Embed Size (px)
Citation preview

Reflections on Cohorts and Longitudinal Studies
Jimmy WhitworthHead of Population Health
Wellcome Trust
FlorenceOctober 2014

• an independent biomedical research-funding charity
• established 1936
• funded from private endowment
• managed for long-term stability and growth
• interests range from science to history of medicine
The Wellcome TrustThe Wellcome Trust

Wellcome Trust Wellcome Trust Vision and strategic aimsVision and strategic aims Our vision is to support research leading to extraordinary improvements in human and animal health
Our five major challenges are:
1. Maximising the health benefits of genetics and genomics
2. Understanding the brain
3. Combating infectious disease
4. Investigating development, ageing and chronic disease
5. Connecting environment, nutrition and health.

• Health research - including public health, health services research, clinical and fundamental research
• Not-for-profit technology transfer activities
• Medical humanities - including biomedical ethics and the history of medicine
• Public engagement and communication
See www.wellcome.ac.uk
The Wellcome Trust: What do we fund?

International funding:Henry Wellcome’s legacy
“We will take forwards major initiatives to build research capacity in India and Africa”
“We help to create world-class research environments in the locations in which we fund”
• Support over 3000 researchers in more than 50 different countries
• Total spend approx £720 million p.a
• £103.2 million for international activities

Cohort and longitudinal studies
• Population and Public health 1990-2011,
Portfolio review published April 2013
www.wellcome.ac.uk/populationhealth
• More than a quarter of the funding allocated to cohort studies and prospective longitudinal research
• Wellcome Trust’s key influences include ‘its committed support to longitudinal studies, both in the UK and in low- and middle-income countries’.

Longitudinal population studies
• Include:
• Cohorts
• Demographic Health Surveillance Sites
• Biobanks (those with a longitudinal component)
Long-term commitment
Strengths and weaknesses
Niche within landscape
Core resource ± Scientific studies

Landscape analyses
• MRC Strategic Review of the Largest UK Population Cohort Studies. 2014
Maximising the value of UK population cohorts
Covers 33 UK cohorts
• We have conducted a similar survey of cohort studies in LMICs

Survey of LMIC cohorts
• Covers 77 studies, 107 sites in 32 countries.
• Over 50 different funders: national agencies, NGOs, private companies, charities, academic institutions
• Mainly Africa and Asia, but generally good coverage
• Central Asia and Middle East poorly represented
• Large numbers in India, South Africa, Brazil, China
• Few urban
• Few mental health or injuries
• Few linked to other sources of data, other studies, little harmonisation or standardisation, few provide open access to data

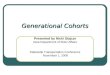
Distribution of LMIC LPS sites by Research Area

Geographical spread and research focus of longitudinal population studies

Recommendations (1)
Data Linkage: to routine datasets, microbiology and hospital records
Co-ordination: networking between studies
Emerging Technologies: standardised techniques, development of best practice guidelines
Capacity-strengthening: interrogating large and complex datasets, infomatics, data management

Recommendations (2)
Data-sharing and discoverability:
searchable directories, data sharing policies, access to samples.
Standardization: common data standards, improving meta-data quality
Cost-efficiency: new digital technologies and remote data and sample capture
Translation: stakeholder engagement to increase the impact of research outputs and potential for translation

As health research funders, we want…
• To support high quality health research that is:
– timely and widely used
– transparent and available to others
– quickly translated into better policies and better health
• To minimise duplication
• To get maximum “bang for buck”
– data useful both locally and more widely
– data answer several questions
– data endure for (now unforeseen) future uses

But the current situation for public health research is often that…• data analysis and reporting are slow
and incomplete
• lack of access to data limits the capacity for comparative analysis or even checking for accuracy
• only immediate research interests are addressed; broader questions are neglected
• lots of duplication in data collection
• data are not archived effectively for long-term preservation and use

There are significant barriers…• Infrastructural - building & sustaining
infrastructures for long-term data storage and curation
• Cultural – incentives and recognition for researchers who share their data
• Technical - developing data standards, metadata, platforms for inter-operability
• Professional – providing training and career paths for data managers
• Ethical - protecting the confidentiality of research participants

• researchers doing crucial work to generate public health research datasets in often difficult circumstances will lose out to better-resourced researchers elsewhere, who have the skills and tools to rapidly analyze the data
• increased data sharing will create unacceptable risks for research participants
• data sharing carries a substantial cost in terms of money and time
17
…And particular concerns over health data in resource poor-settings

The funder position – a growing consensus• major challenges associated with
increasingly large & complex datasets, but also tremendous opportunities
• policy convergence in promoting sharing of research data
− expectation that data outputs be preserved and shared in a way that maximises value
− requirement for data management plans as integral part of the application process
• but building the resources, culture and governance to enable data sharing will require us to work in partnership

Working in partnership – some of our current initiatives• Expert Advisory Group on Data
Access – advice on emerging issues relating to data access across genetics, epidemiology and social sciences
• Clinical Trial Data – funded programme of work with IOM and seeking to build an international consortium to support access to clinical trial data
• Public Heath Research Data Forum – global cross-funder initiative to increase access to research data generated by public health and epidemiology research

Key priorities 1: Data discoverability• Report to examine potential models
for enabling data discoverability published July 2014
• Key conclusion: this is a solvable challenge – with exemplars in other fields that could be applied
• To address this it is critical that we:– Link up existing pockets of activity
– Embed good practice in metadata generation and use
– Address related issues in relation to incentives
• Funders considering next steps – welcome feedback from community
http://www.wellcome.ac.uk/About-us/Policy/Spotlight-issues/Data-sharing/Public-health-and-epidemiology/WTP054675.htm

Key priorities 2: Incentives
• Report by Expert Advisory Group on Data Access (May 2014)
• Research culture and environment not perceived to provide sufficient support or rewards for data sharing
• Funders, institutions, publishers and researchers have key roles
• Need to ensure that data sharing is:– planned and resourced appropriately– tracked and cited routinely– more explicitly recognised– supported by specialist expertise and
resources http://www.wellcome.ac.uk/About-us/Policy/Spotlight-issues/Data-sharing/EAGDA/WTP056496.htm

Key priorities 3: the ‘ethical imperative’
• Major ongoing research project to gather the views and expectations of research participants and stakeholders on data sharing
• Work is being conducted in partnership with research teams in five countries (South Africa, Kenya, Vietnam, Thailand & India)
• Aim to identify good practice and inform appropriate policy development
• Report to be launched in March 2015