Embed Size (px)
Citation preview
Thorax (1960), 15, 154.
DETECTION OF BRONCHIAL AND ARTERIAL OBSTRUCTIONBY CONTINUOUS GAS ANALYSIS FROM INDIVIDUAL
LOBES AND SEGMENTS OF THE LUNGBY
P. HUGH-JONES AND J. B. WESTFrom the Department of Medicine, Postgraduate Medical School of London, Hammersmith Hospital
(RECEIVED FOR PUBLICATION AUGUST 21, 1959)
A mass spectrometer was designed specially forclinical respiratory investigation (Fowler, 1957)and it has been in use for general tests of lungfunction for three years. It performs continuousautomatic gas analysis, and has a gas-samplingtube of only about I mm. external diameter at itstip. This fine sampling tube, which is placed atthe patient's lips during general tests of lungfunction, has now been adapted so that it can beinserted down a bronchoscope into any lobar orsegmental orifice which can be seen directly.From the results of bronchoscopic experiments
on anaesthetized dogs it has been found thatcharacteristic patterns of gas concentrationchanges are observed from regional bronchiduring the breathing cycle and that these canbe related to the ventilation, blood flow, andmechanical properties of the relevant lobe orsegment. In this paper we shall first summarizethese results from animal experiments and thenpresent some examples of these characteristicpatterns seen during routine diagnostic broncho-scopy in man and discuss their significance.
APPARATUS AND METHODSMASS SPECTROMETER.-Fowler's instrument provides
a continuous analysis of the changes of gas concentra-tion, with time, of up to four constituents of a gasmixture recorded simultaneously on a four-channeldirect-writing recorder. A general description of theinstrument and its performance has been published(Fowler and Hugh-Jones, 1957), and only a few factspertinent to the present application need be givenhere. For regional sampling at bronchoscopy onlythree channels of the recorder are used to present theresults of gas analysis, and these are set for recordingcontinuously the changes in tension (partial pressure)of oxygen, carbon dioxide, and argon within thechosen lobe or segment. The argon is introducedas an inert gas into the lungs either during a singletest breath, in order to measure the local ventilationwithin the lobe or segment, or continuously into a
given regional bronchus in order to label the gascoming from that particular bronchus. The fourthchannel of the recorder is used either to record thetotal volume flow of gas expired down the broncho-scope during a test expiration or to record thechanges in intra-oesophageal pressure occurring whilethe regional gas sampling is undertaken (see below).The response time of the spectrometer is such that,
were one gas changed instantaneously for another,90% of full-scale deflection for the new gas would begiven within one-tenth of a second. The gas flowdrawn down the sampling tube by the spectrometer isapproximately 20 ml. per minute. Thus, the instru-ment can record the very rapid variations of gasconcentration which are occurring within a lobar orsegmental bronchus during the breathing cycle.
Full-scale deflection on any channel can be adjustedto suit any particular requirement. In routinebronchoscopic work, the oxygen trace is set for 0-200mm. Hg (calibrated from atmospheric air), the carbondioxide from 0-100 mm. Hg (calibrated from a knowngas mixture), and the argon set to a convenientarbitrary scale.
BRONCHOSCOPIC SAMPLING TUBES.-The samplingtube itself consists of about 4 ft. of 0.013 in.(0.33 mm.) bore (0.6 mm. outside diameter) stainlesssteel tubing like that used for fine hypodermic needles.This is heated electrically, to keep water vapour as agas, the heater current being carried to within half aninch of the tip by an outer concentric steel tube of1.2 mm. outside diameter, electrically insulated fromthe finer sampling tube. This arrangement keeps thewhole sampling tube reasonably rigid for ease ofmanipulation down the bronchoscope, but the terminalinch of the inner sampling tube itself is flexible andcan be bent to any convenient angle for insertion intosegmental orifices which are approximately at rightangles to the main bronchi. The fine tip itself iscovered by a small stainless steel wire cage whichscrews on to a 12 B.A. screw fixed 0.25 in. (6 mm.)from the end of the inner sampling tube; this cagekeeps the fine projecting tip in the centre of thesegmental or lobar bronchus and the whole causeslittle interference with the gas flow there (Fig. 1). Theouter steel tube is itself covered by a layer of smooth
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
BRONCHIAL AND ARTERIAL OBSTRUCTION
C
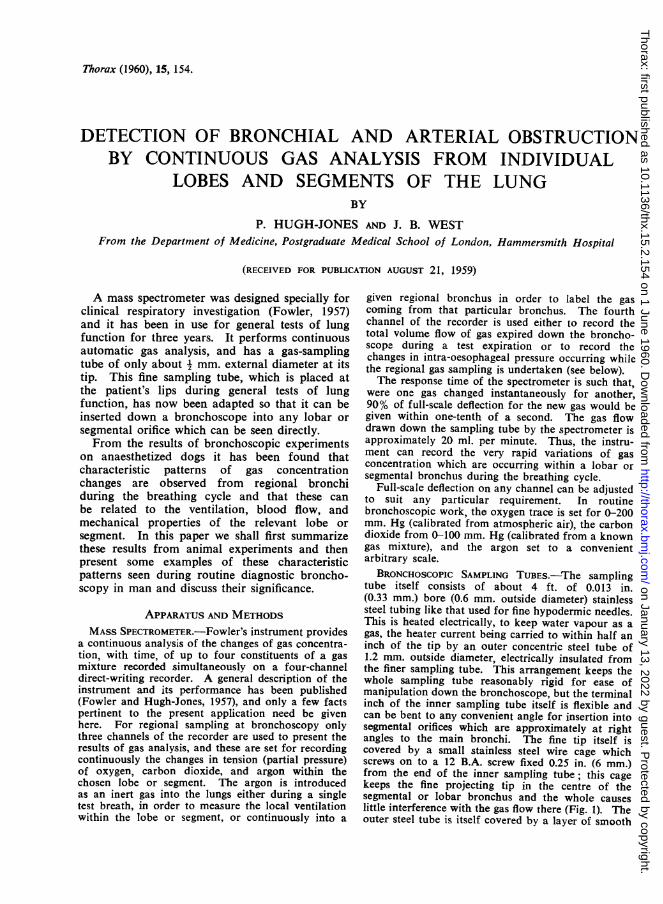
FIG. 1.-Diagram of end of mass spectrometer sampling tube in a
segmental bronchus. W=walls of bronchus. C=protectivestainless wire cage screwed over tip of sampling tube (S.T.),O.T.=outer stainless steel tube, P.C.=polythene covering.
plastic, so that there is adequate thermal insulation.The maximum outside diameter of the main portionof the tube is 2 mm., that of the tip within thebronchus 0.6 mm.
