Embed Size (px)
Citation preview

Lecture 6
Congenital and Acquired Disorders Secondary Hemostasis

Groups of Coagula<on Factors • Fibrinogen group
– Fibrinogen, V, VIII, XIIII – All are acted upon by thrombin – All are consumed during coagula<on (not present in serum) – FV and FVIII à Labile – Fibrinogen and FVIII à acute phase reactants
• Increase during inflamma<on, pregnancy, estrogen therapy, stress
• Prothrombin group – II, VII, IX, X , C, S, Z – Depend on vitamin K during their synthesis – Have a GLA domain at the N-‐terminus – consis<ng of 10-‐12 glutamic acid (GLA) residues – Vitamin K catalyzes the carboxyla<on of the y-‐carbon of the glutamic acids à addi<on of a
second carboxyl group – These groups are nega<vely charged à binding Ca2+ ions – necessary for binding to PF3
• Contact group – PK, HMWK, XII, XI – Involved in ac<va<on of the intrinsic pathway of the plasma-‐based coagula<on model – Moderately stable – NOT consumed during cloZng (found in serum)

Vitamin K Deficiency
• Found in leafy green plants as phylloquinone and in bacteria as menaquinone • Required for the a]achment of gamma-‐carboxyglutamic acid (GLA) residues to the VKDFs • Factors produced in the absence of VK lack the required number of GLA residues and are
func<onally inac<ve à PIVKAs • GLA residues facilitate the a]achment of the factors to PF3 through calcium binding
• VK deficiency seen in 1. Absence of bile salts in GI tract
• VK is fat soluble à bile salts are required for adsorp<on 2. Malabsorp<on syndromes
• VK is absorbed primarily through the GI tract 3. Dietary lack of phylloquinone
• Due to lack of green leafy vegetables in the diet 4. An<bio<c therapy
• Kills the normal flora of the GI tract—responsible for menaquinone 5. Bowel surgery
• Combina<on of loss of phylloquinone and menaquinone 6. Newborn infants
• Deficient in vitamin K at birth
3

What is Vitamin K? • Fat soluble compound
– Necessary for the synthesis of several proteins required for blood cloZng 1) Vit K 1 (Phylloquinone)
-‐ Natural form -‐ Found in plants -‐ Provides the primary source of vitamin K to humans through dietary consump<on
2) Vitamin K2 compounds (Menaquinones) -‐ Made by bacteria in the human gut -‐ Provide a smaller amount of the human vitamin K requirement
Required for: 1) Coagula<on 2) Bone Mineraliza<on 3) Cell growth

Vitamin K -‐ Carboxyglutamate FII, FV, FVII, FX, PC, PS
ACTIVE FII, FVII, FIX, FX, PC, PS
INACTIVE
oxidized reduced

The Vitamin K Cycle • Dietary vitamin K à reduced by vitamin K
reductase to generate vitamin K hydroquinone
• Vitamin K hydroquinone – Serves as a cofactor for the vitamin K-‐
dependent carboxylase – Converts glutamic acid residues at the N-‐
termini of the vitamin K-‐dependent precursors to carboxyglutamic acid residues
– Creates the so-‐called Gla-‐domain
• Gla-‐domain is cri<cal for the interac<on of the vitamin K-‐dependent cloZng factors with nega<vely charged phospholipid membranes calcium bridging
• During vitamin K-‐dependent carboxyla<on 1. Vitamin K is oxidized to vitamin K
epoxide 2. Vitamin K epoxide is then converted to
vitamin K by vitamin K epoxide reductase 6

Vitamin K Deficiency
• Diagnosis – Prolonged PT and aPTT, normal BT and TT – In mild VKD – aPTT will be normal because only FVII will be decreased (FVII has
shortest ½ life) – Factor assays for II, VII, IX, and X
• Note 1. FV is used to differen<ate between LD and VKD 2. FV is not VK-‐dependent, but is synthesized in the liver 3. TT is normal to prolonged in LD 4. TT is normal in VKD
• Treatment – Aquamephyton — colloidal solu<on of vitamin K for parenteral injec<on
• Given intramuscularly and a normaliza<on of the PT is seen in 12-‐14 hours • In life-‐threatening situa<on—FFP to supply the missing factors
7

