Embed Size (px)
DESCRIPTION
National Chronic Care Software Infrastructure
Citation preview

The Vision of an Affordable National Health Information Infrastructure (NHII) Larry Suarez Grid Research Group Agent Net, Inc.
Abstract
The decentralized and fragmented nature of health care delivery in the U.S. creates islands of information and services. The U.S. health care system is unable to neither access or manage these islands of information nor integrate services across institutional boundaries. Compounding the problem is the rapid advancement of medical science and technology which is contributing large quantities of isolated information which has a direct impact on care processes and patient safety. The lack of readily available medical information and services for the treatment of chronic diseases has contributed each year to a large number of deaths in the U.S. as a result of inappropriate care, adverse drug reactions, and missed diagnosis. Supporting advance care processes like those for chronic diseases takes more than just integrating information. Chronic care processes require the ability to create virtual teams consisting of care providers, care institutions, laboratories, nutritionists, educational media, and even food providers. Most medical-care organizations and private physicians cannot afford to build or purchase integrated information systems sophisticated enough to support chronic care. Grid technology coupled with autonomous agents (agent grids) is crucial to engendering a commitment
within the medical industry to build an affordable, national health information infrastructure for chronic care. An infrastructure that will improve health care in the U.S. by providing the right information and services at the right time to care providers with the overall goal of reducing hospital admissions and emergency room visits for patients with chronic diseases.
Introduction
The medical industry continues to struggle with access to distributed information including patient details, medical encounters, prescription usage, and medical research data. Physician groups, hospitals, and other health care organizations operate as silos, often providing care without the benefit of complete information about the patient’s condition, medical history, services provided in other settings, or medications prescribed by other clinicians. The problem is compounded in chronic care situations where multiple care providers participate in the treatment of a patient. The lack of access to condensed and pertinent research data means that scientific knowledge about best care is not applied systematically or quickly to clinical practice. An average of about 17 years is required for new knowledge generated by randomized controlled trials to be incorporated into practice, and even then application is highly uneven.
Improving health care comes down to improving access to information and services.

The Chronic Care Medical Grid 2
Agent Net, Inc. 3/2/2010
Access must be at the national level for the following reasons:
1. Diffuses the cost to individual care providers.
2. Provides quality care services to low-income, poorly funded programs that cannot support fully-staffed chronic care service organizations.
3. Care providers are geographically dispersed including different states.
4. Medical research information such as randomized clinical trials is dispersed throughout the U.S.
5. Lawmakers, patient advocacy groups, and regulatory bodies are requiring care providers to provide data on a national level as to their decision processes, care processes, and their abilities to respond to patient requirements and preferences.
6. Major disease issues, outbreaks, drug reactions, and other issues affecting patient safety require an immediate response at the national level.
Most medical-care organizations and private physicians throughout the U.S. do not have the resources to build information systems to support chronic care. Kaiser Permanente spent an estimated $1.5 billion to $2 billion to implement their information system which provides automated medical records and guidance including support for chronic care. The Internet is a prime example of bringing resources to those who could not previously afford it allowing small businesses to compete with large businesses. Within the medical arena, the Internet will also provide a ―leveling‖ effect in the support of chronic care which ultimately benefits all patients in the U.S. including those under the care of Kaiser Permanente.
Chronic Care
The health care situation will not improve in the next ten years. Chronic conditions (heart decease, cancer, diabetes) are the leading cause of illness, disability, and death in the U.S. This will be compounded by an aging population. Approximately 75 percent of direct medical expenses in the U.S. are devoted to chronic illness. Aetna Insurance spends 65 percent of their medical-care dollars on just 16 percent of their total membership who have late-stage chronic illness. By 2030, roughly two of every three people in the U.S. will have one chronic condition as a result of the aging U.S. population.
Chronic care requires demanding care processes. Processes for chronic conditions involve:
Multidisciplinary (distributed) care teams that must be coordinated.
Multiple institutions including hospitals, nursing homes, and special care facilities.
The participation of medical specialists in consultative and educational roles outside conventional referrals.
Patient self-management which requires monitoring and patient-provider feedback.

