Embed Size (px)
Citation preview
https://youtu.be/8A9xuLmUHcQPeter Gøtzsche
CEBM Oxford. Publicado 3 de junio 2014
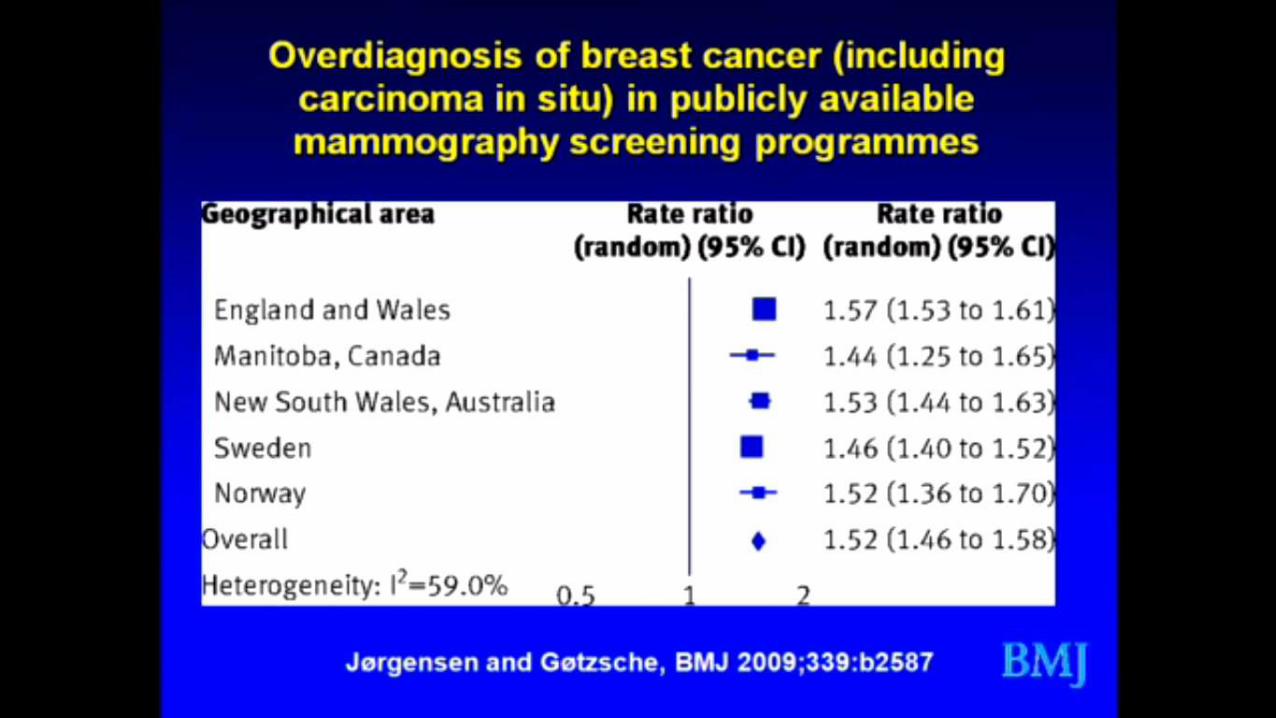
• Esta revisión sistemática encuentra hasta un 50% de sobrediagnóstico.
