Embed Size (px)
Citation preview

I N N O V A T I O N A N D E X C E L L E N C E I N T E L E H E A L T HI N N O V A T I O N A N D E X C E L L E N C E I N T E L E H E A L T H
A Population Based Model for Telehealthwww.telemedcare.co.uk

What is Telehealth ?
SOURCE: Digital Home Health – A PrimerA Parks Associated White Paper, 2006
The use of electronic information and telecommunications technologies to support long-distance clinical health care, patient and professional related education , public health and health administration
SOURCE: Telemedicine Report to Congress, 2001

What’s driving growth in Telehealth?
Unprecedented growth rates of the aged population
Increasing morbidity as population ages placing unsustainable stress on established health care services
Increasing deficits in clinical HR
Expanding disease management programs
Patient demand for self-management

Culling illegal no Voodoo principal delaying maybe Transfer of costs yes
Transfer to the patient Transfer from hospital into the community Transfer from human resources to IT resources (Historically health
spending on IT was LESS than 4%)
CAUSES OF RESISTANCE TO TECHNOLOGY
Culture that clinical services has to be totally human interactive False
Technology cannot provide clinical support False
People don’t want to manage their health to become expert patients False
In the minds of the Government?

Current Model of Home Based Telehealth?
HIGH CARE
LOW CARE
DIS
EA
SE
MA
NA
GEM
EN
T
DIS
EA
SE
PR
EV
EN
TIO
NLEVEL 3: Frequent users of hospital services
£££££££££
LEVEL 2/1: Less frequent users of hospital services
£££
n = 10
n = 100

Challenges of Implementing Telehealth
Case management of frail elderly people introduced an additional range of services into primary care without an associated reduction in hospital admissions*.
Current findings from WSD also reported that the process of implementing Telehealth and telecare technologies for people with long-term conditions had thrown up a number of ‘unexpected’ challenges:
The administrative energy and time required to gain clinical and professional leadership and input was essential, but had been underestimated. However, most professional staff once exposed to the technology were supportive of its use.
Not all individuals and/or their families and carers welcomed Telehealth/telecare in their homes with many claiming they were either well enough not to require the service or simply did not want to be reminded about their condition on a daily basis.
Those consenting to be part of the trial often dropped out at different stages of the process, even at installation.
Integrating data sharing between multiple organisations took time to establish and required the development of sharing agreements
*Impact of case management (Evercare) on frail elderly patients: controlled before and after analysis of quantitative outcome data, Hugh Gravelle, professor of economics, Mark Dusheiko, research fellow, Rod Sheaff, professor of health services research, Penny Sargent, research associate, Ruth Boaden, professor of service operations management, Susan Pickard, research fellow, Stuart Parker, professor of health care for older people, and Martin Roland, director

What’s the Solution?
Level 3
Self Care Solution: Graphical display of data Spirometry, ECG, Video conferencing (bb) Health education (bb) Fingerprint ID Medication reminders
Early Intervention Solution: BP, HR, Weight, SOP2 and temp, Questionnaires Messaging Web Access Health Diary Multiple users
Level 1/2
Data Solution: BP, HR, Weight, & SOP2, Wireless/mobile Multiple users
Level 1

Designing a Telehealth Solution
What features matter?
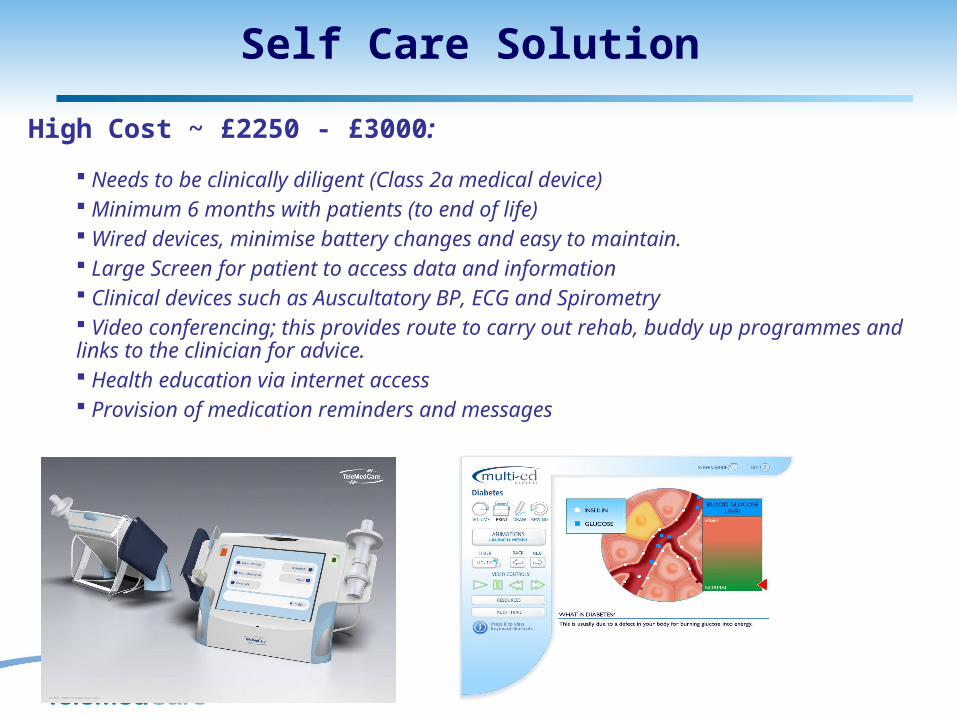
Self Care Solution
High Cost ~ £2250 - £3000:
Needs to be clinically diligent (Class 2a medical device) Minimum 6 months with patients (to end of life) Wired devices, minimise battery changes and easy to maintain. Large Screen for patient to access data and information Clinical devices such as Auscultatory BP, ECG and Spirometry Video conferencing; this provides route to carry out rehab, buddy up programmes and links to the clinician for advice. Health education via internet access Provision of medication reminders and messages

