Embed Size (px)
DESCRIPTION
Anesthesia problems for Laparoscopic surgeries
Citation preview

11
AnesthesiaAnesthesia management of management of Laparoscopic Assisted Laparoscopic Assisted
Surgery.Surgery.
Dr. Mohammed MahdyDr. Mohammed Mahdy
Consultant in Consultant in AnaesthesiologyAnaesthesiology
Al Bukariya general Al Bukariya general hospitalhospital

22
IntroductionIntroduction
Laparoscopy introduced in 20Laparoscopy introduced in 20thth CenturyCentury
1962 : first laparoscopic tubal 1962 : first laparoscopic tubal ligation ligation
1970 -- 80 : used for gyne 1970 -- 80 : used for gyne proceduresprocedures
1989: laparoscopic 1989: laparoscopic cholecystectomycholecystectomy
Rapid advances in technologyRapid advances in technology

33
Lap.chole - 948 Lap.append - 150
Lap.hernia - 80 Lap.ob/gyn - 60
Varicocele -10 Int. obst - 9
Lap.gastric banding -2 Gastric bandoplasty - 1
Total No of cases from 3 / 1421 to 11 / 1425
75.2%
11.9%
6.3%4.7%
Total cases: 1260

44
Laparoscopic ProceduresLaparoscopic ProceduresGeneral Surgery:General Surgery:
CholecystectomyCholecystectomyAppendicectomyAppendicectomyVaricocoelectomyVaricocoelectomyHernioplastyHernioplastyDiagnostic laparoscopyDiagnostic laparoscopyHiatus hernia repairHiatus hernia repairAdhesiolysisAdhesiolysis
OBG:OBG:Ectopic pregnancyEctopic pregnancyMyomectomyMyomectomyLAVHLAVHEndometriosisEndometriosis
Thoracic Surgery:Thoracic Surgery:SympathectomySympathectomyMediastinoscopyMediastinoscopy

55
Advantages of LaparoscopyAdvantages of Laparoscopy
Shorter hospital stayShorter hospital stay Faster recoveryFaster recovery Rapid return to normal activitiesRapid return to normal activities Minimal painMinimal pain Small scarSmall scar Less post-op ileusLess post-op ileus

66
Contraindications for Contraindications for LaparoscopyLaparoscopy
Increased ICPIncreased ICP
V – P shuntV – P shunt
HypovolemiaHypovolemia
CCF CCF
Valvular heart diseasesValvular heart diseases

77
Anaesthetic PlanAnaesthetic Plan Pre-operative assessmentPre-operative assessment Pre-medicationPre-medication
• AnxiolyticsAnxiolytics• H2 receptor blockersH2 receptor blockers• Gastro-kinetic drugsGastro-kinetic drugs
Monitoring:Monitoring:• Pulse oximetryPulse oximetry• CapnographyCapnography• ECGECG• NIBPNIBP
• FiO2FiO2

88
Anaesthetic ManagementAnaesthetic Management
PreoxygenationPreoxygenation InductionInduction Intubation – mandatoryIntubation – mandatory NG tube placementNG tube placement
• Stomach decompressionStomach decompression Maintenance of anaesthesiaMaintenance of anaesthesia
• Muscle relaxantsMuscle relaxants• Volatile anaesthetic agentsVolatile anaesthetic agents
Reversal of NM blockadeReversal of NM blockade Recovery roomRecovery room

99
Anesthetic Problems of Anesthetic Problems of LaparoscopyLaparoscopy
Due to pneumo peritoneumDue to pneumo peritoneum Due to patient positioningDue to patient positioning Cardiovascular effectsCardiovascular effects Respiratory effectsRespiratory effects Gastro intestinal effectsGastro intestinal effects Unsuspected viseral injuriesUnsuspected viseral injuries Difficulty in estimating blood lossDifficulty in estimating blood loss Darkness in the ORDarkness in the OR