Renal Dysfunc<on
• Recognize > 200 years ago • Underlying pathophysiology
– Impaired platelet func<on à one of the main determinants of uremic bleeding
– Mul<factorial • Intrinsic platelet defects • Abnormal platelet –endothelial interac<on • Uremic toxins and anemia also contribute
• Levels of circula<ng coagula<on factors are normal – Normal PT/aPTT – Unless there is a coexis<ng coagulopathy
8

Renal Disease
• Bleeding from uremia is major cause of morbidity in pa<ents with end-‐stage renal disease
• Focus a. Platelet dysfunc<on b. Abnormal platelet-‐vessel wall interac<ons c. Reten<on of uremic toxins d. Increased levels of nitrous oxide
• Correc<on of the anemia with RBC transfusions or rEPO à improve the bleeding tendency
• Hemodialysis par<ally corrects the BT
9

Pathophysiology of Renal Disease
• Platelet dysfunc<on is the most important – Decreased platelet aggrega<on and impaired adhesiveness
• Impaired IIb/IIIa gp receptor • Altered release of ADP and serotonin from α-‐granules • Decreased TXA2 genera<on • Abnormal platelet cytoskeletal assembly
– Uremic toxins • Uremic platelets mixed with normal plasma func<on normally • Uremic plasma with normal platelets à impaired func<on • Guanidinosuccinic acid and methylguanidine may be poten<al contributors
– Urea does not appear to be – No correla<on with azotemia (BUN) and platelet dysfunc<on
10

Pathophysiology of Renal Disease
• Anemia – Common finding in chronic kidney disease
– Due to decreased produc<on of erythropoie<n
– Rheologic factors play an important role • HCT of 30% à RBCs primarily occupy the center of the vessel • Where platelets are in a skimming layer at the endothelial surface • Close proximity of platelets to the endothelium promotes adherence and platelet plug forma<on
• HCT less than 30% platelets are more dispersed à impaired adherence to the endothelium
– Nitric Oxide • NO synthesis is increased in uremic pa<ents à inhibitor of aggrega<on
• Increased NO synthesis may be due to guanidinosuccinic acid (a uremic toxin)
11

Congenital Disorders of Secondary Hemostasis Factor Deficiency ½ Life
Hours Lab Finding Clinical Finding
I 1. Afibrinogenemia No clot, Prolonged PT, aPTT, TT, No Fibrinogen
Umbilical stump bleeding, easy bruising, ecchymoses, oozing, poor wound healing, hematuria
2. Hypofibrinogenemia Prolonged PT, aPTT, TT, Low Fibrinogen
Mild bleeding
3. Dysfibrinogenemia Normal Fib an<gen with low ac<vity (clot)
Possible hemorrhage/thrombosis Possibly asymptoma<c
II Hypoprothrombinemia 100 Prolonged PT, aPTT Postopera<ve bleeding, epistaxis, menorrhagia, easy bruising
V Parahemophilia 25 Prolonged PT, aPTT, BT Epistaxis, menorrhagia, easy bruising
VII Hypoproconver<nemia 5 Prolonged PT, aPTT Epistaxis, menorrhagia, cerebral hemorrhage
VIII Hemophilia A 8-‐12 Prolonged aPTT, normal PT, BT Mild, moderate, severe
vWF 16-‐24 Variable aPTT and BT, normal PT Mild, moderate, severe
IX Hemophilia B (Christmas Disease) 20 Prolonged aPTT, normal PT Mild, moderate, severe
X Stuart-‐Prower Deficiency 65 Prolonged aPTT, normal PT Menorrhagia, bruising, epistaxis, CNS bleeding
XI (Hemophilia C) 65 Prolonged aPTT, normal PT Mild bleeding, bruising, epistaxis
XII Hageman Trait 60 Prolonged aPTT, normal PT Thrombo<c tendency, NO bleeding
XIII Factor XIII Deficiency 150 Normal aPTT and PT, abnormal 5M Urea Solubility Assay
Umbilical stump bleeding, poor wound healing, excessive fibrinolysis, male sterility, difficulty conceiving, intracranial hemorrhage
PK Prekallikrein (Flecther Factor) 35 Normal aPTT and PT Thrombo<c tendency, NO bleeding
HMWK Fitzgerald Factor 156 Normal aPTT and PT Thrombo<c tendency, NO bleeding 12