Intervention Solution
Medium Cost ~ £1200-£1800:
Needs to be clinically diligent (Class 2a medical device) Minimum 2 months with patients (to end of life) Wired devices, minimise battery changes and easy to maintain. Biofeedback and large screen for patient to ensure good quality of data Reminders for patients to do testing. Multiple people can use system with finger print ID Questionnaires and medical scripts FREE internet access (keeps patient interested) Intelligent Alerts, decision support system part of the clinician web portal

Data Solution
Low Cost ~ £300 -£800:
Minimum 2 weeks to 3 months with patients Wireless devices – plug and play. No screen required Has to be cheap solution! No training or installation Flexible w.r.t. to devices (don’t need all peripherals when only one will do) Flexible wr.t. O.S. – can use via mobile phones Open solution; link with telecare devices such as fall monitors Solution is more relevant to clinician (early discharge)

Deploying Telehealth ServicesIssues to Consider?

Interoperability

Monitoring Centre
The Telehealth monitoring system is only part of the Telehealth service
If the data is not monitored and appropriate clinical decisions not taken the service will fail its clients
Studies have shown that Telehealth can create 70% more work for clinicians Monitoring centre can take some of the burden and admin work load.
Risk stratify and alert clinicians to patients with real needs Provide real time support; video conferencing (if required)
Provide the base for installation and maintenance of Telehealth systems A centre for infection control Provide local support for persons with local needs.

UK Case Study
TeleMedCare’s unique clinical solutions have been deployed in Norfolk to monitor patients at home, whose vital signs measurements would otherwise have been taken by community nurses.
Currently community nurses visit a patient with chronic disease an average of 3 times per week at a cost of £65 per visit
In Norfolk TeleMedCare has reduced these clinical nurse visits to 1 visit per month
Average savings per patient £9.2k per annum
There are approximately 1.2m patients with chronic disease receiving nurse visits
TeleMedCare have been shown to reduce hospital admissions of frequent users of hospital services (level 3) by 70%.
One example of a COPD patient with complex needs reduced her admissions by over 100 days compared to her previous year. Saving of £30K (at £300 per day cost)
Norfolk developed strategy for deployment of a sustainable population based model. Telehealth will also be used in Nursing Homes and Pharmacies.
Other Authorities have already been drawn to the Norfolk model as a leader in delivering a telehealth solution

Key Messages
Take a “population health” approach to determine the requirements for that community
Undertake risk stratification of potential clients By severity of symptoms and quality of life By likely clinical outcomes By frequency of admission to hospital
THEN select optimal blend of Telehealth technologies to achieve; Best patient healthcare outcome Best cost benefit
ONE product (..and cost!) does not fit all – it costs more to keep the “frequent flyer” out of hospital but the cost benefits can be much larger!
To Conclude
The alphabet of care is changing- Reactive to Proactive- Responsive to Preventative
Telehealth will have a significant impact on LTC for the elderly
Telehealth providers need to ensure their products/services are safe, accurate, and reliable
Date needs to be interoperable and easy to access (securely)
Telehealth technology has to be easily adopted into the integrated clinical care team via a POPULATION BASED MODEL.

Saneth Wijayaratna
Telemedcare UK Ltd United House Carlton BoulevardLincolnLN2 4WJUK
Tel: +44 (0)1522 563023Fax: +44 (0)1522 563024
Website: www.telemedcare.co.ukEmail: [email protected]
Telemedcare is a member organization of:
Contact
Telemedcare Australia Pty Ltd ABN 65 050 042 192Unit 7, 6-8 Crewe PlaceRosebery, NSW, 2018 Australia
Tel: +61 (0) 2 9313 8136Fax: +61 (0) 2 9313 8564





























