Embed Size (px)
Citation preview

POSTER SESSION IFRIDAY, SEPTEMBER 30, 2005, 9:30–11:30AM
5.01COMBINED FUNCTIONAL AND MORPHOLOGICAL IMAGINGCONSISTING OF GATED MYOCARDIAL PERFUSION SPECT AND16-DETECTOR MULTISLICE SPIRAL CT ANGIOGRAPHY IN THENON-INVASIVE EVALUATION OF CORONARY ARTERYDISEASE: INITIAL CLINICAL RESULTSM Hacker, T Jakobs, F Matthiesen, C Vollmar, K Nikolaou, C Becker, AKnez, T Pfluger, R Tiling, K HahnDepartments of Nuclear Medicine, Radiology, Neurology and Cardiology,University of Munich, Munich, GermanyBackground: Appropriate diagnosis and therapy of coronary artery disease(CAD) frequently require information about both the functional andmorphological status of the coronary artery tree. Aim of this retrospectiveanalysis was to evaluate multislice spiral computed tomography angiogra-phy (MDCTA) compared to conventional coronary angiography (CCA) interms of allocation of perfusion defects as detected by myocardial SPECT(MPI) to their determining coronary lesions in patients with advanced CAD.Methods: 20 patients with advanced CAD were retrospectively studied.Electrocardiographically gated MPI, MDCTA using a 16-detector CTscanner and CCA were performed in each patient. Reversible perfusiondefects were subsequently allocated to their determining lesion separatelyfor MDCTA and CCA. After this, MDCTA was compared to CCA in termsof lesion detection and lesion evaluation and in stating the correct diagnosisof CAD. In a third step, MDCTA and CCA were correlated in allocatingreversible perfusion defects to their determining coronary lesions.Results: 20 patients (14 male, mean age 64 � 9.2 [48-79] years) wereeligible. Correct diagnosis of CAD was stated in 14/20 patients by MDCTA.33/47 coronary artery stenoses as detected by CCA showed coronary arterylesions including coronary stents in MDCTA, while 16/43 lesions inMDCTA were not correlated with any coronary stenosis in CCA. Sensitiv-ity, specificity, NPV and PPV for MDCTA to detect stenoses �50% in 265coronary segments for patients with advanced CAD were 46%, 97%, 92%and 73%, respectively. 5/5 reversible perfusion defects (PD) in MPI couldbe allocated to an appropriate coronary artery stenoses in CCA. Stenoseswere located 4x in the LAD and 1x in the LCX. In MDCTA 5/5 reversiblePD were allocated to the same lesions, all lesions were rated as �50%.Conclusion: The preliminary results of the present study show highaccuracy for MDCTA to allocate reversible perfusion defects in MPI to theirdetermining coronary artery lesions in a small patient collective withadvanced CAD. Further studies are needed to confirm these results fordifferent subgroups of patients with suspected and known CAD.
5.02TWO HOUR THALLIUM-201 INFUSION SPECT, IN CONJUNCTIONWITH REST AND 24 HOUR REDISTRIBUTION MAY DISTINGUISHBETWEEN STRESS-INDUCED ISCHEMIA OR HIBERNATINGMYOCARDIUMRM Iwanochko, R Petrovici, DS Lee, M HusainToronto Western Hospital-University Health NetworkBackground: Thallium-201 is the preferred SPECT tracer for the detectionof viability, and several protocols exist for this purpose. We previouslyshowed that a continuous 2-h infusion of Tl-201 achieved higher blood poollevels, and hypothesized that this protocol would improve the detection ofviable myocardium, and potentially distinguish hibernating from ischemicmyocardium.Methods: Tl-201 infusion was compared to rest and 24-h redistributionTl-201, and dipryridamole stress 99m-Tc Sestamibi scans. Twenty-ninepatients (25 males) with previous myocardial infarction (MI) and systolicdysfunction (LVEF�27�11%) were assessed. Each patient had an initialIV bolus of 2 mCi Tl-201, followed by a 2-h infusion of 1 mCi Tl-201. Arest scan (RS) was acquired at 10 min after the bolus, and an infusion scan(IS) was acquired after completion of the 2-h infusion. At 24 h, aredistribution scan was performed, as the standard viability study (VS).Following this, each patient had a dipyridamole stress 99m-Tc Sestamibistudy (SS). Perfusion was scored using a 9-segment 4-point (0-3) model(Min/Max score: 0/27).
Results: Of the 261 segments analyzed between IS and VS, the scores in198 (75.9%) were concordant (Spearman r�0.83, kappa�0.63, bothp�.001). In the 63 discordant segments, increased uptake occurred in 57(21.9%) segments in VS studies and in 6 (2.2%) segments in IS studies. In11 non-concordant segments, IS showed lower uptake than RS, andreversibility was also seen on SS. Decreased uptake on IS vs. RS had apositive predictive value (PPV) for stress-induced ischemia on SS of 91.7%,but a sensitivity of only 17.2%. Only 4 segments on VS had decreaseduptake compared to RS, of which only 1 showed reversibility on SS. Thus,decreased uptake on VS had a PPV for stress-induced ischemia of 25%.Conclusion: These results suggest an optimal protocol for evaluatingviability and ischemia post-MI may include a combinatorial strategy.Standalone use of IS does not supplant the utility of VS for identifyingviability, as it underestimates viability. In conjunction with RS, loweruptake in segments on the IS can predict ischemia on SS.
5.03IN HYPERTROPHIC CARDIOMYOPATHY, REGIONAL HYPER-TROPHY IS NOT ASSOCIATED WITH PERFUSION DEFECTSCORES ON STRESS MYOCARDIAL IMAGINGRM Iwanochko, R Petrovici, DS Lee, A Woo, S Siu, M HusainToronto Western Hospital-University Health NetworkBackground: Patients with hypertrophic cardiomyopathy (HCM) arethought to exhibit perfusion defects on stress-rest SPECT myocardialperfusion scans (MPS), that may not be related to stress-induced ischemia.We sought to examine the presence of defects on SPECT MPS, correlatingthem with regions of hypertrophy on echocardiography.Methods: In 50 patients (40 males) with documented HCM, we comparedechocardiographic findings with stress-rest SPECT MPS. Echocardiographywas performed within 31�44 days of the MPS. Bruce protocol treadmillexercise was performed in 36 patients, pharmacologic stress in 14 (13dipyridamole, 1 adenosine), 99m-Tc Sestamibi in 33, 99m-Tc Tetrofosminin 2 and Thallium-201 in 15. On MPS, the left ventricle was scored on a9-segment model with tracer uptake being graded from 3 (normal) to 0(absent) (Min/Max scores: 0/27). The summed difference score (SDS),representing reversibility, was the difference between the summed rest score(SRS) and summed stress score (SSS). MPS segments were compared to thecorresponding anterior, septal, inferior, lateral and apical wall segments asdefined by echocardiography.Results: Hypertrophy was concentric in 7 patients, apical in 5, septal in 6,septal�anterolateral in 17, septal�anterior in 6, septal�apical in 2, andseptal�inferior in 7, with echocardiographic parameters of hypertrophy forthe whole group being IVSD: 17�5 (mm), PWD: 10�2 (mm), and LVMI:264�78 (g/m2). On SPECT, 16 patients had normal scores, 8 had fixeddefects, 24 reversible defects and 2 had reverse-redistribution. Univariateregression showed no association between SRS, SSS and SDS with IVSD,PWD, LVMI, or concentric hypertrophy. Importantly, comparing regions,no pattern was found between segments with hypertrophy and correspond-ing MPS scores. When assessing only treadmill exercise patients, thosehaving a normal MPS exercised significantly longer (10.3�2.9 vs. 8.8�2.9min; p�0.04) and achieved a higher heart rate with exercise (164�20 vs.148�22 bpm; p�0.003), than those having an abnormal MPS.Conclusion: Neither SRS, SSS or SDS correlated with any global orregional parameters of hypertrophy on echocardiography. In HCM patients,a normal scan predicts improved exercise-capacity.
5.04DIAGNOSTIC UTILITY OF STRESS SPECT DETECTION OFCORONARY ARTERY DISEASE IN DILATED CARDIOMYOPATHYHZ El Masry, Z Jaradat, BR Khan, VG Kalaria, J MahenthiranKrannert Institute of Cardiology, Indiana University, Indianapolis, INBackground: Stress myocardial perfusion using single-photon emissioncomputed tomography (SPECT) is an established diagnostic tool fordetection of coronary artery disease (CAD). However, the diagnosticaccuracy of stress SPECT in patients (pts) with a dilated left ventricle (LV)has not been studied. We evaluated the diagnostic ability of stress SPECT
S100 Journal of Nuclear CardiologyJuly/August 2005

perfusion study, as compared to coronary angiography, for detection ofobstructive CAD in dilated cardiomyopathy (DCM).Method: We studied 48 pts with a dilated LV, as defined by an end-diastolicvolume of � 120 cc on post-stress gated SPECT calculation. All pts hadundergone a cardiac catheterization within � 90 days (median of 12 dayspost stress) of the SPECT study. A standard 17-segment, 5-point scaleperfusion analysis was performed by SPECT. Regional and total sum stressscore (SSS), sum rest score (SRS) and sum difference score (SDS) werecalculated as per standard nomenclature. A regional SSS � 3 and SDS �1was considered a marker of regional ischemia by SPECT. Any CAD wasdetermined by a total SSS � 3 and a total SDS of �1.Criteria for significantCAD was defined as � 50% stenosis in any of the three major epicardialcoronary arteries corresponding to the SPECT regional perfusion. Valuesare expressed as mean � STD.Results: Study cohort age: 58 � 9 years, 42 (87%) males. LV ejectionfraction: 42 � 11%. Gated SPECT post-stress end diastolic volume: 172 �48 cc and end systolic volume: 101 � 52 cc. Total SSS: 14 � 10, SRS: 9 �9 and SDS: 4.3 � 4.5. The diagnostic sensitivity and specificity, as per SSSand SDS criteria compared to cardiac catheterization is shown on the table:
Any LAD LCX RCA 1 vessel 2 vessel 3 vessel
Sens 0.93 0.77 0.68 0.62 0.67 0.64 0.92Spec 0.73 0.66 0.58 0.58 — — —
Any� any territory, Sens�sensitivity, Spec�specificityThe overall diagnostic accuracy of cardiac stress SPECT perfusion study isgood in pts with DCM. The regional sensitivity and specificity of CADdetection is somewhat limited and detection of triple vessel disease asdetermined by cath remains good with stress SPECT in DCM.Conclusion: Stress SPECT is a good (sensitivity) diagnostic tool fordetecting obstructive CAD in DCM, especially for triple vessel disease.However, the specificity of regional perfusion abnormalities may be limitedin the setting of DCM. While the reduced regional diagnostic accuracy ofstress SPECT is likely multi-factorial, the least accuracy in the RCA or LCXsegments may be partly related to greater tracer count attenuation and anoverlap in regionayl perfusion in DCM.
5.05SPECT REST PERFUSION AND GATED WALL MOTION SCORECORRELATES OF ECHOCARDIOGRAPHY WALL MOTIONZ Jaradat, HZ El Masry, A Raiesdana, SG Sawada, J MahenthiranKrannert Institute, Indianapolis, INBackground: Gated SPECT quantitative analysis has enhanced detection ofregional and global wall motion and the final scan interpretation. Two-dimensional echocardiography (ECHO) regional wall motion analysis is stillconsidered gold standard for analyzing regional wall motion abnormalities.However, no previous studies have compared the quantitative extent by ECHOwall motion to resting perfusion and regional wall motion by gated SPECT.Method: We analyzed 176 patients who had a rest / stress SPECT and anECHO within � 90 days (median: 4 days; mean 68 days) of each other. Astandard 17 segments 5-point scale perfusion and wall motion analysis wasperformed on post stress resting gated SPECT study. A total and regionalsum rest score (SRS); and a total and regional sum motion score (SMS)were calculated for comparison by SPECT. A 16-segment, 8-point scaleanalysis was performed by ECHO at rest. Wall motion score index (WMSI)by ECHO was calculated from the total sum of all segments scored dividedby the number of segments visualized. A total and corresponding coronaryregional WMSI was calculated from the ECHO by independent readers. Theextent of correlation of total and regional scores by both methods and theROC analysis of a normal LVSI compared to SRS and SMS values wereestimated. Variable values are expressed as mean � SD.Results: In 176 pts (age 57 � 14 years, 49% females) the post-stressgated-SPECT left ventricular (LV) ejection fraction was 57 � 12%. SPECTperfusion total SRS was 3.8 � 5.8, total SMS was 3.8 � 6.6 and globalECHO-WMSI was 1.2 � 0.3. Total SRS and SMS scores had goodcorrelation to global LV WMSI by ECHO (r�0.72 and r�0.75, p�0.001for both). Similarly, regional rest perfusion by LAD SRS (r�0.75,p�0.001), RCA SRS (r�0.66, p�0.001), LCX SRS (r�0.4, p�0.01) andregional SMS abnormality by LAD SMS (r�0.78, p�0.001), RCA SMS(r�0.69, p�0.001) and LCX SMS (r�0.38, p�0.01) had acceptablecorrelation to regional WMSI by ECHO. On ROC analysis, a cut-off of 3.5for rest SRS (0.85, 95% CI: 0.78-0.93, p�0.001) and a cut-off score of 3.5
for SMS(0.86, 95% CI: 0.79-0.94, p�0.001) provided the maximum areaunder the curve for detecting a normal WMSI (�1) by ECHO.Conclusion: Gated SPECT semi-quantitative resting perfusion and poststress regional wall motion analysis have good correlation to quantitativeWMSI by ECHO. Correlation was least in the lateral segments. A restingsum perfusion score � 3.5 and a post-stress gated SPECT wall motionscore � 3.5 effectively(85% sensitivity and 79% specificity) identifies anormal regional wall motion (WMSI) by ECHO. This may help betteridentify normal function by SPECT in the borderline abnormal scans.
5.06HIGH RISK MYOCARDIAL PERFUSION SPECT FINDINGS AREPREVALENT IN PATIENTS WITH PERIPHERAL ARTERIALDISEASE DIAGNOSED BY ANKLE BRACHIAL INDEX TESTINGDP Shah, DE Virnich, RP WardUniversity of Chicago, Chicago, ILBackground: Patients (pts) with peripheral arterial disease (PAD) diagnosed byankle brachial index (ABI) evaluation are known to have a high cardiovascularmortality. While this has primarily been attributed to coexistent coronary arterydisease (CAD), the stress myocardial perfusion SPECT (MPS) findings in ptswith PAD by ABI evaluation have not been studied in a systematic manner.Accordingly, our goal was to determine the prevalence of high risk (HR) MPSfindings in pts with PAD diagnosed by ABI who are referred for MPS testing.Methods: Eligible pts were identified from a database of 565 pts who hadclinically indicated ABI evaluation in the vascular imaging laboratory at theUniversity of Chicago between 1/2002 and 3/2003. Pts were included (n�157) if they also had completed MPS testing at our institution. Ptcharacteristics, mode of stress, and SPECT results including summed stressscore (SSS), summed rest score (SRS), summed difference score (SDS),LVEF, quantitative transient ischemic dilation (TID, defined as � 1.22), andthe composite of any HR finding (SSS8, LVEF � 35%, or TID) wererecorded. Pts with PAD (ABI � 0.9) [n�87] were compared to pts withoutPAD [n�70]. Mild-moderate PAD (ABI 0.5-0.9) [n�62], and severe PAD(ABI � 0.5) [n�25], were also noted.Results: The study group was a mean 68 yrs, 44% male, 65% pharmaco-logic stress, and there was a high prevalence of HTN (87%), DM (48%),hyperlipidemia (54%), and prior CAD (35%). The results of MPS testing forthe total study group are listed in Table 1. Any HR MPS findings remainedmore prevalent among PAD pts in subgroups without prior CAD (57% vs33%, p* �0.02), and when only mild-moderate PAD pts were compared tothose with no PAD (58% vs 34%, p* �0.03)Conclusion: Pts with PAD diagnosed by ABI evaluation who are referred forMPS testing have a high prevalence of HR MPS findings, and significantlymore HR findings than pts without PAD, even after adjusting for important ptfactors. HR findings are more prevalent even in pts with mild-moderate PAD(ABI 0.5-0.9) in whom vascular surgery, and thus routine preoperative MPS,would not be expected. Further study is needed to determine if PAD pts withoutan indication for MPS testing would benefit from screening MPS.
Table 1 PAD (n� 87) No PAD (n�70) Adjusted p value*
SSS �8 51% 27% 0.02LVEF � 50% 30% 13% 0.09LVEF � 35% 12% 3% NSTID 41% 27% NSAny HR finding 69% 44% 0.01
*Adjusted for age, gender, HTN, DM, hyperlipidemia, prior CAD, pharm stress
5.07OVERESTIMATION OF POST-ISCHEMIC MYOCARDIAL STUN-NING ON STRESS GATED SPECT IMAGING; CORRELATIONWITH ECHOCARDIOGRAPHYEL Gundeck, KA Williams, KT Spencer, RM Lang, RP WardUniversity of Chicago, Chicago, ILBackground: Post-ischemic global and regional LV dysfunction on stressGated SPECT (GS) imaging is reported frequently and are widely attributedto post-ischemic myocardial stunning, despite clinical imaging that fre-quently occurs �30 minutes (min) after stress and the inability of GS todirectly visualize the endocardium. We hypothesized that true myocardialstunning is rare at the time of clinically performed post-stress GS imagingand sought to determine the prevalence and specificity of regional wallmotion abnormalities on GS scans after ischemic stress.
Journal of Nuclear Cardiology Abstracts S101Volume 12, Number 4;S2-S13