The Talmud (2nd century AD) states that male babies do not have to be circumcised if two brothers have died from the procedure In 12th century Albucasis, an Arab physician, wrote about a family in which males died of excessive bleeding from minor injuries In 1803, Dr. John O]o, Philadelphia, wrote about an inherited hemorrhagic disposi<on affec<ng males In 1828 at the University of Zurich, “hemophilia" was first used to describe a bleeding disorder
Bleeding disorders have been recognized since ancient <mes…

Congenital Factor Deficiencies • Most common
– Hemophilia A – deficiency of FVIII – Hemophilia B – deficiency of FIX Occur very early in life
• Characterized: 1. Sow <ssue bleeds 2. Joint bleeds 3. Bleeding into body cavi<es 4. Bleeding into CNS
• Manifest: – Awer minor trauma, surgery, tooth extrac<ons – May be spontaneous
• Physical Exam: – Petechiae, ecchymoses, hematomas, joint deformi<es
• Lab Exam: – CBC including platelet count, PT, aPTT, Fibrinogen, Thrombin Time

Hemophilia • The hemophilias are a group of related bleeding disorders
that most commonly are inherited • “Hemophilia" is used, it most owen refers to the following two
disorders – Factor VIII deficiency (Hemophilia A) – Factor IX deficiency (Hemophilia B à Christmas disease)
• Hemophilia A and B are X-‐linked recessive diseases • They exhibit a range of clinical severity that correlates well
with assayed factor levels

Disorders of Secondary Hemostasis
• Hemophilia A and B – Sex-‐linked recessive disorders first described in the Talmud in the 5th century – By the end of the 19th century the cloZng <mes of plasma from persons with
hemophilia were found to be greatly prolonged compared with the cloZng <mes in nonbleeders
– By 1947 hemophilia was a]ributed to a single protein deficiency – Pavlovsky showed that plasma of some hemophilic pa<ents could correct the in
vitro or in vivo defects of other pa<ents with clinically iden<cal bleeding disorders à led to recogni<on of mulLple types of hemophilia
– Hemophilias A and B together occur in about 1/5,000 of the general popula<on – Hemophilia A is about 4-‐6x more common than Hemophilia B
– Defect in hemophilia is due to a muta<on located on the “X” chromosome • Females can be carriers
– One normal + one defecLve “X” chromosome • Females are asymptoma<c
1. Transmit one abnormal X chromosome to each male offspring 2. Male offspring would have hemophilia
16

Disorders of Secondary Hemostasis
• Hemophilia A and B – Sex-‐linked recessive disorders first described in the Talmud in the 5th century – By the end of the 19th century the cloZng <mes of plasma from persons with
hemophilia were found to be greatly prolonged compared with the cloZng <mes in nonbleeders
– By 1947 hemophilia was a]ributed to a single protein deficiency – Pavlovsky showed that plasma of some hemophilic pa<ents could correct the in
vitro or in vivo defects of other pa<ents with clinically iden<cal bleeding disorders à led to recogni<on of mulLple types of hemophilia
– Hemophilias A and B together occur in about 1/5,000 of the general popula<on – Hemophilia A is about 4-‐6x more common than Hemophilia B
– Defect in hemophilia is due to a muta<on located on the “X” chromosome • Females can be carriers
– One normal + one defecLve “X” chromosome • Females are asymptoma<c
1. Transmit one abnormal X chromosome to each male offspring 2. Male offspring would have hemophilia
17

Hemophilia • Hemophilia A and hemophilia B are clinically idenLcal and must be dis<nguished from
von Willebrand disease – Hemophilia A demonstrates sex-‐linked inheritance
• Muta<on occurs on the FVIII gene located on Xq28
– Hemophilia B (Christmas disease) demonstrates sex-‐linked inheritance • Muta<on occurs on the FIX gene located on Xq27
• Primarily a disease of males—females carry the defec<ve gene (asymptoma3c)
• Hemophilic females are exceedingly rare • Carriers possess ~ 50% factor levels – protec<ve against bleeding – Hemophilic females
1. Doubly heterozygotes – affected inherited from a carrier mother and an affected father
2. Carriers with a defec<ve allele on one X chromosome and the normal allele on the other X chromosome undergoes inacLvaLon (lyoniza3on)
3. Turner’s Syndrome – loss of one X chromosome
18

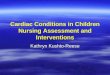
X-‐Linked Recessive Inheritance
Carrier female
Affected male
Normal male
• Affected males (XY): – sons unaffected (no male to male transmission) – daughters obligate carriers
• Carrier female (XX): – ½ sons affected; ½ daughters carriers
• Affected females: very rare.
New muta<on in germ cell
New muta<on in maternal or paternal germ
cell

20
X-‐linked recessive inheritance of hemophilia. Asterisk (*) designates affected chromosome
XX
What’s wrong with this picture?