Sampling tube cages are sterilized by boiling, andthe rest of the tube by immersion in a 1% solution of" sudol," a proprietary preparation of solution ofcresol with soap. A two-way tap has been fitted tothe spectrometer so that compressed air can be blowndown the sampling tube to clear it after sterilization.Likewise, if the tube becomes blocked during thebronchoscopy, it is withdrawn from the lungs and thetap turned to clear the tube with compressed air. Thetube can then be reinserted into the local bronchusand sampling resumed within less than a minute withlittle disturbance to the calibration of the spectro-meter.
PROCEDURE AT BRONCHOSCOPY.-A local anaestheticis used, though additional sedation is given. Carewith the anaesthetic is important both for efficiency inthe procedure and for the comfort of the patient.The ideal is to have a patient so anaesthetized as tobe practically unaware of the procedure but co-opera-tive enough to take a deep breath if an argonmeasurement of local ventilation is required.For most adults a 25 mg. tablet of promethazine
hydrochloride is given by mouth four hours beforethe procedure, and, one hour before, a subcutaneousinjection of a mixture of 50 mg. of promethazinehydrochloride, 100 mg. of pethidine, and 0.5 mg. ofhyoscine hydrobromide. Further intravenous pethi-dine is used at the time of bronchoscopy, should itbe necessary in nervous patients. A 2°/ lignocainesolution is used for local anaesthetic, with a limit of15 ml. If intra-oesophageal pressure measurementsare to be taken, a rubber balloon is inserted into theoesophagus before the bronchoscopy, when theMackintosh laryngoscope is being used to spray thevocal cords and trachea with lignocaine.
L
A Negus bronchoscope is used for the broncho-scopy. This is inserted and the tree fully inspected inthe usual way. The sampling tube from the spectro-meter is then passed down the bronchoscope into therequired lobar or segmental orifice so that the wholecage is within the relevant orifice. When this hasbeen done, the bronchoscope itself is withdrawn intothe trachea (because animal experimental work hasshown that a bronchoscope in the main bronchi causesconsiderable interference with the normal lung venti-lation) and the continuous record of the local gasconcentration changes taken with the spectrometer.The bronchoscope is then reinserted lower down thebronchial tree, the sampling tube moved elsewhere,and the procedure repeated as needed.
If oesophageal pressure records are to be taken theoesophageal balloon is linked to an electro-manometerbefore the bronchoscope is inserted and the pressureis recorded on the fourth channel of the recorderduring the bronchoscopy.For some purposes, another fine 0.5 mm. tube is
inserted into a bronchus adjacent to that in whichsampling is being done and a stream of argon feddown it. For others, a modified Negus broncho-scope is used which has an inflatable thin rubbercuff 3 in. from its distal end and has a side tube atthe proximal end. When this bronchoscope is with-drawn into the trachea, after the sampling tube hasbeen placed in the regional bronchus, the cuff can beinflated, the side orifice of the bronchoscope attachedby a push-fit to a small perspex valve-box with lowresistance rubber J-valves and a dead space of only20 ml., and the end of the bronchoscope sealed roundthe sampling tube by sliding down a rubber stopper.The whole of the patient's ventilation is then throughthe side tube and valve-box, and on turning a tap hecan take in a single breath of a gas mixture of argon(about 10%) in air from a spirometer. The volumeof the subsequent exhalation from the bronchoscopeis recorded on the fourth channel of the spectrometerrecorder (instead of the oesophageal pressure) byelectrical integration of the signal from a wire-meshflow-meter attached to the exit of the valve-box.When the tap is turned for this single-breathprocedure during an expiration, the dead space ofvalve-box and tubing is automatically flushed withargon-air mixture before the test inspiration.
Since this work was started other methods ofmeasuring air flow in the bronchial tree have beendeveloped so that the use of the cuffed bronchoscopeis often unnecessary (West, 1960). Thus, most of thetracings obtained from patients, described below, donot indicate an argon single breath.When regional gas sampling is completed with any
of these techniques, a biopsy specimen can be taken,if required, in the usual way. Thus the wholeprocedure can be done during routine diagnosticbronchoscopy.With practice it is possible, in most patients, to
insert the sampling tube into the right upper lobe,middle lobe, and the individual apical and basalsegments of the right lower lobe. On the left it can
155
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
P. HUGH-JONES and J. B. WEST
be inserted into the upper lobe and into the individuallower lobe segments. It is sometimes possible toinsert it into either of the two divisions of the leftupper lobe. It is fortuitous and rare to be able toinsert it into any of the individual segments of theright upper or middle lobes, and it is probably nearlyalways impossible to enter the segments of the lingulaor of the upper division of the left upper lobe.