Methods: 27 patients (pts) referred for clinically indicated dual isotopeexercise myocardial perfusion SPECT testing were prospectively enrolled ifthey had an ischemic response of exercise stress based on symptoms and/orECG criteria. A transthoracic echo was performed just prior to clinical stressGS imaging for assessment of regional wall motion (RWM) and quantitativeLVEF (biplane method of discs). Each coronary distribution (CD) for eachpt (n�81) was scored for myocardial perfusion (normal, reversible, fixed)by GS, and RWM (normal, abnormal) by GS and echo. Baseline wallmotion was determined by repeat echo � 24 hrs after enrolment in pts withan abnormal post-stress echo.Results: The mean age was 61.2 yrs and the mean duke treadmill score was-8.5. The mean stress injection to GS time � 54.7 min, mean injection toecho time 41.1 min. Of the 81 CD, 57% had perfusion defects (PD) (51%reversible, 6% fixed), 22% had GS RWMA, 7.4% had post-stress echoRWMA, and 6.2% had baseline RWMA. All fixed PD were associated witha GS RWMA, and matching post-stress echo RWMA and baseline RWMA.Among reversible perfusion defects, 32% had GS RWMA, but only 2% hada post-stress echo RWMA and no baseline RWMA were present. Thus, trueregional myocardial stunning was confirmed in only 8% of reversibleRWMA on GS. Overall, a GS RWMA had a sensitivity �100%, specific-ity � 84%, and a PPV �33%. In CDs with a reversible PD, a GS RWMAhad a sensitivity �100%, and a specificity �70%. Among PD of �moderate severity, a GS RWMA had a specificity � 43% and a PPV � 8%.GS LVEF and post-stress echo LVEF were similar for all pts (62.6% vs63.0%, P�NS). GS LVEF was lower than post-stress echo LVEF among ptswith reversible PD (61.1% vs 64.4%, p�0.09), and significantly lower in ptswith reversible PD of � moderate severity, (58.6% vs 63.0%, p�0.01).Conclusion: True myocardial stunning after ischemic stress is rare at thetime of clinically performed post-stress GS imaging, and GS appears tooverestimate global and regional stunning in this setting, possibly due to theinability to directly visualize ischemic endocardium. Caution should beexercised in interpreting post-stress global or regional LV function on GS inscans with reversible ischemia.
5.08IMPAIRED CHRONOTROPIC RESPONSE IS STILL PRESENT 60MINUTES AFTER EXERCISE STRESS TESTING IN PATIENTSWITH TRANSIENT ISCHEMIC DILATATIONY Akutsu, H Gewirtz, SA Gregory, GD Zervos, GS Thomas, T YasudaNuclear Cardiology, Massachusetts General Hospital, Boston, MABackground: Transient ischemic dilatation (TID) after exercise testing hasbeen associated with severe ischemia, but a relationship between TID andimpaired chronotropic response post-exercise has not been described. Ourhypothesis is that patients with TID will have post-exercise chrontropicincompetence.Methods: One day Rest/Stress 99mTc sestamibi myocardial perfusionSPECT imaging (MPI) was performed in 728 consecutive patients (meanage 58 � 12 years, 239 female) suspected of having ischemic heart disease.Images were gated 60 min. after treadmill exercise. Patients heart rates(HR), blood pressures and ECGs were recorded at rest, peak exercise, thenat 1 min., 5 min. and 60 min post-exercise. LVEF, TID ratio, summed stressscores (SSS), and summed difference scores (SDS) were calculated using anautomated program (4DM).Results: 118 pts. had ischemia (group A), 678 pts. had no evidence ofischemia (group B). The groups differed significantly (p�0.001) withrespect to: EF (%): 57 �13 vs. 67 � 11, TID: 1.0 � 0.1 vs. 0.9 � 0.1, andSDS: 4 � 4 vs. 0 � 1 (group A vs. B respectively). The mean HR at 60 min.was higher than rest-HR in both groups (p�0.0001). However, the mean HRwas lower in group A than B despite their rest-HRs being similar. Further,there is a significant (p�0.0001) negative correlation between TID ratio andpeak-exercise and post-exercise HR.Conclusion: Impaired chronotropic response associated with TID is stillpresent at 60 minutes post-exercise. Findings suggest an “after effect” ofsevere ischemia persist over 60 min. This may prompt us for an additionalpts. care before discharging from a stress laboratory.
HR Rest Peak Post 1 min. Post 5 min. Post 60 min.
Group A 67 � 13 130 � 20 108 � 19 80 � 15 70 � 12Group B 69 � 12 145 � 24 119 � 21 87 � 14 74 � 13
(p�N.S) (p�0.0001) (p�0.0001) (p�0.0005) (p�0.0329)
5.09DOES ATTENUATION CORRECTION IMPROVE THE INTERPRE-TATION OF MPI IN PATIENTS WITH LBBB?WL Duvall, LB Croft, C Pungoti, MJ HenzlovaMount Sinai Medical Center, New York, NYBackground: Myocardial perfusion imaging (MPI) in patients with leftbundle branch block (LBBB) is a well described diagnostic challenge. Toour knowledge, no one has investigated the use of attenuation correction(AC) in interpreting MPI in the setting of LBBB.Methods: We retrospectively reviewed all patients from 2000-2004 with aLBBB without known coronary artery disease (CAD) who underwent aTc-99m gated stress SPECT imaging study with AC (Vertex, Philips/ADAC, VantagePro). Vasodilators were used in all patients. Imaging resultswere categorized as normal, normal after AC, abnormal with a perfusiondefect consistent with a LBBB which did not normalize after AC, orabnormal consistent with CAD. Studies were reviewed for hemodynamicresponse and left ventricular ejection fraction (LVEF). The results ofsubsequent cardiac catheterization and survival based on the Social SecurityDeath Index were determined.Results: A total of 215 patients were identified but 115 patients hadmultiple perfusion defects consistent with CAD. Of the remaining 100patients, 26 patients had no perfusion defects, 33 normalized with AC,and 41 remained abnormal. There was a greater proportion of males(p�0.001) and a lower ejection fraction (p�0.0001) in those patientswhose images did not normalize after AC. There was no significantdifference in resting or peak heart rate, or in the blood pressure responseto stress. There was no statistical difference in mortality during meanfollow-up of 22 months.Conclusions: Patients with normal images, both with and without AC,had similar LVEF and mortality. Patients whose images did notnormalize after AC were more likely male and had a lower LVEF. Themechanism of normalization with AC is unclear, but the use of AC inpatients with LBBB may decrease false positives and improve imageinterpretation.
All PatientsN�100
NormalN�26
CorrectedN�33
AbnormalN�41
Pvalue
Age 68 � 13 yrs 74 � 12 yrs* 71 � 12 yrs 66 � 14 yrs* *p�0.02
Gender 74 (74%) 25 (96%)† 26 (79%)‡ 23 (56%)†‡ †p�0.001
(Female) ‡p�0.05
‚ HR bpm 18 � 9 17 � 9 15 � 8 17 � 10 p�NS
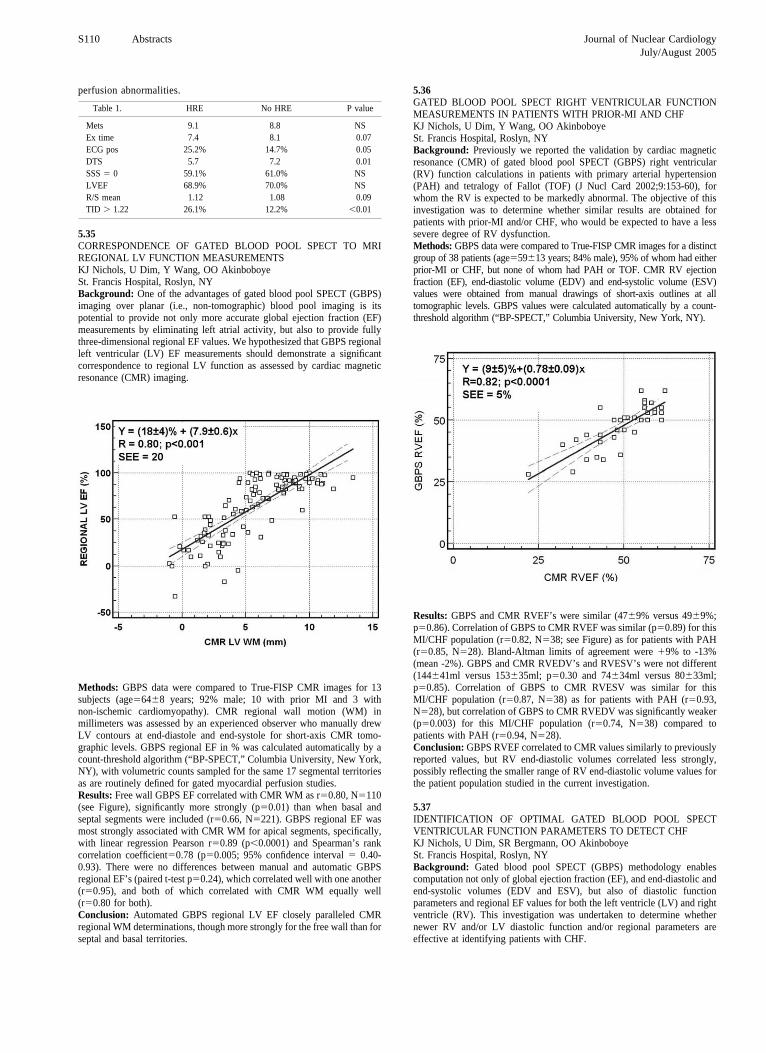
‚ SBP mmHg -21 � 20 -21 � 20 -18 � 19 -21 � 20 p�NS
‚ DBP mmHg -9 � 13 -11 � 10 -8 � 9 -13 � 12 p�NS
LVEF 62 � 10% 66 � 10%† 63 � 10%‡ 55 � 11%†‡ †p�0.0001‡p�0.002
LVEF�50% 15 (15%) 1 (4%)* 2 (6%)* 12 (29%)* *p�0.02
Mortality 4 (4.0%) 1 (3.8%) 2 (6.1%) 1 (2.4% p�NS
5.10OUTCOME OF PATIENTS WITH NORMAL PERFUSION BUT WITHST SEGMENT DEPRESSION DURING ADENOSINE TOMOGRAPHICIMAGINGFG Hage, J Heo, AE IskandrianUniversity of Alabama at BirminghamBackground: ST depression during adenosine infusion suggests coronary-dependent steal and ischemia and the single-photon emission computedtomographic [SPECT] images reveal reversible perfusion defects. Occasion-ally ST depression is observed in the setting of normal perfusion images.The outcome of such patients has been controversial.Methods: We identified 74 patients who underwent gated SPECT perfusionimaging using adenosine as the stress agent. These patients were selectedbased on the following criteria: none had prior myocardial infarction or
S102 Abstracts Journal of Nuclear CardiologyJuly/August 2005
coronary revascularization [CR], all were in sinus rhythm and none had leftbundle branch block. The 74 patients had normal SPECT images butischemic ST response [�1 mm ST depression]. The primary end-point wasoutcome in terms of cardiac death, non-fatal myocardial infarction [MI] orneed for CR.Results: There were 61 women and 13 men, aged 66�13 years. History ofdiabetes mellitus was present in 22 patients [29%] and of hypertension in 56patients[75%].At a mean follow-up of 21 months, there were no cardiac death or MI and6 CR [2 coronary artery bypass grafting and 4 coronary stenting of 1-vesseldisease]. One patient died of cancer.Conclusions: patients with no prior MI or coronary revascularization whohave normal SPECT images have a benign outcome despite the presence ofST depression [0% for death or MI and 0.5%/year for coronary revascular-ization]. Balanced ischemia could not be a common cause for discordantperfusion and ST responses.
5.11INCREASING BODY MASS INDEX OVER A 10-YEAR PERIOD INPATIENTS REFERRED FOR PERFUSION STRESS TESTINGNP Johnson, SM Leonard, P Kansal, E Wu, TA HollyNorthwestern University Feinberg School of Medicine, Chicago, IllinoisBackground: Epidemiology of the general population suggests that bodymass index (BMI) is increasing in the United States. However, it isunknown how this has affected the patient population referred to our nuclearcardiology stress testing laboratory over the last 10 years.Methods: All patients who underwent exercise or pharmacologicSPECT myocardial perfusion imaging from 1995 to 2004 and hadcomplete data were included in a retrospective analysis. This sample of22,859 patients was grouped by year. In addition to BMI, the age,percentage of males, percentage of exercise and pharmacologic tests, andpercentage of abnormal scans (summed stress score [SSS] greater than 0)were computed for each year. A linear regression was performed on BMIas a function of the year.Results: Average BMI increased over time (ANOVA p�0.05). Averagemale percentage and age did not differ over time (ANOVA p0.05). Aweighted linear regression of BMI as a function of year has a slope of 0.148kg/m2/year (p�0.05, R�0.896, R2�0.802).
Year NBMI
(kg/m2)Male(%)
Age(yr)
Exercise(%)
Pharm(%)
SSS�0(%)
1995 2111 27.5 59.6 61.1 61.7 38.3 53.81996 2568 27.8 60.6 60.8 61.4 38.6 56.31997 1524 27.9 58.1 60.3 59.3 40.7 51.21998 1882 28.4 56.7 59.9 60.3 39.7 48.81999 1760 28.8 58.0 59.8 61.5 38.5 52.42000 2076 28.2 57.1 60.3 57.6 42.4 56.02001 1959 28.6 57.6 60.6 53.0 47.0 61.12002 2844 28.7 59.4 60.3 51.9 48.1 58.42003 2961 29.0 59.9 60.4 45.9 54.1 61.72004 3174 28.9 58.7 60.5 45.1 54.9 59.7
Conclusion: BMI has increased in our population over the last 10 years ata rate of approximately 0.5% per year. The average age and sex of patientshave not change significantly over this time. Our lab has performed a lowerpercentage of exercise tests over time, perhaps due to increasing BMI. Thepercentage of abnormal scans has not changed significantly in the last 10years.
5.12RELATIONSHIP OF BODY MASS INDEX ON EXERCISECAPACITY AND THE SEVERITY OF EXERCISE STRESSPERFUSION DEFECTSNP Johnson, SM Leonard, P Kansal, E Wu, TA HollyNorthwestern University Feinberg School of Medicine, Chicago, IllinoisBackground: Higher body mass index (BMI) is associated with havingmore cardiac risk factors and decreased exercise capacity. The relationshipbetween BMI and myocardial perfusion imaging (MPI) findings wasretrospectively analyzed in patients referred to our nuclear cardiology stresstesting laboratory over a 10-year period.
Methods: All patients who underwent exercise SPECT MPI from 1995to 2004 were included if they had complete data recorded. This sampleof 8,869 patients was grouped according to BMI and the presence ofknown coronary artery disease (CAD). The average number of CAD riskfactors (diabetes mellitus, hypertension, dyslipidemia, family history,smoking), age, percentage of males, exercise time (Bruce protocol),peak systolic blood pressure (SBP) and heart rate (HR) double product,and summed stress score (SSS) from a 20-segment model were com-puted.Results: As the BMI increased, exercise time decreased and the peak doubleproduct increased. Interestingly, while the number of risk factors increasedwith increasing BMI, the SSS did not increase consistently and evendecreased in the higher BMI groups.
BMI(kg/m2) CAD N
# ofRisks
Age(yr)
Male(%)
Time(sec)
Peak SBP*HR(mmHg*bpm) SSS
18.5-25 yes 728 1.4 64.3 79.4 604 23496 8.3no 1709 1.1 57.5 52.1 596 26499 2.2
25-30 yes 1214 1.6 62.0 89.9 596 24569 8.3no 2525 1.3 56.4 68.4 574 27498 2.7
30-35 yes 472 1.7 59.0 85.0 539 24787 8.3no 1245 1.4 54.2 57.5 509 27984 2.8
35-40 yes 144 1.9 56.6 79.2 478 24331 7.3no 472 1.6 51.9 47.0 454 28383 2.3
40 yes 52 1.9 56.9 63.5 446 25819 6.8� no 308 1.6 48.6 41.2 386 28482 2.0
Conclusion: BMI correlates as expected with exercise capacity, but notwith semi-quantitative measures of myocardial perfusion. Although CADrisk factors increased with increasing BMI, the perfusion findings may beexplained in part by the lower average age and lower percentage of malesin higher BMI groups.
5.13SIGNIFICANCE OF VENTRICULAR ECTOPY DURING STRESSMYOCARDIAL PERFUSION IMAGINGP Kansal, E Wu, SM Leonard, NP Johnson, TA HollyNorthwestern University Feinberg School of Medicine, Chicago, IllinoisBackground: Ventricular ectopy during exercise stress myocardial perfu-sion imaging (MPI) has been associated with an increased likelihood ofperfusion defects and increased cardiovascular mortality. There are limiteddata comparing the significance of ventricular ectopy during adenosinevasodilator and exercise stress testing and its association with myocardialperfusion defects. Accordingly, we evaluated the relationship of ventricularectopy and perfusion abnormalities in patients referred for adenosinevasodilator or exercise stress testing.Methods: 2040 patients, referred for either adenosine vasodilator orexercise stress testing were divided into two groups based on the presenceor absence of ventricular ectopy. Ventricular ectopy was defined aspremature ventricular depolarizations or non-sustained ventricular tachycar-dia. Summed stress (SSS), summed rest (SRS) and summed differencescores (SDS), were calculated based on a 20-segment model for all patients.Results: 765 patients had ventricular ectopy and 1285 did not have ectopy.The average age in each group was 62.9 � 12.6 yrs and 58.8 � 13.4 yrs(p�0.0001) and EF was 60.4 � 14.2% vs. 64.0 � 11.3% (p�0.0001),respectively. In both the adenosine and the exercise groups, those withectopy had higher SSS (7.7 � 9.9 vs. 4.1 � 6.5; p�0.0001 and3.7 � 6.8 vs. 2.2 � 4.8; p�0.0001). SDS showed a similar relationship(3.7 � 4.7 vs. 2.7 � 4.0; p� 0.0004 with adenosine and 2.6 � 4.5 vs.1.5 � 3.0; p�0.0002) with exercise.
Ectopy No Ectopy
SSS SDS SRS SSS SDS SRS
Adeno 7.7 � 9.9 3.7 � 4.7 4.0 � 7.9 4.1 � 6.5 2.7 � 4.0 1.4 � 4.1Exer 3.7 � 2.6 2.6 � 4.5 1.1 � 4.1 2.2 � 4.8 1.5 � 3.0 0.7 � 2.7
Conclusions: Ventricular ectopy during both adenosine and exercise stresstesting is associated with significantly higher stress perfusion scores incomparison to those without ectopy. Subjects with ventricular ectopy also
Journal of Nuclear Cardiology Abstracts S103Volume 12, Number 4;S2-S13

were older with lower ejection fractions. Ventricular ectopy may be amarker for a higher ischemic burden during stress MPI.
5.14EVALUATION OF EXERCISE PERFORMANCE IN OBESEPATIENTS UNDERGOING PREOPERATIVE EVALUATION FORBARIATRIC SURGERYHI Michelena, D Stepnowski, V Frain, DT Dempsey, C Kowalski, WAVan DeckerTemple University, Philadelphia, PABackground: Extreme obesity may be an indication for bariatric surgery.Preoperative evaluation with exercise nuclear myocardial perfusionimaging may be indicated in this setting. It is common knowledge thatduring exercise testing, both an appropriate target heart rate andsufficient exercise time are required to achieve full coronary flow reserveand thus, elicit relative coronary flow differences. We sought to evaluatethe adequacy of the exercise performed by obese, pre-bariatric surgerypatients.Methods: Surgical databases identified 252 consecutive patients whounderwent preoperative evaluation for bariatric surgery from 01/2001 to2/2005. Of these, 76 (30%) underwent Bruce protocol treadmill exercisetesting and constituted our study population. Target heart rate (TR)achievement (85% of maximal predicted heart rate by age), doubleproduct (DP; maximum heart rate times maximum systolic bloodpressure) and total exercise time (ET) were evaluated. A linear regres-sion model was applied to identify any relation between ET and othervariables.Results: Of the 76 patients, 66 (87%) were female, mean age 42 years(SD10), mean weight 297 lbs (SD 49), mean body mass index (BMI) 49(SD 7). Eighteen patients (24%) were diabetics, 31 patients (41%) hadarterial hypertension and 53 (70%) had obstructive sleep apnea. TR wasreached in 62 patients (82%), DP �20000 was achieved in 69 patients(91%) and ET was �5 minutes in 50 patients (66%). Of the patients thatexercised �5 minutes (26 patients), 73% still reached TR and 85% stillachieved a DP�20000 despite a relative short duration of exercise.There was a negative relation between BMI and ET such that, a unitincrement in BMI would result in an average decrease of 0.08 minutesin ET (p�0.007). A negative relation was also observed between weightand ET such that, a unit increment in weight would decrease ET by 0.01minutes (p�0.007). The relation between age and ET was non-signifi-cant.Conclusions: Although a high proportion of the population studied reachedTR as well as a significant DP, the ET was adequate for a significantly lowernumber of patients. A significant negative relation between BMI-weight andET was observed. This relation could help identify patients unlikely toachieve sufficient ET despite reaching TR and adequate DP, and therefore,more likely to benefit from vasodilator testing.
5.15ADDITIONAL VALUE OF TRANSITORY LEFT VENTRICULARDILATION TO MYOCARDIAL SCINTIGRAPHY IN DETECTINGCARDIAC EVENTS AFTER 18 MONTHSP Smanio, F Rodrigues, R Meneghelo, L Mastrocolla, A Thom, L PiegasInstituto Dante Pazanese de Cardiologia, Sao Paulo, BrazilBackground: Previous studies suggest a correlation between the occurrenceof transitory left ventricular dilation (TD) after the exercise phase ofmyocardial perfusion scintigraphy (MPS) and a more severe coronarydisease. However there are few studies describing the late follow-up ofpatients presenting TD. Objective: To verify the additional prognosticinformation of the TD to the presence of myocardial ischemia at the MPSin 18 months of follow up.Methods: The clinical histories of 204 patients who had performed MPS in2002 were reviewed retrospectively. From those, 141 were male and themean age was 64 years. In the MPS, transient dilation was present in 102and absent in 102. Unstable angina, myocardial infarction or any othersymptoms suggestive of acute ischemic syndrome were defined as cardiacevents (CE) and registered during a mean of 18 months (12-24 m). No ptsdied during the follow-up. MPS were performed by two-day protocol, withsestamibi-99mTc and gated-SPECT technique. The QGS software processeddata. TD was considered present when a more important left ventriculardilation was seen in the stress phase of MPS in comparison to the rest phase,
or when the stress/rest rate of the endocardial border was higher than 1,22.Ischemia was considered present when at least 2 of 20 analyzed myocardialsegments had reversible perfusion defects. Statistic analysis was performedby the chi-square test. Differences associated to p�0,05 were consideredsignificant.Results: As shown in Table 1, the group of pts presenting TD hadsignificantly more CE than those pts without TD.
With Cardiac Events Without Cardiac Events
TD/Ischemia 62(76%)* 20(24%)TD/ no Ischemia 14(70%) 6(30%)No TD/Ischemia 37(60%) 25(40%)No TD / no Ischemia 10(25%) 30(75%)*
*P�0,05
Conclusion: The results might suggest that the presence of DT at the MPSadds prognostic information to the presence of myocardial ischemia at theMPS in 18 months of follow up.
5.16CARDIAC EVENTS AFTER FOUR YEARS OF A NORMALPERFUSION SCINTIGRAPHY IN DIABETIC WOMENP Smanio, P Beraldo, R Mello, F Rodrigues, A Thom, L PiegasInstituto Dante Pazzanese de Cardiologia – Sao Paulo – BrazilBackground: Despite of a decreasing of cardiac mortality due to coronaryartery disease (CAD), the number of deaths and cardiac events for whichdiabetes was listed as the underlying cause has been increased. Previousstudies have already shown that a normal myocardial perfusion scintigraphy(MPS) is related with a low cardiac rate after a year (less than 1%).Objective: To compare the event rate after four years of normal MPS inwomen with and without diabetes.Methods: We evaluated 2.500 consecutive patients (pts) who performedMPS in 1998, and 160 women with normal MPS were selected. The ptswere divided in two groups. Group I: 33 pts with diabetes and Group II:127 patients without diabetes. All MPS were performed using SPECTtechnique and sestamibi-Tc-99m as radioisotope. The studies withoutany perfusion defects in both stress/rest phases were considered normal.Death and Myocardial infarction were defined as hard events and CABGor PTCA as soft events in the follow up. The statistic analysis wasperformed using qui-square and Fisher tests. The logistic regression wasalso used to verify if diabetes could be considered as independentpredictor of cardiac event or only in addiction to any other cardiac riskfactors (RF).Results: Both groups had presented similar prevalence of RF. Onlyhypertension was more prevalent at the diabetic group (P�0,005). Thediabetic women group had presented higher hard event rate than non-diabetic group, 12,1% versus 2,4%, respectively (p�0,034). Most of theevents were observed soon after MPS (2-6 months). After the logisticregression analysis, diabetes was considered an independent predictor ofhard events in diabetic women. Comparing both groups about soft events,the diabetic women had presented more CABG in relation with non-diabeticwomen (12,1% versus 7%), but there was not significant statistic difference(p�0,217).Conclusion: The results may suggest that after a normal MPS, diabetes isthe only independent predictor of hard events and maybe non-invasivecardiac evaluation ought to be repeated within a period shorter.
5.17DOES CHRONOTROPIC INCOMPETENCE ADD INCREMENTALVALUE TO EXERCISE STRESS TEST IN DETECTING CORONARYARTERY DISEASE? COMPARISON WITH MYOCARDIALSCINTIGRAPHY AND ANGIOGRAPHYP Smanio, S Tebexreni, L Mastrocolla, R Meneghelo, A Thom, L PiegasInstituto Dante Pazzanese de Cardiologia. Sao Paulo, BrazilBackground: Several papers have shown the high number of falsepositive exercise stress tests (EST) in the detection of coronary arterydisease (CAD) in women. Myocardial perfusion scintigraphy (MPS)after pharmacological stress has already shown high value in detectingCAD. Diabetic women are considered at high risk of CAD even withoutcardiac symptoms.
S104 Abstracts Journal of Nuclear CardiologyJuly/August 2005

Objective: To verify if the chronotrophic incompetence (CI) adds informa-tion to the ST- segment analysis in the detection of CAD in diabetic womenwithout symptoms and to compare with the results of MPS.Methods: We analyzed, prospectively, 98 diabetic women who performedEST, MPS with dipyridamole and angiography (angio) within 2 months andwithout cardiac procedures between these studies. Angio was consideredabnormal (abnl) at the presence of at least one coronary artery withobstruction greater than 50%. EST was considered abnl at the presence ofST-segment change equal to or greater than 1,5 mm at peak exercise inrelation to rest. We calculate the CI by the standard equation: [peak heartrate (HR) - rest HR]/ [maximal age-predicted RH - rest HR] X 100. CI wasdefined as values � 80%. MPS was considered abnl if there were reversibledefects after the stress phase. We correlated the obtained results with theangio.The statistic analysis was performed by chi-square and Fisher testsand differences were considered significant at p�0,05.Results: From the 98 women, 67 had abnl EST and from those, 20 hadpresented abnl angio (31,2%),p�0,150. Sexty-two women had IC and fromthose, 29 (47%) with abnl angio, p�0,087. Both abnl EST and CI werepresent in 42 women ans from those, 30 (71,4%) had abnl angio, p�0,05.In the 42 pts of the group with abnl MPS, 39 (93%) presented an abnormalcine. p�0,001.Conclusion: The obtained results may suggest that CI adds informationto EST in order to identify CAD in non-symptomatic diabetic women,but pharmacological stress MPS has shown a better rate of CADidentification.
5.18PACEMAKER RELATED MYOCARDIAL PERFUSION DEFECTSWORSEN DURING HIGHER PACING RATE AND CORONARYFLOW AUGMENTATIONTJF ten Cate, FC Visser, NM Panhuyzen-Goedkoop, JF Verzijlbergen,NM van HemelSt. Antonius Hospital NieuwegeinBackground: Asynchronous activation resulting from RVA pacing canadversely affect left ventricular function and myocardial perfusion despitenormal coronary arteries. This troubles the detection of coronary heartdisease in paced patients.Methods: Fourteen patients with permanent RVA pacing with angiographi-cally normal coronary arteries underwent myocardial perfusion SPECT atrest with low and high pacing rate, and with pacing at low rates withadenosine. Data were analysed semi-quantitatively using a 20 segmentscoring model and coded using a 4-point scoring system.Results: At rest, 23 of 42 (55%) coronary flow territories showedabnormal perfusion and 52 of 280 (19%) corresponding segmentsdemonstrated abnormal perfusion; mean perfusion score 0.22. After highrate pacing, perfusion was abnormal in 31 of 42 (74%) flow territoriesand 122 of 280 (44%) segments: mean perfusion score 0.67. Adenosineinfusion resulted in 28 of 42 (67%) abnormal flow territories and 90 of280 (32%) abnormal segments; mean perfusion score 0.44. Perfusiondefects were most often observed in close proximity to the origin of thepacing site.Conclusion: RVA pacing results in myocardial perfusion defects. Thefalse-positive findings are present at rest and more outspoken with highrate pacing than during adenosine infusion. Detection of coronary arterydisease should be carried out with caution in RVA paced patientsbecause of the high number of perfusion defects in the absence ofcoronary artery disease.
5.19ARTEFACTUAL MYOCARDIAL PERFUSION DEFECTS IN RIGHTVENTRICULAR APICAL PACINGTJF ten Cate, FC Visser, NM van Hemel, JF VerzijlbergenSt. Antonius Hospital NieuwegeinBackground: It is generally accepted that myocardial perfusion is dimin-ished in patients with a right ventricular apical pacemaker. The regionsaffected are those with an abnormal contraction pattern. This study aims toassess the effects of abnormal contraction pattern on myocardial perfusionimaging.Methods: Eight patients with a permanent dual chamber pacemaker with aright ventricular apical lead for bradytachycardia syndrome were studied.All underwent myocardial perfusion SPECT at rest with technetium-99-sestamibi. Technetium-99m-sestamibi was injected at rest during normalatrio-ventricular (AV) conduction. Myocardial SPECT was performedduring AAI pacing with a rate of 5 above the resting heart rate and repeatedin DDD pacing mode with the same heart rate. The first pacing mode ofperfusion imaging was randomized.Results: Myocardial perfusion at rest with normal AV conduction wasnormal in 6 patients. The average summed rest score (SRS) was 0.875.During abnormal AV activation, myocardial perfusion was abnormal in 3patients. The SRS increased to 3. The summed motion (SMS) and summedthickness scores (STS) also increased from 3 to 7 and from 0.875 to 3.5.Conclusion: During normal atrio-ventricular conduction normal perfusionis found in most patients. Subsequent DDD-pacing obviously results in newperfusion defects despite the fact that tracer distribution is not changed. Thedefects are strongly related to abnormal wall motion and thickening. Whichsuggests that these perfusion defects must be caused by partial volumeeffect.
5.20COMBINED DIPYRIDAMOLE-EXERCISE TC-99M SESTAMIBIGATED SPECT MYOCARDIAL PERFUSION IMAGING: HOW DOESIT COMPARE TO STANDARD VASODILATOR OR EXERCISESTRESS IN RISK STRATIFICATION?J Thompsen, H Athar, V Sainani, D O’Sullivan, I Leka, GV HellerHartford Hospital, Hartford, CTBackground: The prognostic value of standard exercise (EX) and vasodi-lator (VASO) SPECT is well established. However, there are few data onthe utility of combining both modes of stress. We compared gated SPECTvariables, outcomes and risk stratification between patients undergoing EX,VASO, or dipyridamole-exercise (DIP-EX).Methods: After excluding patients who underwent PCI or CABG �60 daysafter gated SPECT, 10,718 consecutive patients who underwent EX(n�5683), VASO (n�3220), or DIP-EX (n�1815) with Tc-99m sestamibiMPI were evaluated. Selection of stress modality was based on theperceived ability to exercise. Follow-up was 86.3% complete over 29�18months. The patients had an age of 61�14 years, 49.9% were female and25.4% had a history of MI, PCI or CABG. Risk stratification was examinedusing the summed stress score (SSS) and post-stress ejection fraction (EF).Images were classified as normal (SSS�3 and EF�50%) or abnormal(SSS3 or EF�50%). Patients were followed for cardiac death (CD) ormyocardial infarction (MI).Results: A significant increase in the incidence of abnormal perfusion orfunction and worsening of SSS and EF was found between modes of stress,the lowest with EX and highest with VASO. The cumulative event rate was1.9%, 3% and 6.9% with EX, DIP-EX (p�0.01 versus EX) and VASO(p�0.001 versus EX and DIP-EX), respectively. With each mode of stress,
Journal of Nuclear Cardiology Abstracts S105Volume 12, Number 4;S2-S13