Thrombin Genera<on in Normal Individuals • Normal individuals
1. Forma<on of TF/VIIa complex following vascular injury 2. Extrinsic pathway ac<va<on of FX via Extrinsic Tenase complex
[TF:FVIIa:PF3:Ca2+] 3. Ini<al burst of thrombin 4. TFPI is released from endothelial cells and down-‐regulates the
[TF:VIIa:FXa] complex à turns off the extrinsic genera<on of thrombin
5. Thrombin generated from the Extrinsic Pathway à thrombin genera<on
6. Thrombin converts FVIII à FVIIIa 7. FVIIIa is a cofactor for the forma<on of the Intrinsic Tenase complex
[VIIIa:IXa:PF3:Ca2+]
8. Intrinsic tenase complex is responsible for con$nued thrombin genera<on

Pathophysiology Hemophilia A • Insufficient genera<on of thrombin by
– FIXa/VIIIa complex through the intrinsic pathway of coagula<on cascade
– Bleeding severity complicated by excessive fibrinolysis 1. IIa cannot feedback to ac<vate VIII à VIIIa—VIII is defec3ve
[Hemophilia A] 2. As a result —VIIIa cannot bind to FIX (FIX is normal but
nonfunc3onal) 3. Due to lack of thrombin ac<va<on of TAFI
– IIa à genera<on of TAFI – In normal TAFI turns OFF fibrinolysis – In hemophilia there is a decrease in TAFI so TAFI cannot turn off fibrinolysis
» Decreased cloZng due to decreased FVIII/FIX » Increase in fibrinolysis

Pathophysiology Hemophilia B
• Insufficient genera<on of thrombin by – FIXa/VIIIa complex through the intrinsic pathway of coagula<on cascade
– Bleeding severity complicated by excessive fibrinolysis 1. IIa feedbacks to ac<vate VIII à VIIIa —FVIIIa serves
as a cofactor to orient FIXa in forming the intrinsic tenase complex
2. As a result —FIX cannot bind form the intrinsic tenase complex to ac3vate FX [FIX is defec3ve] – In hemophilia TAFI cannot turnoff fibrinolysis
» Decreased cloZng due to decreased FVIII/FIX » Increase in fibrinolysis

Hemophilia • Pathophysiology of hemophilia A and hemophilia B is based on
– Insufficient generaLon of thrombin by the FIXa/FVIIIa complex in the intrinsic pathway of the coagula<on cascade – defec3ve intrinsic tenase complex forma3on
24
Hemophilia A
Defec$ve FVIII
Hemophilia B
DefecLve FIX
Intrinsic Tenase Defec$ve
Extrinsic Tenase Normal

Disorders of Secondary Hemostasis
• Clinical Symptoms of Hemophilia A and B – Clinical symptoms are iden$cal 1. Deep muscle hematomas 2. Hemarthroses 3. Intracranial bleeding 4. Delayed bleeding 5. Prolonged oozing awer injuries and tooth extrac<on ??? 6. Superficial ecchymoses
• Hemophilia A and B can be divided into 3 groups
25
Severe cases
ClassificaLon ConcentraLon of factor
Symptoms Age at diagnosis
Mild 6-‐30% (FVIII) 4-‐50% (FIX)
1. Bleeding awer major trauma, surgery, dental extrac<on 2. No spontaneous bleeding seen
Owen in adulthood
Moderate 1-‐5% 1. Muscle and joint bleeding awer minor trauma 2. Excessive bleeding awer minor surgery and dental
extrac<ons 3. Occasional spontaneous bleeding may occur
<5-‐6 yrs
Severe ≤1% 1. Frequent spontaneous bleeding 2. Deep muscle bleeds, hemarthroses, intracranial bleeds 3. Profuse bleeding awer trauma, minor surgery, dental
extrac<ons