INTERPRETATION OF NORMAL PATTERNS OFREGIONAL GAS ANALYSIS
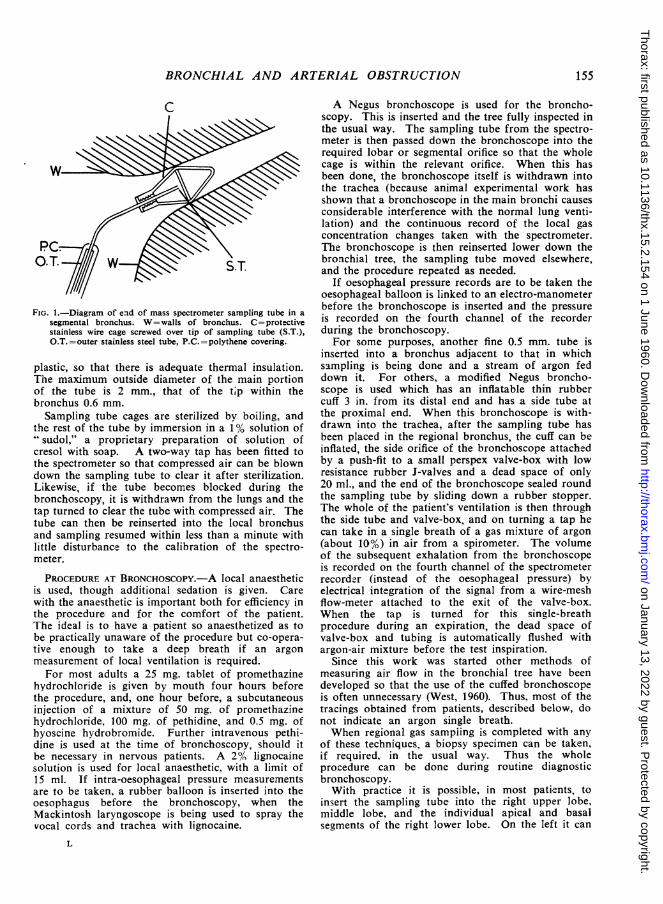
A characteristic record of the changes in gastensions locally within the bronchial tree is seenin Fig. 2, which represents those in the apical seg-ment of the right lower lobe of a patient who was
LLJ0-UTc
cI-
c)
L-
0
LuIOO
Z E
0 5
i0
LU 0SEC.
FIG. 2.-Mass spectrometer record from the apical segment of the right lowerlobe in a patient who appeared to have a normal right lung.
Id at bronchoscopy to have an apparentlynal right tree.ie tracing shows on the top three channels therd of the local changes in oxygen, argon, andon-dioxide tensions during breathing; and on:ottom channel the record of the total volume)as expired from the cuffed bronchoscopeng each expiration.will be seen that the carbon-dioxide tensionhe segment rises to a peak during eachration and that the oxygen curves are almosttirror image of the carbon-dioxide curves.Lng the fourth expiration shown, the argonadded to the air inhaled so that the
tension of argon rapidly rose in thesegment, and then, during the subsequentlong expiration, there is a plateau of con-centration of this gas which is "washedout" by the three succeeding breaths ofair shown in the figure.The interpretation of these segmental
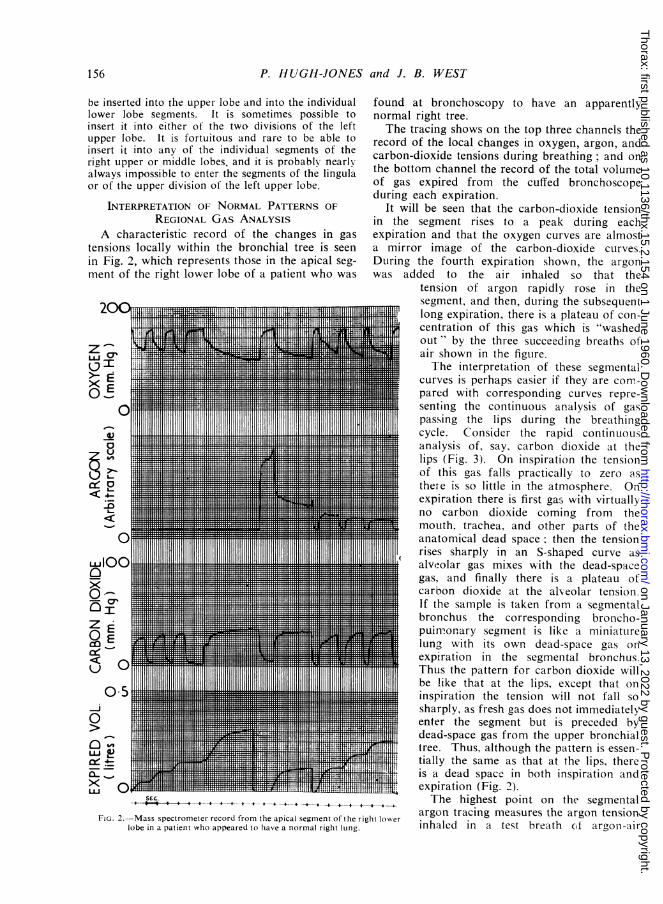
curves is perhaps easier if they are com-pared with corresponding curves repre-senting the continuous analysis of gaspassing the lips during the breathingcycle. Consider the rapid continuousanalysis of, say, carbon dioxide at thelips (Fig. 3). On inspiration the tensioniof this gas falls practically to zero asthere is so little in the atmosphere. Onexpiration there is first gas with virtuallyno carbon dioxide coming from themouth, trachea, and other parts of theanatomical dead space; then the tensionrises sharply in an S-shaped curve asalveolar gas mixes with the dead-spacegas, and finally there is a plateau ofcarbon dioxide at the alveolar tension.If the sample is taken from a segmentalbronchus the corresponding broncho-puin'-onary segment is like a miniaturelung with its own dead-space gas onexpiration in the segmental bronchus.Thus the pattern for carbon dioxide willbe like that at the lips, except that oninspiration the tension will not fall sosharply, as fresh gas does not immediatelyenter the segment but is preceded bydead-space gas from the upper bronchialtree. Thus, although the pattern is essen-tially the same as that at the lips, thereis a dead space in both inspiration andexpiration (Fig. 2).The highest point on the segmental
argon tracing measures the argon tensioninhaled in a test breath cf argon-air
156
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
BRONCHIAL AND ARTERIAL OBSTRUCTION
E
z
z
O TIME\FIG. 3.-Diagram of the continuous changes in carbon dioxide
concentration, recorded at the lips, when a normal subjectexhales. D=gas from upper respiratory dead space, M=mixceddead space and alveolar gas, alv.=alveolar plateau.
mixture. The height of the subsequent plateauduring expiration depends on the dilution of theargon with the gas in the segment and is a measureof the ventilation of the segment relative to itsvolume.The levels of the oxygen and carbon-dioxide
plateaux during expiration are a function of theventilation of the segment relative to its bloodflow. If the perfusion is low compared with theventilation, less carbon dioxide will be added andless oxygen extracted so that the end-expiredcarbon-dioxide tension will be low and the oxygenhigh. Conversely, if the ventilation is poor relativeto blood flow, the end-expired tension of carbondioxide will be greater and that of oxygen less.Hence there is a change in respiratory quotient,which can be related to the ventilation-perfusionratio (West, Fowler, Hugh-Jones, and O'Donnell,1957).