patients with abnormal images had a higher event rate than those withnormal images (p�0.01).
Conclusion: For patients with abnormal MPI, the ability to exercise duringdipyridamole stress is associated with a better prognosis than patientsundergoing vasodilator stress who may not be able to exercise. Effectiverisk stratification by combining exercise and vasodilator stress is possibleusing perfusion and function data from gated SPECT in patients with knownor suspected coronary artery disease.
5.21INCIDENCE OF PERFUSION ABNORMALITIES CONSIDERINGTHE DIFFERENT FORMS OF STRESS SELECTEDM Jansen, M Grasman, A Stier Jr, O Kormann, JA Silva, JV VitolaQuanta Medicina Nuclear, Curitiba – Brazil, Vrije Universiteit,Amsterdam - The NetherlandsBackground: Several stress alternatives are available for nuclear cardiologyand many are the factors influencing the physician�s decision of choosing oneversus another, including co-morbidities such as diabetes mellitus (DM) andage. We evaluated the presence of SPECT abnormalities, comparing itsincidence considering the different types of stress selected in a population ofoutpatients, with special attention to the influence of gender, age and DM.Methods and Results: All patients undergoing myocardial perfusionimaging (MPI) during a 6 months period at a nuclear laboratory in Brazilwere included (n� 986). Stress was accomplished in 1 of 3 ways: exercisealone (EX), dipyridamole plus exercise (DipEx) and dipyridamole alone(Dip). We found that most patients 677 (69%) were able to performtreadmill exercise, while 309 (31%) required pharmacologic stress, dividedin DipEx (n�175) and Dip (n� 135) groups. We found that 27% of patientsin the EX group had an abnormal scan, contrasting with 52% in the DipExand 47% in the Dip group (p�0,05). Patients with diabetes were more likelyto undergo a pharmacologic study compared to non-diabetics (43 vs 29%,p�0,001), however when diabetics were able to exercise they were lesslikely to have an abnormal study. Women were more likely to undergopharmacologic stress compared to men (p�0,001), however women had alower incidence of abnormal scans (36 vs 29%, respectively, p�0,02).Conclusion: The ability to exercise in a nuclear cardiology laboratory,defines a subgroup of patients much less likely to have an abnormal scan.Diabetics had a higher chance of requiring pharmacologic stimulation,however when able to exercise they were less likely to have an abnormalstudy compared to diabetics who required pharmacologic stress. Womenwere more likely to undergo a pharmacologic stress compared to men,however overall they showed a lower incidence of abnormal scans com-pared to men.
5.22INCIDENCE OF ABNORMAL MYOCARDIAL SPECT IN DIABETICPATIENTS REFERRED TO NUCLEAR CARDIOLOGY – IMPACT OFAGINGME Grasman, M Jansen, C Cunha, MS Cerci, OF Ribeiro, JV VitolaQuanta Medicina Nuclear, Curitiba - Brazil , Vrije Universiteit,Amsterdam - The NetherlandsBackground: Diabetes Mellitus (DM) and aging are factors known toaccelerate the development of coronary artery disease (CAD). We evaluatedthe incidence of myocardial abnormalities in diabetic patients, of differentages, referred to an outpatient nuclear cardiology laboratory.Methods and Results: All patients (n� 986) undergoing rest-stress 99mTc- MIBI myocardial perfusion imaging (MPI) during a 6 months period atour laboratory were included, prospectively, in a computer database,
allowing for retrospective review of different variables. Of these,181patients had a history of DM, while 805 had no history of DM. . DM patientshad a much higher incidence of abnormal scans compared to non-diabetics(49 vs 31% p�0,000). An abnormal MPI scan is based on any form ofischemia, scar, or a combination of the both. In the group of non-DM a nicepositive linear correlation was found between age and abnormal scans.There were striking differences in the incidence of MPI abnormalitiesbetween these 2 groups, to the point that non DM patients age 40-49 yo hadnear the same incidence of abnormal scans compared to non-DM patientsage � 80 yo.Conclusions: A positive linear increase on the incidence of abnormal scanswas found for non-DM patients with increasing age, however DM patientswere found to have a much higher incidence of abnormalities whencompared to the same age group. Abnormalities occurred at a much higherincidence at younger age in DM, to the point that DM patients age 40-49 hadthe same incidence compared to non DM age � 80 yo. These findingsjustify a more aggressive work up of DM patients at younger age comparedto non DM patients.
5.23DIFFERENCES IN THE INCIDENCE OF SPECT ABNORMALITIESIN WOMEN COMPARED TO MENMHA Jansen, ME Grasman, T Zukovski, C Mickevicz, F Visser, JV VitolaQuanta Medicina Nuclear, Curitiba - BrazilBackground: There are known gender differences in the incidence ofcoronary artery disease (CAD). In many parts of the world, there is atendency to apply technological advances to a lesser extent in womencompared to men, which may, at times, lead to an under estimation on thediagnosis of CAD in women. We evaluated differences in referral of womenand men to an outpatient nuclear cardiology laboratory in Brazil and howthe results compared between these 2 groups at different ages.Methods and Results: All patients undergoing myocardial perfusionimaging (MPI) during a 6 months period at nuclear laboratory in Curitiba-Brazil were included (n� 986). This group was subdivided into severalgroups of different ages. The number of women referred for evaluation wasmuch lower than men: 341 women (34%) and 645 men (66%) (p�0,001).An abnormal scan was defined as a result of any form of ischemia or scaror a combination of both. Despite women being 4 years older than men(64�12 vs 60�12 yo, p � 0.03)), men had a much higher incidence ofabnormal scans (36 vs 29%, p�0.02). The incidence of abnormal scans wasonly comparable to women 10 to 20 years older.Conclusion: Women were less likely to be referred to a nuclear cardiologystudy compared to men, and when referred they were older. The incidenceof abnormalities on MPI was lower for women. Compared to men, womenpresented the same incidence of abnormalities on MPI at an age 10 - 20 yearolder.
5.24IMPROVED PREDICTION OF HIBERNATING AND SCARREDTISSUE BY GATED MYOCARDIAL PERFUSION SPECT ANALYSISK Snyder, D Polepalle, KJ Nichols, U Dim, OO AkinboboyeCardiology, State University of New York Stony Brook, New YorkHypothesis: We hypothesized that hibernating and scarred myocardium canbe differentiated by wall thickening analysis using gated myocardiumperfusion SPECT and a 20-step linear color scale.Methods: Patients who underwent a clinically indicated dual isotope (restthallium, STRESS technetium sestamibi) gated myocardium perfusionSPECT, followed by 24 hour thallium imaging for viability assessment wererecruited if they had at least one perfusion defect with less than 50% uptakeand a fixed pattern on rest-stress perfusion analysis. Gated wall motionthickening analysis was performed on the stress sestamibi scan using QGSsoftware (Cedars-Sinai Medical Center, Los Angeles, California) with a20-step linear color scale. Each color transition represents a 5% change inwall thickness. Percent wall thickening was calculated based on the numberof color transitions from diastole to systole. Percent wall thickening insegments that subsequently showed evidence of significant redistribution on24 hours scans, consistent with hibernating myocardium, was comparedwith thickening in segments that failed to redistribute consistent with scar.Results: A total number of 30 patients with a total number of 36 fixeddefects were analysed. There were 14 viable segments and 22 nonviablesegments based on 24-hour redistribution scans. All 9 segments with �10%
S106 Abstracts Journal of Nuclear CardiologyJuly/August 2005

thickening (� 2-step color transitions) were viable and all 16 segments with5% or less thickening (1-step or no color transition) did not show anyevidence of viability. Of the 11 segments with 10% thickening (2-step colortransitions) 6 segments were not viable and 5 were non-viable.
% Wall Thickening Total segments % Viable
5 16 010 11 45
�10 9 100
Conclusions: Analysis of segmental percent wall thickening on stress scansusing gated myocardial perfusion SPECT and a sensitive 20-step linearcolor scale can differentiate between hibernating myocardium and scar. Thisapproach might be useful in guiding decisions to bring patients back for a24-hour scan to assess viability after a dual isotope stress perfusion study.
5.25DOES CORONARY ARTERY CALCIFICATION PREDICT THEEXTENT OF TRANSIENT ISCHEMIC DILATATION INASYMPTOMATIC DIABETIC SUBJECTS?D Vijay Anand, E Lim, K Nagar, U Raval, A LahiriCardiac Imaging and Research Centre, Wellington Hospital, London, U.KBackground: Transient ischemic dilatation (TID) of the left ventricle (LV) isa marker for severe multivessel coronary artery disease (CAD) that is associatedwith an adverse prognosis. Possible mechanisms of TID include myocardialstunning, nonvisualisation of an extensive amount of subendocardial myocar-dium due to ischemia and microvascular dysfunction. Diabetic patients have anincreased prevalence of endothelial dysfunction, coronary artery calcification(CAC) and myocardial ischemia. We prospectively evaluated the relationshipbetween CAC, myocardial perfusion and the extent of stress induced LVdilatation in asymptomatic uncomplicated type 2 diabetic patients.Methods: Risk factors and CAC scores were assessed in 510 patients (meanage 53�8 years, 61% males). Myocardial perfusion scintigraphy wasperformed in all subjects with CAC � 100 Agatston units (n � 127), anda random sample of the remainder (n � 53). A 2-day stress-rest 99mTcsestamibi protocol was used with combined dypyridamole infusion �maximal treadmill exercise. Perfusion was scored semiquantitatively usinga 17-segment model and the summed stress, rest and difference scores werecalculated. LV volumes and TID ratio were measured using automatedprograms (QGS/QPS, Cedars-Sinai, Los Angeles, U.S.A).Results: Significant CAC (� 10 Agatston units) was found in 46.3%.Perfusion abnormalities were seen in 57 patients (31.7%); 28.3% (n � 51)had reversible and 3.3% (n � 6) had fixed defects. No perfusion abnormal-ities were seen in patients with CAC � 10. Increasing CAC scores wereassociated with a greater prevalence/severity of myocardial perfusionabnormality. The extent of ischaemia was related to the change in LVend-diastolic (p � 0.009), end-systolic dimensions (p�0.0001) and ejectionfraction (p�0.0002) post stress. Mean TID ratio (SD) was highest inpatients with reversible ischaemia (1.21[0.09]) followed by those withnormal perfusion but CAC �10 (1.07[0.09]) and those with normalperfusion and CAC � 10 (0.98[0.07]) (p � 0.003).Conclusion: Increase in cardiac size following exercise stress is clearlyassociated with the extent of ischemia. No significant perfusion abnormal-ities or TID was seen in asymptomatic diabetic patients with CAC � 10Agatston units. CAC imaging may be helpful in identifying microvasculardysfunction and CAD in those diabetic patients with TID but normalmyocardial perfusion.
5.26ASSOCIATION OF MYOCARDIAL ISCHEMIA ON STRESS 99MTECHNETIUM TETROFOSMIN SPECT IMAGING WITH ALLCAUSE MORTALITY IN PATIENTS WITH DIABETES MELLITUSA Elhendy, A Huurman, AF Schinkel, JJ Bax, RT van Domburg, RValkema, D PoldermansThoraxcenter, Rotterdam, NLBackground: Stress myocardial perfusion imaging is a useful method forevaluation of coronary artery disease (CAD) in patients (pts) with diabetesmellitus. However, its role in predicting all cause mortality is not well defined.Aim of this study was to find whether myocardial ischemia on stress myocardialperfusion imaging can predict all cause of death in pts with diabetes mellitus.
Methods: We studied 297 pts with diabetes mellitus and known orsuspected CAD by dobutamine or exercise stress 99m technetium tetrofos-min myocardial perfusion SPECT. Ischemia was defined as reversibleperfusion abnormalities. End points were death from any cause and hardevents (cardiac death and non-fatal myocardial infarction).Results: An abnormal scan was detected in 179 (60%) pts. Myocardialperfusion abnormalities were fixed in 76 (26%) pts, and reversible in 103 (35%)pts. During a mean follow-up period of 6 � 2.1 y, 80 (27%) pts died. Nonfatalmyocardial infarction occurred in 14 (5%) pts. The annual mortality rate was2.5% in pts with normal perfusion, 4.5% in pts with fixed defects and 6% in ptswith ischemia. The annual cardiac death rate was 4.2% in pts with ischemia, and2.6% in pts with fixed defects. In pts with normal perfusion, the annual cardiacdeath rate was 0.9% during the 5 years following the stress test. In a Cox model,independent predictors of death were age (risk ration [RR] 1.04, 95% CI1.02-1.07), male gender (RR 1.9, CI 1.2-3), heart failure (RR 1.6, CI 1.1-2.5)and reversible perfusion defects (RR 1.9, CI 1.2-2.6).Conclusions: Myocardial ischemia on stress 99m technetium tetrofosminSPECT is associated with an increased risk of all cause mortality among ptswith diabetes mellitus. Pts with normal perfusion have a low cardiac deathrate during the 5 years following stress, and should not routinely undergorepeated testing, unless these is a change in their clinical status.
5.27OPTIMIZED RISK ASSESSMENT OF CORONARY DISEASE (CAD)PATIENTS BY ADDITIONAL EVALUATION OF POST ISCHEMICMYOCARDIAL STUNNING AMOUNT IN STRESS PERFUSIONIMAGINGSI Heiba, JA Katzel, E Altinyay, R Milarodovic, I Castellon, B Raphael,HA Abdel-Dayem, J CoppolaNuclear Medicine & Cardiovascular Services, St. Vincents Hospital &New York Medical College, New York, NYThe evaluation of stress-induced ischemia amount has been established as avaluable predictor of future cardiac events (CE). Patients with ischemia thatalso exhibit prolonged reversible myocardial stunning (stunning) in poststress gated SPECT studies (GSPECT) may be at higher risk for suchevents. We further explored the incremental prognostic value of the quantityof stunning measured by both wall motion (WM) & thickening (WT)changes to perfusion (MP) parameters in GSPECT.Methods: We evaluated 231 consecutive patients (age 64 � 12) withknown or suspected CAD (146 men) who underwent adenosine (120),dobutamine (39) or treadmill exercise (72) rest/stress Tc-99m sestamibiGSPECT. Of those, 12 patients with absent counts severe defects wereexcluded, & 20 patients were lost to follow-up. The remaining 199 patientswere followed up for a mean of 36 � 14 months. Myocardial segments weresemiquantitatively scored according to MP & regional contractility by WM&/or WT. MP & contractility summed stress, rest & difference (ischemia &stunning respectively) scores were determined for all patients.Results: Hard CE (cardiac death & infarction) & soft CE (angina & heartfailure requiring revascularization & hospitalization respectively) wereidentified in 18 & 40 patients respectively. History of infarction, diabetesmellitus, amount of ischemic, stunned, fixed hypoperfusion & dysfunctionalmyocardium were predictive of CE in univariate analysis. However, onlythe amount of ischemia & stunning were significant in multivariate Coxanalysis for hard & soft CE (also fixed dysfunctional amount in soft CE).Patients’ classification according to combined ischemia & stunning quantityrevealed further significant predictive power of CE as shown in figure.
Conclusions: The amount of stunning detected during post stress GSPECThas important & independent prognostic value. The integration of suchinformation to the amount of ischemia can further enhance risk stratificationof CAD patients.
Journal of Nuclear Cardiology Abstracts S107Volume 12, Number 4;S2-S13

5.28ANGINAL SYMPTOMS ARE NOT PREDICTIVE OF MYOCARDIALPERFUSION OR FUNCTION IN DIABETICSTF HestonNorthwest Molecular, Kellogg, IdahoBackground: Patients with diabetes are more than twice as likely to diefrom coronary artery disease than non-diabetics. Deciding which diabeticpatients require an aggressive workup, however, is challenging becausetheir diabetic neuropathy may mask anginal symptoms. Thus, in diabetics,initiating a workup for coronary artery disease based exclusively on thepresence or absence of symptoms alone may not be ideal. The objective ofthis study was to help determine whether or not the presence of anginalsymptoms in diabetics can predict abnormal myocardial perfusion orfunction.Methods: A retrospective review was made of 1074 consecutive patientspresenting to an outpatient clinic for myocardial perfusion imaging. Clinicalvariables obtained included a history of hypertension, hyperlipidemia, apositive family history of coronary artery disease, diabetes, and smoking.Patients were categorized as asymptomatic if they had either no symptomsat all, or had nonanginal chest pain according to the Diamond and Forrestercriteria. Patients were categorized as having angina if they had eithersuspected or definite angina (i.e. atypical or typical chest pain). Thesevariables were then correlated with the scan findings of the summed stressscore (SSS), summed difference score (SDS), left ventricular ejectionfraction (LVEF), and the ratio of the post-stress to rest end systolic volume.Gated SPECT images were obtained using a single headed camera. TheCedars-Sinai QGS program was used to measure ventricular size andfunction.Results: The average patient age was 63 �/- 13 years; 51% were men, and21% were diabetic. Among all patients, the presence or absence of anginawas significantly correlated with the SSS (p�0.043), the SDS (p�0.040),and the post-stress LVEF (p�0.001). However, among diabetics, anginalsymptoms were not correlated with the SSS (p�0.795), the SDS (p�0.888),or the post-stress LVEF (p�0.223). Diabetics as a group (both asymptom-atic and symptomatic) were more likely to have an elevated SSS (p�0.006),an elevated SDS (p�0.001), and an elevated post-stress to rest end systolicvolume ratio (p�0.013).Conclusion: Among all patients, the presence of anginal symptoms isstrongly correlated with abnormal myocardial perfusion and function. Indiabetics, however, anginal symptoms do not help predict whether or notmyocardial ischemia or ventricular dysfunction is present. A symptom-based algorithm for the workup of coronary artery disease in diabetics islikely to be ineffective.
5.29ARE ALL LOW RISK STABLE ANGINA PECTORIS PATIENTS ATLOW RISK?PF Høilund-Carlsen, A Johansen, W Vach, HW Christensen, M Møldrup,T HaghfeltDepartment of Nuclear Medicine, Odense University Hospital, DenmarkBackground: In most guidelines for management of patients with stableangina pectoris it is stated that patients with a low risk of coronary arterydisease according to clinical evaluation and estimation of pretest likelihoodof disease need not undergo stress testing including radionuclide myocardialperfusion imaging (MPI). We wanted to test the reliability of this dictum inthe era of invasive intervention for acute coronary syndromes.Methods: In a prospective series of 507 of 972 patients referred consecu-tively to coronary angiography (performed in 476) for known or suspectedstable angina pectoris, we selected three groups of patients being at low risk,i.e. having non-cardiac or no chest pain (n�83) instead of atypical or typicalangina, Canadian Cardiovascular Society grade �1 chest pain (n�227) ora low pretest likelihood of coronary artery disease judged from type of pain,age, and gender (n�71) as originally proposed by Diamond and Forrester 25years ago and recommended by current guidelines. Patients fulfilling allthree criteria (n�54 of whom 48 underwent angiography) were consideredto be at very low risk. The value of a normal resting electrocardiogram wasalso examined. MPI was performed in all patients on the day of clinicalexamination.Results: In the three separate groups, we found that 31%/12%, 36%/13%,and 29%/16% of male/female patients had reversible perfusion defects, andthat 36%/15%, 41%/14%, and 39%/15%, respectively, had significant
coronary artery disease. In patients fulfilling all three criteria, the corre-sponding rates were 29%/15% and 39%/20%, respectively. In patients witha normal electrocardiogram at rest, 36% had reversible perfusion defectsand 43% had significant coronary artery disease.Conclusion: It appears that standard clinical evaluation including estima-tion of pretest likelihood cannot reliably identify angina pectoris patientsbeing at low risk. This suggests that the population of stable angina pectorispatients has changed over the years and that recommended systems forclinical evaluation and estimation of pretest likelihood of disease in thiscategory of patients may no longer be as predictive as expected.
5.30RELATIONSHIP BETWEEN SYMPTOMS AND MYOCARDIALPERFUSION BEFORE AND AFTER REVASCULARIZATION INPATIENTS WITH STABLE ANGINA PECTORISA Johansen, PF Høilund-Carlsen, W Vach, HW Christensen, M Møldrup,T HaghfeltDepartment of Nuclear Medicine, Odense University Hospital, DenmarkBackground: In stable angina patients, revascularization has been proven toalleviate symptoms. From a pathophysiologic point of view, reversal ofperfusion abnormalities by revascularization should be the fundament ofangina relief. We wanted to examine the association between changes inchest pain and changes in perfusion status before and after revascularizationas assessed by clinical evaluation and myocardial perfusion imaging (MPI).Methods: A prospective series of 144 patients (31 females) with a mean ageof 60.3 �7.9 years underwent coronary revascularization for stable anginapectoris. MPI was performed before angiography and again two years later.The decision of invasive management was based exclusively upon historyand findings at coronary angiography since the result of MPI was keptsecret. Change in type and severity of angina versus change in perfusion(summed stress score) before and two years after revascularization wererecorded.Results: Initially, 107 (74%) patients had typical and 27 (19%) atypicalangina pectoris, while 3 (2%) had non cardiac chest pain and 7 (5%) had nopain. At follow-up, respective numbers were 29 (20%), 23 (16%), 12 (8%)and 80 (56%). Mean severity of pain (Canadian Cardiovascular Society(CCS) grades 0-4) was reduced from 1.79 �0.73 to 0.63 � 0.79 (p �0.0001). The number of patients with inducible ischaemia (reversible ormixed perfusion defects) was reduced from 111 (77%) to 42 (29%) (p �0.026). A change in summed stress score was significantly associated withan improvement in pain status (p � 0.0001) as well as CCS classification(p � 0.022).Conclusion: Mitigation of stable angina two years following revasculariza-tion is associated with improvements in perfusion.
5.31PROGNOSTIC VALUE OF MYOCARDIAL PERFUSION IMAGINGIN PATIENTS WITH KNOWN OR SUSPECTED STABLE ANGINAPECTORISA Johansen, PF Høilund-Carlsen, W Vach, HW Christensen, M Møldrup,T HaghfeltDepartment of Nuclear Medicine, Odense University Hospital, DenmarkBackground: Almost all previous investigations on the prognostic value ofMPI were in a setting, in which the test result was known to the patient’sphysician. In the present study, we wanted to study prospectively in patientswith known or suspected stable angina, the prognostic value of MPI in asetting in which MPI could not influence the diagnostic and therapeuticstrategy.Methods: A prospective series of 507 patients referred to coronaryangiography for known or suspected stable angina were included. MPI wasperformed before angiography. Management was based on symptoms andangiographic findings, since the results of MPI were not communicated.Patients were followed in mean 45.3 � 7.7 months.Results: During follow-up, 20 (3.9%) patients had myocardial infarction, 19(3.7%) died and 8 (1.6%) were revascularized �1 year after MPI resultingin a combined annual event rate of 2.5%. Patients with normal MPI had alow annual event rate of 1.6% (or 1.1% regarding only risk of myocardialinfarction or death). In contrast, event rates in patients with reversible ormixed ischaemia were 4% per year. MPI added value to the clinical data ina Cox proportional hazards analysis. In an univariate model, the prognosticsignificance of an abnormal versus a normal MPI expressed as the hazards
S108 Abstracts Journal of Nuclear CardiologyJuly/August 2005

