Embed Size (px)
Citation preview

Resilient Health Care: reconciling work-as-imagined
and work-as-done
Date: September 16, 2015 Melbourne, Australia
Jeffrey Braithwaite Professor and Director
Australian Institute of Health Innovation
Director
Centre for Healthcare Resilience and
Implementation Science
2
You
3
Fantasy Work
Plan
4
To do list
Tada list
5
When you get to the end of the day
you always find two things …
6
1. You didn’t accomplish everything
you imagined you would.
2. Your day wasn’t anything like
how you’d imagined.
7
8
This distinction
between
WAI
and WAD is …
everywhere
9
My own
expertise is in
health care, so
I’ll occasionally
use hospitals
as an example.
10
You’re not the only one
who imagines how work
is done.
11
Policy-makers, managers,
legislators, governments,
boards of directors, software
designers, safety regulation
agencies, teachers,
researchers.
Are you on
this list?
12
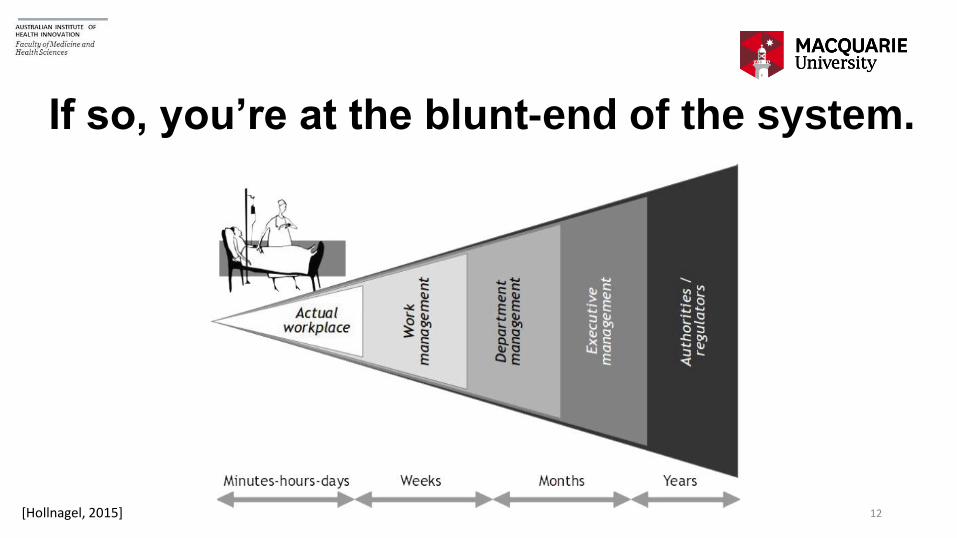
If so, you’re at the blunt-end of the system.
[Hollnagel, 2015]
The blunt end
tries to …
shape,
influence,
nudge
behaviour. 12
What they do
seems perfectly
logical, obvious
and feasible. 13
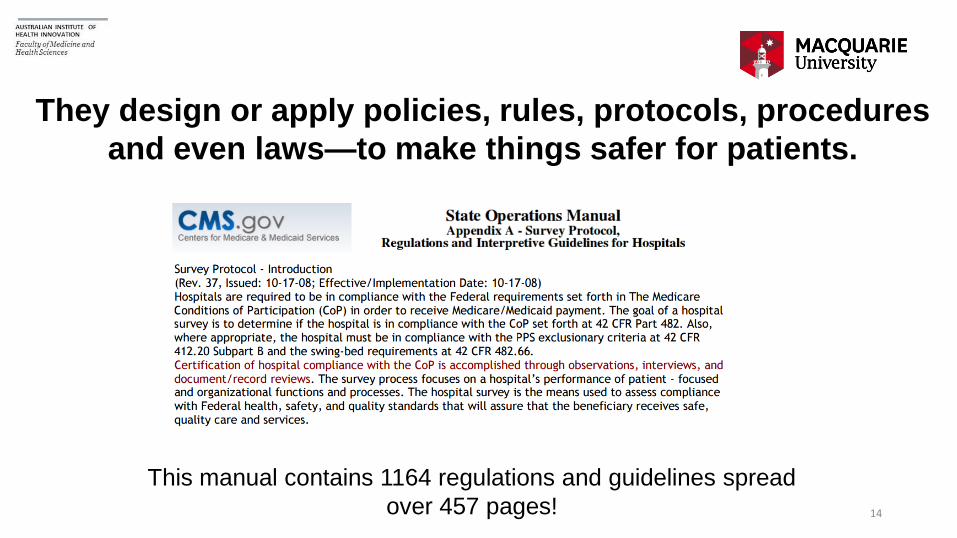
They design or apply policies, rules, protocols, procedures
and even laws—to make things safer for patients.