In summary, the expired argon plateau gives anindication of the segmental ventilation relative tothe segmental volume and the oxygen and carbon-dioxide plateaux an indication of the segmentalventilation-perfusion relations. This will be seenin the abnormal tracings to be described below.
INTERPRETATION OF ABNORMAL PATTrERNS FROMANIMAL EXPERIMENTS
TECHNIQUE. IIn order to interpret abnormal tracingsfound in man, dogs were bronchoscoped in circum-stances where the ventilation or blood flow to theleft lower lobe studied could be altered at will. Fulldetails of the technique and the results have alreadybeen published (West and )Hugh-Jones, 1959) and will
only be summarized here in order to make the humantracings intelligible. The animals were anaesthetizedby intravenous pentobarbitone, a tracheal cannulainserted and, under positive pressure ventilation, thechest was opened and screw clamps put round thebronchus and branch of the pulmonary artery goingto the lobe. A perspex respirator was then placedover the dog with both the tracheal cannula andcables controlling the clamps led outside (Fig. 4). Themass spectrometer sampling tube was then introducedinto the lobe, down a bronchoscope, as in the humantechnique, and the bronchoscope withdrawn into thetrachea. With this arrangement, partial obstructionto the ventilation of the lobe or obstruction to theblood supply could be produced at will and the effectsstudied. It was found that repeatable characteristicchanges in the normal lobar pattern of gas-concentra-tion tracing were produced which can be read like anelectrocardiographic pattern (Fig. 5).OBSTRUCTION TO BLOOD FLOW.- When the
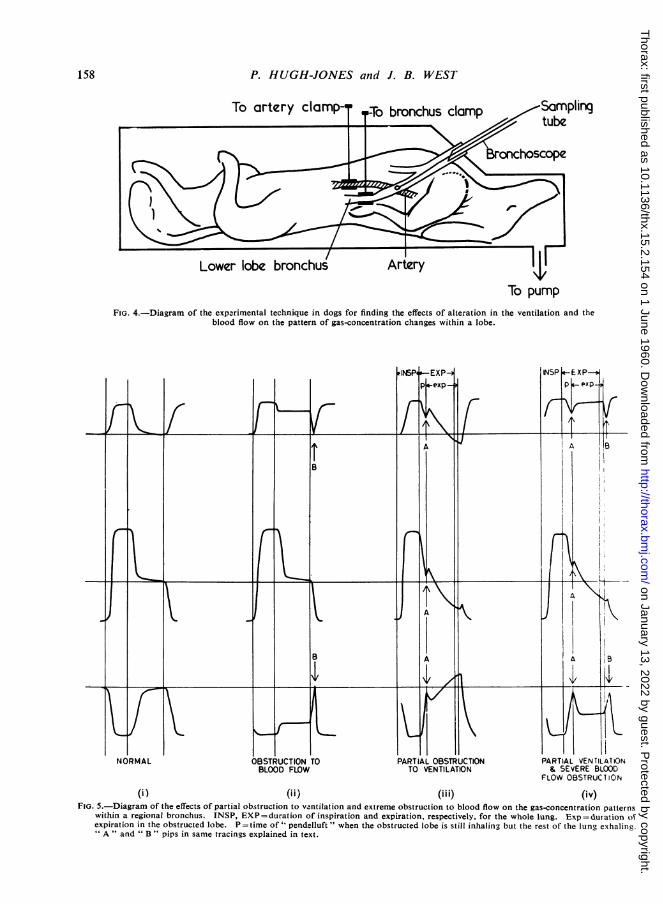
arterial supply to the lobe was completelyoccluded, leaving its ventilation normal (Fig. 5, ii),the expired alveolar CO2 tension falls and theoxygen tension rises since little CO2 is added oroxygen extracted. The argon tracing, determinedby ventilation, remains unaltered. A characteristicsharp peak, which we have called a " pip," markedB in the diagram, appears at the end of thealveolar plateaux of CO2 and 02. This pipactually starts at the beginning of inspiration andarises because gas filling the upper bronchial tree(which was exhaled by the rest of the lung andhas the normal oxygen and carbon-dioxide ten-sions of expired gas) is inhaled into the lobe pastthe sampling tube before fresh air reaches it.
PARTIAL OBSTRUCTION TO VENTILATION.-Whenthe blood flow was normal, but the bronchialclamp was partially screwed up so that the venti-lation of the lobe was grossly reduced, the lobewas seen to ventilate out of phase with the rest ofthe lung because of its delayed inspiration andexpiration. The characteristic pattern shown inFig. 5, iii, was observed. The end-expired argontension is reduced, because of the reduced venti-lation. Secondly, the end-expired CO2 tension isslightly higher and the tension of oxygen slightlylower than normal because of the reducedventilation-perfusion ratio and the slopes of thealveolar plateaux of all three gases are steeper.But most important is a small pip, marked A inthe tracing at the start of the alveolar plateauxof CO2 and 02- This arises because there is asmall time period (P, Fig. 5) when, because of thedelayed inspiration along the obstructed bronchus,the lobe is still inspiring while the rest of thelung is starting to expire. Thus gas is actually" shunted " from adjacent lobes past the tip of the
157
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
158 P. HUGH-JONES and J. B. WEST
To pumpFIG. 4.-Diagram of the experimental technique in dogs for finding the effects of alteration in the ventilation and the
blood flow on the pattern of gas-concentration changes within a lobe.
(i ) (i i ) (i i i) (iv)FIG. 5.-Diagram of the effects of partial obstruction to vantilation and extreme obstruction to blood flow on the gas-concentration patterns
within a regional bronchus. INSP, EXP =duration of inspiration and expiration, respectively, for the whole lung. Exp = duration ofexpiration in the obstructed lobe. P =time of " pendelluft " when the obstructed lobe is still inhaling but the rest of the lung exhaling." A" and " B " pips in same tracings explained in text.