ratio was 2.6 and 2.8 when comparing summed stress score (SSS) �8 withSSS �8. After adjusting for age or sex or other covariates the prognosticvalue of MPI was still high with hazards ratio of 2.2 to 2.4 (p � 0.018 top � 0.003). However, when adjusting for all four covariates, the hazardratio was 1.7 (p � 0.082). In non-revascularized patients (n � 326) therewere only 17 events. Using SSS 0-8 and SSS8 to evaluate the prognosticpower of MPI with sex and age as covariates, the hazards ratios for MPI inthe univariate analysis and for MPI adjusted for sex only, for age only andfor both sex and age were 4.6 (p � 0.003), 4.2 (p � 0.006), 5.1 (p � 0.001)and 4.3 (p � 0.006), respectively.Conclusion: In a setting in which MPI could not influence the diagnosticand therapeutic strategy we could confirm that MPI is a valuable riskstratifying tool.
5.32FRAGMENTED QRS COMPLEXES NOT RELATED TO TYPICALBUNDLE BRANCH BLOCK: A MARKER OF REGIONALMYOCARDIAL SCAR BY SPECTBR Khan, A Kumar, S Stricker, MK Das, J MahenthiranIndiana University, Indianapolis, INBackground: Terminal QRS conduction delay with fragmented QRS(FQRS) complexes on electrocardiography (EKG) is thought to be due toaltered ventricular depolarization surrounding a myocardial scar. However,the extent of scar by SPECT corresponding to FQRS complexes (RSR’variants), not related to a typical bundle branch block (BBB), is not known.Methods: EKG’s of 501 patients (pts) referred for stress SPECT wasanalyzed. FQRS was defined as QRS duration �120 ms, with more than oneR wave on two contiguous coronary region leads. Regional scar by SPECTwas defined as sum stress (SSS) and sum rest scores (SRS) of � 3 and a sumdifference score � 3 to the corresponding coronary region, using thestandard 17-segment 5-point scale. Left ventricular (LV) function, summotion (SMS) and volumes were obtained. Pts with a typical BBB (n�26),paced rhythm (n�2) and Q-waves (n�64) were excluded.Results: In 409 pts (47% CAD), 155 (38%) had FQRS complexes and 107(69%) of them had a regional scar. FQRS complexes had 75% sensitivity,94% specificity, 88% PPV and 84% NPV for a scar. Regional FQRS had65-75% sensitivity, and 94-96% specificity for a corresponding SPECTregional scar. FQRS pts were more males, had higher regional SSS, globalSSS, SRS, SMS and end-diastolic volumes; and a lower LV ejectionfraction when compared to the no FQRS pts (see table).
VariableFQRS
(n�155)No FQRS(n�254) p-value
Age (years) 57 � 12 58 � 13 0.3Male (%) 112 (72%) 102 (40%) �0.001Sum Stress Score (SSS) 7.8 � 8.2 2.1 � 3 �0.001Sum Rest Score (SRS) 5.9 � 7.9 1.6 � 2 �0.001Sum Difference Score (SDS) 2 � 3.4 0.6 � 2 �0.001LV Diastolic Volume (cc) 126 � 56 93 � 32 �0.001Total Sum Motion Score (SMS) 6.2 � 9 1 � 2.7 �0.001LV Ejection Fraction (%) 54 � 13 63 � 9 �0.001SPECT regional scar (%) 107 (69%) 29 (11%) �0.001LAD SSS (% Scar) 3 � 4.4 (75%) 0.7 � 1.2 (4%) �0.001LCX SSS (% Scar) 1.5 � 3.1 (72%) 0.3 � 1 (1.2%) �0.001RCA SSS (% Scar) 4.1 � 3.6 (65%) 1.1 � 2 (5.8%) �0.001
Conclusion: FQRS complexes, not related to a typical BBB, in the absenceof a Q wave, is a highly specific marker of a regional scar in CAD pts. FQRSpts have greater perfusion and functional abnormalities, and more focalregional myocardial scar by SPECT.
5.33EFFECT OF PATIENT POSITIONING ON LEFT VENTRICULARFUNCTIONAL AND VOLUMETRIC MEASUREMENTS BYQUANTITATIVE GATED CARDIAC SPECTCV Oddis, D Byrne, JS Myers, AL Churchwell, KB ChurchwellVanderbilt Page-Campbell Heart Institute - Vanderbilt University MedicalCenter, Nashville, TNBackground: Left Ventricular (LV) ejection fraction (EF) is a crucialparameter for assessing the severity of cardiac disease, determining thepatient’s prognosis, and determining if the patient will benefit from deviceand/or pharmacologic therapy. More recently, LV mass, LV volume, andtransient ischemic dilation (TID) have also been shown to provide diagnos-
tic and prognostic information on the severity of a patient’s cardiovasculardisease. A comparison of patient positioning and how these parametersmaybe affected has not been studied. The purpose of this study was tocompare the effects of supine or reclining (20 degrees) patient positioningon LVEF, LV mass, LV volume, cardiac output (CO), and TID.Methods: We examined 57 consecutive patients who underwent exercise orpharmacologic stress testing for evidence of myocardial ischemia. The patientsunderwent a resting sestamibi gated SPECT study randomly assigned to asupine (Siemens E.Cam) or reclining (Siemens C.Cam) position and thenimmediately re-imaged in the second position. The patients then underwent astandard, same day, exercise or pharmacologic stress study and imaged usingstandard time intervals in the supine and reclining positions. LVEF, LVvolumes, CO, and TID were calculated from the gated SPECT data bycommercially available software (4DM-SPECT). Bland-Altman and pairedsample 2 tailed t-test analyses were employed for data analysis.Results: The mean difference between supine and reclining patient posi-tions were 2.95�/-0.70% for LVEF, 1.12�/-1.25g for LV mass, 0.93�/-1.26ml for LV end diastolic volume, 3.21�/-0.67ml for LV end systolicvolume, 1.84�/-0.10L/min for CO, and 0.04�/-0.03 for TID. There was asignificant statistical difference in LVEF and LV end systolic volume(p�0.01) between the two patient positions. There was no significantstatistical difference in LV mass, CO, LV end diastolic volume, and TID.Conclusions: This study reveals a statistical difference in LVEF and LVend systolic volume between supine and reclining patient positions. Thedifference is small (�5% for LVEF) and well within an acceptablerange. Comfortable placement of the patient in the reclining positionshould limit motion artefact and make gated cardiac SPECT available topatients with conditions such as severe degenerative joint disease anddecompensated heart failure, who are unable to lie comfortably in thesupine position.
5.34A HYPERTENSIVE RESPONSE TO EXERCIE IS ASSOCIATEDWITH A HIGH PREVALENCE OF TRANSIENT ISCHEMICDILATION IN PATIENTS WITHOUT SIGNIFIGANT PERFUSIONDEFECTS ON MYOCARDIAL PERFUSION SPECT IMAGINGDE Virnich, KA Williams, RP WardUniversity of Chicago, Chicago, ILBackground: Transient ischemic dilation (TID) of the left ventricle (LV) isassociated with future cardiac events even in patients with normal myocar-dial perfusion. A hypertensive response to exercise (HRE) is associatedfalse positive stress echocardiograms and defects on myocardial perfusionSPECT (MPS) imaging even in the absence of obstructive CAD. Our goalwas to study the prevalence of TID in pts with HRE and without significantmyocardial perfusion abnormalities.Methods: In this case control study, we retrospectively identified 230 ptswithout resting LV dilation with a summed stress score (SSS) � 4. 115 pts(cases) experienced a HRE (peak SBP210 mmHg for men, � 190 mmHg forwomen, or an increase in DBP � 10mmHg � peak DBP �90 mmHg), and115 controls without an HRE matched for age, gender, and resting systolicblood pressure (SBP), were included. Comorbidities and cardiac risk factorswere recorded and pre-test Framingham risk (FR) was calculated. TID wasdetermined using a validated quantification program and was defined as astress to rest ratio of �1.22.Results: The study group was well matched with a mean age of 55.3 yrs,54% female and had a mean resting SBP of 139 mmHg. Cases and controlswere also similar in diabetes, hypertension, hyperlipidemia, tobacco use,family history of CAD, BMI, prior CAD (p�NS for all), and pre-test FR(FR � 5%: 29% vs 30%; FR � 20%: 38% vs 37%, p�NS for both).Exercise MPS results are listed in Table 1. A HRE was associated with atrend toward a higher mean stress to rest ratio [R/S] (1.12 vs 1.08, p�0.09)and significantly more TID (26.1% vs 12.2%, p � 0.01), than no HRE. Onmultivariate analysis considering age, risk factors, and exercise results, anHRE (OR 2.19 [1.06-4.52], p�0.03), pre test Framingham risk (OR 1.27[1.02-1.57], p�0.03), and a lower Duke treadmill score (OR 0.91 [0.84-0.98], p�0.02), were the only independent predictors of TID.Conclusion: A HRE is associated with a high prevalence of TID, and isan independent predictor of TID in patients without significant perfusiondefects, possibly due to global subendocardial ischemia induced by aHRE. Further study is needed to determine the effect of HRE oncardiovascular prognosis in patients with TID and without significant
Journal of Nuclear Cardiology Abstracts S109Volume 12, Number 4;S2-S13
perfusion abnormalities.
Table 1. HRE No HRE P value
Mets 9.1 8.8 NSEx time 7.4 8.1 0.07ECG pos 25.2% 14.7% 0.05DTS 5.7 7.2 0.01SSS � 0 59.1% 61.0% NSLVEF 68.9% 70.0% NSR/S mean 1.12 1.08 0.09TID � 1.22 26.1% 12.2% �0.01
5.35CORRESPONDENCE OF GATED BLOOD POOL SPECT TO MRIREGIONAL LV FUNCTION MEASUREMENTSKJ Nichols, U Dim, Y Wang, OO AkinboboyeSt. Francis Hospital, Roslyn, NYBackground: One of the advantages of gated blood pool SPECT (GBPS)imaging over planar (i.e., non-tomographic) blood pool imaging is itspotential to provide not only more accurate global ejection fraction (EF)measurements by eliminating left atrial activity, but also to provide fullythree-dimensional regional EF values. We hypothesized that GBPS regionalleft ventricular (LV) EF measurements should demonstrate a significantcorrespondence to regional LV function as assessed by cardiac magneticresonance (CMR) imaging.
Methods: GBPS data were compared to True-FISP CMR images for 13subjects (age�64�8 years; 92% male; 10 with prior MI and 3 withnon-ischemic cardiomyopathy). CMR regional wall motion (WM) inmillimeters was assessed by an experienced observer who manually drewLV contours at end-diastole and end-systole for short-axis CMR tomo-graphic levels. GBPS regional EF in % was calculated automatically by acount-threshold algorithm (“BP-SPECT,” Columbia University, New York,NY), with volumetric counts sampled for the same 17 segmental territoriesas are routinely defined for gated myocardial perfusion studies.Results: Free wall GBPS EF correlated with CMR WM as r�0.80, N�110(see Figure), significantly more strongly (p�0.01) than when basal andseptal segments were included (r�0.66, N�221). GBPS regional EF wasmost strongly associated with CMR WM for apical segments, specifically,with linear regression Pearson r�0.89 (p�0.0001) and Spearman’s rankcorrelation coefficient�0.78 (p�0.005; 95% confidence interval � 0.40-0.93). There were no differences between manual and automatic GBPSregional EF’s (paired t-test p�0.24), which correlated well with one another(r�0.95), and both of which correlated with CMR WM equally well(r�0.80 for both).Conclusion: Automated GBPS regional LV EF closely paralleled CMRregional WM determinations, though more strongly for the free wall than forseptal and basal territories.
5.36GATED BLOOD POOL SPECT RIGHT VENTRICULAR FUNCTIONMEASUREMENTS IN PATIENTS WITH PRIOR-MI AND CHFKJ Nichols, U Dim, Y Wang, OO AkinboboyeSt. Francis Hospital, Roslyn, NYBackground: Previously we reported the validation by cardiac magneticresonance (CMR) of gated blood pool SPECT (GBPS) right ventricular(RV) function calculations in patients with primary arterial hypertension(PAH) and tetralogy of Fallot (TOF) (J Nucl Card 2002;9:153-60), forwhom the RV is expected to be markedly abnormal. The objective of thisinvestigation was to determine whether similar results are obtained forpatients with prior-MI and/or CHF, who would be expected to have a lesssevere degree of RV dysfunction.Methods: GBPS data were compared to True-FISP CMR images for a distinctgroup of 38 patients (age�59�13 years; 84% male), 95% of whom had eitherprior-MI or CHF, but none of whom had PAH or TOF. CMR RV ejectionfraction (EF), end-diastolic volume (EDV) and end-systolic volume (ESV)values were obtained from manual drawings of short-axis outlines at alltomographic levels. GBPS values were calculated automatically by a count-threshold algorithm (“BP-SPECT,” Columbia University, New York, NY).
Results: GBPS and CMR RVEF’s were similar (47�9% versus 49�9%;p�0.86). Correlation of GBPS to CMR RVEF was similar (p�0.89) for thisMI/CHF population (r�0.82, N�38; see Figure) as for patients with PAH(r�0.85, N�28). Bland-Altman limits of agreement were �9% to -13%(mean -2%). GBPS and CMR RVEDV’s and RVESV’s were not different(144�41ml versus 153�35ml; p�0.30 and 74�34ml versus 80�33ml;p�0.85). Correlation of GBPS to CMR RVESV was similar for thisMI/CHF population (r�0.87, N�38) as for patients with PAH (r�0.93,N�28), but correlation of GBPS to CMR RVEDV was significantly weaker(p�0.003) for this MI/CHF population (r�0.74, N�38) compared topatients with PAH (r�0.94, N�28).Conclusion: GBPS RVEF correlated to CMR values similarly to previouslyreported values, but RV end-diastolic volumes correlated less strongly,possibly reflecting the smaller range of RV end-diastolic volume values forthe patient population studied in the current investigation.
5.37IDENTIFICATION OF OPTIMAL GATED BLOOD POOL SPECTVENTRICULAR FUNCTION PARAMETERS TO DETECT CHFKJ Nichols, U Dim, SR Bergmann, OO AkinboboyeSt. Francis Hospital, Roslyn, NYBackground: Gated blood pool SPECT (GBPS) methodology enablescomputation not only of global ejection fraction (EF), and end-diastolic andend-systolic volumes (EDV and ESV), but also of diastolic functionparameters and regional EF values for both the left ventricle (LV) and rightventricle (RV). This investigation was undertaken to determine whethernewer RV and/or LV diastolic function and/or regional parameters areeffective at identifying patients with CHF.
S110 Abstracts Journal of Nuclear CardiologyJuly/August 2005
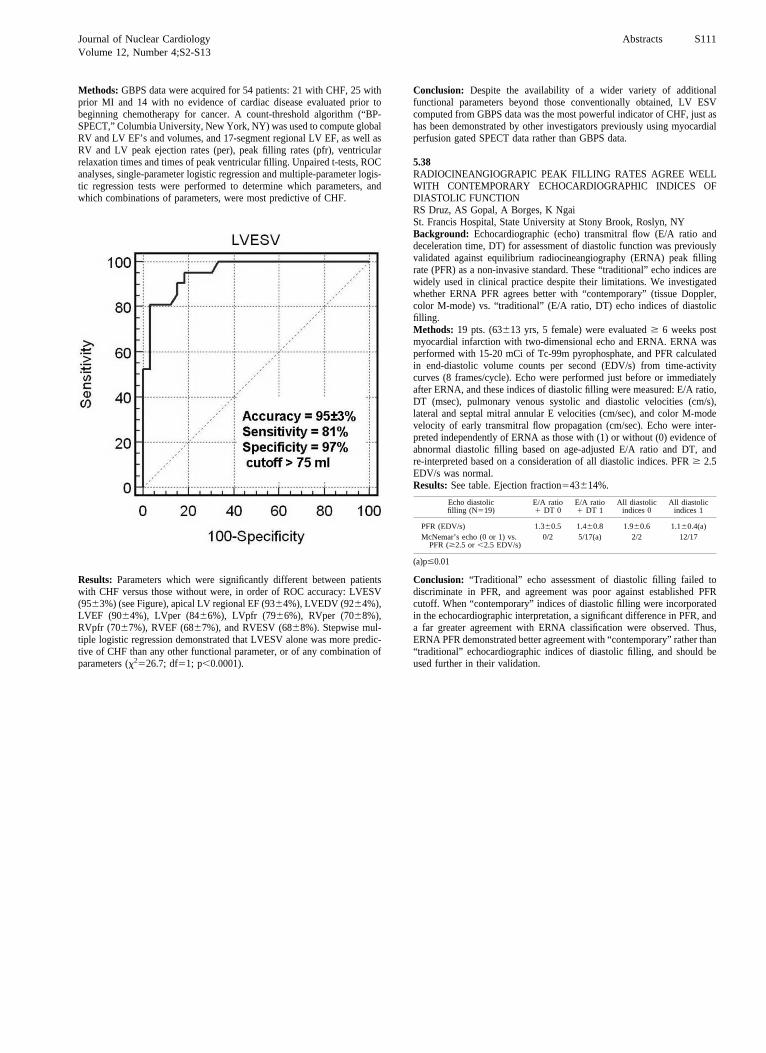
Methods: GBPS data were acquired for 54 patients: 21 with CHF, 25 withprior MI and 14 with no evidence of cardiac disease evaluated prior tobeginning chemotherapy for cancer. A count-threshold algorithm (“BP-SPECT,” Columbia University, New York, NY) was used to compute globalRV and LV EF’s and volumes, and 17-segment regional LV EF, as well asRV and LV peak ejection rates (per), peak filling rates (pfr), ventricularrelaxation times and times of peak ventricular filling. Unpaired t-tests, ROCanalyses, single-parameter logistic regression and multiple-parameter logis-tic regression tests were performed to determine which parameters, andwhich combinations of parameters, were most predictive of CHF.
Results: Parameters which were significantly different between patientswith CHF versus those without were, in order of ROC accuracy: LVESV(95�3%) (see Figure), apical LV regional EF (93�4%), LVEDV (92�4%),LVEF (90�4%), LVper (84�6%), LVpfr (79�6%), RVper (70�8%),RVpfr (70�7%), RVEF (68�7%), and RVESV (68�8%). Stepwise mul-tiple logistic regression demonstrated that LVESV alone was more predic-tive of CHF than any other functional parameter, or of any combination ofparameters (�2�26.7; df�1; p�0.0001).
Conclusion: Despite the availability of a wider variety of additionalfunctional parameters beyond those conventionally obtained, LV ESVcomputed from GBPS data was the most powerful indicator of CHF, just ashas been demonstrated by other investigators previously using myocardialperfusion gated SPECT data rather than GBPS data.
5.38RADIOCINEANGIOGRAPIC PEAK FILLING RATES AGREE WELLWITH CONTEMPORARY ECHOCARDIOGRAPHIC INDICES OFDIASTOLIC FUNCTIONRS Druz, AS Gopal, A Borges, K NgaiSt. Francis Hospital, State University at Stony Brook, Roslyn, NYBackground: Echocardiographic (echo) transmitral flow (E/A ratio anddeceleration time, DT) for assessment of diastolic function was previouslyvalidated against equilibrium radiocineangiography (ERNA) peak fillingrate (PFR) as a non-invasive standard. These “traditional” echo indices arewidely used in clinical practice despite their limitations. We investigatedwhether ERNA PFR agrees better with “contemporary” (tissue Doppler,color M-mode) vs. “traditional” (E/A ratio, DT) echo indices of diastolicfilling.Methods: 19 pts. (63�13 yrs, 5 female) were evaluated � 6 weeks postmyocardial infarction with two-dimensional echo and ERNA. ERNA wasperformed with 15-20 mCi of Tc-99m pyrophosphate, and PFR calculatedin end-diastolic volume counts per second (EDV/s) from time-activitycurves (8 frames/cycle). Echo were performed just before or immediatelyafter ERNA, and these indices of diastolic filling were measured: E/A ratio,DT (msec), pulmonary venous systolic and diastolic velocities (cm/s),lateral and septal mitral annular E velocities (cm/sec), and color M-modevelocity of early transmitral flow propagation (cm/sec). Echo were inter-preted independently of ERNA as those with (1) or without (0) evidence ofabnormal diastolic filling based on age-adjusted E/A ratio and DT, andre-interpreted based on a consideration of all diastolic indices. PFR � 2.5EDV/s was normal.Results: See table. Ejection fraction�43�14%.
Echo diastolicfilling (N�19)
E/A ratio� DT 0
E/A ratio� DT 1
All diastolicindices 0
All diastolicindices 1
PFR (EDV/s) 1.3�0.5 1.4�0.8 1.9�0.6 1.1�0.4(a)McNemar’s echo (0 or 1) vs.
PFR (�2.5 or �2.5 EDV/s)0/2 5/17(a) 2/2 12/17
(a)p�0.01
Conclusion: “Traditional” echo assessment of diastolic filling failed todiscriminate in PFR, and agreement was poor against established PFRcutoff. When “contemporary” indices of diastolic filling were incorporatedin the echocardiographic interpretation, a significant difference in PFR, anda far greater agreement with ERNA classification were observed. Thus,ERNA PFR demonstrated better agreement with “contemporary” rather than“traditional” echocardiographic indices of diastolic filling, and should beused further in their validation.
Journal of Nuclear Cardiology Abstracts S111Volume 12, Number 4;S2-S13

POSTER SESSION IISATURDAY, OCTOBER 1, 2005, 11:30–1:30PM
34.01AUTOMATED QUALITY CONTROL OF EMISSION-TRANS-MISSION MISALIGNMENT FOR ATTENUATION CORRECTION INMYOCARDIAL PERFUSION IMAGING WITH SPECT-CT SYSTEMSJ Chen, SF Caputlu-Wilson, H Shi, JR Galt, TL Faber, EV GarciaEmory University School of Medicine, Atlanta, GABackground: Emission-transmission misalignment can be seen in myo-cardial perfusion imaging with SPECT-CT systems and impairs theaccuracy of attenuation correction (AC). This study is to developautomated quality control (Auto-QC) to detect the critical misalignmentthat may impact AC.Methods: Auto-QC segmented the myocardium from emission recon-struction and the lung and mediastinum from attenuation map, respec-tively. A QC index (QCI) was calculated as the fraction of myocardialpixels either moving into the lung or moving out of the mediastinum. ANCAT (NURBS-based cardiac torso phantom) simulation study wasused to determine a QCI threshold above that the misalignment wouldcritically impact AC. The simulated attenuation map was shifted by 0.5,1, 1.5, and 2 pixels (6.4 mm/pixel) along either x (left or right) or y (upor down) axes, and 0.5 and 1 pixels along both axes (up-left, up-right,down-left, down-right), respectively. Visual comparison of the ACimages using the shifted attenuation maps with the AC images using theunshifted attenuation map by a blinded physician indicated the shifts thatsignificantly distorted the AC images, and then the QCI thresholddetermined. Auto-QC was tested with 22 patient studies acquired by aGE Millennium VG/Hawkeye SPECT-CT system. Visual assessment ofthe emission and transmission images of these patients by a blindedphysicist was used to check the Auto-QC accuracy.Results: The simulation showed that a one-pixel shift, no matter in whichdirection, resulted in artifacts in the AC images. Artifacts appeared atdifferent locations for different directions. With the determined QCIthreshold (3%), Auto-QC detected the critical misalignment concordantlywith the visual QC (sensitivity: 1.00, specificity: 0.82).Conclusion: The QCI calculated by Auto-QC quantitatively indicatedthe significance of emission-transmission misalignment. Auto-QC withthe QCI threshold yielded concordant results with the visual QC. TheQCI threshold should next be confirmed with patient studies and theAuto-QC algorithm should next be prospectively validated with a largegroup of patient studies.
34.02USE OF MULTIWIRE GAMMA CAMERA WITH NOVEL MOTIONCORRECTION TO EXAMINE ADAPTATION TO TREADMILLEXERCISEV Cole, R Habtemarkos, L Sun, J Lacy, J Heo, AE IskandrianUniversity of Alabama at Birmingham Medical Center, Birmingham, ALBackground: Previous radionuclide imaging studies examined cardiovas-cular adaptation to bicycle exercise with Tc-99m-labeled tracers and gatedor 1st pass radionuclide angiography [RNA]. The treadmill studies wereoften limited by patient motion. However, treadmill is the preferred exercisemodality due to greater sensitivity in the detection of coronary disease aswell as the elicitation of greater hemodynamic stress. Furthermore, exerciseLV function is an important prognostic predictor of cardiovascular events inhigh-risk patients. This study used 1st pass RNA to examine the changes inLV and RV EF and volumes and cardiac output [CO] with a short livedtracer [Ta-178] and a multiwire camera specially equipped with a 3Dalgorithm for motion correction.Methods: There were 25 men and 25 women with a mean age of 50years who all had normal SPECT perfusion images. None had chest painor ST changes during the symptom-limited treadmill exercise test. 1st
pass RNA was obtained at rest and peak exercise. A novel motioncorrection algorithm used an electromagnetic position/orientation track-ing system with a sensor output that consists of 6 degree-of-freedom(6-DOF) position information.
Results: The % mean and standard deviation of changes in HR, SBP, strokevolume [SV], CO, LV end diastolic volume [EDV], and LV end systolicvolume [ESV] are listed in the table with the absolute increases andcorresponding standard deviations of LVEF and RVEF. There were nosignificant differences between men and women. There were significantincreases from rest to peak exercise in HR [P�0.01], SBP [P�0.01], LVEF[P�0.01], RVEF [P�0.01], SV [P�0.01], CO [P�0.01], EDV [P�0.01]and ESV [P�0.09 men, P�0.05 women].
LVEF RVEF HR SBP SV CO EDV ESV
Men 12�9% 10�8% 69�20% 30�14% 98�63% 226�90% 65�52% 23�56%
Women 8�9% 8�9% 68�23% 24�10% 78�60% 196�87% 57�57% 26�72%
The change in EDV was greater than the change in ESV in men and womenaccounting for the increase in EF [P�0.001 each].Conclusions: The multiwire camera with its novel motion correctionalgorithm makes it possible to examine the pertinent physiologicalmeasurements during upright treadmill exercise that were not possiblebefore due to patient motion. There are no gender-related differences incardiovascular adaptation to exercise in this selected group of normalpatients.
34.03COMPARISON OF ATTENUATION CORRECTION IN MYO-CARDIAL SPECT USING GADOLINIUM-153 LINE SOURCES ORLOW-DOSE CTA Kjaer, A Cortsen, M Federspiel, S Holm, M O’Connor, B HesseDepartment of Clinical Physiology, Nuclear Medicine & PET,Rigshospitalet, University of Copenhagen, DenmarkBackground: The aim was on a head-to-head basis to compare attenuationcorrection (AC) in myocardial SPECT using either 153Gd transmission linesources or low-dose CT.Methods: SPECT was performed in 26 patients (mean age: 56 years, 14men) using 99mTc-sestamibi and 1) a Millennium MG (GEMS) dual headcamera with 153Gd transmission line sources for AC (interleaved), and 2)a Hawkeye (GEMS) with low-dose CT used for AC (sequential). In bothsystems scattered photons were acquired in a window below the 99mTcpeak. All images were processed using the same iterative algorithm withscatter subtraction and AC. Images obtained with Gd attenuation mapsand CT attenuation maps were compared with regard to impact ondefects in 5 regions of the left ventricle (anterior, lateral, inferior, septaland apical) by consensus reading without knowledge of clinical orangiographic data.Results: A total of 26 studies were evaluated, of which 3 studies wereomitted due to substantial difference in bowel activity between theinvestigations. Of the remaining 23 studies interpretations of non-corrected images were similar on both systems. In 17 of the patientspatterns were identical following AC with Gd or low-dose CT: AC didnot change interpretation in 9 cases and in 8 cases inferior defects wereeliminated. In the remaining 6 studies, there were differences betweenthe 2 AC systems: Using Gd-based AC 3 inferior defects disappearedwhich were not eliminated by low-dose CT AC. CAG in all 3 cases werenormal. Furthermore, low-dose CT AC introduced 3 anterior defectswhereas the Gd-based AC introduced no new defects in these cases. Inone case CAG was normal, in one case two LAD stenoses (60 and 80%)were present. CAG was not available in the last discrepant case.Conclusions: Both Gd and CT AC have great impact on myocardialSPECT. However, when compared on a head-to-head basis in patients thetwo systems in some cases create important differences in the correctedimages. Using CAG as reference, the Gd-based AC seems superior to thelow-dose CT based AC system.
S112 Journal of Nuclear CardiologyJuly/August 2005