14
This manual contains 1164 regulations and guidelines spread
over 457 pages!
16
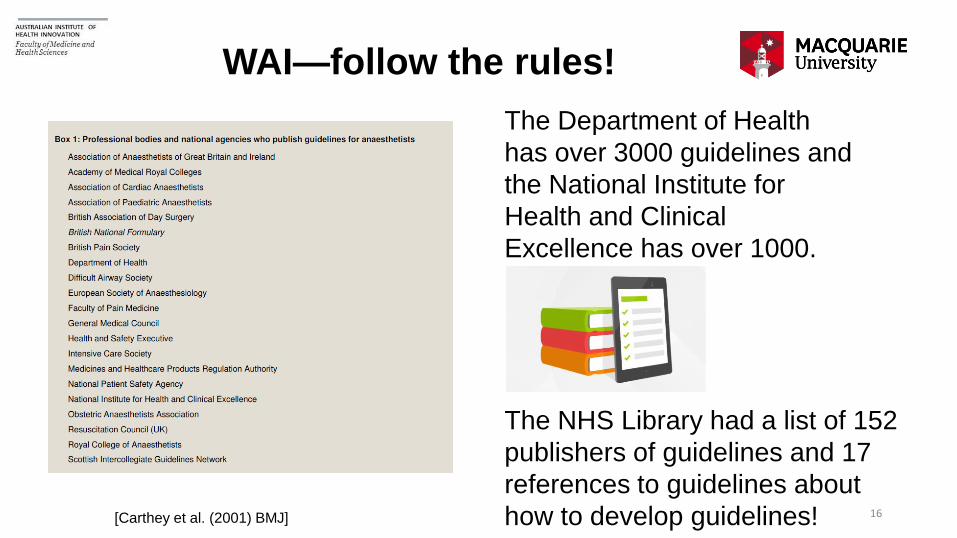
WAI—follow the rules!
The Department of Health
has over 3000 guidelines and
the National Institute for
Health and Clinical
Excellence has over 1000.
The NHS Library had a list of 152
publishers of guidelines and 17
references to guidelines about
how to develop guidelines! [Carthey et al. (2001) BMJ]
In health care, those
doing WAI have designed,
mandated or encouraged
a bewildering range of
tools, techniques and
methods, to reduce harm
to patients. 15
E.g., root cause analysis, hand hygiene
campaigns, failure modes effects analysis ...