Factor VIII Deficiency (An<hemophilic Factor)
• Deficiency of the FVIII:C por<on of the circula<on FVIII:vWF complex – In Hemophilia A—the FVIII component is missing or defec$ve while the vWF
component is normal – In vWD—the vWF component is defecLve while the FVIII component is NORMAL
• FVIII:C may be decreased since vWF is not protec<ng the circula<ng FVIII • Defect in secondary hemostasis à unable to form stable fibrin clot
– Primary hemostasis is normal – Abnormal bleeding is due to delayed fibrin forma<on and results in inadequate fibrin
forma<on • Factor VIII has molecular weight of 330,000 D
– Gene was first characterized in 1980 and located near the <p of the long arm of the X chromosome
– Glycoprotein that par<cipates in the middle phase of the intrinsic pathway – Synthesized in the liver (and endothelium) and secreted into plasma where it
complexes with vWF
26

Structure FVIII • Factor VIII gene is located on the X chromosome – Xq28 • One of the largest known genes • Divided into 26 exons that span 186,000 base pairs • Synthesized as a single chain polypep<de of 2351 amino acids • A 19-‐amino acid signal pep<de is cleaved by a protease shortly awer synthesis so
that circula<ng plasma factor VIII is a heterodimer • FVIII circulates in plasma in a noncovalent complex with von Willebrand factor

• The func<ons of factor VIII reflect binding at specific sites within the molecule
• Factor VIII consists of – A heavy chain with A1 and A2 domains
• A2 domain is a site of factor IXa binding, the ac<ve enzyme in the X-‐ase pathway
– A connec3ng region with a B domain • Connec<ng region that separates
the second and the third A domains but is not required for cloZng ac<vity
– A light chain with A3, C1, and C2 domains
• C2 domain binds to the procoagulant phospholipid phospha<dylserine on ac<vated platelets and endothelial cells and to von Willebrand factor
www.tankonyvtar.hu/hu/tartalom/tamop425/0011_1A_Molekularis_te

FVIII Deficiency • Most muta<ons occur in intron 22
1. Most defects are point muta<ons 2. Dele<ons and nonsense muta<ons lead to truncated molecules of FVIII – High frequency of intron 22 inversions may relate in part to the flexibility
of the telomeric end of the long arm of the X chromosome—called flip-‐Lp mutaLon
– Intron 22 inversions are responsible for ~43% of severe hemophilia A cases
29

Clinical Manifesta<ons • Hallmark of hemophilia is hemorrhage into the joints
– Resul<ng in • Permanent deformi<es
– Painful and lead to long-‐term inflamma<on and deteriora<on of the joint 1. Misalignment 2. Loss of mobility 3. Extremi<es of unequal lengths
– Intracranial hemorrhage – Hemorrhage into sow <ssue around vital areas
• Pathophysiology – Bleeding probably starts from synovial vessels into the synovial space – Reabsorp<on of blood is owen incomplete à chronic prolifera<ve synovi<s à
thickening of the snynovium crea<ng a “target joint” with recurrence of bleeding – Destruc<on of surrounding structures and bone necrosis with cyst formaLon and
osteophytes

Clinical manifesta<ons Intracranial hemorrhage
• Leading cause of death of hemophiliacs
• Spontaneous or following trauma
• May be subdural, epidural or intracerebral
• Suspect always in hemophilic pa<ent that presents with unusual headache
• If suspected-‐ FIRST TREAT, then pursue diagnos<c workup
• LP only when fVIII has been replaced to more than 50%

Clinical manifesta<ons Pseudotumors
• Dangerous and rare complica<on
• Blood filled cysts that are gradually expanding
• Occur in sow <ssues or bones. • Most commonly in the thigh • As they increase in size they
erode con<guous structures. • May require radical surgeries
or amputa<on, and surgery is owen complicated with infec<on
A pseudotumor is deforming the cortex of the femur (arrow). Other ossified masses in the sow <ssues (arrowheads) are probably sow-‐<ssue pseudotumors.

• Queen Victoria was a carrier – Queen of England (1837-‐1901) – Spontaneous muta3on
• Her father (Duke of Kent) was not affected
• Her mother did not have any affected children from the previous marriage
• Leopold (her 8th child) had hemophilia – Died brain hemorrhage (age 31) – Had children – Alice (carrier)
• Beatrice (QV youngest child) had 2 hemophilic sons and a daughter (Victoria Eugene) who was a carrier)
– Victoria Eugene introduced hemophilia into the Spanish royal family by marrying king Alfonso XIII
• Alexandra (QV granddaughter) married Nicholas – Tsar of Russia
– Alexandra was a carrier – her 1st son Alexei had hemophilia
• Raspu<n (monk) used hypnosis to relieve Alexei’s pain