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
sampling tube before the obstructed lobeitself starts to expire (" pendelluft "phenomenon). In so far as the expiredgas from neighbouring lobes has asimilar composition to that from theobstructed lobe, the A pip may not bevery obvious.MIXED OBSTRUCTION.-When marked
arterial obstruction was produced con-currently with partial obstruction to ven-tilation, the pattern shown in Fig. 5 (iv)was seen. Here the argon plateau againreflects the reduced ventilation, the lowCO, and high oxygen alveolar levelsreflect the lack of blood flow, and the Bpip is again apparent. The A pip is nowmore obvious because the compositionof the " pendelluft" gas differs widelyfrom that of the alveolar gas exhaledfrom the experimental lobe whose bloodsupply is obstructed.
ABNORMAL PATTERNS AT BRONCHOSCOPYIN MAN
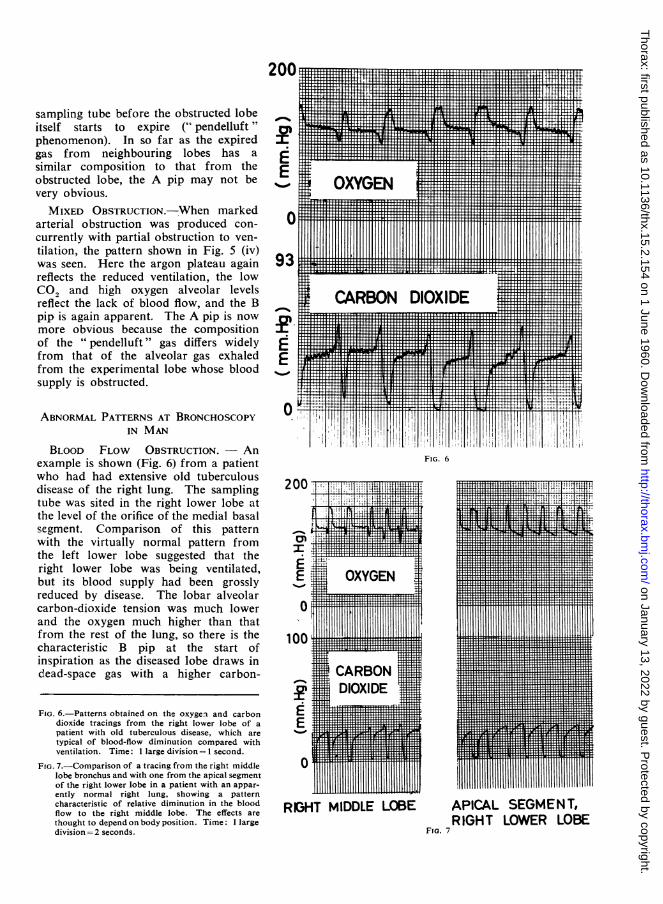
BLOOD FLOW OBSTRUCTION. - Anexample is shown (Fig. 6) from a patientwho had had extensive old tuberculousdisease of the right lung. The samplingtube was sited in the right lower lobe atthe level of the orifice of the medial basalsegment. Comparison of this patternwith the virtually normal pattern fromthe left lower lobe suggested that theright lower lobe was being ventilated,but its blood supply had been grosslyreduced by disease. The lobar alveolarcarbon-dioxide tension was much lowerand the oxygen much higher than thatfrom the rest of the lung, so there is thecharacteristic B pip at the start ofinspiration as the diseased lobe draws indead-space gas with a higher carbon-
EE gg!! W !-1F -,......O 111 11 1111111 111IIIlIIiti IWTF-
C93aov^n^.~~~~~~..^ .n .........liilliill
E|.rT.
0 I'
't!I,lil{UIIIT11111171i1111111lllllllliI I I I & I lli | l s E | X s s s | | lEX I | X [ s l | i | X I I I [e llt!§lllP*illlllllllllUlflIIIIIII_-,l';;lll,[7111[111L1'f 'llllilrx-tl+llllitlllilllll§§liLlululllF,llW[HTlllITllllllllTllilllllllifllf'11 I!I 1
FIG. 6
200
0'2:
TnE2 Tr
100
FIG. 6.-Patterns obtained on the oxygen and carbondioxide tracings from the right lower lobe of apatient with old tuberculous disease, which aretypical of blood-flow diminution compared withventilation. Time: 1 large division=I second.
FIG. 7.-Comparison of a tracing from the right middlelobe bronchus and with one from the apical segmentof the right lower lobe in a patient with an appar-ently normal right lung, showing a patterncharacteristic of relative diminution in the bloodflow to the right middle lobe. The effects arethought to depend on body position. Time: I largedivision= 2 seconds.
RIGHT MIDDLE LOBE
Fra. 7
APICAL SEGMENT,RIGHT LOWER LOBE
............ ........
1 !III Il
orrT
TTliTT
1|1 11Z1 v
T
A.20
I1
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
200
E
E
0
200 i-!_
- -1 L1. ,-'
OXYGEN
0 -
100 - L
c)
E-
0
in,.-i
_L- K!
hAI .
CAVRBON DIOXIDE-77
r-4..
.t
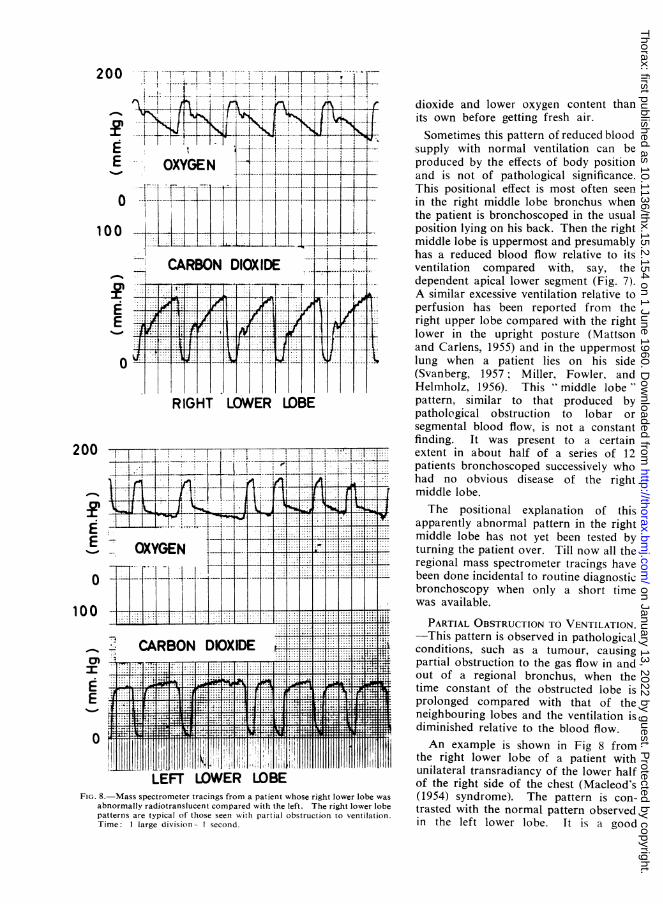
LEFT LOWER LOBEFIG. 8.-Mass spectrometer tracings from a patient whose right lower lobe was
abnormally radiotranslucent compared with the left. The right lower lobepatterns are typical of those seen with partial obstruction to ventilation.Time: I large division second.