16
And there’s lots of
others …
But the rate of
harm has flatlined
at 10%
17

Heart bypasses on
eight year olds, key
hole surgery, treatment
for HIV/AIDS. 18
But the rates
of harm
haven't
reduced far
enough 21
Meanwhile
work is getting
done, often
despite all the
policies, rules
and mandates 221
23
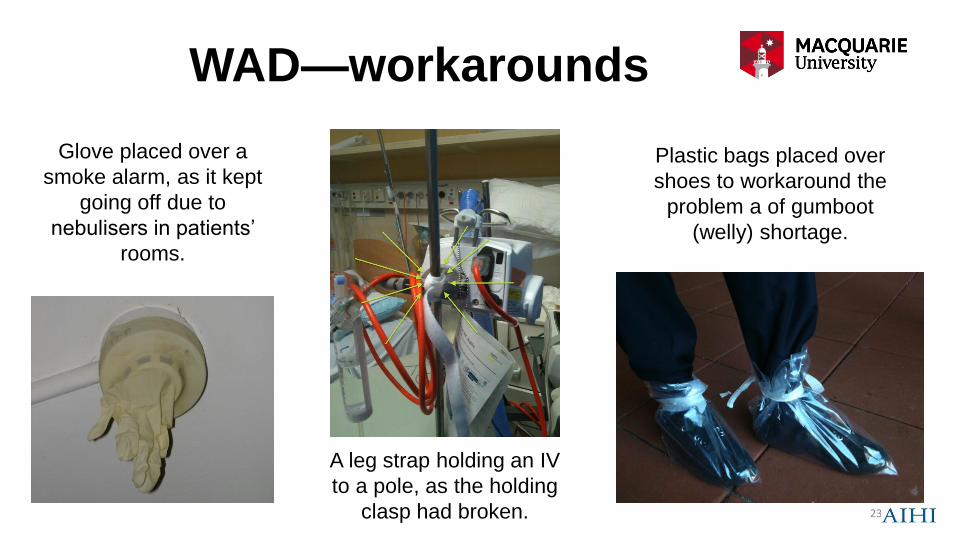
WAD—workarounds
Glove placed over a
smoke alarm, as it kept
going off due to
nebulisers in patients’
rooms.
Plastic bags placed over
shoes to workaround the
problem a of gumboot
(welly) shortage.
A leg strap holding an IV
to a pole, as the holding
clasp had broken.
24
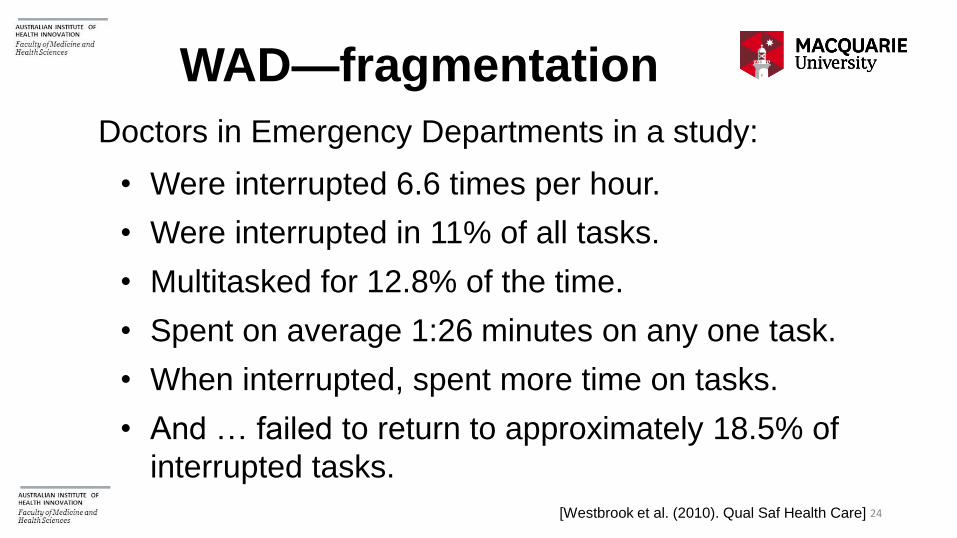
Doctors in Emergency Departments in a study:
• Were interrupted 6.6 times per hour.
• Were interrupted in 11% of all tasks.
• Multitasked for 12.8% of the time.
• Spent on average 1:26 minutes on any one task.
• When interrupted, spent more time on tasks.
• And … failed to return to approximately 18.5% of
interrupted tasks.
[Westbrook et al. (2010). Qual Saf Health Care]
WAD—fragmentation
So work-as-imagined folks
often have some sort of linear,
mechanistic view of the system.
