5. Posterior auricular artery supplies the facial
nerve at & distal to stylomastoid foramen
38

Child Adult
Chorda tympani may exit through
Stylomastoid Foramen
Chorda tympani exit proximal to
Stylomastoid Foramen
Nerve trunk is more anterior and lateral
on exit through Stylomastoid Foramen
Nerve trunk is less anterior and deeper
Nerve more superficial over angle of
mandible
Nerve less superficial over angle of
mandible
AGE CHANGES 39

40

DISORDERS OF FACIAL
NERVE
Facial nerve lesions:
1. Supra-nuclear type
2. Nuclear type
3. Peripheral lesions
Injury at internal acoustic meatus
Injury distal to geniculate ganglion
Injury at stylomastoid foramen
41

1. SUPRA NUCLEAR TYPE:
Features:
a) Paralysis of lower part of face (opposite
side)
b) Partial paralysis of upper part of face
c) Normal taste and saliva secretion
d) Stapedius not paralysed
42

2. NUCLEAR TYPE:
Features:
a) Paralysis of facial muscle (same side)
b) Paralysis of lateral rectus
43

3. PERIPHERAL LESION
a) At internal acoustic meatus
Features:
i. Paralysis of secretomotor fibers
ii. Hyper acusis
iii. Loss of corneal reflex
iv. Taste fibers unaffected
v. Facial expression and movements paralysed
44

b) Injury distal to geniculate ganglion
Features:
i. Complete motor paralysis (same side)
ii. No hyper acusis
iii. Loss of corneal reflex
iv. Taste fibers affected
v. Facial expression and movements
paralysed.
45

c) Injury at stylomastoid foramen
• Condition known as Bell’s Palsy
46

47

1. BIRTH
Forceps delivery
Dystrophia myotonica
Moebius' syndrome (facial diplegia
associated with other cranial nerve deficits)
2. TRAUMA
Basal skull fracture
Facial injuries
Penetrating injury to middle ear
Altitude paralysis (barotrauma)
Scuba diving (barotrauma)
48

49
3. INFECTIONS
External otitis
Otitis media
Mastoiditis
Chicken pox
Herpes zoster (Ramsay Hunt
syndrome)
Encephalitis
Poliomyelitis (type I)
Mumps
Leprosy
Coxsackievirus
Malaria
Syphilis
Scleroma
Tuberculosis
Botulism
Mucormycosis
Lyme disease

4.TOXIC 5.METABOLIC 50
Thalidomide (Miehlke syndrome,
cranial nerves VI, VII with
congenital malformed external
ears and deafness)
Tetanus
Diphtheria
Carbon monoxide
Diabetes mellitus
Hyperthyroidism
Pregnancy
Hypertension
Acute porphyria

6.NEOPLASTIC
7th nerve tumour
Leukaemia
Meningioma
Haemangioblastoma
Sarcoma
Carcinoma (invading or metastatic)
Haemangioma of tympanum
Facial nerve tumour (cylindroma)
Schwannoma
Teratoma
Fibrous dysplasia
von Recklinghausen's disease
51

7. IATROGENIC 8. IDIOPATHIC 52
Mandibular block anesthesia
Head and neck surgery
Myasthenia Gravis
Guillain-Barre Syndrome
Sarcoidosis
Familial Bell's Palsy

BELL’S PALSY
53

Background of BELL’S PALSY
First described more than a
century ago by Sir Charles Bell
Controversy still surrounds its
etiology and management
Bell palsy is certainly the most
common cause of facial paralysis
worldwide
54

DEMOGRAPHICS OF
BELLS PALSY
Race: slightly higher in persons of Japanese descent.
Sex: No difference exists
Age: highest in persons aged 15-45 years.
Bell palsy is less common in those younger than 15 years
and in those older than 60 years.
55

Pathophysiology of Bells palsy
Main cause of Bell's palsy is latent herpes viruses
(herpes simplex virus type 1 and herpes zoster virus),
which are reactivated from cranial nerve ganglia
Polymerase chain reaction techniques have isolated
herpes virus DNA from the facial nerve during acute
palsy
56

I. Unilateral involvement
II. Inability to smile, close eye or raise eyebrow
III. Whistling impossible
IV. Drooping of corner of the mouth
V. Inability to close eyelid (Bell’s sign)
VI. Inability to wrinkle forehead
VII. Loss of blinking reflex
VIII.Slurred speech
IX. Mask like appearance of face
X. Loss/ alteration of taste
FEATURES OF BELL’S PALSY57

MANAGEMENT OF BELLS PALSY
It focuses on protecting the cornea from drying and
abrasion due to problems with lid closure and the
tearing mechanism.
Lubricating drops should be applied hourly during
the day and a simple eye ointment should be used at
night.
EYE CARE
58

Treatment consists of Infra-red radiation on affected
side of the face at 2 ft (60cm) ,followed by interrupted
galvanism on affected side
Treatment was given daily at first few weeks & later
thrice weekly.
All patients are instructed to massage the face daily
70-80% of these patients recover completely, while the
reminder develop various sequelae within one to three
months
59

MEDICAL TREATMENT
Corticosteroids :
Prednisolone 1 mg/kg/day 7-10 days
Corticosteroids combine with antiviral drug is better
Acyclovir 400 mg 5 times/day
Famciclovir and valacyclovir 500 mg bid
60

SURGICAL
TREATMENT
Facial nerve decompression
Indication:
Completely paralysis
Appropriate time for surgery is 2-3 weeks after paralysis
61

FACIAL NERVE PARALYSIS
Most commonly during inferior alveolar nerve block or
infraorbital nerve block
Cause
LA into the capsule of the parotid gland
Prevention
Use of proper technique
Avoid over insertion of needle
Treatment
Transient, self correcting with 3 hours or less.
62

63

Gray's Anatomy By Richard Drake, A. Wayne Vogl, Adam W. M.
Mitchell.
A.K. Datta Essentials Of Human Anatomy Head And Neck. 4th
Edition
B D CHAURASIA’S Human Anatomy. Volume 3 Edition 4th
Atlas Of Anatomy Edited By Anne M. Gilroy, Brian R.
Macpherson, Lawrence M. Ross
Monheim’s Local Anaesthesia And Pain Control In Dental
Practice
64REFERENCES

65