34.04A CLINICAL COMPARISON OF AN UPRIGHT TRIPLE-HEADDIGITAL DETECTOR SYSTEM TO A STANDARD SUPINE DUAL-HEAD GAMMA CAMERAHC Lewin, MC HyunCardiac Imaging Associates, Los Angeles, CABackground: Recently a small, solid-state, triple-head upright camera formyocardial perfusion SPECT (mps) has been introduced. This new systemoffers high quality images with a reduced acquisition time. We sought tocompare this system to a standard dual-head gamma camera.Methods: 18 consecutive outpatients referred for MPS were imaged in thestandard supine position (Phillips CardioMD™ - C-MD) as well as in theupright position (DIGIRAD Cardius-3™ – C-3). Both rest (R) and stress (S)images were acquired on both cameras and the order of acquisition, for bothR and S, was chosen randomly. All patients were imaged using a low-doseR/high-dose S Tc99m sestamibi protocol. Imaging time was 35 seconds/stop(C-MD � 18.6 min, C-3 � 11.6 min) at rest and 25 seconds/stop (C-MD �13.3 min, C-3 � 8.3 min) at stress. Processing was performed using iterativereconstruction and no attenuation correction was used. The ‘gold-standard’(GS) was the clinical imaging protocol, which included both supine andprone imaging at S, as well as review of raw and clinical data at the time ofinterpretation. The images were read blindly, in random order, for bothquality (using a 5-point scale, 1 – unacceptable to 5 – excellent) and clinicalresults. Raw data was not reviewed during the blind read as this would allowthe reader to identify the camera used (based on the differing size of the fieldof view).Results: The patients were 70.2�11.8 years old and 61% male. 39%underwent exercise S and 59% underwent pharmacologic S using adenosine(of these 60% underwent concomitant low-level treadmill exercise duringthe adenosine infusion). Image quality was 4.4 and 4.9 for R and 4.8 vs. 4.9for S (C-3 vs. C-MD, p � .02 R and p � NS S). There was no significantdifference in the SSS (3.4 & 2.9), SRS (2.3 & 1.6) or SDS (1.1 & 1.1) forC-3 vs. C-MD. In 16/18 (89%) cases there was no difference in the clinicalimpression between the two systems. In the remaining cases 1/18(6%) wasdeemed to be false positive (compared to GS) for both C-3 and C-MD.Conclusion: C-3 offers high-quality images that are equivalent to C-MD inboth quality and clinical results with an acquisition time that is 38% faster.
34.05DIASTOLIC RESERVE IMPAIRMENT ON RADIONUCLIDEAMBULATORY MONITORING SCREENS CLINICAL INSTABILITYAND SEVERE PROGNOSIS IN ISCHEMIC CARDIOMYOPATHYGP Carboni, M TavolozzaUniversita Campus Bio-Medico di Roma, Roma, ItalyBackground: Global perfusion scoring when combined to measures of leftventricular (LV) ejection fraction (EF), LV volumes and LV diastolicfunction during daily life activities could explain the mechanisms for severeprognosis in ischemic dilatative cardiomyopathy (ICMP).Methods: After a routine Tl-gated spect, 16 consecutive pts with icmp withchronic heart failure (chf), mean age of 68 �8 years, with � 30% LV EF,an abnormal exercise defect (ex AD) of an extent of 27�17% pixels andwith reversibility (R) of 13�25% pixels on polar maps were carefullyselected. After 1 week time, global LV function was then continuouslymonitored by radionuclide ambulatory monitoring (C-VEST II) and restbasal values were immediately validated against multigated blood poolanalysis (MUGA). The C-VEST II recordings lasted for an average time of242�126 min.Results: When EFs values measured on MUGA and C-VEST II werecompared there was any significant difference (30�9% vs 27�11%, p �ns) on student t-test as well as on Bland-Altman plotting. When on C-VESTII, heart rate (HR), EFs, end-diastolic volumes (EDVs), end-systolicvolumes (ESVs) and peak filling rate (PFR) measured at rest were comparedwith the same values measured at peak of stairs climbing (SC) there was anydifference in EDVs (104 �5 ml vs 103� 19 ml, p � ns) but not for HR(86�12 bpm vs 102�15 bpm , p � 0.05), ESVs (73�11% vs 62�17%, p �0.04), EFs (30�9% vs 38�13%, p � 0.05) and pfr values (1.3�0.3 edv/svs 2.0�0.6 edv/s, p � 0.02), respectively. A ratio of 50% (8/16) of severecardiovascular events (1 death, 1 stroke and re-hospitalizations for heartfailure in further 6 pts) was observed in a 12�3 months follow-up. Whensuch values were considered in a backward stepwise multiple regression
model, only EDVs, EFs and PFR values during SC had a significant (p �0.05) role in predicting severe cardiovascular events.Conclusions: Increases in cardiac work demand (EFs and PFR valuesduring daily activities) without increases in EDVs indicate failure of theFrank-Starling mechanism. Such a failure is an adjunctive element ofclinical instability in pts with CHF with ex ADs and R of the ADs on gatedspect. The use of C-VEST II, when combined to global perfusion scoringinformations, seems thus to be a valid method for a prognostic evaluationand a precise therapeutical intervention in pts with ICMP and severe CFF.
34.07CAN ANGINA PECTORIS PRIOR TO MYOCARDIAL INFARCTIONIN DIABETIC PATIENTS PROTECT AGAINST SUBSEQUENT LEFTVENTRICULAR REMODELING?S Fukuzawa, S Ozawa, M Inagaki, J Sugioka, S Okino, S IchikawaDiv. of Cardiology, Funabashi Municipal Medical Center, Funabashi,Chiba, JapanBackground: Ischemia occurring before acute myocardial infarction (MI)has been shown to reduce infarct size and to improve outcomes in patients.The extent to which ischemia occurring before MI influences subsequentchanges in ventricular size and function in diabetic patients is unclear. Thegoal of study is to investigate the hypothesis that prior angina pectorisconfers protection from remodeling occurring after myocardial infarction indiabetic patients.Methods: We studied prospectively 88 consecutive patients with the firstanterior AMI undergoing primary coronary angioplasty within 6 hrs fromsymptom on-set, 42 non-diabetic patients and 46 diabetic patients. Allpatients underwent perfusion tracer SPECT within 2 weeks after the onsetand 6 months later. Summed defect score and left ventricular end-diastolicvolume (EDV), left ventricular ejection fraction (EF) were derived aspreviously described. Ischemic preconditioning (IC) defined as anginapectoris in the 24 hrs pre-MI, was presented in 18/42 non-diabetic patientsand in 15/46 diabetic patients.Results: There were no significant differences between diabetic andnon-diabetic patients in age, gender, time from the onset to reperfusion,angiographic characteristics. Preconditioning was present in 43% of non-diabetic patients and in 32% of diabetic patients. The defect score estimatedin non-diabetic patients with and without IC was 12.4�6.2 and 19.4�5.4(p�0.05), that in diabetic patients with and without IC was 20.4�4.6 and19.8�6.2 (p�ns). In non-diabetic patients with IC, EDV change was–2.2�4.8 ml over the 6-month post-MI period, compared with 5.3�3.8 mlfor patients without IC (p�0.05). However, there were no differences in theextent of remodeling in diabetics with and without IC ( 3.8�2.9 vs.4.1�2.7, p�ns).Conclusions: Although ischemic symptoms occurring before MI mayprotect against LV remodeling in non-diabetic patients, they appear to beattenuated in diabetic patients.
34.08ABILITY OF EXPERIENCED READERS TO DISTINGUISH BREASTATTENUATION ARTIFACT FROM OCCULT MYOCARDIALINFARCTION IN OBESE WOMEN UNDERGOING ECG-GATEDREST/STRESS MYOCARDIAL PERFUSION IMAGINGJM Mohart, JE Fairlamb, AJ Hutter, FR Gutierrez, J Zheng, DM Lesniak,RJ Gropler, PK WoodardWashington University School of Medicine, St. Louis, MOECG-gated rest-stress single photon myocardial perfusion imaging (MPI) isused commonly to detect coronary artery disease in women. However,breast attenuation artifact (AA) frequently confounds the interpretationparticularly in obese women. Typically, review of the projection images andthe ECG-gated images are performed to differentiate myocardial infarction(MI) from AA. In this study we evaluated the accuracy of this approachwhen performed by experienced readers.Methods: 23 women with chest pain (56 � 14 yrs, BMI 33 � 1.8) werereferred for dual-isotope MPI (exercise or adenosine). All studies wereinterpreted as normal with AA. Known CAD was present in 5/23 (withoutMI) whereas the other 18/23 exhibited 2.6 � 1.6 risk factors for CAD(age � 55, hypertension, diabetes mellitus, hypercholesterolemia, currenttobacco use, post menopausal state, or family history). Subsequently(55 � 34 days post-MPI), all patients underwent delayed-enhancementcontrast MR to evaluate for MI. Analysis was performed using a 16 segment
Journal of Nuclear Cardiology Abstracts S113Volume 12, Number 4;S14-S25

model (6 basal, 6 mid, and 4 apical segments of the short axis images). Twoexperienced radiology faculty blinded to the MPI results visually catego-rized the myocardial segments as either MI present, equivocal, or MI notpresent. Any areas of disagreement were re-read in consensus.Results: On the MR images, one reader identified one anterior segment asMI equivocal and the second observer called one anterior and two posteriorsegments equivocal in different patients. After consensus read, no MI waspresent in any of the 368 segments.Conclusion: In obese women with an intermediate risk of CAD undergoingMPI, AA can be differentiated from MI accurately based on the review ofthe projection and ECG-gated images by experienced readers.
34.09QUANTIFICATION OF REST AND STRESS LEFT VENTRICULARFUNCTION USING GATED RB-82 PETH Shi, C Santana, FP Esteves, S Lerakis, R Halkar, EV Garcia, R NarlaEmory University School of Medicine, Atlanta, GeorgiaBackground: Gated myocardial perfusion imaging (MPI) is regularlyperformed using SPECT technology. More recently, gated Rb-82 MPI hasbeen used to assess left ventricular function with new generation PETscanners. The objective of this study was to evaluate the feasibility of gatedRb-82 MPI PET using a 12 year-old PET scanner and to determine whetherthe technique increased the confidence level of the readers.Methods: Twenty patients (6 females, 14 males) underwent rest adenosinestress Rb-82 MPI and rest/stress gated Rb-82 PET (8 frames per cycle).Studies were performed in a 1993 vintage, Siemens ECAT EXACT 921PET with BGO crystals. Emory Cardiac Toolbox quantitative software wasused for processing and interpretation. Left ventricular ejection fraction(LVEF), end-diastolic, end-systolic and stroke volumes were automaticallygenerated. Three expert readers independently reviewed the studies. Visualscoring (1-5) was used to assess the overall quality of the gated images andthe added confidence level of interpretation. Visual assessment of the LVEFwas compared to the automatically generated LVEF. Comparison betweenthe 2 was graded on a 1-5 scale.Results: Rest and stress Rb-82 gated images were acquired in 14 patients.In 6 patients only one gated study was available: 4 stress, 2 rest. A total of102 gated studies were evaluated (34 gated x 3 readers). The overall qualityof the gated images was good (excellent 40%, good 43%, unsure 3%, poor14%, uninterpretable 0%). The readers agreed with the automated LVEF on85% of the gated images (agree 74%, probably agree 12%, unsure 3%,probably disagree 9%, disagree 2%). Moreover, the functional informationprovided additional confidence for image interpretation (helpful 25%,probably helpful 21%, unsure 3%, probably not helpful: 15%, definitely nothelpful 36%).Conclusions: LVEF can be reasonably determined even by using older PETscanners imaging Rb-82 as a perfusion tracer. Even with this older scannerthe additional left ventricular function information increased the degree ofconfidence of interpreting the Rb-82 perfusion distribution.
34.10NEGATIVE PREDICTIVE VALUE OF ADENOSINE STRESS ANDREST MYOCARDIAL PERFUSION IMAGING IN PATIENTS WITHEND-STAGE LIVER DISEASEH Shi, FP Esteves, CA Santana, A Alvarez, RK HalkarEmory University School of Medicine, Atlanta, GABackground: Patients with end-stage liver disease need cardiovascular riskstratification before liver transplantation or transjugular intrahepatic porto-systemic stent-shunts (TIPS). Pharmacologic stress is usually performedbecause these patients cannot exercise adequately. Because of baselinesystemic vasodilation, efficacy of adenosine as a pharmacological stressor isquestionable. Hence the purpose of this analysis was to assess the negativepredictive value of adenosine stress myocardial perfusion imaging in liverfailure patients.Methods: Forty-two patients (25 men, 17 women, mean age54 � 8 years, range 43-75 years) had dual isotope (rest Tl-201 andTc-99m MIBI stress) or Tc-99m MIBI-MIBI one day adenosine myo-cardial perfusion imaging (MPI). Adenosine stress was performed with0.140 mg/kg/min infused over 4 minutes. Tc-99m MIBI was injected atthe end of the second minute of adenosine infusion. Images wereprocessed and interpreted by using the Emory Cardiac Toolbox quanti-
tative software. Hospital admission for acute coronary syndromes orcoronary intervention was defined as a cardiac event.Results: Of the 42 patients, 41 had liver cirrhosis, 15 were diabetics, 20were hypertensive, and 6 were obese. Twenty-eight (67%) patients hadascites. Twelve (29%) had splenomegaly. All patients tolerated the 4-minuteadenosine infusion well. Three patients had reversible defects and coronaryangiography showed significant coronary artery disease. Two patients hadfixed defects. Thirty-seven patients had normal MPI with normal leftventricular ejection fraction (mean 76%, range 50-84%). These patientswere followed-up for 14 � 8.6 months (range 1-32 months). Two patientsunderwent liver transplantation and 4 patients had TIPS. There were nocardiac events.Conclusion: Adenosine stress MPI is probably a reliable study for riskstratification of patients with end-stage liver disease. A normal study islikely associated with a very low risk of short-term cardiac events.
34.11THE CHARACTERISTICS OF MOTION ARTIFACTS INMYOCARDIAL PERFUSION SPECTH Shi, J Chen, S Chen, Z YaoZhongshan Hospital, Fudan Univerisity, Shanghai, ChinaBackground: Patient motion during acquisition creates artifacts in myo-cardial perfusion SPECT images and impairs diagnosis. The availablemotion correction algorithms can only apply to certain cases such as studieswith z-direction (head-foot) motion. It is necessary for physicians to befamiliar with the characteristics of motion artifacts.Methods: A cardiac phantom was moved by 0 mm �30 mm in 5 mmintervals along x (right-left), y (up-down) and z directions during theacquisition (180° circular orbit, 60 projections of 3° each) usinga dual-head SPECT camera. The phantom was moved within the 1st 10th (group 1), 11th 20th (group 2), 21st 30th (group 3) projectionsof each head, and moved back after 1 7 projections, respectively. Thereconstructions from the data with motion were compared tothe reconstructions from the data without motion by three blindedobservers.Results: The amounts (distance) and lengths (number of projections withmotion) of motion resulting in artifacts are listed in the following table fordifferent directions. The x-direction and y-direction motions resulted in hotspots in the anterior wall, whereas the z-direction motion resulted in hotspots in the inferior wall. The hot spots became brighter when the amountand/or length of motion increased. The lateral and septal walls displayeddiscontinuity when motion at any direction was more than 1cm for morethan 3 projections.Conclusion: Artifacts appeared at different locations for motion alongdifferent directions. When motion lasted for 4 or more projections, nomatter in which direction, no matter when the motion started, even asmall amount of motion (0.5 cm) resulted in artifacts in the reconstructedimages.
X-direction(cm) Y-direction(cm) Z-direction(cm)
Length G1 G2 G3 G1 G2 G3 G1 G2 G31 None None None2 1.5 1.0 1.5 1.0 1.0 1.0 1.5 1.0 1.53 0.5 0.5 0.5 0.5 1.0 1.0 1.0 1.0 0.54 or more 0.5 0.5 0.5 0.5 0.5 0.5 0.5 0.5 0.5
34.12DOPAMINE-ATROPINE STRESS SPECT: AN ALTERNATIVEADRENERGIC STRESS AGENT FOR DOBUTAMINE SPECTS Ramrakhiani, AH Safadi, JM Foltz, SL Stricker, J Mahenthiran, SGSawadaKrannert Institute of Cardiology, Indiana University, Indianapolis, INBackground: Afterload reduction with Dobutamine (Dobu) causes lowersystolic blood pressure (SBP) and smaller peak end systolic cavity (PESC)with stress and may lessen detection of ischemia. Dopamine (Dopa) as anadrenergic agent has greater alpha-1 agonist activity that may achievehigher peak SBP and larger PESC due to higher afterload. Hence, westudied the feasibility, safety, hemodynamic profiles of a Dopa-SPECTprotocol.Methods: 17 patients (pts) (age 53 � 6.7 years, 82% males) hadDope-SPECT for pre-liver transplant evaluation. Dopa was infused at 10
S114 Abstracts Journal of Nuclear CardiologyJuly/August 2005