21
Instead, health care is a
complex adaptive system
delivered by people on
the front line who flex and
adjust to the
circumstances. 26

And don’t deliver care in the
way blunt end
prescriptivists want them to.
27
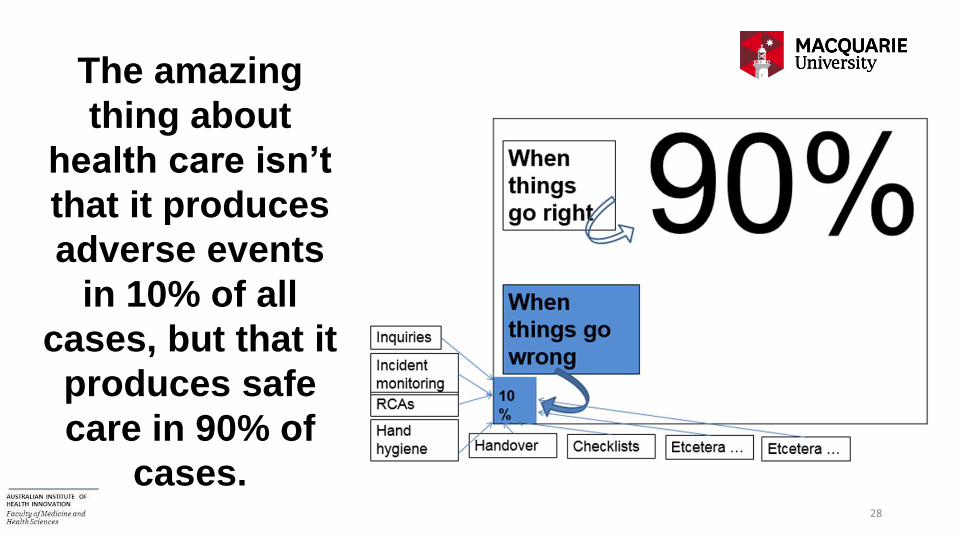
The amazing
thing about
health care isn’t
that it produces
adverse events
in 10% of all
cases, but that it
produces safe
care in 90% of
cases. 28
Few people have ever looked
at why things go right so often
29
If I walk into a
public
hospital in
New South
Wales and
chat to the
front line … 30
What none of them know is that
there are 600 policies in operation
right now, meant to “guide” their
work.
31
Then when I observe
their behaviours and see
them taking patients’
histories, or giving out
medications, or doing
procedures, or taking x-
rays of patients, or
tending to their needs, or
caring for them … 32

I notice instead a lot of fraught, time-
pressed, relentlessly busy work going on
virtually across the entire shift.
29
It doesn’t look like
the pristine, logical
world dictated by the
work-as-imagined
proponents.
And it never, ever
unfolds like a policy
or procedure says it
should. 30
35
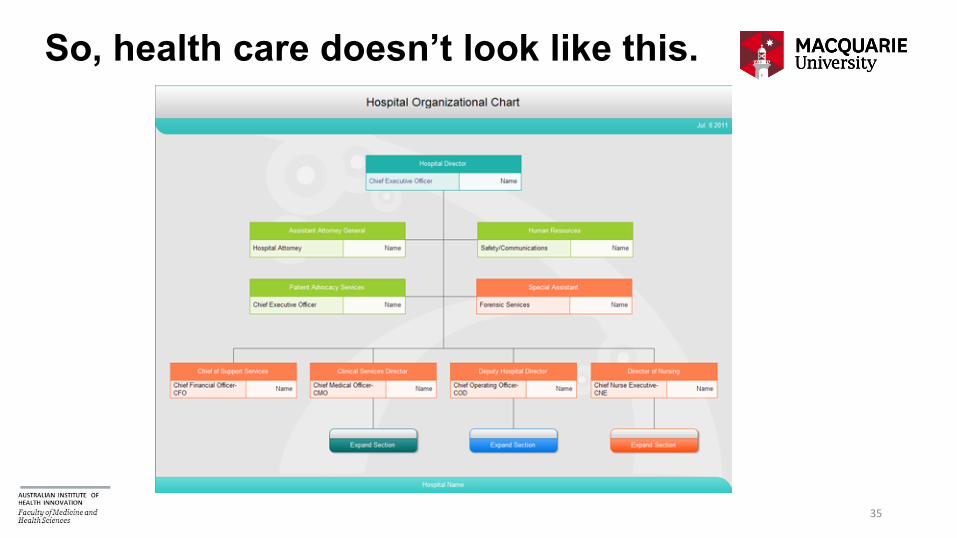
So, health care doesn’t look like this.