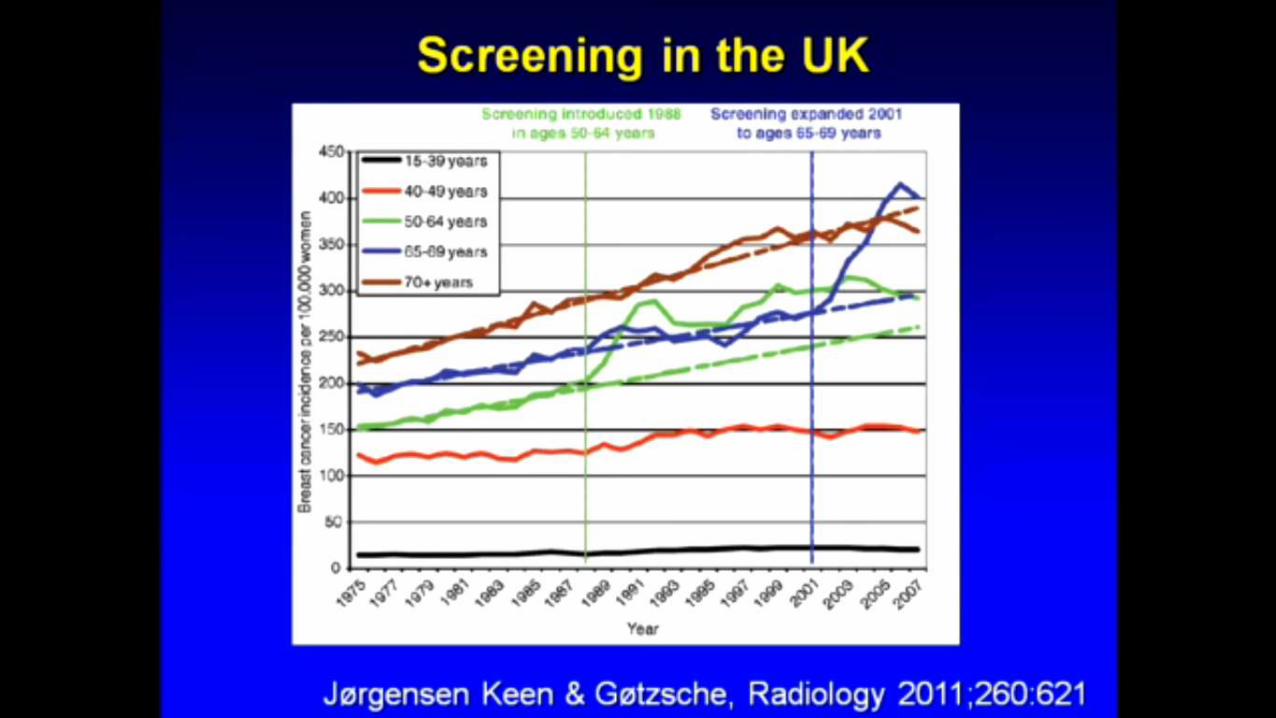
• Cuando comenzó el screening en UK en 1988, la incidencia en el grupo de edad de 50 a 64 se elevó bastante y se mantuvo alta (ver curva verde).
• Cuando se inicia en la franja de edad 65 a 69 en el 2001, igualmente ocurre ese fenómeno (curva azul). Lo mas asombroso es que este grupo de edad ya había sido sometido a screening; ¿Por qué entonces toda este incremento en la incidencia luego de iniciar screening?
Esto solamente puede explicarse por el hecho de diagnosticar cáncer poco agresivo (overdiagnosis)
Peter Gøtzsche
• La mayor parte de los canceres detectados por screening tienen un comportamiento clínico bien diferente (mild) a los tumores de mama que se diagnostican por la aparición de síntomas.