1010
Pneumo PeritoniumPneumo Peritonium
Preferred gas : CO2 Preferred gas : CO2
Working pressure : 12 to 14 mm Working pressure : 12 to 14 mm HgHg
Slow inflation of 1 litre / minuteSlow inflation of 1 litre / minute

1111
CO2 as Insufflator GasCO2 as Insufflator Gas
More soluble in blood than airMore soluble in blood than air
Carriage is high due to Carriage is high due to bicarbonate buffering and bicarbonate buffering and combination with Hbcombination with Hb
Rapidly eliminated by lungsRapidly eliminated by lungs
Inert & not irritant to tissuesInert & not irritant to tissues

1212
Ventilatory problems during Ventilatory problems during LaparoscopyLaparoscopy
Increase in PaCO2Increase in PaCO2
PneumothoraxPneumothorax
Gas-embolismGas-embolism

1313
Causes for Increased PaCO2Causes for Increased PaCO2
Absorption of PaCO2 –peritoneal Absorption of PaCO2 –peritoneal cavitycavity
V/Q mismatchV/Q mismatch• Increased physiological dead Increased physiological dead
spacespace•Abdominal distentionAbdominal distention•Patient’s positionPatient’s position•Controlled ventilationControlled ventilation•Reduced cardiac outputReduced cardiac output
Lighter planes of anaesthesiaLighter planes of anaesthesia

1414
PneumothoraxPneumothorax
Patent pleuro-peritoneal Patent pleuro-peritoneal channelschannels
Pleural injuriesPleural injuries
Ruptured emphysematous Ruptured emphysematous bullaebullae

1515
Management of PneumothoraxManagement of PneumothoraxRecommended GuidelinesRecommended Guidelines
Stop N2OStop N2O Adjust vent settings to correct Adjust vent settings to correct
hypoxemiahypoxemia Apply PEEPApply PEEP Reduce intra-abdominal Reduce intra-abdominal
pressurepressure Communicate with surgeonCommunicate with surgeon Avoid thoracocentesisAvoid thoracocentesis

1616
Gas EmbolismGas Embolism
Most feared & fatal complicationMost feared & fatal complication
Seen frequently when Seen frequently when laparoscopy is associated with laparoscopy is associated with hysteroscopyhysteroscopy
Intra vascular injection of gas Intra vascular injection of gas following direct trocar placement following direct trocar placement into vesselinto vessel

1717
Suspicion of Gas EmbolismSuspicion of Gas Embolism
Blood on aspiration from Vere’s Blood on aspiration from Vere’s needleneedle
Pulsation of flow meter pressure Pulsation of flow meter pressure gaugegauge
Disappearance of abdominal Disappearance of abdominal distention despite sufficient distention despite sufficient volume of gasvolume of gas

1818
Effects of Massive Air EmbolismEffects of Massive Air Embolism Rapid insufflation of gas into bloodRapid insufflation of gas into blood Gas lock in RA & venacavaGas lock in RA & venacava Fall in cardiac outputFall in cardiac output High pressure in RAHigh pressure in RA Open foramen ovaleOpen foramen ovale Embolus in cerebral & coronary bedsEmbolus in cerebral & coronary beds Paradoxical embolismParadoxical embolism

1919
Diagnosis of Gas-embolismDiagnosis of Gas-embolism Detection of gas in right side of HeartDetection of gas in right side of Heart Recognition of physiological changes Recognition of physiological changes
secondary to emboli:secondary to emboli:• TachycardiaTachycardia• Cardiac arrhythmiaCardiac arrhythmia• HypotensionHypotension• CVP riseCVP rise• Mill-wheel murmurMill-wheel murmur• CyanosisCyanosis• Right heart strain pattern in ECGRight heart strain pattern in ECG• Pulmonary edemaPulmonary edema
Doppler & TEE ---- very sensitiveDoppler & TEE ---- very sensitive