dioxide and lower oxygen content thanits own before getting fresh air.Sometimes this pattern of reduced blood
supply with normal ventilation can beproduced by the effects of body positionand is not of pathological significance.This positional effect is most often seenin the right middle lobe bronchus whenthe patient is bronchoscoped in the usualposition lying on his back. Then the rightmiddle lobe is uppermost and presumablyhas a reduced blood flow relative to itsventilation compared with, say, thedependent apical lower segment (Fig. 7).A similar excessive ventilation relative toperfusion has been reported from theright upper lobe compared with the rightlower in the upright posture (Mattsonand Carlens, 1955) and in the uppermostlung when a patient lies on his side(Svanberg, 1957; Miller, Fowler, andHelmholz, 1956). This " middle lobe"'pattern, similar to that produced bypathological obstruction to lobar orsegmental blood flow, is not a constantfinding. It was present to a certainextent in about half of a series of 12patients bronchoscoped successively whohad no obvious disease of the rightmiddle lobe.The positional explanation of this
apparently abnormal pattern in the rightmiddle lobe has not yet been tested byturning the patient over. Till now all theregional mass spectrometer tracings havebeen done incidental to routine diagnosticbronchoscopy when only a short timewas available.
PARTIAL OBSTRUCTION TO VENTILATION.-This pattern is observed in pathologicalconditions, such as a tumour, causingpartial obstruction to the gas flow in andout of a regional bronchus, when thetime constant of the obstructed lobe isprolonged compared with that of theneighbouring lobes and the ventilation isdiminished relative to the blood flow.An example is shown in Fig 8 from
the right lower lobe of a patient withunilateral transradiancy of the lower halfof the right side of the chest (Macleod's(1954) syndrome). The pattern is con-trasted with the normal pattern observedin the left lower lobe. It is a good
I .1 *.- ...I....I....z
IIIl- I! 2~-~ I .I-- I. F-11-1 --!-I-- -rIILff6"
i " A -!
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
BRONCHIAL AND ARTERIAL OBSTRUCTION
example of this pattern and shows both the Apip caused by " pendelluft" gas and the steepalveolar plateaux. Other evidence in this patientshowed that both the blood flow and ventilationof the right lower and middle lobes were reducedcompared with the rest of the lung, but, sincethe ventilation appeared to be less than the bloodflow, the pattern of bronchial obstruction ratherthan that of " mixed " obstruction was obtained.The latter requires partial ventilatory obstructionwith a disproportionately great reduction in bloodflow (as in the conditions of the animal experi-ment).
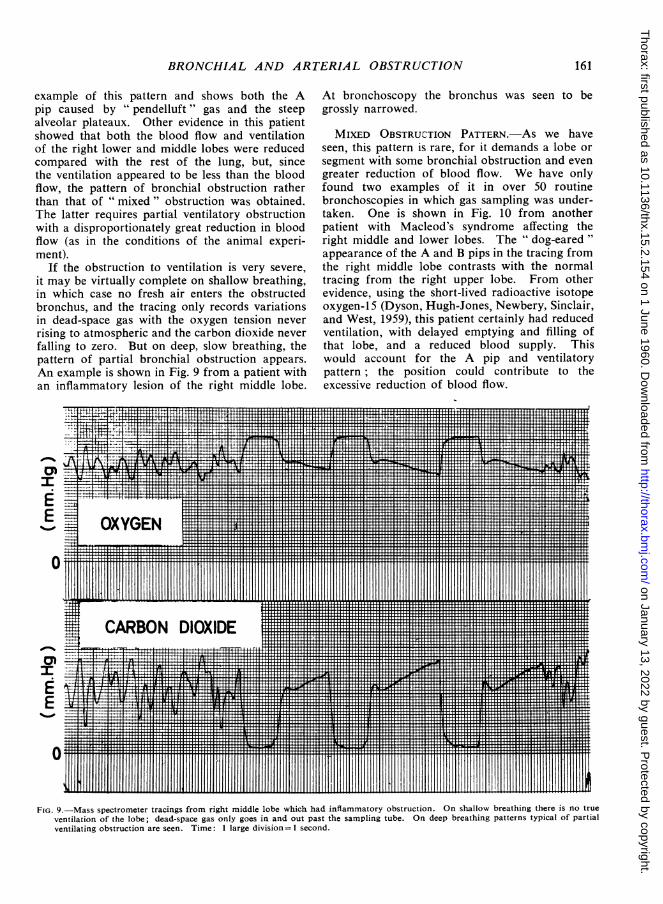
If the obstruction to ventilation is very severe,it may be virtually complete on shallow breathing,in which case no fresh air enters the obstructedbronchus, and the tracing only records variationsin dead-space gas with the oxygen tension neverrising to atmospheric and the carbon dioxide neverfalling to zero. But on deep, slow breathing, thepattern of partial bronchial obstruction appears.An example is shown in Fig. 9 from a patient withan inflammatory lesion of the right middle lobe.
EE
s 21111uOYGENH.. H-Il..
111 .1111 112111111
At bronchoscopy the bronchus was seen to begrossly narrowed.