Complica<ons of Treatment
• Inhibitors/an<body development – Defini<on
• IgG an<body to infused factor VIII or IX concentrates, which occurs awer exposure to the extraneous VIII or IX protein
– Prevalence • 20-‐30% of pa<ents with severe hemophilia A • 1-‐4% of pa<ents with severe hemophilia B
• Hepa<<s A • Hepa<<s B • Hepa<<s C
• HIV

Inhibitors • Inhibitors are alloan<bodies directed against a specific factor –
neutralizing the effect of replacement therapy • Directed against specific epitopes on the factor VIII molecule • FVIII Inhibitors
• Usually IgG – IgG4 subclass • Occur in ~30-‐40% of pa<ents with large dele3ons or missense muta3ons • Lead to severe deficiency of FVIII • Overall occurrence in all types of FVIII deficiencies is ~20%
• Low Responders – < 5-‐10 BU – Titers do NOT increase in response to exposure to FVIII
• High Responders – > 10 BU – Titers increase with exposure to FVIII
• FIX Inhibitors – Less common – occurring in ~3% of cases
Dived these into
two grou
ps

Inhibitors
• Inhibitors are iden<fied by performing mixing study – Corrects in the immediate and prolongs in the incubated • FVIII inhibitors are IgG – warm-‐reac<ng an<bodies – $me dependent
• FIX inhibitors are IgG – usually immediate-‐ac<ng inhibitors
– Bethesda Assay is used to determine the amount of inhibitor present

Acquired Hemophilia • Rare, poten<ally life-‐threatening bleeding disorder • Development of autoan<bodies directed against FVIII –spontaneous autoimmune
disorder – FIX autoan<bodies are less common – Alloan<bodies in congenital hemophilia – Autoan<bodies in acquired hemophilia
• Type II kine<cs – complex – Ini<al rapid inac<va<on followed by a slower inac<va<on curve and resul<ng in some level of residual FVIII
• Associated with: – Idiophathic, pregnancy, autoimmune disorders – Inflammatory bowel disease, ulcera<ve coli<s – Rheumatoid arthri<s, systemic lupus mul<ple sclerosis, Graves disease,
Sjogren syndrome – Drugs – Some hematologic malignancies

Treatment of Hemophilia • Replacement therapy
– Plasma • FFP – did not raise FVIII levels too high, many suffered volume overload, pa<ents spent a lot of <me in hospital
• Before 1985 all plasma derived products were highly contaminated by blood borne virus such as HIV, HBV and HCV à not so much not due to screening of donors and viral inac<va<on techniques such as pasteuriza<on, solvent detergent treatment and ultrafiltra<on
• Some theore<cal concern about non lipid coated parvovirus, HAV and prion disease such as Creutzfeld-‐Jakob

Treatment of Hemophilia • Cryoprecipitate
– Contains high levels of FVIII, Fibrinogen, vWF, and FXIII – 1 unit of FFP prepared by cryoprecipitate contains 50-‐120 U of VIII
• Plasma derived FVIII using monoclonal an<bodies
• Recombinant FVIII • First genera<on – hamster cell culture – contains albumin for stabiliza<on – possible source of viral contamina<on
• Second Genera<on – mutated FVIII lacking the B domain (no role in cloZng) – stabilized by sucrose (albumin-‐free)
• Porcine FVIII

Treatment of Hemophilia • Replacement of missing cloZng protein
– On demand – Prophylaxis
• Prophylac<c transfusions must be started at age 2 to 3 – Need central access, risk of bacteriemia, costly
– Humate-‐P, Alphanate, Mononine • DDAVP / S<mate – release of vWF and FVIII
• An<fibrinoly<c Agents – Amicar
• Suppor<ve measures – Icing, immobiliza<on, rest
• Prophylac<c transfusions must be started at age 2 to 3 – Need central access, risk of bacteremia, costly

Hemophilia is an ideal disease for gene therapy: • caused by a single malfunc<oning gene • just small increase in factor level will provide great benefit: raising factor by 2% will prevent spontaneous hemorrhages into joints, brain and other organs; levels greater than 20% to 30% will prevent bleeding in most injuries

Recombinant FactorVIII: Inser<on of human factor VIII DNA into vector system allowing incorpora<on into non-‐human mammalian cell
lines for con<nued propaga<on

Financial & Insurance Issues• > 70% of cloZng factor distribu<on is by for-‐profit companies average cost/yr for human plasma derived or recombinant factor is $50,000 -‐ $100,000
• Prophylaxis requires about 150,000 units/yr for a 65-‐pound child cos<ng $85,000 per year
• Prophylaxis is covered by insurance on a case-‐by-‐case basis.