The Chronic Care Medical Grid 3
Agent Net, Inc. 3/2/2010
Continual monitoring of newly available drugs, applicable clinical research, and advancements in care processes.
Information access to hospitals, clinics, laboratories, suppliers, and payers.
Evidence-based care processes that must be continually evaluated.
Non-medical support like travel to and from appointments, food deliveries, and health status information to family and love ones.
Chronic care management has been increasingly relegated to disease management companies because of the inability of primary care providers to absorb the time, cost, and expertise to handle chronic disease patients. Minimizing costs, a primary goal of service companies, is questionable in the long term. Primary care providers are the first line of support for chronic disease patients and must have the necessary tools and support to deliver quality care without patients having to go to specialized care companies.
Chronic care must be seamless — supporting the ability of interdependent people and technologies to perform as a unified whole, especially at points of transition between and among caregivers, across sites of care, and through time. Safety failures occur during transition points. Information should not be lost, inaccessible, or forgotten in transitions. Knowledge about patients, such as their allergies, their medications, their diagnostic and treatment plans, and their specific needs, must be available with appropriate assurances of confidentiality to all who need to know it regardless of where and when they become involved in the process of giving care.
The National Health Information Infrastructure
The National Health Information Infrastructure (NHII) was first proposed in 1996 by the National Committee on Vital and Health Statistics in the U.S. Department of Health and Human Services. The NHII is defined as a ―set of technologies, standards, and applications that support communication and information". The NHII, as envisioned by Agent Net, is an integration of nation-wide chronic care information and services coupled with new services to create virtual care teams. The NHII is not a single-site Application Service Provider (ASP). It is a collection of information and services distributed throughout the U.S. It takes the best parts of solutions already in place in organizations like Kaiser Permanente and Evercare/United Healthcare. It uses services brought on-line by organizations willing to contribute to the NHII. The NHII is a nation-wide collective effort to reconstruct the U.S. Healthcare system to function as a ―system‖. The NHII provides one face to U.S. health care. As organizations contribute to the NHII, the NHII improves by providing better services resulting in increased patient safety. The NHII will be based on grid technology with the addition of autonomous agents. Both technologies are standards-based with supported open-source software toolkits.
Grid Technology
Grids are defined as the hardware and software that is concerned with the integration, virtualization, and management of services within distributed, heterogeneous, dynamic ―virtual organizations‖. Next-generation software systems will involve data from numerous distributed data sources and services provided by numerous distributed

The Chronic Care Medical Grid 4
Agent Net, Inc. 3/2/2010
vendors. Researchers and practitioners in the grid arena have tried to construct standards to ensure that participants can communicate and collaborate across a network. Researchers have also defined basic services that are required to keep the grid accessible including naming services (global identification of services), security services, replication services, and data access services.
Grids can be divided into three main areas:
Resource or Computational Grids –grids which allow users to access physical
resources across a wide network such as CPUs, disk storage, and servers.
Data Grids –grids which allow users to access data distributed throughout the
network in fast and secure ways.
Service Grids – grids which make software services available to users including
advance imaging algorithms, patient authorization, and patient adjudication services.
New solutions in the grid arena are blurring the boundaries between the different types of grids. For example, a medical grid that provides access to imaging data would require data (the images themselves), computation resources to search large data sets of images quickly, and services that provide the advance algorithms necessary to infer information from the images. It is now evident that new grid solutions will need enough sophistication to provide resources, information, and services.
Grid solutions offer the necessary components to effect collaboration across a network including standard interfaces and standard object naming. Recent efforts by organizations like the Open Grid Services Architecture (OGSA) have proposed standards for grid construction. OGSA builds on existing grid and Web services technologies.
Medical Grids
Grid technology remains the only valid hope in solving the problems associated with health care: the access and assimilation of distributed information and services. Health care problems will continue until information and service access is solved. The medical arena has already seen the appearance of a number of grids although primarily in the research arena where collaborative studies require the integration of imaging, clinical, and laboratory data. The initial grids within the medical industry began with multi-institutional collaborative clinical biomedical research studies carried out by virtual organizations. Studies required the pooling and support of distributed analysis of epidemiological, clinical, laboratory, imaging, tissue and molecular information.
Existing medical grids include the Biomedical Informatics Research Network, the Shared Pathology Informatics Network, BioGrid, and the Cooperative Human Tissue Network. These grids are targeting shared access to medical data in a wide area environment. However, these projects focus on development of middleware and infrastructure support for specific application domains. We argue that the medical community can leverage more generic grid-based systems in many of the same ways in which other scientific applications have been using them.