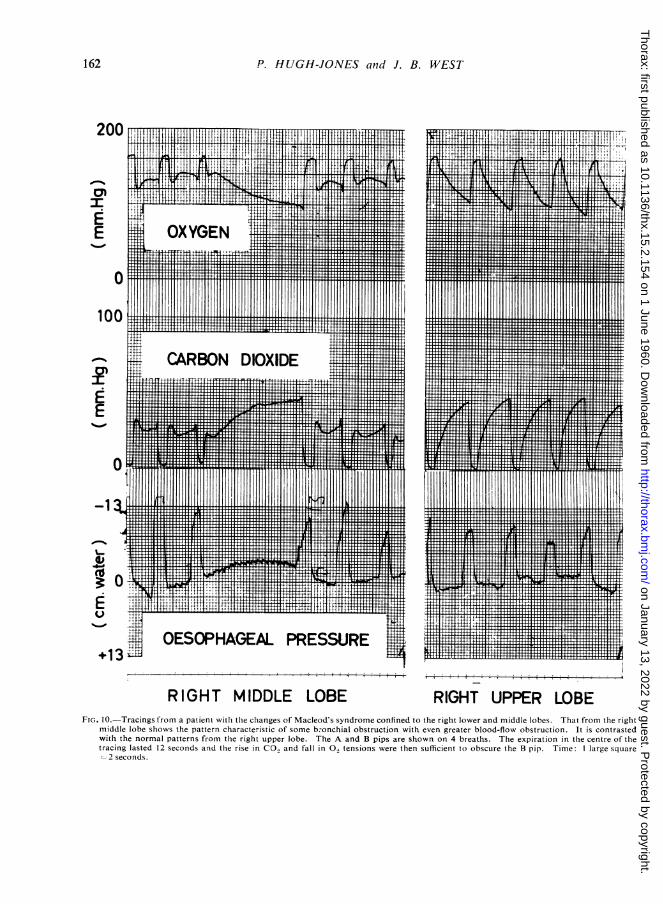
MIXED OBSTRUCTION PATTERN.-AS we haveseen, this pattern is rare, for it demands a lobe orsegment with some bronchial obstruction and evengreater reduction of blood flow. We have onlyfound two examples of it in over 50 routinebronchoscopies in which gas sampling was under-taken. One is shown in Fig. 10 from anotherpatient with Macleod's syndrome affecting theright middle and lower lobes. The " dog-eared "appearance of the A and B pips in the tracing fromthe right middle lobe contrasts with the normaltracing from the right upper lobe. From otherevidence, using the short-lived radioactive isotopeoxygen- 15 (Dyson, Hugh-Jones, Newbery, Sinclair,and West, 1959), this patient certainly had reducedventilation, with delayed emptying and filling ofthat lobe, and a reduced blood supply. Thiswould account for the A pip and ventilatorypattern; the position could contribute to theexcessive reduction of blood flow._111111111111111111111
gg CARBON IH
' EIjv!-l ;lrF_ x * Mr r n 11 E:;
-e_* gIi'*.01lill-i11§[ l^,m Ii!L S ' 1, l#n ' I t- t I i T",STlTM__ , .f llilpli, llillj§Siilull_ tX tili!ll-i}l-AlGlilUlilF I I . i i 1 U 41 F I i I I @ I 111 1 i I> Xtv GT Y wffiffM[lTif: flil_ a I L I 5r i l I I I I l y sS 11. I 1i111111111 IYIH 11 lllibll ;rlulllilllllil_ .f a lilfl X £ £ Isf X . filfl l E x f l X
.... l:, X: 1nTT TT, Tlr s ITT [TE 1 _11
rT aTrT - f T TT f r I 1 X r: T f fT TTT r T I IT * I L I s 1 T a,f[l If lielaxia xrl lullrliIralil
.s r T jr I I r X X X T r lT1 T T rr * r - | X I 1 1L oXrTTllulfExlxlwlillwvgg 1100211'1111111111112
J1IJjJ1JwrFIG. 9.-Mass spectrometer tracings from right middle lobe which had inflammatory obstruction. On shallow breathing there is no true
ventilation of the lobe; dead-space gas only goes in and out past the sampling tube. On deep breathing patterns typical of partialventilating obstruction are seen. Time: I large division= 1 second.
..... ..... ....
.44
D IOXIDE
161
too,
c:1EE
1 on January 13, 2022 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.15.2.154 on 1 June 1960. D
ownloaded from
P. HUGH-JONES and J. B. WEST
200
100~~~~~~~~~~~~~~~~~~~~~~~~~~~~-
E O
E
RIGHT MIDDLE LOBE RIGHT UPPER LOBEFIG. 10. Tracings from a patientw.it the changes of Macleod's syndrome confined to the right lower and middle lobes. That from the right
middle lobe showvs the pattern characteristic of some b:onchial obstruction with even greater blood-flow obstruction. It is contrastedwith the normal patterns from the right upper lobe. The A and B pips are shown on 4 breaths. The expiration in the centre of thetracing lasted 12 seconds and the rise in CO, and fall in 0., tensions were then sufficient to obscure the B pip. Time: I large square
2seconds.~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~--
162
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from
BRONCHIAL AND ARTERIAL OBSTRUCTION16
100
CARBONVT!.. DIOXH IDEk CtM1r"iI14I111I11M I411t11,HH T, ....
E~~~~~~~~~~~~....E~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...