Screening detected VS Clinical detected
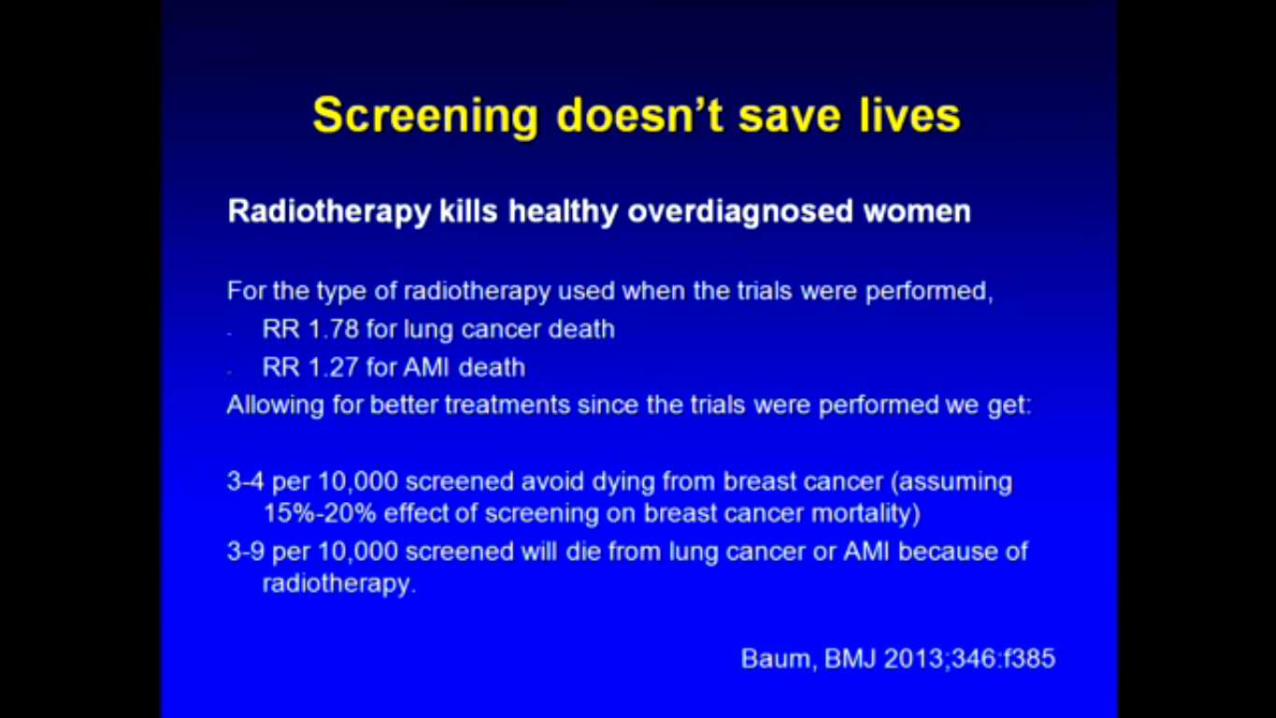
Harms from breast cancer screening outweigh benefits if death caused by treatment is includedMichael Baum professor emeritus of surgery, Divisionhttp://sci-hub.cc/10.1136/bmj.f385
Each new intake of medical students to my surgical “firm”
started off with a tutorial where I posed a rhetorical question:
“Why do we screen for cancer?” To which the inevitable answer
would be, “To catch it early, sir.” Wrong. The question should
be reframed, as “Does screening for cancer improve length or
quality of life?” All other outcomes are surrogates.
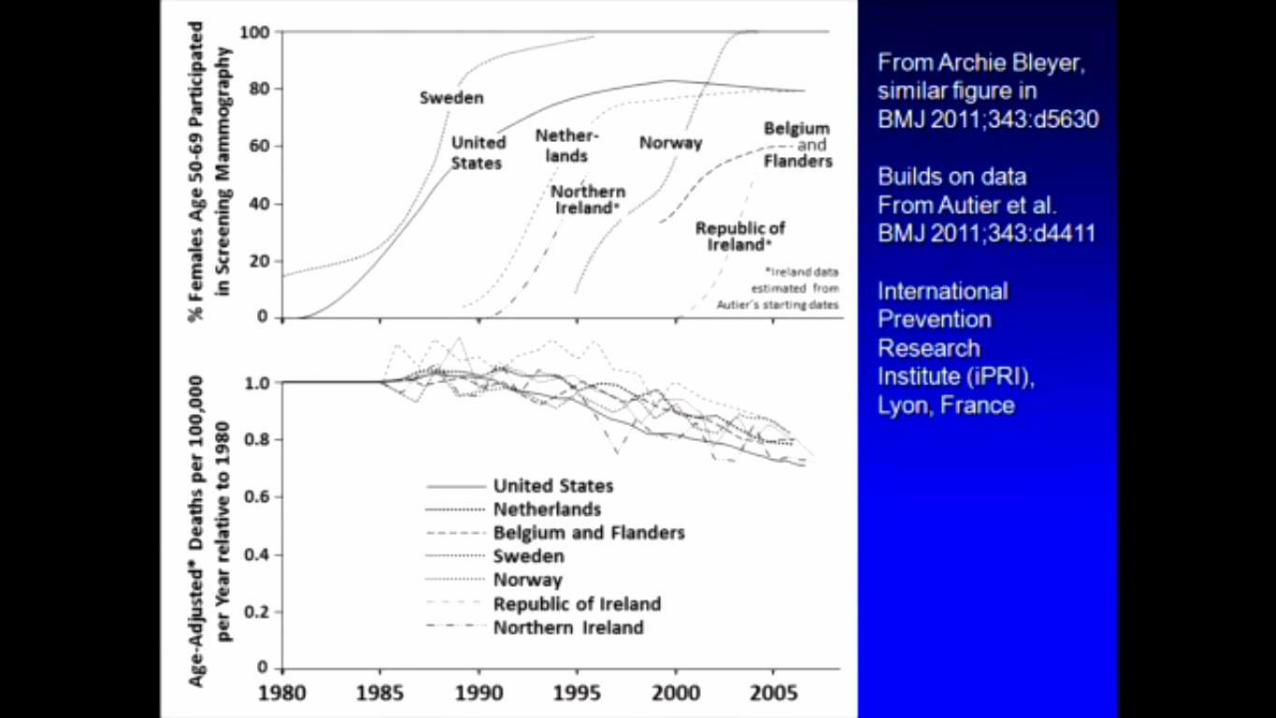
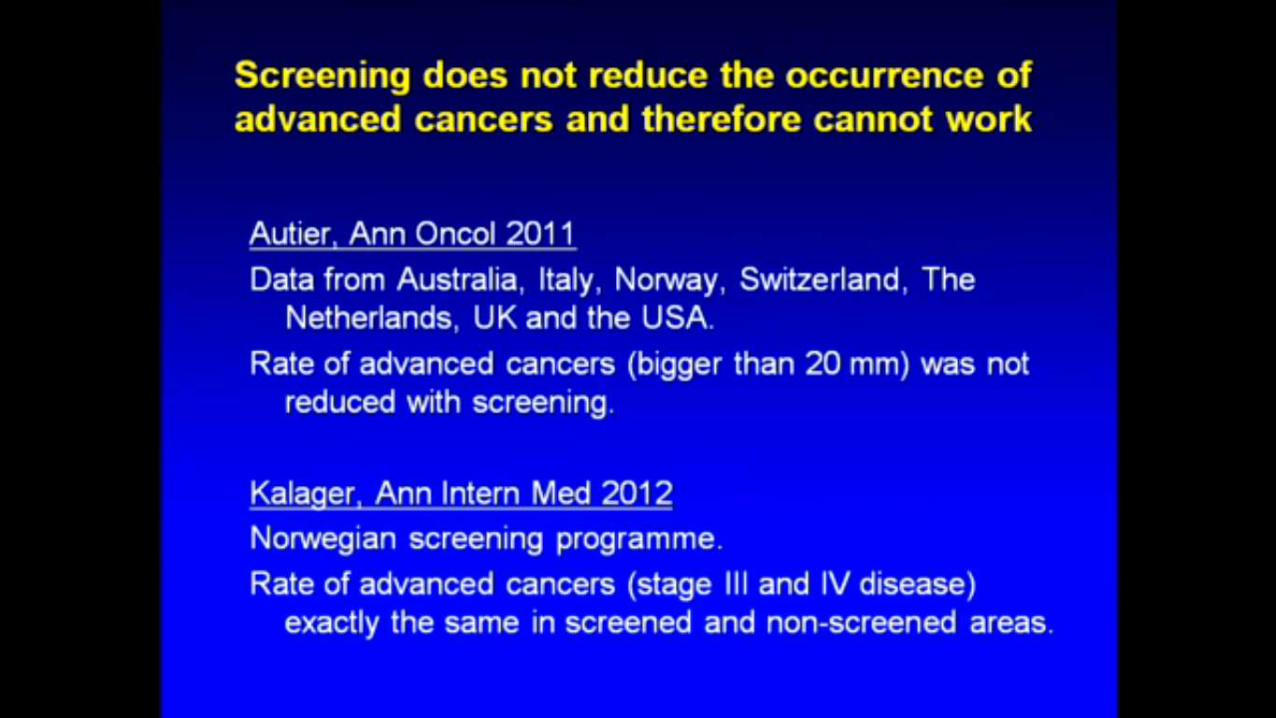
Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality databasePhilippe Autier https://sci-hub.cc/10.1136/bmj.d4411
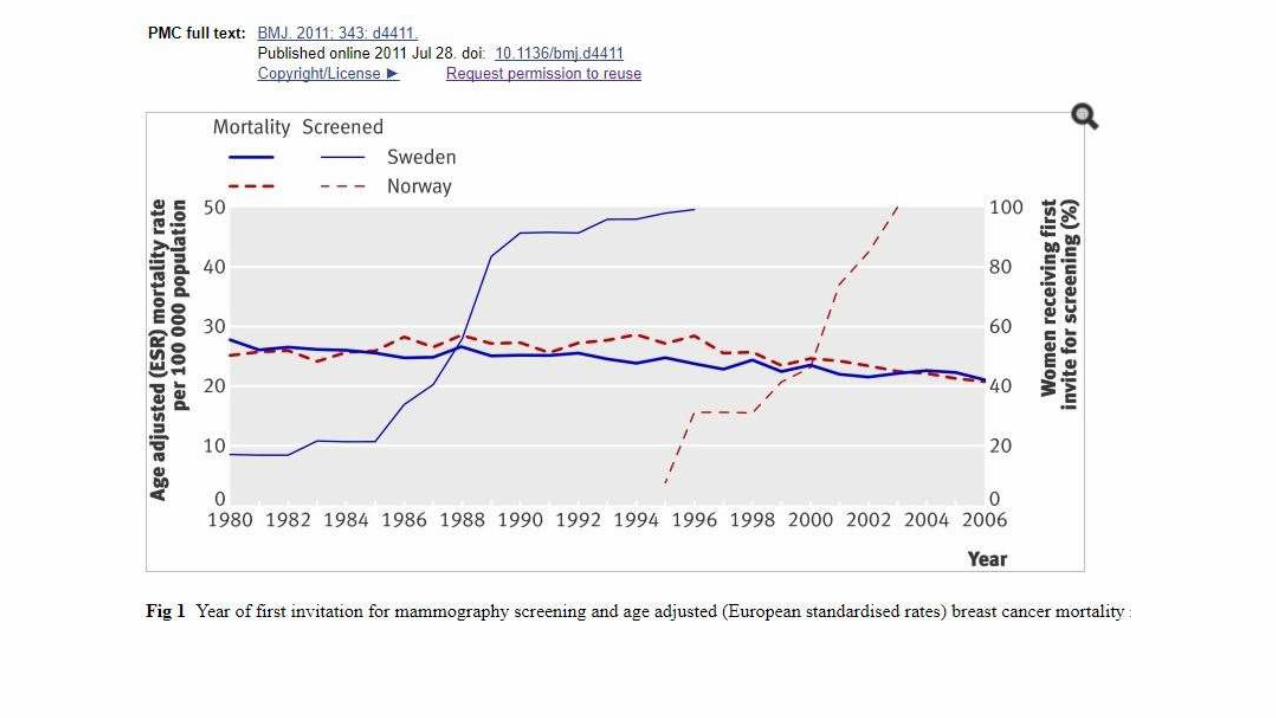
Results Sweden and Norway The national organised mammography screening programmein Sweden was implemented from 1986 onwards after a pilot study and the results ofclinical trials carried out in the country in the 1970s and 1980s (table 1).10 In 1990 about90% of Swedish women had received a first invitation. Nationwide coverage was attainedin 1997 (fig 1). All women aged 50-69 are invited, but in most counties (60-70%) womenaged 40-49 are also invited.11 In half the counties women aged 70-74 are invited.Attendance for screening in Sweden has been consistently among the highest recorded inany country.12 Non-organised screening is uncommon.
The Norwegian organised mammography screening programme was initiated in 1996 as apilot project in four counties, which include 40% of Norway’s population (Akershus,Hordaland, Oslo, Rogaland).13 14 Since then organised screening has been graduallyimplemented, with all women aged 50-69 invited every two years. By 2005 the programmehad reached nationwide coverage. For the implementation of nationwide screening thetime difference between Sweden and Norway was about 12 years. Non-organisedscreening was uncommon after implementation of the nationwide programme. From 1989to 2006, breast cancer mortality decreased by 16.0% in Sweden and by 24.1% in Norway(table 2 and fig 1).