The Chronic Care Medical Grid 5
Agent Net, Inc. 3/2/2010
Agent-Based Grids
Grids will provide the connectivity of medical entities and basic services such as security. However, we argue that to create an effective national infrastructure for the care of chronic diseases there needs to be more than just connectivity. Grid initiatives have also included minimal non-connectivity solutions with the inclusion of workflow and rule systems. Workflows and rule systems allow the automation of static procedures like simple care processes. But that is still not enough to construct effective grids for chronic care.
In order to provide more advance ―collaboration‖ solutions, autonomous agents were introduced to grid technology. Grids containing autonomous agents were known as agent-based grids or agent grids. The computing industry has long seen the need for autonomous agents in grid solutions. Organizations like the Foundation for Physical Agents (FIPA) and DARPA’s Control of Agent-Based Systems (CoABS) have been researching the application of autonomous agents to grids. There are numerous international workshops and conferences on autonomous agent grids and thousands of research papers on the subject.
Autonomous agents provide a number of attractive attributes because of their dynamic nature. This is a step beyond a ―static‖ approach using web services or care-management software. Those attributes include:
Autonomous – agents are designed to function without human intervention which
is necessary when thousands of agents exist on the grid.
Self-Healing – agents have the ability to self-heal. When an agent functions
incorrectly according to its internal policy, the agent can add or remove internal behavior to heal itself. This is known as autonomic computing.
Cooperative – agents can collaborate and form virtual teams. This is a major
requirement for solutions in the medical industry.
Dynamic – agent behavior can be manipulated in real-time. Behaviors can be
added to agents either from an outside source (physicians) or two agents can augment each others behaviors. Agent populations can be increased or decreased in real-time. For example, to support new sources of information or to reflect new care pathways that should be integrated into existing pathways.
Workflow – agents can form ―chains‖ to accomplish a goal (for example, a
chronic care pathway). These chains are fluid and can form or change without user intervention based on a policy or goal.
Agent grids will provide features not found in standards grids but are required for chronic care:
Ability to track and monitor the progress of our national mandate to improve health care and patient safety. This includes being able to catch errors in real-time.
Ability to manage automatically and without human intervention (known as autonomic computing) the grid infrastructure to ensure maximum availability

The Chronic Care Medical Grid 6
Agent Net, Inc. 3/2/2010
especially in support of medical emergencies.
Formation of ―agent communities‖ representing patients and clinicians with shared interests to improve care, share results, and share data.
Formation of ―virtual teams‖ that represent all providers and clinicians contributing to the care of a particular patient. The virtual team shares information, events (episodes), and evidence-based data.
Formation of ―virtual teams‖ that represent providers, hospitals, institutions to better their practices and reduce costs.
Tracking patient care with the interest of rewarding providers who have improved their care processes to ensure patient safety, effectiveness, and efficiency.
Test bed (application, monitoring, and feedback) for implementing new experimental efforts in care processes, payment policies, and evidence application.
Tracking of medical outcomes to help contribute to better care pathways.
Critical Issues and Agent-Based Grids
There are a number of critical issues that are currently being addressed to support the National Information Infrastructure:
Security – includes user authorization for access to medical grids.
Quality of Service (QoS) – ensures that requests via the National grid return
information within specified constraints including time and cost.
Privacy – well known issues of moving sensitive data across unprotected
networks.
Policy Application – data providers/owners may have organizational policies
which dictate how information or services are shared on the grid. Those policies may include access control rules, time restrictions, patient consent, usage fees, and data content restrictions.
Regulatory Compliance – issues dealing with government (local, state, federal)
requirements and regulations.
Patient Diversity – supporting the differences between patient culture, religious
background, language, and beliefs.
Solutions to the above issues include patient identification hiding, date masking (hospital admittance, date of birth, etc.), encryption, adding erroneous data noise (invalid information mixed with valid information), and lock-box technology. The system must be able to guarantee, both at the data supplier and data provider, security requirements.
Agents within the Medical Grid will act as pre-filters and pre-processors of information at the source to ensure security requirements, large data sets, locality of services, or data