mcg /kg / min increments every 3 minutes, to a maximum of 50mcg/kg/min. Atropine was front loaded, up to a maximum dose of 2 mg.Pre-medication with Ondansetron and nasal oxygen was administered.Post- procedure intravenous betablocker (Metoprolol 5-10 mg) was usedas needed for heart rate recovery. Peak stress tracer was injected at peakheart rate, one minute prior to completion of infusion and post stressimages were obtained at 30-40 minutes after. 16 Dobu pts (age 46� 9years, 56% males) referred for pre-liver transplant evaluation wascompared as a control group.Results: The hemodynamic profiles of Dopa vs. Dobu are summarizedon table. Dopa-SPECT achieved higher peak SBP, greater change instress SBP (p�0.05); and greater stress rate pressure product (RPP) andchange in RPP (p�0.05). Four transient arrhythmias were recorded withDopa-SPECT (AIVR, PSVT, junctional tachycardia, intermittent AVdissociation). Additional side effects recorded with Dopa-SPECT werenausea (47% pts- 1severe, 4 moderate, 3 mild; vs. 12% with Dob), mildpalpitations (29% vs.12%), mild tremors (6% vs.0%), chest pain (11%vs. 38%) and mild dyspnoea (11% vs. 32%). 75% of pts achieved agepredicted maximum heart rate with both stress agents and all Dopa ptscompleted the SPECT study.Conclusion: Dopa-SPECT is a safe, feasible and acceptable alternativeadrenergic stress agent to Dobutamine. Nausea is common. Dopamineseems to achieve a favourable peak stress hemodynamics. A higherchange in SBP and RPP with Dopa may cause greater wall stress andlarger PESC in pts with baseline vasodilatation (liver disease) and asmall LV cavity.
Variables Dopa (n�17) Dobu (n�16) p- value
Peak Heart rate (bpm) 143 � 12 140 � 22 0.1Peak SBP (mm Hg) 155 � 33 126 � 38 0.01Change in SBP (peak-rest, mm Hg) 37 � 31 14 � 31 0.04Peak Rate Pressure Product (103) 22.5 � 5 18 � 7 0.02Change in Rate Pressure Product
(Peak RPP-Rest RPP) (103)14 � 5 9.5 � 7 0.01
34.13DISCREPANCIES IN ESTIMATING LEFT VENTRICULAR VOLUMESAND EJECTION FRACTION BY TWO COMMERCIALLY AVAILABLEGATED SPECT ALGORITHMSAA Williams, KS Grewal, PB George, DR Richards, DA CalnonMidWest Cardiology Research Foundation, Columbus, OHBackground: The Cedars-Sinai (QGS) and University of Michigan (4DM)algorithms are routinely used to estimate left ventricular ejection fraction(EF), end-diastolic volume (EDV), and end-systolic volume (ESV). How-ever, QGS and 4DM use slightly different geometric assumptions andconstraints for estimating left ventricular volumes, and therefore the resultsmay differ for the QGS and 4DM algorithms.Methods: The QGS and 4DM algorithms were applied to 1290 consecutiveoutpatients (526 women, mean age 60�/-13 years) who underwent gatedSPECT Tc-99m sestamibi myocardial perfusion imaging on a Siemensdual-headed gamma camera from 4/29/03 to 6/16/04. Images were gated at8 frames per cardiac cycle. In a subgroup of 99 patients who underwenttransthoracic echocardiography (ECHO) within 8�/-19 days of the gatedSPECT study, EF was estimated visually by expert interpreters blinded tothe gated SPECT results.Results: The QGS and 4DM algorithms showed good linear correlation forEF (r�0.80), EDV(r�0.97), and ESV(r�0.96). However, EF was signifi-cantly higher for 4DM than for QGS (67.8�/-14% vs. 63.7�/-16%;p�0.001), resulting from both a higher EDV (91�/-48mL vs. 85�/-40mL;p�0.001) and a lower ESV (34�/-35ml vs. 36�/-32mL; p�0.001) for the4DM algorithm. By Bland-Altman analysis, patients with lower EF tendedto show the largest discrepancy in EF between the QGS and 4DMalgorithms. Correlation with ECHO for estimation of EF was modest withQGS (r�0.64) and 4DM (r�0.69), but agreement was slightly better forQGS than for 4DM (RMS deviation 10.5�/-10.5% and 11.9�/-7.9%,respectively; p�0.006).Conclusions: Although the QGS and 4DM estimates of EF, EDV, and ESVcorrelate linearly with one another, the computed values differ significantlyfor these algorithms. Therefore, discrepancies in EF, EDV, or ESV resultson serial gated SPECT studies must be interpreted in the context of thesoftware algorithm employed. In the echocardiography subgroup, agree-
ment with visual estimation of EF by ECHO was slightly better for QGSthan for 4DM.
34.14VALIDATION OF A COUNTS-BASED GATED SPECT METHODFOR CALCULATION OF LEFT VENTRICULAR EJECTIONFRACTION: COMPARISON AGAINST TWO COMMERCIALLYAVAILABLE ALGORITHMS IN 1238 PATIENTSA Bhama, DA Calnon, PB George, DR Richards, KS GrewalMidWest Cardiology Research Foundation, Columbus, OH, USABackground: The Cedars-Sinai (QGS) and Emory (EDTb) algorithms arewell-validated and routinely used to estimate left ventricular volumes andejection fraction (EF), but rely on automatic endocardial edge detection,which may be problematic in patients with perfusion defects. A uniquecounts-based method (CB) relies on detection of changes in apparentregional counts during systolic contraction, and is independent of edgedetection or geometric assumptions. This method is now commerciallyavailable (SMV Vision, GE Healthcare, Milwaukee, WI) but has not beenvalidated against QGS or ECTb.Methods: The QGS, ECTb, and CB algorithms were applied to 1238consecutive patients who underwent gated SPECT Tc-99m sestamibimyocardial perfusion imaging on a GE system over a 14-month period.Results were reported for the total population, patients with ischemia (withor without infarction, n�300), and infarction without ischemia, (n�165).Results:
Mean LVEF (%) R value
CB ECTb QGS CB vs. ECTb CB vs. QGS
TOTAL 60�11* 57�13 58�12 0.75 0.81Normal 64� 9* 61�10 63� 9 0.61 0.68Ischemia 57�11* 52�13 54�12 0.75 0.82Infarction 50�12* 46�15 48�13 0.78 0.81
*p-value �.05 for CB vs. ECTb and CB vs. QGS.
Using Bland-Altman analysis, the difference in EF with CB versus bothQGS and ECTb was more pronounced in patients with a lower mean EFand those with lower EDV (�90 ml). Conclusions: The CB methodcorrelates well with ECTb and QGS in all patients as well as subsets withischemia and infarction, although the mean EF by CB is slightly higherin all of these patient groups. This discrepancy of EF results by CB ismore pronounced in patients with systolic dysfunction and those withsmall hearts. Because QGS and ECTb are known to have limitations inpatients with small hearts or perfusion defects, the CB method may bemore accurate in these settings, though this hypothesis would requireconfirmation against a gold standard EF determination.
34.15EFFECTS OF MISREGISTRATION BETWEEN SPECT AND CT FORATTENUATION CORRECTED MYOCARDIAL PERFUSION SINGLEPHOTON EMISSION TOMOGRAPHYS Goetze, RL WahlThe Russell H. Morgan Department of Radiology and RadiologicalScience, Division of Nuclear Medicine, Johns Hopkins University,Baltimore, MDBackground: Current recommendations for myocardial perfusionSPECT scintigraphy (MPS) are to incorporate attenuation correction(AC) strategies based on the evidence that it adds to diagnostic accuracy.Compensation strategies using CT, while attractive, have the potential tolead to misregistration of the emission and transmission scans since theCT and SPECT images are obtained sequentially. In our experience, thiscan affect a substantial number (42%) of clinical scans. Our objectivewas to assess the effect of the misregistration errors on the AC-SPECTimages.Methods: Thirty-four consecutive patients who underwent CT-AC stressMPS (with Tc99m methoxyisobutylisonitrile; acquired on a GE Mille-nium VG/Hawkeye® SPECT/CT system) who had misregistration of theSPECT and CT images and a normal filtered back projection (FBP) studywere selected. The FBP and AC images were assessed for “new” defectson the AC images not seen on FBP (group A � no AC defects, groupB�subtle AC defects, group C � significant AC defects).
Journal of Nuclear Cardiology Abstracts S115Volume 12, Number 4;S14-S25
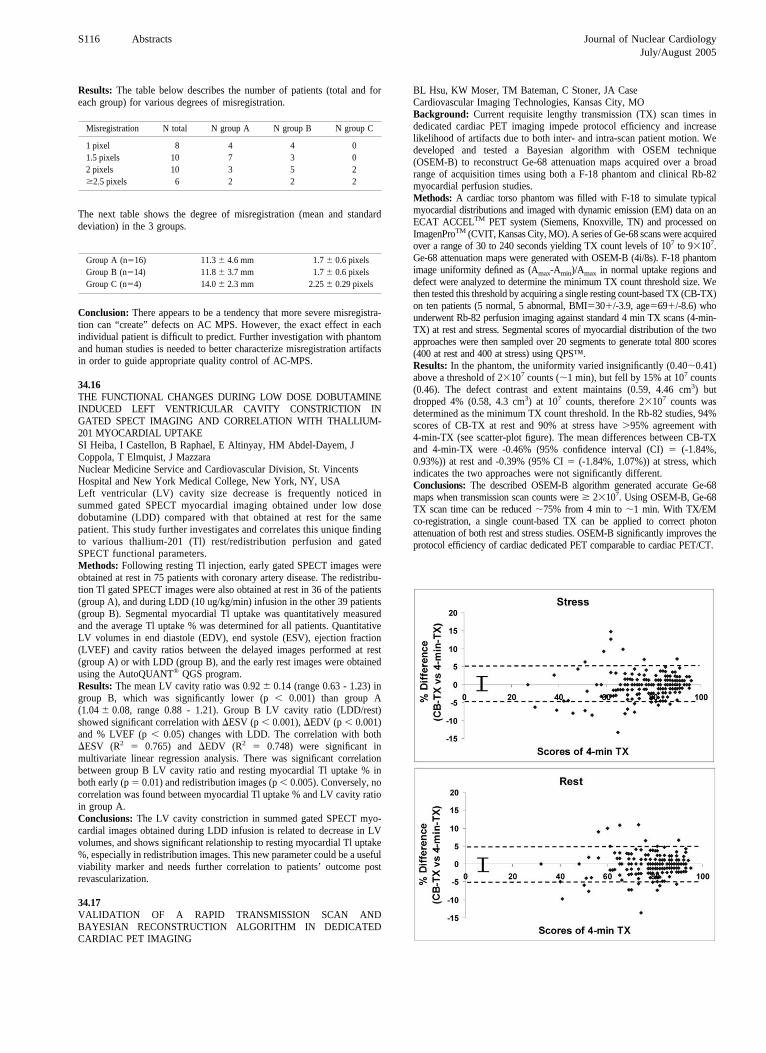
Results: The table below describes the number of patients (total and foreach group) for various degrees of misregistration.
Misregistration N total N group A N group B N group C
1 pixel 8 4 4 01.5 pixels 10 7 3 02 pixels 10 3 5 2�2.5 pixels 6 2 2 2
The next table shows the degree of misregistration (mean and standarddeviation) in the 3 groups.
Group A (n�16) 11.3 � 4.6 mm 1.7 � 0.6 pixelsGroup B (n�14) 11.8 � 3.7 mm 1.7 � 0.6 pixelsGroup C (n�4) 14.0 � 2.3 mm 2.25 � 0.29 pixels
Conclusion: There appears to be a tendency that more severe misregistra-tion can “create” defects on AC MPS. However, the exact effect in eachindividual patient is difficult to predict. Further investigation with phantomand human studies is needed to better characterize misregistration artifactsin order to guide appropriate quality control of AC-MPS.
34.16THE FUNCTIONAL CHANGES DURING LOW DOSE DOBUTAMINEINDUCED LEFT VENTRICULAR CAVITY CONSTRICTION INGATED SPECT IMAGING AND CORRELATION WITH THALLIUM-201 MYOCARDIAL UPTAKESI Heiba, I Castellon, B Raphael, E Altinyay, HM Abdel-Dayem, JCoppola, T Elmquist, J MazzaraNuclear Medicine Service and Cardiovascular Division, St. VincentsHospital and New York Medical College, New York, NY, USALeft ventricular (LV) cavity size decrease is frequently noticed insummed gated SPECT myocardial imaging obtained under low dosedobutamine (LDD) compared with that obtained at rest for the samepatient. This study further investigates and correlates this unique findingto various thallium-201 (Tl) rest/redistribution perfusion and gatedSPECT functional parameters.Methods: Following resting Tl injection, early gated SPECT images wereobtained at rest in 75 patients with coronary artery disease. The redistribu-tion Tl gated SPECT images were also obtained at rest in 36 of the patients(group A), and during LDD (10 ug/kg/min) infusion in the other 39 patients(group B). Segmental myocardial Tl uptake was quantitatively measuredand the average Tl uptake % was determined for all patients. QuantitativeLV volumes in end diastole (EDV), end systole (ESV), ejection fraction(LVEF) and cavity ratios between the delayed images performed at rest(group A) or with LDD (group B), and the early rest images were obtainedusing the AutoQUANT® QGS program.Results: The mean LV cavity ratio was 0.92 � 0.14 (range 0.63 - 1.23) ingroup B, which was significantly lower (p � 0.001) than group A(1.04 � 0.08, range 0.88 - 1.21). Group B LV cavity ratio (LDD/rest)showed significant correlation with ESV (p � 0.001), EDV (p � 0.001)and % LVEF (p � 0.05) changes with LDD. The correlation with bothESV (R2 � 0.765) and EDV (R2 � 0.748) were significant inmultivariate linear regression analysis. There was significant correlationbetween group B LV cavity ratio and resting myocardial Tl uptake % inboth early (p � 0.01) and redistribution images (p � 0.005). Conversely, nocorrelation was found between myocardial Tl uptake % and LV cavity ratioin group A.Conclusions: The LV cavity constriction in summed gated SPECT myo-cardial images obtained during LDD infusion is related to decrease in LVvolumes, and shows significant relationship to resting myocardial Tl uptake%, especially in redistribution images. This new parameter could be a usefulviability marker and needs further correlation to patients’ outcome postrevascularization.
34.17VALIDATION OF A RAPID TRANSMISSION SCAN ANDBAYESIAN RECONSTRUCTION ALGORITHM IN DEDICATEDCARDIAC PET IMAGING
BL Hsu, KW Moser, TM Bateman, C Stoner, JA CaseCardiovascular Imaging Technologies, Kansas City, MOBackground: Current requisite lengthy transmission (TX) scan times indedicated cardiac PET imaging impede protocol efficiency and increaselikelihood of artifacts due to both inter- and intra-scan patient motion. Wedeveloped and tested a Bayesian algorithm with OSEM technique(OSEM-B) to reconstruct Ge-68 attenuation maps acquired over a broadrange of acquisition times using both a F-18 phantom and clinical Rb-82myocardial perfusion studies.Methods: A cardiac torso phantom was filled with F-18 to simulate typicalmyocardial distributions and imaged with dynamic emission (EM) data on anECAT ACCELTM PET system (Siemens, Knoxville, TN) and processed onImagenProTM (CVIT, Kansas City, MO). A series of Ge-68 scans were acquiredover a range of 30 to 240 seconds yielding TX count levels of 107 to 9�107.Ge-68 attenuation maps were generated with OSEM-B (4i/8s). F-18 phantomimage uniformity defined as (Amax-Amin)/Amax in normal uptake regions anddefect were analyzed to determine the minimum TX count threshold size. Wethen tested this threshold by acquiring a single resting count-based TX (CB-TX)on ten patients (5 normal, 5 abnormal, BMI�30�/-3.9, age�69�/-8.6) whounderwent Rb-82 perfusion imaging against standard 4 min TX scans (4-min-TX) at rest and stress. Segmental scores of myocardial distribution of the twoapproaches were then sampled over 20 segments to generate total 800 scores(400 at rest and 400 at stress) using QPS™.Results: In the phantom, the uniformity varied insignificantly (0.400.41)above a threshold of 2�107 counts (1 min), but fell by 15% at 107 counts(0.46). The defect contrast and extent maintains (0.59, 4.46 cm3) butdropped 4% (0.58, 4.3 cm3) at 107 counts, therefore 2�107 counts wasdetermined as the minimum TX count threshold. In the Rb-82 studies, 94%scores of CB-TX at rest and 90% at stress have �95% agreement with4-min-TX (see scatter-plot figure). The mean differences between CB-TXand 4-min-TX were -0.46% (95% confidence interval (CI) � (-1.84%,0.93%)) at rest and -0.39% (95% CI � (-1.84%, 1.07%)) at stress, whichindicates the two approaches were not significantly different.Conclusions: The described OSEM-B algorithm generated accurate Ge-68maps when transmission scan counts were � 2�107. Using OSEM-B, Ge-68TX scan time can be reduced 75% from 4 min to 1 min. With TX/EMco-registration, a single count-based TX can be applied to correct photonattenuation of both rest and stress studies. OSEM-B significantly improves theprotocol efficiency of cardiac dedicated PET comparable to cardiac PET/CT.
S116 Abstracts Journal of Nuclear CardiologyJuly/August 2005

34.18RAPID LOW-DOSE/HIGH-DOSE ONE DAY 99MTC-SESTAMIBIGATED MYOCARDIAL PERFUSION SPECT IN JAPANESEPOPULATIONN Matsumoto, Y Sato, S Yoda, M Muromoto, HC Lewin, MC HyunNihon University, Tokyo, JapanBackground: Same day single-isotope rest/stress myocardial perfusionSPECT using 99mTc agents is a commonly used methods, however the studytime is long due to the 3-4 hour delay between rest and stress acquisitions.We examined the accuracy of a rapid rest low-dose/stress high-dose99mTc-sestamibi protocol (RP) previously reported, which could be com-pleted in under 120 min.Methods: 53 patients (age: 62.0�10, male: 46 (75%), height: 164.1�8.0cm,weight: 66.8�18.1kg) were imaged immediately after the injection of sestamibi(287.4�33.3MBq) at rest. Subsequently, patients performed exercise or vaso-dilator stress immediately, followed by stress acquisition by 99mTc-sestamibi(1468.9�214.9MBq). The relative count ratio was calculated by dividing thecounts in a region of interest (ROI) on stress SPECT images by the counts in thesame ROI on rest images. The image quality was scored using a 4-point-scalemodel (1:unacceptable to 4:excellent) for perfusion and gated images by 2readers. Coronary angiography was performed in 35 patients within 2 weeksafter SPECT acquisition.Results: All patients successfully performed this protocol and the totalexamination time was 101.5�11.3min. The relative count ratio (stress/rest)was 6.4�2.3. Image quality was good to excellent for both perfusion(stress�3.6�0.6, rest�3.1�0.9) and gated images (stress�3.8�0.4,rest�3.7�0.7). The sensitivity to detect significant coronary artery stenosis(luminal narrowing�50%) is 83% and the specificity is 91%.Conclusions: RP is a rapid same day rest/stress protocol which providedvery good image quality, excellent relative count ratios and excellentcorrelation with coronary angiography.
34.19UTILITY OF THE STRESS MINUS DELAY BULLSEYE MAP INIMPROVING INTERPRETIVE ACCURACY OF MYOCARDIALPERFUSION SCANSVRP Nalamolu, RN Patel, JK Dias, RJ Kaminski, TW Kersey, VJBRobinsonMedical College of Georgia, Augusta, GABackground: Myocardial perfusion imaging (MPI) is subject to considerablenoise due to re-registration and attenuation artifact, as well as overlap fromother structures with radiotracer uptake. We hypothesized that the pattern ofencircling reperfusion in the Stress-Delay Bullseye map (S-D) could serve toimprove diagnostic accuracy by excluding the above confounders.Methods: We performed a retrospective review of 4861 myocardialperfusion studies at Medical College of Georgia from 01/98- 07/01. Weidentified 51 studies that showed encircling reperfusion on S-D withconcurrent cardiac catheterization (CAngio) within 4 months. Encirclingreperfusion was defined as a band of reversibility �2.5 SD above that of thenormal data file. This had to surround the delay defect for at least 2/3rd ofits circumference on the S-D. Three expert readers, blinded to CAngioresults, individually interpreted MPI without and with S-D using commer-cial software Inspect/Prospect. The interclass correlation coefficient be-tween readers was excellent for interpretations without S-D 0.947(p�0.001) and with S-D 0.937 (p�0.001) indicating strong agreementbetween readers.Results: Using a certainty index 1-100 (100 being highest certainty forpresence of perfusion defects) for image interpretation, average readings ofall three readers, without S-D showed sensitivity 58%, specificity 67% withpositive predictive (PPV) and negative predictive (NPV) values of 81% and40% respectively for diagnosis of significant (�50%) coronary stenosis.Overall accuracy for correct diagnosis was 61%. Utilizing the S-D withencircling reperfusion, sensitivity was significantly increased to 83%(p�0.004) with specificity unchanged at 67%. PPV and NPV increased to86% and 63% respectively. Overall accuracy improved to 78%. Nine falsenegative cases (17% of total) were correctly reclassified using S-D encir-cling reperfusion without any loss of true positives.Conclusions: We conclude that the finding of encircling reperfusion on theS-D can improve the interpreter’s confidence and sensitivity for identifyingtrue myocardial perfusion defects. As a result PPV, NPV and overallaccuracy of diagnosis are also improved.
34.20WIDE BEAM RECONSTRUCTION METHOD FOR SHORTENINGSCAN TIME OF GATED CARDIAC STRESS SPECT: PRELIMINARYEVALUATIONJH Oaknin, SC Shwartz, RA Pagnanelli, RE Coleman, S Borges-NetoUltraSPECT, Haifa, IsraelBackground: Myocardial perfusion SPECT studies have a scan timebetween 12 and 25 minutes, according to the guidelines of the ACC/AHA/ASNC, that often results in patient motion with image artifacts as well asthroughput limitations. This study evaluates image quality and potentialclinical benefit of a new gated stress myocardial perfusion SPECT protocol,with scan time reduced by one-half and the data are reconstructed using theWide Beam Reconstruction method (WBR).Methods: The WBR™ technology (UltraSPECT Ltd), based on an accuratemodeling of the emission – detection process, was designed to simulta-neously suppress noise and improve image resolution. The WBR algorithmwas optimized specifically for short gated cardiac stress perfusion scanswithout applying any post-filter. Several phantom studies were recon-structed using both WBR and FBP/OSEM: NEMA SPECT protocols, coldand hot sphere phantoms (6 spheres: 9.5 - 31.8 mm diameter) and theanthropomorphic torso phantom with a cold insert (2cm x 2cm x 1cm)simulating clinical conditions, was scanned twice with full and half scantimes. Relative activity concentration in the phantom, were 100%, 20%,16% and 0% in liver, ventricle cavity, torso and insert, respectively. Foreach reconstruction method, the respective spatial resolution, coefficient ofvariation (CV) and contrast recovery (CR) were measured. Full scan timeimages were reconstructed for 26 patients (18 males) using filtered backprojection. Half of the projections data were then discarded and theremaining data were reconstructed using WBR.Results: Average FWHM following NEMA were 7.5mm and 10.1mm forWBR and FBP respectively. Cold spheres’ CV was 3.8% for WBR and 4.9%for OSEM Average CR of the WBR was 42% higher than OSEM. WBR CRof the 2 smallest spheres was 40% higher than for OSEM, For the “hot” spheres,the superiority of WBR was even higher. For the torso phantom, the average CRfor VLA and SA between normal and “cold” lesion was 68% for the WBRhalf-time and 51% for full-time FBP. VLA’s CV was identical for bothmethods. The results of 26 patients demonstrated no clinical differencesbetween the two types of protocols and reconstruction algorithms.Conclusions: The WBR method demonstrates improved resolution,better uniformity and enhanced “cold” and “hot” lesion detectabilityover current reconstruction methods through phantom studies. Thismethod appears to have clinical benefits by potentially allowing forreduction of stress SPECT scan time to 50% of the typical clinicalvalues, without introducing artifacts.
34.21SENSITIVITY OF MYOCARDIAL PERFUSION PET/CT IMAGINGSCAN APPEARANCE ON ACCURATE TRANSMISSION/EMISSIONREGISTRATIONJA Case, GV Heller, SJ Cullom, BL Hsu, GL Noble, M Masse, TMBatemanCVIT Kansas CityBackground: Misregistration (MR) between transmission (TX) and emis-sion (EM) datasets is a potential source of image artifacts in myocardialperfusion Rb-82 PET imaging. In this study, we examined the impact ofvarying degrees of lateral and transaxial MR to establish tolerance to MRand precision needed for MR compensation algorithms.Methods: 10 clinically indicated myocardial perfusion PET/CT studieswere reprocessed on an ImagenPRO™ (CVIT, Kansas City, MO) PETprocessing workstation to simulate varying amounts of lateral and transaxialMR. The original scans were first corrected for MR. Then each scan wasreprocessed with transaxial and lateral MR of -4 through �4 pixels. Theresulting 340 image sets were then analyzed using QPSTM (CSMC, LosAngeles, Ca) SPECT software to quantitate raw relative uptake. Toleranceto MR was determined by comparing changes in the lateral to septal andanterior to inferior wall count ratios.Data Acquisitions: Data were acquired on a GE Discovery DS PET/CTsystem. CT imaging was performed using a 20 sec free-breathing 20 – 40mA CT scan. PET imaging began 150 secs after the conclusion of infusionof 40 mCi of Rb-82. After rest imaging, the patient was stressed withdipyridamole and imaged with the same imaging protocol.
Journal of Nuclear Cardiology Abstracts S117Volume 12, Number 4;S14-S25

Results: MR of less than 2 pixels (7.8 mm) in any direction did notintroduce a measurable change in septal to lateral or anterior to inferiorwall ratios. However, MR � 2 pixels in the left lateral direction changedseptal/lateral wall ratios, while MR � 2 pixels in the plus transverse(“up”) direction resulted in significant changes in anterior/inferior wallratios.
Conclusion: MR of more than 7.8 mm can introduce significant andmisleading artifacts into PET images. Misregistration compensation algo-rithms must utilize both lateral and transverse translations to compensate forthese artifacts and be accurate to shifts of � 7.8 mm.
34.22ATTENUATION-CORRECTED TC-99M SESTAMIBI SPECT COMPAR-ED WITH RB-82 MYOCARDIAL PERFUSION PETTM Bateman, GV Heller, AI McGhie, JD Friedman, SJ Cullom, JA CaseMid America Heart Institute, Kansas City, MOBackground: Several studies have confirmed a higher diagnostic accuracyof Rb-82 myocardial perfusion PET, where image data is routinely attenu-ation corrected (AC), compared to non-AC SPECT. We investigated thehypothesis that same-day technetium-99m sestamibi AC SPECT wouldprovide similar diagnostic accuracy to that of PET.Methods: Four nuclear cardiologists interpreted by consensus and with noclinical data 102 PET and 102 AC SPECT studies in pts matched by gender,body mass index, and presence and extent of CAD. Studies were interpretedfor quality (excellent, good, fair, poor), artifacts (none, minor, significanteffects on interpretation), diagnosis, and coronary territory of abnormality.All studies were rest/pharmacologic stress without concomitant exercise andECG-gated at rest and stress. Patients were either low CAD likelihood orhad catheterization (CATH) � 90 days post-scan (n�79). SPECT scanswere acquired on a Cardio60TM dual-detector camera (Philips, Milpitas, Ca)and PET scans on an ECAT AccelTM (Siemens, Knoxville, TN) dedicatedPET scanner. There were 46 women in each group; BMI mean for PET was32�/-7 (range 17–50) and for SPECT 33�/-7 (range 16–50) (p�0.35); atCATH, 32 pts had 0 CAD, 13 had 1 vessel CAD, and 57 had multivesselCAD in each group.Results: Overall PET accuracy for CAD was 90% vs 80% for AC SPECT(p�0.04). PET vs AC SPECT accuracies by vessel were: LAD � 90% vs76% (p�0.01); LCx � 83% vs 78% (p�0.35); RCA � 90% vs 77%(p�0.01); and for all coronaries combined 88% vs 77% (p�0.001). PETimage quality was excellent for 80% vs 24% for AC SPECT (p�0.001).90% of PET studies had no artifacts vs 50% of AC SPECT studies – 50 ACSPECT studies had excessive liver/bowel activity interfering with inferiorwall interpretation.Conclusions: Rb-82 PET image quality and diagnostic accuracy are bothsuperior to those of SPECT despite attenuation correction. SPECT AC issignificantly hampered with pharmacologic stress because of accentuationof commonly present liver and bowel activity with resulting scatter into theinferior wall. Concomitant exercise and better methods of scatter correctionmay improve AC SPECT results.
34.23SIGNIFICANCE OF QUANTIFICATION OF MYOCARDIAL BLOODFLOW BY CARDIAC PET IN DIABETIC PATIENTS FOR THEDIAGNOSIS OF SMALL VESSEL DISEASEM Devabhaktuni, KT Hickey, RR Sciacca, KN Giedd, LJ Johnson, S BokhariThe College of Physicians and Surgeons of Columbia University. NY, NY
Objective: To determine if there is a difference in quantitative myocardialblood flow reserve between diabetic and non-diabetic patients with similarqualitative scan interpretation.Methods: 77 consecutive patients undergoing NH3 rest and stress (adenosine)PET myocardial perfusion imaging (MPI) were studied. Fifteen patients haddiabetes mellitus (mean age 62�8; 14 males) and 62 were non-diabetics (meanage 60�11; 45 males). There was no significant difference in FraminghamLDL risk score between the groups. NH3 blood flow was measured in ninedifferent regions of the heart using a two compartment model.Results: Qualitatively 9 out of 15 (60%) of diabetic patients had perfusiondefects on MPI and 35 out of 62 (56%) of non-diabetic patients hadperfusion defects on MPI (p � NS). There was no difference in summeddefect score and reversibility score between the two groups. Quantitativelythere was no significant difference in regional or global myocardial bloodflow at rest between diabetic and non-diabetic patients (0.65�0.2 ml/g/minvs. 0.77�0.2 ml/g/min; p � NS). At stress, global coronary flow reserve(stress flow – rest flow) was significantly lower in diabetic compared tonon-diabetic patients (0.59�0.5 ml/g/min vs. 1.04�0.5 ml/g/min; p �0.006). There were also significant differences in regional coronary flowreserve in 8 of 9 myocardial regions at stress.
Basalanterior
Distalanterior apex
Distalinferior
Basalinferior
Distalseptal
Basalseptal
Distallateral
Basallateral
0.005 0.004 0.012 0.006 0.022 0.011 0.016 0.027 0.09
Conclusion: There is no significant difference in resting myocardial bloodflow in diabetic patients compared to non-diabetic patients. However, bothglobal and regional myocardial flow reserve is decreased in diabetic patientscompared to non-diabetic patients. This likely reflects small vessel diseaseor endothelial dysfunction and quantification of myocardial blood flow bycardiac PET may be useful to assess total extent of blood flow limitation.
34.24PROGNOSIS OF NORMAL RUBIDIUM-82 PET MYOCARDIALPERFUSION STUDYD Nemirovsky, MJ Henzlova, J Machac, D AlmeidaMount Sinai Medical Center, New York, NYBackground: The reported sensitivity of PET perfusion studies for detec-tion of angiographic CAD is similar to SPECT studies; PET specificityexceeds that of SPECT. A favorable prognosis (�1% yearly cardiacmortality) of patients with normal SPECT study has been confirmed bymultiple studies. The prognosis of patients with normal PET perfusionstudies is unknown.Methods: The Mount Sinai Medical Center Nuclear Cardiology database wassearched for patients with a normal result of Rubidium-82 PET dipyridamole oradenosine perfusion study and normal left ventricular systolic function on gatedPET over a 46 month period (4/2000-2/2004). All patients were followed for allcause and cardiac mortality for a minimum of 12 months using hospital MedicalRecords and the Social Security Death Index.Results: A total of 387 patients were identified: Average age was58 � 13 years, 39% were male, 61% were female and 18% were treated fordiabetes mellitus. Mean follow up time was 33 months (12-59 months).Forty seven patients were excluded because of known CAD or history ofcardiac transplantation. Of the remaining 340 patients, 26 died during thefollow up. The cause of death was end-stage liver disease in 12 patients,end-stage renal disease in 1, metastatic cancer in 6, one patient died of smallbowel perforation, and one died perioperatively after thoracic aorticaneurysm surgery. The cause of death could not be ascertained in 5 patients(3 males/2 females, 42-88 years old) and was considered to be cardiac: Twopatients died during the first year of follow-up, one died at 26 months, oneat 32 and one at 38 months of follow-up, respectively. Thus, with this worstcase scenario, one year cardiac mortality in patients with a normal PETmyocardial perfusion study and a normal left ventricular systolic functionwas 0.6% (2 of 319 patients).Conclusions: In our cohort of patients evaluated for presence of coronaryartery disease, a normal Rb-82 PET stress perfusion study and normal leftventricular systolic function, conferred one year cardiac mortality similar tothat of a normal SPECT perfusion study.
S118 Abstracts Journal of Nuclear CardiologyJuly/August 2005