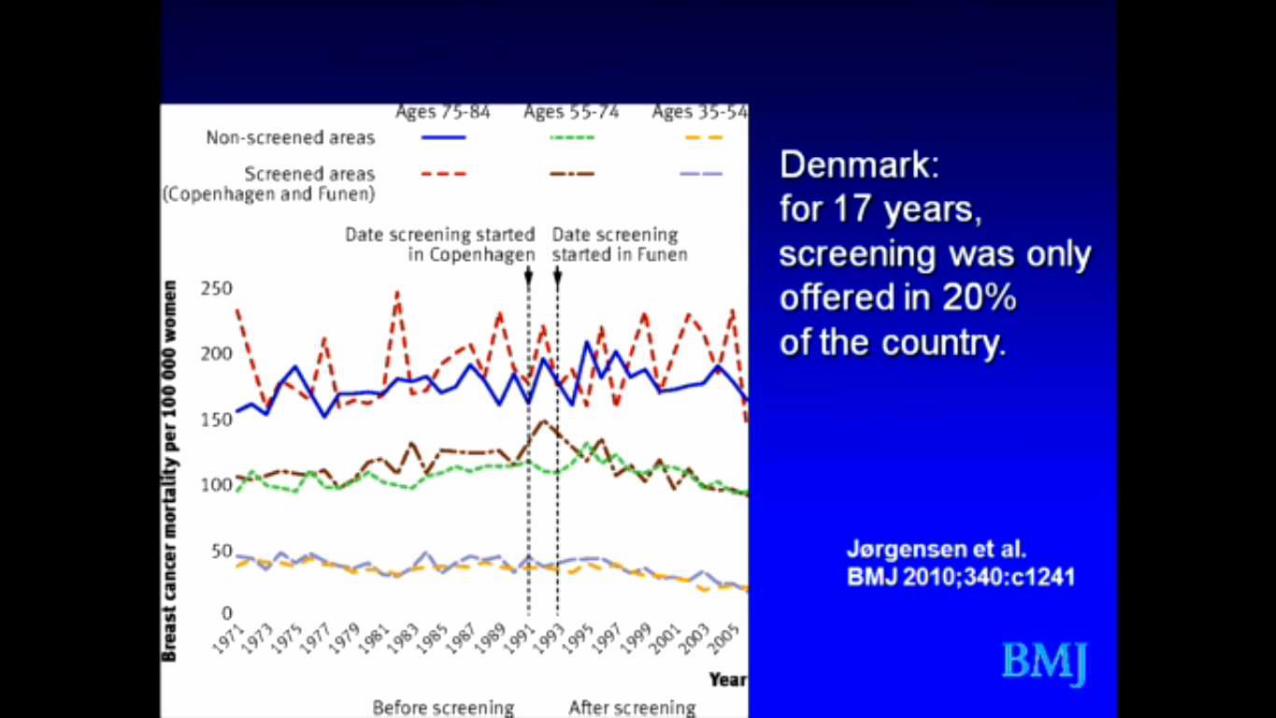
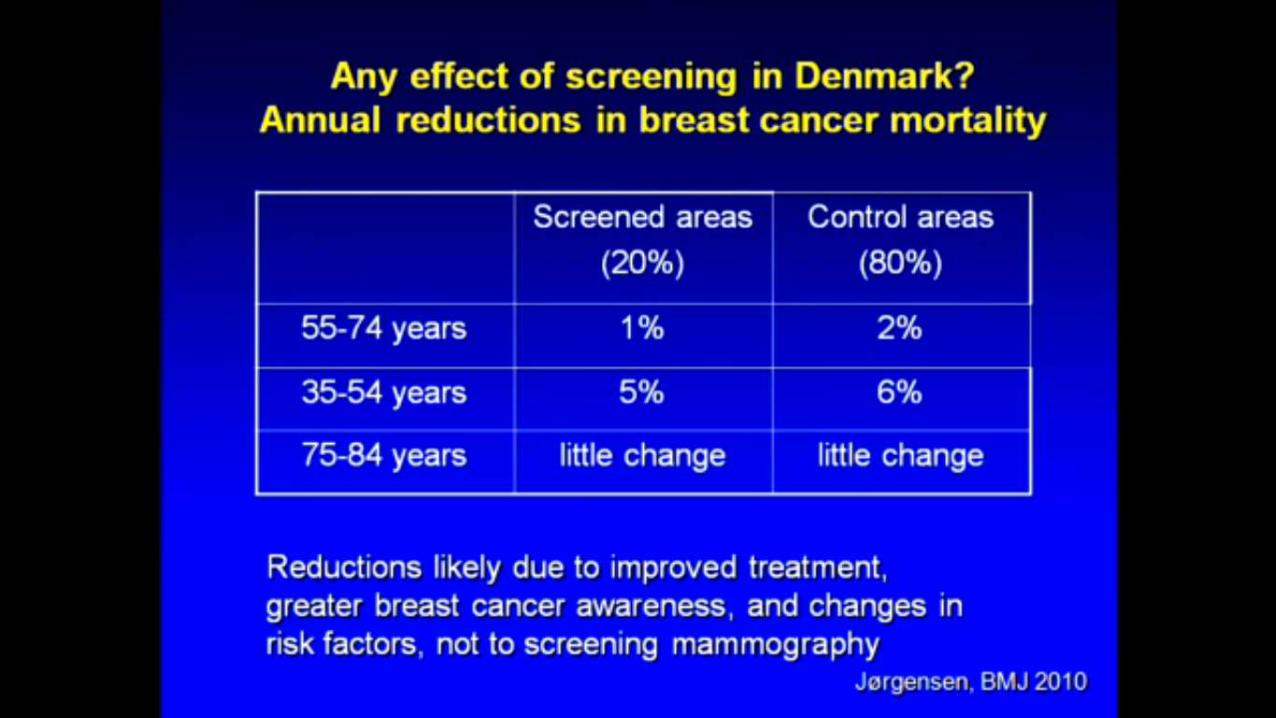
¿Y la mortalidad?
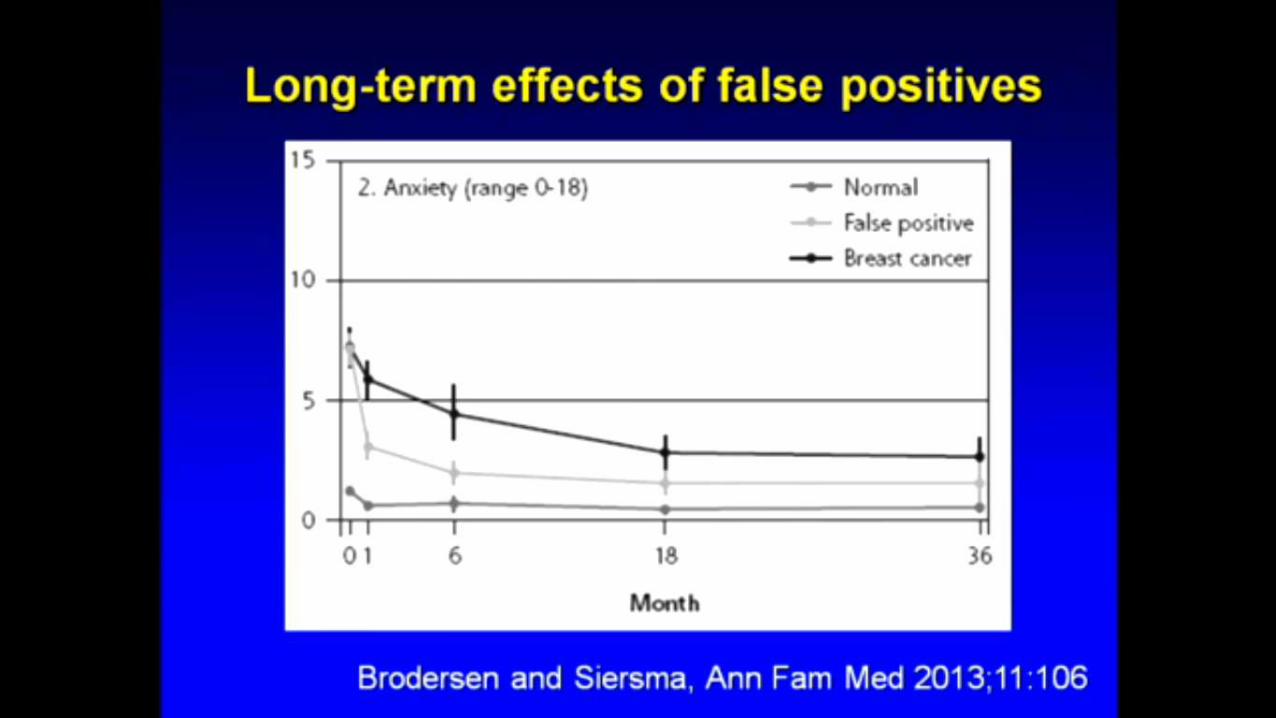
Efectos adversos insospechados del screening
Dos grandes mentiras
El screening salva vidas
El screening salva mamas
Ninguna de las dos respuestas es cierta