36
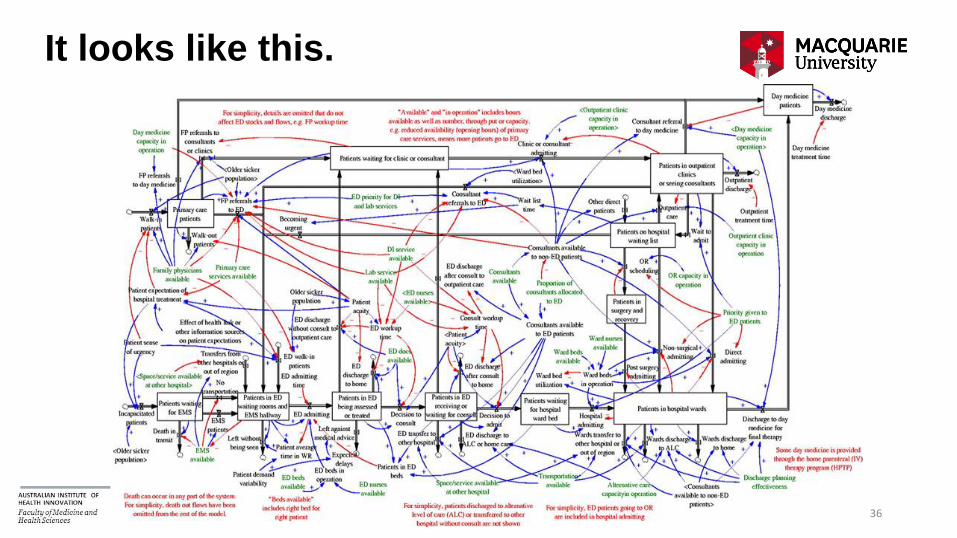
It looks like this.
And therefore
the only real
solution is to try
and reconcile
work-as-
imagined and
work-as-done. 32
A health system where
the work-as-imagined
policies, regulations,
standards etc are much
closer to an
understanding of how
work is actually done. 33
A message to blunt end people—
learn how work actually works.
34
A message to sharp end people—
work more closely with WAI people.
35
The bottom line?
36
In life, in marriage, in affairs of the
heart, in friendships, in international
relations, and in working
environments:
It’s always better to engage with your
partner. 36

Thank you for listening
37
44
Recent Books
• Reconciling Work-as-imagined and Work-as-done
• The Sociology of Patient Safety
• Successful Health Care: the Experience of 60 Countries
• Gaps: the Surprising Truth Hiding in the In-between
• Culture and Climate in Health Care Organizations
• Resilient Health Care
• The Resilience of Everyday Clinical Work
• Healthcare Reform, Quality and Safety
Published In Press
2010
2013
2015 2015

45
Contact
Jeffrey Braithwaite, PhD
Foundation Director
Australian Institute of Health Innovation
Director
Centre for Healthcare Resilience and Implementation Science
Professor, Faculty of Medicine and Health Sciences
Macquarie University
Email: [email protected]
Web: jeffrey.braithwaite.com
Web: http://aihi.mq.edu.au
Wikipedia: http://en.wikipedia.org/wiki/Jeffrey_Braithwaite