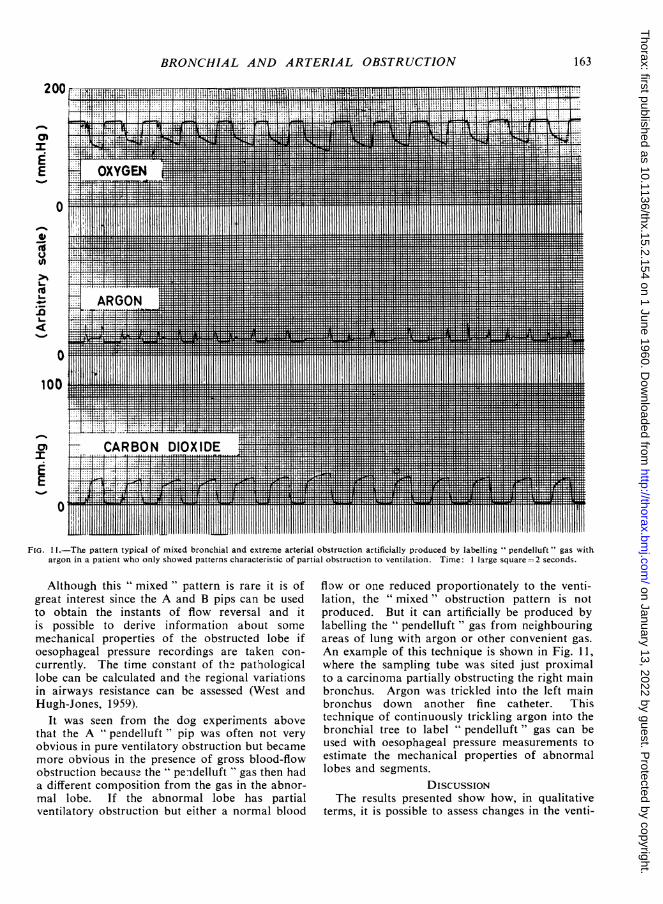
FiG.11.The pattern typical. of. mixedbrnha.n.xr. reilostuto riiilypoue y aeln pnef"gswtargoninapatientwhoonlyshowedpatterns characteristic of partial obstructi3n to ventilation. Time: 1 large square 2 seconds.
Although this " mixed " pattern is rare it is ofgreat interest since the A and B pips can be usedto obtain the instants of flow reversal and itis possible to derive information about someme-chanical properties of the obstructed lobe ifoesophageal pressure recordings are taken con-currently. The time constant of th2 pathiologicallobe can be calculated and the regional variationsin airways resistance can be assessed (West andHugh-Jones, 1959).
It was seen from the dog experiments abovethat the A " pendelluft " pip was often not veryobvious in pure ventilatory obstruction but becamemore obvious in the presence of gross blood-flowobstruction because the " pendelluft " gas then hada different composition from the gas in the abnor-mal lobe. If the abnormal lobe has partialventilatory obstruction but either a normal blood
flow or one reduced proportionately to the venti-lation, the " mixed " obstruction pattern is notproduced. But it can artificially be produced bylabelling the " pendelluft " gas from neighbouringareas of lung with argon or other convenient gas.An example of this technique is shown in Fig. 11,where the sampling tube was sited just proximalto a carcinoma partially obstructing the right mainbronchus. Argon was trickled into the left mainbronchus down another fine catheter. Thistec.-hnique of continuously trickling argon into thebronchial tree to label " pendelluft " gas can beused with oesophageal pressure measurements toestimate the mechanical properties of abnormallobe-s and segments.
DISCUSSIONThe results presented show how, in qualitative
terms, it is possible to assess changes in the venti-
163
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from

P. HUGH-JONES and J. B. WEST
lation and blood flow in different lobes or
segments of the lung during routine bronchoscopy.Other techniques, complementary to the observa-tion of the changes in gas-concentration patterns,are now being developed which should enablemore precise quantitative measurements of theventilation, blood flow, and mechanical propertiesof the different individual lobes or segments to bemade. Usually it is our present practice first toassess a patient by using oxygen-15, which enablesthe ventilation and blood flow in different zonesof the lungs to be compared without any intuba-tion of the patient (Dyson, Hugh-Jones, Newbery,and West, 1958 ; Dyson and others, 1960) andthen, if required, bronchoscopy can be done andthe anatomical localization of the variations inventilation, blood flow, and mechanical changesinto the relevant lobes or segments attempted.The two techniques of using short-lived gaseousisotopes and continuous gas analysis at broncho-scopy are thus conveniently complementary.
SUMMARY
The technique of continuous gas analysis fromindividual lobes and segments of the lungs duringdiagnostic bronchoscopy is described. This isachieved by inserting a sampling tube, from a
special mass spectrometer, into the regionalbronchus. The gas analysis is presented on a
four-channel direct-writing recorder.
It is shown how simultaneous records of thelocal changes in oxygen, carbon dioxide, andargon (following introduction of argon into thebronchial tree) give characteristic patterns fromwhich the presence of partial bronchial obstruc-tion, arterial obstruction, or a combination of bothin different lobes or segments can be inferred.
We wish to express our thanks to the MedicalResearch Council for supporting this work; to MissHeather MacLeish, Sisters N. M. Cooke and P. A.Stock, and the nursing staff working in the Departmentof Medicine of the Postgraduate Medical School fortheir help during the development of these techniques;and to Mr. Len Smith for his skill in constructingthe various bronchoscopic sampling tubes which weredesigned for use with the spectrometer.
REFERENCE3Dyson, N. A., Hugh-Jones, P., Newbery, G. R., and West, J. B.
(1958). Tne Preparation and Use of Oxygen-I 5, with ParticularReference to its Value in the Study of Pulmonary Mal-function.In Proceedings of Second United Nations International Confer-ence on the Peaceful Uses of Atomic Energy. Vol. 26: Isotopesin Medicine, p. 103. Geneva.
Sinclair, J. D., and West, J. B. (1960). Br-it. uused. J.,1, 231.
Fowler, K. T. (1957). A Mass Spectronmeter for Rcapid anid Conl-tinuous Analysis of Gas Alixtures in Respiratory Research. Ph.D.thesis. London University.and Hugh-Jones, P. (1957). Brit. nted. J., 1, 1205.
Macleod, W. M. (1954). Thorax, 9, 147.Mattson, S. B., and Carlens, E. (1955). J. thorac. Surg., 30, 676.Miller, R. D., Fowler, W. S., and Helmholz, H. F. (1956). J. Lab.
clin. Med., 47, 297.Svanberg, L. (1957). Scand. J. clin. Lab. Invest., 9, Suppl. 25.West, J. B. (1960). J. appl. Ph tsiol. In the press.
and Hugh-Jones, P. (1959). Ibid., 14, 743.- Fowler, K. T., Hugh-Jones, P., and O'Donnell, T. V. (1957).
Clin. Sci., 16, 529.
164
on January 13, 2022 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.154 on 1 June 1960. Dow
nloaded from





