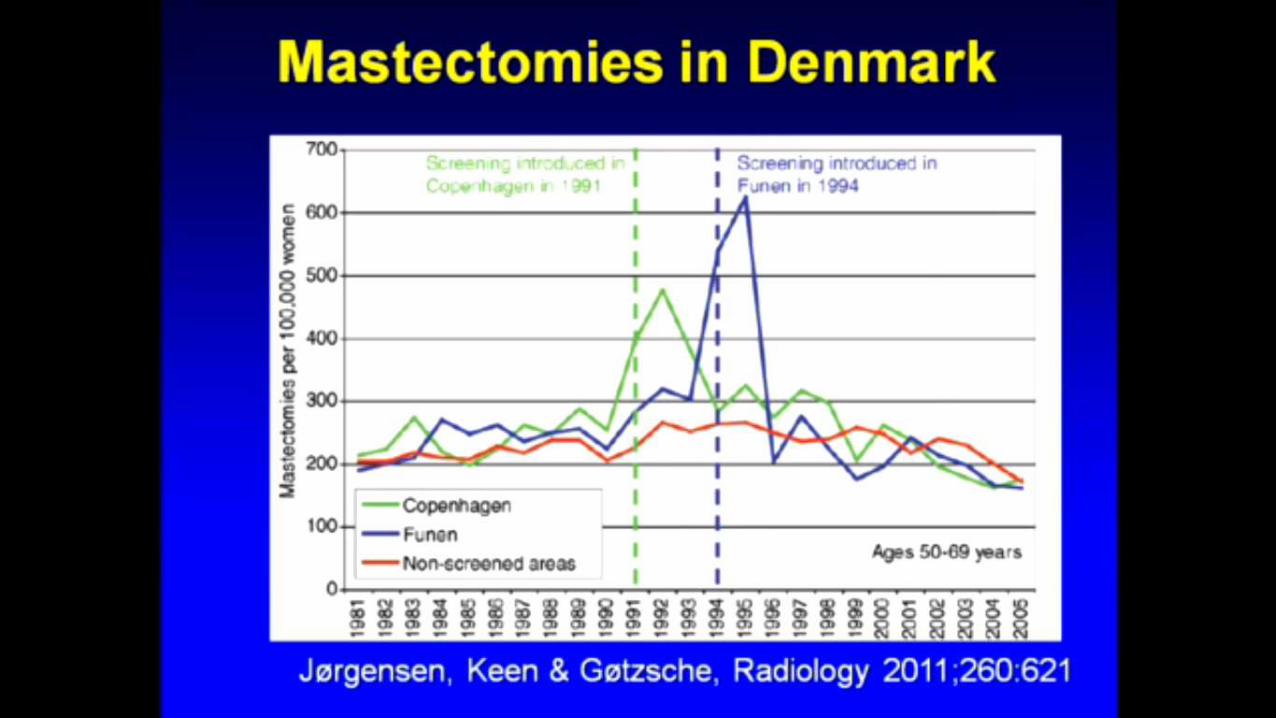
Pueden verse dos enormes picos en el número de mastectomías realizadas tras a la introducción del screening en Dinamarca
Hay una forma de reducir la incidencia del cancer de mama• Mantenerse alejada del screening
¿Por qué toda esta red de volutariostraduciendo este documento?• Porque incluso en sus países la información sobre los programas de
screening esta sesgada y es deshonesta.
¿Qué país tendrá las agallas políticas para detener el cribado mamográfico?• Espero que sea mi país, Dinamarca