Summary Hemophilia A and B
Hemophilia A -‐ (Classic Hemophilia) Hemophilia B -‐ (Christmas Disease)
Factor Deficiency Factor VIII Factor IX
Inheritance X-‐linked recessive X-‐linked recessive
Gene 1. FVIII gene on X chromosome –cloned 1984
2. Large gene—187kb, 26 exons 3. 98% of pa<ents have muta<on – on locus
Xq28, 48% of individuals with severe have inversion of intron 22
1. FIX gene on X chromosome – cloned 1982
2. 34 kb, 8 exons 3. 99% of muta<ons – on Xq27.1-‐q27.2
Incidence 1/10,000 males 1/50,000 males
Severity Related to Factor Level
1. Severe = <1% ac<vity Bleeding awer major trauma, major surgery, dental extrac<on; no spontaneous bleeding seen, owen seen in early infancy (<1 year)
2. Moderately Severe = 1-‐5% ac<vity
Muscle and joint bleeding awer minor, trauma; excessive bleeding awer minor, surgery and dental extrac<ons; occasional spontaneous bleeding occurs, owen seen <5-‐6 years of age
3. Mild = 6-‐30% ac<vity Bleeding awer major trauma, major surgery, dental extrac<on; no spontaneous bleeding seen, owen seen only in adulthood
Complica<ons • Sow <ssue bleed, Intramuscular bleed, Hemarthrosis, Urinary tract bleeding, CNS (major life threatening bleed) 44

Lab Diagnosis in Hemophilia A and B
• Laboratory Diagnosis
1. Why do hemophiliacs bleed? 2. Delayed bleeding (secondary hemosta<c defects) 3. Rapid bleeding (primary hemosta<c defects 4. Oozing
45
Hemophilia A Hemophilia B
PT Normal Normal
aPTT 1. Prolonged 2. May be normal in mild cases
1. Prolonged 2. May be normal in mild cases
Platelet Ct Normal Normal
PFA/BT Normal Normal
Mixing Study 1. Corrects immediately and awer incuba<on
2. Time-‐dependent inhibitor
1. Corrects immediately and awer incuba<on
2. Immediate-‐ac3ng inhibitor
vWF Normal Normal
FVIII Decreased FIX Decreased
How do these differ?

Factor XI Deficiency
• Hemophilia C –– (Plasma Thromboplas<n Antecedent) • Also called Rosenthal Syndrome (described in 1953)
• Autosomal dominant or recessive à occurs in males and females – 2 common muta<ons (one nonsense, one missense) – Allele frequency as high as 10%, 0.1-‐0.3% homozygous – Most affected pa<ents compound heterozygotes with low but
measurable levels of XI ac<vity
– Different from hemophilias A and B which are sex-‐liked
• Rare in the general popula<on 1 in million – More common in the Ashkenazi Jewish popula<on 1 in 450
• In vivo FXI is ac<vated by thrombin • in vitro FXI is ac<vated by XIIa
• aPTT is abnormal with normal PT, FIX levels are decreased
46

Factor XI Deficiency
• 50% of pa<ents with FXI deficiency bleed and 50% do not bleed – Bleeding is associated with <ssues high in fibrinoly<c ac<vity – Variable, generally mild bleeding tendency
• Bleeding awer trauma & surgery • Spontaneous bleeding uncommon • Bleeding risk does not correlate well with XI level
• Mucous membranes, oral cavity • FXI is a nega3ve regula<on of TAFI – this may explain why a deficiency leads to bleeding in some pa<ents
• Treatment • FFP, cryoprecipitate, FXI concentrates, and an<fibrinoly<c agents
47

Congenital Deficiency of the Contact Factors
• FXII Deficiency – Markedly prolonged aPTT – Pa<ents do NOT exhibit a bleeding tendency – Pa<ents have thrombo<c tendency
• Due to a defect in contact ac<va<on of the fibrinoly<c system – requires FXII and PK
• Tendency to develop thromboemboli par<cularly following trauma or surgery
• Prekallikrein Deficiency (Fletcher Trait) – Prolonged aPTT – Pa<ents do NOT exhibit a bleeding tendency – Pa<ents have a thrombo<c tendency – Defect in contact ac<va<on of the fibrinoly<c system requiring PK – Prolonged aPTT will normalize by increasing the incuba$on $me
• High Molecular Weight Kininogen (Fitzgerald Factor) – Markedly prolonged aPTT – Pa<ents do NOT exhibit a bleeding tendency – Pa<ents have thrombo<c tendency
• Due to a defect in contact ac<va<on of the fibrinoly<c system – requires FXII and PK