34.25COMPARISON BETWEEN GATED AMMONIA PET AND GATEDMIBI SPECT FOR QUANTIFICATION OF GLOBAL ANDREGIONAL LEFT VENTRICULAR FUNCTIONS Kanayama, O Satake, K KajinamiDept of Cardiology, Kanazawa Medical University, Ishikawa, JapanBackground: The aim of this study is to compare gated 13N-NH3 PET and99mTc-MIBI SPECT to assess global and regional left ventricular function inpatients with coronary artery disease (CAD).Methods: Fifty-one patients with CAD underwent both gated NH3 PET andgated MIBI SPECT. The EDV, ESV and EF were calculated by using QGS.The quantitative regional wall motion (WM) and thickening (WT) scores in20 segmental model were also measured by QGS.Results: The EDV, ESV and EF measured by NH3 PET showed highlysignificant correlation with those by MIBI SPECT measurements (R�0.97,R�0.97 and R�0.84, respectively). The mean correlations of WM and WT onpatient basis between NH3 PET and MIBI SPECT were 0.81 and 0.84respectively. Circumferential variations of mean WM and WT in 20 segmentsshowed similar pattern in NH3 PET and MIBI SPECT. The mean correlationsof WM and WT in the 20 segmental model were 0.69 and 0.69 respectively, andthese were 0.79 and 0.77 when basal segments were excluded from the analysis.Conclusion: Gated NH3 PET combined with QGS provides information onglobal and regional left ventricular function similar to that obtained by gated99mTc-perfusion myocardial SPECT in patients with CAD.
34.26AN EVALUATION OF ADENOSINE PEAK-STRESS MYOCARDIALPERFUSION IMAGING WITH ECG-GATED RUBIDIUM-82 PETKW Moser, SJ Cullom, JA Case, GK Hertenstein, LL Volker, TMBatemanCardiovascular Imaging Technologies, Kansas City, MOBackground: A unique potential of myocardial perfusion PET is thesimultaneous assessment of perfusion and function under peak-stressconditions. Dipyridamole, an indirect adenosine receptor agonist, is pre-dominantly used because it maintains hyperemia long enough to acquiretransmission (TX) and emission (EM) image sets. The objective of thisstudy was to evaluate a protocol that might permit peak-stress ECG-gatedRb-82 PET with the shorter-duration adenosine.Methods: We studied 20 pts (16 M) with a prior clinically-indicatedrest/dipyridamole-stress Rb-82 myocardial perfusion PET on a SiemensECAT Accel™ system. The research protocol included rest TX, rest EM,peak-stress EM (2-3 min), and post-stress TX scans, where the EMacquisitions were in 3D mode with ECG-gating. Peak-stress EM imagingwas performed during a 7 min adenosine infusion (140 �g/kg/min) withRb-82 introduced at 90 sec (Pts. 1-10) or 120 sec (Pts. 11-20). Both clinicaland research images were reconstructed using OSEM (6it/8sub). Segmentalscores of the myocardial distribution were sampled over 20 segments usingQPS™; ejection fraction, end-systolic, and end-diastolic volumes werecalculated using QGS™ (Cedars-Sinai).Results: At rest, there were no significant differences in the mean segmentalscores for the clinical (C: 83.3�6.6) and research (R: 83.7�6.8) images. Atstress, segments were classified as “normal” or “abnormal” based on theclinical images and then evaluated to determine the time required to achievecoronary hyperemia comparable to dipyridamole. For Pts. 1-10, defect sizeand contrast was lower with adenosine vs. dipyridamole in the abnormalsegments (C: 70.5�9.5, R: 78.3�7.8; p�0.001). For the patients tested withthe 120 sec Rb-82 infusion delay (Pts. 11-20), the scores in the abnormal
segments were equivalent (C: 75.0�7.6, R: 74.4�8.2; p�0.48). Based onthe perfusion data, the QGS™ analysis was performed for Pts. 11-20. Atrest, the clinical and research images gave equivalent ejection fractionmeasurements (C: 56.4�12.8; R: 56.3�9.6; p�0.95). In the peak-stressimages, adenosine consistently gave lower ejection fractions than dipyrid-amole (C: 61.1�13.2; R: 57.4�12.0; p�0.02), mainly due to largerend-systolic peak-stress volumes observed with adenosine (p�0.001).Conclusion: This study established that peak-stress myocardial perfusionPET imaging with adenosine is feasible using a 120 sec Rb-82 infusiondelay. However, the differences in functional measurements betweenadenosine and dipyridamole will require further investigation.
34.27GENDER-MATCHED NORMAL VALUES AND PROSPECTIVEVALIDATION OF TRANSIENT ISCHEMIC DILATION (TID) INDEXUSING RB-82 MYOCARDIAL PERFUSION PET IMAGINGC Santana, L Verdes, R Narla, RD Folks, S Lerakis, EV Garcia, TLFaber, H Shi, F Esteves, R HalkarEmory University School of Medicine, Atlanta, GeorgiaObjectives: To determine normal values and validate TID index using rest/pharmacologic stress Rb-82 PET myocardial perfusion imaging.Methods: TID was determined in 95 rest/pharmacologic stress Rb-82 PETscans of patients who had either �5% likelihood of CAD (n�30, 25dipyridamole, 5 adenosine) or who had coronary angiography � 15 days(8 � no CAD � 50% stenosis, 21 � single-vessel CAD, 36 � multivessel(MV) CAD, all adenosine). All scans were acquired using a whole-bodySiemens ECAT EXACT 921 PET tomograph. Emory Cardiac Toolbox(ECTb) quantitative software was used to calculate TID as the ratio of stressto rest mean LV endocardial volume. Statistical comparisons betweenpopulations were performed using the Student t-test and p � .05 wasconsidered statistically significant.Results: Mean and standard deviation TID values and normal limits(Mean � 2SD) are shown below for each population. No significantdifferences in TID were found between genders.
�5% likelihood of CAD
TID ALL (n�30) Male (n�12) Female (n�18)
Mean � 1SD 1.01 � 0.07 0.99 � 0.07 1.02 � 0.06Normal Limits 1.15 1.13 1.14
The average of TID by ECTb was 1.05 � 0.11(range: 0.84 to 1.15) forpatients without CAD, 1.08 � 0.08 (range: 0.94 to 1.31) for patients withsingle CAD and 1.1 � 0.11 (range: 0.84 to 1.35) for those with multivesselCAD. There is no significant difference between groups (p0.05). Using 1.15as a criterion for abnormality yielded sensitivity and specificity of 19% and100% for any CAD and 31% and 90% for MV CAD.Conclusions: The normal values of TID using rest/pharmacological stressRb-82 PET myocardial perfusion imaging are similar for males and females.Using the normal limits as cut-off criteria for abnormality on patients withcoronary angiography shows a low sensitivity, but high specificity, foreither single or multivessel CAD.
34.28OPTIMAL THRESHOLD FOR DETERMINING CARDIAC VOLUMESUSING TOMOGRAPHIC EQUILIBRIUM RADIONUCLIDE ANGIO-CARDIOGRAPHYIP Clements, BP Mullan, JF Breen, CG McGregorMayo Clinic, Rochester, Minnesota, USABackground: The purpose of this study was to define the threshold for edgedetection that optimally determined right and left ventricular volumes usingtomographic equilibrium radionuclide angiocardiography (TERNA).Methods: Twenty-seven patients on 34 occasions underwent bothelectron beam computed tomography (EBCT) and TERNA for measure-ment of right and left ventricular volumes (end-systolic and end-diastolic). In seventeen acquisitions, following reconstruction of theTERNA, the end-systolic and end-diastolic right ventricular regions ofinterest on the horizontal-long axis slices and the left ventricular regionsof interest on the short axis slices were outlined and thresholds rangingfrom 30 to 55% of maximal pixel activity were tested to determine thethreshold value or values that optimally determined cardiac volume
Journal of Nuclear Cardiology Abstracts S119Volume 12, Number 4;S14-S25

when compared with EBCT. In the remaining 17 acquisitions, thethreshold or thresholds that were defined as optimal were used tovalidate TERNA volume compared to EBCT; in addition the TERNAanalysis was repeated to determine reproducibility.Results: Ventricular volume (combining end-diastolic and end-systolic)using EBCT was 178�99 ml (right) and 84�43 ml (left). It was foundthat the 45% threshold was optimal for the right ventricle whereas 50%was optimal for the left. Using these thresholds TERNA volume for theright ventricle was 175�84 and 76�36 for the left (differences betweenEBCT and TERNA were not significant). In the validation group, usingthe optimal thresholds, EBCT compared to TERNA volumes did notdiffer in the right (188�82 vs 181�76) or left ventricle (84�43 vs87�35); furthermore excellent correlations were evident between EBCTand TERNA for the right (r� 0.93) and left ventricle (r�0.87) andregression equations relating TRNV and EBCT volume were close to theline of identity. Repeated TERNA volumes measurements were highlycorrelated with low standard errors of the estimate in the right (r�0.987,SEE� 12ml) and left ventricle (r�0.997, SE� 3ml).Conclusion: The application of a threshold method to TERNA allowedaccurate and reproducible measurement of right and left ventricularvolume.
34.29IMPACT OF DIABETES AND PROTEINURIA ON SILENTCORONARY ARTERY DISEASE DETECTED BY STRESS SESTAMIBISPECT IMAGING IN ASYMPTOMATIC HYPERTENSIVESC Cote, M Dumont, J Lefebvre, L Poirier, Y LacourciereCentre Hospitalier Universitaire de Quebec, CanadaBackground: The concomitant presence of essential hypertension (EH) andtype 2 diabetes mellitus (DM) increases the risk of coronary artery disease(CAD). Moreover, the presence of proteinuria has been shown to be anindependent risk factor for CAD. We hypothesized that the presence of DMwith or without proteinuria would be associated with an increased preva-lence in silent CAD in asymptomatic hypertensive patients.Methods: The study population consisted of 736 patients (pts) � 45 yearswith EH (n � 425) or EH with DM (n � 311) without typical angina orknown CAD selected according to the criteria defined by the AmericanDiabetes Association (ADA). All pts underwent a dipyridamole stress andrest 99mTc Sestamibi myocardial SPECT imaging. Stress and rest imageswere divided into 20 segments and blindly analysed by two observers.Summed stress score (SSS) and summed rest score (SRS) were obtained byadding the scores of the 20 segments. The difference between SSS and SRSwas defined as the summed difference score (SDS), an index of the severityof reversible myocardial ischemia.Results: There was a significant difference (p � 0.001) between theproportion of EH pts with (39.2%) and without DM (25.4%) with regards toabnormal SSS. The frequency of abnormal SDS was significantly (p �0.0001) higher in EH pts with DM (36.7%) than in EH pts without DM(22.1%). Furthermore, there was a significantly greater severity of silent(p � 0.001) and reversible (p � 0.0001) ischemia in EH pts with DM. In EHpts with DM, proteinuria was associated with higher (p � 0.05) prevalenceof silent and reversible ischemia.Conclusion: In this high risk population screened according to the ADAcriteria with dipyridamole Sestamibi SPECT imaging, a significantly greaterproportion of pts with EH and DM has silent and more severe CAD than ptswith hypertension alone. Our study also demonstrates a close relationshipbetween proteinuria and myocardial perfusion abnormalities in pts with EHand DM. These findings suggest that essential hypertensive pts with othermajor cardiovascular risk factors should be screened for early detection ofsilent CAD.
34.30DISTRIBUTION OF RESTING PERFUSION DEFECTS INHYPERTROPHIC CARDIOMYOPATHYR Gupta, RA Aqel, D Mehta , MA Clay, G Zoghbi, AE IskandrianDivision of Cardiology, Department of Medicine, University of Alabamaat Birmingham
Background: Hypertrophic obstructive cardiomyopathy (HOCM) is oftenassociated with asymmetric septal hypertrophy. Resting myocardial perfu-sion defects can be present in such patients despite normal epicardialcoronary arteries.
Methods: We studied patients with HOCM who had NYHA III or IVsymptoms despite optimal medical management with resting SPECT myo-cardial perfusion imaging.Results: There were 14 patients (3 men) with mean age 56 � 22 years.There were resting perfusion defects in 10 patients (71%). 9/10 had defectsin the lateral wall, 1/10 had a defect in the inferior wall and 4/10 had defectsin the anterior-septum (4 patients had defects in more than one location).These regions however, had normal wall motion and thickening by gatedimaging. The defect size in patients with abnormal scan was 11.0% � 6%.The mean left ventricular (LV) ejection fraction was 52%. The end diastolicvolume was 128 � 51 ml, the end-systolic volume was 60 � 39 ml and theLV mass was 159 � 35 gm. The mean gradient across the outflow tract bysimultaneous LV and aortic pressure measurement was 59 � 22 mm Hg andby Doppler echocardiography 70 � 58 mm Hg. The lung to heart ratio was0.3 � 0.09 and 11 out of 14 (78%) patients had asymmetric septalhypertrophy by 2D echocardiography.Conclusion: HOCM is associated with abnormal myocardial perfusionin a large proportion of patients despite normal coronary angiograms.Most defects are localized to the lateral wall. These abnormalities aremost likely secondary to hot-spots in the septum and apex due toasymmetric septal hypertrophy. Recognition of these artifacts couldeliminate false positive scans in such patients. The current databasesshould not be used in these patients for quantitative analysis andHOCM-specific databases need to be developed.
34.31COMPARISON OF CARDIAC FUNCTION BETWEEN POST-MENOPAUSAL AND PRE-MENOPAUSAL WOMEN: EVALUATIONBY GATED MYOCARDIAL SPECTK-H Hwang, J-H Kim, W Choe, N-B KimDepartment of Nuclear Medicine, Gachon Medical School, Incheon,Korea
Background: In addition to inhibiting coronary atherosclerosis, estro-gen is expected to have protective effects on cardiac myocytes indepen-dent of the coronary vasculature. We investigated the difference incardiac parameters evaluated by gated myocardial SPECT after ade-nosine-stress between post-menopausal and pre-menopausal healthywomen.Methods: This study included 22 healthy post-menopausal women (meanage: 53.0 � 1.7 yr) and 20 pre-menopausal women (mean age:43.0 � 3.0 yr) who performed Tc-99m tetrofosmin gated myocardialSPECT after adenosine-stress. Measured hemodynamic parameters, EDV,ESV, stroke volume, EF, cardiac output and cardiac index were comparedbetween the two groups. For comparison, similar-aged two male groups(mean age: 53.2 � 2.4 yr vs 43.1 � 3.2 yr) with matched numbers were alsostudied.Results: There was no significant difference in hemodynamic parame-ters, EDV, ESV, stroke volume, EF or cardiac output between thepost-menopausal and pre-menopausal women. However, post-meno-pausal women have a smaller cardiac index (1.95 � 0.29 � � min-1m-2 vs2.20 � 0.50 � � min-1m-2; p�0.045) and adenosine-induced HR increase(80.5 � 11.8/min vs 89.7 � 14.1/min; p�0.03), compared to the pre-menopausal women. On the contrary, the two male groups of the sameage range and numbers with the women groups showed no significantdifference in any cardiac parameters.Conclusion: These results suggest that menopause may be correlated withreduced increase in cardiac index and HR after adenosine-stress.
34.32GENERATION OF NORMAL LEFT VENTRICULAR MYOCARDIALMASS, EJECTION FRACTION, GATED AND UNGATED VOLUMESUSING TECHNITIUM-99 SPECT MYOCARIAL PERFUSIONIMAGINGR Khateeb, PM Keefer, G VedalaMichigan Heart at St. Joseph Mercy HospitalBackground: SPECT myocardial perfusion imaging has increasedsignificantly throughout the United States. Generation of normal valuesusing electrogardiographic gated images for left ventricular end-dia-stolic, end-systolic volumes and left ventricular ejection fraction(LVEDV, LVESV, LVEF, respectively) is recommended, but fre-quently not performed, and often without large patient numbers. Pub-
S120 Abstracts Journal of Nuclear CardiologyJuly/August 2005

lished data are available for normal LVEDV, LVESV, and LVEF;however, approximately 10-15% of patients undergoing stress perfusiontesting are unable to be gated due to arrhythmia, and limited data isavailable for ungated volumes (UV). Additionally, normal values formyocardial mass (LVM) in large number of patients has not been wellestablished.Methods: Using 4D-MSPECT (commercially available myocardial per-fusion analysis software developed at University of Michigan), andgating at 8 frames per R to R interval, LVEDV, LVESV, LVEF, UV andLVM were measured and calculated in low risk patients (nonsmokerswith normal perfusion and lack of known: coronary artery disease,dyslipidemia, diabetes, cerebrovascular accident, family history ofpremature coronary artery disease) who underwent stress myocardialperfusion imaging for clinical indications.Results: (mean � standard deviation)
Gender (n)LVEDV
(mL)LVESV
(mL)LVEF(%)
UV(mL)
LVM(g/m2)
Male (105) 99 � 21 38 � 14 62 � 8 72 � 17 66 � 8Female (116) 73 � 19* 22 � 11* 71 � 8* 48 � 15* 64 � 9
*p � 0.001 vs. male
No difference in male and female ages (59�12 vs. 60�13 years, respec-tively). Body mass index (BMI) was greater in males (29�5) vs. females(27�5). UV correlated well with LVEDV and LVESV (r�0.92, r�0.89,respectively).Conclusions: Normal Limits (� 2 standard deviations)
GenderLVEDV
(mL)LVESV
(mL)LVEF(%)
UV(mL)
LVM(g/m2)
Male 57-141 10-66 46-78 38-106 50-82Female 35-111 0-44 55-87 18-78 46-82
Female left ventricular volumes and ejection fractions are significantlydifferent from males using this imaging modality, as shown in previousliterature. No difference in myocardial mass between genders. UV corre-lated well with LVEDV and LVESV.
34.33ROLE OF NUCLEAR STRESS TEST AS A NON INVASIVE TOOLIN DETECTION OF ISOLATED AND SIGNIFICANT LEFT MAINCORONARY ARTERY DISEASE: THERE IS NO UNIQUE PATTERNOF PERFUSION DEFICITNM Mahajan, VS Shetty, DT Thekkott, GH Hollander, AG Greengart, JSShani, EL LichsteinMaimonides Medical Center, Brooklyn, NYBackground: Left main coronary artery (LMCA) obstruction is the mostsevere coronary disease. The data on use of nuclear stress test to identifypatients with Isolated And Significant Left Main Coronary Artery Disease(ILMCAD) is scarce.Methods: We compared nuclear stress test results for patients withILMCAD (n�25; Group I) with stress results of patients with isolated LADdisease (n�25; Group II). Group I was selected over a period of 10 years.We compared electrocardiographic portion and perfusion deficits in thestudy groups.Results: Electrocardiography portion of stress tests was non-revealing. Ingroup I, perfusion deficits were absent in 4 (16%) patients. The differentpatterns are compared in figure 1. Inferolateral and inferior wall ischemiawere commonly seen in group I as compared to significantly higherproportion (p�0.02) of anterior wall ischemia in Group II. The perfusiondeficits in group I were independent of site of LMCA stenosis, coronaryartery dominance, electrocardiogram changes, and severity of symptoms.Conclusion: This is the largest series of nuclear stress test results analysisinvolving ILMCAD. There is no unique pattern of ischemia associated withILMCAD. Nuclear stress test may vary from being normal to diffuseischemia in 3 vessel distribution. Its role may be limited to being an adjunct
to clinical parameters including electrocardiography for diagnosing ILM-CAD.
Figure 1: Comparison of perfusion deficit pattern in study groups.
34.34SPECT MYOCARDIAL PERFUSION IMAGING IN HYPERTROPHICCARDIOMYOPATHY PATIENTS AFTER ALCOHOL SEPTALABLATIOND Mehta, RA Aqel, R Gupta, GJ Zoghbi, J Heo, AE IskandrianUniversity of Alabama at BirminghamBackground: Alcohol septal ablation (ASA) is an emerging treatment forhypertrophic obstructive cardiomyopathy (HOCM) with advanced symp-toms. We evaluated the use of SPECT in HOCM patients to study theirperfusion pre and post septal ablation.Methods: Resting gated SPECT was performed with Tc-99m myoview in14 patients before and 1-4 days after ASA.Results: There were 3 men and 11 women aged 55 � 22 years. The leftventricular (LV) outflow gradient decreased from 63 � 23 to 7 � 6 mm Hgafter ASA. There was no difference in the mean LV ejection fraction before andafter ASA (p�0.24). Perfusion abnormality at the antero-basal region was seenin all patients after ASA and measured 5-10% of the LV myocardium. Thelung/heart ratio did not change significantly from 0.3 � 0.09 to 0.32 � 0.08 af-ter ASA (p�0.43). The septal/lateral wall count ratio decreased from0.95 � 0.1 to 0.77 � 0.15 (p�0.001). There was no significant correlationbetween defect size and change in pressure gradient (r�0.13, p�0.68). Therewas no correlation between the defect size and the peak CK (r�0.42, p�0.13),peak CK-MB (r�0.53, p�.051) or TnI (r�0.15, p�0.62).Conclusions: Myocardial SPECT perfusion imaging can be used to assessinfarct size after ASA. The defects are small by quantitative analysis and donot alter LV function or size. The most remarkable observation is that smalldefects in the appropriate location result in almost complete amelioration oflarge pressure gradient.
34.35PREVALANCE OF INCIDENTAL NONCARDIAC FINDINGS ONSPECT PERFUSION STUDIESM Raza, G Panjrath, M Meesala, A Ghanbarinia, D JainDrexel University College of Medicine, Philadelphia, PAObjective: To determine the frequency and clinical relevance of incidentalbut significant noncardiac findings (NCFs) in patients with known orsuspected coronary artery disease on stress-rest SPECT perfusion studies.Methods: 610 consecutive patients undergoing SPECT perfusion, wereanalyzed for the presence of noncardiac findings. All the images wereinterpreted by a single observer with meticulous attention to the presence ofincidental noncardiac abnormalities on raw rotating images. Wherevernoncardiac abnormalities were noted, an attempt was made to confirm theirpresence and significance by other imaging modalities and by clinicalfollow up of the patients.Results: Of the 610 patients, a total of 48 (8%) noncardiac findings wereobserved. Of these, 71% were abdominal abnormalities (Hepatosplenomeg-
Journal of Nuclear Cardiology Abstracts S121Volume 12, Number 4;S14-S25