The Chronic Care Medical Grid 7
Agent Net, Inc. 3/2/2010
volume.
Agents will be used to provide the data provider with the insurances that the operations on their patient data are restricted to all legal and contractual obligations.
Agents can subsume patient attributes including their religious beliefs in medicine, language, and colloquial meanings.
Grid solutions have to protect personal data against accidental or unlawful destruction or accidental loss, alteration, unauthorized disclosure or access, in particular when the processing involves the transmission of data over a network, and against all other unlawful forms of processing. With regard to the state of the art and the cost of their implementation, such measures have to ensure a level of security appropriate to the risks represented by the processing and the nature of the data to be protected. Consequently, the more sensitive the data is the more risky the processing will be. As personal data related to health are very sensitive, the security level of the data processing has to be at maximum.
The Chronic Care Medical Grid
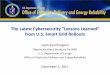
The Chronic Care Medical Grid is an OGSA-compliant medical agent-based grid. The Chronic Care Medical Grid is considered to be just one grid composing the eventual NHII. Agent Net, Inc. has been researching grids and agent grids for ten years. With the advent of numerous grid solutions in medical research and the acceptance of grid standards via standard bodies, the time is right for Agent Net, Inc. to introduce agent grids as the starting point of the NHII. Figure 1 shows a diagram of the components of the Medical Grid.
Figure 1: Chronic Care Medical Grid. Part of the NHII.
The Chronic Care Medical Grid can be used in localized settings or across the Internet.
Internet
NHII (Grid Software)
Autonomous Agents
Chronic Care Medical Services
Computing Resources

The Chronic Care Medical Grid 8
Agent Net, Inc. 3/2/2010
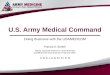
There are a number of services required on the grid for chronic care. Figure 2 shows a number of services in the Grid architecture which include:
National Registry – used to identify and track patients including medical
information.
Registry Agents – allows registries across the U.S. to combine information to
create a nation-wide view of chronic conditions and to ensure proper care as a patient moves through multiple care providers and institutions.
Monitoring Device Agents – provides connections to home monitoring devices.
Media Agents – provides access to media and knowledge information for
patients.
HIPPA Agents – agents whose task is to ensure that Health Insurance Portability and Accountability (HIPPA) requirements are followed by grid participants.
Survey Agents – agents who provide disease-specific surveys for patient
feedback both at the national level and the virtual team level.
Service Agents - connections to food services, airlines, transportation.
Information Agents (secure, policy-based) – provides connections to information
sources including hospital records, clinic records, physician records.
Care Provider Agents – agents representing patients, physicians, pharmacists,
dietitians, laboratories, nurses, and other care providers. These agents can form ―societies‖ or ―virtual teams‖ to provide a team approach to medicine.
Agent-Based Workflow – workflows representing care pathways, emergency
response pathways, and other complex and fluid processes.

The Chronic Care Medical Grid 9
Agent Net, Inc. 3/2/2010
Figure 2: Medical Grid Architecture

























![[Industry report] U.S. Grid Automation Report](https://img.pdfslide.net/doc/110x75/55d5141bbb61eb8a6b8b4570/industry-report-us-grid-automation-report.jpg)