FXIII Deficiency • FXIII is a tetrameric zymogen that is
converted into an ac<ve transglutaminase by thrombin and Ca2+ in the terminal phase of the cloZng cascade
• Hallmarks of FXIII deficiency 1. Umbilical stump bleeding in
neonatal period 2. Intracranial hemorrhage with li]le
or no trauma 3. Recurrent sow <ssue hemorrhage 4. Recurrent spontaneous abor<on 5. Impaired wound healing and
spontaneous abor<on
• Bleeding – Usually associated with trauma – Bleeding at <me of surgery is not
excessive • Delayed bleeding can occur

Inherited factor XIII deficiency • Autosomal recessive, rare (consanguineous parents) • Heterozygous woman may have higher incidence of spontaneous abor<on • Most have absent or defec<ve A subunit
• F XIII ac<vity < 1% (1-‐2% is adequate for hemostasis) – Bleeding begins in infancy (umbilical cord) – Poor wound healing – Intracranial hemorrhage – Oligospermia, infer<lity
• Diagnosis: – Urea solubility test – Quan<ta<ve measurement of XIII ac<vity – Rule out acquired deficiency due to autoan<body
• F XIII concentrates available (long half life, can administer every 4-‐6 weeks as prophylaxis)

Clinical Testing for Factor XIII
Urea Clot Solubility Test • Qualita<ve assay • Pa<ent sample is clo]ed and then clot is placed in 5 M urea for 24 hours at
room temperature – Clots formed by normal individuals remain stable – Clots from factor XIII deficient pa<ents dissolve
• Detects only the most severely affected homozygous pa<ents with 1% to 2% factor XIII ac<vity or less
• Urea solubility assay • Factor XIII forms covalent cross links between fibrin chains • In the absence of Factor XIII à the fibrin clot will be dissolved by 5 M urea which disrupts the hydrogen bonds
• This assay will be abnormal only if the factor XIII level is <2-‐5%

FXIII Deficiency • Laboratory results
– Normal PT, APTT, TT, BT despite history of bleeding – Solubility of fibrin clots in 5 M urea or 1% monochloroace<c acid – Minimal ac<vity (2-‐5%) needed to maintain hemostasis – Therapy if needed
• FFP, cryoprecipitate, FXIII concentrates are available in Europe • Acquired factor XIII deficiency
– Autoan<body-‐mediated • Very rare • Most pa<ents elderly • May be drug-‐induced (isoniazid, other an<bio<cs) • Bleeding may be severe • Diagnosis:
– Urea solubility – F XIII ac<vity – Mixing study?

Factor Assays
• Principle – Ability of the pa<ent’s plasma to correct a prolonged PT or APTT of a known factor
deficient plasma – Normal ac<vity range is 50-‐150% or 50% factor ac<vity
• Determines type of factor deficiency and ac<vity • Targets either
– PT: Factors VII, X,V, III and II – APTT: Factors XII, XI,IX and VIII
• Methodology – Factor deficient plasmas are used that contain 100% of all factors except the one in
ques<on – 1:10, 1:20, 1:40 dilu<ons are made, 1:10 is considered 100% – A control to compare results to, normal plasma (containing 100% of all factors) is added
to the commercially prepared factor deficient plasma in the same way – Pa<ent sample and control are compared to a standard curve where the cloZng <mes
have been established using known concentra<on

FIGURE 40-4 Factor activity curve. The factor activity curve is prepared by plotting the clotting time in seconds for each reference plasma dilution on the y-axis and the percent factor activity for each dilution on the x-axis. (Reprinted, with permission, from Brown BA. Hematology: Principles and Procedures, 6th ed. Philadelphia: Lea & Febiger; 1993.)

Coagulation Screening Test Results in Congenital Deficiencies
McKenzie









![[LECTURE] Coagulation and Flocculation](https://img.pdfslide.net/doc/110x75/577d2b6f1a28ab4e1eaac2f2/lecture-coagulation-and-flocculation.jpg)