aly, hiatal hernia, ascites, gastrointestinal tumors) and 29% thoracic (Breast,Lung and Mediastinal abnormalities).Conclusions: Incidental noncardiac findings are relatively common inpatients undergoing SPECT myocardial perfusion imaging and often timeprovide first clue to the presence of significant non-cardiac disease. It’sprudent to diligently look for these abnormalities. These can revealmalignancies involving lung, mediastinum, lymph nodes and abnormalitiesof gastrointestinal tract.
34.36EXTRACARDIAC LESIONS: WHY MORE PROMINENT ON THEREST SPECT?I Seo, E Del Priore, A Almonte, R Kappes, A Fedida, K OngThe Brooklyn Hospital Center, Brooklyn, NYTc-99m tetrofosmin or sestamibi (Tc-complex) has been shown as anexcellent tumor-seeking agent as Tl-201. Incidental discovery of extracar-diac lesions, particularly breast and lung cancer, during myocardial perfu-sion scan has been reported frequently. It has been strongly recommendedthat these incidental findings should be reported to the referring physiciansfor further investigation. While evaluating these lesions, we noticed thatthese lesions were better defined on the rest than the stress SPECT.Objective: To verify our observation of lesions having greater uptake on therest SPECT and to postulate its pathophysiologic mechanism.Method: All patients underwent one-day protocol of rest and stress SPECTusing Tc-complex. Whenever we noticed extracardiac lesions on cine display,additional reconstruction of the chest was performed. We calculated the relativeratio between the lesions and myocardium (L/M) on both rest and stressSPECT. We also calculated the differences between the rest and stress L/M.Result: Since January 1, 2003, we found extracardiac lesions in 21 patients:14 at the breast and 7 at the lung/mediastinum. When there were multiplelesions, we evaluated the lesion with the highest uptake. Sixteen of 21patients showed 11% to 950% higher L/M on the rest, 3 patients had 5% to23% lower L/M on the rest, while 2 patients had equal L/M. Majority of thepatients used IVP (17 of 21) and tetrofosmin (19 of 21). We found nosignificant statistical differences among exercise, IVP and dobutamine aswell as between tetrofosmin and sestamibi. Five patients with thyroidabnormalities (3 with diffuse toxic goiter; 1 with substernal goiter; 1 with ahot nodule) were used as control: all 5 also showed significantly higherthyroid/myocardial ratio on the rest SPECT.Conclusion: Relatively higher delivery of blood to the myocardium duringstress would cause the relative reduction of the passive, membrane poten-tial-dependent influx of Tc-complex into the tumor cell. At rest, it would bereversed: the passive, membrane potential-dependent influx of Tc-complexinto the tumor cell would be higher than into the myocardium. As a result,L/M would be higher on the rest than the stress SPECT. Sixteen of 21(76.2%) patients showed higher L/M on the rest SPECT. In 2 patients, thelesions were almost unrecognised on stress SPECT.
34.37CHANGES IN NORMAL CARDIAC INTENSITY DISTRIBUTIONDUE TO TRANSLATION DIFFERENCES BETWEEN CT ANDSPECT FOR A HYBRID IMAGING SYSTEMJN Kritzman, S Dey, JR Corbett, EP FicaroUniversity of Michigan Health System, Ann Arbor, MIBackground: With the introduction of hybrid SPECT/CT imaging systems,misregistration errors between the SPECT and CT images can have asignificant impact on the attenuation corrected SPECT images. The purposeof this study was to quantify the affects of misalignment from inducedmisregistrations in normal cardiac phantom SPECT/CT images to determinethe acceptable tolerances and required quality control for registration.Methods: The Siemens Symbia SPECT/CT (6 slice CT) was used toacquire images of an anthropomorphic phantom (Data Spectrum) with anormal cardiac insert. CT images were acquired first using a breath hold ACprotocol (35 mAs, 0.6 second rotational speed and a pitch of 1.0), followedby the acquisition of SPECT images as outlined by the ASNC imagingguidelines. Prior to correcting the SPECT for attenuation, the CT attenua-tion maps were translated up to �/-15mm along each of the three body axesn 5mm increments producing 19 data sets (18 translated, 1 baseline).Attenuation corrected (AC) images were reconstructed for each of the 19CT attenuation maps. The AC normal activity distribution in the heart was
resampled into polar map format and regionally quantified using a 17segment overlay.Results: Changes of 5mm or less produced less than a 2% change inuniformity and the images were not discernibly different visually. Withtranslation offsets of 10mm or greater, noticeable differences were apparentcompared to the baseline distribution producing changes in uniformity aslarge as 6%. For this phantom and heart orientation, translations along thez-axis toward the head produced the most significant change that was seenin the lateral wall of the heart.Conclusion: Small misregistrations offsets between the attenuation mapsand SPECT images can produce significant changes in the normal distribu-tion of activity in the heart. Offsets of 10mm or more along the z-axis of thebody will not be uncommon for sequentially acquired images as the heartchanges position due to changes in breathing. It is critical that accurateregistration QC tools be provided for these systems for the user to correcttranslation offsets between the CT and SPECT data sets prior to correctingthe SPECT data for photon attenuation.
34.38COMPARISON OF END-EXPIRATORY BREATH HOLD ANDSHALLOW BREATHING PROTOCOLS FOR CT BASED ATTENU-ATION CORRECTION OF 99TC-SESTAMIBI MYOCARDIAL PERFU-SION IMAGES USING MULTI-SLICE SPECT-CTS Dey, JN Kritzman, EP Ficaro, JR CorbettUniversity of MichiganBackground: Image artifacts caused by photon attenuation affect thediagnostic accuracy for coronary heart disease (CHD) of cardiac SPECTperfusion studies. Improvements have been demonstrated using attenuationcorrection. The availability of hybrid multi-slice SPECT-CT presents newchallenges, one of which is the best breathing protocol for acquisition of theCT used for attenuation correction. The purpose of this study was toevaluate two CT image acquisition protocols: end tidal expiration breathhold (BH) and shallow free breathing (SFB).Methods: Using a new multi-slice SPECT-CT imaging system (SYMBIA-6),31 patients were studied. All patients were imaged using stress 99Tc -Sestamibiprotocol and CT based attenuation correction. BH CT acquisitions wereacquired with 0.6 sec rotational speed, effective mAs of 35 kV and pitch of 1.0.SFB CT acquisitions were acquired with 1.5 sec rotational speed, effective mAsof 70 kV, pitch of 0.45. Patients were risk stratified based on Diamond andForrester (DF) criteria to analyze probability of coronary disease. SPECTimages were reconstructed for attenuation and scatter correction. Uncorrected(NC) images were compared to CT corrected images using 4D-MSPECT. Allperfusion defects were semi-quantitatively assessed by scoring the severity andextent in each of the three coronary artery distributions (LAD, LCX, and RCA)using the standard 17 segment model.Results: For low likelihood patients(DF�5%), quantitative analysis showedimproved normalcy with AC compared to NC imaging however there wereno significant differences in image scores between the BH (4.82 �/-1.65)and SFB (5.18 �/-1.55) CT protocols. In the intermediate likelihoodpatients (DF 6-50%), mean scores were NC: (4.85 �/- 0.83), BH (1.85 �/-0.55) and for SFB (1.31 �/-0.28). Finally, in the high likelihood patients(DF50%), mean scores were NC: (12.14 �/- 1.59), BH: (7.57 �/-1.77), andSFB (7.29�/-1.64). Defects associated with angiographically confirmeddisease were preserved while attenuation artifacts were well corrected.There was no significant difference in image quality between the BH andSFB acquisitions although both were generally judged better than the NCimages.Conclusions: SPECT imaging with CT based AC showed a consistentimprovement in image quality and apparent diagnostic accuracy for theidentification of CHD compared to conventional NC imaging. There wereno significant differences between the BH and SFB CT acquisitions forattenuation correction in this patient population.
34.39CORONARY ARTERY FRACTIONAL FLOW RESERVE AND ITSCORRELATION WITH THE SEVERITY OF REVERSIBLEMYOCARDIAL PERFUSION DEFECTS ON GATED SPECT INPATIENTS WITH CORONARY ARTERY DISEASESA Stowers, GC Tomlinson, MS Cunningham, NM GuilarteSouthpoint Cardiology Associates, Jacksonville, FL
S122 Abstracts Journal of Nuclear CardiologyJuly/August 2005

Background: Calculation of coronary fractional flow reserve (FFR) hasbeen shown to provide additional valuable information in determining alesions clinical significance. However FFR determinations between 0.8 and0.75 have been described in the literature as borderline significant. In thisstudy we have correlated the FFR with the severity of the reversibleperfusion defect in the distribution of the coronary artery being measured todetermine whether the correlation might provide added benefit in patientswith coronary artery stenosis and borderline significant FFR.Methods: FFR was measured in 18 arteries in17 patients who were referredfor coronary angiography and who had undergone Gated SPECT myocar-dial perfusion imaging and were felt to have a significant coronary arterystenosis that might be responsible for the patient’s symptoms. The pressurewire was passed distal to the stenosis in the coronary artery to be measured.Intracoronary NTG 100mcg was administered followed by maximal hyper-emic stimulation with 48mcg and 96mcg of intracoronary adenosine. FFR
was then correlated with the severity of the reversible myocardial perfusiondefect in the distribution of the coronary artery measured. 20 myocardialsegments were divided into the 3 epicardial coronary territories. Segmentswere scored normal�0; slightly reduced�1; moderately reduced�2; se-verely reduced�3; and absent�4. A reversible segment is defined as onewhere the stress score is greater than the rest score and the stress score is atleast 2.Results: All the coronary arteries with a FFR � 0.82 (n�11) had asignificant reversible perfusion abnormality. All coronary arteries (n�5)with a borderline significant FFR had a reversible perfusion severityscore � 5. Only one coronary artery with a FFR � 0.82 had a reversibleperfusion severity score � 1 (n�7).Conclusion: Correlating borderline FFR with the severity of a reversibleperfusion defect may be beneficial in selecting appropriate candidates forpercutaneous coronary intervention.
Journal of Nuclear Cardiology Abstracts S123Volume 12, Number 4;S14-S25

ORAL ABSTRACTS – YOUNG INVESTIGATOR COMPETITIONSATURDAY, OCTOBER 1, 2005, 1:30–3:00PM
37.01OPTIMIZATION OF ACQUISITION AND PROCESSING PROTOCOLSFOR I-123 CARDIAC SPECT IMAGING WITH LOW-ENERGY HIGH-RESOLUTION COLLIMATORSJ Chen, JR Galt, RD Folks, EV Garcia, I CarrioEmory University School of Medicine, Atlanta, GeorgiaBackground: Multiple, low-abundance, high-energy photons in I-123cardiac imaging causes septal penetration in the collimator, challengingquantification. 3D Deconvolution of the Septal Penetration (DSP) has beendeveloped to allow the use of the widely available low-energy high-resolution (LEHR) collimator in I-123 cardiac SPECT imaging. This studyis to optimize its acquisition and processing protocols.Methods: A cardiac torso phantom, loaded with a heart-to-background ratio(HBR) of 23.4, was imaged with a GE Millennium VG/Hawkeye system.SPECT acquisition was done as 25 seconds per projection, 60 projectionsover 180°. Two energy window (EW) setups were examined: 1) 20% EWat 159 keV, 25% EW at 126 keV; and 2) 15% EW at 159 keV, 28% EW at128 keV. HBRs were computed from: planar projection (PP), filteredbackprojection (FBP), iterative reconstruction (IR) with DSP, IR withattenuation correction (AC), and IR with AC and DSP (ACDSP). Short-axisuniformity (UN, standard deviation / mean counts) and defect contrast (DC,(maximum – minimum) / maximum counts) were analyzed to compare thetwo EW setups and to optimize the filter parameters.Results: The calculated HBRs, uniformities, and defect contrasts are listedin the table below. DSP was essential for accurate quantification. 15% EWsetup produced better quantification, uniformity and defect contrast.Conclusion: The marginally optimized acquisition (15% photopeak EW,28% scatter EW) and processing (DSP or ACDSP, 3D Butterworthpost-filtering (cutoff frequency: 0.5 Nyquist; order: 5)) protocols promise toproduce accurate quantification and acceptable image quality with LEHRcollimators. These results should next be confirmed in patient studies andvalidated by a prospective clinical trial.
PP FBP DSP AC ACDSP Actual
15% Peak EW HBR 3.64 8.2 22.2 14.2 21.0 23.4DC N/A 0.469 0.535 0.400 0.501 0.5UN N/A 0.060 0.083 0.054 0.080 0 (ideal)
20% Peak EW HBR 3.59 8.9 19.5 13.9 20.2 23.4DC N/A 0.418 0.535 0.377 0.483 0.5UN N/A 0.060 0.118 0.066 0.116 0 (ideal)
37.02IMPROVED EARLY POST-STRESS TC99M-SESTAMIBI MYO-CARDIAL PERFUSION SPECT USING AN ENERGY-BASEDSCATTER CORRECTION METHODBL Hsu, JA Case, TM Bateman, SJ CullomCardiovascular Imaging Technologies, Kansas City, MOBackground: Conventional same-day Tc-99m SPECT protocols requiresignificant delay prior to imaging and provide only delayed post-stressfunction. Early post-stress SPECT (EPS) with ECG-gating may provideimproved detection of coronary artery disease and greater laboratoryefficiency. However, EPS accuracy can be limited by scatter and artifactsfrom extracardiac activity. We therefore studied the feasibility of perform-ing EPS using a novel energy-based scatter correction method (IESD, Hsuet al JNC 2003) to improve the quality of EPS images.Methods: 20 patients (10 normal/10 abnormal, 9 adenosine, 11 TMET)referred for clinically-indicated same-day rest/stress Tc-99m-sestamibi(MIBI) SPECT with attenuation correction (AC) had EPS in addition totheir clinical scan. MIBI was injected 3 min prior to cessation of adenosine,or at peak TMET stress. On average, EPS was started 6.0 min post-MIBIinjection and the clinical stress acquisition followed 30-60 min after EPS.EPS included simultaneous Gd-153 AC using a research list-mode acqui-sition on a Cardio60 dual 90o scanner (Philips Medical Systems, CA). Allstress images were acquired with 30s/stop, 32 stops and 180o RAO-LPO arc.List-mode data was rebinned to form energy spectra of the emissionprojections. IESD was applied to EPS data for separation of photopeak and
scattered photons. EPS images with AC and motion corrections were thenreconstructed from non-corrected and IESD-corrected projection imagesusing MLEM (30 iter). Clinical stress images were processed with Van-tagePro/EXSPECTII for comparison. Clinical images were sampled withQPS™ and analyzed to determine normal segment variance. Paired t-testanalysis was applied to the clinical, non-corrected EPS and IESD-correctedEPS segmental scores derived from QPS to evaluate the effect of IESD.Results: All EPS studies showed a greater proportion of counts in theextracardiac region adjacent to the inferior myocardial wall compared withthe clinical studies (7 (35%) hepatic uptake only, 13 (65%) hepatic andbowel uptake). Patient motion was significantly greater in EPS than theclinical studies (p�0.05). IESD reduced these counts by 24%, improvingthe defect contrast by 11% in the abnormal studies and reducing the ratio ofextracardiac to normal myocardial counts by 20%. Furthermore, the EPSimages with IESD correction showed a greater correlation with the clinicalimages in defect segments (r�0.9, p�0.55) compared to non-corrected EPSimages (r�0.78, p�0.13), all while preserving the correlation betweennormal segments (r�0.73, p�0.18; r�0.75, p�0.2).Conclusions: IESD scatter correction compensates effectively for scatter-induced artifacts in early post-stress Tc99m-sestamibi myocardial perfusionSPECT and demonstrates the feasibility when combined with attenuationand motion corrections.
37.03ATTENUATION-CORRECTED ADENOSINE STRESS TC-99MSESTAMIBI MYOCARDIAL PERFUSION SPECT NORMAL FILES:PROSPECTIVE VALIDATION AND COMPARISON TO EXERCISESTRESS NORMAL FILESFP Esteves, CA Santana, RD Folks, TL Faber, TM Bateman, EV GarciaEmory University School of Medicine, Atlanta, GABackground: The aim of the study was to determine and prospectivelyvalidate the normal distribution and abnormality criteria for attenuation-corrected (AC) adenosine stress Tc-99m sestamibi myocardial perfusionSPECT and to compare it to AC exercise stress normal files.Methods: All studies were AC using Gd-153 transmission sources andpatients stressed using adenosine. Emory Cardiac Toolbox (ECTb) quanti-tative software was used for processing and interpretation. 59 patients (meanage 65 � 12 yrs, 29 men) with low likelihood (LLK) of coronary arterydisease (CAD) were used to define the normal distribution. Student t-testwas used to compare the mean normal distribution (MND) in each of 17myocardial segments between AC adenosine and AC exercise stress. A pilotgroup of 114 patients (mean age 63 � 11 yrs, 67 men) was visually scored(0-4) by consensus of 2 expert readers. Optimum criteria for abnormalitywere determined by ROC analysis for each of 7 myocardial wall segments.Criteria were prospectively validated in 90 patients (mean age 63 � 10 yrs,42 men) who had coronary angiography within 3 months of the myocardialperfusion study and in 20 LLK patients (mean age 62 � 15 yrs, 7 men).
S124 Journal of Nuclear CardiologyJuly/August 2005

Results: The MND was not statistically different in 16/17 myocardialsegments between AC adenosine and AC exercise stress. MND in segment10 (mid inferior wall) was significantly higher in the AC adenosine normalfile population (p�0.001). Validation of optimized AC-adenosine stresscriteria using the AC-adenosine stress prospective group yielded sensitivityand specificity of 80% and 54% respectively for detection of CAD and anormalcy rate of 95%. The accuracy was not statistically different using theAC-exercise stress normal files and corresponding abnormality criteria.Conclusions: We have developed a normal database for AC adenosinestress Tc-99m sestamibi myocardial perfusion SPECT. Mean normaldistribution is statistically similar in 16/17 myocardial segments ascompared to AC exercise stress. Prospective validation also yieldedsimilar results regardless of which normal files were used. Validationof non-AC adenosine stress studies will follow to determine whetherAC adenosine stress specific normal database is needed for optimalresults.
37.04ASSESSING THE DIAGNOSTIC ACCURACY OF CT ASATTENUATION CORRECTION FOR 99TC-SESTAMIBI SINGLEPHOTON EMISSION COMPUTED TOMOGRAPHY (SPECT)-PRELIMINARY OBSERVATIONSS Dey, JN Kritzman, EP Ficaro, JR CorbettUniversity of Michigan, Ann Arbor, MIBackground: Image artifacts caused by photon attenuation commonlyaffect accuracy (especially specificity) of cardiac SPECT perfusion studies.Several available methods have demonstrated improvements using attenu-ation correction. The purpose of this study was to use a novel imagingtechnique of combined SPECT and fast multislice CT imaging to evaluatethe effect on diagnostic accuracy for coronary heart disease (CHD) usingCT attenuation correction (AC).Methods: Using SPECT-CT (SYMBIA-6), imaging, 31 patients werestudied. All patients were imaged using stress 99Tc-Sestamibi protocol.Patients were risk stratified based on the Diamond and Forrester (DF)criteria using a score of �5% likelihood of CHD as low likelihood normal.Uncorrected (NC) filtered-backprojection images were compared to CTcorrected images (AC). All scans were semi-quantitatively assessed byscoring the severity of perfusion defects in each of the three coronary arterydistributions (LAD, LCX, and RCA) using the standard 17 segment model.Scans were also assessed for overall quality and motion artifacts.Results: For the low likelihood patients (DF criteria) �5%, quantitativeanalyses showed improved accuracy with the AC images. 92% of thepatients showed a significant reduction in their coronary defect perfusionscores with greatest effect in the inferior wall. 8% of this subgroupshowed an increase in coronary defect perfusion score intensifyingdefects in the LAD distribution. For intermediate likelihood patients6-50% (DF criteria) and high probability patients �50% (DF criteria),quantitative analyses also showed significant reductions in overallcoronary defect perfusion scores. Defects associated with angiographi-cally confirmed disease or defects judged as definite by another imagingsystem were well preserved while attenuation artifacts were corrected.81% of the patients showed significant improvements in scan qualitywith SPECT-CT system. There was a consistent increase in apparentapical thinning compared to other AC SPECT systems requiring thedevelopment of new normal databases.Conclusions: SPECT-CT imaging showed a consistent improvement inimage quality and apparent diagnostic accuracy for the identification ofcoronary heart disease compared to conventional uncorrected imaging.These scans allow for better localization of disease and decrease patientattenuation artifacts.
37.05DUKE TREADMILL SCORE WITH MYOCARDIAL PERFUSIONIMAGING PREDICTS EARLY REVASCULARIZATION IN WOMENJB Lundbye, GL Noble, D Katten, A Ahlberg, WE Boden, GV HellerIntroduction: The Duke Treadmill Score (DTS) has been demonstrated tobe a useful tool for the diagnosis of coronary artery disease (CAD) inwomen. However, false positive tests, which subject patients to downstreamconfirmatory testing, are common consequences for women undergoingETT only.
Methods: To determine the referral rate for revascularization based on DTSand myocardial perfusion imaging (MPI), we reviewed prospectivelycollected data on 1548 women without known CAD but with intermediateto high pretest risk of coronary artery disease who underwent ETT/MPI withthe endpoint of revascularization within 30 days of testing.Results: Low risk DTS was present in 688 (44%) women, only 2 (0.3%) ofwhich underwent revascularization. In the intermediate DTS risk group,there were 839 (54%) women, of these, 761 had normal MPI, and 78 hadabnormal MPI. Overall revascularization rate among those with intermedi-ate DTS was 3.1%. Of these, revascularization occurred in 6/761(0.8%)with normal and 20/78 (25.6%) with abnormal MPI. (P�0.0001) Overallrevascularization rate in the group with high risk DTS was 28.6%. Likewise,among those with high risk DTS (n�21) 1/14 (7.1%) with normal MPIversus 5/7 (71.4%) with abnormal MPI were revascularized. (P�0.002).Conclusion: In women with intermediate or high risk Duke TreadmillScore, myocardial perfusion imaging results better correlate with referral forearly revascularization than Duke Treadmill Score alone. Stress MPI meritsconsideration for first line testing in women with intermediate or highpretest likelihood of coronary artery disease.
37.06RISK STRATIFICATION OF PATIENTS UNDERGOING DIPYRIDA-MOLE-EXERCISE TC-99M SESTAMIBI GATED SPECT MYO-CARDIAL PERFUSION IMAGINGH Athar, J Thompsen, A Ahlberg, V Sainani, D O’Sullivan, G Cyr, DKatten, GV HellerHartford Hospital, Hartford, CTPrevious studies have shown that exercise combined with dipyridamolestress reduces noncardiac side effects and improves both myocardialperfusion image quality and detection of ischemia and its severity.However, there are limited data on the prognostic value of dipyridamole-exercise (Dip/Ex) stress MPI. This study examines the prognosticvalue of gated tc-99m Sestamibi SPECT in patients undergoing Dip/Exstress.Methods: We assessed 1814 consecutive patients referred for Dip/Ex.Patients were excluded who underwent PCI or CABG �60 days afterDip/Ex, without available gated SPECT information or with incompletefollow-up data. Patients were risk stratified by perfusion alone (using thesummed stress score [SSS]), function alone (using the ejection fraction[EF]), and by using both in combination. Accordingly, a SSS �3 or anEF �50% were considered abnormal. Using both perfusion and functiondata, images with a SSS �3 and an EF �50% were classified as normal,whereas images with a SSS �3 or an EF �50% were abnormal. Patientswere followed for cardiac death (CD) or non-fatal myocardial infarction(MI). Cardiac event rates were annualized.Results: The patients had a mean age of 63�13 years, 54.7% werewomen and 28% had a history of MI, PCI or CABG. In follow-up, 55(3%) patients had CD or MI. Using perfusion alone, patients with a SSS�3 had a higher event rate than those with a SSS �3 (Table). Similarfindings were observed using EF alone. When the SSS and EF were used
Journal of Nuclear Cardiology Abstracts S125Volume 12, Number 4;S26-S28

in combination, patients with abnormal images had an event rate of2.43% versus 0.74% (p�0.006) in those with normal images.
Variable Event Rate Variable Event Rate
SSS �3 0.80% EF �50% 0.80%SSS �3 2.48% EF �50% 3.60%p Value 0.009 p Value �0.001
Conclusion: Using perfusion and function data from gated SPECT is highlyeffective in the risk stratification of patients undergoing dipyridamole-exercise tc-99m Sestamibi gated SPECT imaging. The presence of normalperfusion and function in this population is associated with an excellentcardiovascular prognosis. Therefore, the addition of exercise should beconsidered routine in patients referred for vasodilator stress MPI.
37.07CARDIAC SPECT VARIABLES IN ICD PATIENTS: BEYONDEJECTION FRACTIONA Paiesdana, DR Murthy, BR Khan, J MahenthiranIndiana University, Indianapolis, INBackground: The implantable cardioverter-defibrillator (ICD) improvessurvival in patients (pts) with ischemic cardiomyopathy and reduced leftventricular ejection fraction (LVEF). SPECT perfusion and function vari-ables, beyond EF, in those who get an ICD are not known. Hence, westudied the SPECT variables of a cohort of ICD pts vs. gender and LVEFmatched (�2%) non-ICD patients with ischemic cardiomyopathy.Method: 98 patients who underwent rest, stress, and gated SPECT imaginghad a standard 17-segment, 5-point scale perfusion and wall motion analysisperformed. A regional sum stress score (SSS) and sum rest score (SRS) was
calculated for each major coronary artery territory, as well as a global SSSand SRS. End diastolic and end systolic volumes were determined for eachpt. Regional and global gated sum motion scores (SMS) were alsocalculated. A paired t-test was used to compare the ICD and non-ICDgroups for SPECT variables.Results: The mean age was 61 � 12 years, and 74% of the pts were male.The mean left ventricular EF was 42 � 15%, as measured by gated SPECT.SPECT myocardial perfusion imaging variables in pts with and withoutICDs are shown in the below table (mean � SD). The global SRS (p�0.048)and the global gated SMS (p�0.004) were significantly different between thetwo groups. The right coronary artery (RCA) gated regional sum scoredemonstrated a trend for statistical significance (p�0.073) in ICD pts.
SPECT Variable ICD (n�49) Non-ICD (n�49) p-value
Age 62 � 12 63 � 9 0.777Gender (males) 74% (36) 74% (36) 1.0EF 42 � 15% 42 � 15% 0.358Global SSS 14.7 � 10.8 12.3 � 10.3 0.144Global SRS 13.2 � 10.0 10.2 � 9.8 0.048Global Gated SMS 15.1 � 10.6 11.2 � 10.4 0.004RCA Gated Regional SMS 6.7 � 4.5 5.5 � 5.3 0.073LAD Gated Regional SMS 5.4 � 6.3 4.0 � 5.2 0.188LCx Gated Regional SMS 2.7 � 3.4 2.0 � 3.1 0.305
Conclusion: The degree of abnormal myocardial perfusion at rest (mea-sured by SPECT global SRS) and the extent of wall motion abnormality(determined by the global gated SMS) provide important additional infor-mation to EF in ICD pts. The RCA gated SMS shows a trend towardssignificance when compared to other regional scores.
S126 Abstracts Journal of Nuclear CardiologyJuly/August 2005





