2020
Treatment of Gas EmbolismTreatment of Gas Embolism
Immediate cessation of Immediate cessation of insufflationinsufflation
Release of pneumo-peritoneumRelease of pneumo-peritoneum Patient in Durrent’s positionPatient in Durrent’s position Cessation of N2O Cessation of N2O Give 100% oxygenGive 100% oxygen CVP insertion and aspiration of CVP insertion and aspiration of
gasgas

2121
Risk factor for RegurgitationRisk factor for Regurgitation
Increased intra-abdominal Increased intra-abdominal pressurepressure
Decreased lower oesophageal Decreased lower oesophageal sphincter tonesphincter tone
Head down positionHead down position
NG tube mandatoryNG tube mandatory

2222

2323
Cardiac Arrhythmias during Cardiac Arrhythmias during LaparoscopyLaparoscopy
Volatile anaesthetic agents Volatile anaesthetic agents
HypercarbiaHypercarbia
Sudden stretching of peritoneumSudden stretching of peritoneum
Electro coagulation of fallopian Electro coagulation of fallopian tubestubes
Light planes of anaesthesiaLight planes of anaesthesia

2424
Problems related to patient’s Problems related to patient’s positioningpositioning
Head – Down tilt for pelvic and Head – Down tilt for pelvic and sub sub meso-colic surgerymeso-colic surgery
Head -Up tilt for supra Head -Up tilt for supra mesocolic surgerymesocolic surgery
Lithotomy position for gynec Lithotomy position for gynec proceduresprocedures

2525
Position – Respiratory EffectsPosition – Respiratory Effects
Head-down positionHead-down position• Promotes atelectasisPromotes atelectasis• Decreases FRCDecreases FRC• Decreases TLCDecreases TLC• Decreases pulmonary complianceDecreases pulmonary compliance
Head-Up position:Head-Up position:• Endo-bronchial intubationEndo-bronchial intubation

2626
Position- Cardio-Vascular EffectsPosition- Cardio-Vascular Effects Head down Position:Head down Position:
• Increases CVPIncreases CVP• Increases cardiac outputIncreases cardiac output• Increases cerebral circulationIncreases cerebral circulation
Increased ICPIncreased ICP Increased intra-ocular pressureIncreased intra-ocular pressure
Head up Position:Head up Position:•Decreased cardiac outputDecreased cardiac output•Decreased mean arterial Decreased mean arterial
pressurepressure•Decreased venous returnDecreased venous return

2727
Positions : Nerve InjuryPositions : Nerve Injury
Hyper extension of armHyper extension of arm --- --- brachial plexus injurybrachial plexus injury
Lithotomy positionLithotomy position --- --- common common peroneal injuryperoneal injury

2828
Bibilography:Bibilography:
Short practice of anaesthesia – Short practice of anaesthesia – Churchill DavidsonChurchill Davidson
Synopsis of anaesthesia – Synopsis of anaesthesia – Atkinson & LeeAtkinson & Lee
Text book of anaesthesia – Text book of anaesthesia – Ronald MillerRonald Miller
Anaesthesia & coexisting Anaesthesia & coexisting diseases - Stoeltingdiseases - Stoelting

2929

3030
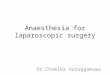
Haemodynamic Repurcussions Haemodynamic Repurcussions of Pneumo - Peritoneumof Pneumo - Peritoneum
↑ ↑ Intraabdominal pressureIntraabdominal pressure
↓ ↓ Venous returnVenous return ↑↑ Intrathoracic pressureIntrathoracic pressure
↑↑Pulmonary vascular resistancePulmonary vascular resistance
Cardiac outputCardiac output

3131
Haemodynamic Repurcussions Haemodynamic Repurcussions Of PneumoperitoneumOf Pneumoperitoneum
↑ ↑ Intra abdominal pressureIntra abdominal pressure
↑ ↑ Venous resistanceVenous resistance
↑ ↑ Systemic vascular Systemic vascular
resistanceresistance
↑ ↑ Arterial pressureArterial pressure